
Abstract
Menopausal transition and post-menopause constitute windows of increased vulnerability to depression. Recently, the Meno-D was introduced, a novel 12-item, with five distinct subscales. The aim of our study was to translate and validate the electronic version of the Meno-D among Greek post-menopausal women. Translation and back-translation were performed by an expert group, while face validity was assessed by five experts. Along with the Beck Depression Inventory-II, the Meno-D scale was distributed online to 502 post-menopausal women. A confirmatory factor analysis was performed to investigate construct validity and both convergent and discriminant validity were evaluated. The data analysis was performed using Statistical Package for Social Sciences and AMOS. The 5-factor model of Meno-D achieved adequate levels of goodness-of-fit indices, scoring lower values in discriminant validity examined with heterotrait-monotrait ratio and composite reliability. The significant correlation with the Beck Depression Inventory-ΙΙ revealed for all subscales was indicative of good convergent validity. An exploratory factor analysis was additionally performed, suggesting a 12-item tool comprising two subscales: (i) psychological and (ii) biological and achieving good levels of fit. Our data confirmed that the electronic version of Meno-D is a valid tool that can be used for screening and evaluation of depression in Greek post-menopausal women.
Introduction
In the course of the female reproductive life cycle, several stages have been described as windows of increased vulnerability to depression. 1 These include the luteal phase of the menstrual cycle, the peri-menopausal, and the post-partum period, indicating the multifaceted implications of the hormonal milieu in the pathogenesis of mood disorders in women. 1 Regarding menopause, recent longitudinal studies have identified the STRAW stages of menopausal transition and early post-menopause as the most crucial for the emergence of depressive episodes. 2
The most prevalent menopausal symptoms often causing women to seek treatment are hot flushes and night sweats, belonging to the cluster of vasomotor symptoms. 3 Other somatic complaints include pain, sleep disorders, fatigue, vaginal atrophy, and sexual problems. 4 Apart from the emotional burden, hormonal variations also directly impact women’s psychology, causing symptoms such as malaise, anxiety, irritability, mood swings, cognitive decline, and mental fatigue.5,6 All these factors combined lead to the soaring prevalence of significant depressive symptomatology, estimated at around 25% during post-menopause.7,8
The aforementioned figures highlight that depression constitutes a major challenge for peri-menopausal women, underlining the need to effectively screen this high-risk population for depression. However, existing depression scales fall short of assessing all aspects of this subtype of depression, perpetuating its underdiagnosis. For instance, the Beck Depression Inventory-ΙΙ (BDI-II) does not assess somatic symptoms, memory disturbances, or paranoid thinking. 9 These aspects of post-menopausal depression are equally left unaddressed by the Montgomery–Asberg Depression Rating Scale. 10 Similarly, the Menopause Specific Quality of Life questionnaire does not examine social withdrawal, concentration difficulties, and self-esteem. 11
Due to these limitations, Kulkarni et al. developed in 2018 the Meno-D, a novel 12-item questionnaire assessing five principal factors: sleep, somatic, cognitive, self, and sexual. 12 The “self” factor investigates levels of self-esteem, isolation, anxiety, and paranoid thinking, the “sexual” factor is focused on libido and energy levels, the “somatic” factor assesses weight changes and pain, the “cognitive” factor examines concentration and memory, and the last factor of “sleep” checks for sleep disturbances and irritability. According to the developers of Meno-D, this tool has good construct and convergent validity, with discriminant validity and reliability being equally satisfactory. Additionally, it can be self-administered or clinician-rated, constituting a valuable tool for rating peri-menopausal depression. 12 Furthermore, the Meno-D is a brief questionnaire, therefore time-saving and practical, significantly facilitating its daily use in clinical settings, as well as its electronic self-administration via web or mobile apps, like chatbots.
Considering the salutary properties of this novel screening tool and the pliable prospective benefits of its widespread use, enabling an earlier diagnosis and management of depression, this study aimed to translate and validate the electronic version of the Meno-D in a cohort of Greek post-menopausal women.
Methods
Data collection, participants, and Ethical approval
The study population included post-menopausal women fulfilling the STRAW criteria and having a satisfactory understanding of the Greek language. 13 Women having undergone surgical menopause due to hysterectomy, as well as those receiving hormone replacement therapy were excluded from this survey. Data was collected through a web-survey to the members of the Hellenic Menopause Society, via the official webpage of this Greek non-profit organization. After informing the eligible women on the aim of our study, we received their consent through completion of a web-based questionnaire.
The study was approved by the scientific council of the Hellenic Menopause Society and received the ethical approval of the Bioethics committee of the Aristotle University of Thessaloniki (5.172/28.2.2020). Moreover, it complied with all ethical guidelines for online researches suggested by the Association of Internet Researchers. 14 The participants’ anonymity was safeguarded by ensuring that the organization would not collect their IP addresses and that the confidentiality of this material would be maintained. Additionally, a brief yet fully informative note regarding the repository process of the data collected was included in the introduction section of the web-based questionnaire used.
