
Abstract
We present a pilot study to investigate the impact of introducing a hospital-specific smartphone application into a cohort of British junior doctors. We created the iPhone application ‘iTreat’ that contained disease management and antibiotic dosing guidelines specific to our hospital, together with a postgraduate education department really simple syndication feed, a contact number phonebook and a favourites section. This intervention was trialled in a group of 39 foundation grade junior doctors, in a UK hospital, for a time period of 4 months. Mixed methods data capture, utilising survey and semi-structured interviews, was used to evaluate application usage patterns and potential barriers to endorsement of smartphone technology in the hospital setting. Sixty eight per cent of participants felt the application saved them time during clinical activities, with a decrease in the frequency of participants not referring to hospital clinical guidelines. The findings from this pilot study point towards the internal hospital environment as having a major impact upon smartphone usage. Participants viewed smartphone use as unprofessional in the ward-based setting, with a perceived negative attitude from other healthcare staff. An understanding of how healthcare staff choose to utilise smartphones in the clinical environment is crucial to enable the successful assimilation of smartphone technology into the hospital setting. This pilot study provides experience and parameters for future substantive studies being carried out by this group.
Introduction
As modern healthcare systems seek to fully integrate Information Computer Technology (ICT) into hospital settings, the smartphone is an obvious tool to utilise. Over 80 per cent of British doctors own a smartphone, 1 with the popularity of such a device not surprising owing to its ability to combine mobile phone features together with handheld computer capability. In the hospital setting, smartphones have the potential to offer many benefits; delivered by medically relevant smartphone software applications (apps) that provide evidence-based medicine at point of care. 2 Recent evidence demonstrates high levels of clinical use of smartphone apps, both in British 3 and American 4 doctor populations.
The ability to create customised apps provides hospitals with the opportunity to streamline how clinicians access both disease management and patient clinical data. Apps linked directly to the hospital allow clinicians to access patient clinical data, such as patient notes or laboratory test results.5,6 The above-mentioned benefits relate to the level of integration the smartphone has within the hospital system. One step down in the level of hospital integration are hospital-specific apps, where hospitals create apps specific to their individual guidelines, published openly and available to all clinicians via the relevant app store. A select few UK hospitals choose this strategy, commonly providing quick-reference apps such as drug dosing aids.7,8 Non-hospital-specific smartphone apps have also been shown to be of benefit to clinicians, when provided in personal digital assistant (PDA) format. 9 Apps used in this context are developed by third party authors and available for download via the app store associated with the smartphone manufacturer. These are commonly disease diagnosis, drug reference and medical calculator apps, 2 representing the majority of medical apps downloaded by clinicians.
We aimed to conduct a pilot study to investigate the impact of a hospital-specific smartphone app upon the working activities of junior doctors in a UK hospital environment and to discover app usage patterns and potential barriers to endorsement of smartphone technology in the hospital setting, with the view to implementing this strategy in our organisation and undertaking a subsequent substantive study.
Method
App design
The app (iTreat) was developed using Xcode SDK (Apple) software, specifically for the iOS iPhone platform. iTreat contained clinical data from the Hospital Trust intranet system, broadly divided into Antibiotic Formulary and Disease Management Protocol categories. All data within the app had been created and reviewed by the Trust and approved for distribution among its staff. The authors wrote no new clinical material. Data was pre-loaded onto the app to negate the need for in-hospital Wi-Fi or 3G connectivity. The app also included a really simple syndication (RSS) feed from the hospital Postgraduate Education department, a ‘Favourites’ section and a ‘Contacts’ extension number phonebook (Figure 1).
