
Abstract
To determine whether emergency department patients want to share their medical records across health systems through Health Information Exchange and if so, whether they prefer to sign consent or share their records automatically, 982 adult patients presenting to an emergency department participated in a questionnaire-based interview. The majority (N = 906; 92.3%) were willing to share their data in a Health Information Exchange. Half (N = 490; 49.9%) reported routinely getting healthcare outside the system and 78.6 percent reported having records in other systems. Of those who were willing to share their data in a Health Information Exchange, 54.3 percent wanted to sign consent but 90 percent of those would waive consent in the case of an emergency. Privacy and security were primary concerns of patients not willing to participate in Health Information Exchange and preferring to sign consent. Improved privacy and security protections could increase participation, and findings support consideration of “break-the-glass” provider access to Health Information Exchange records in an emergent situation.
Keywords
Introduction
A Health Information Exchange (HIE) is a secure repository of electronic health records (EHRs) organized by collaborative agreements between health systems, providers, and payers with the goal of providing access to critical elements of patients’ medical records across multiple providers. The goals include expediting patient care, improving safety and quality, and care coordination. HIEs can also serve as a resource to track population health and public health. While HIEs vary in the information available, they typically allow providers to access a patient’s treatment notes from other providers in other systems and integrate their own treatment plan with a patient’s previous care plans in real time.
In emergency medicine, it is of particular importance to have easy access to a patient’s prior health records as decisions about both testing and treatment need to be made in real time, usually without input from the patient’s regular providers. While information that patients and family members may provide, if able, is vitally important, it is often incomplete. 1 It is notable that one-third of patients making a repeat visit to an emergency department (ED) also return to a different ED 2 where the records from their initial visit are not available. Access to information about current medications, recent electrocardiograms (EKGs), imaging results, and laboratory tests is hypothesized to improve the efficiency of an emergency evaluation, save time, and reduce costs, radiation exposure, and the potential for medical errors. 3 Without this access, EDs perform more tests to diagnose a patient’s condition, which is not only expensive to the healthcare system but also increases a patient’s exposure to harmful radiation. 4 Indeed, HIE has been shown to reduce repeat imaging and laboratory tests by 25 percent.5,6
Although much has been published about provider perspectives6–8 and workflow integration issues,9,10 less is known about patient preferences and concerns regarding the sharing of their personal health information across different health systems via an HIE. Prior surveys and focus groups have evaluated patients’ opinions regarding sharing their records for research purposes,11,12 but only a few studies have evaluated patient understanding of the risks and benefits of sharing their personal health records with their own healthcare providers for care coordination purposes through an HIE.13,14 Knowledge of how patients perceive HIE can inform partnerships and data sharing agreements between HIEs and providers and payers which are required for successful HIE implementation.
The goal of this investigation was to survey ED patients who would be eligible to participate in an HIE being established in the area to determine (1) whether they currently have healthcare visits in multiple hospital systems in which their providers could benefit from information sharing, (2) whether they want their providers to share their health records across systems in the setting of an emergency visit, and (3) whether they prefer to sign consent or have their health records shared automatically.
Methods
Study design and population
Adult patients presenting to a large, urban, academic, tertiary hospital-based ED in the United States between the hours of 7 a.m. and midnight between 28 April and 11 August 2015 were approached by research assistants and verbally consented to participate in a brief questionnaire-based interview. This ED sees about 65,000 patients annually and is part of a three-hospital system with an extensive network of outpatient primary and specialty clinics. The patient population is primarily English speaking and predominantly insured through either commercial or public plans. ED physicians belong to a single salaried group. The system is in the process of converting to one electronic record system across all settings, but to date records can be shared for ED visits and discharge summaries between the three hospitals, but not for outpatient visits or the majority of inpatient notes.
Survey content and administration
The survey instrument (Supplementary Appendix 1) was designed to gather data on patients’ needs and interest in care coordination, including preferred methods of contact, medication risks, and opinions about HIE. The opinions about HIE form the basis for the data presented in this study. Questions were largely multiple choice, but two open-ended responses were included to preliminarily explore thought-processes when certain responses were chosen. The study and survey instrument were approved by the local institutional review board with a waiver of written consent.
