
Abstract
Introduction
In Australia, one in four young people between the ages of 16 and 24 years struggle with at least one diagnosable mental health problem.1,2 Even though mental health issues represent the highest burden of disease in young people, only a fraction of those who experience distress access traditional mental health. 2 Against this background, mobile health (mHealth), defined as the utilisation of technology to deliver mental health interventions, 3 is increasingly being regarded as a viable alternative to traditional attempts to reach those in need, particularly young people as they are regarded as natural technology users. 4 Technology can help solve some of the barriers young people experience when accessing help for mental health issues, these include the following: distance, accessibility, cost, stigma, limited youth mental health specialists, absence of out-of-hours support and lack of anonymity. 5 A number of online mental health services in Australia currently offer services to young people. An example of an online service designed to promote mental health is ReachOut.com.6,7 ReachOut.com is a fully online service that offers comprehensive mental health resources to youth and parents around education, support and self-management; in 2020, according to their website 132,000 people in Australia access ReachOut.com every month. Although use of these resources has increased over time, only a third of young people diagnosed with a mental health issue report using online services for help and information, 8 so improving engagement with these services could have a significant impact in their effectiveness.
In addition to technologically based clinical interventions that target mental health issues, recent developments in mHealth are investigating strength-based approaches to develop an individual’s strengths and positive resources (e.g. self-efficacy and goal-orientation) 9,10. These interventions focus on increasing a person’s level of well-being as opposed to exclusively addressing the reduction of their mental illness symptoms (e.g. depression and/or anxiety). 11 Well-being encompasses mental health, defined as the presence of positive symptoms in the emotional, psychological and social areas of functioning.12,13 The significance of building and supporting an individual’s well-being is demonstrated by the effect it has on the prevention and management of mental illness, as well as the development and maintenance of positive symptoms of functioning (e.g. increase of life satisfaction, happiness, meaning and purpose).12,14 Recent studies show that well-being can effectively be targeted by technology, particularly by the use of apps given their prevalence, appeal, accessibility and personalisation. 15
Despite the benefits, mHealth interventions usually suffer from high attrition.16–18 Areas suggested to contribute to this attrition include poor design, 19 lack of behaviour change techniques 20,21 and lack of attention given to broad individual characteristics (e.g. gender, mood and age) 22 as well as psychological mediators such as personal motivation, perceived usefulness, expected benefits, enjoyment and personality types.23,24 While findings in this area are inconsistent, age and gender seem to be significant elements when trying to explain who uses mobile health interventions and why.25,26 Studies that have explored app features by gender have found that women value the social features more than men, 27 and that men were more likely to use fitness apps while women gravitate towards nutrition, self-care and reproductive health apps. 28