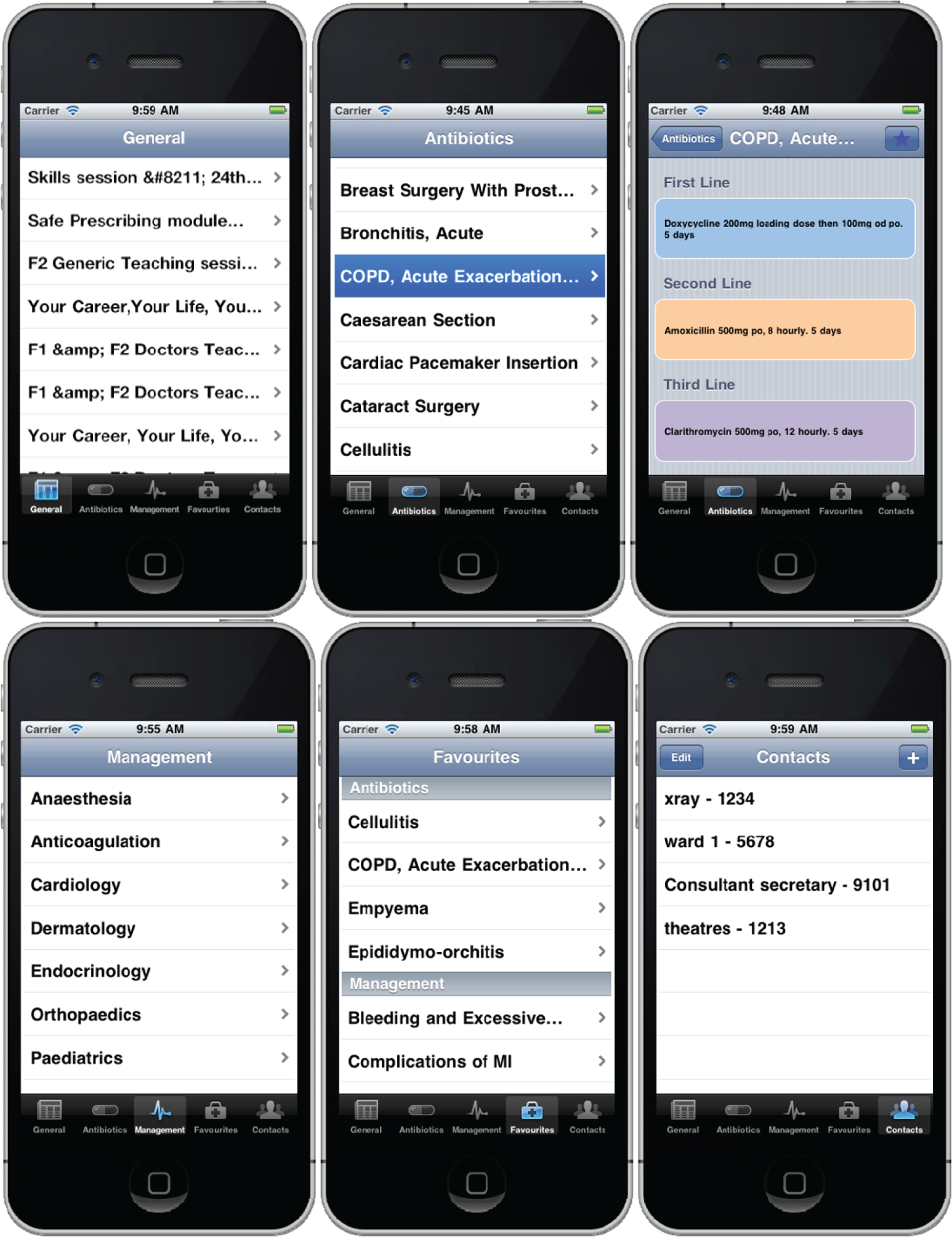
Screen shots of the iTreat app being viewed on an iPhone. Screen shot taken of each app section as shown by highlighted bottom row tab button.
The app was made available for download via the Apple App Store, with a passcode entry system embedded into the app to prevent persons not enrolled onto the study from accessing the app and its clinical data.
Pre-study data capture
During a mandatory teaching session, foundation level junior doctors were approached to participate in the study; those owning an iPhone or iPod Touch were eligible. Those who enrolled gave consent and were asked to fill out a paper-based pre-study questionnaire (Appendix 1). The questionnaire was constructed by the lead researcher and was reviewed by an expert panel for content validity and reliability. Questions were derived and adapted from previous literature3,10 and explored the authors’ personal experience and that of other informants (see acknowledgements section). The study was performed across two separate hospital sites within an East Midlands (UK) National Health Service (NHS) Trust.
Post-study data capture
The study was active for 4 months, after which time the app was removed from the App Store and participants asked to stop using the app and delete it from their device. Participants were contacted at mandatory teaching sessions or individually, to complete a post-study questionnaire (Appendix 2). Nine willing participants attended semi-structured interviews to further explore their experience of using the app.
