
Abstract
Despite the current popularity and potential use of mobile applications (apps) in the area of behaviour change, health promotion, and well-being for young people, it is unclear whether their design is underpinned by theory-based behaviour change techniques. Understanding the design of these apps may improve the way they can be used to support young people’s well-being.The objectives of this study were to investigate what behaviour change techniques are included in the content of health and lifestyle apps, and determine which of these are prominent in app design. Thirty of the top-listed health and lifestyle apps across three categories (physical activity, diet, and sleep) were freely downloaded from the two most popular app stores (GooglePlay™ and AppStore™). Selected apps were used by trained researchers and the features identified coded against the Behaviour Change Techniques Taxonomy 1, a systematic classification of techniques used in behaviour change interventions. It was found that 9 of the 93 behaviour change techniques listed in the Behaviour Change Techniques Taxonomy 1 were common across the chosen health and lifestyle apps. The app found to include the most behaviour change techniques had 20 (21%), while the app found to include the least had 1 behaviour change technique (1%). The most frequently used behaviour change techniques were related to goal setting and feedback. Entire categories in the Behaviour Change Techniques Taxonomy 1 were absent in the design of the selected apps.
Introduction
Freely available mobile applications (apps) are being used in a range of lifestyle and health settings which is aided by the increasing availability and use of smartphones. Mobile applications (apps) are being used as co-adjuvants for a range of health interventions 1 such as weight loss and physical activity, 2 smoking cessation, 3 and psychological distress (e.g. depression, anxiety, and post-traumatic stress disorder). 4 The aim of these apps is to help prevent lifestyle-related illnesses as well as the improvement of overall health. 5 Positive health behaviours can be defined as ‘any activity undertaken for the purpose of preventing or detecting disease or for improving health and wellbeing’. 6 Negative health behaviours including physical inactivity, poor diet, and tobacco smoking are linked to chronic mental and physical disease.7–9 Improving health behaviours can positively improve mental and physical health at an individual and population level.10,11
A new opportunity is emerging for apps to be utilised in well-being.12,13 Well-being encompasses both an individual’s positive feelings and positive functioning in life. 14 Apps associated with well-being are designed to support a positive outlook on life and drive ongoing positive health behaviours. These health and lifestyle apps are relevant for young people given their affinity with new technologies. 15 In Australia, over 20 per cent of young Australians (15–19 years) are thought to meet the criteria for mental illness, and 60 per cent of these report to be uncomfortable in seeking face-to-face help or advice for mental illness. 16 It is clear that finding new ways of supporting mental health and well-being are needed. The use of apps to improve well-being is a nascent area of research which aims to cost-effectively promote the engagement of young people with health services by minimising stigma and improving accessibility.15,17 A review of 126 studies 18 found that mental health services delivered using technology resulted in high levels of satisfaction for practitioners, families, and young people and that young people preferred getting mental health support via technology.
The app stores categories ‘health & fitness’ and ‘lifestyle’ contain a number of resources for promoting positive health behaviours. Health apps account for 2.9 and 8.8 per cent of apps found in the GooglePlay™ and AppStore™ libraries, respectively. 19 However, there has been an increase in their use over the last couple of years, registering a growth of 89 and 174 per cent in both app stores in 2014. 19 Tracking technologies (capable of recording users’ behaviour) are a particular area of growth granting users cost-effective insight into their daily behaviours. 20
Despite the potential of apps to influence changes in health behaviour, 4 there is limited evidence of their foundation in health theory. This study investigates behaviour change techniques (BCTs) within popular health and lifestyle apps. BCTs are the basic mechanisms derived from theory that drive behavioural change. 21 A number of taxonomies have been designed to analyse the BCT content of health interventions, such as alcohol consumption, 22 physical activity, 23 and sexual health. 24 These taxonomies allow contrasting multiple theoretical frameworks, drawing from multiple behaviour change theories to identify the basic components that change behaviour. Previous studies of BCTs in apps have contributed to our understanding of how behavioural interventions work in this context.20,25 One study suggested that effective incorporation of BCTs in an app facilitates increased engagement and effectiveness. 26
This study focused on tracking apps and their impact on physical activity, 11 diet, 27 and sleep. 28 These categories were chosen given their importance in mental health. Tracking apps were chosen because they offer personalised and quantifiable feedback versus generic information. The following questions were addressed: What BCTs do the selected health and lifestyle apps include in their design and which are used more often? To the researchers’ knowledge, this is the first study to analyse BCTs in three categories simultaneously (comparing similarities).