Identifying the elements that may influence use and predict higher engagement with well-being apps could potentially inform the design and implementation of these resources and increase their potential. To that end, the current study analysed cross-sectional data obtained from the Online Wellbeing Centre (OWC)-RCT 29 in an attempt to identify and understand predictive variables related to the use of well-being apps. The OWC-RCT had two distinct components, the first was a portal called ‘The Online Wellbeing Centre’ used to sign in participants, collect baseline data, administer evaluation measures and randomise participants. The second component was an app self-recommendation service called ‘The Toolbox: the best apps for your brain and body’ (The Toolbox). 30 The focus of the current study was on identifying relationships between previous app usage as reflected in the initial app use survey of the OWC-RCT, and the independent variables collected: demographics (e.g. age, gender and location); ecological momentary assessments (e.g. mood, energy and sleep); and well-being.
Methods
Participants
Participants in the OWC-RCT were predominantly recruited online using mixed strategies, consistent with the procedure described in Musiat et al.
31
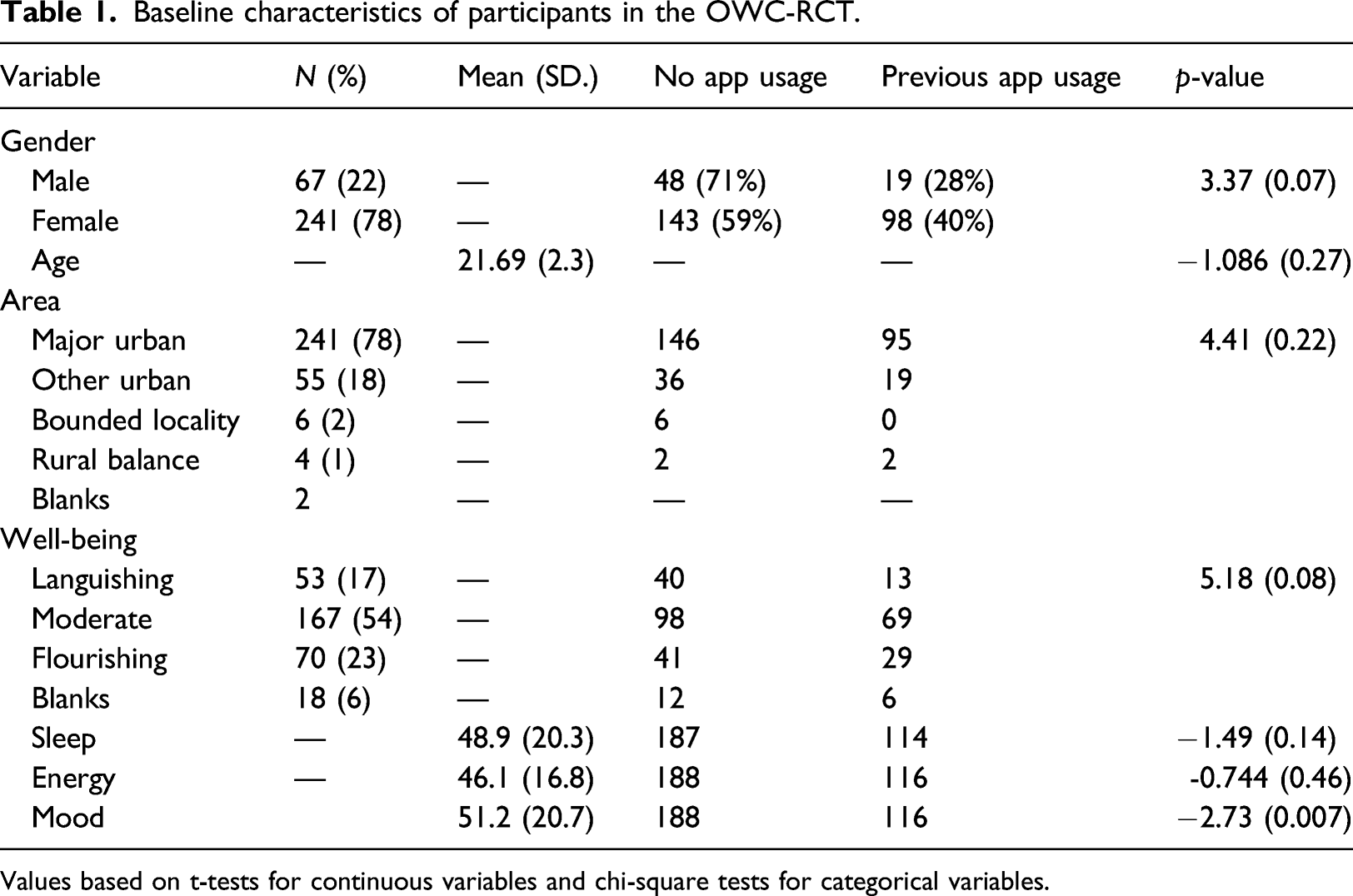
At recruitment, participants were required to provide demographic information (e.g. age, gender and postcode) and complete the Mental Health Continuum Short Form-MHC-SF32,33; recruitment flow can be found in Figure 1. The characteristics of participants app use in relation to the outcome variable (app use before randomisation), using t tests for continuous variables, and chi-square tests for categorical variables, are presented in Table 1. The trial recruited 488 participants, 308 completed the registration process. OWC-RCT recruitment and baseline data collection. Baseline characteristics of participants in the OWC-RCT. Values based on t-tests for continuous variables and chi-square tests for categorical variables.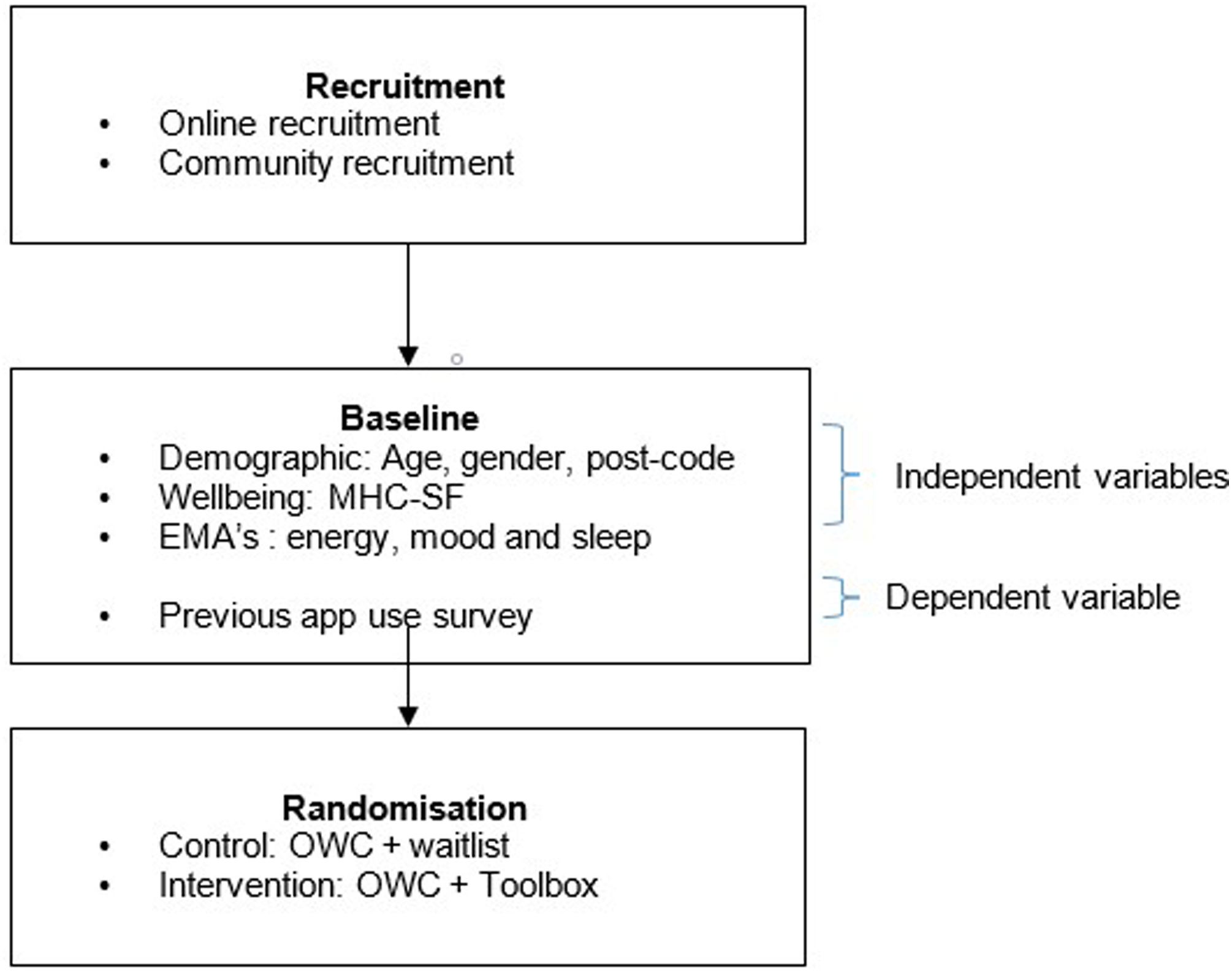
Measures/Procedure
When participants first signed on to the OWC, they were randomised into the treatment arms. Group 1 represented the intervention arm (OWC with The Toolbox); Group 2 represented the waitlist control arm (OWC without The Toolbox). The OWC first used the MHC-SF to assess psychological, social and emotional well-being where, depending on the scores, people were classified into three diagnostic categories: languishing, moderate mentally healthy and flourishing, consistent with the classification that has been validated across different cultures and demographics.34,35 Participants were then asked to self-assess their energy, mood and sleep on three independent Likert scales designed as ecological momentary assessments (EMAs), with 100 being ‘excellent’ or high and 0 being ‘poor’ or low. Lastly, participants were asked to complete a survey designed to identify if they had used any of the 46 apps included in The Toolbox during the previous month prior to signing into the study.