Data analysis and ethical approval
In line with current opinion, quantitative pilot data underwent descriptive analysis only. 11 Interview transcript data were initially coded and organised into key themes by the lead author, then verified by the co-authors to support rigour of analysis, trustworthiness and reliability in the interpretation of the data. 12 Quotations illustrating the key themes were later selected and used alongside literature evidence to illustrate the key issues. Ethical approval for this study was granted by the East Midlands NHS Research Ethics Committee (reference: 11/EM/0278).
Results
Pre-study survey
Thirty-nine foundation doctors enrolled in the study, with a female-to-male split of 53.8 per cent (n = 21/39) and 46.2 per cent (n = 18/39), respectively, and a mean age of 24.6 years (range of 23–29). In all, 19 doctors were on a medical attachment, 13 on a surgical attachment, 3 on an anaesthetics attachment, with 2 being within general practice and 2 doctors on an ‘other’ attachment.
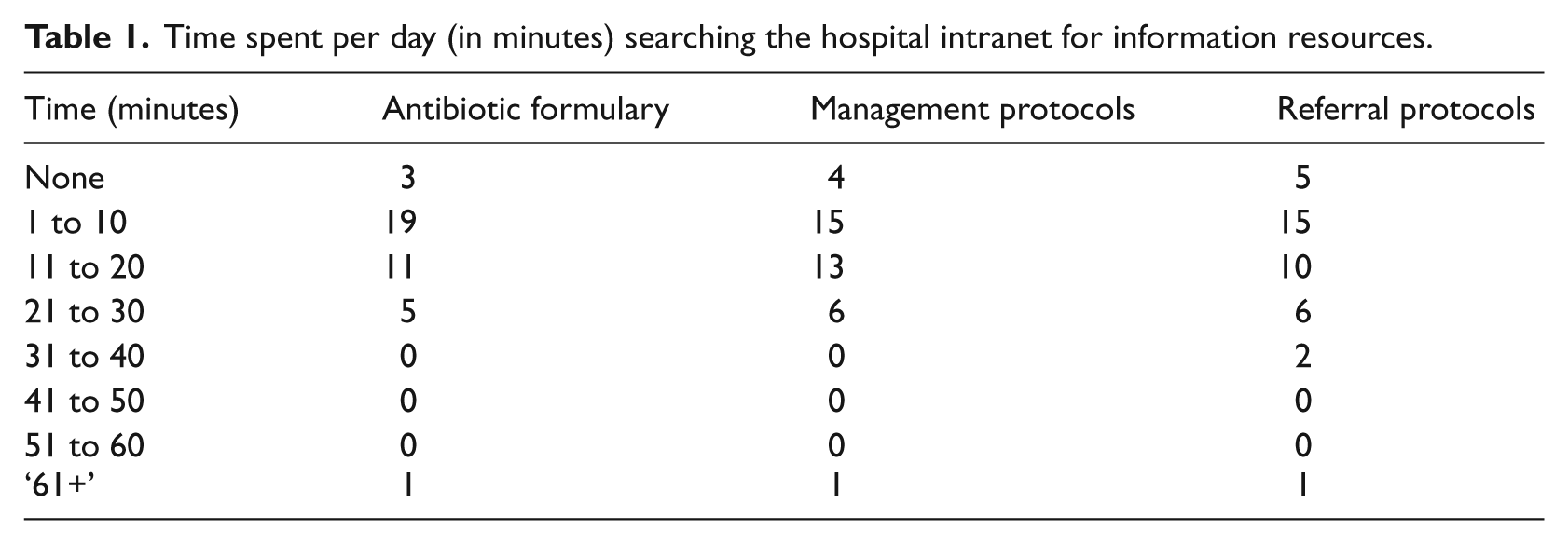
The time participants spent per day, in minutes, searching the existing (non-smartphone or non-app mediate) hospital intranet for antibiotic, clinical management and referral protocols is shown in Table 1. Of the participants, 25.6 per cent (n = 10/39) stated that time spent accessing information resources on the intranet had a ‘moderate’ negative impact upon the quality of patient care they could provide, 5.1 per cent (2) described a ‘major’ negative impact upon patient care, 30.8 per cent (12) and 12.8 per cent (5) described a ‘minor’ and ‘no’ negative impact upon patient care, respectively, with 25.6 per cent (10) stating ‘neutral’ feelings. Nineteen participants (48.7%) were satisfied with the current hospital intranet system, and 20 participants (51.3%) reported being not satisfied with the current system.