Method
App selection
Apps were identified and selected from GooglePlay and AppStore and coded according to the Behaviour Change Techniques Taxonomy 1 (BCTTv1). 29 Accessibility and availability were prioritised in the context of young people as target users. Apps were selected following two main criteria. First, apps had to be present in both of the most popular app stores. Second, apps had to be free (i.e. no monetary cost to the user) even if they also offered paid versions. Additional criteria included selecting apps that had a user rating of 4 stars or more out of 5 in GooglePlay, offered tracking capabilities, and focused on at least one of the chosen areas of analysis (physical activity, diet, or sleep). The top 10 apps arising from the selection process in each category were compared. It is important to clarify that the star rating system in GooglePlay works as an indicator of popularity and is calculated from users’ feedback, AppStore ratings were not used as a criterion. Similar studies have also used this criterion for app selection.30,31 The selection process is illustrated in Figure 1.
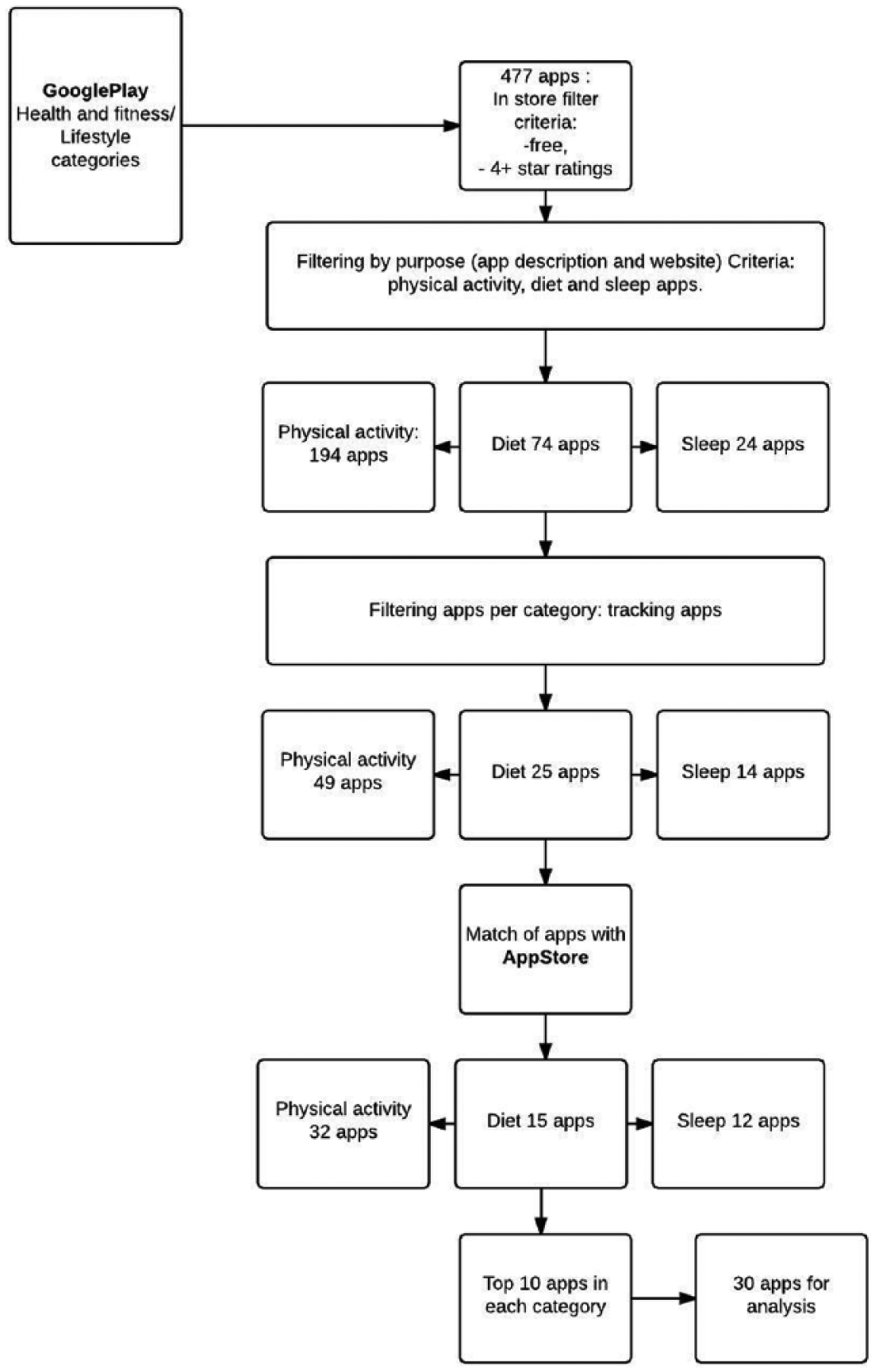
The process followed for app selection.
Coding
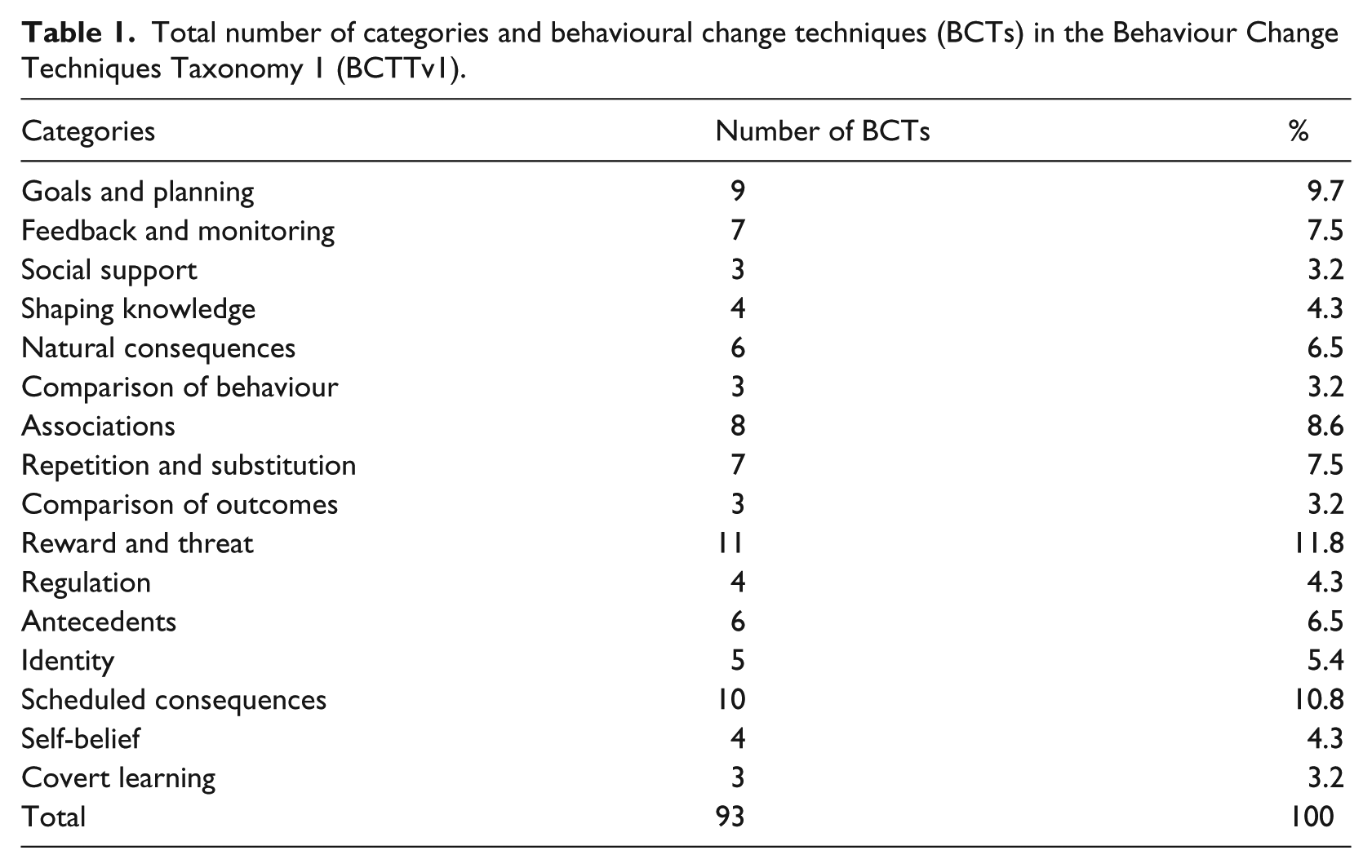