Translation of Meno-D
Translation of the Meno-D was performed using the guidelines suggested by Beaton et al. 15 Initially, the English version of the Meno-D was translated into Greek and back to English by two independent translators. The back-translation of the Meno-D was then compared to the original version for any discrepancies. Subsequently, the Greek translation was assessed by a group of experts of the research team, including a general practitioner, a psychologist, a psychiatrist, and the two translators. 16 The group worked on the development of the final Greek version of the Meno-D. Pretesting of the new questionnaire was assessed through cognitive interviews with eight native Greek post-menopausal women not encompassed in the sample that were asked on their comprehension of each item. 17
Other measures
The Beck Depression Inventory-II (BDI-II) was also used to evaluate depressive symptomatology. The BDI-II is a 21-item self-report inventory which uses a 4-point Likert-type scale ranging from 0 to 3 and displays very good psychometric properties. 9 A summed score ranging from 0 to 63 assesses depression, with higher scores being indicative of higher levels of depression. The BDI-II has been translated and validated in Greek with high internal consistency (Cronbach alpha coefficient = 0.85). 18
Data analysis
Assessment of face validity was performed by a group of five experts including two obstetricians-gynecologists, one psychologist, one psychiatrist, and one general practitioner. 19 Consequently, the construct validity of the questionnaire was examined, through convergent and discriminant validity assessment. Absolute fit was measured using root mean square of error approximation and goodness-of-fit index with levels of acceptance being less than 0.08 and more than 0.9, respectively. 20 Incremental fit was calculated using comparative fit index, Tucker–Lewis index, and normed fit index, all of which were expected to be more than 0.9.21,22 Last, parsimonious fit was examined by chi-squared/degree of freedom which should be less than 5. Size of factor loading, average variance extracted (AVE), with a required value of more than 0.5, and composite