
Abstract
This study aimed to describe older persons’ experiences of eHealth services in home health care. A meta-ethnographic approach was applied, and a systematic literature search was conducted in three databases. In total, 11 articles were included and analysed, which resulted in two themes and six sub-themes. The results show that for older persons to use the eHealth services, they must provide some additional value compared to current contacts with healthcare professionals. Those with regular healthcare contact do not experience the eHealth service as adding anything to the care they already receive. The introduction of eHealth services involves learning how to use the new technology, and some older persons experience the technology as motivating and inspiring. The eHealth service makes some feel safer while some do not trust the technology. In order to make the best use of eHealth services, it is important that the services are adjusted not only to each person’s needs but also to their personal capabilities and resources, while the older person must feel valued as an active partner in the care process. Thus, when using eHealth services, the older person’s perspective needs to be given priority and decisions should not only be based on organizational considerations.
Introduction
Global demographic trends such as the increasing number of persons 60 years and older 1–4 are challenging health care due to growing requests for home-based health care. 3 Even if many older persons enjoy relatively good health into their later years, they often live with one or more chronic conditions and are in need of help with various activities if their independence in their own homes is to be ensured. 5 Home health care takes place in the older person’s home and depends on the collaboration of various people who can play active roles, such as family members and healthcare professionals. 6 However, the current home healthcare system has its limitations. The consequences of these limitations and the chronic nature of cognitive impairment result in individual care needs for many older people. 7 To improve the quality of care, more frequent care that targets individual needs seems to be what is needed. 8 A possible solution to the need for improved home health care is the use of eHealth services.9,10 eHealth services are defined as ‘health services and information delivered or enhanced through the internet and related technologies’. 11 They include the use of information and communication technologies (ICT) in supporting health. 12 In this study, we define eHealth as the use of ICT in home health care as used either by the older person him/herself or by the healthcare professional. There are a variety of eHealth services that can be used to enhance the quality of life of persons who have reduced health capacity. eHealth services can be central in providing support to family members through enhancing access to information and community resources and to connections with formal and informal support services. 5 Research14,15 indicates, for example, that the use of eHealth in home health care is successful in supporting older persons with cognitive impairment and their caregivers through the earlier detection of needs, increased self-monitoring and the encouragement of the resulting independence.13,14 Despite promising results regarding the use of eHealth services in the elderly population, the implementation of eHealth can be difficult as older persons are often unfamiliar with this type of technology.
Various eHealth service frameworks show the importance of involving users early in the development process to get their perspective during continuous and systematic evaluations. 15 Nearly 1.5 billion, or 22% of people worldwide, use the internet regularly. 16 However, increased internet use has not yet resulted in the greater use of eHealth technologies in chronic disease populations. 17 Sociodemographic factors, including age, gender, socioeconomic status18,19 and a lack of user-friendly interfaces have been identified as key barriers to eHealth use among older persons, 20 and the challenge is to design systems that are acceptable and can be used effectively by older people. 21 eHealth services can facilitate the management of complex comorbidities, and as older persons represent the most frequent users of home health care, 3 an integrated and interpreted understanding is important. Therefore, this meta-ethnography aims to describe older persons’ experiences of eHealth services in home health care.
Methods
Meta-ethnography as described by Noblit and Hare 22 was applied in this study. Meta-ethnography is used for reviewing and synthesizing the findings of published qualitative research. Noblit and Hare describe meta-ethnography as being primarily an interpretive and inductive process that aims to develop new conceptual understanding, that is, it ‘seeks to go beyond single accounts to reveal the analogies between the accounts’ (p.13). The method includes three phases that are conducted in sequential order: systematic literature search, quality appraisal and synthesis of findings.
Systematic literature search
The systematic literature search was conducted in the following three databases: (i) PubMed, (ii) Cumulative Index to Nursing and Allied Health Literature (CINAHL) and iii) Scopus. The search strategy was developed in collaboration with a health science librarian and conducted during August and September of the year 2019. The search terms were identified according to the aim of the study and finally lead to four search blocks: (i) aged, (ii) experiences, (iii) eHealth and (iv) home health care. In each search block, keywords were combined with the Boolean operator OR, and the final search combined the blocks with the Boolean operator AND. In CINAHL and PubMed, indexed search terms, MeSH and CINAHL headings, as well as non-indexed keywords were used. In Scopus, only keywords were used since Scopus does not have indexed search terms.
