
Abstract
Introduction
The rise in online health information access has shifted health-seeking behaviors, yet a validated tool to assess eHealth literacy for the Taiwanese context remains unavailable. This study aimed to translate the eHealth Literacy Scale (eHEALS) into Traditional Chinese and validate its factor structure and reliability among individuals with type 2 diabetes (T2D).
Methods
The original 8-item eHEALS was translated into Traditional Chinese (eHEALS-TC) using forward and backward translation techniques, with input from four experts in pharmacy practice and educational psychology. A cross-sectional study was conducted to examine the validity and reliability of the eHEALS-TC in adults with T2D who were taking diabetes medication. Participants were recruited from five community pharmacies in Taiwan between June 2023 and May 2024. The internal consistency of the eHEALS-TC was assessed using McDonald's omega (ω), while construct validity was evaluated through exploratory factor analysis. Criterion validity was determined by exploring the correlation between the mean total eHEALS-TC score and demographic factors, self-efficacy, health status, medication adherence, and A1C levels.
Results
A total of 273 patients participated in the study. Exploratory factor analysis revealed that all eHEALS-TC items were loaded onto a single factor, accounting for 84.95% of the total variance. The internal consistency reliability yielded a McDonald's ω of 0.974. The mean total eHEALS-TC score was positively associated with younger age (r = .382, P < .001), higher education attainment (rs = .525, P < .001), greater household income (rs = .359, P < .001), better self-reported health status (rs = .191, P = .002), stronger self-efficacy in medication use (r = .167, P = .006), and fewer barriers to medication-taking (r = .143, P = .018). However, no association was found between the mean total eHEALS-TC score and A1C levels (r = .048, P = .427).
Conclusions
The findings provide empirical evidence supporting the validity, reliability, and efficiency of the eHEALS-TC as a tool for assessing eHealth literacy among individuals with varying demographics and health conditions in Taiwan.
Introduction
Health literacy refers to the ability to search, understand, and apply health information and services to make informed health-related decisions. 1 The widespread availability of online health information has significantly influenced individuals’ health-seeking behavior, with many now turning to the internet as their primary source of information before consulting healthcare professionals. 2 This shift has broadened the availability of health information beyond traditional in-person sources to include a variety of health-related websites. 3 As online health resources expand, the number of people using the internet to search for health information has also increased. 4 However, because many online sources lack professional oversight, information quality can vary and lead to inconsistencies. 5 This abundance and diversity of information may contribute to health information overload. 6 For instance, the onset of the COVID-19 pandemic in 2020 saw an explosion of online disease-related content, resulting in an “infodemic.” 7 As a result, the health literacy skills traditionally used to interpret printed information have expanded to include electronic health (eHealth) literacy, which emphasizes digital health information over conventional resources like pamphlets and printed handouts. 8
eHealth literacy specifically involves the ability to seek, locate, understand, evaluate, and engage with electronic health information to address or solve health-related issues. 8 With the internet serving as a primary source of health information, 9 the global population of internet users reached 5.4 billion in 2023, representing 67% of people worldwide. 10 Research indicates that over half of mobile phone users have downloaded health-related applications, and approximately 70% of those users used them to track progress toward health goals in 2020. 11 The widespread availability and affordability of information and communication technologies have made eHealth a focal point for policymakers, practitioners, and researchers. 12 Digital health tools now include health applications, wearable devices, and online medical resources to support health management and informed decision-making. However, the growing need to adapt quickly to these digital tools depends on individuals’ access to technology and the skills necessary for effective use. 13 While these resources can be invaluable, their benefit relies on accessibility and perceived value. 14 Patients with limited eHealth literacy may find these tools less valuable or struggle to access them in their preferred language. 15 As a result, they are unlikely to use these resources, which can reduce their engagement in health management and hinder overall health improvement. 16 In this digital era, eHealth literacy has become essential for leveraging online health information to achieve better health outcomes. 17 Recently, it has been recognized as a super social determinant of health due to its far-reaching influence on broader social determinants. 16
