
Abstract
In order to understand if a physician prescribed medical information changes, the number of hospital readmission, and death among the heart failure patients. A 12-month randomized controlled trial was conducted (December 2013–2014). Totally, 120 patients were randomly allocated into two groups of intervention (n = 60) and control (n = 60). Accordingly, the control group was given the routine oral information by the nurse or physician, and the intervention group received the Information Prescription (IP) prescribed by the physician as well as the routine oral information. The data was collected via telephone interviews with the follow-up intervals of 6 and 12 months, and also for 1 year after the discharge. The patients with the median age of (IQR) 69.5 years old (19.8) death upon adjusting a Cox survival model, [RR = 0.67, 95%CI: 0.46–0.97]. Few patients died during 1 year in the intervention group compared to the controls (7 vs 15) [RR = 0.47, 95%CI: 0.20–1.06]. During a period of 6-month follow-up there was not statistically significant on death and readmission between two groups. Physician prescribed information was clinically and statistically effective on the reduction of death and hospital readmission rates among the HF patients in long term follow-up.
Keywords
Information interventions in diverse forms such as oral education, multimedia, and written information are common in patient care.
Information therapy or prescribing specific evidence-based medical information to patient is different from formal patient education.
Information to be effective on the patient care need to be prescribed by physician/specialist who is in medical relationship with the patient and be personalized with the patient’s condition at the time of care.
Information prescription intervention in long term follow-up is effective on the heart failure outcomes. The impact of information intervention on death and hospital readmission after 12 months was more effective compared to 6 months.
In information intervention, the patients’ engagement, concentration, and preference are the key factors.
The effect of information intervention diminishes at sever stage of HF patients with heart failure
Introduction
Heart failure (HF) is a chronic condition, which has a substantial place in the global burden of diseases, and is known as the main cause of hospital admission among the elderly people. 1 Moreover, HF usually leads to the hospital readmission within 60 days after the discharge,2,3 and also causes death within 1 year after the hospitalization. 4 “Three-fourths of all HF hospitalizations are due to intensification of the symptoms in the patients with the known HF. One-half of the hospitalized HF patients experience readmission within 6 months.” 5 The non-compliance with the treatment regimen, either diet or drug, is known as the primary cause of hospital readmission after discharge for the whole chronic conditions, 6 which is exceed over 50% in the case of HF. 3 To reduce HF re-hospitalizations or death, identification and implementation of low cost and low risk interventions are essential. Information prescription is known as a risk-free and low cost intervention dealing with the patients’ awareness and adherence.7–9 Patient information contents and decision aids are essential tools for helping patients with informed decisions and share in decision-making. But the quality of patient information materials available at general practices is not evidence base and based on recommendations. 10 Recent studies are indicator of high knowledge expectations of patients with heart failure that majority of them (83 %) remains unfulfilled. 11 Prescribing evidence based information by medical doctor for the specific patients is one of the novel approaches in the field of patient care, which is originated from the philosophy of evidence-based medicine (EBM). Information prescription (IP) is defined as prescribing and providing a patient with evidence-based health information to help him/her understand, manage, and then control the illness.8,12 In information prescription, the key issue is to provide right patient with right information at the right time. 13 The right information can play a therapeutic role for a specific person at the time of care. Moreover, right information has some general features and some specific criterion. In this regard, the general features of IP are that it must be backed with scientific evidence; need to be helpful in decision making on the suggested medicine, exercise, food and nutrition; should be easy to understand; and be free from commercial bias. 14 The specific features of IP differ from a patient to another, so information prescription needs to be personalized based on the patient’s medical condition, literacy, culture, and beliefs. The best IP is the one, which is prescribed by the medical doctor who is involved in the patient’s treatment and health care using evidence based and up-to-date information based on the guidelines and recommendation. Once the doctor prescribed the information, then it can be provided and dispensed by a clinical librarian, 14 health information management (HIM) professional, 15 and a nurse 16 However, it needs to be confirmed by the medical doctor before the application to ensure that information meet the patient’s specific medical condition and interindividual variabilities. When a physician prescribed and personalized information is delivered to the patient, the commitment and concentration of patients and the patient-doctor relationship will be improved. This is supported by the related literatures,14,17,18 even by the Chinese QiTherapy that is a kind of Information therapy.19,20 Information is usually prescribed by medical specialist or health care provider along with other remedies as complementary medicine or sometimes just as the only remedy depending on the patient’s medical history and condition.13,14 Information can be delivered to the patients via different channels such as a file sent by email, a link to a website, a printed/electronic copy of information directly given to the patients by the physician, 21 by a pharmacist via integrated pharmacy management software with patient electronic health record (EHR), 22 or by information provider/librarian following a prescription directed by a physician.14,23 Also, information prescription is usually implemented/performed under chronic condition when the patients’ self-care, engagement in control and management of illness, maintaining health, or coping with illness is essential.
Review of the related literature showed that, the content of online information is complex, not easy to read, has compliance with the patient’s level of literacy,24,25 insufficient and unreliable.10,11,26 Up to now, there is no sufficient evidence on the effectiveness of physician prescribed information delivered to the heart failure patients to minimize the rate of hospital readmission and or death. Therefore, the primary aim of this randomized clinical trial study was to assess the effect of a patient centered and physician prescribed evidence-based information prescription (IP) intervention on reducing the hospital readmission and death among the HF patients.
Methods
Design and participants
This randomized controlled study was conducted in one of the tertiary referral heart hospitals in Iran (Shahid Madani Heart Hospital). Accordingly, Madani Heart Hospital consists of cardiology and cardiac surgery wards, heart emergency care section, and Coronary Care Unit (CCU), and serves as the main hospital for Angiography, Percutaneous Coronary Intervention (PCI), Coronary Artery Bypass Graft (CABG), and many other heart operations and inpatient and outpatient managements in the East Azerbaijan Province and also neighboring countries. The sample size was identified based on the hospital’s internal statistical reports referring to the daily admission of an average number of three patients with HF. Also, it was estimated that, at least 120 patients should be included based on the average assumption of the readmission rate in a period of 3-month data collection. The power analysis was performed by STATA v.14.0 and addressed 0.62 (62%). HF patients were admitted to Tabriz Shahid Madani specialty heart hospital from December 2013 to December 2014. Upon the approval by the ethics committee of the Tabriz University of Medical Sciences, the patients have been asked to participate in this study. Afterward, the patients were enrolled in the study during a 3-month period from December 2013 to February of 2014, and were randomly allocated into two groups of intervention (n = 60) and control (n = 60). The investigator was available in the morning and afternoon present at the hospital to conduct the interview to collect the demographic data and the written informed consents. In addition to the patients’ self-reported information, we checked the patients’ medical record to derive background information about their age, marital, literacy, and gender before conducting the interview sessions. Also, we used their self-report information about their prior knowledge on HF and not having someone knowledgeable among the care givers and family members. Moreover, we considered these data to be sufficient because their attitude and behavior were also the indicator of their honesty. After the intervention, we used the interviews to collect data. The interview was done in the patient’s convenient time by his/her agreement. Notably, in these sessions, we used voice recorder to record the interviews. We also took note while they were giving response to the questions. Following completing each interview, we entered the data into Microsoft Excel file for future analyses. This gave us opportunity to check the questions and the data once more, before moving to the next phase of the study. Also, the follow-up interviews were done by telephone conversation. The telephonic interviews were also recorded by the cellphone voice recorder. The informed consents were completed before the intervention through the written forms provided by the committee of research ethics.
