
Abstract
The objective of this study was to test the feasibility of video discharge education to improve self-efficacy in dealing with medication barriers around hospital discharge. We conducted a single-arm intervention feasibility trial to evaluate the use of video education in participants who were being discharged home from the hospital. The scores of pre- and post-intervention self-efficacy involving medication barriers were measured. We also assessed knowledge retention, patient and nursing feedback, follow-up barrier assessments, and hospital revisits. A total of 40 patients participated in this study. Self-efficacy scores ranged from 5 to 25. Median pre- and post-intervention scores were 21.5 and 23.5, respectively. We observed a median increase of 2.0 points from before to after the intervention (p = 0.046). In total, 95 percent of participants reported knowledge retention and 90 percent found the intervention to be helpful. Video discharge education improved patient self-efficacy surrounding discharge medication challenges among general medicine inpatients. Patients and nurses reported satisfaction with the video discharge education.
Keywords
Introduction
Discrepancies between hospital discharge medication lists and patient-reported regimens are common and can affect up to half of patients after they leave the hospital.1–4 These discrepancies can lead to patient harm, including preventable adverse drug events and hospitalization.5–7 In addition, as American hospitals faced up to $500 million in penalties in 2017 for higher than expected rates of patient readmission within 30 days, the nationwide attention toward preventing readmissions has put medication-related contributors squarely in focus. 8 Systematic reviews of resource-intensive medication reconciliation programs around the time of discharge to reduce readmissions have yielded mixed results with heterogeneity of interventions, patient populations, and settings limiting their generalizability.9–13 Recent studies have focused on what patients perceive as causes for their return to the hospital. The inability to anticipate and surmount challenges that may arise with obtaining and adhering to discharge medications has been cited recently.14–17 As a result, communicating what these barriers are during discharge education may be an important strategy to reduce readmissions.
Time constraints and lack of standardization among discharge educators often hamper effective communication about discharge medications and potential barriers that patients may encounter. 18 Even when patients perceive that their discharge plan was adequate, many have poor comprehension of written instructions, especially among those with lower health literacy and the elderly.3,19,20 Multimedia solutions such as use of video may provide effective complementary education to spoken and written instructions.21–23 Video discharge instructions have successfully improved comprehension and knowledge in the Emergency room (ER) setting and have improved self-care behavior among heart failure inpatients, but videos have not been studied in the general medical inpatient population.24–26 Interventions that standardize discharge education while engaging the patient and improving their self-efficacy in successfully overcoming medication-related barriers may help reduce harm and preventable hospitalization.
The overall objective of this pilot study was to evaluate the feasibility of using video discharge education (VDE) related to discharge medication barriers to improve self-efficacy for medical inpatients who were being discharged home. We also examined patient knowledge retention, patient and nursing feedback, follow-up data on medication barriers, and hospital utilization.
