
Abstract
Studies on use of IT in residential care are limited; thus, there is a need for investigations to understand both older people’s and nursing staff’s perspectives on experiences of new technology. ‘Smart homes’ provide home automation solutions, making life easier for those residing there. The aim was to explore, from the users’ perspective, experiences of a sensor system installed in the home. The sensors are meant to provide notifications of deviations in behaviours or routines by the resident, requiring healthcare staff or relatives to do a supervisory visit. The sensor notification system made the users feel secure by being monitored, having control over the situation, and allowing them to become more independent in their daily lives; furthermore, they emphasised the importance of having well-functioning systems. Further development of the technology and use, in co-creation with the users, is needed. Careful preparation in installing/starting the system and repeated information about its aim are needed.
Introduction
Worldwide, there is an ongoing demographic transition towards an increased proportion of older people.1,2 In Sweden, one-fourth of the Swedish population will be older than 65 years in 2050, an increase of 30% 3 ; thus, there is a predicted increase in the need for social services and healthcare at the same time as the tax base is declining. The same trend is seen in Europe. By the year 2020, 25% of the population will be 65 years and above, and an estimated increase by 40% between 2010 and 2030 of those aged 65–80 years. 2 These demographic and socio-economic challenges need to be met with measures that can help prevent dependency later in life and respond to the needs of older people.1,2
In a health context, Information Technology (IT) may provide the possibility for older people with complex needs and chronic conditions to remain in their homes and maintain an acceptable quality of life, 4 enable independence in daily life,5,6 allow for functional monitoring and emergency fall detection,7,8 and provide sensory and cognitive assistance. 9 Installation of sensors in ‘Smart homes’ provides home automation solutions, making life easier for those living there. 10 However, studies on the use of IT in residential care are limited 11 ; thus, there is a need for investigations to understand both older people’s and nursing staff’s perspectives and experiences of using a different new technology.11,12
Background
The advent of the Internet-of-Things (IoT) with low cost and prolific sensors has furthered the trend in home automation and monitoring solutions being used for elderly healthcare.6,13,14,15 Remote monitoring can be used for monitoring activities of daily living or health status, for example, in chronic diseases (14). A previous pilot-study 15 presented intelligent, privacy-aware, home care assistance using a sensor system, by learning the user’s daily activity patterns and automatically issuing warnings if an unusual situation was detected. This was a passive system not requiring any input from the user. The main idea was to answer the question whether the loved one is all right, and the case study was shown to prolong the independence of older people living alone, while offering peace of mind to their relatives and/or caregivers. Another study with a qualitative design explored the experiences of patients living with a novel home-monitoring sensor system during the period around joint replacement. 12 The technology (passive system for activity monitoring, active system with a wearable alarm) was experienced as acceptable, but informal support networks were a key factor to enable them to use the technology at home. Other studies investigated experiences of using glucose sensor-based mobile technology (active system) in persons with type 1 diabetes 16 and cancer patients’ attitudes and experiences of online access to their electronic medical records. 17 Reactions to the use of technology could be both positive and negative, for example, being perceived as an empowering tool; a source of psychosocial support, offering relief from worry; supporting positive feelings; concerns due to being too demanding of information or not being attuned to socio-economic background; generating substantial anxiety and concerns; and frequent calls to the hospital. These are reasons why technological measures need to be individualised and delivered in combination with adequate staff support. The use of modern technology raises issues of security, privacy and integrity.14,18 A review of community-dwelling older people’s experiences with the use of telecare (technological solutions promoting safety in the persons’ homes) in home care services 19 supported this and concluded that the experiences are diverse. Some devices do not work outside the home and therefore active ageing is limited. Autonomy is important, but a negative identity as helpless and frail may be imposed on older adults by telecare. Lack of understanding might be a barrier to correct use of the equipment, and therefore support from service providers are needed. However, the studies included focused on first-generation devices (active alarms with user-triggered alarm buttons), while further study is needed of experiences of newer systems such as (second-generation) passive alarms with sensors detecting specific risks, not requiring user input and (third-generation) data sent to an internet portal assessed by caregivers monitoring the user.