The Toolbox included 46 well-being apps that had been reviewed by a panel of both mental health professionals and consumers using the Mobile Application Rating Scale (MARS). 36 The Toolbox was designed by ReachOut.com to improve emotional, physical, social and psychological well-being of young people between 16 to 25 years of age by the individualised recommendation of apps according to personal goals. 32 In the current study, results from the initial app use survey of the OWC trial were used in order to code app use before randomisation, used as the dependant variable ‘app-use’. Independent variables of the OWC were grouped according to demographics: age (targeted to 16–25 years), gender (male, female) and location (urban, rural and remote); ecological momentary assessments (EMAs): mood, energy and sleep; and well-being measured by the MHC-SF in three categories (languishing, moderate mentally healthy and flourishing). Outcomes of the trial are reported in Bidargaddi et al., 29 and no significant differences in the well-being of participants from either condition were shown, attrition at 4 weeks post-randomisation was 45.1% in the control group versus 55.2% in the active group.
Analysis
Binary logistic regression was used to investigate what predicted participants past use of well-being apps. Accordingly, ‘app-use’ was used as the outcome variable: non-use (0) vs. use (1) in relation to the independent variables: age, gender, location, mood, energy, sleep and well-being as described above. A binary variable was produced by coding all the cases that had not used any app (n=191) vs the cases that had used 1 or more apps (n=117). Statistical analyses were conducted using STATA. 37 The model was also adjusted to the RCT’s attrition rate as a direct indicator for engagement with apps, this variable was included in the model as an interaction term with study groups, this is consistent with previous research that showed that intervention assignment can influence patterns of attrition, particularly those of a behavioural nature.38,39 We also reported model estimates for the unadjusted model. All variables were analysed against the dependent variable in one comprehensive regression model.
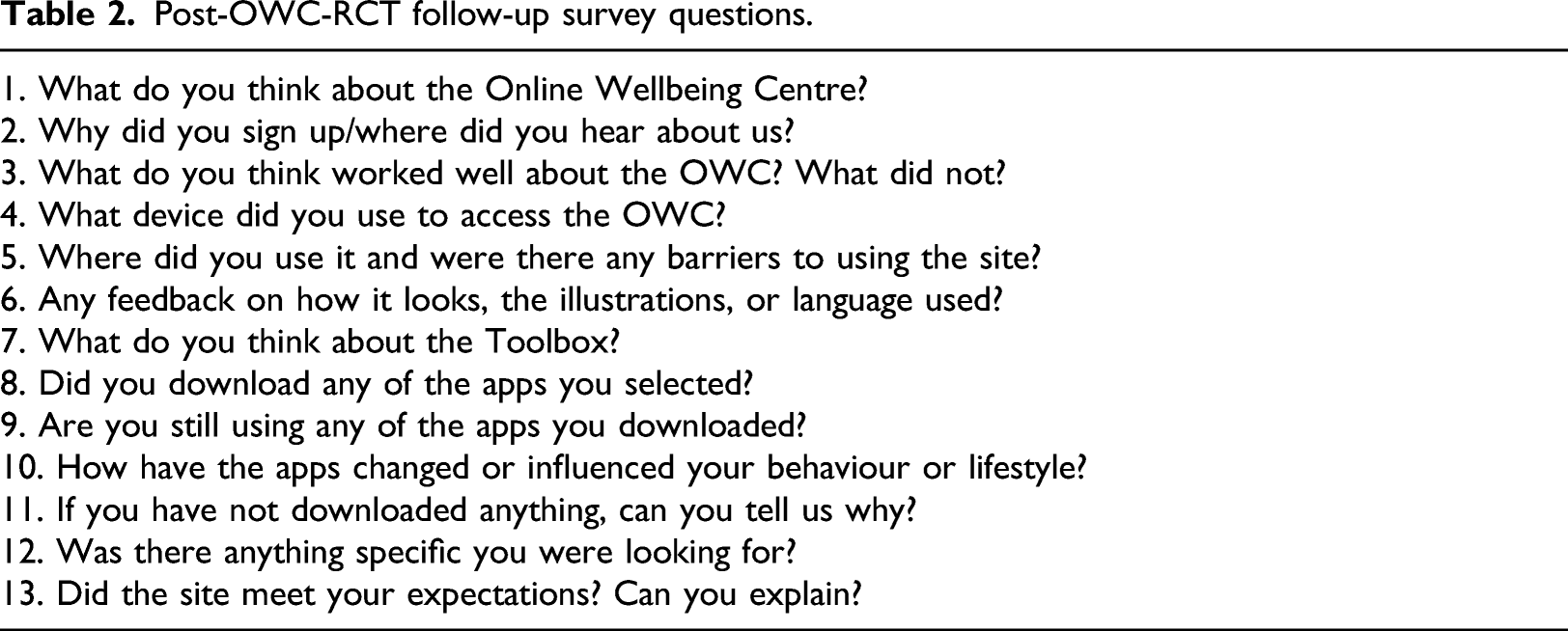
Post-intervention surveys
Post-OWC-RCT follow-up survey questions.
