
Abstract
Reminiscence therapy is beneficial for improving the quality of life for older adults living with dementia. However, it is difficult for caregivers in care homes to make this part of their daily practice because remembering a resident’s individual stories is difficult. Proximity-aware technologies can make rapid connections between residents, their histories, and nearby artefacts. Through a user-centred iterative design approach, we designed Memento, a prototype technology system that makes it easy and convenient for caregivers to connect residents with real stories from their past and engage them in meaningful conversations. Memento displays connections between a resident’s stories and their surroundings on a caregiver smartphone. Caregivers can then subtly use this information to start spontaneous reminiscences with residents, as they go about their everyday activities. Remembering their histories was highly enjoyable for residents, giving them a renewed sense of self-confidence and well-being.
Keywords
When people living with dementia move from their own home into a care home, they find themselves in a world filled with new spaces, new people, and new processes - this can be very confusing for them. The quality of life for older adults drops dramatically when they move into residential care homes, 1 which can also lead to an increased risk of mortality. 2 This reduction in personal belongings, personal freedom, and mobility, coupled with the tendency of care homes to focus on the physical health care of their residents, results in limited daily stimulation of cognitive abilities of residents with dementia. 3
With an ageing world population, there will be an increase in the prevalence of age-related health problems such as dementia, 4 increasing the number of older adults needing to live in residential aged care homes. Enacting reminiscence therapy as part of people’s everyday activities has been proven to add enjoyable experiences for people with dementia in care homes. 5 Reminiscence therapy (RT) is a well-known and widely used non-pharmaceutical method, used to stimulate positive intact memories of a person and involve them in conversations about these memories. It is easy to find things to reminisce about when living at home surrounded by artefacts gathered over their lifetime, or talking with people who know your history. However, spontaneous meaningful conversations are more challenging for those living in care homes. It has been shown that caregiver conversations with people who are living with dementia tend to be very brief during personal care tasks and often the interactions that take place are not very satisfying. 6 This is partly since caregivers in aged care homes cannot easily remember the history of the many individuals in their care because they each deal with multiple residents, do shift work, change jobs relatively frequently, and might work across several different care facilities. This indicates an opportunity for technology to improve this situation since advances in personal devices, sensor technologies, and tangible computing offer new possibilities to support reminiscence and communication for people with dementia. Since the use of technology is not widespread in care practice, Huldgren et al. 7 suggest that more research is needed to advance this approach.
Ageing and dementia are important focus areas for health informatics, interaction design, and human-computer interaction. 8 User-centred iterative design of digital systems ensures they are tailored to the people and places they will benefit, 9 and therefore benefits the design of supportive and enabling technologies. Emerging personal proximity-aware technologies such as smartwatches and smartphones represent an opportunity to design interventions that assist human memory by making substantial amounts of information available when and where it is needed. This technology can be designed to seamlessly integrate into everyday activities, enabling caregivers to help people with dementia access their personal memories and past competencies in a way that is natural, spontaneous, and part of their daily lives.
The Memento system was designed to explore and understand how technology can improve the quality of life for care home residents with dementia by facilitating spontaneous reminiscence therapy during everyday interactions. Memento senses nearby residents and artefacts, makes connections between the resident and documented stories from their past, and sends a story “hint” to the caregiver’s smartwatch. With a subtle glance at their watch, the caregiver can draw the resident into reminiscing, linking their stories to nearby artefacts as conversational prompts.
A key benefit of Memento is that increasing or changing the residents allocated to a caregiver does not affect the quality of interactions with each resident. The design is therefore scalable. It would benefit both residents and caregivers in many different situations - from small to large residential homes with either agency, independent, or in-house caregivers. It could also support people with dementia in their own homes, where agency and independent caregivers may not be familiar with their histories. Additionally, Memento is a relatively low-cost solution, using simple, affordable, everyday technologies in a configuration that supports the initiation of meaningful conversations and interactions between caregivers and residents at any time and in any place.
In this paper, we report on the user-centred design of Memento and present the promising outcomes from a case study of the use of the system in “a day in the life” of a caregiver at an aged care home. Based on this, we confirm the ability to conduct spontaneous reminiscence therapy using Memento, as part of everyday activities in a care home, showing that conversations around memories, linked to nearby artefacts, gives the aged care resident an increased sense of well-being and feelings of confidence through remembering their past.