Specific to the goals of this study, patients were asked questions to gauge whether an HIE would be relevant to them, including whether their usual provider used EHR, and whether all of their healthcare was in the same health system where the survey was conducted or whether they had also visited providers in other health systems. Patients were asked whether they expected their ED providers to be able to see their records from their other providers. Regarding HIE, patients were asked whether they would be willing to share their own health data in an HIE, and if so, which types of records they would want to share through an HIE. They were also asked, “Would you want your records to be shared automatically or would you prefer to sign permission before sharing your records?” A 10-percent sample of patients who said they preferred to sign permission were asked “In the case of a medical emergency where you were not able to give consent, would you want the doctors caring for you to be able to access your records automatically from other doctors and hospitals where you receive medical care?” to see whether they changed their answer from preferring to give consent to wanting their records shared automatically in the case of an emergency.
Demographic information was collected along with questions about general comfort with technology. Patients were asked whether they owned a text-capable cell phone, whether they were comfortable sending text messages, whether they had Internet in their home, and whether they sent emails. To minimize question fatigue and the burden on patient time, the patient’s race and insurance were collected from the EHR. Based on the hypothesis that patients using controlled substances may wish to withhold that information from their providers, the survey also included the three-item Alcohol Use Disorders Identification Test (AUDIT-C). 15 If patients gave consent, their current medication record was also reviewed in the EHR to collect their actual use of controlled prescription medications (opiates and benzodiazepines).
After the authors piloted the survey with a small cohort of patients, questions were changed slightly to address common areas of confusion and create the final survey instrument used in this study. The choice “I don’t know” or “unsure” was added as a possible response to whether the patient’s primary physician used EHR. An initial third choice about whether patients would want to give consent once for HIE or would prefer to be re-consented each time their records were accessed through HIE was simplified to preference for either consent or no consent.
Patients who were under the age of 18 years, pregnant, or in police custody were not approached. Patients who were in mental or physical distress, with critical illness or injury, unable to provide informed consent due to intoxication, delirium, or other cognitive impairment, or non-English speaking were also excluded. Age was determined from the EHR. Police custody was visibly apparent from the presence of a police escort and/or handcuffs on the patient. Pregnancy and cognitive impairments were ascertained by asking the the patient’s care provider. Eligibility was determined using an eligibility checklist. Consistent with Institutional Review Board (IRB) approval, verbal consent was obtained from all patients prior to the interview and patients were free to decline to participate, skip questions, or to stop their participation at any time. In order to comprehensively document participation rates, all patients presenting to the ED during the study period were entered in the study database, including those who declined to participate or met exclusion criteria.
The 12 research assistants are post-baccalaureate or undergraduate premedical students who are based in the ED and received training from two program coordinators on research ethics, obtaining informed consent, and survey delivery, as well as specific piloting of the survey instrument used in this study.
Data analysis
Chi-squared univariate tests compared willingness to share data in an HIE by patient demographic characteristics and other responses. A multivariable logistic regression analysis was then conducted to identify patient characteristics associated with willingness to share data in an HIE. We included variables with univariate p value <0.1 adjusted for all hypothetically relevant patient characteristics including age, race, educational level, use of technology, controlled substance use, and having healthcare providers outside of the health system in which the study was conducted (relevance of HIE). All analysis was performed using Stata (13.1, College Station, TX).
Results
Of 1152 potentially eligible ED patients approached, 1017 (88.3%) agreed to participate in the verbal questionnaire. Of these 1017, 982 (96.6%) responded to our primary outcome question of whether or not they were willing to share their data in an HIE and are therefore included in the analysis. Reasons recorded for not approaching patients (N = 321) included the patient was sleeping (N = 203; 63.2%), too ill or in too much pain (N = 105; 32.7%), under the influence of drugs/alcohol (N = 3; 0.9%), cognitively impaired (N = 5; 1.6%), or non-English speaking (N = 5; 1.6%). Of those who completed the survey (N = 982), 850 (86.6%) gave permission for medication review in their charts and 827 (84.2%) answered all questions included in the multivariable analysis.