In total, 921 articles were identified following the database searches and through manual searches (see Figure 1). At the title and abstract level, 869 articles were read, and were assessed as being duplicates or not relevant to the study’s aim. Finally, 52 articles were read at full-text level of which 41 articles were excluded, resulting in 11 articles for quality appraisal. Flow diagram.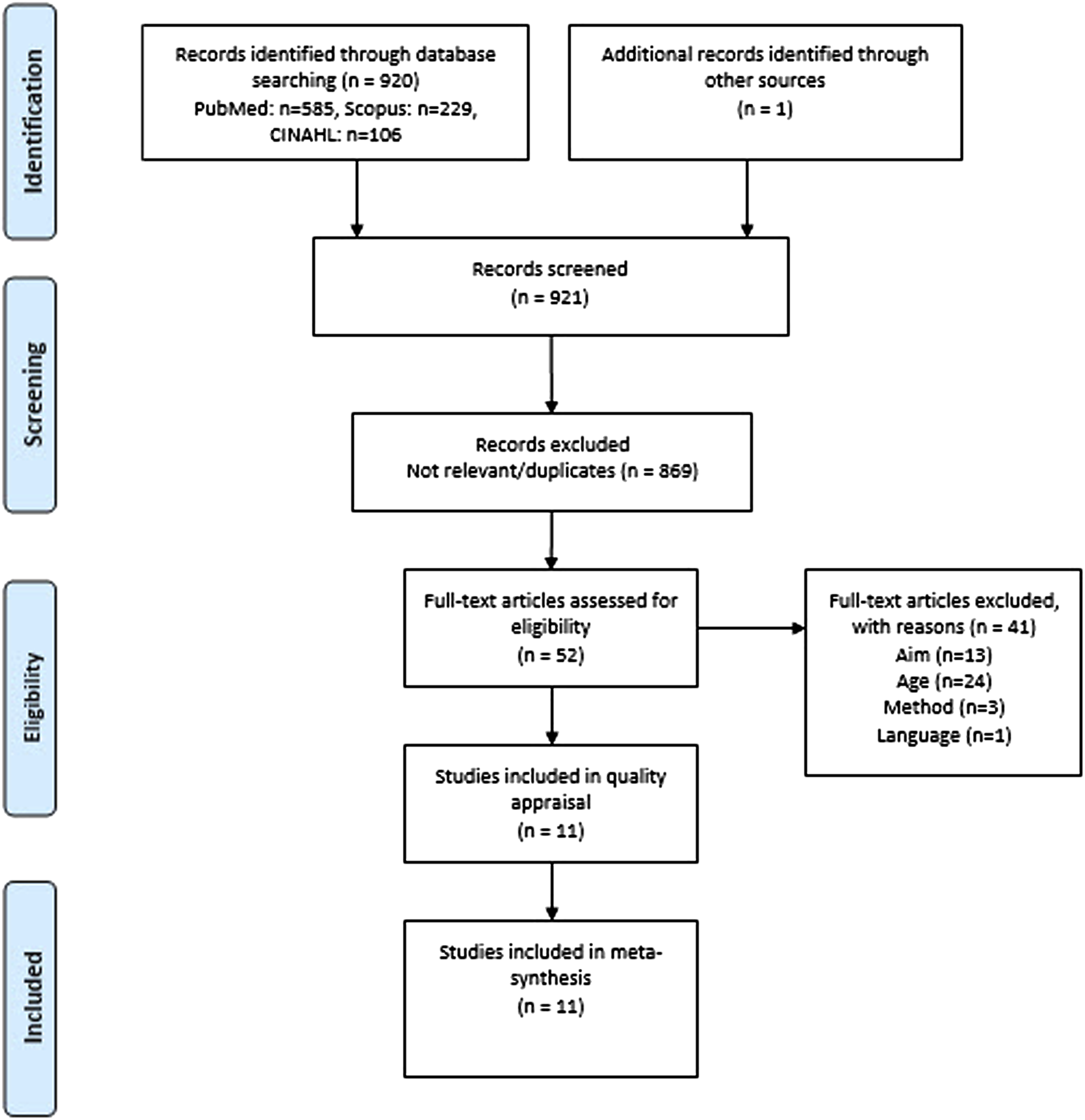
Quality appraisal
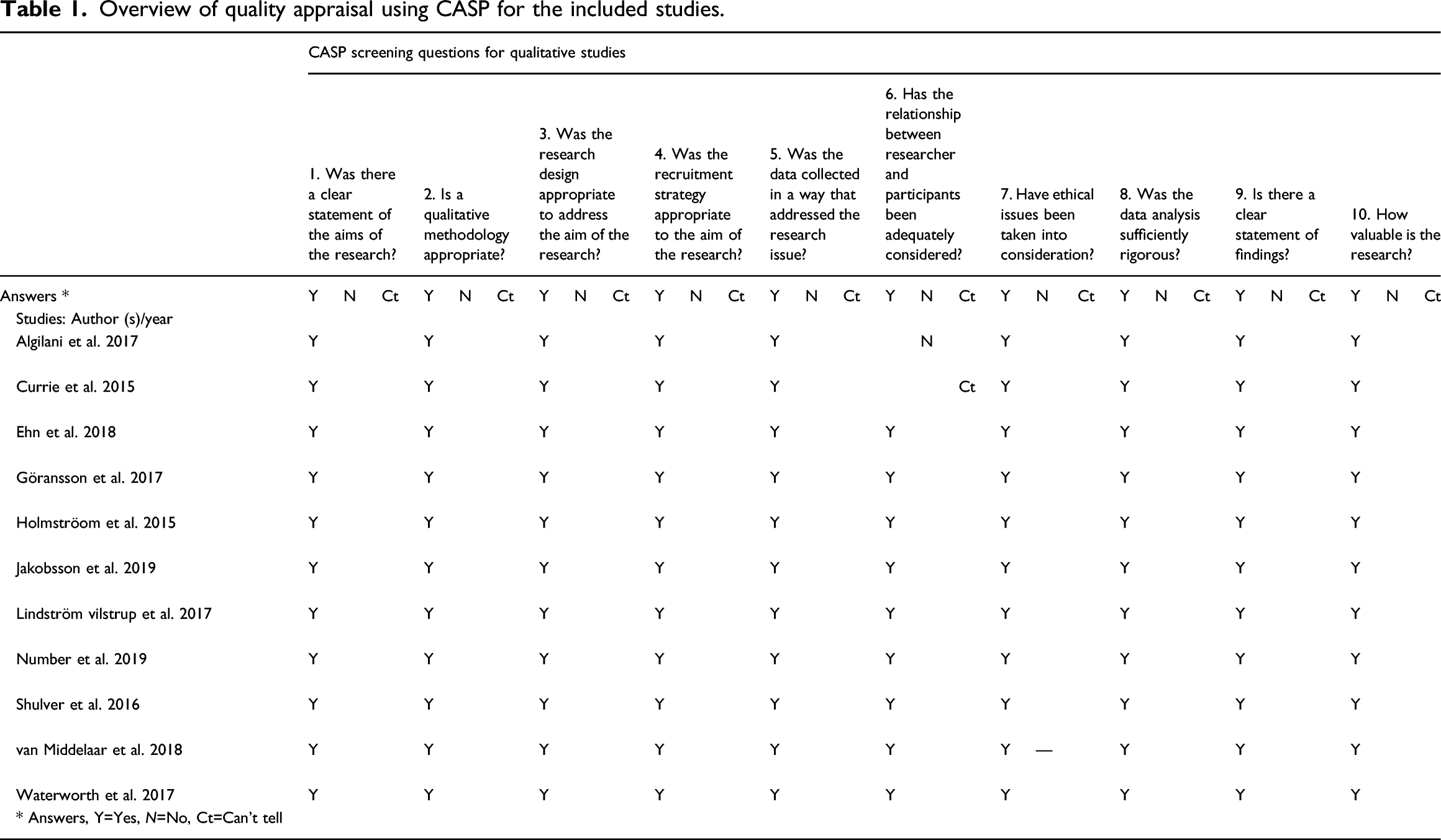
Overview of quality appraisal using CASP for the included studies.
Articles included.
Synthesis
The synthesis process was based on the approach described by Noblit and Hare. 22 The findings sections of the articles were read through repeatedly by three of the researchers in order to get an understanding both of the whole and of the specific details of each article. The researchers noted the interpretative metaphors, that is, the terms, concepts, phrases and expressive quotations. In the next phase, the researchers juxtaposed the findings to make their initial assumption of the relationships between these findings. In this phase, a data extraction template was conducted and the findings of each article were summarized independently. The researchers found that the content was analogous. In the next phase, the extracted findings were related to one another, involving a systematic search for similarities and differences. The last phase, synthesizing translations, was an iterative and inductive process in which the researchers worked together in an ongoing process of moving forwards and backwards between the whole and the parts of the texts. Several possible interpretations were discussed, while pre-existing concepts were re-created into new ones. Finally, after several critical reflections, consensus was achieved between the authors and resulted in six sub-themes that were further synthesized into two themes.