Background
Reminiscence therapy for dementia
Dementia affects cognition and memory such that abstract concepts and recent events tend to escape people with dementia. 10 They may not remember what happened yesterday or know the present time and place. Cognitively they may forget the names of people and things they used to know well, and they may have difficulties in engaging in meaningful conversations. People with dementia often experience this as a daily challenge; they are constantly reminded about things they used to know well but now have faded away. Some react with irritability and apathy, some withdraw from social interactions. 11 While dementia heavily affects short-term memory, parts of long-term memory often stay intact. In particular, there are usually vast amounts of intact childhood and early adulthood memories. 12 Memories constitute a vital part of the sense of personal identity of any person. 13 Impaired cognition and inability to remember recent events are not the same as a loss of abilities. Skills and abilities may still be there but are harder to access. 14 If these memories can be triggered by seeing or hearing things, or through conversation, a person with dementia can experience a renewed feeling of participation, confidence, and self-esteem. 15
Dementia is affecting a growing number of people. It is mainly seen with older people but the syndrome is not necessarily a normal part of ageing. The World Health Organization reported in September 2019 that around 50 million people worldwide are living with dementia with nearly 10 million new cases every year. 4 WHO also reports that the estimated proportion of the general population aged 60 and over with dementia is between 5-8%. The number of people with dementia is increasing, projected to be 82 million in 2030, and 152 million by 2050. 16
Currently, there is no cure for dementia and so existing treatments focus on improving the quality of life of people with dementia as well as alleviating behavioural and psychological symptoms of dementia (BPSD). Alleviating BPSD in the early stages, when people are still very aware of their losses, can improve their quality of life significantly. 11 Among these treatments are non-pharmaceutical methods used in daily care to increase the quality of life and reinforce cognitive and functional abilities. Music has been used successfully in daily care to alleviate BPSD through ambient music or caregivers who sing during daily care and prompt residents to sing along. 17 Therapists also perform structured music therapy in one-to-one sessions which is helpful for those with impaired language. 18 Video-game-based music therapy delivered by untrained caregivers has also proven to reduce behavioural symptoms. 19 Marte Meo counselling is another non-pharmaceutical method used with people with dementia that improves care by videotaping situations that allow the caregiver to get to know the person with dementia. 20
People with dementia have life histories, personalities, knowledge, and experience. They have “past competencies and failures” 21 [p.973] to share and through sharing, can “value their lives and achievements…and to have those feelings validated” 22 [p.354]. When people with dementia remember past competencies, they gain an increased sense of personal identity and self-esteem.13,15 A controlled experiment by Gonzalez et al. 23 shows support for the effectiveness of reminiscence in alleviating BPSD and improving happiness, self-acceptance, positive relations with others, autonomy, and mastery of their environment. A systematic review by Woods et al. 12 reported that RT is both highly rated by its users and has indications of improved functional ability, mood, and cognition after therapy sessions. Woods et al. showed that improvements in quality of life, cognition, and communication through RT are more strongly indicated in people with dementia in care homes, than those living in the community, and particularly, when conducted on an individual level, rather than in group therapy settings. RT is particularly relevant for residents in care homes who are in the early stages of dementia as it may slow down the progression to later stages. 23
Memory triggers can facilitate people with an advanced stage of dementia to recall past events. Surfacing these triggers in conversations helps them remember and communicate their stories with others. These triggers can include old photo albums, memorabilia, audio tapes/CDs, music, videos, paintings, and familiar views or environments. Activating more than one of the person’s senses can increase the cues that help them to make sense of the reminiscence experience. Therefore, talking about memories is often enhanced by having physical items present that they can look at and touch, providing an additional source of conversational inspiration. 12 These items remind and refocus their attention on what is being discussed.
Much of the responsibility for stimulating conversations in care homes fall to the caregivers, who need to be aware that the person with dementia can feel like they are being tested and need to avoid giving that impression when they initiate conversations. In caring for people with dementia, to be able to enact reminiscences, caregivers must be helped in every way to know about the residents’ histories. To initiate and sustain a conversation about a personal subject with someone with dementia requires detailed information about that person. Even in modestly sized care homes, it is difficult for caregivers to remember details about each resident. In residential care homes, such information is typically stored as personal life stories in a document containing information about childhood, parents and siblings, significant events, former occupation, and the like, for each resident. The life story document is typically created when a person moves into a care home and is stored in paper files or on a central computer. Therefore, RT is generally quite time-consuming and requires planning and organization, 23 and consequently is usually done in planned sessions where the caregiver or occupational therapist has time to prepare, using the life story document of the person or people they are meeting with. However, this research showed that conducting RT spontaneously, rather than in planned or group sessions, has a more positive effect on residents but requires that carers are supported in integrating reminiscences into residents’ daily life as often as opportunities arise. 23
Interactive computer technology in reminiscence therapy
Since RT depends on the recall of memories of events and experiences from peoples’ histories, visual and audio aids can improve its effectiveness. 12 Not surprisingly, interactive digital technologies have proven an effective platform for providing both caregivers and people with dementia with connections between objects in their environment, and residents’ life stories. Some of the specific technologies used to assist people with dementia include: context-aware memory aids; a photo stroller device using photos to engage the user; a music creation system; an interactive multimedia tool for prompting reminiscences; a photo/video sharing system; using 3D virtual worlds to create experiences based on memories have all been used in assisting people with dementia, 24 as well as Augmented Reality and Virtual Reality. 28
Recent research on new care technologies for supporting reminiscence of people with dementia found that tangible multimedia, especially the use of familiar objects, has a high potential to support reciprocal communication. 7 The Digital Life History application 25 is a tablet application used to record life stories. This supports one-to-one reminiscence sessions where a caregiver and a resident share reminiscence using the tablet to access stories. The application also supports the caregiver in learning about a resident’s stories or preparing stories in advance to talk about. SenseCam 26 uses images from residents’ everyday lives for cognitive stimulation therapy (CST). Participants wear a SenseCam camera, taking up to 3000 photos to capture their day, which can be used to help caregivers start conversations about the resident’s day. Tales of I 27 is an interactive ‘art piece’ with a computer inside an old-fashioned television cabinet. It links themes to tangible materials, as well as enabling residents to share personal images and film clips to help individuals reminisce about their past experiences, either alone, or with others. In Tsao et al. 28 integrated virtual and augmented reality in a reminiscence therapy system for providing entertainment and supporting dementia prevention for elderly people through presentation of “nostalgic elements”. Also using Augmented Reality, Morel et al. 29 created Memory Palaces, allowing the construction of a digital model of the residence of a person with early dementia still living at home, to be populated with which photos of family and significant others connected to the physical environment. This can then be used to facilitate “augmented” walks with caregivers or family members through a familiar environment, triggering them to remember their relatives and encouraging them to tell stories from their life.
Opportunities for technology in dementia care
This body of related work indicates the potential for technology to be designed to support one-to-one RT sessions between caregiver and resident that can be enacted at any place and time within the care home environment. It could leverage residents’ personal histories, connecting them to tangible objects in the environment, possibly personal items, and use this information to inspire meaningful conversations around topics of interest to the resident.