Time spent per day (in minutes) searching the hospital intranet for information resources.
Regarding baseline smartphone habits of study participants, 76.9 per cent (n = 30/39) of participants already owned medical apps on their iPhone, with the remainder of participants not owning medical apps. Of those participants who owned medical apps, 6.7 per cent (n = 2/30) used medical apps ‘always’, 20.0 per cent (6) used medical apps ‘often’, 40.0 per cent (12) used medical apps ‘sometimes’, with 23.3 per cent (7) and 10.0 per cent (3) using medical apps ‘rarely’ and ‘never’, respectively.
Post-study survey
Thirty-one participants completed the post-study survey, with eight participants unable to be contacted.
Impact upon working activities
Of the participants, 67.7 per cent (n = 21/31) reported the perception that the app saved time compared to previous experience. Time spent per day, in minutes, accessing app sections is shown in Table 2. Of the participants, 6.5 per cent (n = 2/31) reported a ‘major’ increase in frequency of referring to trust protocols, 16.1 per cent (5) reported a ‘moderate’ increase in frequency, and 51.6 per cent (16) reported a ‘minor’ increase in frequency, with 25.8 per cent (8) reporting ‘no’ increase in frequency of referring to trust protocols. Figure 2 compares pre- and post-data of the frequency of making clinical decisions without referring to hospital protocols, when this may have been necessary.
Time spent per day (in minutes) using each app section.
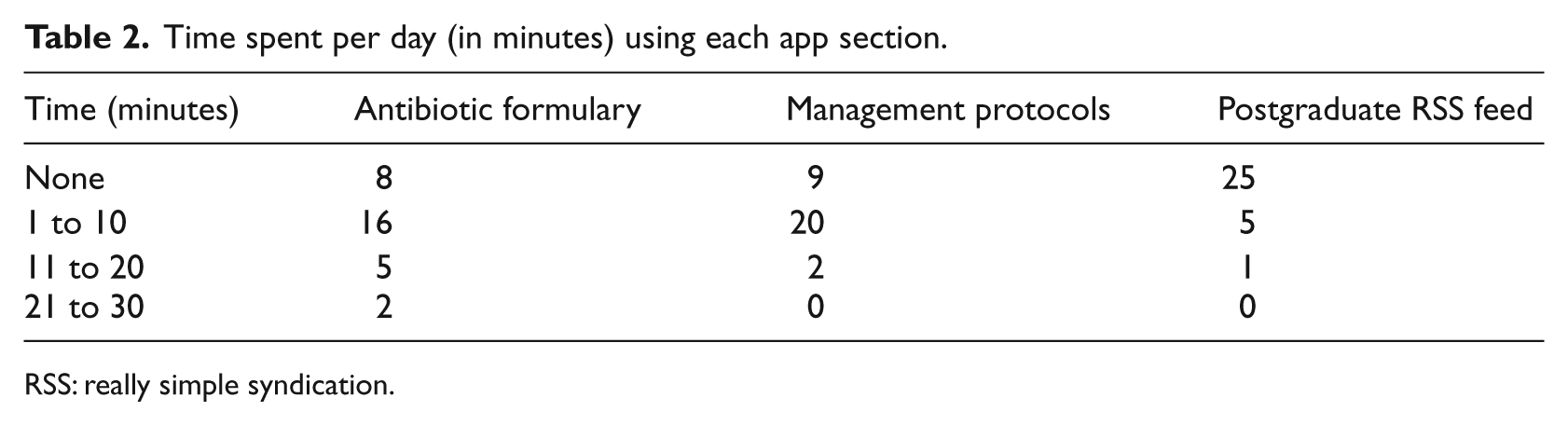
RSS: really simple syndication.
