
Abstract
A record number of immigrants, many Arabic speaking, arrived in Sweden during the years 2015/2016. Immigrant women have a higher risk of pregnancy complications than native European women and cultural and communicative problems have been identified as a cause of such disparities. Maternity services are under pressure because of language and cultural barriers. Language translation programmes are sometimes used but these are not evidence-based so are not considered safe for use in maternity care. The aim of this research was to create an evidence-based app for communication with Arabic-speaking women in maternity care. User-centred iterative design was used to develop an evidence-based, fit-for-purpose app. Data were collected from midwives in a focus group interview, field observations and workshops. The iterative approach resulted in an evidence-based prototype that is currently being tested in the field.
Introduction
Sweden received a record number of immigrants, almost 300,000, in 2015 and 2016. 1 A large number of these new immigrants were young Arabic-speaking women (ASW) of child-bearing age. This placed already stretched maternity services under increased pressure; it implied more clients as well as challenges that language and cultural barriers can imply. All non-Swedish speaking women are legally entitled to an interpreter but interpreters are not always available and may not always be conversant with the challenges of midwife/client meetings. Swedish healthcare aims to provide equal care to all of its inhabitants, 2 and it is important to address language and cultural barriers experienced by immigrants to ensure equity of care. Information technology (IT) may have the potential to address these problems.
Background
Immigrant women have a higher risk of complications than native Europeans. An international review study found that immigrant women in Europe had a higher incidence of low birth weight, pre-term delivery, perinatal mortality, and congenital malformations. 3 Immigrant women in Italy were at higher risk of pre-term deliveries and low birth weight babies. 4 Swedish studies have shown that women from low income countries who do not speak Swedish had a higher rate of maternal and infant mortality.5,6 Immigrant women tend to contact maternity services late in the pregnancy.7,8 Cultural and communicative problems have been identified as one reason for disparities in pregnancy outcomes for immigrant women. 9
To overcome communication difficulties, healthcare professionals (HCP) often rely on translation programmes, such as Google Translate, 10 or a language application (app) on a mobile device. The accuracy of these devices cannot be assured and may be unsafe with regard to diagnoses and medical treatment. In one study, Google Translate was found to be unsafe for use in maternity care but purpose-designed IT may have the potential to alleviate language and cultural barriers. 10
Pilot study
In late 2015, we carried out a pilot study. 11 The aim of the study was to identify the types and extent of communication and cultural problems experienced by midwives in antenatal care (ANC). The results demonstrated that midwives had a stressful and difficult work situation, largely due to communication and cultural challenges when meeting women who could not communicate in Swedish. The suggestion of developing an ‘app’ with multimodal components to promote cultural and linguistic understanding was received with enthusiasm from the midwives.
App development
There are many medical software applications (apps) available and widely used by HCP, 12 but new systems often fail to meet the needs of the end-user. 13 Mobile healthcare apps often fail because of poor attention to usability, lack of clinician involvement and inadequate understanding of the healthcare setting. 14 Moreover, many medical apps have not followed evidence-based guidelines which can compromise quality and safety. 15 Apps that improve communication between clinicians and patients have been identified as an ‘unmet need’. 16
To create an evidence-based app to meet the needs of midwives and their clients in ANC, careful design planning was required. There are several design options. Participatory design (PD) focuses on technological solutions to practical problems. 17 It emphasises ‘designers and users working actively together’. 18 Requirement engineering (RE) emphasises requirement elicitation, prioritising usability in context and ‘defining precisely the problem that the software is to solve’. 19 Sociotechnical approaches stress end-user perspectives, in-depth understanding of work processes and effectively eliciting in-context user needs. This approach can use an iterative process to promote the interlinking of human factors and technology, with co-development of a system by addressing problems that emerge during the development process. 20
A design which drew on the fore-mentioned approaches was adapted for the research project described in this paper. It embraced three key principles. First, the perspectives of end-users should be included in the development process.17,20,21 This implied observing what people do and listening to what they say. 16 Second, there needed to be in-depth understanding of work processes in health care.20,22 Finally, medical apps should be evidence-based and reliable to ensure quality and safety. 15
Aim
The aim of the research was to elicit user needs for interactive communication in ANC and to translate these into specific user requirements to develop and test a multi-modal communication app.
Objectives
to assess midwives’ needs and frame an understanding of midwives’ work processes and responsibilities during planned encounters.
to define the challenges to communication that midwives and Arabic-speaking women encounter during appointments.
to develop an evidence-based app that was fit-for-purpose.
Methods
This study adopts an innovative approach, applying elements of PD and RE, and draws on a sociotechnical approach with an iterative process. The approach was cyclical (Figure 1) and merged development and evaluation of an IT application. 20 The proposed app is intended as a complement to interpreters.