Diabetes ranks as the eighth leading cause of death worldwide, 18 and its management presents significant challenging due to complex treatment regimens, individual variability in responses, and the need for sustained adherence to medication and lifestyle modifications.19,20 Approximately 50% of individuals with diabetes adhere to their treatment, with non-adherence contributing to suboptimal blood sugar control, an increased risk of complications, and higher healthcare costs. 21 Evidence from previous reviews underscores the effectiveness of eHealth programs in promoting physical activity and supporting improved self-management behaviors in diabetes care, such as adherence to medications and specific dietary recommendations.22–24 This suggests substantial potential for eHealth technologies to enhance patient health outcomes. Digital tools, for instance, could facilitate tracking medication intake, monitoring blood glucose levels, and encouraging healthy dietary habits, ultimately optimizing glycemic control (e.g., A1C levels) and reducing the risk of diabetes-related complications. 14 Furthermore, interventions that integrate digital tools have shown significant improvements in both eHealth literacy and self-efficacy. Enhanced eHealth literacy empowers individuals’ confidence in managing their health effectively, which highlights the connection between these skills. 25 Assessing eHealth literacy is an essential first step in identifying skill gaps. This allows for targeted support to assist individuals with low confidence in using eHealth resources, enabling them to maximize the potential benefits of these tools and engage more fully in health-related decision-making. 26 To realize these benefits, it is essential to identify and validate patient-reported outcome measures that assess perceived eHealth literacy skills. Such measures are critical for developing effective, patient-centered eHealth information strategies in the future. 27
The eHealth Literacy Scale (eHEALS) is one of the most widely used self-reported tools for measuring perceived eHealth literacy.16,28,29 The scale is grounded in the Self-Efficacy Theory and Social Cognitive Theory, which emphasize that competence and confidence are key precursors to behavior change and skill development.8,30 Specifically, the eHEALS is based on the premise that eHealth literacy is shaped by factors such as an individual's health issues, educational background, current health status, motivation for seeking health information, and chosen technologies. 27 The eHEALS has demonstrated reliability in multiple languages and has been validated across numerous countries. 28 Its psychometric properties have also been tested in various populations, including students, adults, and individuals with chronic conditions, as well as across diverse cultural backgrounds.16,26–28,31 While Koo et al. translated the eHEALS into Traditional Chinese, their study did not follow forward-translation and back-translation techniques, leaving the semantic equivalence of the Traditional Chinese version to the original English eHEALS unverified. 32 Furthermore, their study sample consisted of sixth-grade students rather than individuals who use electronic resources for health-related decisions, limiting the generalizability of the translation. Therefore, they recommended that future studies test the translated eHEALS with broader populations to improve its applicability. 32
Considering the limitations of the previous Traditional Chinese eHEALS translation, this study aimed to translate the eHEALS into Traditional Chinese and to evaluate its factor structure and reliability among individuals with type 2 diabetes (T2D) in Taiwan.
Methods
Study design and setting
This cross-sectional study included both translation and validation phases. After obtaining permission from the original author, 30 the research team translated the eHEALS into Traditional Chinese (eHEALS-TC) and subsequently evaluated its psychometric properties. Trained researchers administered the eHEALS-TC to eligible participants in person at five community pharmacies in northern and central Taiwan from June 2023 to May 2024.
Ethical consideration
This study protocol received approval from the Research Ethics Committee at the National Taiwan University Hospital (202303022RIND). Participants were informed about the research purpose and assured that their participation would remain anonymous. Each eligible participant was required to provide written informed consent before taking part in the study. All procedures were conducted in accordance with the Declaration of Helsinki.
Translation procedure of the eHEALS-TC
The eHEALS (Appendix A) was translated into Traditional Chinese following the Principles of Good Practice for the Translation and Cultural Adaptation Process for Patient-Reported Outcomes Measures. 33 Initially, two research team members, both native Chinese speakers fluent in English and practicing pharmacists in Taiwan, independently translated the original English version of the eHEALS into Traditional Chinese. This initial draft was then reviewed by a systematic expert panel, which included the two translators and two academic faculty members who specialize in pharmacy practice and educational psychology. The second draft was back-translated into English by a bilingual pharmacist with expertise in educational psychology. The four experts from the previous panel compared the back-translation with the original English version, identifying only minor discrepancies, thus ensuring content validity. Cognitive interviews were conducted with ten patients with T2D to confirm that all items were easy to understand, free of offensive language, and non-discriminatory in terms of age or gender. Data from these ten pilot patients were excluded from the study analysis. No issues were reported regarding comprehension or clarity during the completion of the questionnaire, and face validity was established. The final version of the translated eHEALS-TC (Appendix B) was then proofread before being distributed to study participants.