The dementia treatments discussed in Reminiscence Therapy For Dementia can all be used in daily care home settings and are non-pharmaceutical but require a special location, additional equipment, or a trained therapist to conduct them. Reminiscence therapy is highly effective, but in care homes with many residents, it requires preparation to know each resident’s history. Additionally, the technology solutions covered in Interactive Computer technology in Reminiscence Therapy tend to require some form of specialised or bespoke equipment that needs to be managed and/or physically interacted with by the person with dementia. This motivates the discovery of a solution that uses everyday non-intrusive technologies, can be undertaken at any time, in any place, and by any caregiver. An ideal solution would not require additional preparation as caregivers already have sufficient duties to keep them busy and with the onus of technology interaction on the caregiver not the care home resident. A solution that can be easily adapted to work both one-on-one and, in a group, would also be desirable in supporting social interactions between residents.
Method
To understand the opportunities for technology to make a positive contribution to the quality of life of care home residents with dementia, we conducted a design case study, where we developed and evaluated a system, Memento, to connect people, artefacts, their stories, and multiple places within a care home. The proximity-aware technologies included a smartwatch, proximity beacons, and a mobile phone supporting caregivers in integrating spontaneous RT into the everyday activities of care home residents with dementia. The method included a user-centred design process 4 ensuring the needs of all potential users of the system are considered throughout the design process, coupled with explorative field visits informing iterative design and innovation prototyping and an evaluative field study to understand the potentials of this design in real-world use.
Memento was developed during a two-year collaboration with Farsøhthus Care Home in Djursland Denmark. The care home has 53 apartments distributed into five sections. Approximately 80% of the residents are living with dementia in differing stages. Each caregiver, during their daily 8-hour shift, is the direct contact person for three to four residents, responsible for keeping track of their appointments, upcoming visits, and their health and well-being.
We were mindful that this research falls within the realm of sensitive human-computer interaction (HCI) design, and therefore, during initial contact with stakeholders, particularly residents of the care home, we worked to build rapport and to be sensitive to the fact that this is both a place of work for the caregivers and a home to the residents, and that some residents may be experiencing emotional issues associated with moving into residential care. 30 While most of the residents were happy to have visitors and enjoyed the new company, we did not want them to feel like test subjects. To reduce the level of intrusion, only one researcher went onsite. The caregivers and the care home manager guided that person on how to behave and accompanied them so that the residents did not experience negative impacts from our research. 31
Design process
Reflective practice
In design studies involving people with dementia, who may have difficulties with verbal communication, it is important to use a reflective approach.
32
To design Memento, we gathered insights from all who would be affected by its use at the care home, to understand current practices and to identify carer needs for a system to support them in enacting spontaneous RT. The overall process of designing Memento is shown in Figure 1. The overall design process used to design Memento.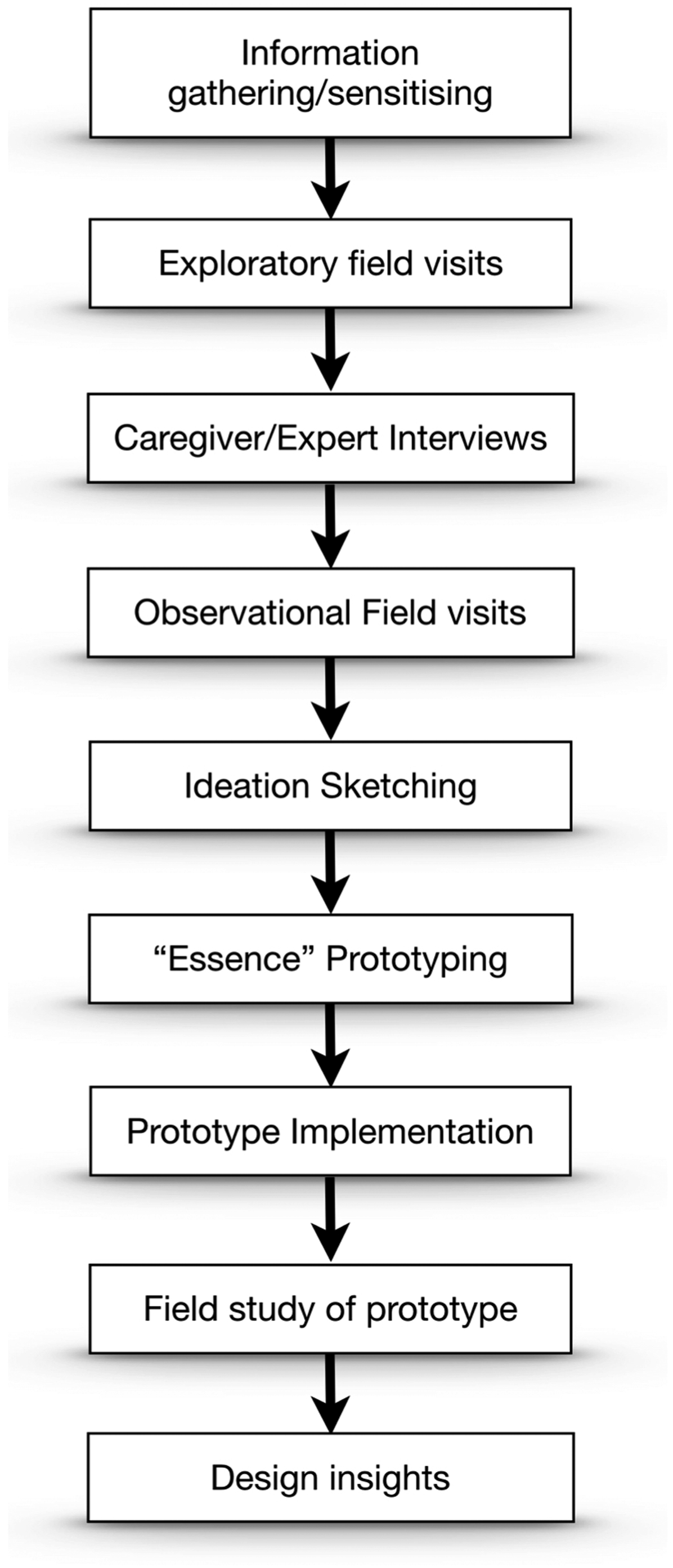
Field Visits
Our initial exploratory field visits were conducted to help us understand the context of use and identify key stakeholders. Expert caregiver/care home manager interviews provided a deeper understanding of the current practice and were used to gather aspirational ideas about improving RT support through digital technology design. We conducted 8 expert semi-structured interviews, of between 30-60 minutes duration with different stakeholders, including the care home manager, a qualified nurse, an occupational therapist, two social work caregivers, two health caregivers, and the IT manager of the care home. Interviews were conducted in Danish. We also conducted three 2-hour unstructured observational field visits, at different times of the day, to familiarise ourselves with the daily activities and experiences of the caregivers and residents at the care home. The semi-structured interviews were audio and video recorded and transcribed in Danish. Field notes were made during and after observations. No formal analysis was conducted at this stage, rather the data collected was used to inspire the design ideation sketching phase. The data was also used to support the innovation prototyping process using the Essence methodology. 33
Field visit findings
Outcomes from the exploratory field visits, expert interviews, and observational field studies gave a good understanding of the current practice and design opportunities for technology to support RT. With a user-centred focus on the needs of both the caregivers and the residents, we gained understanding around current individual and group RT sessions, access to residents’ life stories, memory triggers in the care home environment, and current technology use.