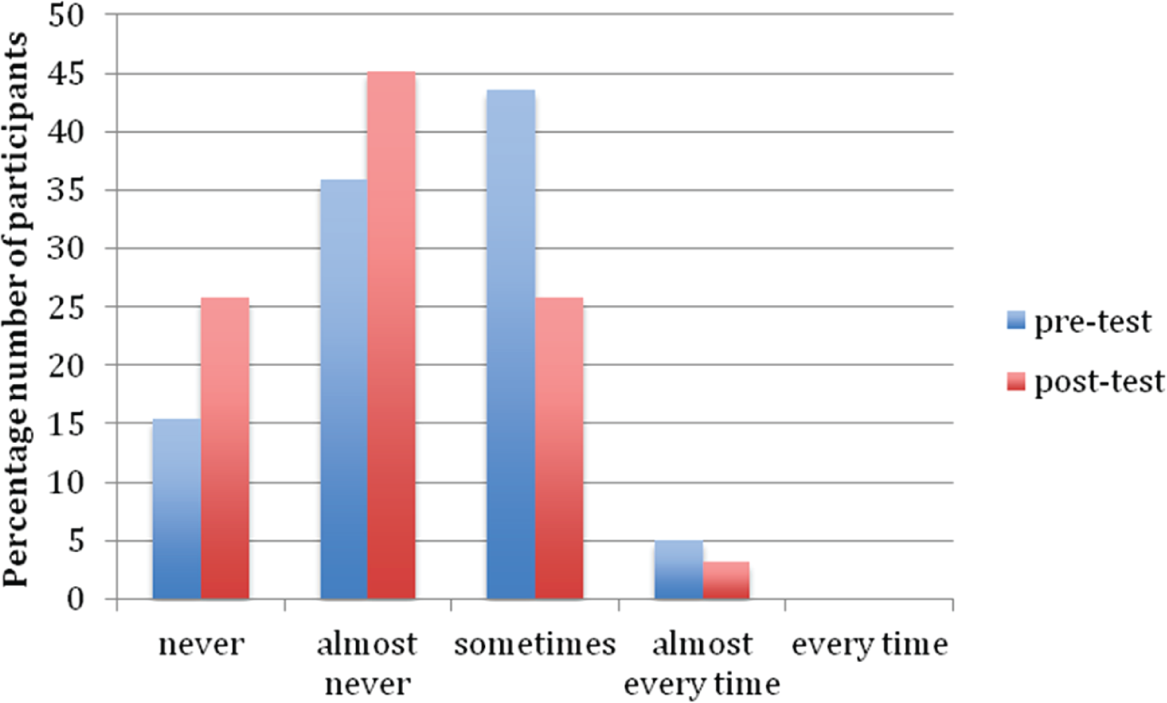
Comparison of pre- and post-data of the frequency junior doctors made clinical decisions without referring to hospital protocols, when necessary (data displayed as a percentage of total cohort for comparison purposes).
Of the participants, 38.7 per cent (n = 12/31) viewed the app as having a ‘moderate’ positive impact upon patient care, 6.5 per cent (2) described a ‘major’ positive impact, 22.6 per cent (7) remained neutral, with 19.4 per cent (6) and 12.9 per cent (4) stating a ‘minor’ or ‘no’ positive impact upon patient care, respectively. Regarding the impact of the RSS feed upon communication between the postgraduate education department and participants, 54.8 per cent (n = 17/31) reported ‘no’ impact, 12.9 per cent (4) reported a ‘minor’ impact, with 29.0 per cent (9) and 3.2 per cent (1) reporting a ‘neutral’ and ‘moderate’ impact, respectively.
App functionality
Of the participants, 54.8 per cent (n = 17/31) and 22.6 per cent (7) felt the app was ‘easy’ and ‘very easy’ to use, respectively, with 16.1 per cent (5) being ‘unsure’ and 6.5 per cent (2) finding the app ‘difficult’ to use. A total of 51.6 per cent (16) thought app aesthetics were ‘good’, with 16.1 per cent (5) and 9.7 per cent (3) describing app aesthetics as ‘very good’ and ‘excellent’, respectively, with 16.1 per cent (5) and 6.5 per cent (2) stating ‘fair’ and ‘poor’ app aesthetics, respectively. Usefulness of each app section is displayed in Figure 3. In all, 51.6 per cent (16) reported a ‘good’ overall experience of using the app, and 29.0 per cent (9) reported a ‘fair’ experience, with 12.9 per cent (4) and 6.5 per cent (2) reporting ‘very good’ and ‘excellent’ experiences, respectively.