Validation procedure of the eHEALS-TC
The eHEALS-TC was included within a broader set of assessments for a project investigating psychosocial factors that may impact diabetes medication adherence. It was administered as a paper-based survey alongside other health measures in this study, recognizing that not all patients have easy access to the internet. Following the approach used by Norman et al. in their validation of the eHEALS, we adopted the same method for survey administration to ensure consistency with the original study. 30
Participant recruitment
We recruited eligible participants through convenience sampling who were 18 years or older, diagnosed with T2D, had valid A1C levels within the past six months, were prescribed at least one oral diabetes medication, and could read Traditional Chinese proficiently. The National Health Insurance MediCloud System was used to verify participants’ diagnoses (i.e., the International Classification of Diseases, Tenth Revision, Clinical Modification diagnosis code of E11.XXX), diabetes medications, and recent A1C levels. Individuals were excluded if they lacked active electronic health records, could not understand Traditional Chinese, or had cognitive impairments, such as dementia or Alzheimer's disease.
Two trained researchers handled recruitment and data collection. Pharmacists at the research site assisted in identifying and referring potential participants who were refilling prescriptions to the trained researcher. The trained researcher then took eligible patients to a private area, explained the study purpose and process, provided information sheets, and allowed them five to ten minutes for review. Interested participants were invited to sign an informed consent form and were given a copy of the unsigned form for their records. Following consent, researchers administered the survey and collected clinical data through the MediCloud System. Of the 315 patients approached, 273 (86.7%) enrolled and completed the survey. The survey was a paper-and-pencil format containing 46 items and took participants an average of seven minutes to complete. Once participants completed the survey, they received NT$200 (approximately US$7) in cash as compensation. This amount was determined in accordance with ethical research practices and local standards, ensuring it was neither coercive nor excessive.
Given prior research showing variations in eHEALS factor structures across different populations,28,30 we performed exploratory factor analysis (EFA) to investigate the psychometric properties of the eHEALS-TC. Although there is no definitive consensus on sample size for EFA, recommendations suggest a minimum of 20 subjects per variable, with at least 200 participants considered generally adequate for assessing psychometric properties of instruments measuring social constructs. 34 As the eHEALS-TC includes 8 items, these guidelines set a minimum sample size of 200 for EFA, with a larger sample size expected to increase statistical power.
Measures
Sociodemographic and clinical backgrounds
Collected sociodemographic data included age, gender, education attainment, and annual household income. Clinical information included the number of prescribed diabetes medication, diabetes control status, and self-reported health status. Diabetes medications were confirmed by cross-referencing participants’ medication histories with their electronic health records. Diabetes control was further evaluated using each participant's most recent A1C level from the past six months, as recorded in their electronic health records. Lower A1C values indicate better glycemic control, with an A1C of 7.0% or below recommended for individuals managing diabetes. 35 Self-reported health status was measured on a five-point scale running from poor to excellent (1 = poor, 5 = excellent). 36
The Traditional Chinese version of the eHealth Literacy Scale (eHEALS-TC)
We used the eHEALS-TC to assess participants’ combined knowledge, comfort, and perceived skills at finding, evaluating, and applying eHealth information for managing health issues. 12 The original eHEALS is a self-reported instrument that can be administered by healthcare professionals and assesses an individual's self-perceived skills and knowledge in each of its focus areas. 30 This instrument is grounded in the Lily model, which outlines six essential literacies: (1) traditional literacy, (2) health literacy, (3) information literacy, (4) scientific literacy, (5) media literacy, and (6) computer literacy. 8 The 8-item eHEALS-TC rates on a 5-point Likert scale from strongly disagree to strongly agree (1 = strongly disagree to 5 = strongly agree). The original study confirmed a single-factor structure with acceptable reliability, reflected by a Cronbach's alpha of .88. 30 The eHEALS-TC has a total score ranging from 8 to 40, where higher scores indicate greater perceived eHealth literacy.
The Medication Understanding and Use Self-Efficacy Scale in Traditional Chinese (MUSE-TC)
The 8-item MUSE-TC was employed to assess participants’ self-efficacy in understanding and using their prescription medications. 37 This scale has shown high internal reliability, with a McDonald's omega (ω) exceeding 0.9. 37 It uses a four-point Likert scale (1 = strongly disagree, 4 = strongly agree) to assess self-efficacy in medication use, yielding a total score from 8 to 32. Higher scores represent greater confidence in learning about and managing medications.