reliability (CR), with a required value of 0.6 or more, were used to estimate convergent validity.23,24 Both AVE and CR were manually calculated. To further investigate convergent validity, correlation of the Meno-D score with the BDI-II was examined, the latter being considered as the gold standard for the assessment of depression. Discriminant validity was examined by the heterotrait-monotrait ratio (HTMT) of the correlations. 25 The discriminant validity (by the HTMT method) compared the model HTMT ratio to the threshold of 0.85. 26 The reliability of the entire scale and subscales was examined using Cronbach’s alpha coefficient. Values from 0.6 to 0.7 and from 0.7 to 0.9 were indicative of satisfactory and high internal consistency, respectively. Statistical analysis was performed with Statistical Package for Social Sciences version 25 and AMOS 25v.
Results
Participants’ characteristics
General characteristics of the study population (n = 502).
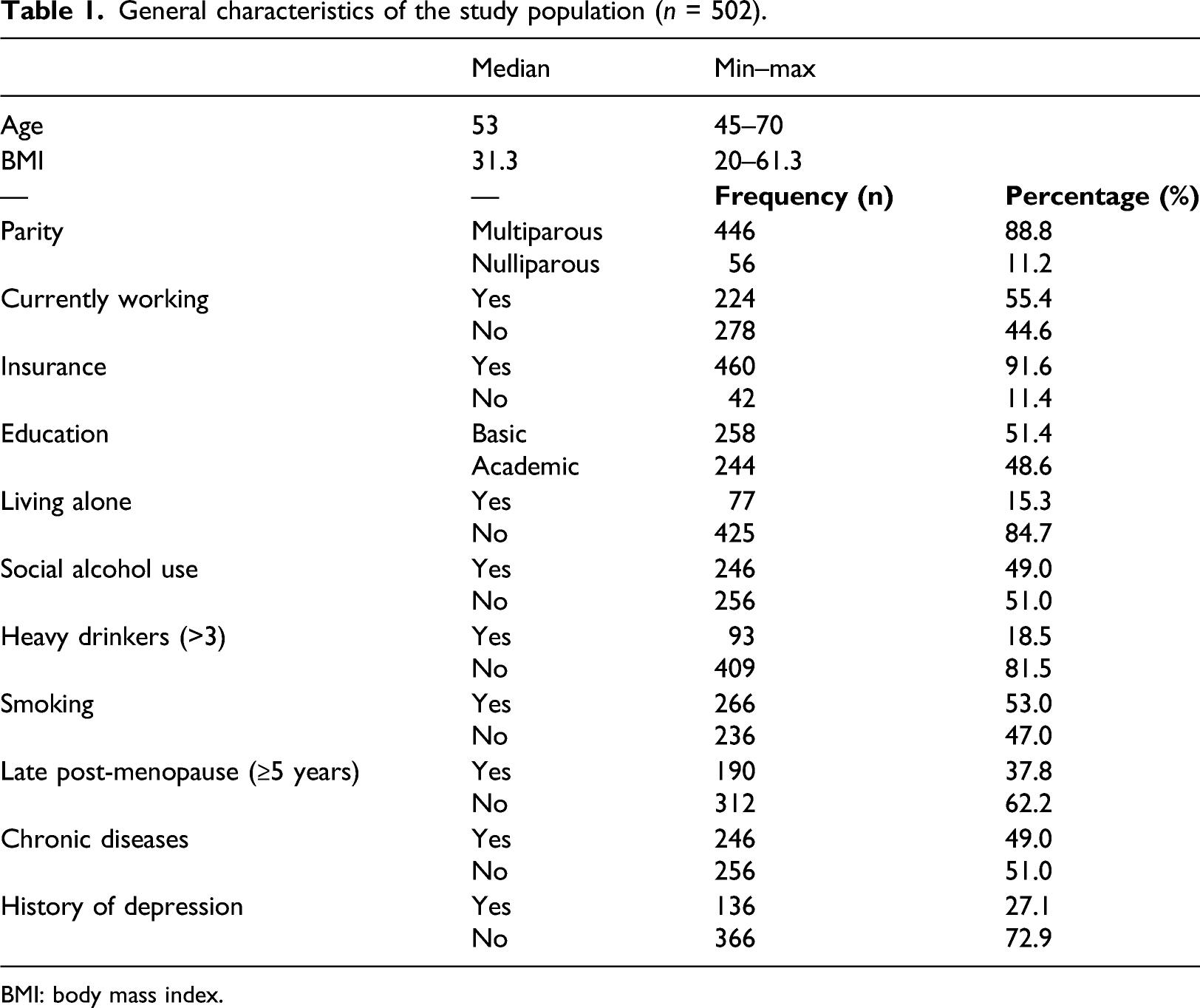
BMI: body mass index.
Construct validity
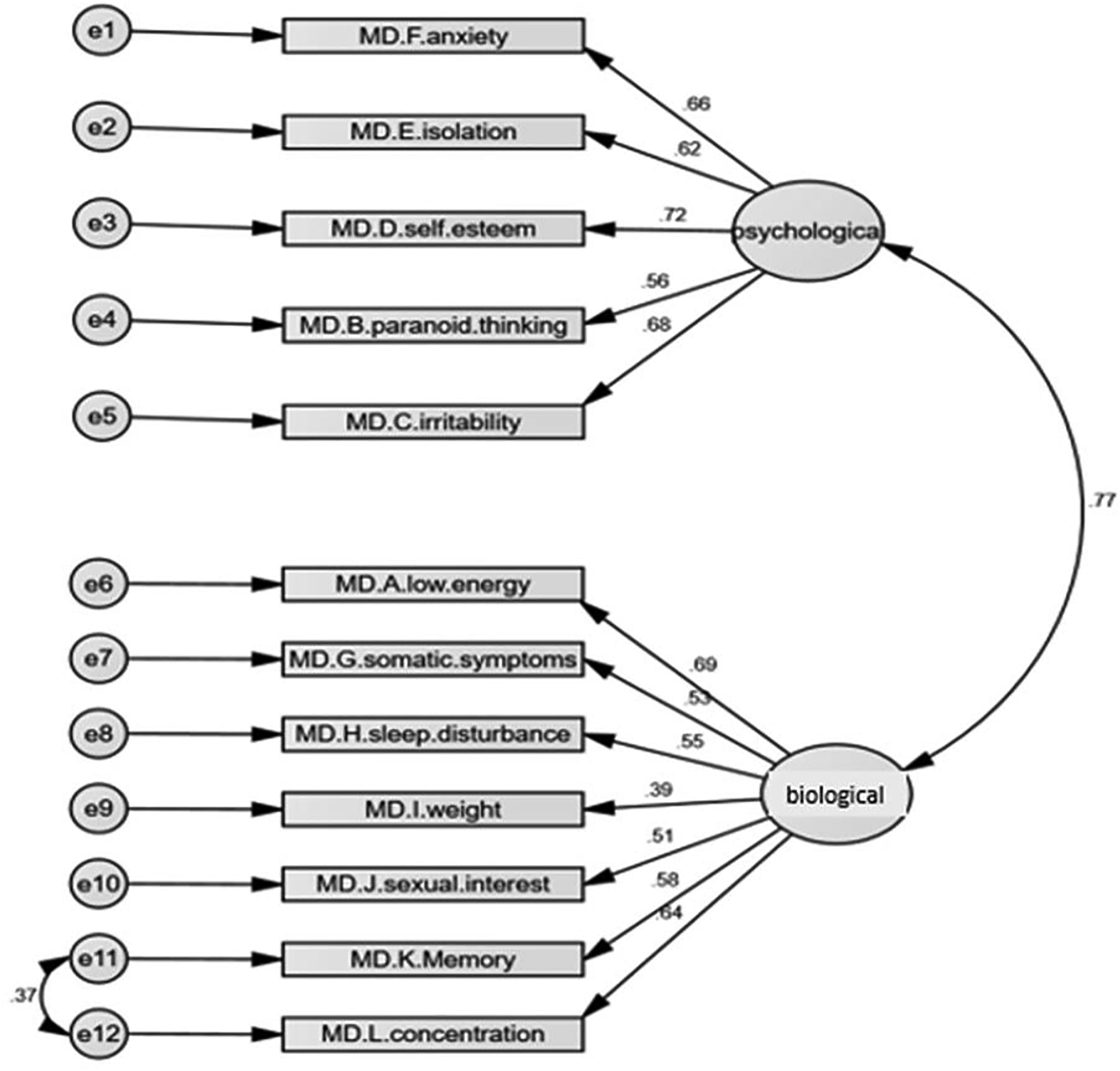