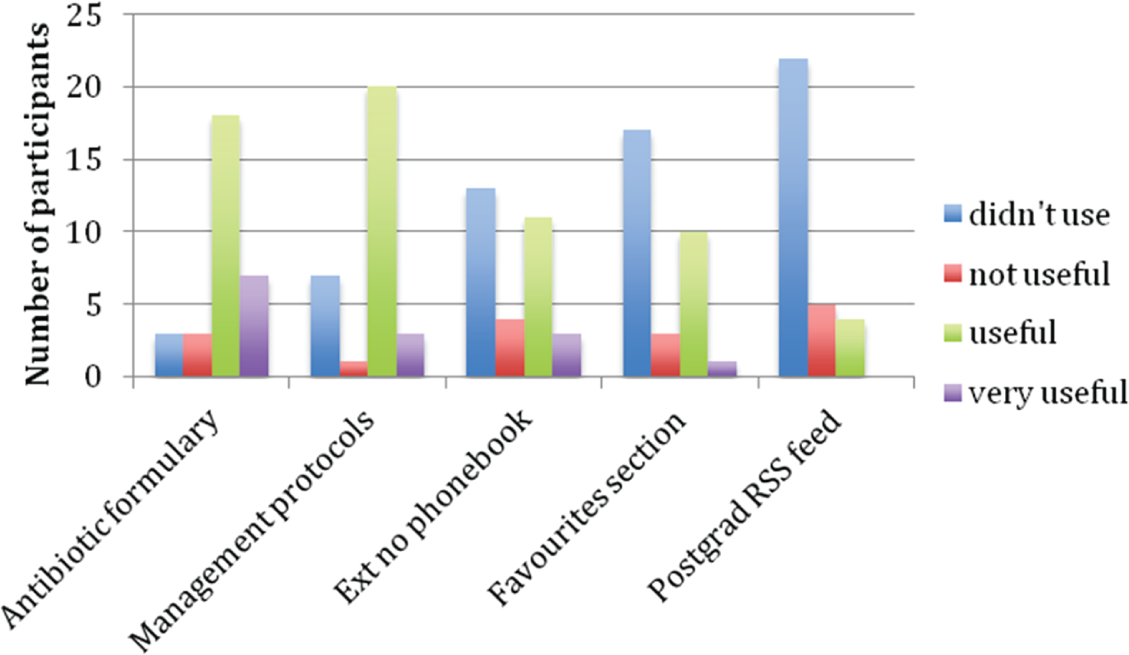
How useful participants found each section of the app.
Interview analysis
Interview questions were directed towards three categories of investigation: barriers to smartphone use, where and when the app was used, and factors for future app success. Analysis of interview transcripts revealed key themes grouped into one of the above three categories (Box 1). Interview quotations for each key theme are provided in Box 2.
Key interview themes, grouped into three predetermined categories.
Unprofessionalism – uncomfortable using smartphone in front of senior colleagues,other hospital staff and patients
Technical concerns – preferring to view information resources on a large screendesktop computer and unconfident that app content was accurate
Ward desk setting – not used in front of patients and used as secondary point of reference if computer is not available
Time-pressurised environment – used in acute care setting (emergency department) and while on-call for quick-reference drug dosing
Education and publicity – inform patients, hospital staff and notably, senior colleaguesof clinical purpose of smartphone use
Integration of smartphone within hospital ICT system – culture change within hospitals to endorse smartphones and be able to view patient clinical data
Interview quotations relating to each theme.
I feel it looks bad and unprofessional playing on your phone even if you explain its often a bit long-winded explaining why you have your phone out so it is easier not to do
I feel a bit inappropriate using a mobile phone in front of patients even though itwould be for clinical reasons, but they wouldn’t know that so I feel I would have to explain to them that I wasn’t texting or phoning someone
I think its hard to tell if you are using your phone for professional or personalreasons, there is no way to tell if you are using it to send a text message or using it to look up guidelines
I would look things up on the computer as it is easier on a big screen and sitting down
I didn’t use it in front of patients, I used it at the desk while the computer is busyotherwise I would prefer to use the computer
I used it for prescribing if I was on-call and didn’t have access to a computer andwanted to search quickly on my phone
Pretty much all the doctors in A&E (emergency department) use their phones to do guideline searches and calculations
If you have the app in acute situations where you don’t need to leave the patientbedside that’s really useful
If it was publicised that smartphone apps were being used for clinical work thatwould help
I don’t think patients would be opposed to it as long as you let them know what youare doing
I think it’s a really good idea if the culture is going to change on wards where ourphone is a recognised diagnostic tool, and we can take them out and use them
Barriers to smartphone use
Barriers to smartphone use are separated into two main categories: belief that other healthcare staff perceived smartphone use as negative and physical preference relating to viewing information and smartphone use.