To be eligible, the chosen patients had to meet the following inclusion criteria:
Clinically diagnosed as HF patients:
To have New York Heart Association class II–IV symptoms in the first admission.
Patients who had no previous information on the treatments that was going to receive, and had no source to obtain the necessary knowledge about the HF and treatments other than this process.
Being literate (able to read and write) or being cared by a literate person who was responsible for the reading and then following the information prescriptions for the patient.
Age not greater than 85 years old.
Exclusion criteria were as follows for the clinical condition and personal ability:
Lower level of consciousness (LOC), so that the patient cannot receive information or respond to the questions.
Diagnosed with other chronic diseases such as kidney or thyroid (based on the patient’s medical record).
Being under dialysis (based on the patient’s medical record).
History of a clinically diagnosed mental disorder, any type of mental disorders (based on the patient’s medical record).
Being informed (those patients who had prior knowledge of his/her disease, treatments, drugs, trials, symptoms, and management of diseases were excluded).
Control group: the control group matched to the intervention group. Before dividing to the intervention and control groups, all the criteria were matched. The patients enrolled in the control group received the routine oral information given by their nurse or physician.
Random allocation and blinding
Randomized controlled trials (RCT) are known as the best method to demonstrate causation and the best evidence in the level of evidence, despite having various limitations. Random allocation is a technique that chooses the individuals for the treatment groups and control groups entirely by chance disregarding the will of researchers or the patients’ condition and preference. This allows researchers to control all the known and unknown factors that may affect the results in the treatment and control groups. Based on the randomization guideline developed by Kim and Shin Kim and Shin (2014) a block randomization was used. Afterward, we created a block to equally assign the sample numbers to each group as well as assigning the block. The patients were randomly divided into the intervention and control groups using an allocation sequence based on the block size of forty, generated by the computer random-number generator (RALLOC, STATA module) using the Microsoft Excel software. The allocation concealment was done by the marked series of the closed envelops including the allocation code. As it was not possible to execute the classic (double) blinded-experiment for the patients or the service providers in terms of the type of the intervention, we used the blinded-experiment to decrease the possibility of biases, so to this end, the service providers and the assessors were selected in a way to be different people. The assessor received no primary information about the intervention and the related contents. The eligible patients, who agreed to participate in this study, were classified into two groups as follows: the intervention and control groups. Determining that, if a patient will receive information prescription along with the routine oral explanation (intervention group) or only the routine oral explanation (control group), was done by the reference to the statistic series created by the HSB random sampling. The details of serials were kept unknown for all the contributors as the researcher, patients, and the analyzer. The follow-up time was 3, 6, and 12 months after the admission
Intervention protocol
In this study, the intervention was an Information Prescription (IP) directed by the related cardiologist (MD), along with the patients requested information, which was personalized and prepared by the clinical librarians. The process similar to the method used by Gavgani 23 was used in this study with some necessary changes based on the outcomes of the present study. Moreover, this process was done in three phases as follows: (i) prescribing information by MD/information prescription direction, (ii) dispensing IP by clinical Librarian, and (iii) approval by MD and delivering it to patient.
In our study, the information prescription is a piece of paper in which the MD wrote the name of the patient, the bed number, and order for information and then stamped it with his seal of National Medical Council, which is called IP direction. When the IP was directed by the cardiologist for the evidence-based and accurate information on the HF, Risk factors, medicines, and the related background information about exercise, daily activities, and diet for the patients that were sent to the librarian as a clinical team member. Clinical librarian received the IP and searched for the prescribed information from the evidence based patient information sources such as UpToDate (the library subscription provided by the government access), Medline Plus (https://medlineplus.gov/), MD Consult (www.mdconsults.org), and Cochrane evidence (http://www.cochrane.org/evidence). The IP was prepared in line with the medical concerns of the patient, as well as any additional factors such as the co-morbid conditions, medications, treatment options. After collecting the information, the librarian translated the information into Persian, and afterward, simplified the information to meet the reading ease standards for patients (grade 6–7) in terms of the Flesch-Dayani reading ease guideline for Farsi language (Dayani, 2000 #53). 27 When the information was prepared and ready to be used, it was evaluated in terms of the IP standards 28 and DISCERN criteria (www.dicsern.org.uk). Accordingly, this phase was done by the trained clinical librarians as IP. Finally, the information was submitted to MD for the approval and following the MD’s approval, a printed copy of the physician approved information linked to the main information and references were presented to the patients in the intervention group. In addition to the standard IP, the patients were allowed to ask for additional information on their self-care management. For example, an IP was ordered the effectiveness and safety of nitrates (one drug group used for the treatment of acute heart failure syndrome AHFS) by MD. The librarians searched for evidence about the effectiveness and safety of nitrates compared with alternative interventions in the treatment of the patients with AHFS through Cochrane.org. The evidence were collected from four studies conducted on 634 patients. “The study population in the trials was predominantly male (469/634 or 74% of all the patients included in the studies were men).” The evidence revealed that “Nitrates appeared to be well tolerated in all four studies. Also, Headaches was reported by the patients as the most common side effect which occurred more frequently when compared with Nesiritide.” Moreover, there was no significant difference in the occurrence of symptomatic hypotension, pain, nausea, and angina between the patients administered Nitroglycerin and Nesiritide. 29 This evidence was combined with background information about HF/AHFS from Medline Plus and then inserted in a MS Word file. Afterward, the collected information were translated into Persian and simplified to be simple and easy to understand at level 6–7 in terms of the Flesch-Dayani reading ease guideline. Also, the next steps were performed based on the above-mentioned protocol.