Methods
Study population
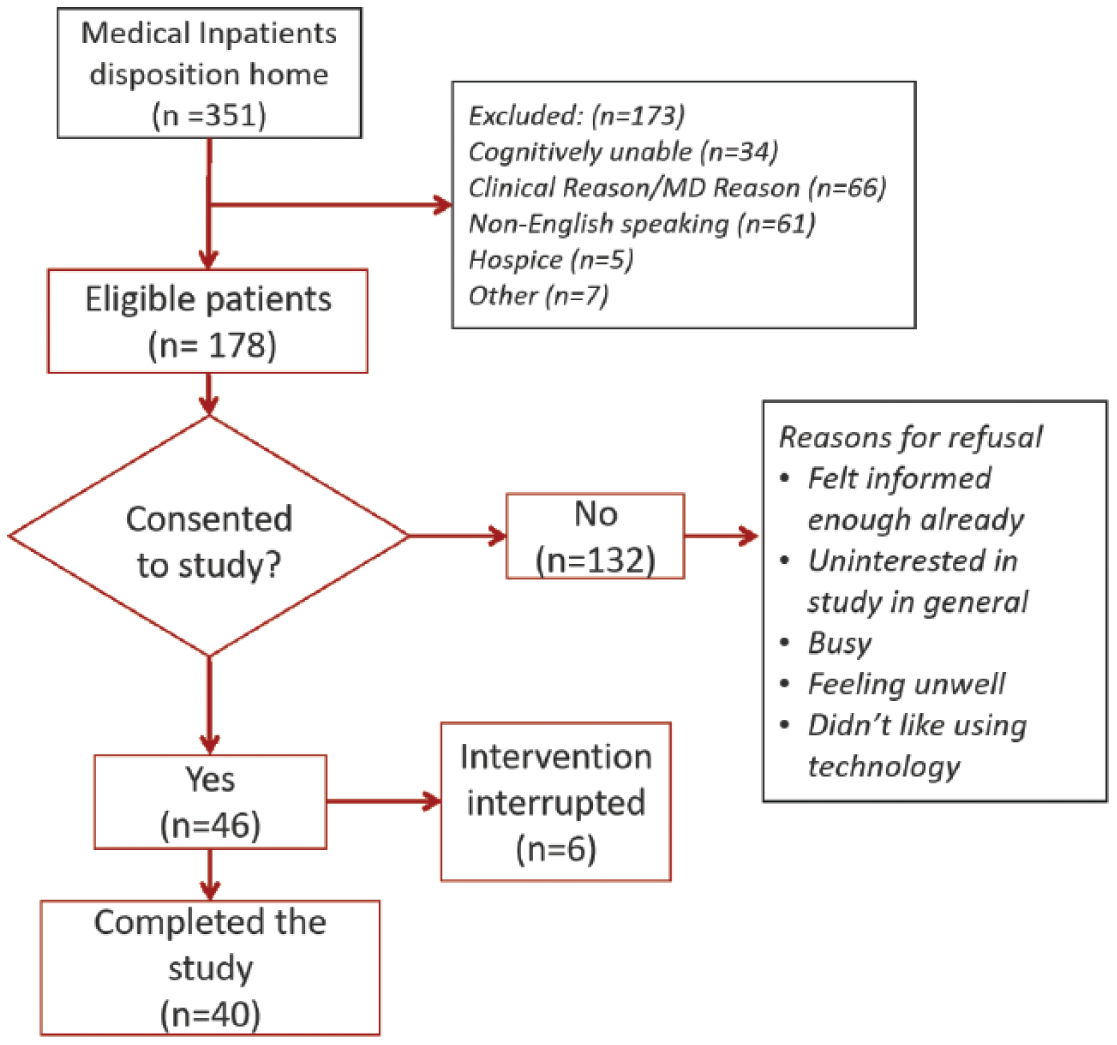
A single-arm feasibility pilot study was conducted from January to April 2017 with participants recruited from the general medicine service at NewYork-Presbyterian Hospital/Weill Cornell Medicine. Eligibility criteria included the following: inpatients on one of two general medicine wards with plans to be discharged home, age > 18 years, English-speaking, and cognitively able to complete the intervention. Patients who were unable to provide informed consent, unwilling to complete follow-up phone calls, unable to provide a phone number, on medical isolation, or deemed unsuitable by the medical team were excluded (Figure 1). Three senior medical students served as research assistants (RAs) who delivered the intervention following a study protocol. Written informed consent was obtained from all participants and the Institutional Review Board of Weill Cornell Medicine approved this study.
Patient selection.
Intervention development
We thoroughly reviewed the literature in order to identify potential barriers for successful transition to home as targets for our intervention. We also consulted both physicians and patients about the most difficult barriers to overcome involving medication discrepancies in the post-discharge period. We identified five primary barriers to be addressed in this feasibility study. These barriers were medication reconciliation, medication uncertainty, medication administration, medication availability, and access to delivery of medication. For each of the five barriers, a summary of the evidence of the barrier and possible solutions was documented and reviewed by physicians on the Patient Activated Learning System (PALS) Team in the Division of General Internal Medicine, a group dedicated to creating innovative patient educational content. Expert opinions regarding processes and solutions from inpatient staff were also considered. From these summaries, scripts were created using patient-centered lay language (see Supplement A). Scripts were reviewed by physicians, nurses, social workers, pharmacists, and care coordinators. Each script title was phrased in the form of a question, aligning with the self-efficacy questions described below.
Patient feedback on the helpfulness and likability of the scripts was collected by engaging 30 patients who met the same inclusion criteria as the study participants. Depending on patient preference, scripts for each topic were read aloud by an RA or read independently by patients. All survey items and knowledge assessment questions were evaluated during this phase to confirm that patients could answer questions without confusion. Data from this phase of the study informed the development of five videos ranging in length from 1 to 2 minutes (see videos here: https://www.palsforhealth.com/Pals/Search?query=hospital). Feedback on video content, use of images and animation, and messaging was collected from the PALS team, inpatient physicians, pharmacists, nurses, and patients. Videos were produced by a senior medical student member of the PALS team. The videos were found in a single link on a tablet that patients were able to click and watch on their own. After each educational topic, one multiple choice knowledge assessment question with three choices was asked pertaining to the material participants just viewed.
