
Abstract
Aim/Objective
To examine the perceptions of low-income adults in suburban/rural China regarding health and health management mobile applications. Investigating barriers affecting their adoption of mobile health technology will facilitate better mobile intervention design, lower the medical burden on governments and society, and improve access to health knowledge for vulnerable groups.
Methods
Semi-structured interviews were conducted with low-income adults aged 25–45 (eight women, eight men). The interviewees were asked about their perceptions of health, user experiences with wearables, and mobile health applications.
Results
Interviewees lacked a clear understanding of mental health. Most stopped using wearables due to unpleasant experiences. Making medical appointments or consultations using mobile devices was common to save time and cost, but interviewees did not find devices for monitoring health useful. Interviewees used a variety of mobile applications for getting health information through active searching or by following specific health influencers.
Conclusions
The adoption of digital and mobile technologies for health monitoring and management among the interviewed low-income adults in suburban/rural China is low. Most of the interviewees used multifunctional and content platforms for health information. Low perceived benefits of using mHealth technology hindered adoption. Some stopped using mobile health devices because of poor user experiences. Interviewees found difficulties in identifying genuine health products on popular content and e-commerce platforms. There is an unmet need to provide them with high-quality health knowledge.
Introduction
In China, there are significant disparities in healthcare resources between urban and rural areas,1–3 making mobile health (mHealth) a potential equalizer.1,3,4 mHealth has shown promise in improving access to care for low-income and remote populations in China, particularly in supporting weight and disease management.3,5 Mobile Health encompasses a range of applications, including smartphones and wearables, which are increasingly used by patients, especially for managing chronic diseases and mental health conditions.6,7 As China faces an aging population and rising chronic disease rates, mobile health is transforming healthcare in China by utilizing mobile technologies to enhance access to healthcare for elderly individuals. 1 However, challenges persist in China, such as uneven healthcare resource distribution, regulatory gaps, and public concerns about the service quality of mHealth applications.8,9 The urban–rural divide further complicates access, 2 highlighting the need for targeted efforts to support low-income and underserved communities.
Research conducted on mobile health adoption in rural areas across multiple countries found that mHealth can effectively improve access to healthcare services, remote monitoring, and timely medical interventions.10,11 A study among low-income Latin communities in the United States also found an increased interest in adopting mobile tools to monitor health data for long-term COVID-19 symptoms. 12 As community healthcare resources shrank post COVID-19, low-income interviewees desired to use health wearables for preventative health measures. 12
However, regarding mHealth adoption in low-income communities, research conducted in the United States has identified barriers, including low health literacy, lack of empowerment, and historical mistrust of remote healthcare systems. 13 Similar challenges also emerged in a review of 18 studies in Nepal, where barriers such as weak digital infrastructure, policy gaps, low digital literacy, and lack of financial means hindered the widespread adoption of digital health solutions. 11 These barriers are also highlighted in the rural China context, where factors such as education and income significantly influence mHealth services usage. 14
To improve adoption, it is crucial to focus on user-friendly designs and involve trusted community health workers. 13 There is a need to understand the target population of low-income adults in China, how they perceive health, and whether they are adopting technology in health management. By addressing these needs, mHealth can better help reduce health disparities in underserved populations across China. Mobile health has a promising future in China, with recent rapid growth in initiatives. This study, therefore, addresses an important health issue of understanding the digital divide and health management among low-income adults in China.
Policy motivation of research
Our research has important policy implications. Disseminating health knowledge via digital channels, especially smartphones, is an urgent policy call. In 2024, the National Health Commission in China initiated a three-year Action Plan to improve national health literacy from 2024 to 2027. 15 This Action Plan emphasizes the importance of regulating misleading health information and disseminating scientific health knowledge on the internet. 15 The internet as a health resource is particularly important for vulnerable groups (e.g., people with low income) who are often disadvantaged in access to health knowledge and have limited access to on-site health services.16,17 It is widely accepted that a digital divide exists among different social groups (e.g., the rich and the poor, the young and the elderly).18–20 Recent concepts and definitions of digital divide encompass gaps in access, attitudes, skills, and types of technology usage. 18 As one's eHealth literacy, or the “ability to seek, find, understand, and appraise health information from electronic sources and apply knowledge gained to addressing or solving a health problem” 21 is built on their digital and health literacy, 22 even if useful health knowledge is provided digitally, low-income groups may lack the awareness and skills to access and apply useful health knowledge. To mitigate the digital divide, the Chinese government released the Implementation Plan for Digital Economy to Promote Common Prosperity in December 2023. 23 The plan aims to advance digital development in rural areas and facilitate the inclusive supply of social services through digital means. 23 This study is well-situated within China's health literacy initiatives and digital economy strategies.