Intervention group: The researchers used the interview as a method to identify the eligibility of the participants for the study. The eligible patient was the one who had no information about his/her disease or any other source to receive the information. If anyone had prior information on HF and the related topics, she/he was excluded from the study. Those who were assigned to the intervention group have received the written information prescriptions (IPs), as well as their own requested and preferred information and the verbal description of the importance of IPs in understanding the physician’s diagnosis, treatment, and recommendations.
Data collection tool and follow-up
primary and secondary outcomes of the study were considered to be reduction in the hospital readmission and or death rate .The clinical and demographic data were collected from the medical chart of the patients, and if needed, were completed by asking question from the patient. The data on the number of re-admissions and death have been collected from the medical charts of the patients by a data extraction form and a follow-up questionnaire, respectively. The follow-up questionnaire consisted of eight items regarding the time of hospital admission and discharge, time of re-hospitalization, cause of re-hospitalization, reading the IPs, and death and time of the death. A panel of 10 specialists evaluated the reliability of questions. Also, the level of “interpreter reliability” reliability of questionnaire was identified as strong >0.88 using the value of Cohen’s Kappa, ranging from 80 to 90, which means that 64%–81% of data were reliable 0.23 The follow-up intervals were 6 and 12 months after the first intervention. Accordingly, the follow-up was carried out by telephonic interview with the patient and/or the care giver and review of the medical charts. Scores of 0 and 100 were used for each criterion. The score of 100 was considered for each criterion observed in a patient chart, and the score of 0 was considered for each criterion that was not observed.
Statistical analysis
The hospital readmission and death were considered as the primary outcome for the analysis. The obtained data were analyzed using the SPSS16 and STATA14 statistical software packages. The bivariate analysis tests such as T-test and Chi-square, were used for the analyses of qualitative variables differences like gender in two groups. For testing the normality of continuous variables, the Kolmogorov–Smirnov test was used. The Kaplan–Meier survival curve was used to compare the patients’ survival rates in the intervention and control groups. The Relative Risk (RR) was calculated and reported along with 95% confidence intervals. The Cox proportional-hazards model was used to control the potential confounding effects and to determine the adjusted hazard ratio of readmission and death. Moreover, the proportional hazard assumption was checked to assess the appropriateness of the model using the –ln –ln survival curve method. The p value below 0.05 was considered as the statistical significant border line in all the statistical procedures. The LL-LN residual curve method was also used to know which type of cox model should be used.
Results
Patients
A total of 233 patients have been screened in a 3-month period from December to February 2013. About 120 patients met the eligibility criteria and then agreed to participate in this study (Figure 1)
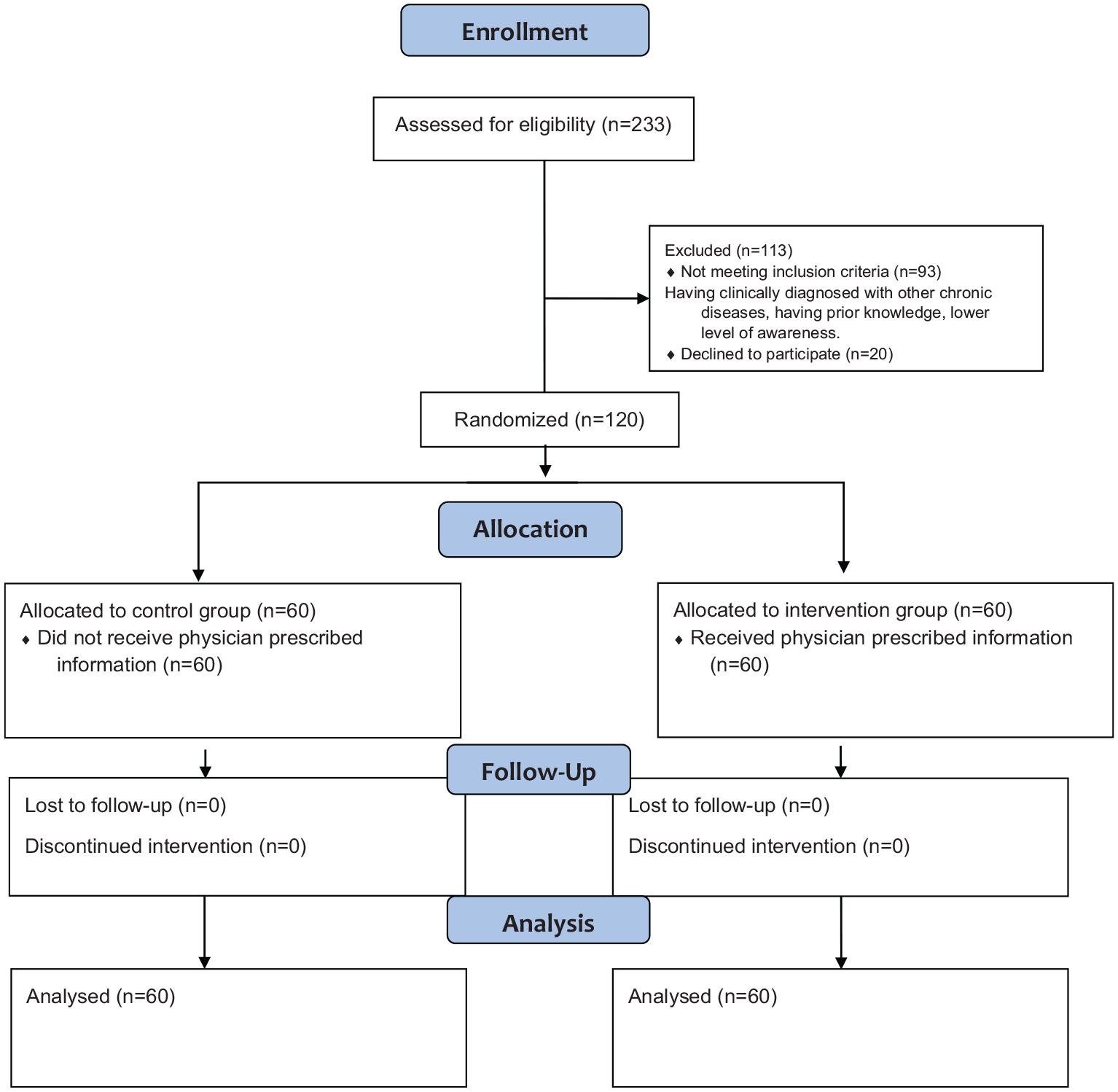
Flow chart diagram.