Intervention implementation
Allscripts Care Manager is a cloud-based, electronic health record–agnostic population health management application that serves as a daily rounding tool for interdisciplinary inpatient teams. Using this tool, clinical and non-clinical key information about all inpatients on the ward allows for care managers and social workers to share tasks and resolve concerns about discharge planning with the medical team during daily morning rounds. A swimlane analysis was completed to analyze workflow changes between the current and future states in identifying patients for video education and subsequent patient involvement with care coordinators or social workers based on patient barriers (see Supplement B). Using Allscripts Care Manager, the RA screened patients and identified those with planned discharge to home. Once the RA identified potential patients, they confirmed eligibility with the care team, reviewed the electronic medical record (EMR), and approached patients. After obtaining informed consent, participants were surveyed about demographics, health literacy, and self-efficacy. Participants then viewed the videos and completed knowledge assessment questions on an iPad. The time to complete viewing of the videos and the assessment questions was recorded. Once all videos and assessment questions were completed, participants completed a post-intervention reassessment of self-efficacy and provided feedback on the video content and format.
The RA contacted participants 7 and 30 days after discharge by telephone and administered brief surveys to determine if they faced any of the five medication barriers discussed in the videos. Patients were also asked about any visits to the ER or hospital readmissions since discharge and reasons for these possible visits.
Primary outcome
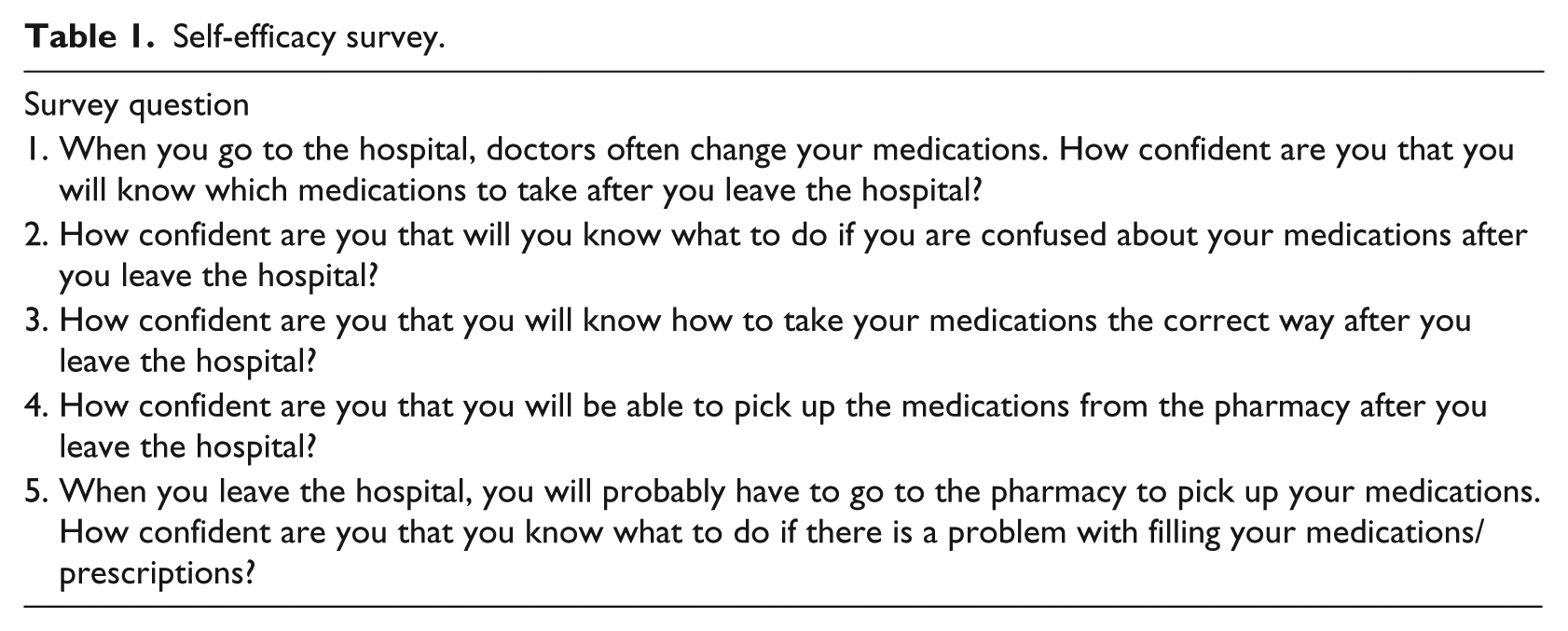
Self-efficacy related to medication challenges was assessed both pre- and post-intervention using a five-item Likert-type scale instrument (Table 1). Response options included not confident at all (1), somewhat confident, no opinion, confident, and very confident (5). The five ordered response options from each self-efficacy question were summed to calculate an overall confidence score ranging from 5 to 25 with higher scores representing greater levels of self-efficacy. As no validated self-efficacy measures for discharge medication barriers currently exist, the instrument used for this study was developed by experts at our institution.