Table 115,16 presents the demographics of the 982 participants, along with a univariate analysis of the association between these characteristics and their willingness to share data in an HIE. The median age of participants was 53 (interquartile range (IQR): 35.5–64). Of the patients who reported having outpatient providers in the same hospital system as the ED (N = 903), 883 (97.8%) expected their emergency physicians to be able to see their records from those outpatient physicians. While 492 of all 982 participants (50.1%) stated that all of their care was in the same hospital system as the ED, 770 (78.4%) reported having seen healthcare providers in other systems at least once.
Univariate analysis of willingness to share health data in an HIE by patient demographics (N = 982).
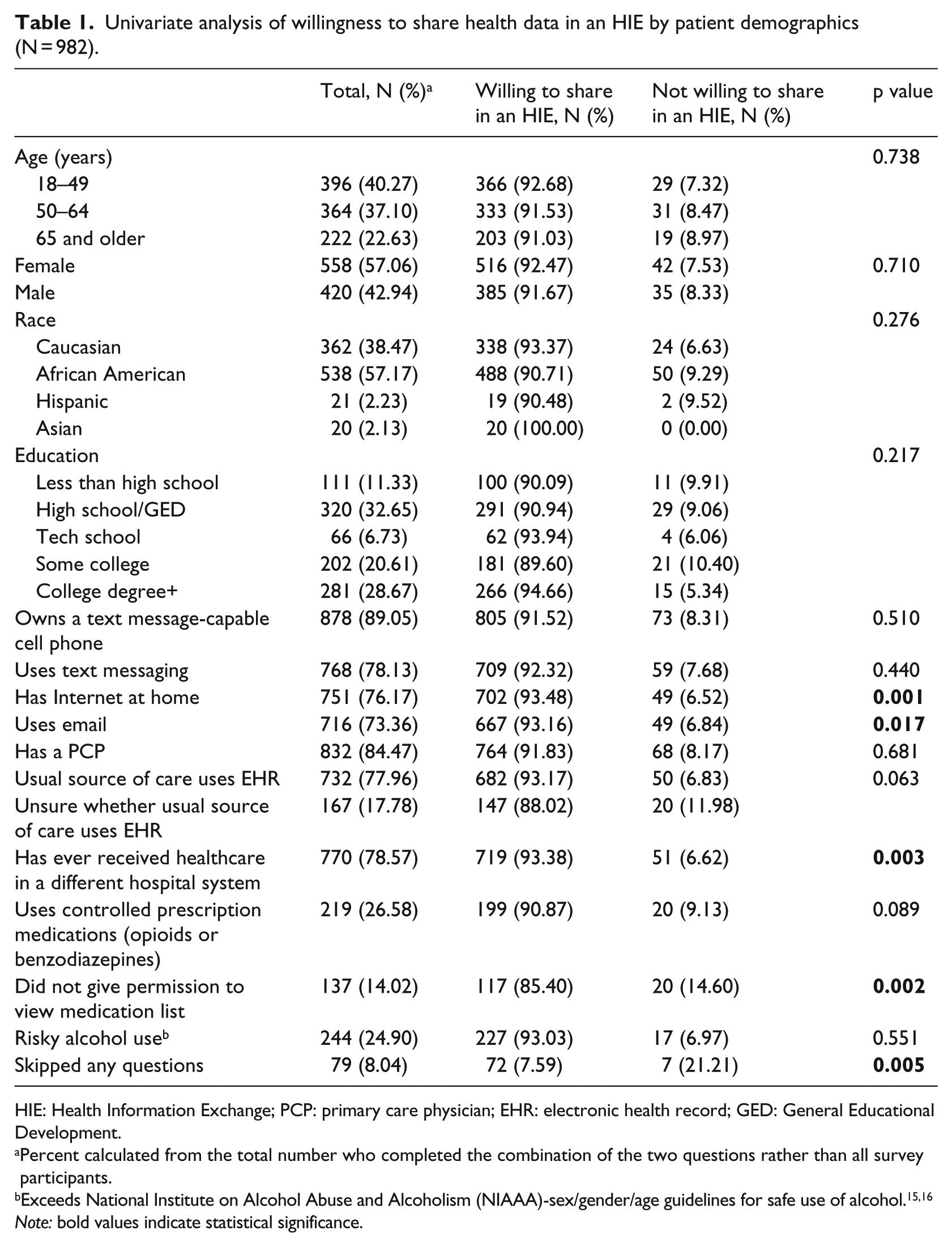
HIE: Health Information Exchange; PCP: primary care physician; EHR: electronic health record; GED: General Educational Development.