The Adherence to Refills and Medications Scale in Traditional Chinese (ChARMS-T)
The ChARMS-T was used to measure participants’ self-reported adherence to prescribed diabetes medications. We applied the 8-item medication-taking subscale of the ChARMS-T to identify barriers to medication intake, 38 which has been shown to be closely associated with individuals’ eHealth literacy. 31 This subscale has shown high internal consistency (McDonald's ω = 0.841) and strong construct validity among individuals with T2D. 38 Each item is rated on a 4-point Likert scale (1 = none of the time, 2 = some of the time, 3 = most of the time, and 4 = all of the time). The total score for these 8 items ranges from 8 to 32, with higher scores reflecting greater barriers to medication adherence. To facilitate interpretation, responses were reverse scored so that higher scores indicated better medication adherence. 21
Statistical analysis
The characteristics of study participants were summarized with descriptive statistics. For continuous variables, the mean and standard deviation (SD) were reported, while categorical variables were described using counts and percentages. McDonald's ω was used to assess scale reliability, with scores of 0.7 or higher indicating acceptable or good internal consistency. 39
The validation of the eHEALS-TC involved assessments of construct and criterion validity. Construct validity was examined through EFA to identify the minimal number of underlying constructs explaining the observed covariation among the measured variables.40,41 Initially, we reviewed the correlation matrix of all eight items, calculating the mean inter-item correlation to evaluate the strength of associations between items. Bartlett's test of sphericity confirmed the non-randomness of the correlation matrix, and the Kaiser–Meyer–Olkin (KMO) statistic had to exceed 0.5. To determine the number of factors, we considered the eigenvalue-greater-than-one criterion and the scree plot. 40 With the assumption that factors were correlated, we employed oblimin rotation to assess the proper grouping and loading of items onto latent factors. The EFA model was estimated using maximum likelihood estimation. Items with loadings of 0.4 or higher were considered sufficient for measuring a factor, while those with loadings of 0.4 or higher on two factors were designated as cross-loaders. 42
Criterion validity was assessed by examining how well the eHEALS-TC aligns with theoretically relevant constructs. Accordingly, hypotheses regarding the relationships between eHEALS scores, demographic characteristics, and health outcomes were developed a priori. 27 These analyses included indicators such as the medication-taking subscale of the ChARMS-T, self-reported health status, self-efficacy, and A1C levels, given prior research linking eHealth literacy to patient behaviors and health outcomes. 43 Additionally, previous studies suggest that eHealth literacy is associated with sociodemographic factors, such as age, education attainment, and economic status. 17 Thus, we hypothesized that younger age, higher education levels, greater household income, better medication adherence, positive self-reported health status, stronger self-efficacy, and improved diabetes control would be positively correlated with higher eHEALS total mean scores. Pearson (r) and Spearman (rs) correlation coefficients were used to test these hypotheses.
Descriptive statistics and correlation matrix analyses were conducted using SPSS version 28, while McDonald's ω and EFA were performed in JASP version 0.18.3. A two-sided significance level of P < .05 was applied.
Results
Demographic and clinical backgrounds of the study participants
Of the 273 participants, the majority were female (n = 142, 52.0%) with a mean age of 67.72 years (SD = 10.54, range = 28–94). More than half (n = 142, 52.0%) had attained a high school education or less, and 48.7% (n = 133) reported an annual household income under NT$660,000 (approximately US$22,000). Participants were prescribed an average of 1.96 diabetes medications (SD = 0.98), and 21 (7.7%) were using both oral hypoglycemic agents and injectable diabetes medications. The mean A1C level was 6.91% (range = 5.0–13.1, SD = 0.88) (Table 1).
Demographic background and clinical characteristics of the participants (n = 273).

Psychometric analysis
Validity assessment
The mean total score of the eHEALS was 24.78 (range = 8–40; SD = 10.05). Bartlett's test of sphericity indicated that the correlation matrix was non-random (χ2(28) = 4172.632, P < .001), and the KMO statistic of 0.914 exceeded the minimum threshold for EFA. This confirmed the suitability of the correlation matrix for EFA (Table 2). Based on the eigenvalue-greater-than-one criterion, the EFA supported a one-factor solution, which explained 84.95% of the total variance of the eHEALS-TC. The factor loadings for the items ranged from 0.845 to 0.959 (Table 3).
Inter-item correlations of the eHEALS-TC (n = 273).