Self-efficacy survey.
Statistical analysis
We calculated descriptive statistics (medians and interquartile range) of pre- and post-intervention self-efficacy scores. Due to the skewed nature of the distribution, non-parametric Mann–Whitney U tests were used to evaluate differences between pre- and post-intervention median self-efficacy scores.
Health literacy was assessed using a validated three-item scale.27,28 The three questions were about the frequency with which participants needed help: reading hospital materials, filling out medical forms, and learning about their medical condition. Each question had a five-point Likert-type scale. Responses to each question were dichotomized and given a score of 1 or 0, thus yielding a range of 0–3 across the three questions. An overall score of 0 was considered as adequate health literacy, a score of 1 as marginal health literacy, and a score of 2 or 3 as inadequate health literacy. Knowledge questions were analyzed as a sum of the number of correct items out of a total of five. Frequencies were dichotomized and reported as less than four correct, or greater than or equal to four correct. Time (in minutes) to complete the intervention was not normally distributed and was therefore reported as medians and interquartile ranges. The 7- and 30-day follow-up data were calculated as frequencies. Statistical analyses were conducted using STATA 14 and α = 0.05 (StataCorp. 2015. Stata Statistical Software: Release 14. College Station, TX: StataCorp LP.)
Nursing feedback
An RA conducted semi-structured interviews with nurses on wards where the intervention was implemented (see Supplement C). A series of 12 free response questions elicited their views on the ease of implementation, utility, and intervention style. The interview focused on how incorporating the intervention would impact workflow and on if nurses believed the intervention would have a positive effect on patient discharge planning.