Results
Research Question 1
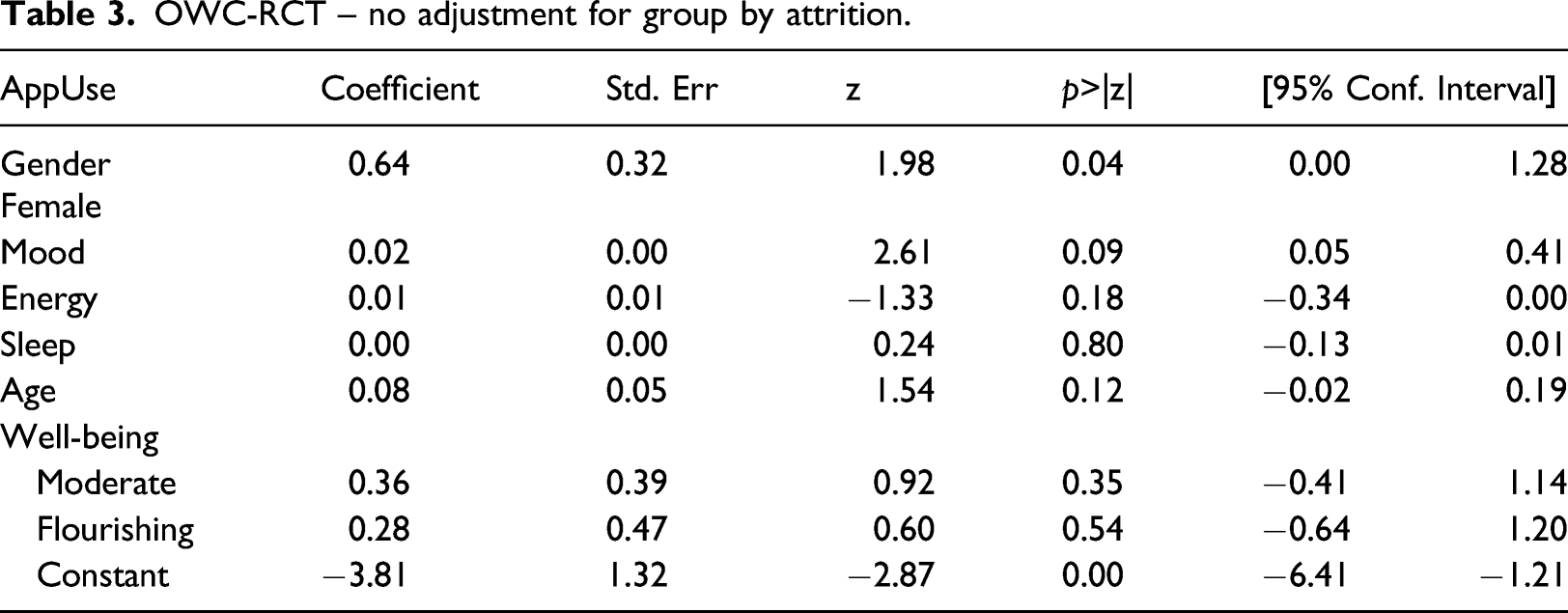
OWC-RCT – no adjustment for group by attrition.