The care home uses spontaneous RT during daily care whenever possible, as caregivers share information about residents with each other, using the life story documents, orally and using calendars. The caregivers are skilled in asking questions without over-stimulating the resident and causing BPSD. Spontaneous reminiscences are typically carried out through spontaneous interactions in common areas of the home, as well as being used to divert an exit-seeking or wandering resident, or one who is externalizing difficult behaviours.
Group RT sessions are facilitated by a professional occupational therapist (OT). Before these sessions, the OT accesses and familiarises themselves with residents’ stories and goes to great lengths to find people with shared interests and identify relevant triggers for upcoming group sessions.
Residents’ life stories are the primary source of information about their pasts. When moving into the care home, the resident and relatives are asked to compose a life story - typically together with a caregiver to help personalise their care. Information is also collected about personal preferences (e.g. music, conversation topics, food). The life story is first written on paper, then stored in a document on the shared staff computer and made accessible to all caregivers and management. Newly discovered information about residents is shared orally during handover between shifts. A day calendar is kept in the staff room with notes on it that are used to pass on new information. Caregivers are responsible for keeping the notes up to date with appointments and important events for each resident. Caregivers can add new information to the computer document that they learn from the resident or their family during visits. However, updating stored information is an ad-hoc process, depending on how busy a caregiver is with other duties.
The care home has many artefacts throughout, including shared artefacts in common areas and personal artefacts in individual residents’ rooms, that they bring with them when they move into the care home. Caregivers are mostly aware of the personal triggers and can refer to them during daily care duties in the resident’s room. However, caregivers often lack the information needed to connect the shared artefacts in the common areas to the life story of the resident they are interacting with, missing an opportunity to enrich their engagement with that resident.
The current generation of residents has limited experience with using digital technologies. The staff was adamant that any technology introduced must not put additional cognitive load on the residents and also must not diminish the natural, familiar and personal aspects of direct interactions between caregivers and residents.
Informing design - the essence methodology
Collected data informed the design of Memento, ensuring it supports spontaneous RT in a way that is non-intrusive, simple, and relevant to both the caregiver and the residents.
Memento was developed by iterating through a series of prototypes. The process was based on the Essence methodology, 33 an experimental software development methodology designed for innovation. Variants of the “seeing-moving-seeing” schema 32 were used in combination with Essence, to gain a greater understanding of the problem. Evaluation of each iteration helped the design team to reflect on the design, facilitating design innovation, discovery in iteration, and reflection in action.
Sensitive design
In considering the role that any introduced technology should play in this context, we identified challenges specific to sensitive HCI design. 30 This included making sure that the design of any technology introduced into the care home environment needs to be approached empathetically 31 while carefully managing any negative impact that its introduction might incur. 34 Digital technologies should afford peace of mind for the residents while providing practical care assistance for the caregivers and easing their workload. 35 It is also important to respond to the preferences and expectations of other stakeholders, such as the care home manager, nurse, and occupational therapist who have a broader view of the context, and the wider implications of adding technology into daily practices. Since the residents have limited experience with using technology, the design had to ensure that direct interaction with technology is done by the caregiver, rather than the resident.
In considering the design of any digital health intervention, it is necessary to give due consideration to how the processes of designing and evaluating the system, might expose vulnerabilities of participants. 30 It is important that resulting designs support users within their current capabilities, and do not make the situation worse. For example, a design should not make it obvious that residents have trouble remembering certain things. To this end, technology interventions need to be discrete. In our case, the use of a smartwatch as the end-user delivery platform means that only the caregiver needs to be aware of the technology support. Caregivers can glance at the watch for history “hints” when prompted by a subtle vibration, without the resident being aware this has happened. Technologies mustn’t be designed in such a way that they are “more disruptive or harmful than the circumstances they are meant to improve” 36 [p.2272]. The caregiver also needs to have agency to make professional judgements on information delivered, and only use them to initiate conversations with nearby residents, in a way that is not harmful or disruptive.