Results
This meta-ethnography aimed to uncover knowledge about older persons’ experiences of eHealth services in home health care. The results are presented under two themes, each with its own underpinning sub-themes.
Overview and context of included articles
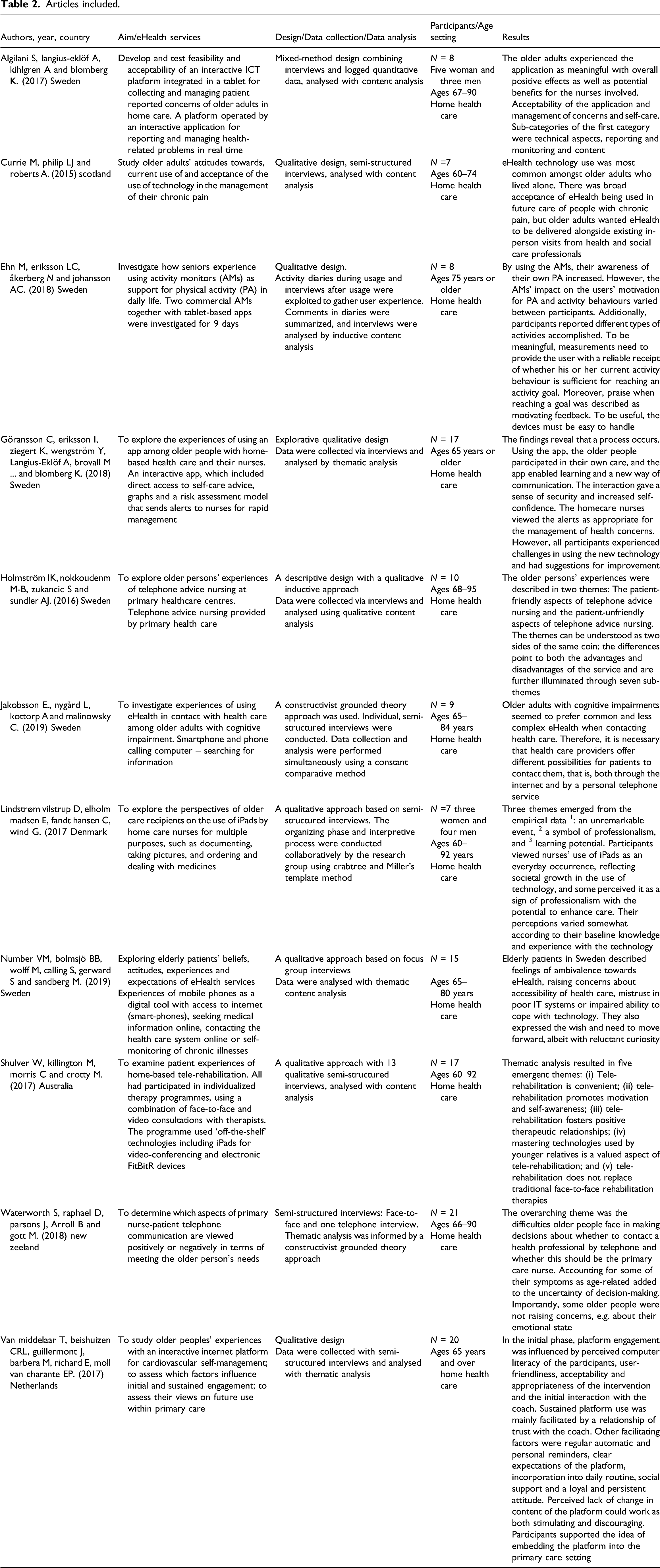
The summaries and context of the articles included are presented in Table 2. 11 studies published in scientific journals between 2016 and 2019 were included in this meta-ethnography. Six were conducted in Sweden with one each from Australia, Denmark, Netherlands, New Zeeland and Scotland. A total of 137 older persons were included (75 women and 58 men). The gender of the three participants in the study from Scotland was not reported. The samples varied between 7 and 21 participants with a gender distribution of 33–75% women and 25–67% of men. All participants were between 60 and 101 years old.