Apps were coded using the BCTTv1. 29 The BCTTv1 is a comprehensive non-specific classification (refer to Table 1 for the 16 categories included in the BCTTv1 and the total number of BCTs in each) that has been used effectively in several research projects including a similar study that analysed electronic activity monitors.32–34 The BCTTV1 was created by experts following a Delphi-type exercise that analysed and classified BCTs from published classification systems and was validated by coding behavioural interventions in which adjusted kappas of ⩾0.60 were obtained. 29
Total number of categories and behavioural change techniques (BCTs) in the Behaviour Change Techniques Taxonomy 1 (BCTTv1).
The authors (G.A., A.V., and V.B.) were self-trained in the BCTTv1 taxonomy by completing the online course designed by Prof. Susan Michie and her colleagues from University College London (UCL). 35 This training does not establish protocols to code apps specifically, but provides information regarding the underlying principles of each BCT in the 16 categories. All coders had backgrounds in one or more of Psychology, Mental Health, and Youth Work. Coders were required to download and use the apps for a month. Triple coding was carried out in 50 per cent of the apps selected randomly from the finalised list using the statistical software package Stata version 13. 36 Coders completed two rounds of analysis. After the first round of coding, agreement was reached in 48 per cent of the total number of BCTs identified (two or more coders). At the end of the second round, agreement between two or more coders increased to 70 per cent; this was considered acceptable in the context of three coders using an extensive taxonomy in comparison to similar studies using more specific taxonomies with just two coders obtaining interrater agreements between 80 and 90 per cent.22,37 Most differences between coders referred to overlapping concepts and their practical implementation within the apps, for example, ‘Goal setting (behaviour)’ versus ‘Goal setting (outcomes)’; these two BCTs differentiate depending on the way goals are established and how they are used during the intervention. However, it was clear that there was strong agreement at a categorical level, in this case ‘Goals and planning’. Discussion was guided by analysing the different techniques using specific definitions established by the BCTTv1. After the second coding round was completed, GA completed the analyses of the remaining 50 per cent of apps. Coding focused on features found in the apps as executed in their mobile phone version; this means that features offered in external websites or third parties were not coded as they were not considered to be part of the mobile apps.
Results
To investigate which BCTs are included in health and lifestyle apps, selected apps were used and features identified coded against the BCTTv1. Results indicated that all chosen apps did contain at least one BCT. The most BCTs found in one app was 20. Only a small portion of the 93 BCTs listed in the BCTTv1 were present overall and entire categories were absent.