The IoT project studied
The present study is part of a project aimed to build on existing systems, based on the Internet-of-Things (IoT), in municipalities in Sweden, by extending the system with new IoT units and to exchange information to support the municipalities in making healthcare and social services more efficient and to support secure living for recipients of these services (run 2017–2020). IoT is used to develop prerequisites to handle demographic challenges with the growing needs for care in the community6,13,20 delivered by the municipalities. In Sweden, the municipalities are responsible for care and social services delivered in the home, in nursing homes for older people and in accommodations with special services, for example, for persons with functional disabilities. Three different municipalities, representing both rural and urban areas, and a more densely populated city with suburbs were included in the project. In the present user study, following a pilot-test, an evaluation was conducted from November 2018 to February 2019 on how IoT support works in secure housing and how the users – care recipients, relatives and healthcare staff – accept the technology. Specifically, we evaluate what aspects work and give feedback to the municipalities and those working with developing the new technology, namely, the municipality including a densely populated city. To ensure that technologies are developed so they fit the purpose and are acceptable, there is a need to understand and characterise the perspectives of the people who have experience of using them. 12
A sensor system for notifications of deviant behaviours and routines in the home
Environmental IoT sensors were installed in the residences of older people. 10 These sensors are wireless devices used to collect different types of information about persons in their residences such as: when moving between rooms, other movements, level of light and temperature in the room, opening and closing of doors, smart electricity plugs registering information about the use of machines and taking medications, or whether a lamp is turned on or not. The sensor is connected via a gateway to a server for data gathering and analytics, referred to as the Sense Smart Region platform. Thus, notifications concerning deviations from the person’s daily behaviour or routines are sent via an app in the mobile phone to healthcare staff, or relatives, requiring them to do a supervisory visit. Notifications via a text message, SMS, include the name of the person and when appropriate the relative or the care or social service institution. Notifications were also sent via an app in the mobile phone to care recipients living in accommodation with special services for persons with functional disabilities, with reminders to do different tasks such as to start daily activities, take a shower, do the washing up, vacuum-clean, close the door, etc. It is thus a passive monitoring system, not requiring any inputs from individuals in their homes. In both types of accommodations, there were also sensors connected to cameras to monitor the care recipient, particularly used by staff at night.
Aim
The aim of the present study was to explore, from the users’ perspective, experiences of a sensor system installed in the home, aimed to provide notifications of deviations in behaviours or routines in the residence, thus requiring healthcare staff or relatives to do a supervisory visit.
Methods
Design
A qualitative, exploratory, study design, using semi-structured interviews to gather data, was chosen, as it provides new insights and increases the researcher’s understanding of a particular phenomenon that has previously been investigated to a limited extent. 21 Qualitative semi-structured interviews were chosen, as they allow participants to respond in their own words and to express their own personal experiences but within a given frame.
Recruitment
In the studied municipality, respondents were recruited from the Elderly Administration, including two elderly homes with persons over 65 years of age with care needs, and from the Care Administration, including persons with functional disabilities, below the age of 65, living in accommodation with special services, with 24 hour access to basic services, if needed. These types of accommodations are considered as the person’s own residence.
Participants
A purposeful sample included persons with sensors installed in their residences, along with staff and relatives involved in their care. Participants comprised 12 persons (seven women, five men). Of these, three care recipients (below 65 years of age) were living in accommodation with special services for persons with functional disabilities, and three others (over 65 years of age) were living in a special residential care home for older people. In addition, five healthcare staff and a relative participated. Older people had continuous contact with healthcare staff, in contrast to persons with functional disabilities who had 24 hour access to healthcare staff at a service house for older people if needed but did not have daily contact with them.