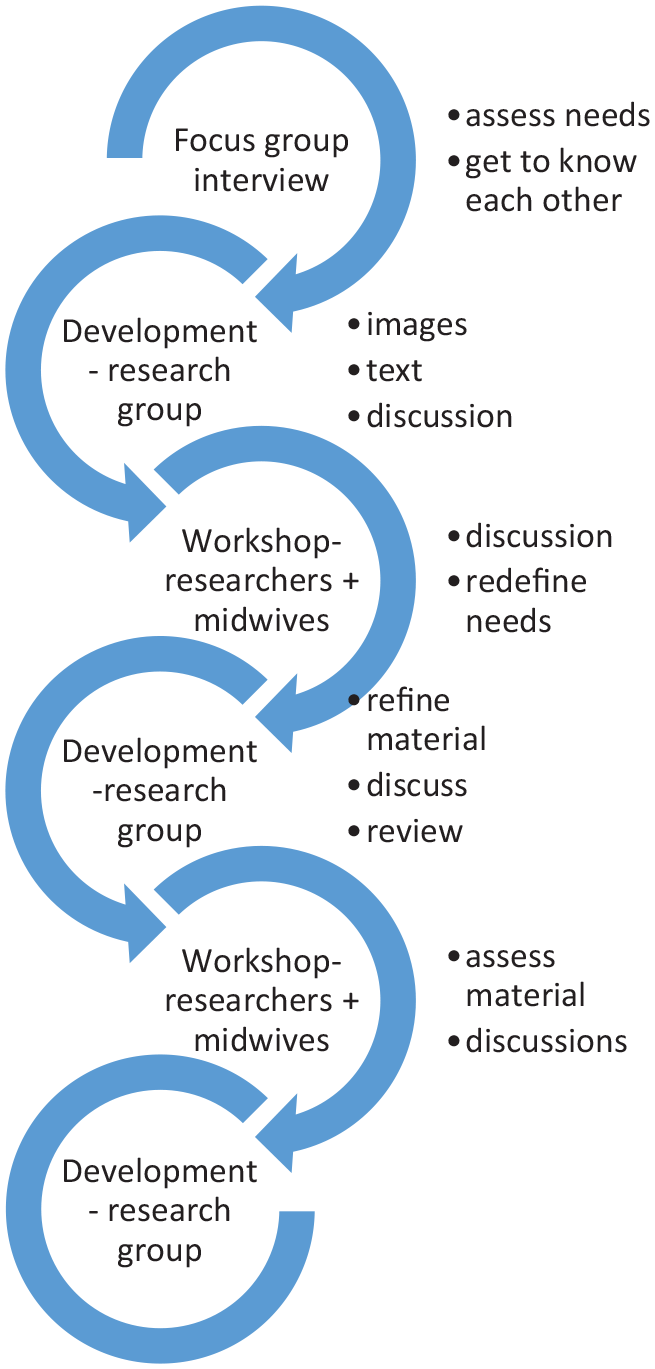
An iterative, cyclical approach.
Multi-disciplinary approach
A multi-disciplinary research team was formed to encompass a wide range of perspectives. It comprised three Swedish language specialists to guarantee linguistic clarity and accuracy in communication, one midwifery researcher and one Arabic-speaking midwife to guarantee evidence-based and reliable health content, and a health informatics researcher to address user-needs and usability. The team acted as intermediaries between end-users and software developers.
Participants
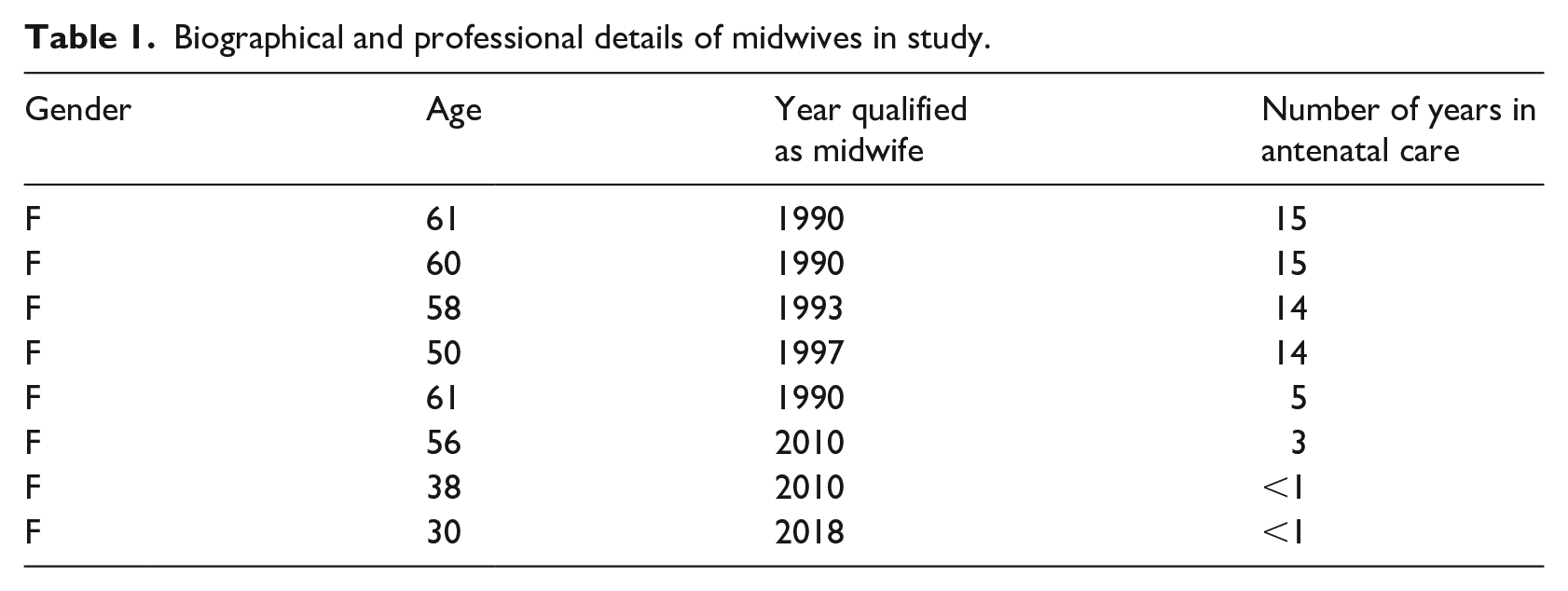
Potential end-users of the proposed app were selected by convenience sampling. To begin with, four midwives were recruited, two of whom had participated in the pilot study and all of whom practised midwifery in ANC. As interest for the project increased, a further four midwives joined the participant group (Table 1). In Sweden, ‘midwife’ is a protected professional title. Midwifery education is an 18-month university education after a 3-year nursing education. Midwives have autonomous responsibility for care during pregnancy, childbirth and the postpartum period for uncomplicated pregnancies. Complicated cases are managed with an obstetrician. Midwives are also responsible for most contraceptive counselling.