Theme 1: eHealth services as a complement to personal visits
This theme and its sub-themes relate to older persons’ responses to being offered the use of eHealth services. For older persons to want to use the eHealth service, it had to provide some added value to their current contacts with healthcare professionals. In regular healthcare contacts, the eHealth service was not experienced as adding anything beyond the care they already received.
Variations in need for eHealth services
The results show that older persons’ experiences of eHealth services varied in relation to their needs. Persons who perceived a limited need also made limited use of the eHealth service.25,26 They tended to follow their usual routines and did not change their habits in order to adapt to the eHealth service. Being monitored by a system had no impact on their performance. There were other things that did motivate them, such as incipient health problems. 25
To those who were aware of their risk status and were motivated to achieve lifestyle changes, the eHealth service was experienced as relevant. Furthermore, self-care advice, self-management and self-measuring of cardiovascular risk factors were considered to be useful and interesting.26,27
Older persons who regarded their existing contact with their healthcare provider as being sufficient 26 experienced no need for the eHealth services,25,28 and to them, the eHealth service offered no additional benefit. Some were interested in digital solutions, but others preferred to receive an ordinary letter rather than an electronic message. 29 If they had a question or wanted to speak to a specific professional, leaving a voice message did not appeal. 30
The need to be in charge
Any use of the eHealth service provided had to be on the older person’s own terms. They did not want to feel controlled, monitored or pushed into something that they did not choose themselves, 25 nor should the required activities be too time-consuming. 26 Waiting for a call back or not being able to call a specific professional on a direct number made some older people feel that they lacked control, and they viewed the eHealth service as an inconvenience.30,31 Older persons were more inclined to engage in the eHealth services when they could incorporate them into their daily routines and complete them at their own pace.26,27
A controversial complement
The convenience of some eHealth services was appreciated by older persons. Videoconferences and tele-rehabilitation were accepted as supplementary to face-to-face contacts to save time and having to travel. 32 Especially for those with disabilities, the eHealth services could serve as a complement to personal visits. On the downside, access to eHealth services could mean fewer or no face-to-face contacts. If the older person knew the healthcare professional initially, before they started using the eHealth services, and if they knew who was receiving their call or measurements, this facilitated their use.26,28,30 Some older persons stated that they did not experience any major difference between meeting in a videoconference versus face-to-face. On the contrary, they felt that they were given more time, that it was easier to ask questions and that the eHealth service did not negatively affect the therapeutic relationship. Others experienced talking to a screen as inconvenient and preferred to meet the professional in-person.28,32 Some older persons even felt resistant to calling healthcare providers on the phone, and this meant that certain concerns were not discussed over the phone.30,31
Theme 2: The use of eHealth services as a challenge
For many of the older persons, the introduction of an eHealth service meant that they had to learn how to use new technology. While some of the older persons experienced this as a major trial, others experienced the new technology as both motivating and inspiring, and the use of the eHealth services had a ripple effect. For many older persons, the eHealth service made them feel safer, but some did not trust the technology to work when needed.
Technological endeavour
EHealth service systems were sometimes experienced as complicated, and technical problems, to a varying extent, could affect the older person’s use of the service. Their lack of experience with new technologies and with the internet could also complicate their use. 25 Some of the older persons described how they were anxious about crashing the tablet or the application, 27 while others found the telephonic nursing advice difficult to follow, and they had negative experiences of the communication. 31 Furthermore, using internet platforms was experienced as time-consuming. 26 Technical challenges made older persons feel daunted, uncertain, discouraged and incompetent, and this could hamper their continued use of the eHealth service.25,26,31,32
Motivational and inspiring
For some older persons, the use of technology and the eHealth services was experienced as motivating and inspiring.26,27,32,33 Many older persons found the eHealth services easy to handle 25 and that only very basic ICT skills were needed. 34 The eHealth service was regarded as technically free from problems even though the older persons experienced some minor problems, such as entering the wrong pin code or forgetting to charge the device. 27 Older persons who used eHealth services to measure their physical activity experienced that, when used in combination with goalsetting, 25 the activity monitors and scheduled video consultations influenced their motivation in a positive way. 32 A clear, simple and attractive website increased the motivation of older persons to use an interactive internet platform for cardiovascular self-management. 26 In some cases, the use of the service also inspired the older person to use the technology for fun, such as surfing the internet. 33
Lack of trust in eHealth services