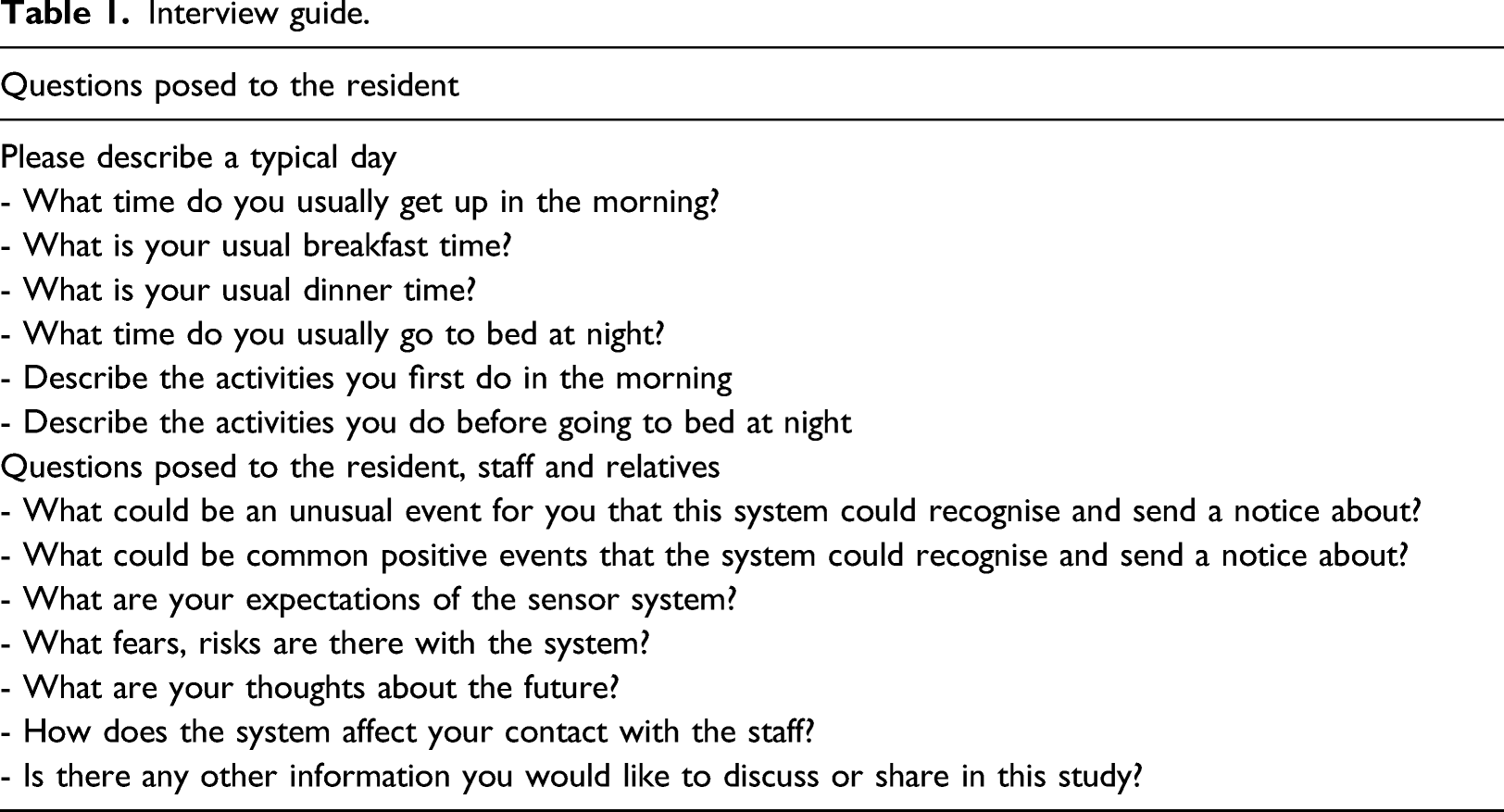
Data collection
Interview guide.
Procedure
The head of the Elderly Administration in the municipality and the unit heads of the elderly homes participating in a research project on digitalisation in the municipality gave their written permission to conduct the study. Unit heads and contact persons informed possible participants – municipality citizens, staff and relatives – about the study, both orally and in writing. Those willing to participate signed a consent form, and the contact person responsible for the project forwarded contact details to the interviewer.
The interviewer then contacted, by telephone, those willing to participate and informed about the study and set a time and place for the interview in order to create a secure interview environment. The interviews were held in the homes of the care recipients, with the staff in staff rooms, and by telephone with the relative.
The interview guide was tested on two individuals, and no changes were made to the guide, thus, allowing for the data to be analysed and included in the study.