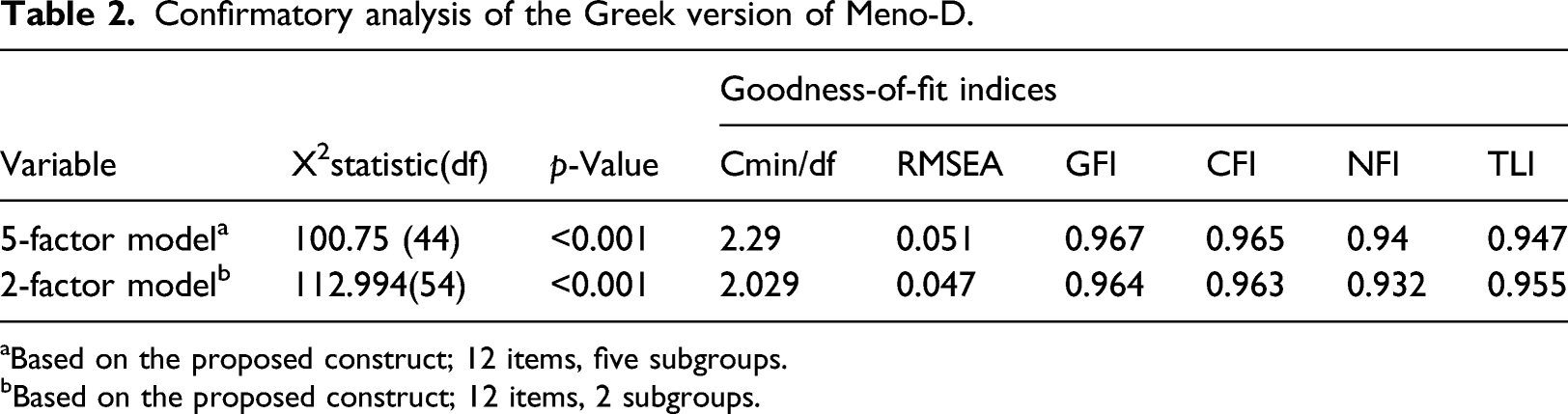
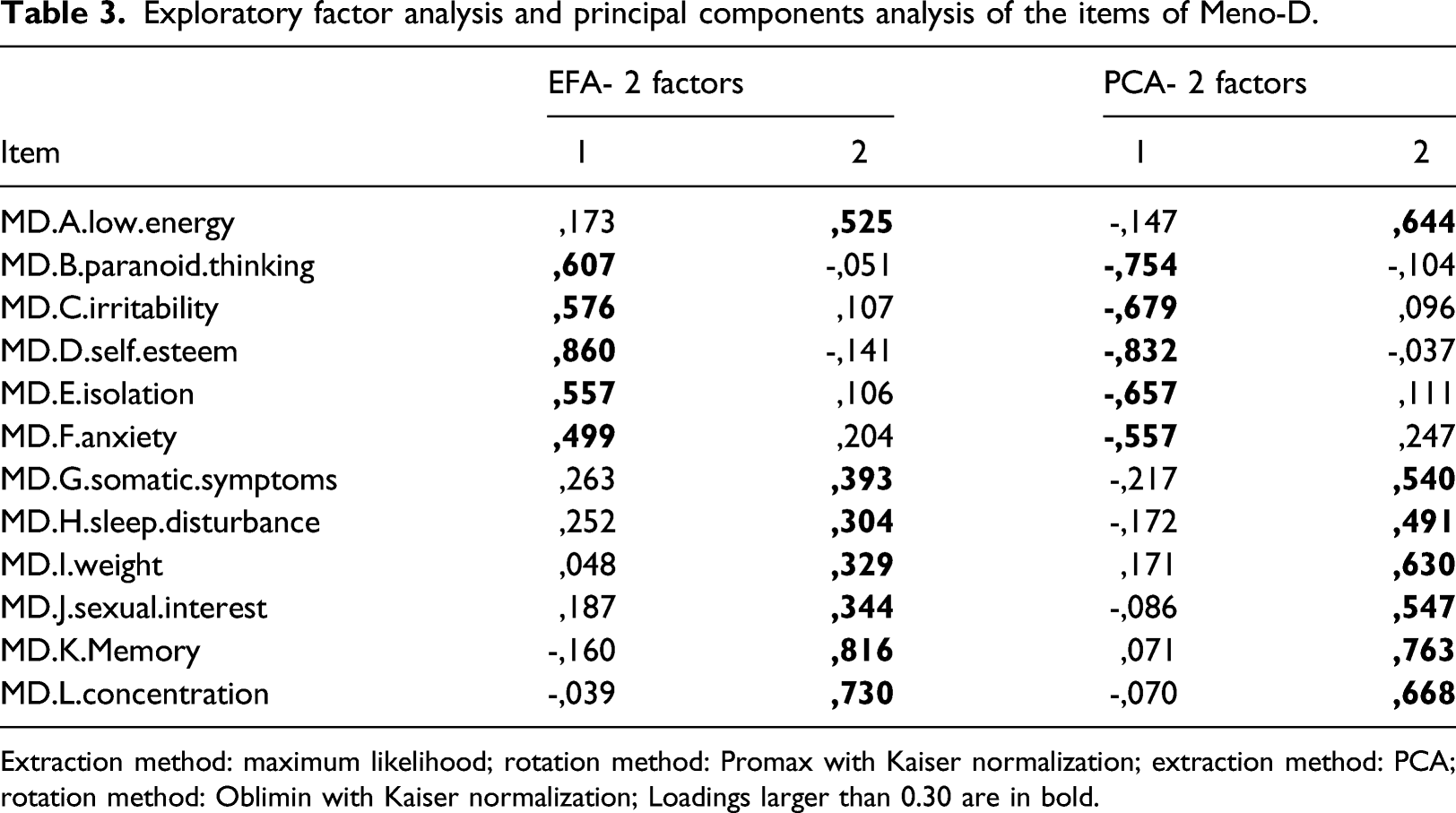
Regarding construct validity, the Greek version of the 5-factor model suggested by the developers was acceptable in terms of goodness-of-fit indices. However, additional principal components analysis (PCA) was performed in order to investigate the adapted version in the Greek population (Bartlett, x2:1654.165, p<0.001) explaining 47.85% of variance. The results of the analysis suggested a 2-factor model with increased factor loadings >0.5 for some items and lower correlation between constructs, while correlation between error of items 11 and 12 was allowed due to overlapping. Both models, along with factor loading, are shown in Figures 1 and 2, respectively. All goodness-of-fit indices for all models are presented in Table 2. Exploratory factor analysis (EFA) with promax rotation was also performed including all items. The Kaiser–Meyer–Olkin measure verified the sampling adequacy for analysis, KMO=0.891. Bartlett’s test of sphericity also indicated that correlation structure was adequate for analysis (x2:1654.165, p<0.001). The maximum likelihood factor analysis with a cut-off point of 0.30 and the Kaiser’s criterion of eigenvalues greater than 1 yielded a 2-factor solution as the best fit data. Similarly with PCA, the model accounted for 47,844% of variance. The results of both EFA and PCA are presented in Table 3. 5–factor model of Meno-D scale. 2–factor model of the Greek Meno-D scale. Confirmatory analysis of the Greek version of Meno-D. aBased on the proposed construct; 12 items, five subgroups. bBased on the proposed construct; 12 items, 2 subgroups. Exploratory factor analysis and principal components analysis of the items of Meno-D. Extraction method: maximum likelihood; rotation method: Promax with Kaiser normalization; extraction method: PCA; rotation method: Oblimin with Kaiser normalization; Loadings larger than 0.30 are in bold.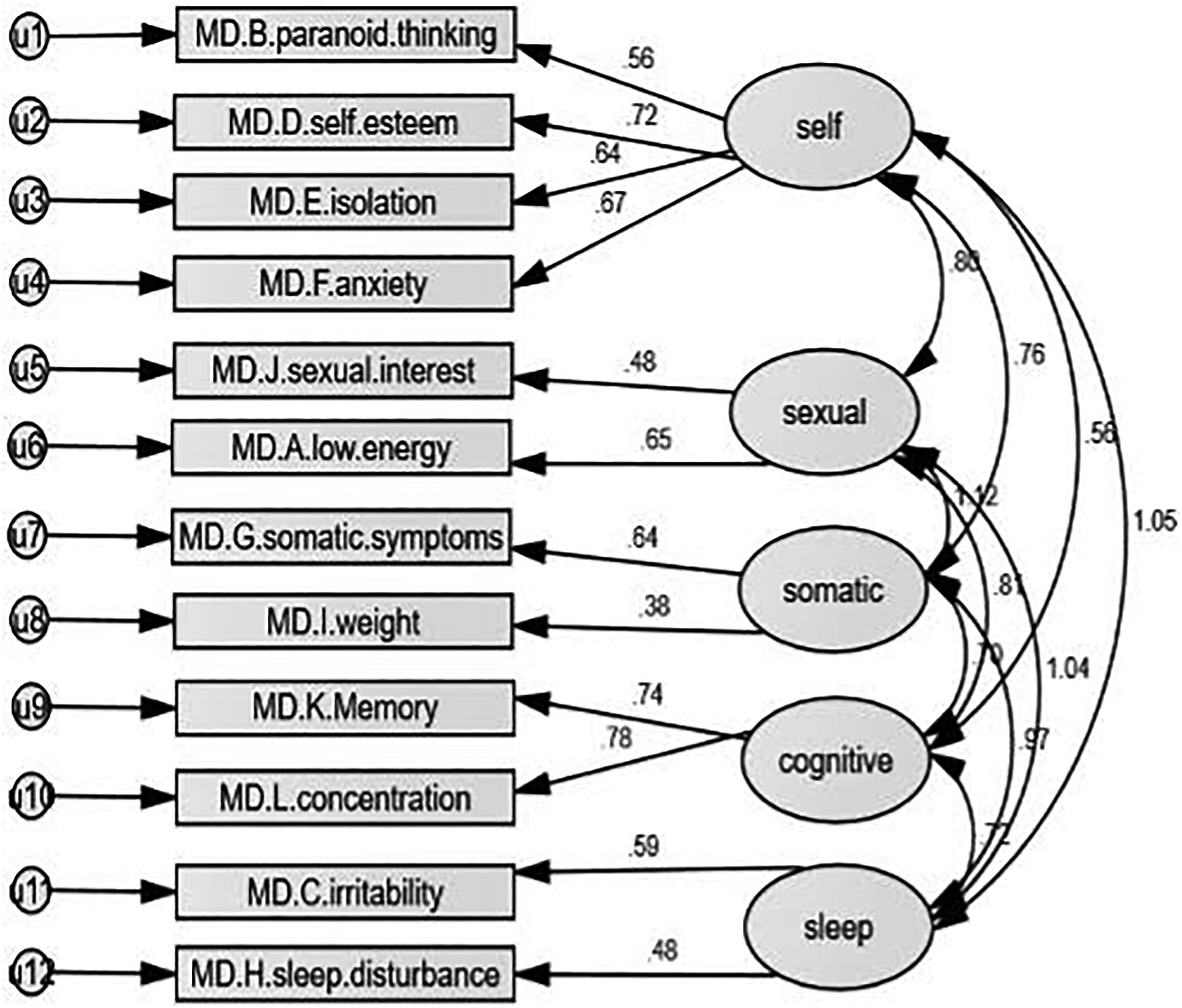
Reliability
Reliability and validity of the Greek Meno-D scale.
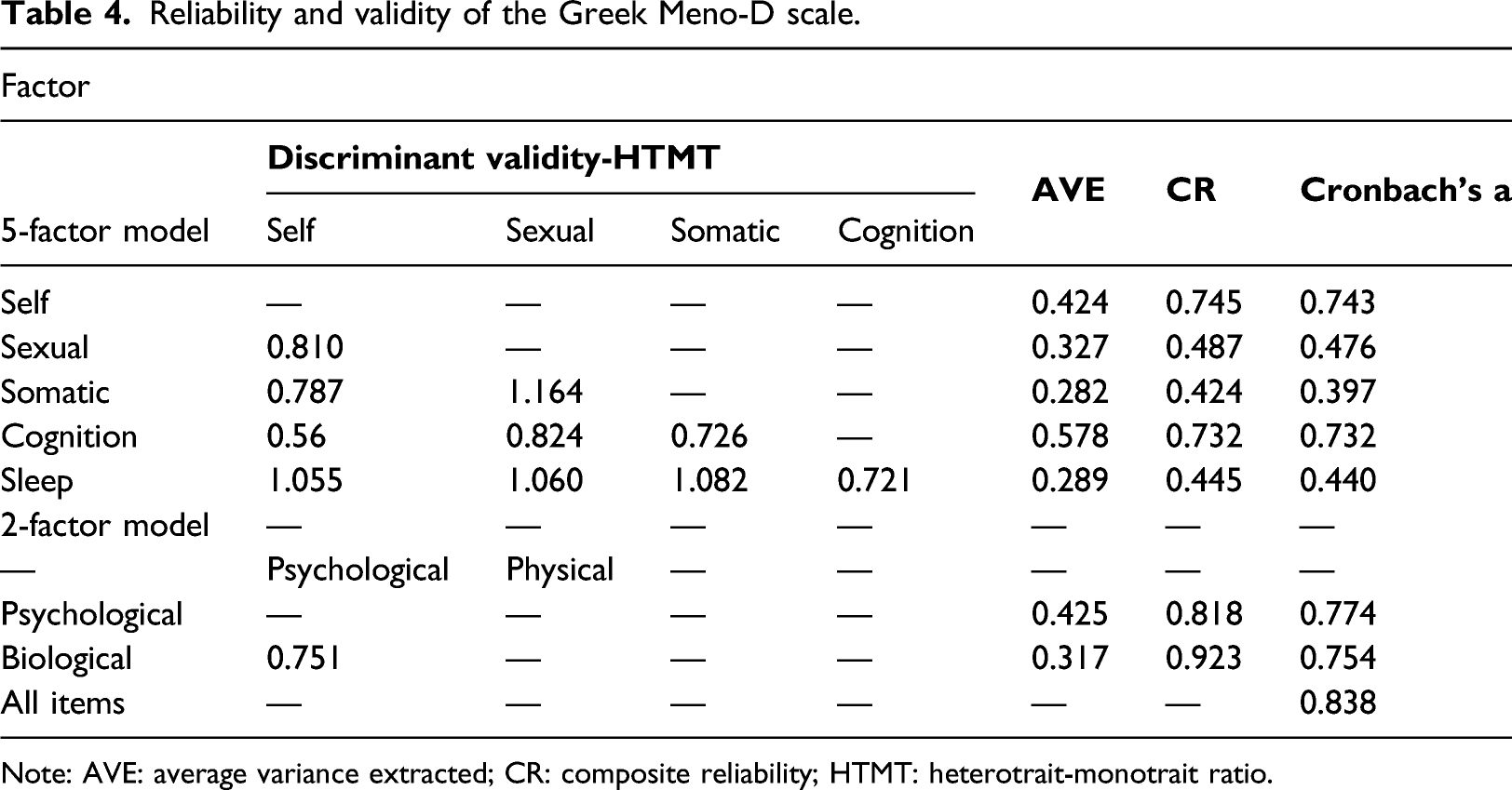
Note: AVE: average variance extracted; CR: composite reliability; HTMT: heterotrait-monotrait ratio.