Literature review
mHealth development and application in China
Mobile health (mHealth) is defined by the World Health Organization (WHO) as healthcare practices supported using mobile and wireless devices. 24 Research has found many ways in which mobile health is producing promising results in improving the healthcare sector globally, such as in healthcare practitioner training, 25 diabetes treatment, and health habit development,26,27 preventing post-partum depressive symptoms, 28 chronic pain self-management, 29 chronic disease management,30,31 and improving healthcare resource accessibility.32–34 mHealth interventions have also been successful in China, where leveraging mobile devices to enhance healthcare service delivery has been recognized as a tool for strengthening the health system. 4 Mobile health demonstrates the potential to improve care quality, reduce costs, and enhance treatment outcomes by leveraging wearable devices, cloud computing, mobile technologies, and the Internet of Things. 1 This development is particularly driven by the widespread adoption of mobile communication and internet services in China. 1 In 2019, China had 466 million active mHealth application/service users. 35 Ray and colleagues 35 found that the most used or accessed mHealth services were online healthcare and online/mobile health management. Ping An Good Doctor was the most popular mHealth application with 16.2 million active users in 2020. 35 There is a rising trend in the availability and accessibility of mobile healthcare and information exchange through smartphones and wearables in China. 9 The COVID-19 pandemic is anticipated to accelerate growth in China's mHealth market size, with projections indicating it will reach $25.6 billion by the end of 2027. 35 As of 2020, China had a population of 1.439 billion and an average annual population growth rate of 0.39%, making it the second most populous country in the world, offering significant opportunities for the mHealth market. 35
As China progresses towards an aging society, mHealth in China is being rapidly developed to address the challenges posed by the growing elderly population and the increasing number of patients with chronic diseases. 1 China holds an advantage in the development of mHealth due to its advanced mobile communication and internet services, as well as the rapid turnover of smartphone technology. 1 Mobile health demonstrates significant potential in early diagnosis, prevention, and treatment of diseases.1,11 The adoption of mHealth services is gaining interest among Chinese patients. 36 The mental health domain is witnessing a surge in the use of mHealth apps in China for symptom monitoring and disease management. 7 Promising results have emerged from the development and testing of mHealth interventions for people living with HIV in China. 6 In the Chinese context, challenges remain in areas such as service delivery, human resources, information systems, access to essential medicines, and financing. 9
mHealth opportunities and challenges in China
A pressing challenge in China's healthcare industry is the uneven distribution of medical resources and the imbalance between supply and demand.1,3 In China, mHealth resources are mainly concentrated in cities.1,3 Most of the research on mHealth in China is also conducted in urban areas. 37
Mobile health involves not only users of services but also poses challenges for professional health knowledge providers, such as doctors and specialists. Jiang and colleagues 38 examined factors that influence the preferences of medical professionals when providing mHealth services and found that medical personnel tend to prefer mHealth services that offer shorter service durations, higher financial compensation, confidentiality of information, and services targeted at the general population. 38 Similarly, a survey of healthcare providers in the rural United States highlighted how providers believed the barriers to adopting mHealth for patients are largely related to privacy, confidentiality, legal concerns, access to the internet, and complexity of mHealth apps. 39
While the Chinese government supports the development of mHealth, there is a lag in relevant regulations and standards that need to be addressed, such as hospital data sharing, insurance coverage for telemedicine, and pricing for new mobile medical services. 37 How to use mobile medical resources to address the challenges of physical medical resources in developing countries or underprivileged areas, particularly the scarcity of high-quality medical services, remains a major difficulty. 1 Leung and colleagues’ analysis of perceptions among social media platform users regarding telemedicine and mHealth in China found that most of the content analyzed expressed concerns regarding the quality and costs of technology. 8 Challenges also arise in the regulatory environment for mHealth in China as regulations related to mHealth implementation, such as data security, workforce, payment, and service provision, are insufficient and lack clarity, presenting obstacles to mHealth implementation. 37
mHealth for low-income communities
mHealth applications have shown promise in addressing health disparities and improving access to care, particularly for low-income populations. Studies have demonstrated the effectiveness of mHealth apps for weight loss and disease management in China.3,5 The difficulty low-income groups or those in remote areas face in accessing high-quality medical resources underscores the significance of supporting patient self-management and personalized treatment plans in medical practice. Eggink and colleagues 40 and Moll van Charante and colleagues 41 examined the effectiveness of mHealth interventions in preventing dementia by setting personal goals and monitoring their progress in underserved populations at high risk in China. In a sense, these mobile health services are attractive to low-income groups.