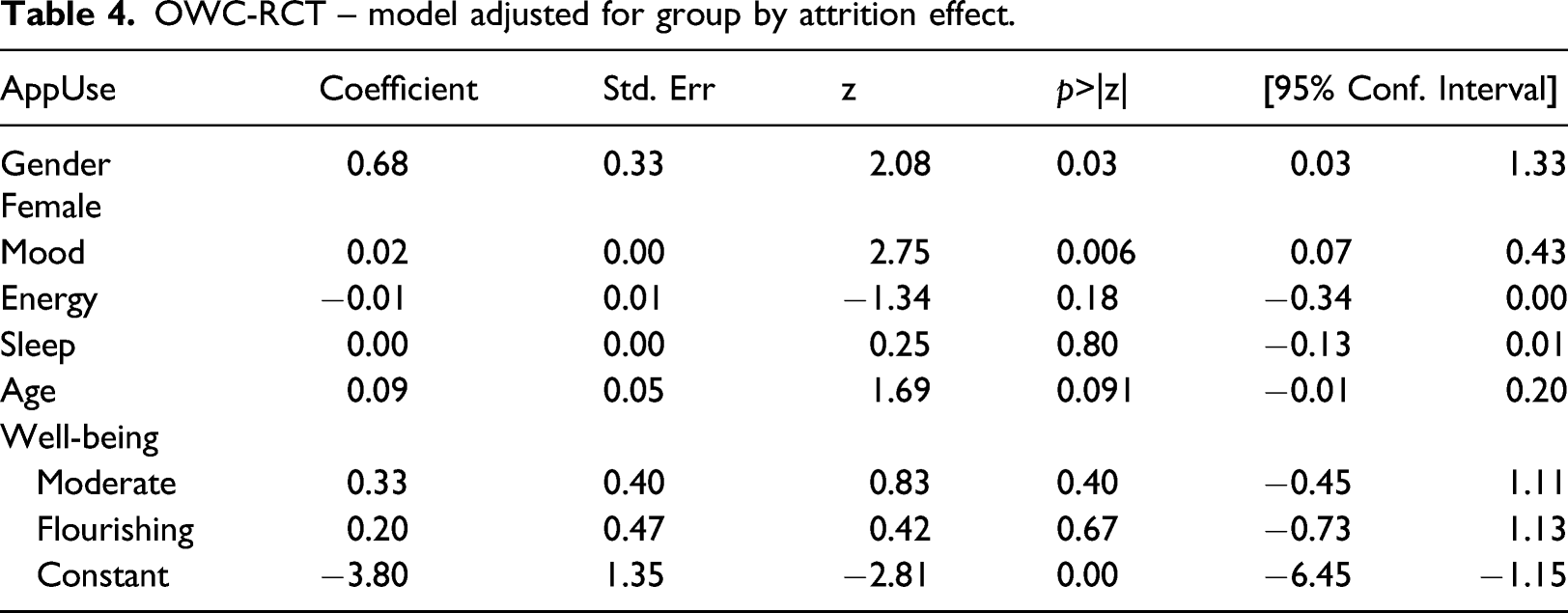
OWC-RCT – model adjusted for group by attrition effect.
Post-estimation analysis – Classification Table. a .
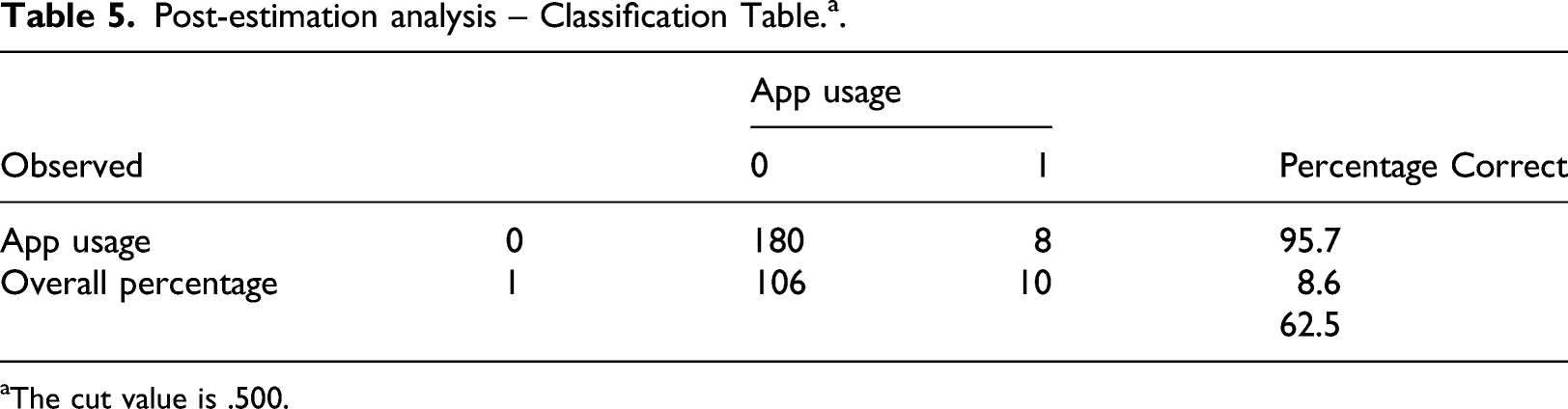
aThe cut value is .500.
Marginal Effects and Representative Cases
Marginal effects can be used to predict how a binary outcome can change in relation to changes in predictive factors.
41
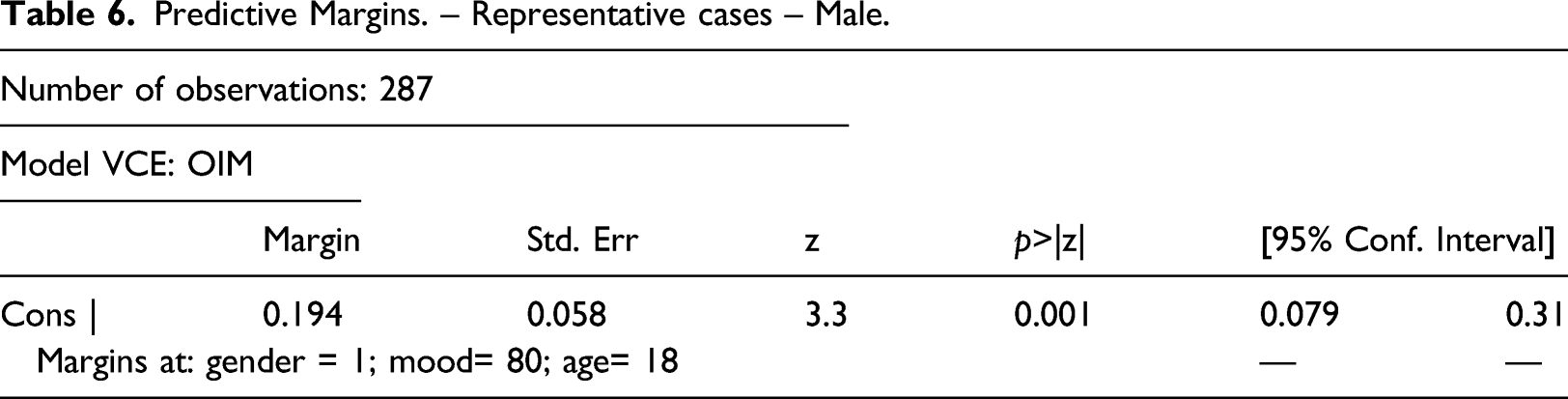
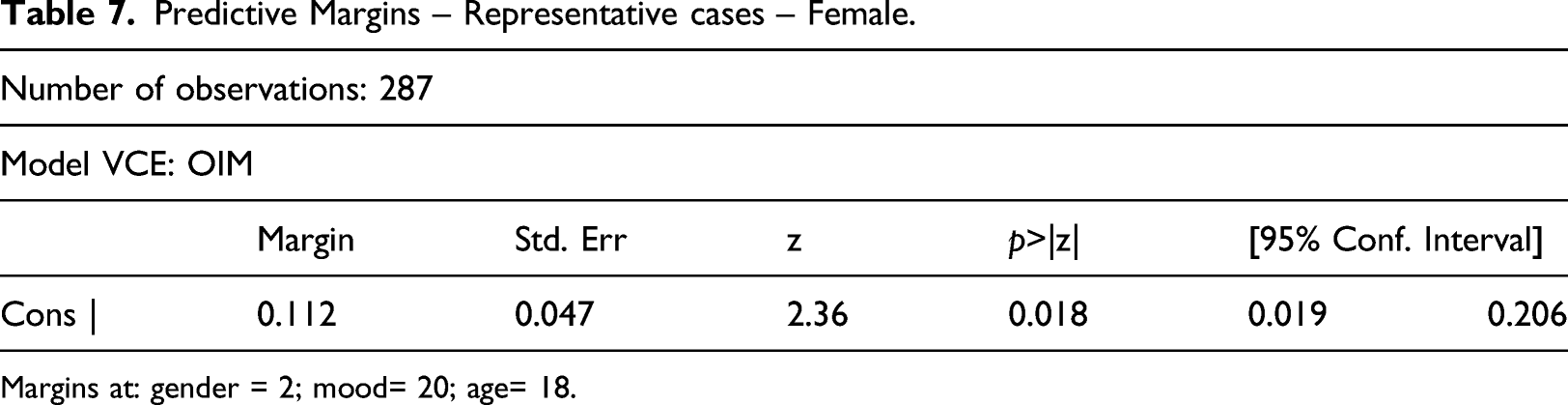
Figure 2 illustrates changes in App-use for male and female in relation to changes in mood. It can be observed that both genders are more likely to use well-being apps the higher their mood scores are. Predictive