Memento
Memento presents a new use of interactive computer technology in RT through its ability to detect and respond to situational context, offering opportunities for spontaneous meaningful conversations in any place, at any time, during everyday activities in a care home. Our primary design focus was to activate memories of people with dementia and hence instil feelings of confidence and sense of identity in the sharing of those memories with others. This is achieved by enhancing opportunities for spontaneous meaningful conversations between residents and caregivers, rather than relying on prepared and planned group therapy sessions. To support the any-where, any-time model of spontaneous RT, Memento is used in both shared living areas of the care home and residents’ private apartments, rather than in a caregiver’s or therapist’s office. Similar to Memory Palace, 29 this design exploits the richness of human experience, helping residents with dementia leverage their past lived experiences to gain confidence and feeling of competencies in their everyday interactions with others. 37
Proximity-based interaction
Memento uses personal mobile Bluetooth-enabled technologies to provide just-in-time and just-in-place information on the life stories of nearby residents. Memento stands out from previously proposed solutions by providing proximity-based information hints that match a nearby resident’s life story with nearby physical artefacts or views. The system takes advantage of a resident’s ability to remember past life events and harnesses their conversational strengths by engaging their emotional memory through reference to artefacts that have personal relevance. By facilitating meaningful conversational reference to both personal and general artefacts in the resident’s current surroundings, the system eases the burden of remembering individual stories of the many residents for the caregivers, while increasing access to RT for residents.
An important aspect of using a smartwatch as the information delivery platform is the ability to subtly inform the caregiver that an information hint connecting a nearby resident’s history to a nearby artefact is available using gentle vibration. The information hint is displayed on the caregiver’s smartwatch, but they can choose if and how to use this. In this way, the system does not interrupt natural interactions between caregivers and residents but gives an opportunity to enhance them. Information is provided without the caregiver sacrificing eye contact with the resident for more than a few seconds. The other benefit is that it can be delivered to them at their current working location in the care home, where the information prompt is most relevant.
System components
Memento is a three-component tool consisting of a smartphone, a smartwatch, and small transmitters (proximity beacons) already carried by residents and additional beacons attached to specific artefacts throughout the care home. Hence, the system does not know or record the location of residents, or artefacts. It merely reacts on them being nearby the caregiver. The smartphone is kept in the caregiver’s pocket and continuoussly scans for nearby residents and artefacts that can be linked to that resident’s life story. When a resident is nearby, their name, apartment number, and photo are presented on the caregiver’s smartphone. If a nearby artefact is detected that matches keywords in a resident’s life story, an information hint about the particular story is pushed to the caregiver’s smartwatch in an easy-to-read format (Figure 2). A resident’s story displayed on the smartwatch in response to nearby herbs.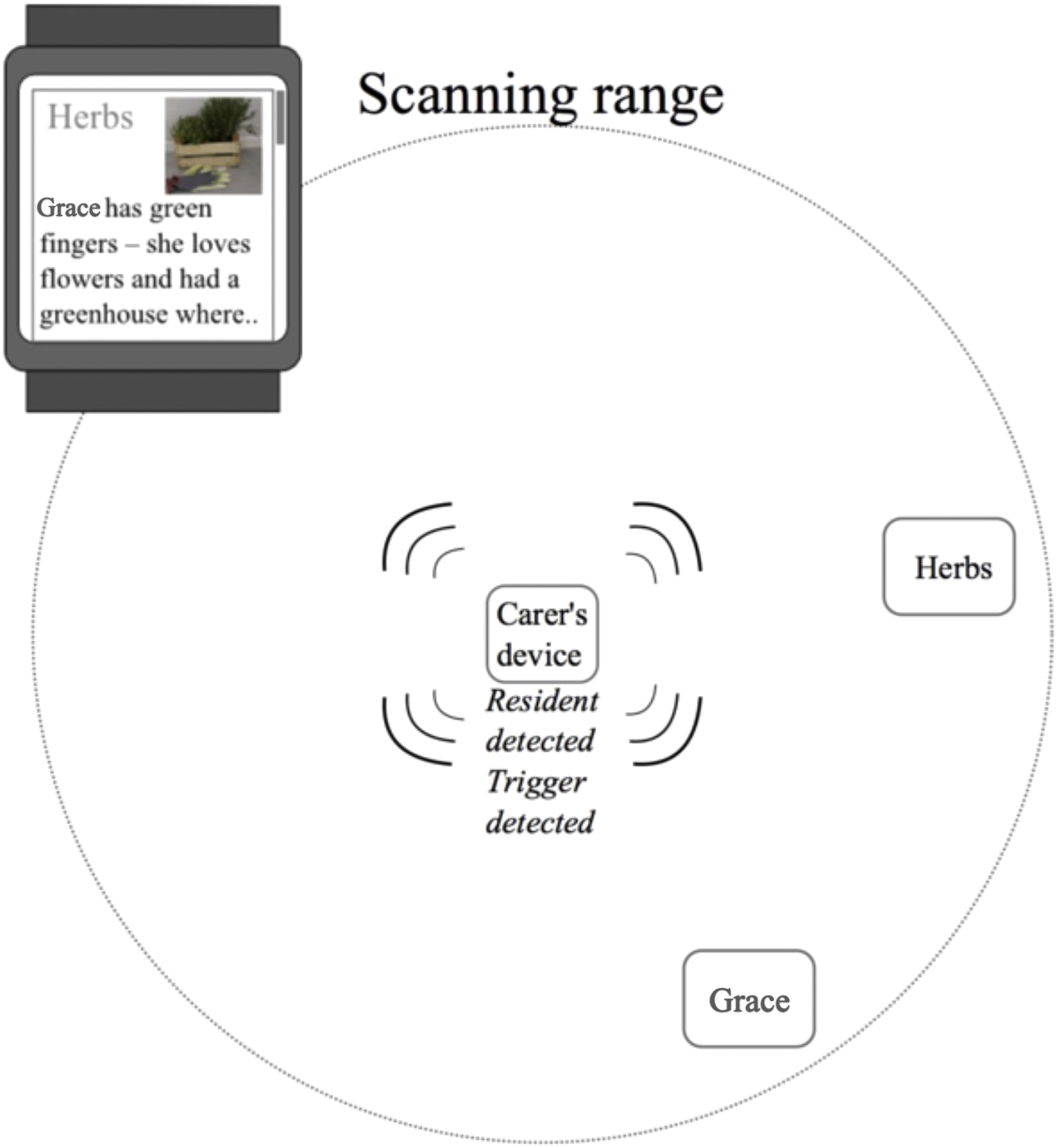
Registration of artefacts involves taking a photo of it, attaching a proximity beacon physically to it, and associating keywords with the signal identifying the beacon. This is done using the smartphone interface. The proximity beacons run on battery, with a life time expectancy of a year or more depending on how often they are used. The application was develop for Android.