The interviews were conducted between November 2018 and February 2019 and led by a nurse specialising in elderly care and particularly trained in leading qualitative interviews (second author) after discussion with the principal investigator (first author). Before the interviews, there was time to establish contact, take part in informal conversations, and create an opportunity for the respondents to ask questions to facilitate the interviews. 21 In this connection, written informed consent was obtained. Interviews were conducted following the semi-structured interview guide to evaluate the users’ perspectives on having sensors installed in their homes. In order to deepen, clarify and develop the informants’ answers, 21 probing questions such as ‘Can you tell me more?’ and questions based on informants’ previous statements were asked. The interviews lasted 30–45 min, and were digitally recorded. After the interviews, there was time for reflection if required by the participants. The interviews were transcribed verbatim by the interviewer using a transcription guide. 23
Data analysis
Data collection and analysis proceeded simultaneously, until no new information was added in the analysis. 21 Qualitative content analysis was performed according to a method described by Patton. 21 Qualitative content analysis focuses on the characteristics of language as communication, particularly the content or contextual meaning of the text. Conventional content analysis is useful when the aim is to describe a phenomenon in an area where existing theory or literature is limited. 24 The aim of the analysis is to be open to as much variation as possible in the material, and to search for patterns, contradictions and overarching themes in the text. 21 Both the shared perspectives of different groups of users and the perspective of separate groups were studied. The analysis started with the researchers reading through the whole texts repeatedly in order to obtain a sense of the whole. To find and highlight exact words in the text that captured key thoughts or concepts related to the aim, the transcripts were read word-by-word. Meaning units answering the aim of the study were identified and coded with labels as close to the original text as possible. Codes were compared and grouped into sub-categories based on similarities, whereafter these were sorted into categories in order to capture its complexity. The categories and their names were derived from data and not from preconceived categories, a procedure known as inductive category development. Quotations for each category were identified from the interview transcripts in order to report the findings and maximise their diversity. As a final step, the last author read excerpts of the raw data to validate the content of the categories. 21
Rigour
The trustworthiness of the findings was increased by including a nurse specialising in elderly care and particularly trained in qualitative studies and a nurse experienced in chronic disease management, long-time researcher in nursing science with vast experience of qualitative studies (first and second author) in the analysis of data. The content of the categorised data was checked by the first author 21 and showed high agreement. Confirmability was established as illuminative quotations are given in the text to illustrate the content and verify the categorisation. 21
Ethical considerations
Ethical approval was sought from the Swedish Ethical Review Authority (Dnr 2018/189–31), and the study was implemented in accordance with the Helsinki Declaration with written informed consent (World Medical Association, 2013). Before the interviews, the informants received the information that participation was voluntary and that they could, at any time, withdraw from the study without any explanation. Transcripts were anonymised, coded and kept in a locked space to which only the two investigators had access.
Main heading on Findings
Categories emerging from the data.
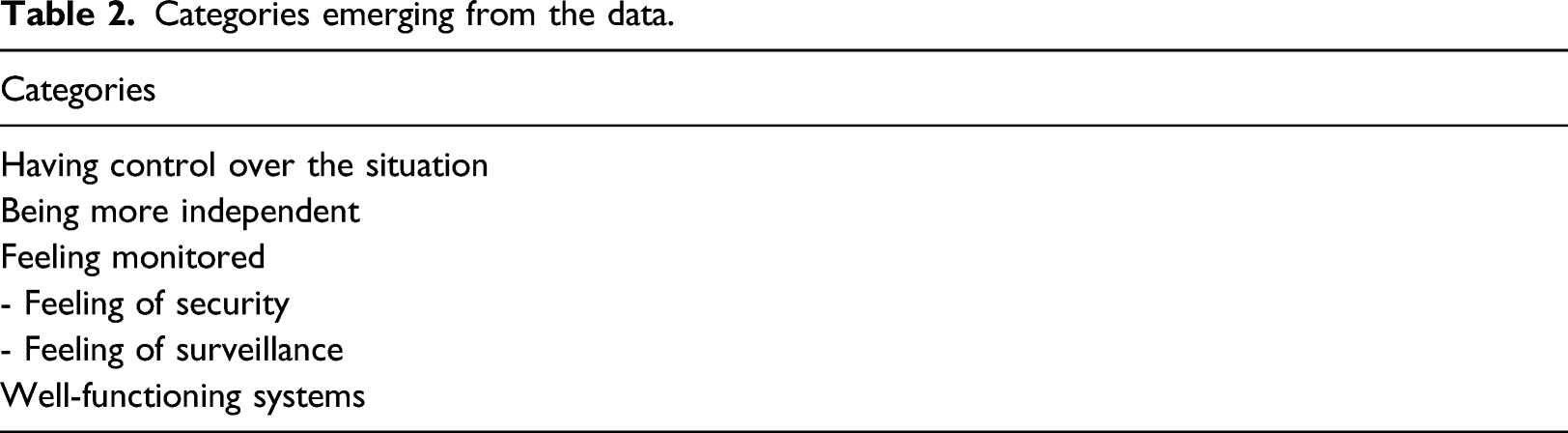
Having control over the situation
The category having control over the situation included experiences of both staff and care recipients. For staff, it concerned when they received notifications about unusual events that could happen to a care recipient to react to. An unusual event could be that a care recipient had not turned on the coffee maker in the morning and that something could then have happened to the person. The fact that the sensor registered when the care recipient walked in and out of the residence and that there was a vital sign from the person also made the staff feel they had control over the situation. The staff wished they could get a notification in emergency situations such as fire, leakage of water and fall incidents for the care recipients living in special residential care. That the care recipients should be able to feel more secure in the home; we can identify deviant behaviours, and they know that there is someone keeping track of them. If they had fallen, they wouldn’t need to lie there for 3 days…You’re able to keep track of things in a different way and don’t have to worry (R 6).