Research in the United States has identified that barriers to adoption of mHealth technology and devices include affordability, limited health literacy, lack of empowerment, and historical mistrust of healthcare systems among underprivileged groups.12,13 A scoping review of research on mHealth adoption by people in low socio-economic positions highlights that low digital literacy and lack of access to infrastructure, such as mobile devices and internet services, were among the most prevalent barriers to mHealth adoption. 42 For example, the adoption of wearables and health mobile applications in Hong Kong is limited for low-income people. 43 Obstacles emerged in the downloading process, health application registration, privacy concerns, and lack of awareness of available health apps, with people preferring to search the internet rather than using a dedicated application. 43 Other factors influencing mHealth adoption in China include resource scarcity, accessibility, gender, age, and prior experience with mHealth services. 3 This dynamic suggests that the limited availability of high-value medical professionals can drive greater adoption of mHealth solutions when patients seek alternative channels to receive care. 3
Factors preventing adoption in low-income communities present unique challenges. A survey conducted across 148 Chinese cities found that higher household per capita income and commercial and multiple insurance were associated with willingness to use mHealth devices. 44 Respondents with high scores for health literacy, self-reported health ratings, social support, family health, neighbor relations, and family social status were more likely to use mHealth devices. 44 Among middle-aged and older patients with chronic conditions in rural China, factors of social influences, perceptions of technology, education level, and monthly income have been identified as significant factors affecting intentions to adopt telemedicine. 14
Essential mHealth features for low-income demographics
MHealth shows potential for development in low-income communities and requires tailored approaches to overcome adoption barriers in underserved communities in low and low-middle-income country contexts. 45 In China, the significant gap between the availability of medical resources in urban and rural areas, 2 has positioned mHealth as a potential equalizer.1,3,4 To increase the adoption of mHealth apps, application design should consider visual and linguistic elements, and be introduced to patients through trusted intermediaries such as community health workers. 13 For increasing the adoption of health wearables, devices need to be durable, affordable, or covered by health insurance. 12 Building close relationships with trusted health information sources is more important than the media platform itself. 46
To utilize online communication effectively, research on undergraduate students at an American university suggests that providing accurate and accessible health information would benefit the likelihood of health app usage. 47 Low-income individuals have specific needs for mHealth apps that focus on several key points: first, apps should support multiple languages and include cultural content, such as recipes and motivational tools, to enhance acceptance. 48 Second, improving accessibility is crucial to ensure usage, while privacy protection is essential for building trust. 48 Another study among low-income working adults in Hong Kong found that an ideal mobile health app should provide guidance for maintaining a healthy diet and exercise routine, help identify health issues from symptoms, and offer suggestions for improving mental well-being. 43 Accessible psychological assessments to support mental health were welcomed, while preference was also expressed for videos on lesser-known health issues, information about local healthcare providers, and tips for pain management. 43
Although Venkatesh and colleagues’ Unified theory of technology acceptance model considers social influence as a predictor of mHealth usage, 49 research found that peer norm was less important than attitudes and usefulness in predicting mHealth usage. 47 These needs highlight the urgent expectations of low-income populations for accessibility, adaptability, and support in managing their health. 48 The features include education to reduce uncertainty, support communities, visual progress tracking, convenient information access, and better management of pregnancy-related tasks. 50 By identifying several key factors affecting low-income people when adopting mHealth, it was proposed that mHealth apps should be accessible, reliable, and culturally and socioeconomically appropriate for low-income communities. 45
Methodology
Convenience sampling was adopted. A total of 16 participants (eight males and eight females) were recruited through the social networks of the first author. Interviewees were aged 24–45 at the time of the interviews and lived in a suburban/rural area of Shandong Province, China. They were students, housewives, unemployed persons, or workers. The demographics of the participants are provided in Table 1.
Interviewee demographics.