Results
Of the 430 consecutive patients initially screened, 351 (82%) were planned to be discharged home. Of these, 178 (51%) were deemed eligible for the study, of whom 40 enrolled and completed the study. Reasons for exclusion and consent decisions are described in Figure 1. Participants had a median age of 55 years and 63 percent were women (Table 2). A total of 50 percent of the patients had either Medicare or Medicaid as their primary insurance and 78 percent reported adequate health literacy.
Patient demographics.
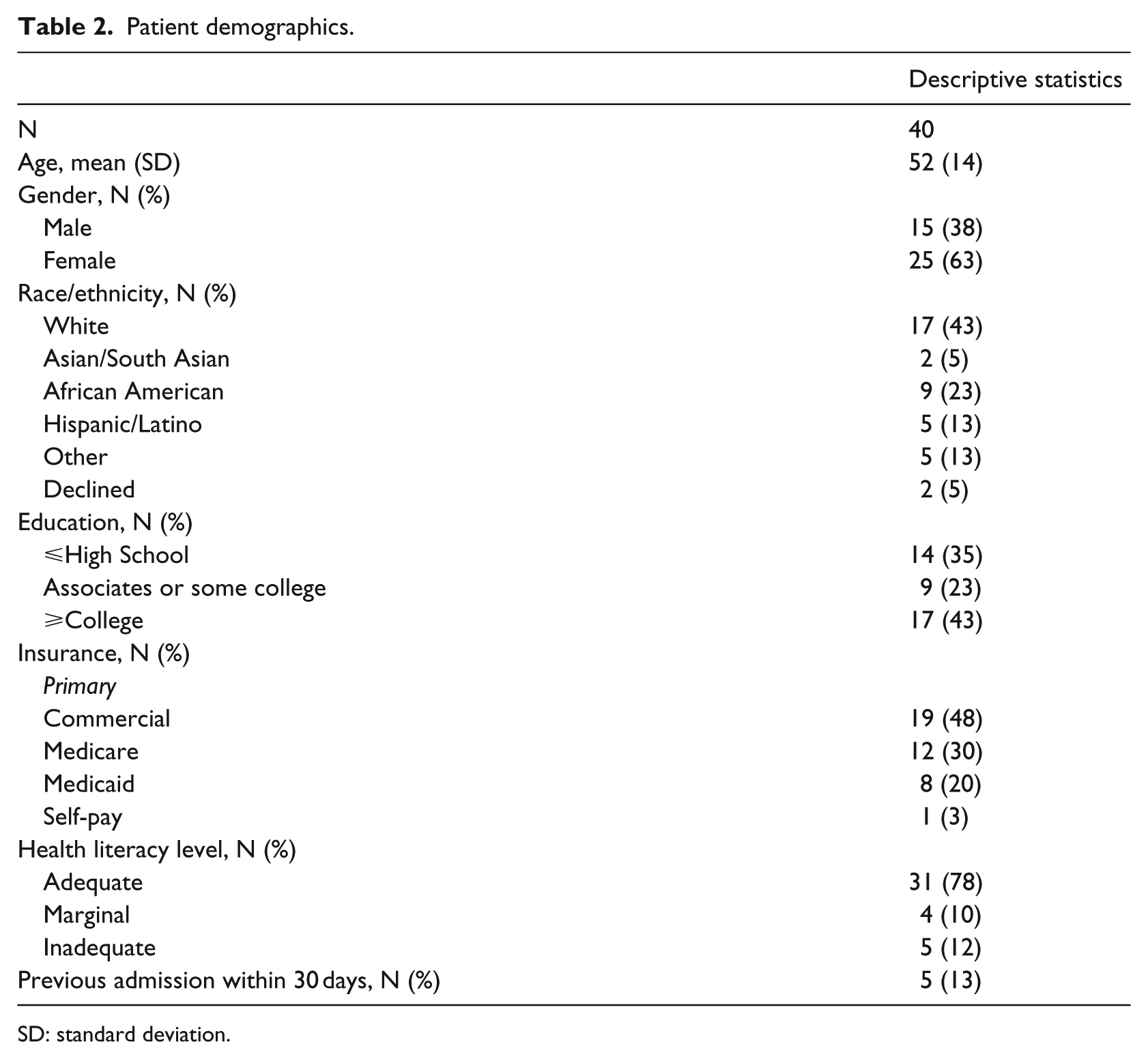
SD: standard deviation.
Primary outcome
Prior to the intervention, the median level of self-efficacy was 21.5 points (19.0–25.0 points). Following the intervention, median self-efficacy scores rose by 2.0 points to 23.5 points (21.0–25.0). The pre–post intervention medians were statistically significantly different with p = 0.046. Of the 40 patients in this study, 20 (50%) increased their self-efficacy, 18 did not change, and 2 reported a decrease in self-efficacy. The self-efficacy question with the greatest average improvement was the first question, which asked about knowing which medications to take after leaving the hospital.
Process measures
Out of the 40 participants, 38 (95%) correctly answered at least four of the five knowledge assessment questions (Table 3); 36 (90%) found the videos to be helpful; and 13 (33%) reported that the videos highlighted at least one medication challenge they had not previously considered. The median time to complete the videos, assessment questions, and comments or questions from patients was 14.4 min (11.3–23.6).
Feasibility and process measures.