Physical activity apps emphasised ‘Feedback on outcomes of behaviour’, ‘Action planning’, ‘Feedback on behaviour’, and ‘Self-monitoring of outcomes of behaviour’ (80%) as the principal BCTs in their design. Feedback consisted of displaying quantified data including distance travelled, steps taken, and calories consumed. At a second level, goal setting BCTs were common: ‘Goal setting outcome’ 60 per cent and ‘Goal setting behaviour’ 70 per cent including forums and communities as well as through the implementation of virtual group workouts (challenges). These features were coded as ‘social support’ (unspecified) in 80 per cent of the apps in this subcategory. All of the apps in this category could be linked to other apps.
‘Feedback on outcome(s) of behaviour’ was present in 100 per cent of the analysed calorie tracking apps (diet apps), displayed as daily calorie or kilojoule consumption, also taking into consideration food intake and self-registered exercise together with body mass index (BMI) scores. The ‘Goal setting (outcome)’ BCT (90%) was present in as these apps require users to set a desired weight. The other two prevalent BCTs in this category – ‘Self-monitoring of outcome(s) of behaviour’ (90%) and ‘Self-monitoring of behaviour’ (70%) – required users to manually input food intake and activity levels. ‘Social support (unspecified)’ (80%) was coded to categorise all of the social sharing features embedded in these apps.
Sleep tracking apps relied on movement sensors embedded within smartphones to provide ‘Biofeedback’ (50%) and ‘Feedback on outcomes of behaviour’ (50%) expressed as sleep cycle reports. These apps also used ‘action planning’ (60%) and ‘Prompts/cues’ (70%) in the form of ‘relaxing sounds’ and ‘smart alarms’ designed to help sleep conciliation as well as prompting the wake-up cycle. Two of the apps in this category ‘Calm’ and ‘Deep Sleep Relax Hypnosis’ were distinct because they did not track sleep cycles, but were retained given their aim to help users improve sleeping patterns by providing feedback. This category showed a much lower incidence of social support BCTs.
Overall, 51 BCTs (54.83%) were unutilised and 9 (9.6%) were used once (by single apps). Non-used categories in the BCTTv1 included ‘Regulation’, ‘Identity’, ‘Covert learning’, and ‘Self-belief’ accounting for 16 BCTs out of the 93 comprising the BCTTv1 (17.2%).
Results indicated that of the 93 BCTs listed in the BCTTv1, only 7 were identified as being present in 50 per cent or more of the apps (refer to Table 2 for the number of categories in the BCTTv1 represented by the BCTs in each app). The most common BCT across apps was ‘Feedback on outcomes of behaviour’ (76%) followed by ‘Self-monitoring of outcome(s) of behaviour’ (67%). Other BCTs over 50 per cent commonality were ‘Goal-setting outcome’ (50%), ‘Action planning’ (50%), and ‘Self-Monitoring of Behaviour’ (53%); the five BCTs mentioned are classified within the categories ‘Goals and Planning’ and ‘Feedback and Monitoring’. The remaining two BCTs ‘Social support – unspecified’ (60%) were present through different features, from in-app diaries to active participation in online communities. Similarly, BCT ‘Prompts/cues’ (57%) were present as reminders, alarms, and customisable messages.
Number of BCTTv1 categories represented by the behaviour change techniques (BCTs) in each app.