Biographical and professional details of midwives in study.
Setting
The study took place in the south-east of Sweden. The midwives were employed at regional antenatal clinics in six municipalities that included both urban and rural settings.
Ethical considerations
To protect the confidentiality of the midwives and their clients, ethical approval was sought and granted from the Regional Ethical Review Board, Linköping, Sweden (Dnr 2017/166-31).
Procedure
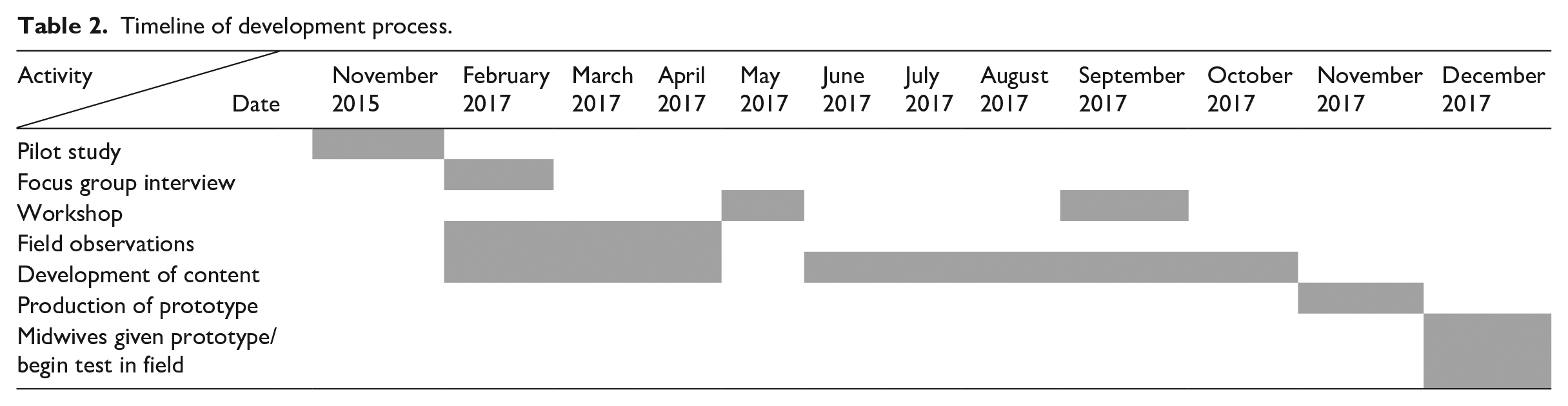
Berg 20 recommends acquiring empirical knowledge in two ways: involve end-users and utilise qualitative research methods. Eight potential end-users took part in the project and three qualitative data collection methods were used to elicit essential information: (A) one focus group interview, (B) four sessions of field observations and (C, D) two workshops. The methods and results of parts A to D are presented below to demonstrate the sociotechnical/iterative process of this research, how we sequentially developed the content of the app by collecting information from the potential users, developed material in the research team and returned to the potential users to discuss progress. This continued as a cyclical process until the material was ready to be sent to the software developers for production of the prototype. Table 2 provides an overview of the development process.
Timeline of development process.
Focus group interview (FGI)
A focus group interview was held initially so that midwives could freely express their ideas and needs. The interview was held at the university in February 2017 and aimed to assess midwives’ needs and responsibilities, and gain an understanding of the type of information and communication midwives exchange with pregnant women during their ANC. The interview was combined with an introductory meeting so that the midwives could meet the research team and enable the team to build trustful relationships with the midwives.
Data collection and analysis
There were four participants, that is, the midwives recruited at this stage of the project. They were invited to respond to the following general questions:
‘Describe your work situation today with regard to non-Swedish speaking women’.
‘What information would you like to see included in a proposed app?’
‘What do you consider to be the most important information that should be included in an app?’