Percent calculated from the total number who completed the combination of the two questions rather than all survey participants.
Exceeds National Institute on Alcohol Abuse and Alcoholism (NIAAA)-sex/gender/age guidelines for safe use of alcohol.15,16
Note: bold values indicate statistical significance.
The vast majority (N = 903; 92.0%) were willing to share their data in an HIE. Patients who were not willing were also less likely to have Internet at home, to use email, to have ever visited a provider outside of the hospital system, to not skip any questions, or to allow researchers to view their medication list in their EHR. Short qualitative reasons given by patients for not being willing to share their data in an HIE included concerns about privacy and confidentiality, security of their information, a belief that HIE would not benefit them because all of their care was already in one system, and a concern for not wanting to be locked out of insurance due to pre-existing conditions (Table 2).
Reasons for not wanting to share health data in an HIE (N = 76; 7.7%).
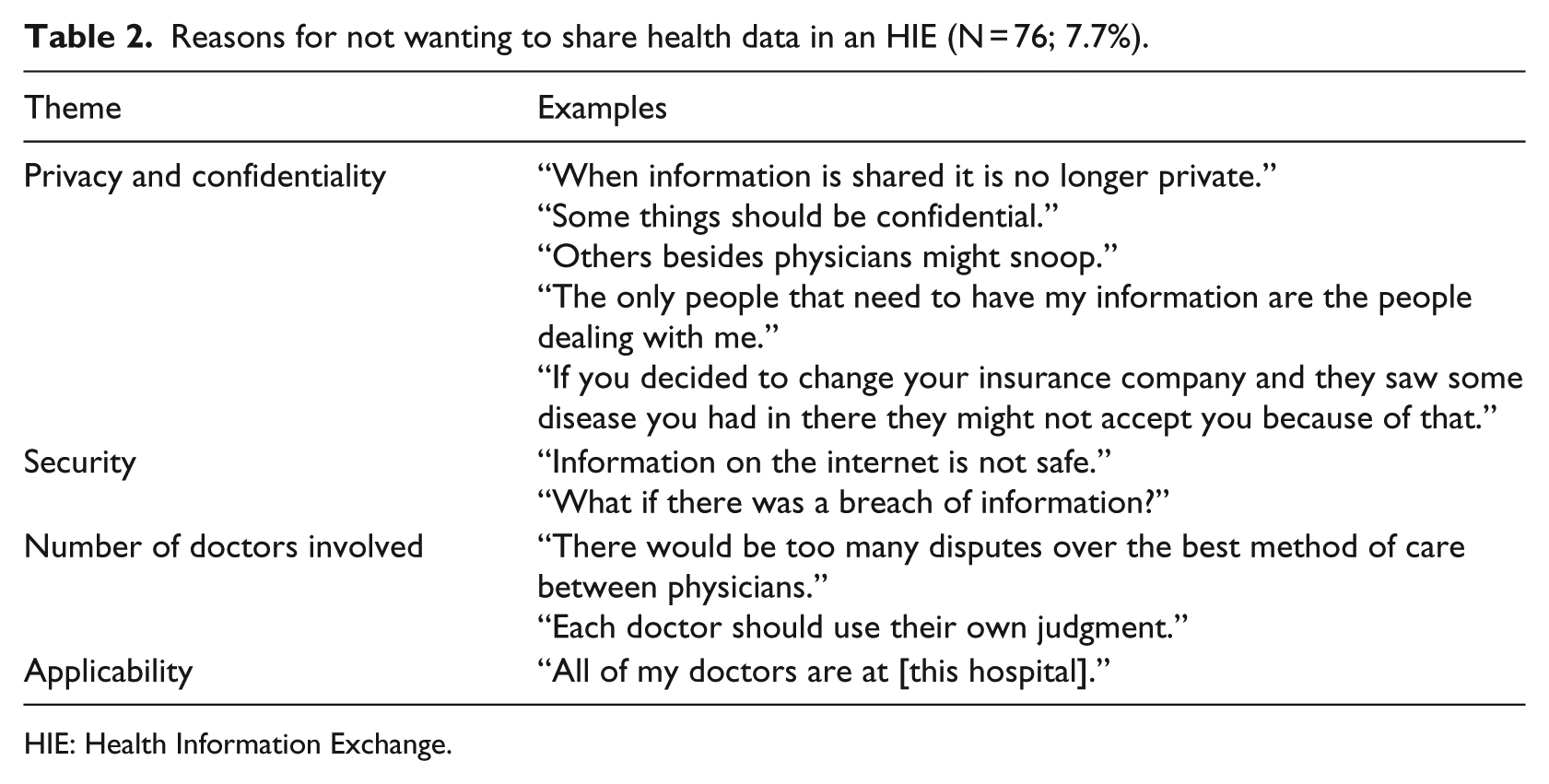
HIE: Health Information Exchange.