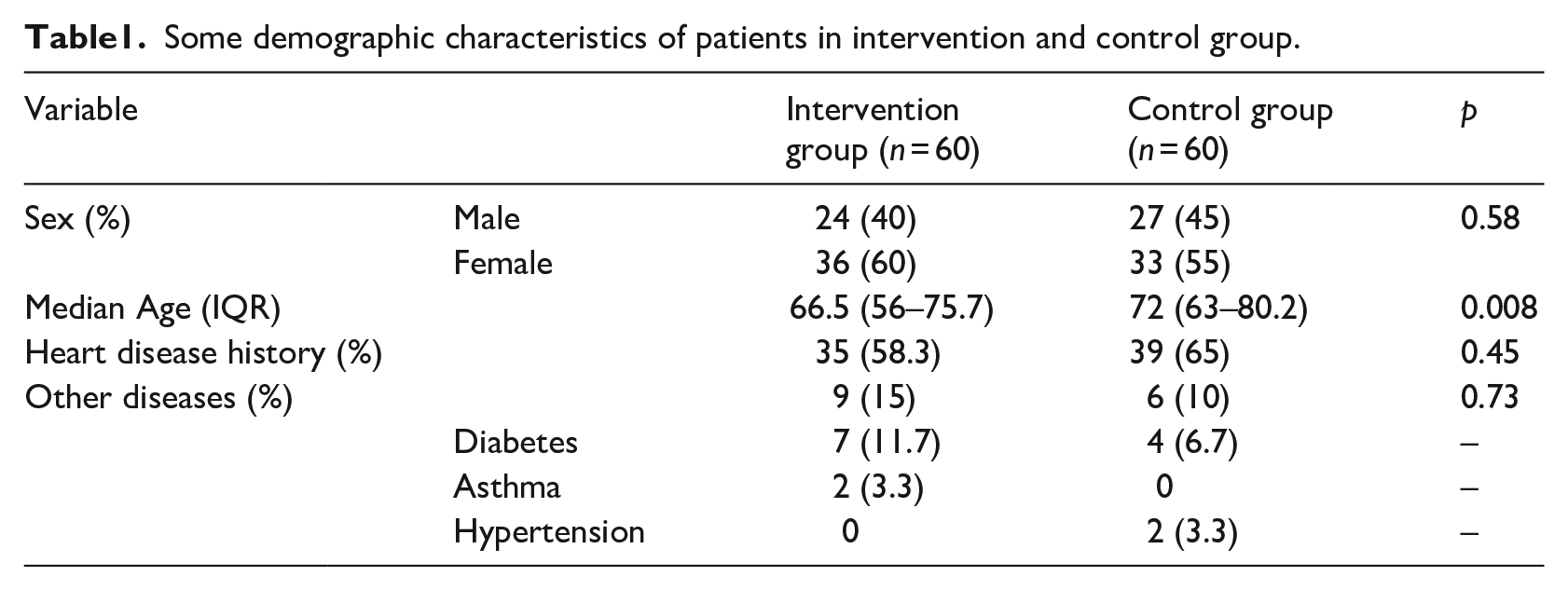
The history of heart disease in the two groups of intervention and control was similar and no significant difference was observed (Table 1).
Some demographic characteristics of patients in intervention and control group.
Outcomes
Readmission and death
The primary outcome of the study was a reduction in the rate of hospital readmission and death among the HF patients. Table 2 shows the number of readmission and death, readmission, and death during 6 months, 12 months, and also 1 year after the intervention for both readmission and death along with each other.
Number of readmission and death in 6 months, 12 months, and after 1 year.

We observed the death and readmission together once 1 year after the discharge in intervention and control groups, the differences of death and readmission was statistically significant, that is, 24 patients were included in the intervention group and 36 patients in the control group [RR = 0.67, 95%CI: 0.46–0.97]. The Kaplan–Meier survival curve for the death and readmission after 1 year follow-up (Figure 2) showed that, the survival was better in intervention group compared to that of the control group (p = 0.005).
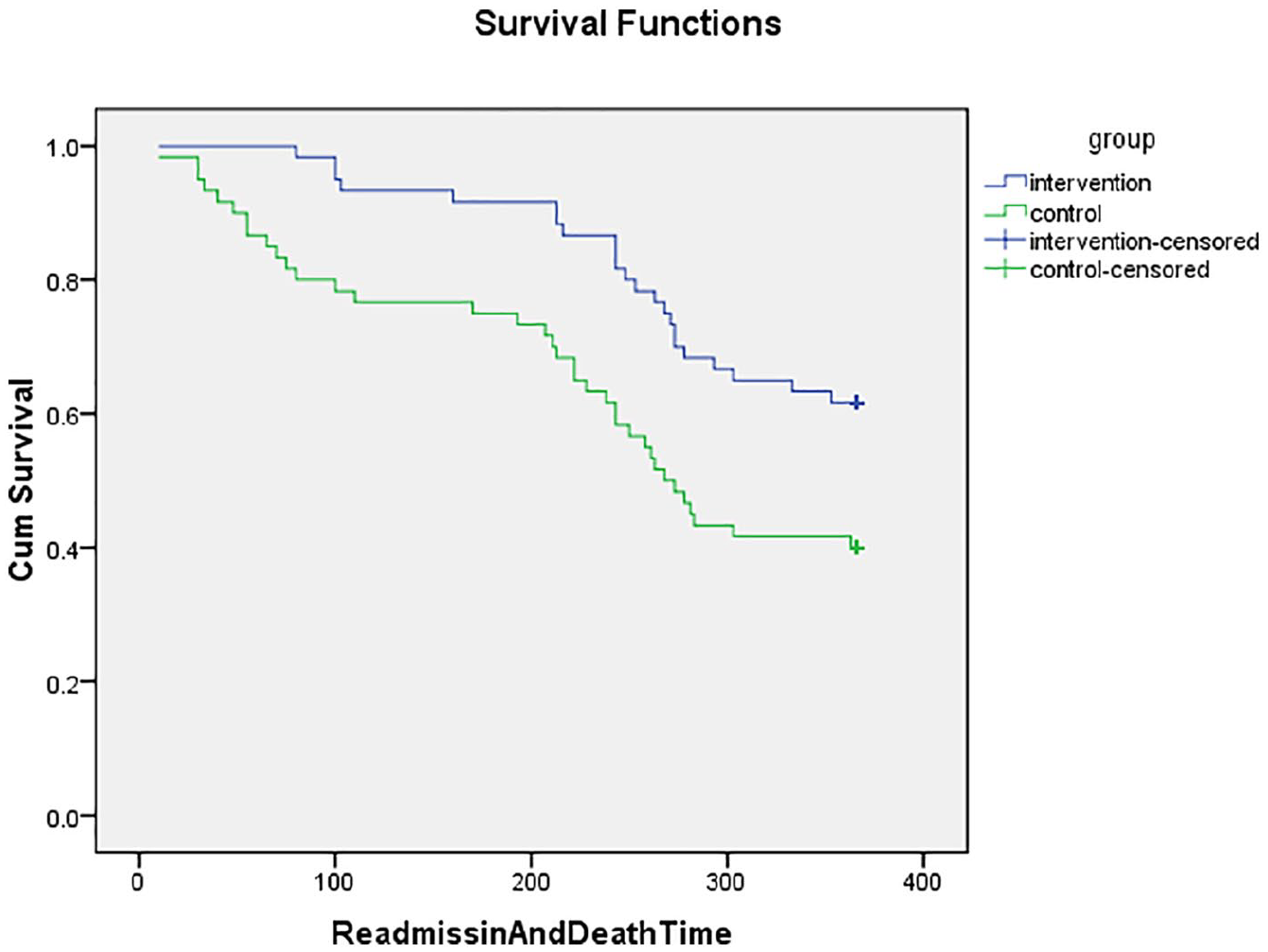
Kaplan–Meier survival curves for readmission after the 12 months follow-up.