margins also allow to describe representative cases by setting desired values. Tables 6 and 7 below correspond to 18-year-old male and female participants with a mood score of 20/100 when accounting for energy, sleep and well-being. Results show an 11.27% probability of app-use for the male vs. 19.4% probability of app use for the female. Marginal effects on previous app use by gender and mood. Predictive Margins. – Representative cases – Male. Predictive Margins – Representative cases – Female. Margins at: gender = 2; mood= 20; age= 18.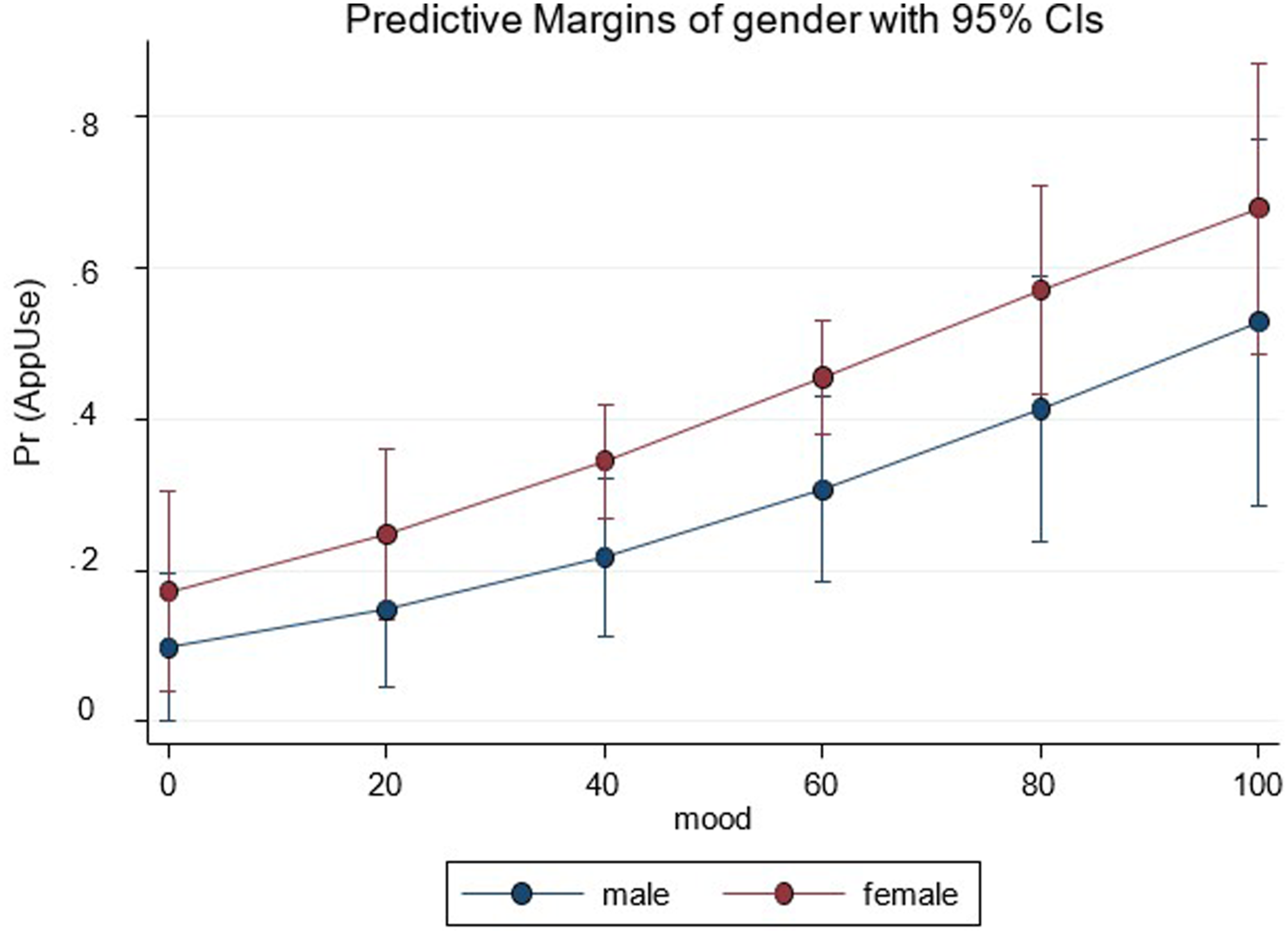
Research Question 2
Post-RCT follow-up survey – Themes identified during coding.