Convergent and discriminant validity
Convergent validity of the Meno-D scale. Correlation of the Meno-D total and subscales with BDI-II.
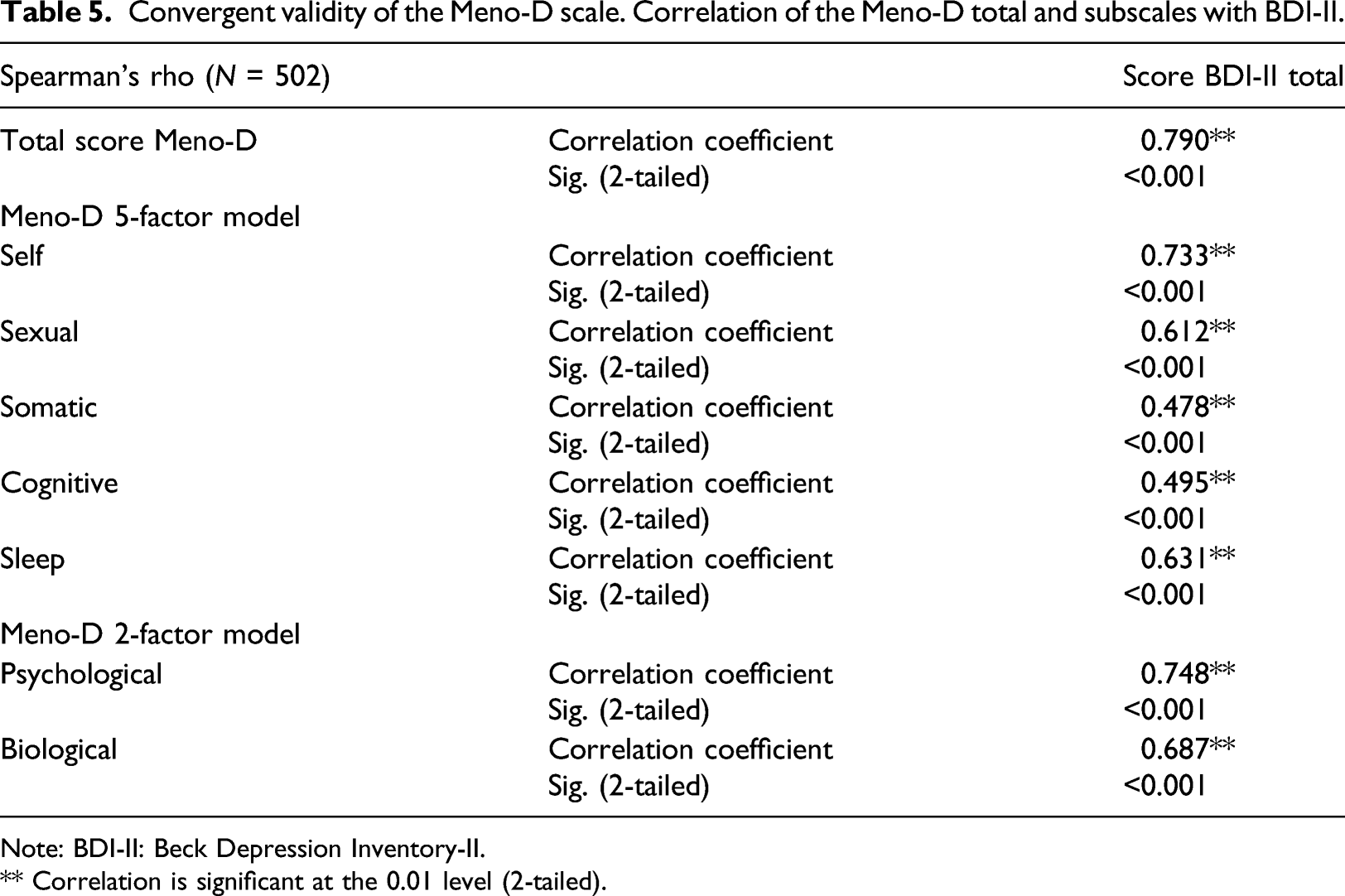
Note: BDI-II: Beck Depression Inventory-ΙΙ.