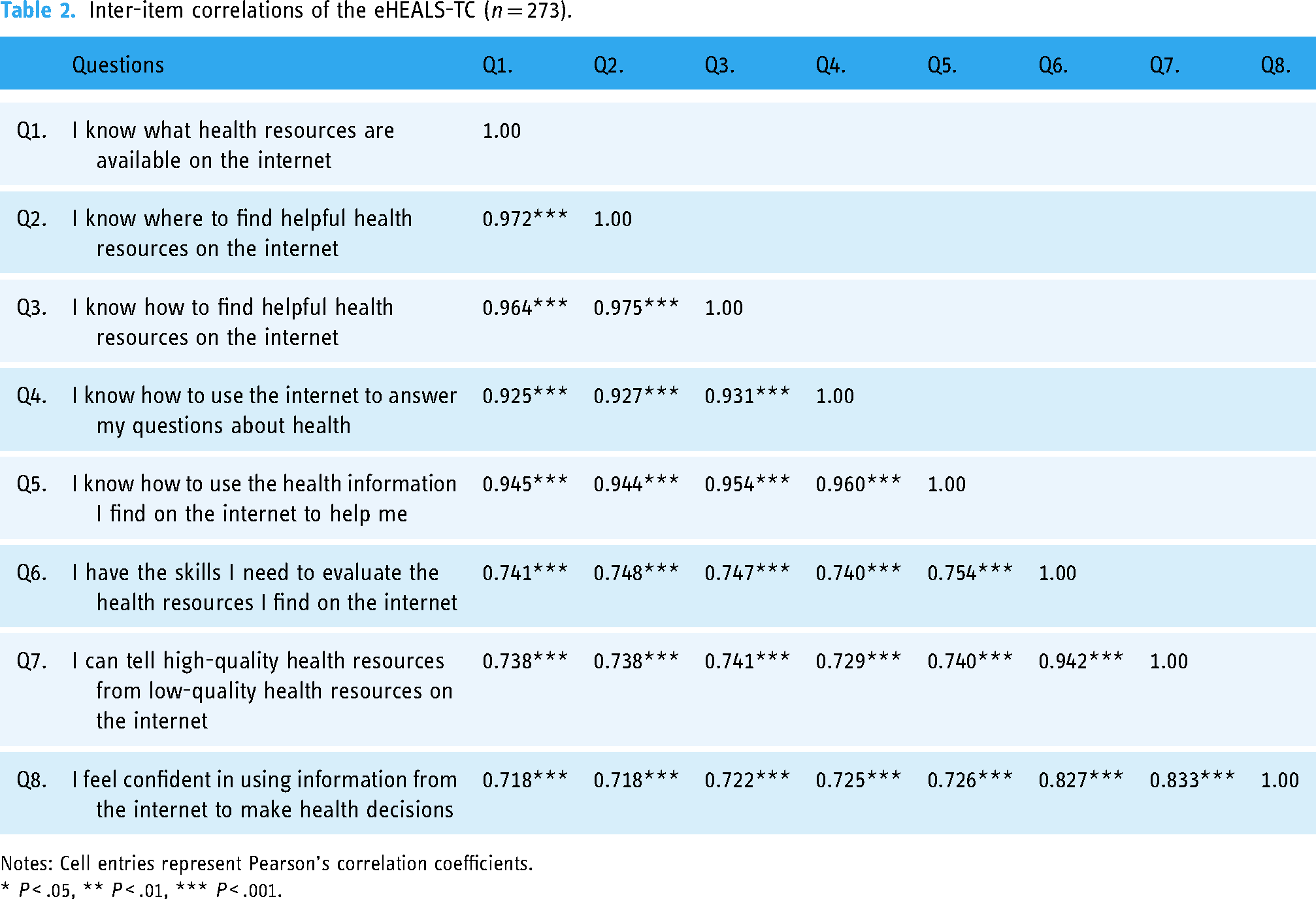
Notes: Cell entries represent Pearson's correlation coefficients.
* P < .05, ** P < .01, *** P < .001.
Exploratory factor analysis for the eHEALS-TC (n = 273).

Regarding criterion validity, our hypotheses for validating the eHEALS components were supported. The mean total eHEALS score was positively correlated with younger age (r = .382, P < .001), higher education attainment (rs = .525, P < .001), greater household income (rs = .359, P < .001), positive self-reported health status (rs = .191, P = .002), stronger self-efficacy in medication use (r = .167, P = .006), and fewer barriers to medication-taking (r = .143, P = .018) (Table 4). However, no association was found between the mean total eHEALS score and A1C levels (r = .048, P = .427) (Table 4).
Bivariate correlations of the study variables (n = 273).