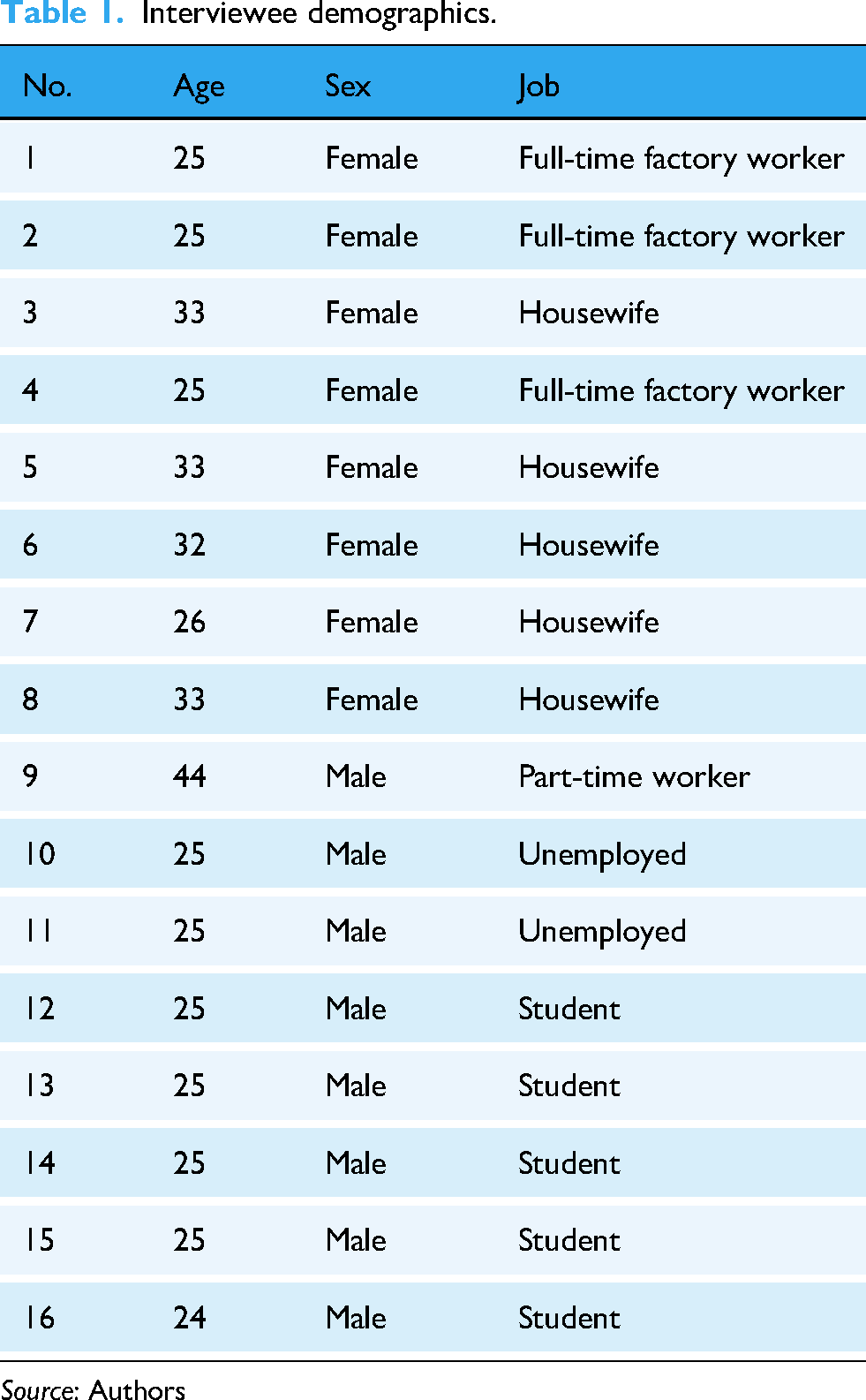
Source: Authors
Ethics approval was obtained from the first author's university before data collection (Approval number: JUME2023/0626). Semi-structured interviews were conducted on a one-to-one basis. The interview questions listed in Appendix 1 were formulated based on a previous study, 43 with modifications to accommodate the mainland China context. The questions cover the following topics: perception of “being healthy” and “not being healthy,” measures taken (or avoided) to stay healthy, use of wearable mobile health devices, use and perceptions of different kinds of mobile health apps, and perceptions of mobile health apps in general. The interviewees were also asked to show the health apps they used and the information they often paid attention to in each app. Screenshots of these apps were captured.
The interviews were conducted face-to-face in December 2023 by the first author. Before the interviews, the research purposes and procedures were explained to all interviewees, and written consent was obtained. Written consent to publish was obtained from all participants. Interviewees were paid 50 yuan (equivalent to seven US dollars) for participating in the study. All interviews were audio-recorded and transcribed. As some interviews were conducted in the local dialect, it was important to transcribe the recordings accurately. To improve accuracy, the transcription was done in three steps: first, the recordings were automatically transcribed via iFLYTEK software, a reputable intelligent voice technology device for transcription. A research assistant then checked and revised the transcripts word by word. Lastly, the first author checked the transcripts against the original recording to ensure accuracy of transcription.
The data was analyzed using an inductive content analysis approach. Analysis was done via NVivo 11 software. Transcripts were first open-coded, i.e., the first and second authors read through two interviews and recorded brief conceptual codes reflecting what was being said by the participants indpendently. 51 Codes with discrepancies between the coders were resolved through discussions. The first author coded the remaining 14 transcripts and the second author cross-examined these codes. Again, discrepancies between the coders were resolved through discussions. The finalized codebook was developed through the process. No formal reliability statistics were compiled. Emerging and recurring concepts in the data were identified and integrated into themes. A coding tree for perception of health contributing to theme 1 is shown in Figure 1 as an illustration. Representative quotes were selected and translated into English.

An example of the theme coding tree. Source: Authors.
Results
All the interviewees were able to recall at least three mobile applications they had used for health-related purposes. On average, they were able to recall seven applications. A total of 29 distinct mobile applications were mentioned. The icons, application names, and the frequency with which interviewees mentioned them are listed in Table 2.