The interview lasted 2 h and 30 min, and was digitally recorded. The interview data were transcribed. Two researchers examined the data and organised it into categories. The categories were: unplanned meetings, giving information and collecting information.
Results
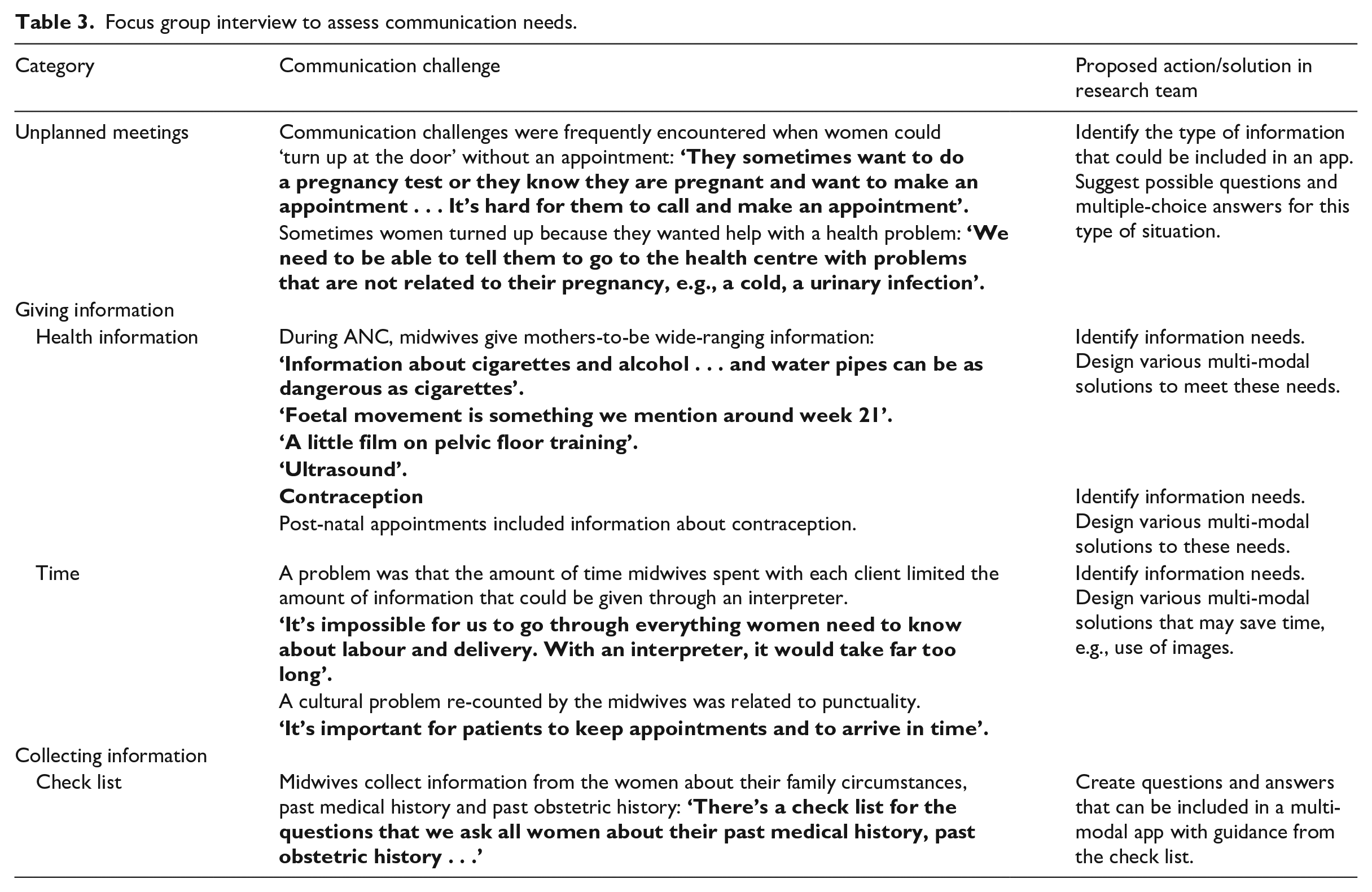
The results are presented in Table 3. Categories are in Column 1. Examples of communication challenges as described by the midwives are given for each of the identified categories in Column 2. Actions and solutions for developing the app were discussed by the research team and are presented in Column 3.
Focus group interview to assess communication needs.
Synopsis of proposed content
The proposed app would have two key functions: giving information and collecting information.
Giving information:
an introduction to ANC,
tests carried out during pregnancy,
advice on lifestyle such as nutrition and exercise,
and later in the pregnancy, information about labour and delivery.
Collecting information:
deal with unplanned visits,
biographical details,
past medical histories,
past obstetric histories.
In summary, the focus group interview provided an understanding of the midwives’ requirements and created a good rapport between the research group and the midwives. Furthermore, the midwives provided a copy of the overall plan they use for routine ANC. In Sweden, women meet a midwife 8–9 times during pregnancy. Each routine visit included giving specific information. This was known as the ‘basic programme’ and covered all aspects of ANC as well as a post-natal visit. The focus group interview provided the information needed to begin developing content for the proposed app.