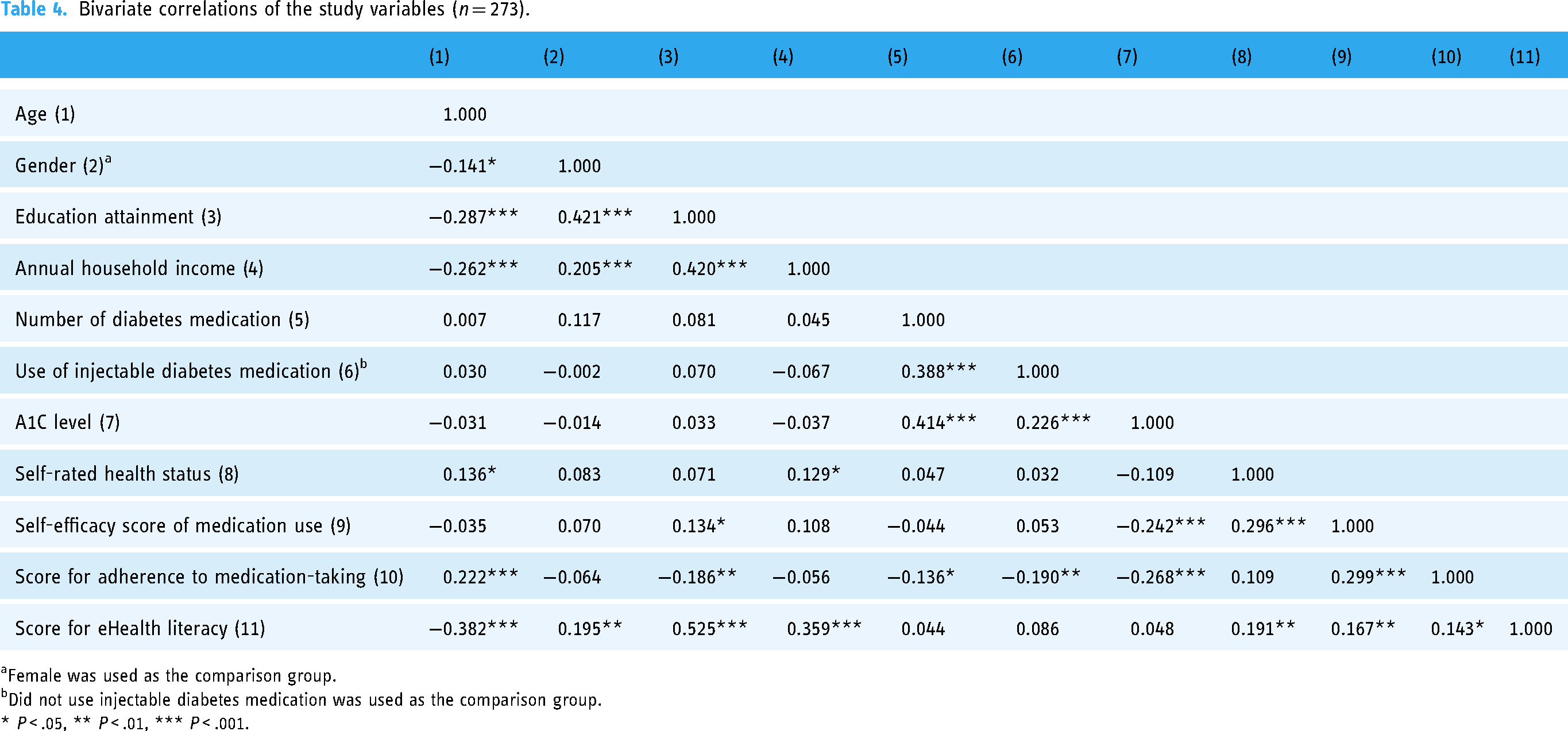
Female was used as the comparison group.
bDid not use injectable diabetes medication was used as the comparison group.
* P < .05, ** P < .01, *** P < .001.
Reliability assessment
Table 5 presents the means, standard deviations, item-total correlations, and reliability coefficients of the eHEALS-TC. The translated scale showed an excellent internal consistency, with McDonald's ω values of 0.974. The item-total correlation coefficients for the eHEALS-TC ranged from 0.844 to 0.959. Furthermore, McDonald's ω values, when each of the 8 items was excluded, ranged from 0.966 to 0.977.
Reliability analysis of the eHEALS-TC (n = 273).

Discussion
Principal findings
This study involved translating the full eHEALS scale into Traditional Chinese and evaluating its psychometric properties, which showed promising reliability and validity. The high internal consistency (McDonald's ω = 0.974) underscores the reliability of the translated version. Construct validity was demonstrated through its unidimensional latent structure, while criterion validity was supported by significant associations of eHealth literacy with health outcomes and demographic factors. Exploratory factor analysis confirmed a one-factor structure for the eHEALS-TC, aligning with the original eHEALS 30 and the prior Traditional Chinese version. 32 Notably, this single factor explained 84.95% of the variance, a higher percentage than previously reported.17,30,32,44 As seen in prior studies on adult populations, eHEALS scores were influenced by factors like age, education attainment, and socioeconomic status.45,46 In addition, echoing earlier research, eHEALS-TC scores were positively associated with medication adherence, 47 self-efficacy in medication use, 48 and self-reported health status. 49 However, eHEALS-TC scores were significantly influenced by gender, but no significant association was found with glycemic control, measured by A1C levels.