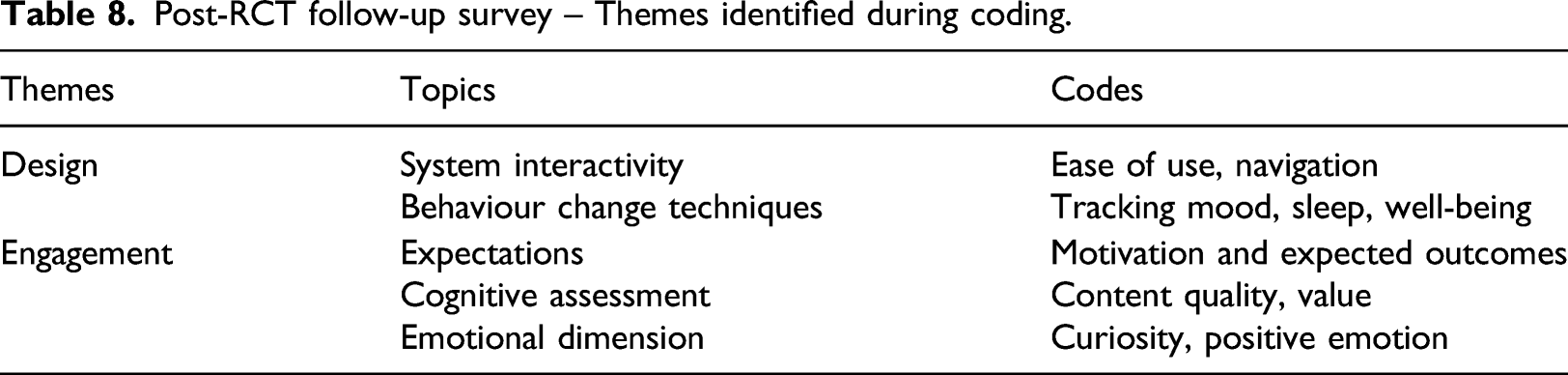
Theme: Design
This theme comprised two codes: system interactivity (usability, individual-app interaction) and the inclusion of behaviour change techniques (bct’s) understood as the active features within the apps that are designed to track users’ behaviours. 44
Several differences were noted in the way females and males interacted with the OWC apps. Males were more likely to focus on specific goals and features (e.g. tracking)
Theme: Engagement
This theme explored the users’ expectations as they pertained their motivations to use the apps, their assessment regarding the apps content, quality and value and the emotional reaction to the apps.
Most respondents said that their interaction with the OWC and Toolbox was positive; however, there was a clear tendency to disengage with these resources after initial contact. Few respondents referred to specific Toolbox apps or their usage with most comments being on the mood and well-being tracking features of the OWC (EMA’s).
Females were able to mention the link between well-being and app usage. To the question ‘was there anything specific you were looking for’, participants responded with thoughts such as: ‘Just something to help improve my wellbeing’. To the question ‘How have the apps changed or influenced your behaviour or lifestyle?’, females were also more likely to specify clear outcomes: ‘managing stress and maintaining wellbeing’; and another: ‘Better understanding of what’s out there to help friends’. Similarly, females were able to clarify the expected and achieved outcomes of app use, indicated by responses to the question: ‘How have the apps changed or influenced your behaviour or lifestyle?’ responses included: ‘made me slightly, more attentive and aware of issues’. Being aware of the impact of these apps was also true for those not perceiving any benefit, for example, a participant said: ‘No. Used for a month, then found they weren't really working for me’, and another: ‘None really appealed, or thought they wouldn't be useful’. In comparison, males were more likely to have accessed the toolbox out of ‘curiosity’, as indicated by responses to the question ‘was there anything specific you were looking for?’ This is illustrated by responses like: ‘just to try, curious’; and ‘Not really, just looking’. When talking about their motivation to use apps, male comments’ were non-specific and signaling towards low interest even prior to been offered the recommended apps; this is shown to answer to the question ‘If you haven't downloaded anything, can you tell us why?’, responses included: ‘Don't feel like I need it’; and: ‘Nothing specific, but I assumed it would help with my overall wellbeing’. Males were also more likely to avoid using the website and apps or stop using them after a short time, some of the comments reflecting this included the following: ‘Accessed it, didn't use it’; ‘Didn't use it originally - intention to use but didn't due to life circumstances’ and ‘It was easy to lose interest in trying’.