Of those who wanted to share their health records through an HIE who also answered the question about consent (N = 897), 410 (45.7%) wanted their records shared automatically, whereas 487 (54.3%) wanted to sign consent before sharing their records. In all, 44 patients who were not willing to share their data in an HIE also answered the method of consent question, and three (6.8%) wished to share their records automatically if participating. Reasons patients gave for preferring to sign consent included privacy, awareness and control over who accesses their information, desire to keep some information secret from some doctors or hospitals, and desire to seek treatment only at one hospital system (Table 3). Patients willing to share their information automatically cited convenience, better quality of care when their providers had their information, and the possibility that they would be unable to sign in an emergency. Among the subset of patients who preferred to sign consent and were asked the follow-up question about emergency situations (N = 100), 90.0 percent said records should be shared automatically in the situation that they were unable to give consent.
Reasons for wanting to give consent to share health data in an HIE (N = 533; 56.2%).
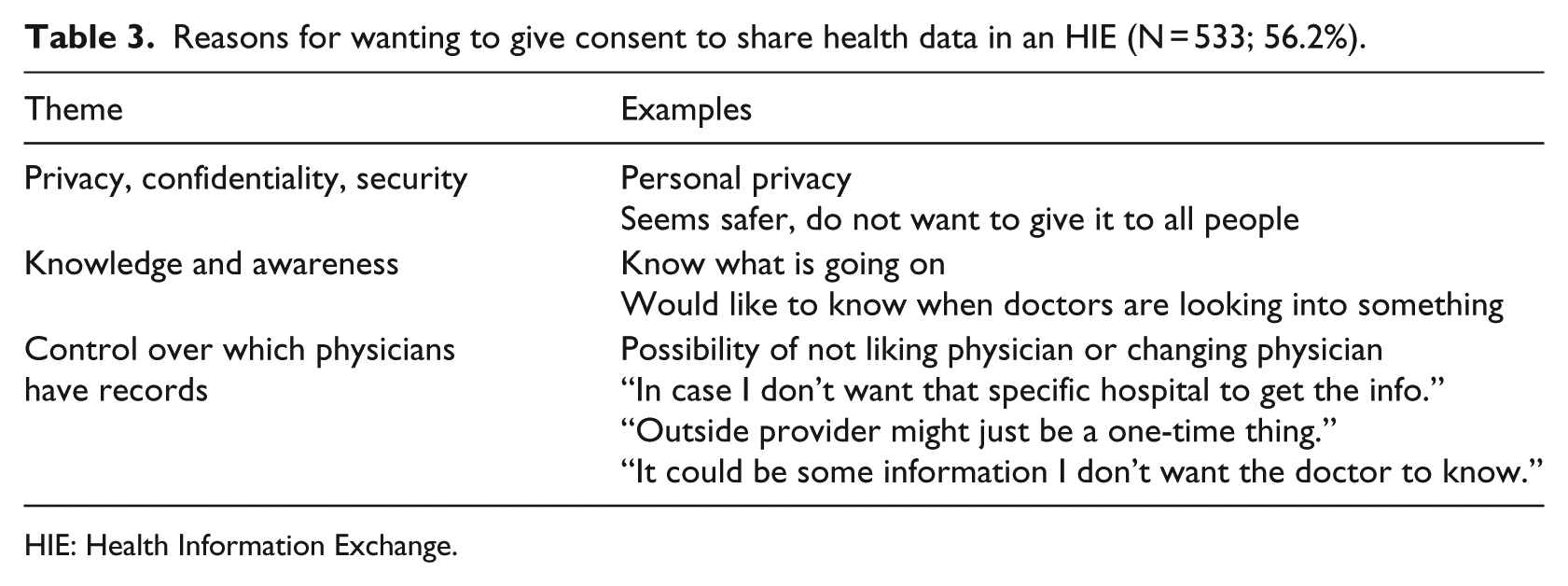
HIE: Health Information Exchange.