Field study observations
To augment the information obtained at the focus group interview, we carried out a series of field study observations in two ANC clinics. The aim of the field studies was to define the challenges to communication that midwives and ASW encounter by observing midwives meeting clients at all stages of pregnancy and during post-natal visits. Four field studies were made during which eight individual meetings were observed.
Data collection and analysis
After gaining consent from the clients, the researcher adopted the role of non-participating observer. 23 Data were gathered by writing field notes. These were analysed by the research team and communication challenges were identified.
Results
The results are presented with examples from the field study notes:
Meetings in which interpreters were employed were allowed an extra 15 min. Generally, there was a good flow of information through the telephone interpreter – from midwife to interpreter to client and from client to interpreter to midwife. However, sometimes meetings were cut short due to lack of time.
There were some instances when the interpreter appeared to misunderstand questions and the woman would seem confused. For instance, ‘the midwife spoke one short sentence and the interpreter asked her to repeat it. Then the interpreter gave a relatively long translation’ (Field study 1). This might indicate that the interpreter did not have the appropriate words for translation and instead would give a long explanation. Consequently, the midwife was unsure whether the correct information had been relayed.
Another example was that ‘the midwife had to ask the woman through the interpreter to give the date of the first day of her last menstrual period. The interpreter hesitated and found this difficult to explain’ (Field study 2). The date of the last menstrual period is very important for planning ANC.
‘A husband who accompanied his wife to the clinic had been in Sweden for seven years and could speak Swedish quite well. Despite a telephone interpreter being present, the husband helped with quite a lot of translation or even answered for his wife’ (Field study 4). This implied that the midwife sometimes did not have direct communication with her client.
Reflections
Field observations allowed the team to gain knowledge on how conversations proceeded when interpreters were engaged and highlighted some issues experienced by midwives and their clients whilst using an interpreter. For example, interpretation may not always be accurate which could lead to misunderstandings. If a husband was involved, clients could be excluded from the conversation, thus, women might be empowered by an app that would allow them to answer questions directly and not be dependent on an interpreter or a husband. Hence, field observations gave the research team insight into cultural and language issues and in-depth knowledge to be considered when developing the app.
Development following FGI and field observations
Each researcher worked on a specific category of content. Images and scripts were created. Images were key to development with the view that ‘a picture paints a thousand words’. By using carefully-selected images, the spoken script could be kept relatively short. The research group met frequently to thrash out the content, exchange ideas and review progress. Drafts were produced in both Swedish and Arabic. When a draft of the content for the ‘giving information’ part was ready, the first workshop was arranged.
Workshops
At workshops, midwives were shown the app content that had been developed thus far. They provided feedback on the content and discussed developments with the researchers.
Workshop 1. May 2017
Four midwives and two researchers attended the workshop which lasted 3 h. The midwives were shown the proposed content for the ‘giving information’ part of the app and gave their feedback and opinions. The material for the ‘giving information’ section had been developed to provide a series of images, headings and a script to describe all aspects of the information that were routinely provided by the midwives. Firstly, the Swedish version of the script to accompany the images was read by the midwives. They could check the script for content and accuracy. Then they listened to a test recording of script to each of the images in a Swedish version. It was also played in Arabic to demonstrate what the clients would see and hear.