Most statements related to mood had positive connotations. Some comments referenced the impact of the Toolbox and associated apps in mood, for example: ‘It’s a good platform to help me, especially when I’m feeling down’, and ‘it makes me feel happy’. Regarding the value of tracking moods in the OWC, participants said: ‘makes me take notice of feelings’; ‘It’s good, helpful for tracking moods’. A number of participants expressed their satisfaction with the intervention with comments like: ‘Love it!’; ‘It was inviting’; ‘it’s engaging and pleasant’ and ‘it’s calming’; these positive appreciations were common on responding questions regarding the layout and navigational features of both the OWC and Toolbox, indicating a possible link between design and engagement.
Discussion
A cross-sectional analysis using data obtained from an online RCT was conducted to identify predictors of app use by young people, followed by an interview with participants to determine what they liked or did not like about the platform. Results indicated that females with heightened mood levels were more likely to adopt these technologies, and that while enticing the apps within the OWC and Toolbox fell short of sustaining engagement. These findings add to existing literature by showing that young women are more likely to engage with apps specifically offered as well-being apps or specifically designed to improve health aspects; whereas young males tended to lose interest quicker and focused mainly in features such as tracking. 27,28
Analysis from the follow-up interviews showed that females were more likely to think about well-being, stress and social elements (i.e. friendships) before they choose a specific app; whereas males were more concerned with the actual functionality of the apps (i.e. tracking). This finding could explain why well-being as a concept may initially appeal more to females, while apps designed following gamification techniques may appeal more to males. This consideration could be important at the time of designing and marketing this type of apps (e.g. females orientated more to the relational/social aspects of well-being vs. male more behaviourally orientated to the ‘doing’ aspects of well-being). As for mood as a predictor of app usage, it could be associated to motivation, enjoyment and expectations. It has been demonstrated that young people show initial interest when first introduced to these types of interventions; however, this effect usually dwindles over time. 22,45
Young people increasingly use apps to mediate and facilitate most of their behaviours in all aspects of daily living including social sphere. 46 The overabundance of information and the ever-changing speed of technological developments makes meaningful engagement with any health app difficult; and even more so with well-being apps. 22 Despite this barrier, the potential of apps to increase well-being should not be overlooked. Apps have the added benefits of abolishing obstacles like accessibility, cost and perceived stigma; they can be discreet, personal and private. 47 The importance of improving engagement with potentially effective well-being apps is highlighted in crisis times such as the current COVID-19 pandemic. 48
From this study’s findings, understanding gender preferences and developing strategies to improve participants’ mood at the time of deciding to install and use well-being apps could improve app uptake and their effects in the long term. These strategies could be included in the actual design of the apps with artefacts such as rewards, social recognition or other types of positive reinforcement. 49 Exploring how gaming features could be included in this design could also be beneficial as studies in this area show promise to increased engagement. 50 Some examples in this direction already exist with apps such as ‘zombies run’ designed to improve fitness while at the same time introducing users in an involving gaming environment. 51 Another example that has had an impressive impact is ‘Pokemon Go’, an app/game that has effectively drawn young people outside of their homes into walking.52,53 Alternatively, if apps were to be used as part of a planned intervention, mood-enhancing techniques and psycho-education could be used during the process to highlight the meaning and importance of well-being at a personal level.
Limitations
There were several limitations arising from the RCT that may have impacted results. The current study was limited by the demographic data collected, this in turn meant that many variables that could have been significant in responding the research question were not present; this scarcity of investigated factors is a considerable limitation. By the nature of the intervention to be tested (The Toolbox), the apps assessed were already pre-determined, and this eliminates the possibility of having a real appraisal of the totality of well-being apps that young people participating in this study could have been using at the time of signing up; having said that, the apps included in the Toolbox were assessed by the MARS scale 36 and as such were relevant in their quality and their potential to increase the well-being of the participants. A larger number of participants were in their 20s and less in the 16–19 year old bracket, this was due to the added difficulty of obtaining parental consent for underage participants during recruitment. 31 Similarly, the great majority of participants came from urban areas, which may be a reflection of the general demographic distribution in Australia as well as an issue of Internet access in rural areas. This study also suffered from high attrition as reflected in literature for similar studies, with the lack of engagement with digital resources as an expected feature. 18 Female participation was higher as consistent with existing literature54,55; however, this can also be considered a limitation. In the context of the OWC trial, the intervention apps were almost entirely comprised by self-help apps focused on improving discreet aspects of the users lives, from relationships to fitness. Very few apps in the intervention could be used in a ‘gamified’ way, despite the fact of including behaviour change techniques related to rewards and goal setting.56,57
Finally, the thematic analysis used in the qualitative phone-based questionnaire must be interpreted with caution, since the questions favoured the identification of specific issues.
Conclusion and future research
Despite the potential of well-being apps to improve well-being in young people, engagement with these resources continues to be a significant problem. To that end, we sought to identify what predicts engagement with well-being apps and found that in the context of this study it was related to personal characteristics like mood and gender. Ignoring the different reasons people are drawn to, remember, and use apps in relation to well-being will do nothing to ultimately increase engagement with these apps. In that context, while this study contributes to knowledge of why young people may or may not engage with well-being apps, given the importance of this area, further research is needed to explore a broader range of variables intrinsic to users such as personality, age, culture and other identity markers.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is part of a collaborative project supported by the Young and Well CRC and in partnership with Flinders University and Country Health SA. The Young and Well CRC is established under the Australian Government’s Cooperative Research Centres Program.