The age-related disparities observed in eHEALS-TC scores may stem from a digital divide, where older individuals are less accustomed to online resources and may approach information-seeking and evaluation differently than younger individuals. 50 Cognitive and medical challenges, such as memory loss, as well as hearing and visual impairments, further contribute to this digital divide among older adults. 16 Xie and colleagues emphasized the role of age in eHealth literacy, 31 while Marsall et al. found significant relationships between age and information-seeking behavior, though not between age and information appraisal. 43 Further research should explore these age-related differences.
Participants with higher educational attainment had greater eHEALS-TC scores, and this trend was also observed in the study among patients with T2D by Guo et al. 14 Education likely enhances basic literacy, technical skills, and health knowledge, which potentially reduces barriers to using digital health tools for diabetes management. 51 Since individuals with higher levels of education often have better access to digital resources, 16 the eHEALS-TC may serve as a useful screening tool for identifying patients who require additional support in using health information and digital health applications.
As expected, individuals with higher socioeconomic status had higher eHEALS-TC scores, likely reflecting their improved access to health resources and digital tools. In a survey by Spooner and colleagues, adults from higher-income households were more likely to communicate with providers via text, phone applications, or social media. In contrast, those who preferred non-internet sources, such as books, primary care providers, or brochures, tended to be over 65, had lower household incomes, or had less than a high school education. 52 Socioeconomic limitations can significantly impede access to the internet and digital health tools, and this underscores the need to target digital health interventions for economically disadvantaged populations. 53 In our study, household income was associated with eHealth literacy, suggesting that greater economic stability contributes to higher eHealth literacy.
Although the influence of gender on eHEALS scores remains inconclusive, 53 this study found that female participants reported higher eHEALS-TC scores than males. Research suggests that women tend to be more proactive in seeking health information compared to men, which may enhance their familiarity with online health resources and improve their eHealth literacy. 54 Additionally, women are more likely to engage in preventive healthcare activities, which may lead them to access digital health resources more frequently. This frequent engagement can build confidence in using digital tools. 8 In some cultural contexts, women often assume the role of primary caregivers, which may require them to stay informed on health-related topics and use digital tools for family health management. 55 Given that frequent searching for health information is positively linked to health literacy, women may tend to have higher eHealth literacy levels than men. While gender is often associated with differences in health outcomes, studies show these disparities are also shaped by other factors, such as cultural background, marital status, and socioeconomic conditions. 56 Thus, the gender effects on eHealth literacy merit further investigation.
This study also highlights the association of eHealth literacy with self-efficacy, self-reported health status, and medication adherence, consistent with prior findings. 31 Individuals with higher eHealth literacy are generally more capable of understanding and using health information, which increases their confidence in managing their health and encourages proactive behaviors, such as consistent medication adherence. 20 With higher eHealth literacy, patients are also better able to navigate digital resources, enabling them to access support and reminders that enhance adherence. Lee et al. found that people reporting poor or fair health status had higher scores for health-related internet use compared to those reporting good, very good, or excellent health. 57 However, in this study, higher eHEALS-TC scores were not associated with lower A1C levels. The relationship between eHealth literacy and health outcomes, based on cross-sectional data, has yielded mixed results. 58 Some studies indicate that neither health literacy nor eHealth literacy has shown direct or indirect effects on glycemic control.14,59,60 Aponte et al. found that even though patients had internet access, they did not always use it to seek diabetes-related information, which may explain why glycemic outcomes did not vary with eHealth literacy levels. 61 The effects of eHealth literacy on health outcomes may be mediated by social support, 59 self-efficacy, 60 or other psychosocial factors. Those who are skilled in using digital resources may not always apply their knowledge due to concerns about the risks associated with behavior change, meaning health outcomes may not improve. 6 A longitudinal study could provide deeper insights and contribute to a stronger evidence base in this area.
In summary, the translated eHEALS-TC appears well-suited for assessing patients’ perceived ability to navigate, evaluate, and apply eHealth information to address health-related challenges within Taiwan's cultural context.