In Figure 2, the resident within scanning range is “Grace” and the artefact is a tagged pot of “Herbs”. When Grace and the tagged pot are detected by the smartphone (Carer’s device, in Figure 2), it wirelessly connects to the staff computer to search Grace’s life story database for any reference to herbs, or related keywords. If found, the system sends a vibration alert and a snippet of information about Grace and “herbs” to the caregiver’s smartwatch. In this way, the smartphone can stay in the caregiver’s pocket while subtly pushing information one piece at a time to their smartwatch.
Accessing resident’s stories
The life stories of residents are structured so that relevant hints can easily be extracted. If a resident and one or more tagged artefacts are in proximity, a matching algorithm connects these with life story snippets using keywords. To do this, we designed a simple entry form for the care home, to assist in entering residents’ stories into the database. Existing records were manually translated into the new format. The format uses separate entry fields for different subjects, such as parents, siblings, upbringing, etc., making it possible to give each entry field a set of predefined alternate keywords useful for identifying and associating relevant snippets of a life story. For example, “mum”, “mother”, and the mother’s name can all be used to search for the resident’s mother in their life story text. Related keywords all have the same value in a hash table, increasing the likelihood of matching the description of a subject with other references in the life story. In this way, a match provides all information that relates to the resident’s mother and their experiences with that person. So, if a photograph of the resident’s mother is an identified artefact, and is proximate to the resident and the caregiver, then relevant information hints are pushed to the caregiver’s smartwatch. The caregiver can then engage the resident in a detailed and relevant conversation about their mother.
The iterative design and innovation prototyping process uncovered the usefulness of being able to differentiate between personal artefacts and general artefacts. A personal artefact is specific to an individual and the artefact itself has a story to tell. An example could be a wedding photograph with the information hint send to the smartwatch saying, “Grace and her husband Aksel on their wedding day in 1958. The wedding was in Holbæk on a sunny day”. This provides the caregiver with relevant information for initiating a conversation with Grace about that happy moment in her life. Additionally, the same trigger can be linked to other parts of Grace’s life story, for example, “Grace worked on [a] farm which she owned with her husband, Aksel. Here, she did both practical outdoor work, as well as housekeeping and bookkeeping”. This allows the caregiver to engage in a richer conversation based on a deeper knowledge of Grace’s life. A general artefact is not linked to a particular person. A pot with herbs or a view to a garden may serve as a memory prompt about gardening, and it may be linked to gardening-related information from many residents’ life stories, as well as Grace’s. In this way, general artefacts can be used to facilitate both personal and group conversations, depending on other residents in proximity.
Field evaluation of use
We conducted a field evaluation of Memento in use at the care home to understand how usefully and useably the system integrated into a caregiver’s daily routines. The study was motivated by four questions that we wanted to investigate: 1. Did Memento deliver relevant information hints about nearby residents? 2. How did the caregiver deal with multiple proximate residents and artefacts? 3. Was the information hint useful in facilitating meaningful conversations, leading to reminiscing?
4. Did reminiscing result in the resident remembering past competencies, and increase their well-being and/or self-confidence?
Methodological and ethical considerations
The field evaluation of Memento used the “research in the wild approach” 38 of direct observation of the system in use during everyday activities at the care home. To be sensitive to the study situation, we minimized disruption to daily routines and residents by having a single researcher shadow a caregiver as she interacted with residents under her care while wearing the smartwatch, with the smartphone in her pocket. A resident already carried a proximity beacon, in this case, in her pocket, and we attached proximity beacons to personal artefacts in her apartment, and general artefacts in the common areas. The resident was encouraged to go about her usual day. To respect the comfort and privacy of care home residents, data was collected through observer notes, post-observation reflections, and discrete video recordings of small snippets of intense interaction between caregiver and resident.
In studying health interventions for dementia, interactions with staff and residents require a high level of researcher sensitivity. 39 People with dementia are a vulnerable group, raising ethical dilemmas on how involved they should be in field studies. Where researchers have actively involved people with dementia in their studies, through focus groups and interviews, participants were almost exclusively in the early stages of dementia. 40 Ethical considerations included approval for the planned research from the care home manager, the resident and her family, and the research was planned and undertaken with respect to the intentions of the WMA Declaration of Helsinki, when dealing with research involving human subjects. Since the Danish Care Home houses people with varying stages of dementia, we relied heavily on the expertise of the care home staff as key informants around the needs of people with dementia. Their expertise helped both in the process of designing Memento, and during the observational studies and field evaluation, as they guided us inappropriate behaviours towards residents.