The readmission rate has reduced in the intervention group in the first 6 months (Table 2), while the bivariate analyses showed no statistically significant differences [RR = 0.8, 95%CI: 0.51–1.26]. This means that the relationship was not significant statistically during 6 months.
Figure 3 shows the curves of survival for the readmission during 12 months (the second half of the year after the first intervention) of the follow-up by the group allocation. The patients in the intervention group were less readmitted compared to those in the control group; the differences between these two groups were statistically significant according to the results of the Log Rank test (p = 0.037). In addition, 20 patients in the intervention group and 33 patients in the control group were readmitted within 12 months after the intervention [RR = 0.61, 95%CI: 0.4–0.93].
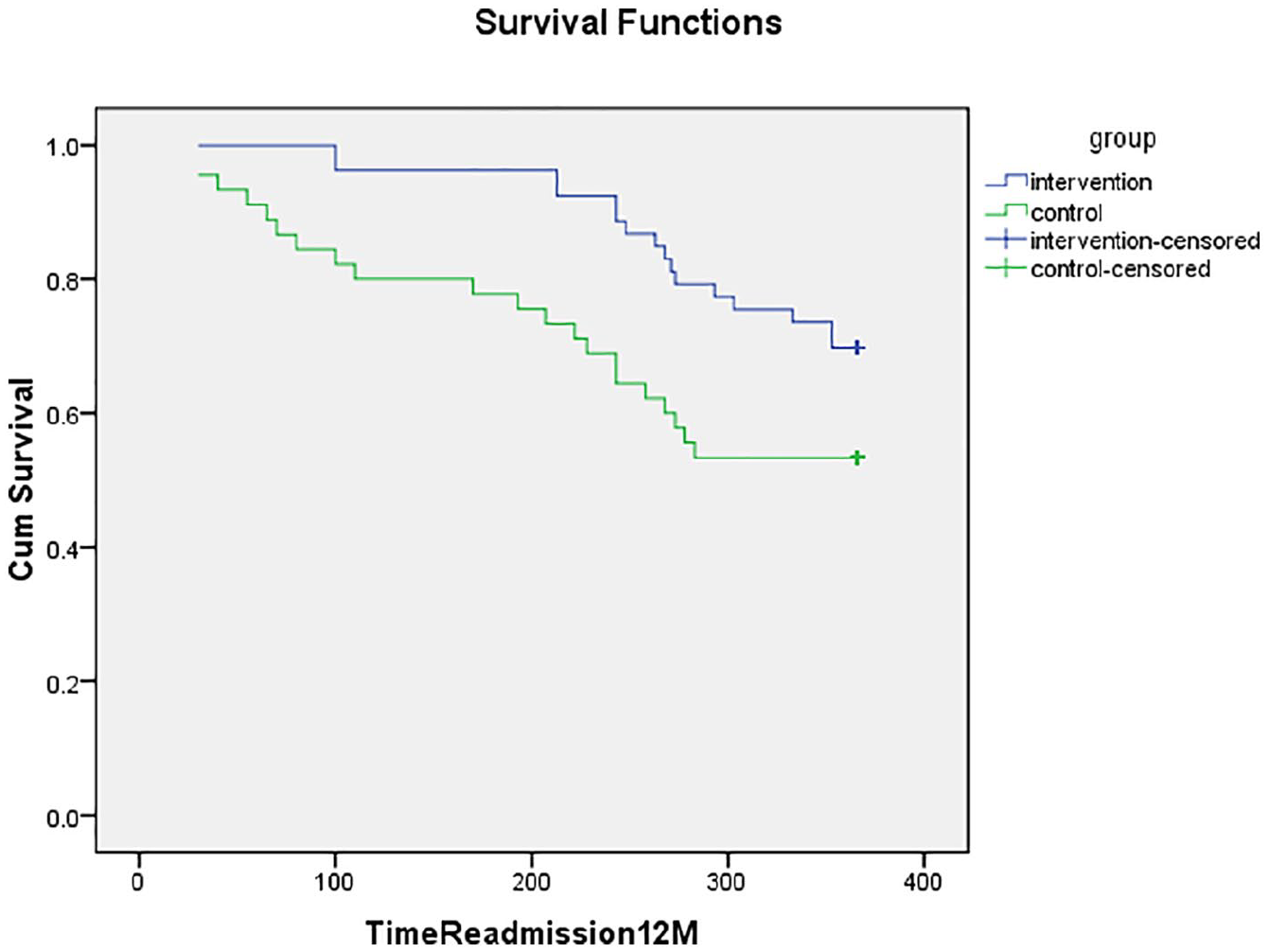
Kaplan–Meier survival curves for readmission after the 12 months follow-up.
Death
During the 12 months (second half of the year) follow-up, 7 patients in the intervention group and 15 patients in the control group died [RR = 0.47, 95%CI: 0.20–1.06]. The Kaplan–Meier survival curve for death alone in 1 year period (Figure 4) shows that the survival rate in intervention group was more than that of the control group; however, according to Log Rank test, this difference was in borderline (p = 0.05) and this differences is clinically valuable, but it is not absolutely significant.