Mobile applications used for health purposes (and frequency of mentions).

Source: Authors
The three most frequently mentioned applications were Douyin (the Chinese version of TikTok), WeChat, and Baidu. A range of mobile app types was cited, including content apps, e-commerce apps, fitness apps, medical service apps, and female-targeted apps. Most of the reported apps were content apps or multifunctional apps with intensive content exposure. For example, WeChat is an example of a multifunctional app. It is the most widely used instant messaging application and the top mobile community in China in 2025, with 1.41 billion global monthly active users, 52 and as of 2021, China was the home of the highest number of WeChat users with approximately 810 million users. 53
In addition to messaging, WeChat users can also pay bills, place orders, play games, etc. It is common for them to spend a large amount of time on WeChat skimming texts and videos generated by other users. Some of the content apps were video-based, such as Douyin and Kuaishou. Some were text-based and blended with videos, such as Xiaohongshu and Zhihu. As for e-commerce apps, interviewees typically used them to purchase health supplements or over-the-counter medicine. Among fitness apps, Keep was the most frequently mentioned. Keep provides one-stop exercise solutions such as fitness teaching, running, cycling, making friends, fitness diet guidance, and equipment purchase. The choice of fitness apps was often affected by the brand of the interviewees’ smartphones. For example, interviewees who use a Huawei smartphone were more likely to use the Huawei Health app. As for medical service apps, only two were mentioned. Medical service apps were rarely used because most medical service institutions have their own WeChat accounts or mini-programs, allowing users to directly access their services via WeChat without the need for a separate app. Several female interviewees mentioned two female-targeted apps, Meiyou and Baobaoshu. Meiyou is a comprehensive health management application for women. Baobaoshu is a maternal and infant community platform. All interviewees had experience of using mobile apps for health-related purposes.
Through thematic coding of the interview transcripts, six themes emerged.
Theme 1: Interviewees had clearer ideas about physical health than mental health
Interviewees generated far more ideas concerning physical health than mental health (referring to Figure 1). Altogether, interviewees mentioned physical health attributes 46 times (some were replicated), but mental health attributes only 17 times. As a general pattern, interviewees tend to describe health either by what it is or by what it is not. As for physical health, interviewees mentioned biochemical indicators, subjective feelings, and healthy lifestyles. Other attributes included having a florid face, a well-functioning body, and perceptions. From an eliminative perspective, interviewees described physical health as freedom from illness, handicap, or sub-healthy conditions. The most extreme response posited that “Being healthy means having six-pack abs. You should be able to run 1000 meters in under three minutes and thirty seconds, do at least ten consecutive pull-ups, and bench-press more than 80 kilograms” (S16, male; student).
Three interviewees reported having no idea about mental health. Mental health was often related to having positive values/mindset/energy. One described mental health as “being normal” from a social perspective. Those who described mental health in an eliminative manner said mental health is not being extreme/unenergetic/bothered/worried/mentally ill. Below is a typical quote. It is also related to mindset. When your mindset is positive, you naturally feel more mentally content and healthier. A healthy mindset involves positive thinking and avoiding negative thoughts, which constitutes mental health. (S7, female; housewife)
The most extreme response posited that “Mentally speaking, people who have received criminal punishment or violated the law—I think that also counts as mental unhealthiness” (S8, female; housewife).
Likewise, interviewees were able to provide more concrete descriptions of not having physical health compared to not having mental health. As for not having mental health, depression or anxiety was most frequently mentioned by five interviewees, followed by “feeling stressed or hopeless.” Some interviewees associate mental health with delinquent thoughts or behaviors. They considered those mentally unhealthy as “holding problematic fundamental values or thoughts,” “being rebellious or violence-prone,” or “having a filthy mindset.”
Theme 2: Half of the sample had used wearables, but most of these had stopped using them due to unpleasant experience or perceived limited benefit
Among the 16 interviewees, eight said they had used wearables such as sports watches or sports bracelets. Only two of them were still wearing wearables at the time of the interview. The remaining six interviewees stopped using wearables mostly because they perceived the user experience to be unpleasant or the perceived marginal gain of using wearables to be minimal. They found the data provided by the wearable redundant after a while. Sometimes these devices can backfire. Below are three typical quotes. I feel that wearing it on my wrist is always uncomfortable. I think it could be designed to be more convenient and comfortable. Right now, I find it quite uncomfortable, especially when sleeping. Although it can track sleep, I always feel it pressing against me. Comfort is one aspect [of the device] that needs improvement. (S1, female; full-time worker) Yes, I wore a Xiaomi sports bracelet before. I used it for a while and found it somewhat useful, but not very much. It can monitor your heart rate, but after a while, you won't pay much attention to it. Constantly checking your heart rate can become a burden, making you feel anxious. If you see your heart rate is too high, you might want to stop exercising and rest, which prevents you from pushing your physical limits. (S10, male; unemployed) You seldom use these devices, like for running. Even when you run, the data it displays isn't very useful; it just provides a reference value…You might consider its data, but it won't really lead to any significant changes. (S14, male; student)
The perceived benefits of using wearables included increased awareness, entertainment, convenience, and precise feedback. Because users can easily check fitness data by looking at the wearables on their wrists, many perceived that wearables are convenient and increase their awareness. Some were not fully convinced that the data was accurate, but may still wear them for fun. Eight interviewees had never used wearables but were aware of such products. They never used wearables because they did not see the value of using them.