In special residential care for older people, there were alarm cameras that allowed staff working night shifts to monitor if a care recipient had fallen. They were able to see if a care recipient was still lying in bed but not whether the person was able to breathe, which would be desirable according to the staff.
The care recipients expressed they felt safe that: the staff had control over the situation, could see when they got out of the bed, if they had fallen, and then could get help if needed. One of the respondents said that the camera was wrongly placed, as it was near the bed and just pointed straight forward. It would have been better if the camera was attached to a corner of the ceiling so that the whole room could be monitored. I think it’s good that one is monitored in here, it feels safer as long as it works and is handled in the right way (R 8).
It also emerged that the most important thing was that the staff reacted and cared when the sensor indicated an unusual event, for example, that a care recipient was lying on the floor or something else was wrong. It was also evident that some of the care recipients experienced that they had to wait a long time before any of the staff responded to their alarm. Another respondent did not think it mattered whether it was a camera that could see if the person had fallen or if it was staff that had gone into the room to see. The care recipient felt less worried when being able to get in contact with the staff and vice versa. That the staff can get in touch with me and I with them (R 9)
Functions that could be added to the system to even further increase the degree of control over the situation were mentioned by the staff. The staff wished that the system could give quick confirmation, via a picture. Worried care recipients who sounded the alarm often felt that a voice was not sufficient; instead, the care recipients wanted to see who they were talking to. The staff also stated that it would be desirable if the system could give notice when a care recipient with dementia walked out so that the he or she did not wander away.
Most said that the sensors did not affect the relation between the care recipient and the staff. The residents feel safe, they know they have sensors, but there is no difference in the contact between us (R 7).
Being more independent
This category related to when the staff received notifications of positive events relating to the care recipients. In accommodation with special services, care recipients with functional disabilities got reminders in their telephones that facilitated for them to manage activities in their daily life independently. The care recipients had reminders to do the washing up, hoovering, taking showers, close the front door, go to bed and take their medication. Both staff and care recipients expressed that this resulted in less nagging from the staff with reminders. Yes, it can become better when you don’t have to hear nagging from the staff (R 1).
It emerged from several of the respondents living in this accommodation with special services that the contact with staff could be more positive because of the reminders. The care recipients could feel that it was their own idea to do the dishes or take a shower after getting a reminder in the app. They found this nicer than being nagged about it by the staff. It improved the relationship between staff and care recipients as the staff could instead praise the care recipient for having done what needed to be done. The staff perceived that the care recipients could be more involved in their own care as they too used an app. Both staff and care recipients believed that reminders could be good for cognitive difficulties such as ADHD and dementia. However, there appears to be a risk, as expressed by the staff, that the care recipients could fool the system, that is, they only switched on the vacuum cleaner so that the staff could see they had used it, but then switched it off again. Reminders to do the hoovering allow the care recipient to initiate the task before the staff arrives to help them; and the person can feel proud, which is good for their self-confidence (R 5). Good aids. That it actually happens that I do the dishes after I get a reminder on the phone (R 1)
One respondent thought the power balance between staff and care recipients living in accommodation with special services should be better as they had been involved in the project together.