Almost all participants (N = 922; 94.0%), including 19 who were not willing to share their data in an HIE, wanted all possible records shared with their emergency physicians in an HIE, including physician notes, laboratory results, imaging results, hospitalization records, a medication list, a list of their medical problems, and a surgical history.
Results of an adjusted multivariable analysis are presented in Table 4. Patients who had never received care in another health system, who refused access to their electronic medication list, and who were uncertain whether their primary source of care used EHR remained significantly less likely to be willing to share their data in an HIE. Patient race, education level, adoption of technology for personal use, and abuse of alcohol or use of controlled prescription medications were not significant predictors of willingness to share health data in an HIE.
Multivariable model of factors associated with willingness to share health data in an HIE (N = 827).
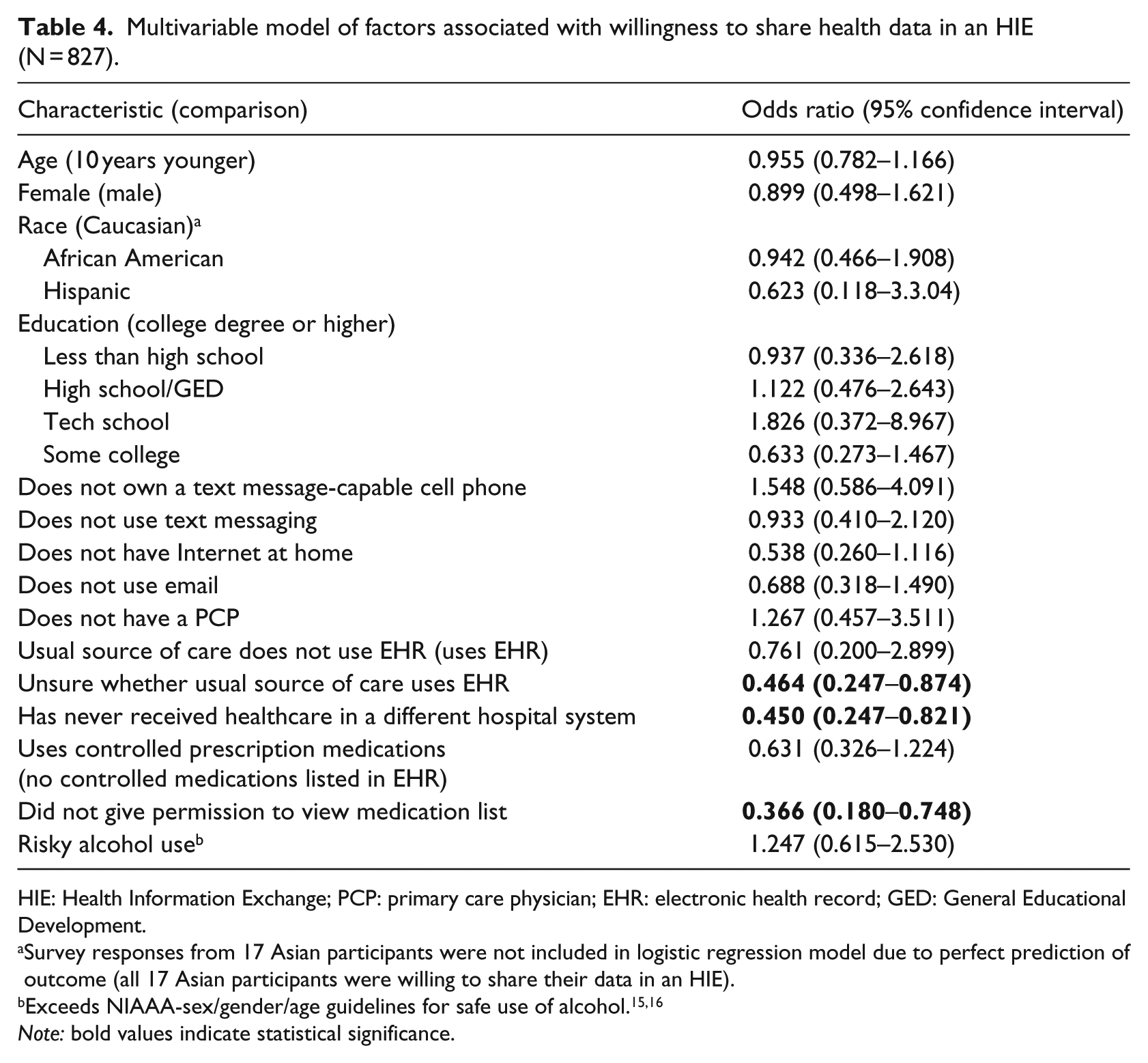
HIE: Health Information Exchange; PCP: primary care physician; EHR: electronic health record; GED: General Educational Development.