Limitations
Although this study used both clinical and behavior-based outcomes to validate the psychometric properties of the eHEALS-TC, several limitations should be considered when interpreting the findings. The translation process incorporated input from both pharmacists and patients, with pharmacists playing a predominant role due to their expertise in medical terminology. Although this ensured technical accuracy, it may have impacted the patient-centeredness of the final translation. Future studies might enhance patient involvement to better balance technical precision with patient perspectives. The data were collected through a cross-sectional design, which supports correlation analysis but precludes causal inferences. 43 Moreover, while the scale used here exhibited excellent internal consistency, its test-retest reliability was not assessed to evaluate stability over time. eHealth literacy is a dynamic and process-oriented skill shaped by evolving technologies and shifts in personal, social, and environmental contexts. 8 Longitudinal studies are needed to further explore the temporal relationships between eHealth literacy and health-related outcomes. 31
The sample for this study included only patients with T2D, so it remains uncertain how well the scale may apply to patients with other conditions, such as acute ailments (e.g., cold) or chronic symptomatic conditions (e.g., arthritis). 27 To broaden the applicability of the evidence, future research involving participants with a wider variety of health conditions would be beneficial. Moreover, the study used a self-reported, paper-and-pencil format for administering the eHEALS-TC in community settings, following the method used in the original study. 30 Future work could explore alternative modes of administration, such as digital formats compatible with eHealth platforms, including tablets, smartphones, and email, to increase the feasibility of using this translated instrument. 27
This study also did not gather data on participants’ internet usage behaviors, including frequency and types of websites visited, potentially limiting the scope of criterion validity. Additionally, information on patients who declined participation was not recorded, possibly introducing potential response bias. 2 Lastly, the eHEALS-TC measures respondents’ perceived eHealth skills and comfort rather than their actual performance or interactive abilities when using the internet.28,30 Future studies may consider incorporating performance-based instruments to more directly assess participants’ eHealth literacy levels.29,62
Implications
Unlike other areas of healthcare, there is no one-size-fits-all solution to addressing eHealth literacy in a single session or brief intervention. 63 Rather, enhancing eHealth literacy is an ongoing process that requires coordinated efforts across multiple stakeholders, including patients, healthcare providers, educators, and community health organizations. The value of eHealth information is limited if users lack the skills to effectively engage with it. 14 Assessing individuals’ eHealth literacy can guide policymakers in developing appropriate guidelines, strategies, and interventions to deliver health information online in ways that accommodate diverse needs, preferences, and abilities. 64 By measuring patients’ eHealth literacy, we can help patients better navigate the digitalization of healthcare, with tools like the eHEALS-TC playing a crucial role. The eHEALS-TC can identify individuals who may struggle to use eHealth resources, allowing for timely support and intervention. Furthermore, it provides a solid foundation for healthcare communication, whether through face-to-face interactions or visual aids.
Conclusions
This study assessed the psychometric properties of the eHEALS-TC among patients with T2D across various community pharmacies. The findings provide empirical support for the validity, reliability, and efficiency of the eHEALS-TC as a tool for measuring eHealth literacy in individuals with diverse demographics and health conditions in Taiwan. Evaluating patients’ comfort with using eHealth can help identify skill gaps and provide better support for those with lower comfort levels in leveraging the benefits of eHealth. This tool can be easily integrated into clinical practice for screening and follow-up, improving communication between healthcare professionals and patients.
Footnotes
Acknowledgments
The authors sincerely thank Dr. Cameron Norman and Dr. Harvey Skinner for granting permission to translate and validate the eHEALS into Traditional Chinese. The eHEALS is © Copyright 2006 by its authors, Dr. Cameron Norman (University of Toronto) and Dr. Harvey Skinner (York University, Toronto).
Contributorship
YMH contributed to conceptualization, data curation, methodology, investigation, formal analysis, validation, resources, project administration, funding acquisition, supervision, as well as drafting and revising the manuscript. YMY and TW contributed to data curation, investigation, formal analysis, validation, and revising the manuscript. HYC contributed to conceptualization, methodology, supervision, validation, funding acquisition, and revising the manuscript. All authors reviewed and approved the final manuscript for publication.
Data availability
The study materials and detailed analyses are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study protocol received approval from the Research Ethics Committee at National Taiwan University Hospital (202303022RIND). Participants were informed about the research purpose and assured that their participation would remain anonymous. Each eligible participant was required to provide written informed consent before taking part in the study. All procedures were conducted in accordance with the Declaration of Helsinki.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Science and Technology Council (grant number NSTC 113-2410-H-003-103-SS2, NSTC 113-2628-B-002-018-MY3).
Guarantor
YMH.
Appendix A The original English version of the eHealth Literacy Scale 30
Appendix B The Traditional Chinese version of the eHealth Literacy Scale