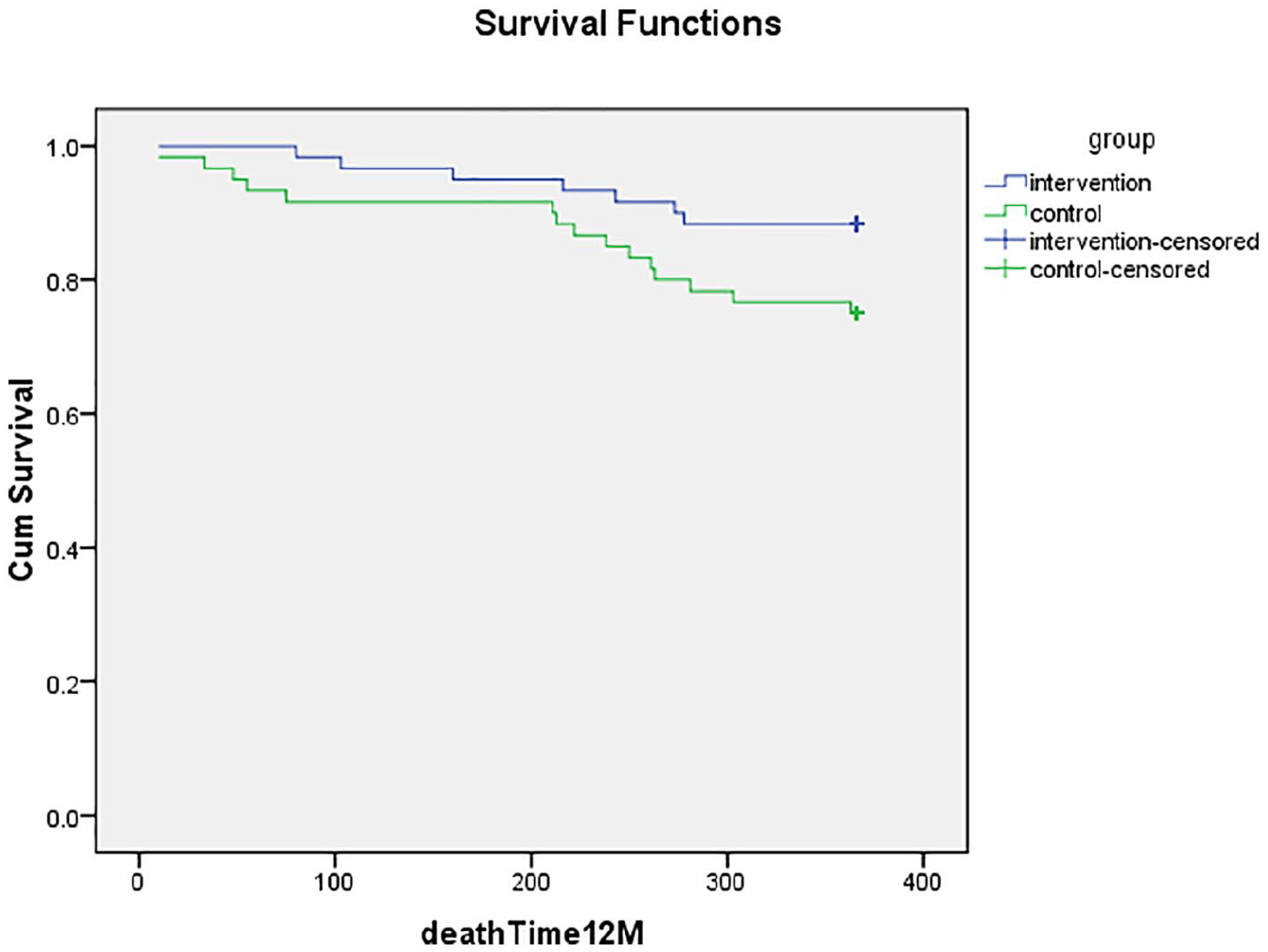
Kaplan–Meier survival curves for death after the 12 months follow-up.
During 6 months (the first follow-up), the number of death in intervention group was less than that of the control group. During the 6 months follow-up, three patients in the intervention group and five in the control group died [RR: 0.6 CI 95% 0.15–2.40]. Accordingly, this was not statistically significant (p = 0.46); however, the death clinically was significant during 6 months follow-up.
Also, according to the Cox Proportional Hazards Model using backward method (Table 3), the intervention (Information Prescription) after adjusting for the effects of sex, age, and heart disease history, had no effect on the outcome during 6 months follow-up [Hazard Ratio = 1.69, 95%CI: 0.993–2.876; p = 0.05].
Hazard ratios and their confidence intervals according to Cox Proportional Hazards Model.
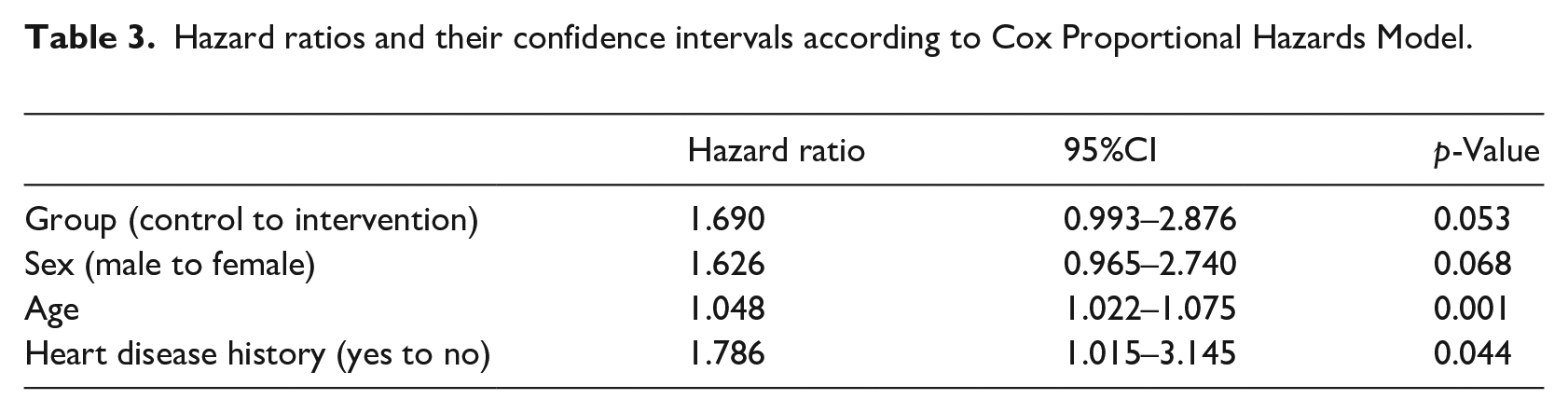
The Hazard in control group was about 69% more than the Hazard in intervention group considering the borderline significance. For using the Cox Proportional Hazards Model, firstly, the Proportional Hazards assumption was checked. The result, which is demonstrated in Figure 5 shows that, Proportional Hazards assumption satisfies for our data; hence, we finally used Cox Proportional Hazards Model.