Survey responses from 17 Asian participants were not included in logistic regression model due to perfect prediction of outcome (all 17 Asian participants were willing to share their data in an HIE).
Note: bold values indicate statistical significance.
Discussion
This study found that the majority of patients are in favor of HIE, but about half want to control who accesses their information through explicit consent. The majority desiring consent are willing to waive it in the case of a true emergency however. Patients wary of HIE or wanting to maintain consent were primarily concerned about the privacy and security of their personal health information although a few other themes were elicited.
This study of patient perspectives on HIE is unique in its recruitment of a large number of patients actively seeking emergency care, whereas most prior surveys have queried potential healthcare consumers in non-healthcare settings17–22 or in outpatient settings. 14 The ED in particular is a setting where patients see physicians they have never seen before who have no knowledge of their prior health history, giving HIE an especially high utility in the ED environment. The vast majority of ED patients surveyed were in favor of an HIE, higher than seen in prior studies.13,14,21–23 The approximately 8 percent who were not willing to share their data in an HIE were less familiar with technology and might be less comfortable with the concept in general. In addition, patients who did not give permission for research assistants to view their medication list were also less likely to want their medical records shared through HIE. This remained significant in multivariable analysis, but it is unclear whether this question tested general distrust of allowing others to view health records, or evasiveness specific to hiding use of controlled substances. Those who skipped questions on this survey were also less likely to want to share their records through an HIE. Unfortunately, only four participants who skipped questions had responses to all variables in the multivariable analysis, all of whom were not willing to participate in HIE, so we were unable to test this association more definitively, but it suggests that general distrust or desire to keep personal matters private was a primary factor.
Patient comments from Tables 2 and 3 highlight distrust about sharing personal health information and electronic data security. Many patients feared that staff members besides their providers or insurers would abuse HIE to access their records inappropriately. Several prior studies have shown that security and privacy are major barriers for patients, 3 and a study that gathered multiple stakeholder input in Taiwan found that patients have greater concerns about privacy than do physicians. 24 This study shows that this disconnect also needs to be addressed in the United States. One patient was also fearful of an insurer denying them coverage based on the HIE information, indicating that either patients are not aware that the Affordable Care Act outlawed denial of coverage for preexisting conditions, or that they do not trust its ability to enforce that rule. Patients also do not seem to recognize how much information their insurers already receive about their diagnoses and medications in order to process their claims.
In our study, patients were somewhat more likely (56% vs 46%) to say they preferred to provide consent before their records were shared via HIE as opposed to having them shared automatically. This is similar to prior surveys in other settings that have found 35–69 percent of participants wanting to sign consent for HIE participation.14,21 However, among the subset of patients who preferred to give consent that were asked a follow-up question, 90 percent indicated that they would want their ED doctors to automatically access their health records in a medical emergency if they were unable to give consent and no one else could be reached. While respondents might have felt pressured to change their response to please researchers when asked a second time, our results are consistent with a prior study where support for access to records without consent increased from 35 to 93 percent when participants were presented with a scenario in which they were in an emergency situation and unable to provide their own medical information, 21 and another study where 90 percent supported access when the question was phrased as a medical emergency. 17 This finding highlights the tension between the Healthcare Insurance Portability and Accountability Act (HIPAA), HIE, and emergency situations.