Theme 3: Interviewees made online medical appointments or consultations through mobile devices and found it convenient
Nine interviewees reported that they have made online medical appointments or used remote consultation services through their mobile devices. The remaining seven interviewees did not use such functions either because they rarely needed any health services, or they preferred traditional in-person consultation. The most frequently used app for making online appointments was WeChat. Interviewees usually made medical appointments through the official WeChat account of a hospital or the mini programs built into WeChat. Interviewees perceived these channels to be convenient, time-saving, and easy to navigate. Below is a typical quote. It is more convenient and timelier. When you need to book an appointment, you can do it directly on your phone. If you do it offline, you might need to get up early in the morning, rush over, and then wait in line. That is very inconvenient compared to this. Also, on your phone, you can clearly see which specialist you want to book, and it shows the available time slots. (S4, female; full-time worker)
The most frequently used app for remote consultation was Baidu. Usually, interviewees would search for certain symptoms they experienced using Baidu. Sometimes chats would pop up automatically, and interviewees could proceed with the consultation, even if it was not free. A paid remote consultation was perceived to be more affordable than a hospital visit, as well as being available 24*7. Even though interviewees did not trust remote consultation as much as they trusted traditional hospital visits, they still treasured the immediate mental comfort brought by the remote service. Some also found remote consultation affordable. Below is one typical quote. I developed a large cyst on my face. At that time, I used Baidu to consult a doctor online about this issue, and it lasted for about a month. It was very affordable because online consultation costs less than 10 yuan for a month. You could send messages to the doctor, and they would reply. I would contact them every one or two days because they had prescribed me medication. I would send photos to show the progress or ask what to do about the cyst on my face.… Baidu is more like a way to relieve psychological anxiety. It addresses urgent needs immediately and gives instant feedback on your anxious emotions, which is quite important to me. (S13, male; student)
Two interviewees expressed concern about the credibility of the apps. They found official apps developed by hospitals more authoritative and credible.
Theme 4: Interviewees did not find digital devices for monitoring health conditions and health-related behavior useful
Many interviewees had the habit of monitoring their daily step count, mostly using WeChat Sports. They chose WeChat Sports because it was easy to access and was linked to a social network. Yet one interviewee reported he stopped using WeChat Sports exactly because of the latter feature. You would feel that WeChat Sports invades your privacy, especially when it publishes your step count on the dashboard. (S11, male; unemployed).
A few interviewees used “Keep” to monitor their jogging performance (e.g., exercise trajectory, step count, exercise duration, and average speed). Some interviewees never recorded health-related behavior using digital devices due to their low awareness. I haven't used any of these. I haven't really paid much attention to related stuff and haven't used this kind of thing. (S6, female; housewife).
One interviewee recorded his behavior in a traditional way, using pen and paper. He would then calculate the calorie intake using a calculator. Some interviewees attributed the infrequent use of health apps on their mobile phones to their limited digital skills. Speaking of smartphones, I don't quite understand them. I just don't really know how to use them well. (S9, male; part-time worker)
Some interviewees used apps to monitor their own health, but stopped the practice because they perceived it to be either unreliable or easily forgettable. App options differed between genders. For example, two female interviewees reported that they used Meiyou, a health management app designed for women. Both women used it to track their menstrual cycles, and one also used it to track the different stages of her pregnancy. Male interviewees did not report the use of any gender-specific apps.
Theme 5: Interviewees had mixed views about the quality of health products offered online
Thirteen interviewees had purchased health products online, mostly through e-commerce apps, with health supplements such as vitamins being the most frequently mentioned product type. Those who purchased medicine online did so either because the medicine was not available offline or because they were attracted by the lower price. Below is one typical quote. There's also a platform called Shengyuan Xinxiangou, which I follow because it focuses on eye health. They sell a product related to myopia, an eye treatment ointment. I’ve bought about four of them from this platform…Because my child's prescription suddenly increased, reaching over 300 degrees, my main goal now is to prevent it from getting worse and stop the prescription from increasing further. (S5, female; housewife)
The most frequently used apps for online shopping were Taobao, Jingdong, and Pinduoduo. Many interviewees purchased health-related products through more than one app and had different impressions of different apps. Interviewees’ purchase decisions were often affected by price, availability, user comments, delivery time, and after-sales service. In general, they found these apps convenient and cost-effective, and rich in product variety.