The perception of other clinicians viewing smartphone use as unprofessional was a recurring theme to all interviews. For junior doctors, the concern of negative opinion from senior colleagues outweighed that of other ward-based hospital staff. This theme also related to smartphone use in front of patients. Central to the above was the reasoning that staff and patients applied to smartphone use; doctors felt that observers, especially patients, would view smartphone use as being for personal reasons and not clinical use.
Several interviewees noted a preference to view information resources on a large screen, when compared to the smaller smartphone screen. Other smartphone technical barriers included a lack of confidence that all data was up-to-date, and the simple fact that not everyone carried a smartphone in the workplace.
Where and when the app was used
The above-mentioned barriers appeared to translate directly to where in the clinical area the smartphone was used. Feeling uncomfortable using their smartphone in front of patients, and in the ‘open ward’ visible to other staff, doctors subsequently preferred to be seated at a ward desk to access the app. Combined with the preference for a large viewing screen, once at a ward desk, the progression was to use a desktop computer to access information resources. As such, it was noted by several interviewees that the app became a secondary point of reference, used if computers were not free.
In contrast to the above, app use was noted to be directly beneficial in time-pressurised situations, notably acute care settings such as the emergency department, and while undertaking busy on-call shifts. In these settings, using the app for quick reference, most often for antibiotic dosing information, was preferable to taking the time to sit down at a desk and access a computer.
Strategies for future app success
When questioned about strategies for future app success, opinion related to two areas: education of patients and senior colleagues/hospital staff, and further integration of smartphones within hospital ICT systems.
Interviewees felt that if patients and senior colleagues were aware of why they were using smartphones, then this would go some way in increasing smartphone use. Notably, junior doctors wanted support from senior colleagues, stating that they were not comfortable with the need to explain why they were using their phone and subsequently, avoided using it. They viewed this as being part of the need for hospitals to fully integrate smartphones into their ICT system, to be able to view patient clinical data via an app and thus make smartphone use commonplace. Opinion was that this change in ICT strategy would provoke a change in smartphone culture in clinical areas, with subsequent publicity by the hospital to educate patients.
Discussion
This article aims to discuss smartphone technology and its impact upon the clinical activities of junior doctors. This pilot study was primarily conducted to investigate the factors relating to launching a hospital-specific app and the parameters for a further substantive study. However, the strengths of this project lie in the ability to evaluate the benefit of providing all types of hospital-specific clinical guidelines in an app format; something not previously investigated in a UK hospital setting. Within the United Kingdom, most hospitals construct their own clinical guidelines and antibiotic formularies, often differing between hospital sites; for a junior doctor rotating between hospitals every 4 to 12 months, this represents an avenue of possible confusion and clinical error.
I have the BNF already on my iPhone and this is great for telling me drug dosing and I use it a lot, but if I want to know what the hospital wants me to prescribe first line for a chest infection I still need to check the hospital guidelines. This is why I thought the app was useful.