It is the current standard of practice that patients in emergency situations who are unable to provide informed consent are presumed to consent to life-saving treatment. Therefore, it could be argued that “break-the-glass” HIE access should be a part of any emergency care where patients are unable to sign consent for access to their medical records. Further public education is needed about the current situation in some HIEs where opting out makes any medical records invisible, even in the case of true emergency scenarios such as unconsciousness after car accidents or medical catastrophes such as heart attack or stroke where access to medical records could be life-saving.
Of the patients surveyed in this urban ED, four out of five said they had providers and hence medical records in another health system, including 61.6 percent of patients who also reported that all of their care was in the current hospital system. These results suggest that a highly functional and accessible HIE would be of benefit to a majority of ED patients. Consistent with patient comments that loyalty to the current hospital system obviated their need to participate in HIE, patients who reported that they had never seen providers outside of the hospital system were less likely to be willing to share their data in an HIE, a characteristic that remained significant on multivariable analysis. Public education on the likelihood of being taken by ambulance to an ED in a different health system in the case of a true emergency could also improve support for HIE access in EDs.
Most patients (97.8%) expected their emergency physicians could already see records from their outpatient physicians in the same system, but in the health system where this study was conducted, emergency physicians can only see occasional notes about phone conversations but not full physician visit notes due to a difference in EHRs between settings and EHR uptake by outpatient providers, highlighting a disconnect between public expectations and the actual state of integrated EHR in the United States where only 54 percent of office-based physicians have achieved meaningful use of EHR, 22 and many different EHRs may be utilized within the same health system without seamless information sharing. 25
Limitations
Although this study has a large sample size, it was performed at a single center and the results may not be generalizable to other areas of the country or to other ED populations. Nineteen percent (N = 190) of surveys had missing responses related to key variables and were therefore excluded from the final multivariable analysis, so there may be systematic differences between patients who answered all questions and those who did not. This was a qualitative study with both multiple-choice and open-ended responses, and not all open-ended responses were captured verbatim nor were they systematically coded. Future studies might consider a more in-depth discussion with the patients who are not willing to share their data in an HIE about their concerns, with coding of the exact responses to elicit themes. The study investigated patients’ reported willingness to share their data in an HIE, but did not actually ask them to enroll. People’s behavior in a real situation does not always match what they say they would do hypothetically. Although concerns regarding privacy were elicited from those not willing to share their data in an HIE and questions were asked regarding alcohol and controlled substance use, substance abuse, psychiatric history, and human immunodeficiency virus (HIV) or sexually transmitted infection history were not explicitly included in the choices of types of information to be shared through an HIE. Future research may wish to determine whether concerns about this type of more sensitive information increase overall privacy and security concerns. Nonetheless, results are strongly supportive of the acceptability of HIE to the ED population, particularly in a truly emergent situation.
Conclusion
Study results show that the majority of ED patients are in favor of HIE, and that consent to access HIE records should be explored for inclusion in the routine “permission to treat” forms that all emergency patients sign when seeking care in an ED. If patients opt-out, there should be an option that also gives patients the ability to make an exception (e.g. opt-in to HIE) in the case of life-threatening emergencies. The qualitative data support a need for patient education regarding the utility of HIEs and the role of insurers in HIEs, and a need for improvements in the security of HIEs and regulation on who can access HIEs.
Footnotes
Acknowledgements
The authors would like to thank Briah Paciotti, Sheila Kelly, Christopher Gibson, Kathryn Wanner, Cjloe Vinoya, Danielle Kovalsky, Felicia Wong, Anjerie Yohn, and the Emergency Medicine Academic Associate Program who helped conduct the surveys and enter the data. Research data and analyses are available upon request by contacting the authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The study was supported by a University of Pennsylvania grant (Rhodes, PI) from the Leonard Davis Institute of Health Economics, the Center for Clinical Epidemiology and Biostatistics, and the Center for Public Health Initiatives.