Staff in both types of accommodation perceived that there was an advantage with the camera connected to the sensors monitoring the care recipients, who thus were not disturbed at night. The staff were able to see if a person woke up and only visited them when that happened, for example, to offer assistance in going to the toilet or to identify other needs. Thus, fall accidents related to difficulties in walking, balance or impaired vision could be prevented and otherwise the person could sleep undisturbed. One care recipient thought it was much better to be left in peace and not have to show whether one is happy or not about being disturbed by staff at night. Another respondent said that personal contact was more important than contact via camera but that it was convenient if there was a limited number of staff and when individuals wanted to be left in peace. Thus, being able to sleep undisturbed and feeling secure about getting help if needed contributed to the sense of not being dependent on others. Other care recipients said that it was important to maintain the personal contact and that the sensors could not replace it. During the night, it’s useful that you don’t need to go in and disturb (R 11). I can be left in peace, I think it is much better and not have to show if you are happy or not (R 8).
Feeling monitored
This category included experiences of being monitored by the sensor system, mostly positive feelings of security, but also some negative feelings of intrusion into privacy and integrity, although these could be overcome with appropriate information. Older people in special residential care felt secure in being monitored. I think it’s good to be monitored here, it feels safer… (R 8).
In accommodation with special services for persons with functional disabilities, however, some felt that they were under surveillance, which was also a reason why some had declined participation in the study. In such living arrangements, not as many alarms were used as in homes for older people in order to avoid the risk of care recipients feeling monitored in an intrusive way. Staff thought first that the care recipients would feel they were under surveillance, but this changed after they had received more information about the project and had understood the purpose. One example cited was where the staff could see that the television had been on all night after a care recipient had fallen asleep, and then when the staff checked they became aware that, the person had not been lying in the bed during the night. In order to reduce the feeling of surveillance, it was therefore important to provide information about why the care recipient had a sensor for reminders, namely, that it was for the care recipient’s sake. That the staff can watch my activities on the sensors; if you have bad luck, there can be some kind of surveillance, and I am not very much for that (R 3).
Well-functioning systems
For this category, both staff and care recipients said it was important that the system worked well and was user-friendly. The importance of the network functioning well was also emphasised. It needed to be a smooth system, otherwise it meant extra work for the staff. The apps in the mobile phone receiving notifications of deviant behaviours or routines were not perceived as being very clear. Another hindrance described by the staff, in both types of accommodations, was that they had ‘double alarm systems’. They had an ordinary alarm bell in their telephone as well as the notifications of the sensors of the camera sent via an app to a special mobile telephone. They wished to have everything in the same telephone. However, this ‘double alarm’ existed only during the testing phase of the project when the mobile phone connected to the sensors was added to the existing alarm system. The staff wished that there would be an alarm when the camera did not work, which happened if a cord had been pulled out while cleaning and it took several days before it was detected by the staff. The care recipients in accommodation with special services felt it was important that the alarm did not disturb them. It was also important that it was a secure system, and that nobody else could access it and watch the cameras. One of the respondents saw a danger that an unauthorised hacker could easily get into the system. We have our alarm bells plus this mobile with apps that one has to try to remember (R 7).
It also emerged that the staff regretted that they had not collaborated more with the care recipients, in choosing different types of sensors and types of activities to be monitored in the planning of the research project. The care recipients seemed to have consented to a finished proposal made by the staff.
Why did we not sit together with the person, and present it to them as ‘this is what we think, what do you think?’ (R 4)
Another aspect of collaboration was that neither the relatives nor the care recipients had received any information about when the sensors would be installed. Care recipients in accommodation with special services were taken by surprise when they discovered the new equipment, for example, wires on the floor, and understood that someone had come unannounced while they were at work. In addition, it emerged in the interviews that in these residences, the technical equipment related to the sensors (e.g. internet connection, connection to cameras for monitoring) was installed with wires that ran straight across the floor and were therefore a tripping hazard for the resident; the staff who had done the installation came to change this. I am positive to this, but we need to be informed before the installation is done. We did not know anything at all (R 12).
All respondents mentioned that in the future, there will be more and more new technologies; some found it positive, while others thought it was costly and unnecessary. The staff wished that there was a priority alarm, so that the care recipient could press it if they just wanted a glass of water or if they had fallen. There is more and more great stuff coming, the healthcare staff are learning how to utilise this and I think, yes, it is great (R 9).