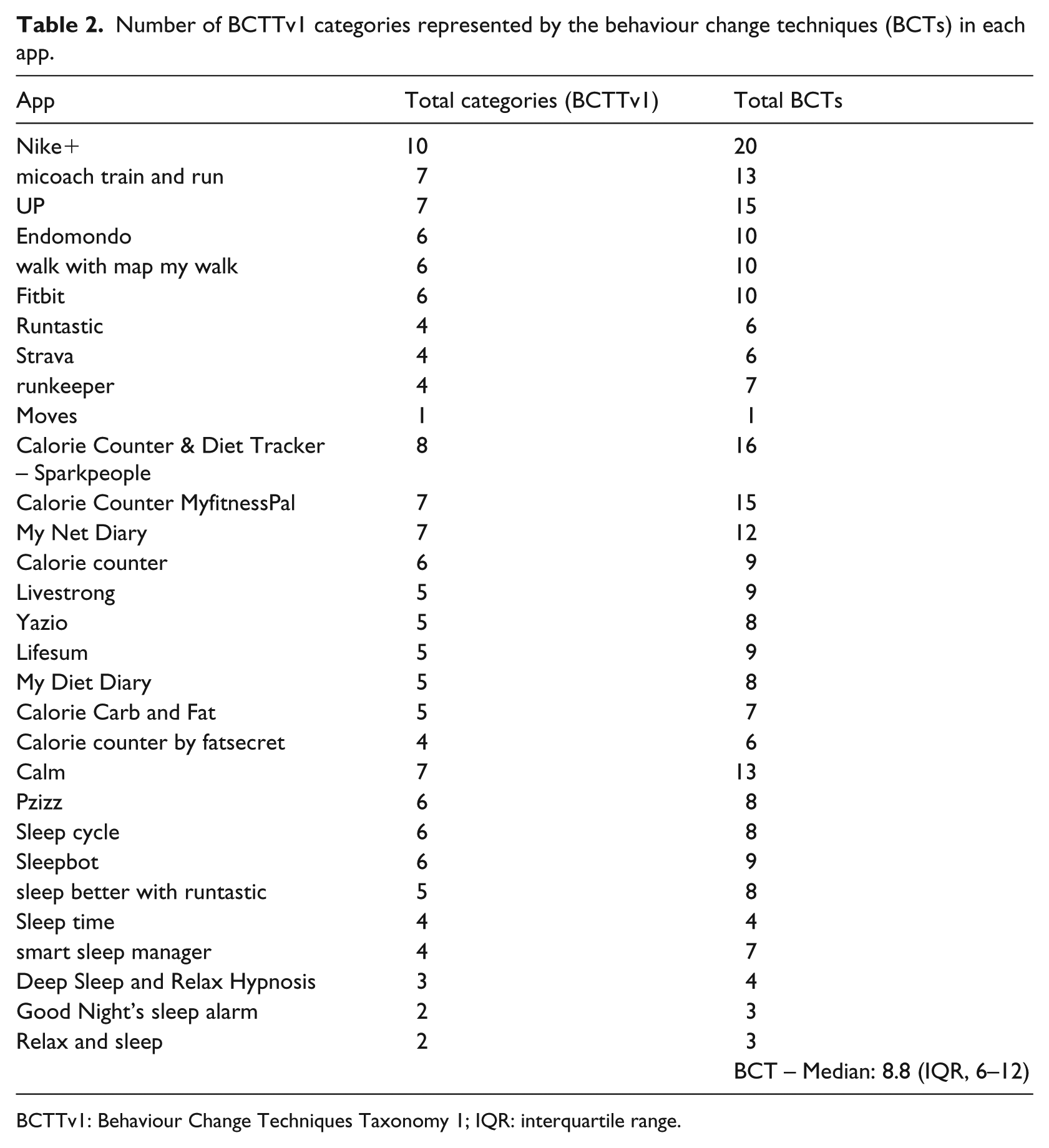
BCTTv1: Behaviour Change Techniques Taxonomy 1; IQR: interquartile range.
Discussion
This study investigated selected health and lifestyle apps and established which BCTs are included in their design. Results indicated that only a small portion of the 93 BCTs listed in the BCTTv1 were present across the selected apps (9.6% commonality). Of the selected apps (i.e. tracking apps), the most frequently used BCTs were related to goal setting and feedback. However, entire categories of the BCTTv1 were not observed, highlighting possible avenues for future app development. Incorporating BCTs of these missing categories in the design of health and lifestyle apps could open new possibilities for app developers in helping users change their behaviour effectively and also in potentially achieving higher engagement with their apps. Previous research 38 highlights that although the use of health tracking apps is increasing, people don’t engage with them in the long term, rendering these resources potentially ineffective. Findings like these support the importance of matching theory and engagement to back up effectiveness. This is illustrated in calorie tracking apps, which require the user to register food intake. Calorie tracking apps can achieve this by implementing different features: one option may be to rely on the user to manually input the food, its ingredients, and amounts; another option may be the provision of extensive food lists for the user to choose from; while another may be the inclusion of an automatic bar code scanner to register their food intake seamlessly. In all three scenarios, the BCT involved is ‘self-monitoring of behaviour’. However, it is reasonable to assume that users will opt for the simplest method and that continued engagement will depend on ease of use.