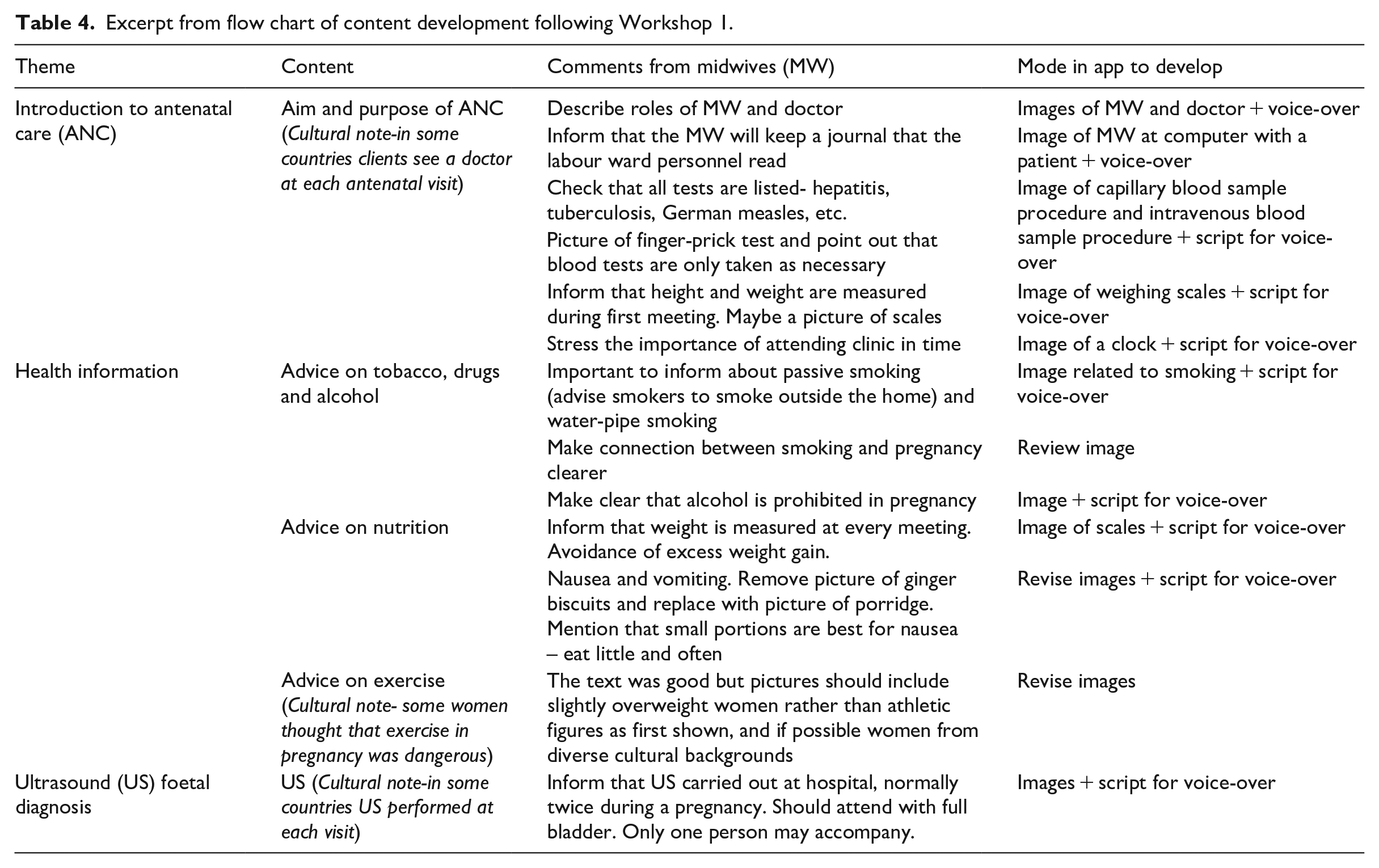
The iterative process ensured that necessary next steps took place during the development process by discussing comments from the midwives in depth. For example, midwives considered that some of the backgrounds in the images looked too clinical. There was a detailed discussion about the information they gave regarding nutrition and smoking. Cultural issues were also mentioned, for example, that some women according to midwives believed it was dangerous to exercise during pregnancy. This kind of information was discussed at length to ensure that both researchers and midwives understood each other. Table 4 shows how comments from midwives informed the next steps in development.
Excerpt from flow chart of content development following Workshop 1.
Researchers then asked the midwives for their views on the ‘collecting information’ section of the app. There was discussion about which questions were routinely asked during antenatal visits and how they could best be supported in collecting this type of information. The midwives provided a copy of a standardised check lists for collecting information on biographical details, past medical histories and past obstetric histories.
Sometimes discussions took place that resulted in midwives reflecting over their own practice. For example, they found that they approached some challenges in communication in different ways and learned from each other, adding a further dimension to discussions. These deliberations helped researchers to gain in-depth understanding of the complexity and requirements of antenatal visits.
Development
The workshop findings were analysed and a list of required modifications were made so that content could be revised and further developed, followed by a period discussion within the research team, revision and further development of content. Some of the images were revised by visiting the actual clinics to take ‘real’ pictures of the premises. Scripts to the images were revised. We endeavoured to create content that was culturally sensitive by selecting images that were diverse. Questions and answers for ‘collecting information’ were drafted. Some questions involved ‘yes/no’ answers while others had multiple choice answers.
Another development area was the issue of how to respond to unplanned visits – when women ‘turned up at the door’ with some kind of problem or question. A battery of possible questions that might help midwives to ascertain the reason that someone had ‘turned up at the door’ with possible answers to their questions was created. The issues ranged from mild, for example, ‘I want to do a pregnancy test/book an appointment’, to serious, for example, ‘I have been bleeding’. The research team continued to meet frequently to discuss and review development and progress. Subsequently, a second workshop was scheduled to examine new and revised material with the midwives, thus continuing the iterative process.
Workshop 2. September 2017
Two researchers held the workshop but unfortunately only one midwife was available. However, the material for both the ‘giving information’ and ‘collecting information’ were closely examined. The next section describes how material evolved through discussion with an experienced potential end-user.
Some questions posed to pregnant mothers are sensitive, for example, in ascertaining how many pregnancies a woman has had.
There was a discussion about ultrasound examination with a midwife indicating that women needed to know:
Regarding ‘collecting information’, the questions we had developed for past medical history and past obstetric history were examined to make sure that all necessary questions were included and that they were asked in an appropriate way. Similar to the previous workshop, there was important feedback when the material was reviewed. In addition to the information received from the midwife, all the material was cross-checked to ensure that it was evidence-based and in agreement with current professional practice.