Discussion
This study explores the users’ perspective – care recipients, relatives and healthcare staff – on how IoT support works in secure housing as well as how they accept the technology. Experiences of a sensor system installed in the home, intended to detect deviations in the resident’s behaviours or routines, were explored from their perspectives. Studies on use of IT in residential care for older people are limited 11 and experiences of using passive alarm systems with sensors detecting risks and connected to internet portals for monitoring (second- and third-generation telecare systems) are lacking. 19 Thus, there is a need for investigations with a qualitative design 16 to understand both older people’s and nursing staff’s experiences of using a different new technology.11,12 The main results showed that the sensor system’s notifications made the users feel they had control and could be more independent in their daily lives. However, they also felt they were being monitored and agreed about the importance of having well-functioning systems.
The main results showed that the sensor system’s notifications made the users – care recipients, relatives and healthcare staff – feel they had control over the situation and could be more independent in their daily lives. However, they also felt they were being monitored and agreed about the importance of having well-functioning systems. The results showed that the users felt that the sensor system made them feel they had control over their situation. The staff, as previously found, 11 could provide faster assistance to the care recipients, as they were able to detect unusual events quickly, for example, someone walking in and out of a room, particularly during the night, or forgetting they had put on a coffee machine. The care recipients, on the other hand, felt secure as they were assured by the new technology of functional monitoring and emergency fall detection.7,8 In line with studies on attitudes to technology requiring active input from the users, the sensor system technology was thus considered to be a source of psychosocial support, offering relief from worry, supporting positive feelings16,17 and contributing to increased safety 11 for the user. ‘Safety first’ [11, p 9] is concluded to be the most important for all parties involved.
The sense of having control also influenced the sense of being more independent, not least thanks to positive notifications from the sensor system. The users, particularly those who were functionally disabled and living in accommodation with special services, appreciated reminders about doing activities of daily living, for example, taking showers or vacuum-cleaning, while healthcare staff emphasised their appreciation of not having to disturb persons during sleep, as the system warned if something was unusual. Information Technology (IT) provides the possibility to maintain an acceptable quality of life, 4 and enables independence in daily life .5, 6 Further, the care recipients felt that their independence also contributed to better relations and improved the power balance with healthcare staff, something not previously studied in either persons with functional disabilities or elderly persons. This was because the staff no longer had to remind the care recipients about performing their daily activities; instead, they had time for other more pleasurable activities (e.g. socialising). The sensor system worked as an empowering tool for the care recipients to take more responsibility in their life. For the users, the technology seemed to offer peace of mind, which has previously been suggested as an important outcome. 15 The results did not support previous findings that telecare could reinforce an identity with negative connotations of older adults as helpless and frail. 19 This could be explained by the technology being different, as previous studies have concerned experiences of using devices including active alarms with user-triggered alarm buttons, instead of the passive alarms in this study with sensors detecting specific risks not requiring active user input. Thus, acceptability is connected to the technology used. 19
The respondents in this study, with few exceptions, felt they were being monitored by the sensor system but in a positive sense, in terms of feeling secure and looked after as opposed to negative feelings of intrusion into privacy and integrity, as previously described.12,15 However, some care recipients living in accommodation with special services felt they were under surveillance and raised concerns about privacy and integrity, which was the reason why some had declined participation in the study. In previous studies, this has been handled by repeated and written information about the technology12,17 and limiting the number of alarms and devices used in the home. 12 Thus, it is important to add individualised information. 17 The use of IoT is an issue of both security and privacy.14,18
From the experiences of all the users in this study, it was evident that having a well-functioning system is important. The technology was perceived as working well and being user-friendly, previously stated as important in a pilot-study of a sensor-based system for smart homes based on the IoT . 15 It has previously been suggested that the use of simple smart-home sensors providing essential and continuous information about the environment and the status of the resident can contribute to the independence of older persons and offer peace of mind to their caregivers and/or family members , 15 as corroborated here. However, co-creation in research is an important task in order to develop new technologies such as IoT.20,25 In this study, elements of usability and acceptability of the sensor system installed in the home were explored from the participants’ perspective and suggestions were made for improvements.