** Correlation is significant at the 0.01 level (2-tailed).
Discussion
This study supports the validity and high reliability of the translated and validated Greek electronic version of the Meno-D, rendering it eligible as an instrument for the detection of post-menopausal depression in the Greek population. To our knowledge, this is the first study to translate and validate Meno-D in a different language other than the original English version while being administered in a digital format. Moreover, the examination of convergent validity using the BDI-II revealed high correlation for both the 5- and the 2-factor models; the 2-factor model consisting of two subscales introduced by our team, achieved better levels of fit, discriminant validity, and reliability compared to the 5-factor model. On these grounds, we support using the Meno-D to detect depression in post-menopausal Greek women.
As already mentioned, it is estimated that about 1 in 4 women manifests depressive symptomatology in the post-menopause. 8 Symptoms may vary from major depressive episodes to cognitive decline 27 or even nonspecific somatic symptoms,28,29 further perplexing the diagnostic process. The principal causes for which menopausal women seek medical advice are somatic symptoms, which, however, very often overshadow underlying emotional complaints. 4 Physicians should be aware of this camouflaged type of depression and seek to screen high-risk groups for the presence of potentially concealed depressive symptomatology.
In general, all types of depression are significantly underdiagnosed, as family physicians fail to recognize 30–50% of patients presenting with major depressive disorder.30,31 This phenomenon is mainly attributed to time constraints and lack of expertise but mainly occurs when depression is disguised in the form of somatic complaints, 28 indicating the potentially larger underdiagnosis of menopausal depression. Moreover, many physicians erroneously underestimate this form of depression, falsely reassured that it is a transient state accompanying menopause. 32 More often than not, this is not the case, as depressive symptoms persist, necessitating their treatment with antidepressants rather than plain hormone replacement therapy.33,34 According to data from Australia, in 2015, the highest recorded suicide rate among females was recorded in the 45–49 age group, followed by the 50–54. 35 Alarmingly, these age groups coincide with the median ages of peri-menopause and menopause onset, estimated at 47.5 36 and 51.336,37 years, respectively, proposing the potential involvement of peri-menopausal depression in this morbid trend. These figures emphasize the imperative need to upgrade our screening tools, in order to effectively confront this hidden morbidity. Therefore, the inclusion of the Meno-D in our screening arsenal and the enhancement of physician awareness on the diagnostic challenges of menopausal depression may decisively contribute to the resolution of this multifactorial issue.
Regarding the structure of the questionnaire, the 5-factor model was adequately fit according to the constructors of this tool. 12 However, loading factors were low for sleep disturbance, interest, and weight (<0.5), while AVE and CR were low for all factors except self and cognition. These results, along with the fact that the Meno-D was applied in post-menopausal women to investigate depression, encouraged the conduction of PCA. The PCA resulted in a 2-factor model—psychological and biological—including all the questions. Therefore, the goodness-of-fit indices were high for the 2-factor model as well, while the model indicated good construct and discriminant validity and reliability. Loading factors for weight remained low, a fact also underlined by the scale developers. 12
Of note, our study participants exceeded 500, overcoming the limitations of the original validation study. 12 Moreover, the sample size exceeded the number of 10–20 samples per item suggested for validation studies. 38 On the contrary, a study limitation includes the absence of a retest reliability method examining consistency over time from our study design. However, a strength of our study was the fact that it was conducted digitally. Web-based, computerized data collection and management systems offer multiple benefits, being more cost-effective, reducing attrition, and enhancing data accuracy and reliability by minimizing the potential of human error occurrence.39,40 Recently, electronic patient-reported outcome measure systems have emerged as a way to collect high-frequency data directly from the patients outside the clinic. However, in order to be implemented in the clinical care context further validation is warranted. Similar studies have been carried out comparing paper and digital administration of several other validated PROMs with promising results both on terms of reliability and validation as well as feasibility and patient acceptance. Exploring the implementation and assessing the feasibility of an electronic version of the translated version of Meno-D may further increase the adoption and outreach of this tool in the Greek community.
To conclude, our findings suggest that the implementation of the Meno-D has the capacity to facilitate the remote assessment of post-menopausal depression among Greek women, even administered in a digital fashion. We recruited post-menopausal women, thus allowing for the assessment of the questionnaire on a population of increased vulnerability to the manifestation of depressive symptoms. The particular properties of post-menopausal depression highlight the intricate nature of this condition and indicate its diagnostic challenges, calling for the inclusion of more specialized instruments in the diagnostic approach of menopausal depression, such as the Meno-D.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.