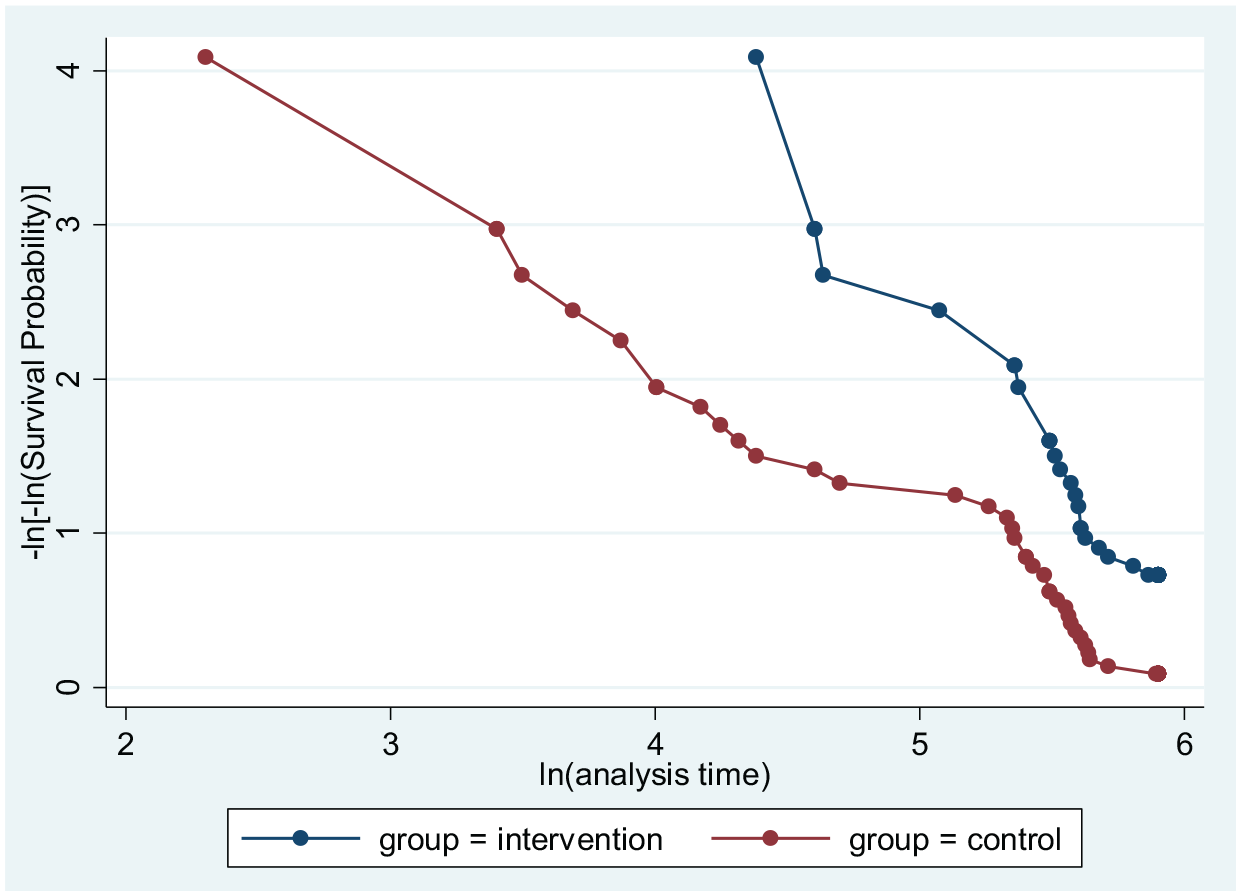
ln –ln survival curve for testing Proportional Hazards assumption.
Discussion
This study was the first randomized controlled trial to test the effect of the physician prescribed evidence-based information with clinical librarian’s value added service on the organization and personalization of information to the HF patients. The main aim of this RCT study was to find out if the physician prescribed and clinical librarian provided IPs is effective on reducing the rate of hospital readmission and mortality in short- and long-term follow-ups.
Death and hospital readmission
In this study, the number of death or hospital readmission was less in the patients who received the IPs intervention compared to the control group. Also, we found that, few patients died in the intervention group after 12 months compared to the control group. This is supported by the findings of the previous studies in term of long term follow-up studies (12 months or more) by the educational interventions, but not necessarily IP intervention. For example; Atienza et al. 30 reported a reduction in the death and readmission rates in the 509 days follow-up (about one and half year) by the educational program delivered to the patients and their family member (95%CI: 29–65; p < 0.001). Krumholz et al. 31 found that, a formal education and support intervention program reduces the adverse clinical outcomes and costs for the patients with HF during a 1 year follow-up (relative risk = 0.69, 95% confidence interval [CI]: 0.52–0.92; p = 0.01). Even in specific group of the HF patients with a low literacy level, a self-management programs proved to be effective on the reduction of hospitalization and death rates during 12 months follow-ups [IRR = 0.69; CI 0.4–1.2; adjusted IRR = 0.53; CI: 0.32–0.89]. 32 A nurse led education program compared to usual care in HF patients’ mortality and morbidity showed that, the event (death or readmission) were fewer after a period of 12 months or more. 33 Unlike the above-mentioned studies, Greene et al. 34 used a Web-based patient-doctor aligned-incentive and information therapy program in emergency room and also revealed a decrease in emergency department visits and hospitalizations as 32 and 14% totally, during 5 years of study.
However, in the short term follow-up of 6 months, the statistical analysis of results for our study showed no statistically significant differences. In this regard, the result of our study was similar to Hope et al.’s 35 study, who primarily compared the result of knowledge test with the number of visits to emergency department among all cause cardiovascular-related and Chronic Heart Failure specific (CHF) visits to emergency department (ED), and consequently, found no change during a 6-month period. In terms of the short term effect of knowledge on ED visits, they also found that, knowledge of the prescribed medication was associated with CHF-specific ED visits (p < 0.001). A quasi-experimental pre-test and post-test study examining a nurse-led education program to improve knowledge, self-care, and reduce readmission for individuals with heart failure also found that short term effect of information intervention is not statistically significant in 30-day readmission (p ⩾ 0.05). 36
But, a recent retrospective quasi-experimental study using a pre-post design to evaluate the impact of a pharmacy-led transition of care (TOC) program in reducing HF 30-day hospital readmissions showed that patient education for mediations based on the written materials from the Heart Failure Society of America (https://www.hfsa.org/patient/patient-tools/educational-modules) and an internally developed education handout is effective in decreasing the number of readmission in 30 days. They found that in the control group, 57 (17.3%) patients had a HF 30-day readmission compared with 35 (10.5%) patients in the intervention group. After adjusting for age, the intervention group continued to show a difference in readmission (odds ratio = 0.578; 95% CI = 0.367–0.911; p = 0.018). 37
This shows that novel intervention is essential in patient education to improve patient care outcome. The more attention should be given for patient education in different pathways of healthcare by various agents (i.e. clinical librarians, nurses, pharmacists, and medical doctors). Use of traditional methods like face-to-face education and consulting with non-evidence-base web content without value added appraisal intervention is not effective and suitable for patient care. Because research studies suggest that web-based patient information used for patient consultation is not reliable, accurate and evidence based. 10 A review of reliability of the patient information provided through YouTube also indicated that the YouTube contents are misleading (in 65% of studied articles), are not from trusted sources (63.7% of studied articles),and only 35% of the research articles recommended that medical videos available through YouTube are useful and can be a good source of patient education. 26
However, our novel intervention contributed in understanding of the impact of information prescription (IP) in association with the clinical librarians’ information services in healthcare outcomes. We delivered evidence-based, physician prescribed and easy to understand information for the patients, which was also personalized in terms of each patient’s literacy level and health condition. Clinical librarians’ expertise was contributed in finding, appraising, and personalization of content in terms of readability of information prior to delivering to patients, unlike the previous research studies.