Being able to contact a nurse through a secure eHealth service was considered important by the older persons and was seen as having the potential to improve care. However, the use of some of the eHealth services created uncertainty and concern lest the wrong information was registered. Older persons expressed concerns about the safety of video consultations 32 and described difficulties in trusting the telephonic nursing advice. Furthermore, there were uncertainties about whether the technology was reliable and functioning correctly. Waiting for a response often created uncertainty and caused the older person to wonder if the information they had entered into the system had really gone through. 31 Some of the older people became worried that they might have pressed the wrong number or buttons and therefore would not be called back. Not knowing if or when they would be called back together with the waiting time were seen as inconveniences that impacted their everyday lives and routines. Increased availability in the form of direct numbers would improve their experience.30,31 The importance of having reliable eHealth services in place for contacting a nurse was described. 30 The nurse’s use of an iPad in the older person’s home was experienced as both reassuring and professional. 35
Discussion
The results show that personal contact was a prerequisite for using the eHealth services. For an older person to be prepared to use the eHealth service, it has to provide some added value to their current contacts with healthcare professionals. Many older persons did not experience that the eHealth service added anything to the care they already received. The Health Authority 36 states that those persons who have access and knowledge of the eHealth area have greater influence and participation in their care, and the most important factors in the development of internet services for older people to utilize are support, needs, positivity, interest and ease of access. 37 This highlights the importance of support in the implementation of eHealth services in home-based care. Findings show that older persons experience eHealth services as both challenging and motivating. While some experience them as providing safety, others do not dare to trust the technology. The participants also want eHealth service use to be based on their own terms and not be something imposed on them that they cannot control. If the eHealth service is already included in their daily life, it is easier for them to become engaged. These findings are confirmed in a scoping review 38 from the fields of gerontechnology and home-based care, and show both advantages and disadvantages in relation to the experience of safety when using technology. This suggests that ethical considerations need to be taken into account when implementing eHealth services in home-based care. One possible approach that could be used in nursing care is to systematically apply the principles of person-centred care. 39 In order to make the best use of the eHealth services, it may be important to adjust the services not only to each person’s needs but also to their personal capabilities and resources while valuing the older person as an active partner in their own care. Thus, when using the eHealth services, the older person’s perspective needs to be given priority, and decisions must not only be based on organizational considerations. This is especially important as research40,41 has pointed out that older persons have limited possibilities for influencing and making decisions about the content of their home-based care. This is in contrast with the Swedish Patient Act, 42 which claims that the patient has freedom of choice regarding care and the right to influence their own care. This act was introduced with the purpose of strengthening the patient’s rights and position in health care. Therefore, an ethical approach must be observed when designing, testing and implementing eHealth services in home-based care.
Methodological considerations
One strength of this study is the comprehensive literature search strategy employed. Three databases were searched, based on the different focus of each as relevant to this study’s aim. The databases included cover the areas of nursing, medicine and technology, and all were deemed to be appropriate to the study. Another strength is that the search strategy included both indexed and non-indexed search terms, as well as manual searches of the reference lists of the included articles. Despite the comprehensive search strategy, some relevant articles may have been missed due to the different indexing systems of the databases. All the included studies were checked by the CASP screening questions for qualitative studies. Only articles published in the English language were included, which possibly narrowed the search results. Since there seem to be relatively few articles describing older people’s experience of eHealth services in home health care, there is value in compiling existing articles to get insight into this knowledge area.
Opinions differ regarding whether it is necessary to conduct quality appraisal of articles to be included in meta-ethnography. 43 Polit and Beck 24 suggest that articles included in meta-ethnography must, at the least, have utilized appropriate methods, and the findings must be supported by the participants’ experiences in the form of quotations. We contend that a certain level of quality appraisal is needed, and we chose a frequently-used instrument for our quality appraisal. Hence, CASP 23 was used to for the quality appraisal of all articles included, and our results confirm the satisfactory quality of the articles.
Another strength is that three researchers with different research expertise conducted the analytical process. Regular reflections and discussions on the analysis were held by all researchers. These discussions brought multiple perspectives on the study’s phenomena into the interpretations, enhancing the trustworthiness of the findings. Furthermore, the analytical process has been described in detail, which makes it possible for the reader to follow its trail, clarifying its transparency.
Conclusion
In order to make the best use of eHealth services, it is important that the services are adjusted not only to each person’s needs but also to their personal capabilities and resources, while the older person must feel valued as an active partner in the care process. Thus, when using eHealth services, the older person’s perspective needs to be given priority and decisions should not only be based on organizational considerations.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.