Participants
The field evaluation involved working closely with one resident, Grace, and a caregiver, Anne. At this formative stage of design, we wanted to cause the least disruption possible to normal care home activities. Grace, aged 83, participated in the study with informed consent given by herself and her family, who held power of attorney. She has moderate cognitive decline (or mild dementia) corresponding to early Stage 4 dementia within the Global Deterioration Scale (GDS). This is characterized by, among others, decreased knowledge of current and recent events and some deficit in memory of ones personal history. Anne is an occupational therapist who had limited prior knowledge about Grace at the time of the study. We did not have set tasks but allowed the field evaluation to be a joint exploration of opportunities supported and offered to both caregiver and resident by Memento. Anne participated as part of her everyday care of residents, with Memento helping her to interact with Grace and initiate conversations as she went about doing her normal duties. We chose to focus on the case of a single resident to gain a deep understanding of how Memento supported Grace’s sense of self and to understand if spontaneous reminiscing increased her self-confidence. This is an accepted approach for in-depth investigations into the design of technologies for people with dementia. 27
Field evaluation set up
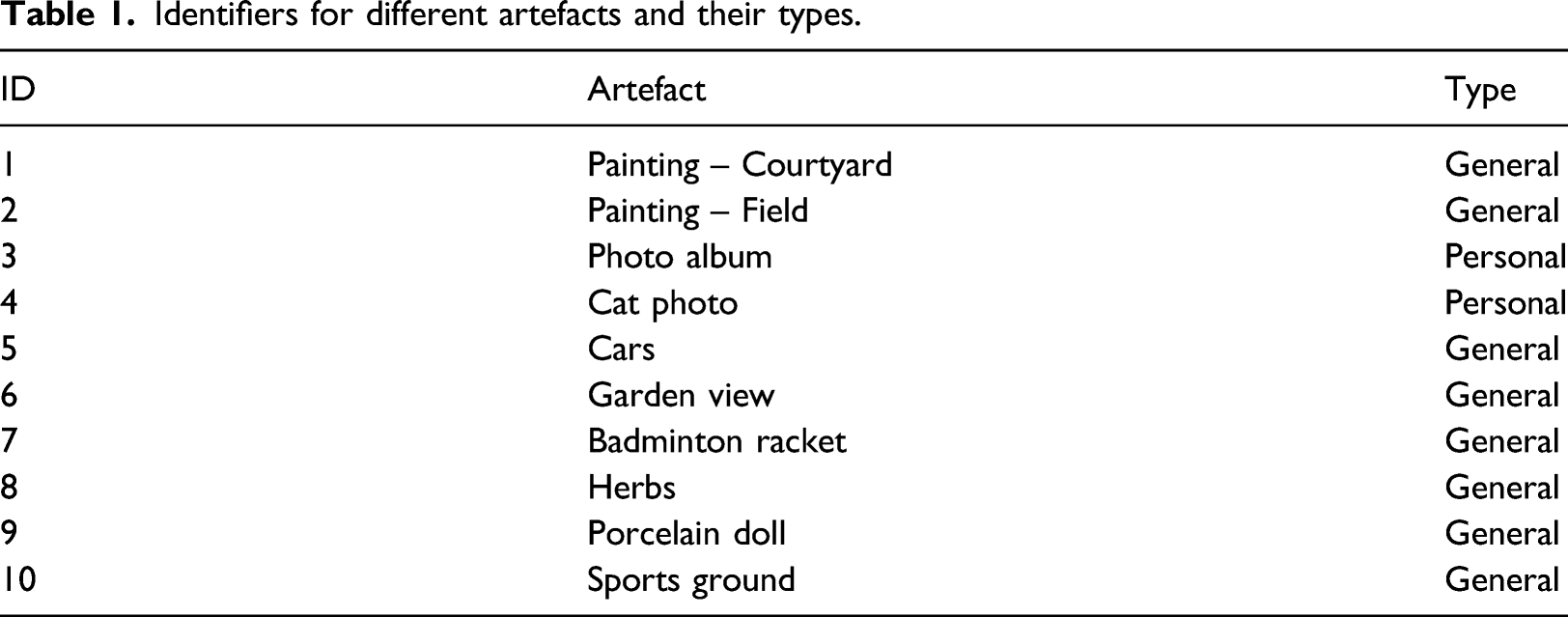
Identifiers for different artefacts and their types.