Development
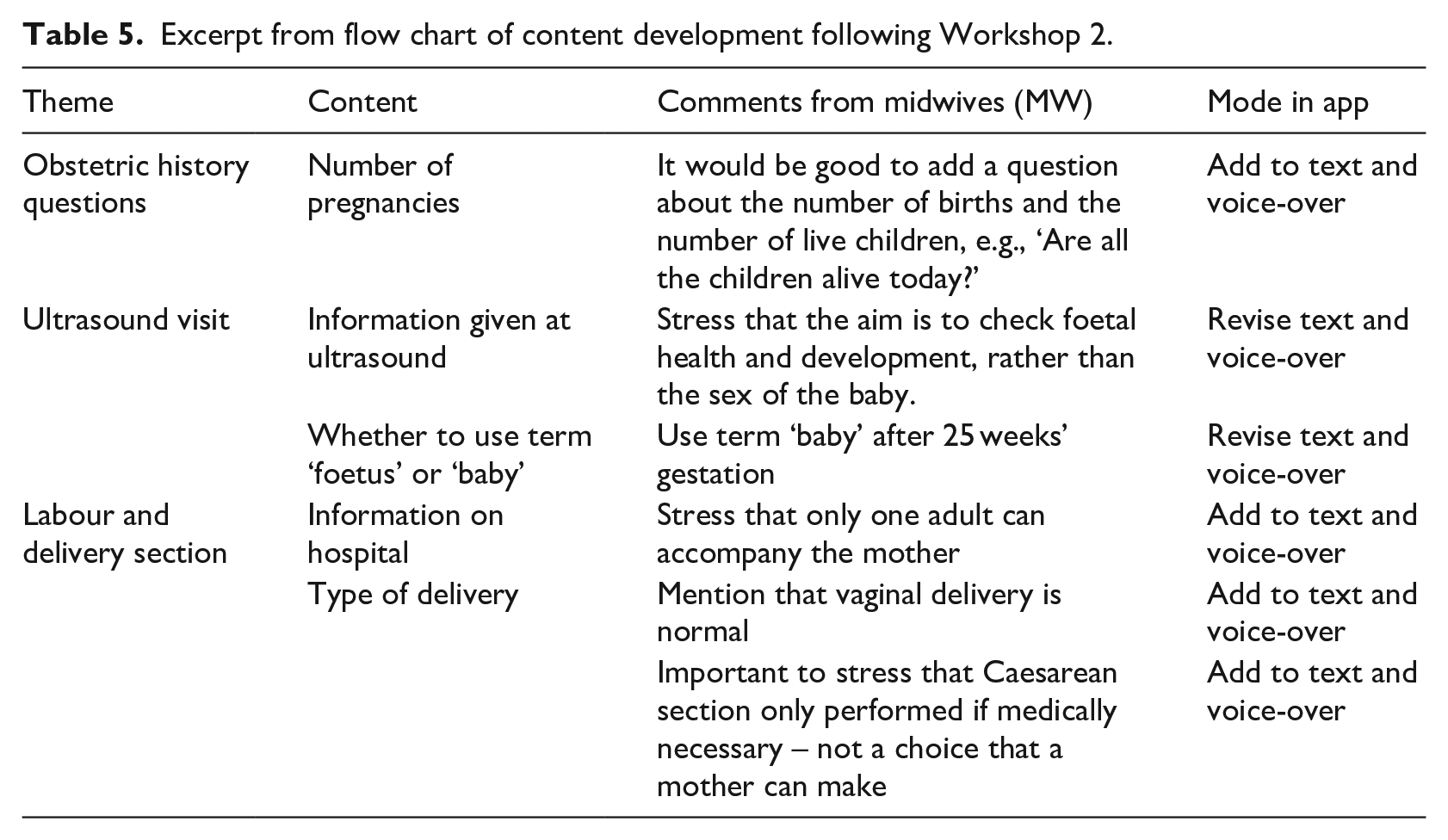
A new list of modifications was devised after analysis of the second workshop (Table 5).
Excerpt from flow chart of content development following Workshop 2.
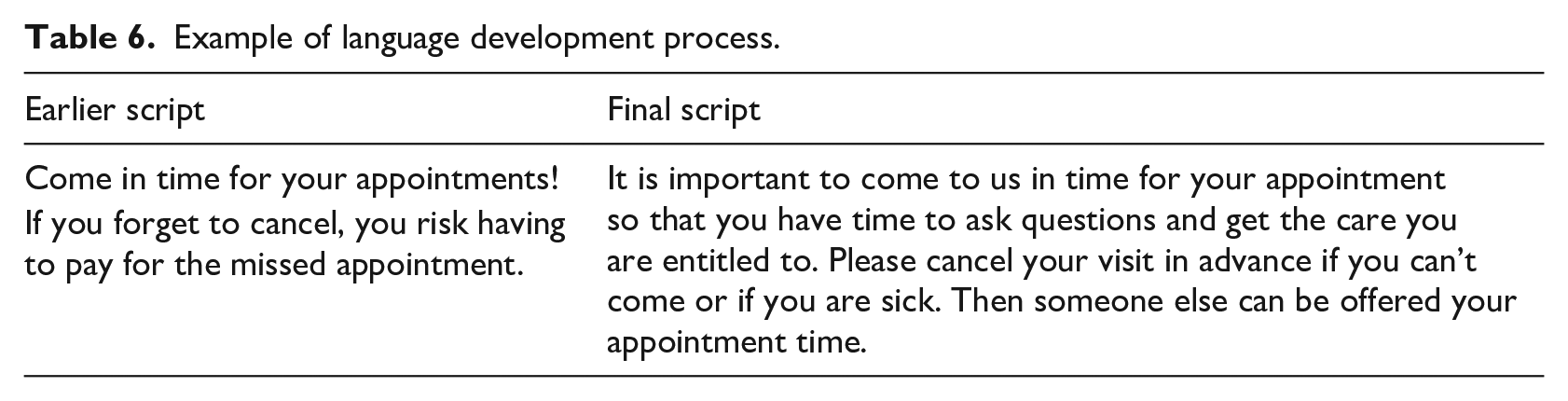
Review and revision of the texts, images and scripts followed. The team met frequently to examine, argue and deliberate over material to make the content increasingly more refined, to maximise good communication and minimise risk of misunderstanding. An example of linguistic refinement can be seen in Table 6.