The result of our study in association with the analysis of the previous studies suggests that, unlike a medicinal intervention that is a tangible commodity, the information is an intangible entity; hence the effect of information cannot be measured immediately and directly by a laboratory test. Moreover, information affects the person’s perception and knowledge, so mentally encourages the person to participate in his or her health care management. Thus, recuperation is the result of the patient’s concentration and engagement in controlling and managing the disease, adherence to medication, and in providing a timely feedback.
Therefore, although no evidence supports the statistical significance of IP on death and or readmission in short time period, despite observation on the differences in number of death and readmission in both of the control and intervention groups, but based on the importance of any changes in patient care outcomes, even a small change, we believe that IP intervention was statistically significant in long term and clinically effective in short term.
Most of the patients in our study fell under the III or IV functional classes based the New York Heart Association (NYHA) Functional Classification that are the sever stage of illness. Therefore, any small change in the outcomes of the patients such as readmission and even death would be considered as a clinically positive effect of the IPs.
Recent studies indicate that poor knowledge of heart failure patients leads to adverse medical outcomes. 11 Today, following the technological advances in HF patients’ care like Artificial Intelligence (AI) for diagnosis, 38 self-care, 39 wearable tools that are used for prediction of heart failure risk, 40 and educational tools such as avatar-based apps, 41 interaction apps, 42 interruptive modal dialogs (i.e. pop-ups) in prescription stage 22 and various methods that can be used through integration of information sources, advanced educational technology and advances in medical equipment for delivering right information to patients at the moment on care. Therefore, clinical librarians can play a vital role in supporting the patients’/caregivers health literacy program by providing them with necessary value added patient information and curated patient information databases and repositories. Clinical librarians have been always engaged with information and knowledge management in health and medical system both in the traditional print information model and the modern online information. They are uniquely trained with skills in providing the evidence-based information, finding, assessing, value adding, and managing the collections of medical information to the physicians and also to the patients. Answers to clinical questions can be obtained more quickly and efficiently when clinical librarians are involved in providing information in the patient care setting. 43 In order to recognize the full range of clinical librarians’ skills and contribution in patient care and patient health literacy, they should play a part in clinical teams for evidence based information delivery service.
One of the limitations of our study was the dominant number of patients with severe stage of HF that contributed with long term effect of IP intervention. The other limitation was that fewer medical specialist show willingness to prescribe information despite their positive attitude towards effect of patient information on the health care outcomes. Lack of evidence-based patient information data base in local language also played a crucial role in the medical doctors reluctant for prescribing information. It also was time consuming for the research team to translate the information from international sources into local language
Conclusions
This study showed that, information prescription if prescribed by the related specialist and personalized by the clinical librarians based on the latest evidence, and patients’ individual variabilities can be effective on the heart failure clinical outcomes in terms of re-hospitalization and mortality rate. This study suggests that, the long-term information prescription intervention is more effective than a short time follow-up in the HF patient. Moreover, it is important to deliver information prescription in onset of disease rather than the level of intensity of HF. However, to achieve the level of certainty in short time follow-ups based on the statistical significance, more evidences are still needed. It can be concluded that, an evidence-based, physician prescribed, and tailored information intervention prevents the risk of re-hospitalization in the patients with HF, and could also provide the key strategies for a successful management of the diseases. At a time with advances in information and educational technologies and medical equipment there is prospects for active participation of clinical information specialists in curation of patient information repositories and databases specially in local languages to support information prescription and patient-centeredness in health care.
Study limitations and suggestions for the possible future studies
One of the limitations of this study was the small number of the recruited patients (the limited number of the eligible patients in the study timespan). The other recognized limitation was that, all the patients recruited in this study were classified in the functional classes of III and IV, using the New York Heart Association (NYHA) Functional Classification. The functional classes of III and IV are clinically at severe stages and it may be too late for getting informed, changing behavior, and sharing decision with physician to improve the health care outcomes. So, it is suggested that, if new studies repeat this trial on heart disease would consider recruiting the patients with all the four functional classes, especially the classes II and III to possibly highlight the impact of the information prescription with more power and confidence. It is also suggested to include different agents like pharmacist, clinical information specialists (informationists), nurses, and medical doctors in information prescription and dissemination trials.
Footnotes
Acknowledgements
We are thankful to the Nurse Section of Shahid Madani Heart Hospital for their selfless collaboration in collecting the necessary data, as well as all the patients who participated in this study. We have used external linguistic editing and statistics analysis service, for which we would expand our appreciation to Homayoun Sadeghi-bazargani for his assistance with statistical analysis of our study.
Authors contribution
The idea was developed by VZG and FKM and put forward with AG for conduction. After agreement VZG, FKM, and AG designed the study, the protocol was written and reviewed by al co-authors. Data was collected by FKM and AG, VZG and AJKH observed data every day is necessary. Data analysis was done by FKM and AJKH. The manuscript was prepared by FKM and VZG. All authors AG, AJKH, FKM, and VZG contributed in reading the manuscript, reviewing the comments in peer review process, and they all approved the final version before submission.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: For conducting research, funded by the Research and Technology Vice-Chancellor of Tabriz University of Medical Sciences. The APC has been paid by authors.
Ethical issues
The ethical research committee of Tabriz University of medical sciences approved the study. This study was registered by the code of ethics: 92157. The informed consent was obtained from the patients individually before intervention and prior to the hospital discharge for the necessary follow-ups.