According to healthcare staff, the alarm system needs to be further developed to prevent the presence of double alarms, by means of alarm bells and mobile phones. Moreover, an alarm should be raised if the system does not work, and there should be a possibility to confirm an alarm via direct contact with the person, perhaps with an image. Technology, in general, can be a source of psychosocial support, providing relief from worries, concerns and frequent calls; however, it needs to be individualised and delivered in combination with adequate staff support.12,16,17 Furthermore, it was clearly expressed that technology should never replace personal contact.
Other proposals for improvement were better picture quality from the cameras and the use of technology to facilitate placement in the room to obtain more detailed information on the person’s status (e.g. if the person was breathing). Although suggestions for improvement of the technology were found to be acceptable, in contrast to a previous study, 12 informal support networks were not a key factor in enabling persons to use the technology at home. This was probably due to another kind of technology, not requiring input from other persons. The sensor system is wireless and characterised as a passive monitoring system, which does not need any input from the person being monitored. 10 Activity recognition systems typically use a sensor-based approach, including body sensor network or smart-home sensor network or both. 26
In this study, staff regretted not having cooperated, to a higher degree, with the care recipients when choosing different types of sensors and types of activities to be monitored, in order to prevent the feeling of being under surveillance, which caused negative emotions, as previously described. 12 The care recipients seemed to have consented to a proposal mainly drawn up by the staff, and the real challenge is to take the new technologies into real-life homes and develop systems based on the residents’ experiences to provide support and timely assistance adapted to their needs. 10 Thus, the care recipients’ involvement has to be strengthened. Furthermore, information relating to when the new technology will be installed in the person’s home, followed by repeated information from the staff as to why a person has a sensor for reminders, should be shared. It was also concluded that some did not participate due to lack of appropriate information and concerns about personal integrity and privacy. It has previously been stated that enhanced safety comes first, 11 but technology can improve relations with healthcare staff; moreover, power imbalance can be prevented when the person feels empowered.16,17 The sensor system should meet specific needs, and the benefits should outweigh privacy and trust issues.14,15
Limitations
The strengths of this study are that it investigates the users’ perspective, and thus includes care recipients, healthcare staff and relatives. Further, the study includes people of different ages, with varying needs of care and access to staff (continuously or on demand or planned) and living in different forms of accommodation, both special residential care home for older people (>65 yrs) and accommodation with special services for functionally disabled persons (<65 yrs). Nonetheless, the different forms of accommodation are defined as the person’s own residence, which raises important questions about how to preserve integrity and privacy.11,15,18
During the course of the project, one elderly home dropped out due to problems with technical installations. Thus, the results are limited; on the other hand, the data show a good quality and a homogeneous pattern indicating high credibility. 21 This was further increased by triangulation of perspectives in the study population and investigator triangulation in the analysis of data. Thus, sampling adequacy and data redundancy 27 were achieved. Further research, however, would need to include more relatives, contributing other perspectives on institutional care in ‘one’s own home’.
Conclusions
In conclusion, notifications of deviations in the care recipients’ behaviours and routines from the sensor system were experienced as making the users (staff, care recipients and relatives) feel secure by being monitored, having control, and becoming more independent in their daily lives. The users emphasised the importance of having a well-functioning system. For further development of the technology, dialogue with the users should start with careful preparation to start the system. Moreover, information should be shared about the sensor installation, followed by repeated information about its aim. Further development of the device should also include the opportunity to have personal contact, for example, through the use of images via a camera. Based on the results, the usability of the new system will be evaluated and the technology and use will be further developed, together with the users, to take the smart-home technologies even further with user profiles and machine learning to develop healthcare solutions for the future.
Footnotes
Acknowledgements
We are grateful to the project coordinator of the VINNOVA project, Henrik Näslund, at the municipality of Skellefteå, and the team in the project group including staff from the municipalities of Skellefteå, Piteå, Uppsala, Umeå, Luleå as well as Uppsala University for giving us the opportunity to explore the users’ perspective. We are also grateful to Dr Alan Crozier for review of the language.
Authors' contributions
Study design: KH; Data collection: LH; Data analysis: KH and LH. Drafting the manuscript: KH, supported by LH who made critical revisions to the paper for important intellectual content. Obtaining funding: KH. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grants from VINNOVA (No 2017-03906), Sweden’s Innovation Agency, and the programme Internet of Things (IoT) Sweden.
Data availability
Data will not be shared in order to protect integrity, anonymity and confidentiality of the respondents with the exception of that anonymized quotations supporting data in the section of Results in the manuscript is shown.