BCT categories such as ‘Self-talk’ or ‘Identity associated with changed behaviour’ may be used to increase user engagement by focusing on intrinsic and social motivation, 39 as these elements have been shown to boost engagement in previous studies. 38 A study analysing behaviour change interventions delivered via SMS (short message service) found that studies using un-tailored SMS suffered greater attrition than studies that considered elements like age, gender, behavioural history, preferences, personal goals, personal barriers, and personal details (such as name or nickname). 40 Another study highlighted that young people emphasised having flexibility in the design and implementation of physical activity interventions based on their personal characteristics including age, gender, and contextual variables. 41
Developers may lack understanding of behavioural theory, hindering the development of higher quality apps. Future developers should aim to embrace the repertoire of BCTs used and establish synergies by linking features together. For example, the pedometer app ‘moves’ can link with the calorie-tracker ‘lifesum’, expanding the scope of both apps. This could represent an opportunity to provide users with a more comprehensive suite of resources to improve their health behaviours. From a well-being perspective, future apps could combine BCT categories such as ‘Social support’ and ‘Identity’ with techniques already in use such as ‘goals and planning’ and ‘feedback and monitoring’ to help young people create and expand their social networks and receive feedback on their behaviours by peers.
Despite all of the above, it could also be argued that as long as the techniques are effective, there is no need to include a wide variety of them. The true impact of BCTs on the effectiveness, uptake, and continued engagement with health and lifestyle apps is not yet fully understood. The effectiveness of BCTs in health and lifestyle apps could also be related to age, gender, location, and other cultural variables. These considerations warrant further research to enhance the design of apps capable of producing sustained behaviour change.
Limitations
Interpretation of this research is limited by the dynamic nature of apps. New app versions are available frequently and can vary from minimal technical improvements to significant changes in function. Some BCTs may have been omitted from the evaluation as apps were only used for a short period of time; however, coders were asked to use the apps as long as needed to obtain the best possible appraisal of their features. It is also important to highlight that not all app features are available for all versions across all platforms (Android vs Apple) and some differ depending on the smartphone being used. Further BCTs may have been omitted by poor app design; however, findings are consistent with user experience. The fact that only free versions were coded and most apps offer paid upgrades with allegedly better features and techniques is also a limitation as we were unable to assess the full capabilities of each app.
Future research
Results highlight the importance of establishing relationships between BCT content and effectiveness in apps to generate sustained behaviour change. Future app development should focus on incorporating evidence-based techniques in a way that is appealing to the user to ensure greater uptake and increased behavioural change. These apps should be assessed either by qualitative (to understand meanings, perception, and personal characteristics of users) or quantitative studies (to understand relationships between specific BCT and engagement dimensions).
Conclusion
Current research suggests that health and lifestyle apps designed to modify health behaviours contain low levels of theory-based BCTs. Increased implementation of BCTs could improve interventions and achieve higher levels of user engagement. The importance of this research is highlighted by the increasing consumption of health and lifestyle apps especially by young people. These apps promise to ‘improve’, ‘support’, and provide solutions to the user’s needs while lacking evidence base. This puts young users at risk by providing ineffective solutions. 42 Young people use technology as a valid alternative to face-to-face mental health support adding to the importance of designing quality products. The increasing reliance on these technologies should highlight the importance of using them to promote well-being, as well as connecting people with services and guide them to access the best available help when they need it.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is part of a collaborative project supported by the Young and Well CRC and in partnership with Flinders University and Country Health SA. The Young and Well CRC is established under the Australian Government’s Cooperative Research Centres Program.