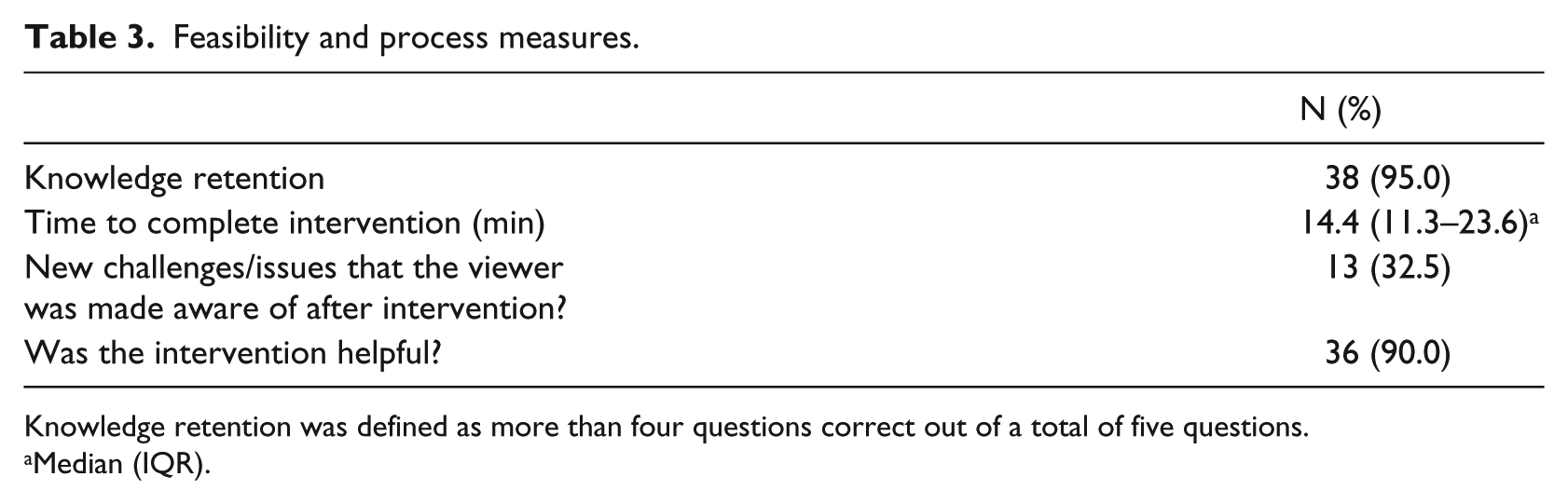
Knowledge retention was defined as more than four questions correct out of a total of five questions.
Median (IQR).
Follow-up
Of the 40 patients, 31 (78%) were successfully contacted for follow-up within 30 days of discharge (Table 4); 10 patients (32%) reported facing at least one of the medication barriers addressed in the intervention. Difficulty filling prescriptions was the most common obstacle, affecting 6 of these 10 patients. Of these 10 patients, 8 were able to resolve their issue, while the other 2 patients were actively working on solutions at time of follow-up. In the 30 days following discharge, there were six hospital readmissions most often due to an unrelated medical condition or inadequate symptom control. Furthermore, seven patients visited the ER without subsequent admission to the hospital. Causes for these seven ER visits included allergies, side effects from medications, unrelated medical illness, and pain management. None of the reported revisits (either to the hospital or ER) were related to medication barriers discussed in our video education intervention.
30-day follow-up data.
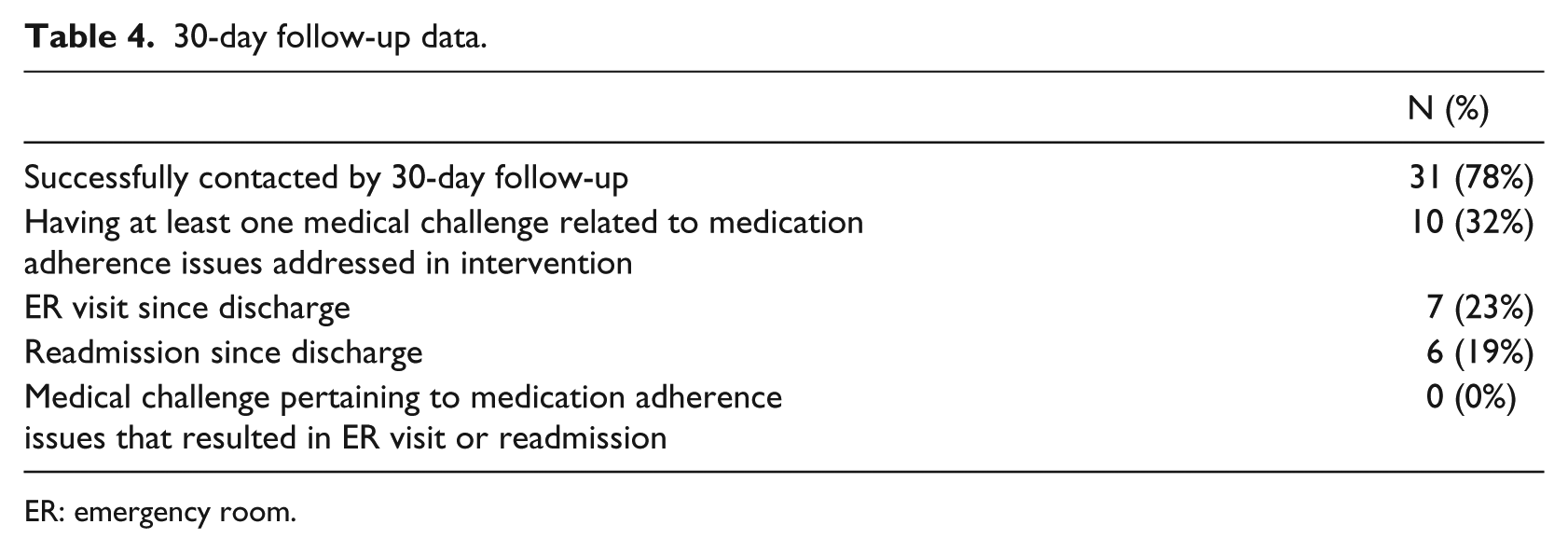
ER: emergency room.