Interviewees expressed concern about the trustworthiness of different online shopping apps. Some perceived them to be trustworthy because the apps showed the sellers’ quality assurance, record of reputation based on credit rating levels, and positive comments from many buyers. Others were dubious about certain apps because of insufficient advertising regulation, difficulty verifying the genuineness of user comments, and a lack of professional endorsement. Some also complained about too many advertisements pushed by the apps. Three interviewees had never purchased any health products online because they were afraid of getting counterfeit products. They felt local pharmacies were more trustworthy than online ones.
Theme 6: Passive information encountering and active host-following were two common ways of getting health information
Interviewees used a variety of apps to acquire health knowledge. A total of 16 apps were reported. Some were search engine apps, including Douyin, Xiaohongshu, Keep, Baidu, and Kuaishou. Interviewees used these apps to gain health knowledge about exercise, training, yoga, body-shaping, posture, healthy recipes, nutritional content, etc. Exposure to health messages was both passive and active. In the passive scenario, interviewees were fed with posts about health topics when they viewed short videos. If they were interested, they would click the link. In the active scenario, interviewees had a health topic in mind and searched for it in the apps. Some went further and followed the hosts to keep updated about certain health topics. Below are two typical quotes. As for Douyin, I think when you want to look up a question, it can be very fast. Since the content is organized into short videos by category, it's relatively easy to quickly grasp where your problem lies…For some topics, it can quickly summarize key points, and then you can rapidly understand the issue. (S12, male; student) I don't actively search on Xiaohongshu, but when I see someone sharing a recipe, I'll click to take a look. (S11, male; unemployed)
Discussion
Poverty is often linked to poor health.54–56 This article focuses on low-income adults from rural/suburban China, exploring their perceptions of health and their user experience of wearables and mobile health applications. This study adds to this important yet understudied field and responds to the call for more empirical evidence on the effects of different socio-economic factors on the usage of mHealth technologies. 57
In line with existing literature, active information seeking and passive information encountering are two major avenues for health information acquisition.58–60 Compared to low-income adults from Hong Kong, 43 and the UK, 61 interviewees in this study on average use more digital health apps and use the apps more frequently and deeply. For example, 13 apps are only mentioned once by certain interviewees, indicating a highly competitive digital application market. This relatively high use of mobile applications for health purposes reflects the high penetration of digital technology into Chinese consumers’ daily lives. The rapid technological innovation driven by the three major players, including Baidu, Alibaba, and Tencent, and the newly evolved tech leaders such as ByteDance and Meituan, is shaping the digital economy and AI-driven content delivery system. 62 Drawing from the identified barriers affecting widespread adoption of digital health solutions in Nepal, our interviewees reported access to mobile devices and digital infrastructure, thus the barriers to their adoption may lie in digital inclusive policy and low digital literacy. 11 This finding indicates that China has overlooked the market of the low-income group and their unmet needs for improving health conditions. If the market demand is better understood and catered to, people are likely to install more mHealth applications on their smartphones.
The low understanding of mental health grounded in interviewees’ accounts echoed a similar finding among the low-income working adults in Hong Kong. 43 Interviewees’ negative perceptions of people with mental issues reflect the public stigma of prejudice against those with mental health problems. 63 From a policy perspective, raising mental health awareness and health literacy among disadvantaged groups is of practical importance and an urgent policy call. 64 This is especially apparent after the COVID pandemic, where economic downturn worsened the job market and elevated people's daily stress.65–67 The Chinese government announced a new nationwide hotline “12356” in December 2024 to provide accessible mental health support. 68 However, no interviewees reported using the hotline. This may reflect insufficient promotion of the availability of this health resource.
Interviewees’ understanding of mental health correlates with positive thinking, optimism, and high energy. Their association of poor mental health with anti-social intention behaviors indicates a lack of understanding of mental health as a state of mind characterized by the American Psychological Association's definition as “emotional well-being, good behavioral adjustment, relative freedom from anxiety and disabling symptoms, and a capacity to establish constructive relationships and cope with the ordinary demands and stress of life.” 69 This finding echoes the results of an in-depth analysis of 146,625 Weibo (Chinese equivalent of Twitter/X) posts identifying stigma and mental health literacy as the major factors influencing attitudes toward mental health issues. 63 Five out of 16 interviewees identified symptoms of poor mental health, such as anxiety or depression. The other interviewees may not know when to seek mental support. Thus, more proactive health education on mental health may be needed, such as accessing voluntary mental health checks and offering free mental health training to the vulnerable.