Although a small cohort pilot study, there appears to be a trend that iTreat produced an increase in frequency of doctors referring to hospital clinical guidelines, with a decrease in doctors not referring to clinical guidelines (when necessary) because of difficulties accessing this information (Figure 2). Furthermore, the majority of doctors perceived iTreat as having a positive impact upon patient care. While not empirical data, the benefit of this should not be underestimated. Any intervention to increase the confidence of newly qualified junior doctors, save time and foster an attitude of referring to evidence-based guidelines should translate to an overall increase in patient safety. This falls in line with recently released UK Department of Health guidelines that place ‘improved patient outcomes, safety & experience’ at the core of their framework for technology-enhanced learning. 13
Based on the reported success of other hospital smartphone interventions, 5 we had expected a greater overall positive impact of introducing iTreat into our hospital environment. While it was encouraging to note that 68 per cent (21) of doctors reported that the app saved them time during clinical activities, there were still 26 per cent (8) who either didn’t use or found the two main sections of the app (antibiotics and clinical management) not useful. In a comparable project, providing UK undergraduate medical students with a resource-loaded PDA, the MoMed project reported a similar ‘non-use’ rate of 24 per cent. 14
To analyse this ‘non-use’ further, we consulted the external variables (termed ‘innovation factors’) proposed by Putzer and Park 15 as influencing a clinician’s attitude and subsequent behavioural intention to use a smartphone. They described the variables of compatibility, observability, job relevance, personal demographics, personal experience, internal environment and external environment as all being significant. Examining how the above-mentioned innovation factors potentially influenced the iTreat project, our findings point towards the internal environment (hospital organisation and support) as being the most pertinent smartphone innovation factor in a UK junior doctor cohort. The perception that other staff and patients viewed smartphone use as unprofessional, while some evidence states to the contrary, 16 appeared to have a profound impact upon smartphone use. These findings are further echoed by the MoMed project and other smartphone qualitative studies. 17
Compatibility of the smartphone in the hospital environment was perceived to be variable and highly dependent upon the clinical setting. In a review by Prgomet et al. 18 of mobile handheld technology and its impact upon hospital physicians’ clinical activity, the benefit of mobile technology to ‘facilitate rapid response’, especially in acute care and emergency situations, was noted. Similarly, doctors within our study noted a preference to use iTreat in time-pressurised environments, for example, while covering a busy on-call shift or in the emergency department. However, in contrast to the above-mentioned emergency ‘point-of-care assistance’, in the ward setting, there was a preference to use the app seated at a desk, away from patients, and subsequently, doctors preferred to then use the desktop computer already present. In this way, the negative perception of smartphone use in front of patients appeared to alter the subsequent behaviour associated with app use.
It should be noted that doctors found the smartphone app format both useful and easy to use, with 71 per cent (22) reporting a positive overall experience of using the app. Regardless of the smartphone platform used, this method of utilising a clinicians’ personal smartphone, when compared to similar projects providing doctors with resource-loaded PDAs, 9 has the potential to negate many of the previously quoted organisational barriers relating to cost and technical concerns. 19 What our study adds to the literature is further evidence for hospitals and other healthcare organisations of the benefit of utilising smartphone technology, even if the app is not fully hospital linked and integrated into the ICT system.
Limitations
It should be stated that our project was a pilot study only, with our small sample size noted as a limitation. Our study cohort represents only one group of junior staff, and the extent to which our data can be extrapolated to senior clinicians and the impact of this upon further work is unknown. Furthermore, potential smartphone innovation factors relating to ‘demographics’ and ‘previous experience’ are somewhat skewed towards the positive. Younger doctors are likely to be more technologically savvy, while doctors within our cohort by definition all owned smartphones, with 77 per cent (30/39) already owning medical apps and the majority using these often during working activities. This prior experience may represent an area of bias if applying our findings as relevant to all junior doctor groups.
Conclusion
The gold standard for integrating smartphone technology into the hospital environment is a hospital-linked app, displaying up-to-date hospital guidelines and providing real-time access to patient clinical data. While shown to be successful in several countries,5,6 this approach requires a considerable investment in monetary and ICT resources, 19 with additional data security concerns. 19 Our approach of a hospital-specific app meets this standard half way. We provide evidence that such a concept has the potential to save time, increases reference to clinical guidelines and is acceptable and user-friendly to junior doctors. As the integration of smartphones into the hospital continues to grow in popularity, organisations are forced to consider the potential barriers and strategies that relate to the planning and success of adopting this approach.
Several lessons have been learnt from this pilot study, to carry forward to future research. Factors within the internal hospital environment appear to adversely impact smartphone uptake, notably, the negative perception from doctors that patients and other healthcare staff view smartphone use as unprofessional. This will impact strategies to fully integrate smartphone technology into the hospital setting within future studies. Therefore, we propose that education of patients and hospital staff is vital to encourage clinicians and further foster a culture change of handheld technology being viewed as a clinical tool in the hospital environment.
Footnotes
Appendix 1
Appendix 2
Acknowledgements
We acknowledge the help of Jo Cooper, Kim Watts and Heather Wharrad in the early stages of study protocol and questionnaire design.
Funding
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.