Nursing feedback
Of 18 nurses approached in this study, 17 agreed to participate in our semi-structured interview. We found that 88% (n = 15) of the nurses interviewed believed that the intervention improved discharge planning, citing that the intervention gave patients more time to consider and ask questions prior to discharge. Furthermore, of the nurses surveyed 76 percent (n = 13) stated that the information in the videos was relevant and useful, either reinforcing topics that would normally be covered during the discharge process and therefore saving time, or addressing topics that would otherwise have been missed, adding value. In addition, 41 percent (n = 7) stated that the videos covered questions that were frequently asked by patients prior to discharge or that patients often called back about post-discharge. A majority of nurses (70%, n = 12) reported that the intervention would likely save time during discharge, particularly with specific patient populations. Nurses who reported that discharge time may increase (n = 4) discussed the need to train patients or deal with technological issues related to the use of a tablet.
Patient feedback
Free response questions in the post-intervention survey asked patients to identify what they found helpful or unhelpful about the videos. The most common responses were positive statements such as “the videos were all good” and positive views of the use of visual imagery for the content (23%, n = 9). In addition, 14 patients (35%) reported that the videos were easy to understand or helped them develop new strategies to overcome common obstacles. Furthermore, six (15%) patients found that the videos inspired them to focus on medication barriers prior to discharge. Common challenges to acquiring medications included insurance issues or physically accessing a pharmacy. Four (n = 10%) patients stated that this was a new concern for them that they wanted to solve prior to hospital discharge.
Discussion, conclusion, and clinical implications
Discussion
This single-arm feasibility study evaluated the ability of VDE to improve patient self-efficacy regarding discharge medications. We observed a statistically significant post-intervention increase in self-efficacy. After watching our VDE, the patients reported a two-point confidence increase with excellent knowledge retention. While the pre-intervention self-efficacy median was high, with a score of 21.5, signifying “confident,” the VDE did lead to clinically meaningful outcomes with half of the patients improving their self-efficacy and improving the lower interquartile value from 19 to 21. As medication non-adherence after discharge can lead to harm and readmission, any improvement in self-efficacy may be considered clinically relevant. Given the ease of VDE implementation, findings from this pilot study are promising and support this pragmatic, standardized method to deliver high-impact discharge education. Furthermore, 90 percent of patients found the intervention helpful, while 30 percent reported that the education highlighted a challenge they had not considered, creating opportunities to reduce unanticipated issues surrounding discharge. Follow-up data at 30 days demonstrated that while medication challenges at discharge were common, patients were able to deal with these barriers without having to return to the hospital. For those who revisited the ER or were readmitted, the reasons given were not related to any of the barriers discussed in the VDE.
Feedback from patients and staff supports the long-term feasibility and sustainability of this patient education intervention. Patients enjoyed the style of education and the range of information presented. The medical teams were supportive and enthusiastic about the videos. Nurses observed that the VDE reiterated important instructions and potentially exposed patients to material that was not otherwise covered. Importantly, nurses did not feel that the VDE process dramatically altered their workflow. This type of buy-in from nursing is important for widespread implementation and may indicate that such an intervention could be useful on other wards and outside of our facility. 29 Qualitative data support overall positive response to the videos, highlighting the value of the videos, and their ability to raise awareness of issues with medications prior to discharge: “What I found helpful was that it made me realize that I need to think about these potential problems before I get home.”