Example of language development process.
Safety and quality were assured by consistently checking that all content was evidence-based and validated by external experts. Two researchers recorded the scripts in Arabic and Swedish respectively. A detailed organisational chart of all the material to be included in the app was created. This, along with the material and recordings were sent to software developers to create the prototype of the app. This concluded the developmental phase of the prototype of the app.
Discussion
The method described in this article was developed over an 11-month period. The aim of this part of the project was to elicit user needs for interactive communication in ANC and to translate these into specific user requirements to develop and test a multi-modal communication app. The process was guided by three main principles: to involve potential end-users, in this case, midwives; to gain in-depth understanding of work processes in health care;20,22 to ensure safety and quality by developing an app based on evidence. 15
Involve end-users
An initial focus group interview provided basic information about midwives’ needs. This meant that end-users were involved from the beginning and provided the starting point for developing useable content. 19 The iterative approach ensured that proposed content could be reviewed by midwives and allow the team to develop material in tandem with potential end-users. This guaranteed that the information in the app was meaningful and accurate. 16 Furthermore, the development process examined what midwives actually do in practice so that the systems can function optimally. 13 By involving clinicians, it conforms to the notion and that an app should have a specific purpose and the possibility to empower end-users. 14
Understanding work processes
Observational studies can promote understanding of complex situations through the observation of actions and activities. 24 Thus, concurrent field observations enhanced understanding of the benefits of, and barriers to interpretation during antenatal meetings, providing in-depth knowledge of how an app should function to be of real benefit to midwives and their clients. 14 For instance, specific issues that proved difficult for an interpreter were analysed and app development for these issues could focus on making the images descriptive and the language accessible. In addition, combining workshops and observations enabled the research team to become familiar with the work processes of midwives and led to understanding specific content that would be useful in the app.
Quality and safety
There is a plethora of health apps available on the current market but concerns have been raised about lack of quality and the absence of evidence-based content.25,26 Conversely, the method used in the development of this app ensured that those involved had sufficient medical training, that clinicians were consulted and that there was awareness of patient safety. 15 Workshops gave the opportunity for the material to be examined and discussed with the midwives and provided an open forum for dialogue to help deepen and expand the accuracy of the content from an evidence-based perspective. Problems were identified and discussed at length so that an in-depth understanding of the complexity of ANC could be reached. How to ask culturally and emotionally sensitive questions was discussed so that empathetic solutions could be attained. Moreover, this project complies with guidelines from the Swedish Standards Institute, 27 which states that data provided in an app should be reliable and based on evidence so that users can trust the information.
Crucial to this research was the diversity of the research team with expertise in language, communication, midwifery and eHealth, meaning that all content was reviewed from a wide range of perspectives. The team acted as intermediaries between end-users and production giving this research a refreshing approach that facilitated the smooth transition of user-needs to the design and development of a purpose-made app.
A strength of this project was its user-centred methodological approach. The requirements of the app were grown through close collaboration between potential end-users and the research team. The information in the app is evidence-based and thus is reliable and safe with an ‘appropriate level of rigour’.26,27
The limitations of this study are that only eight active midwives took part in a single region of Sweden and additional opinions may have been obtained if there had been a larger number of participants. This may restrict the generalisability of the data. However, midwives are responsible for following national guidelines when providing maternity care and therefore we believe the content would not have varied greatly with a larger group.
Testing
By December 2017 the prototype was ready to be tested. Two of the researchers met with the participants to demonstrate the functions in the app and distribute an iPad to each of the eight midwives. Midwives were instructed to use the app as desired to assist in communication with ASW. The prototype of the app was tested in the field by the midwives. Members of the research team met with the midwives periodically to continue the cyclical iterative process of development. Details of this process will be published in a future report.
Conclusion
The qualitative methods used in this research have promoted the development of a user-friendly, evidence-based, fit-for-purpose app. Involving midwives has guaranteed that content was designed to meet specific user-needs in practice. The app is expected to improve and ensure the quality of ANC for ASW and promote healthy pregnancies. There is a strong possibility that this app will be adopted and used by midwives as it will help them to guarantee that their clients have been given the correct information. This work adds to the knowledge base on how evidence-based apps can be developed. Moreover, it is intended that the app will include additional languages in the future.
Footnotes
Ethical considerations
To protect the confidentiality of the midwives and their clients, ethical approval was sought and granted from the Regional Ethical Review Board, Linköping, Sweden (Dnr 2017/166-31).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.