From a practical perspective, the design of wearables may need to prioritize different features (e.g., comfort, fashion, activities measured, durability) depending on the target consumers. Tailoring mHealth interventions to the needs of target groups was amongst the most prevalent factors influencing mHealth intervention adoption in prior research. 42 Moving forward, companies in China should recruit people from low socio-economic status groups to provide input based on their unique needs during the test phase for wearable health products development. The physical activity options available on wearables may be inherently discriminative. For example, researchers found that the emphasis on leisure-based activities (e.g., walking, swimming) likely underestimates the activity levels of those engaged in manual labor and consequently limits the value low-income groups can derive from such devices. 70 In research among low-income Latin communities, interviewees also looked for durable and affordable wearables due to their labor-intensive occupations. 12 This failure of wearable health technology to meet the lifestyle profile of the present study's interviewees may explain why many ceased using wearables.
The design and marketing of mHealth apps in China also need to tackle the potential frictions brought by inherent discrimination towards people with low socio-economic status. Although interviewees have cultivated the habits of monitoring health using mobile devices, health behavior monitoring is shallow and partial. For example, step count is more valued as an entertainment and social event than as a health behavior indicator. On the one hand, the fact that step count features are commonly used among the interviewees signals potential penetration opportunities for companies to develop other health behavior monitoring applications. On the other hand, it is important to retain simple and popular features. Research has shown that ranking improves engagement and performance of participants as well as their perceived happiness. 71
One interviewee reported privacy concerns for a specific feature of WeChat Sports as a barrier to adoption. Contrary to the extant literature,10,11,39,43 privacy and confidentiality issues were not brought up as barriers to general mobile health application adoption. This may be attributed to the low awareness of data privacy among most interviewees about how personal data is monitored, distributed, or used by third parties through the applications. Unlike the study among low-income Latin American interviewees, 12 most interviewees in this study did not express distrust of health systems or the technology companies. They did not express concern about how data collected by the mobile health devices would be disseminated, unlike Cruz et al.'s findings amongst their interviewees. 12 These findings amongst interviewees of this study highlight a digital divide regarding awareness of rights and vulnerability among disadvantaged groups in China that needs investigation and addressing.
Limitations
This study has its limitations. First, interviewees’ heavy reliance on multi-functional and content platforms such as WeChat would shape their exposure to health information. Second, there was the issue of social desirability bias, where interviewees report what they perceive to be socially acceptable. 72 This bias was controlled in this study by establishing rapport in the introduction of the study and the use of factual questions. Third, the sample size was not determined by theme saturation. Therefore, other themes may have been identified if more interviews had been conducted. Fourth, translating representative quotes from Chinese into English introduces the potential for translation bias. Fifth, the qualitative and explorative nature of this study, along with the use of a convenience sampling method, may limit the generalizability of findings. Future research can adopt quantitative study methods to triangulate the findings.
Conclusion
This study explores the interaction between low-income adults and digital health apps/devices in China, adding to the heated discussions on the digital divide and health management. The interviewees had access to digital and mobile technology. However, the adoption of these technologies for health monitoring and management is not prevalent. Access to health information through mobile devices was prevalent. Mobile health devices in health management were considered to offer insignificant benefits. Based on interviewees’ accounts, it can be inferred that there is an unmet need to provide this group with high-quality health knowledge. Findings of this study inform tech companies in the design and marketing of relevant mobile health applications and products catering to this need. Promoting mental health literacy and interventions by means of strategies such as community-based health education should increase overall social welfare and improve public health conditions. In view of interviewees’ difficulties in assessing the quality of health products featured on popular platforms, we call for more vigilant government regulations to address the dangers of misleading health product information on the internet.
Footnotes
Acknowledgments
The authors acknowledge the contribution of Ms. Yuyuan Zhuo in conducting the literature review.
Contributorship
Jie Chen and Kara Chan were responsible for the conceptualization and design of the study. Jie Chen contributed to the investigation through data collection. Jie Chen and Kara Chan contributed to formal analysis and the preparation of the manuscript.
Ethical considerations
This study was approved by the Jiang Su University Medical Ethics Review Board dated June 26, 2023. (Approval number: JUME2023/0626)
Consent to participate
Informed consent was obtained from all participants involved in the study. Written consent was obtained from all interviewees for participation in the study and the publication of the manuscript.
Consent for publication
Written consent for publication was obtained from all participants in this study.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Education Science Foundation of Jiangsu Province (grant number B/2025/01/66), Senior Talent Foundation of Jiangsu University (grant number 22JDG001), and a commissioned research grant from Wenyuan Street Office in Shandong (grant title: Pension Security and Health Status of Farmers in a Steel-Industry Transition City).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Raw data is not publicly available to preserve individuals’ privacy. The data that support the findings of this study are available from the corresponding author, Kara Chan, upon reasonable request.