Several studies have demonstrated the need for effective and diverse discharge education.26,30–32 Our results are consistent with previous findings that VDE is a feasible way to increase patient confidence and knowledge.21,24,26 Unique to this study was the evaluation of VDE covering medication barriers on a general medical inpatient service. Our results demonstrate that VDE can play an important role in increasing confidence in and effectively dealing with discharge medication barriers, potentially leading to safer discharge and lower readmission rates. In addition, VDE complemented current discharge practices without hindering workflow, which further supports its integration into clinical practice.
Using animation significantly reduces the extra resources and logistics involved with using live talent. Using different races, ethnicities, and genders for different roles in each video capitalized on the use of peer modeling, an effective way to bring about desired behavioral change.33,34 The videos also empowered patients by demonstrating how to work with care providers prior to discharge to surmount challenges. Previous studies have demonstrated the impact that empowerment can have on adherence among patients with diabetes. 35
Our study had some limitations. As our intention was to gather preliminary evidence of efficacy and feasibility of a novel discharge educational method, it was pragmatic and valuable to conduct a single-arm study. This design, however, makes interpretation of efficacy difficult. 36 Without a control group, we cannot conclude if the effect observed was due to the intervention, placebo, or a social acceptability bias, where patients are willing to misrepresent their symptoms or experiences to obtain perceived researcher approval.37,38 A larger sample size would potentially allow for study of populations at higher risk for medication discrepancies post-discharge, such as the elderly and those with low health literacy.3,20,21 Of the 352 patients who were discharged home based on screening, we excluded a significant number of people due to cognitive inability, non-English-speaking status, and clinical reasons such as any form of medical isolation. Future studies could include these people once a system of cleaning tablets after every patient is in place. Including caregivers in the education and translating videos in future studies of VDE could address other limitations. A relatively small proportion of eligible patients agreed to participate in the study. Exploring reasons for refusal would have better elucidated how to improve our content or timing of delivery. It is possible that patients who participated are not representative of our patient population, but the study demonstrates that a sizable proportion of participants were receptive to this form of education. 39 As discharge education occurs for 100 percent of patients going home from the hospital, our VDE provides complimentary critical information to best prepare patients for the challenges that lie ahead.
Conclusion
VDE may be an effective and feasible way to deliver standardized information about discharge medication barriers that patients do not often anticipate. Improvements in self-efficacy may lead to fewer medication discrepancies in the vulnerable period after hospital discharge. If videos are made available online, patients can view this information repeatedly after they go home, or with their caregivers at any time, using mobile technology. While our findings are from a pilot intervention and are preliminary, they provide a compelling foundation for future work to explore this promising new approach to support patients. Further work could include conducting a randomized controlled trial with a larger sample size to validate and reinforce the findings here.
Clinical implications
Findings from this study have important clinical implications, as VDE offers a novel and feasible mechanism for increasing patient confidence and activation to overcome common medication barriers observed following hospital discharge. VDE exposes patients to common challenges, provides solutions, and allows for standardized and scalable education efforts. This type of patient-centered approach empowers patients with knowledge and skills to overcome perceived medication barriers and has the potential to reduce subsequent avoidable readmissions.
Supplemental Material
Supplement_Scripts_for_Videos_Supplement_A_(1) – Supplemental material for What to expect that you’re not expecting: A pilot video education intervention to improve patient self-efficacy surrounding discharge medication barriers
Supplemental material, Supplement_Scripts_for_Videos_Supplement_A_(1) for What to expect that you’re not expecting: A pilot video education intervention to improve patient self-efficacy surrounding discharge medication barriers by Sanjai Sinha, John Dillon, Savira Kochhar Dargar, Alexi Archambault, Paul Martin, Brittney A Frankel, Jennifer Inhae Lee, Amanda S Carmel and Monika Safford in Health Informatics Journal
Supplemental Material
Swim_lane_Supplement_B – Supplemental material for What to expect that you’re not expecting: A pilot video education intervention to improve patient self-efficacy surrounding discharge medication barriers
Supplemental material, Swim_lane_Supplement_B for What to expect that you’re not expecting: A pilot video education intervention to improve patient self-efficacy surrounding discharge medication barriers by Sanjai Sinha, John Dillon, Savira Kochhar Dargar, Alexi Archambault, Paul Martin, Brittney A Frankel, Jennifer Inhae Lee, Amanda S Carmel and Monika Safford in Health Informatics Journal
Footnotes
Acknowledgements
We would like to thank Mesha Shaw, MD and Dana C Walker, MD for their work as research assistants and Jessica Ancker, PhD for her help with survey and semi-structured interview design.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental Material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.