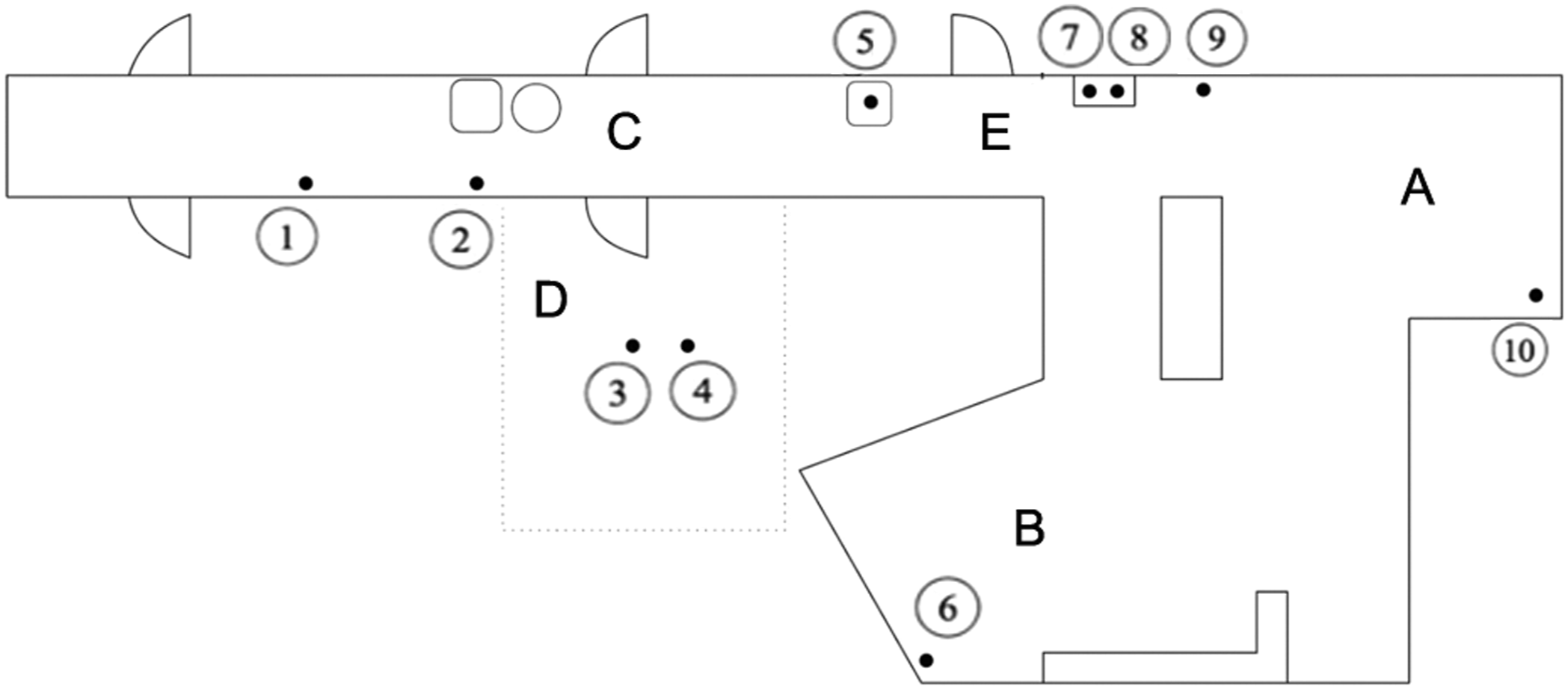
Plan of the care home, showing the location of artefacts (circled numbers refer to Table 1).
The evaluation covered five locations based on Anne’s usual route to check on the well-being of residents. These are marked on the plan of the care home in Figure 3 as: (A) a stairway used to approach the common living area; (B) the common living area; (C) the corridor leading to Grace’s apartment; (D) Grace’s apartment; and (E) the corridor leading into the common living area.
Two fictitious residents were simulated to add extra residents to the evaluation while minimising disturbance for other residents. This was done by placing one beacon under a chair in the common living area (representing Jytte) and another under a chair in the corridor leading to Grace’s apartment (representing Holger). By using fictitious residents, we were able to observe the impact on the caregiver’s attention of simultaneous messages arriving on her smartwatch, concerning multiple proximate residents.
Locations in the care home related to artefact IDs linked to residents’ stories.
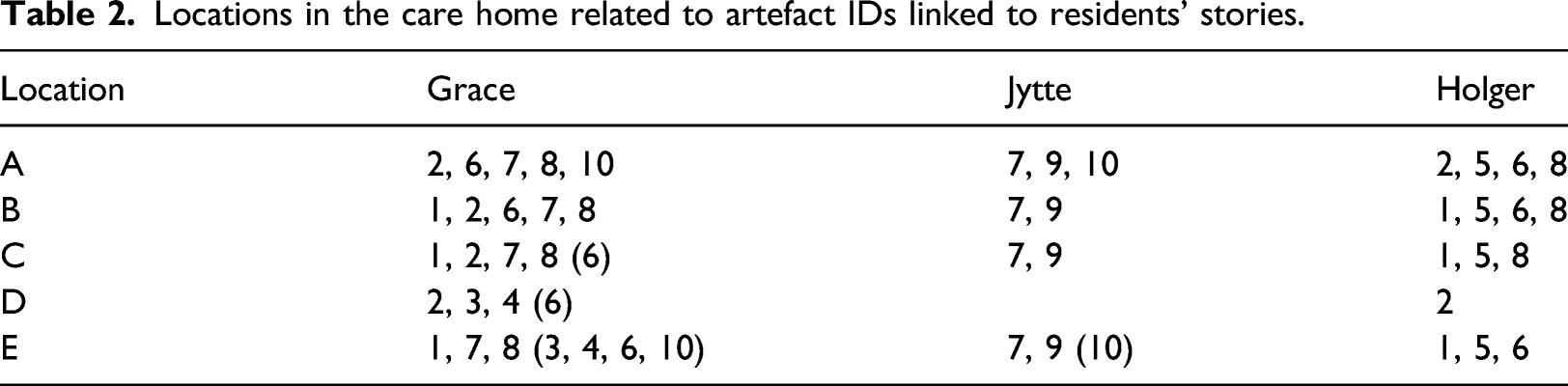
In each location, multiple artefacts are detectable by Memento. However, life story information related to those artefacts only becomes visible on the smartphone interface when artefact beacons are sensed and matched with proximate residents who are associated with that artefact through their life stories. These information hints are then pushed to the smartwatch of the caregiver. If the caregiver needs more information, they can access details on their smartphone.
Field evaluation procedure
Before the field evaluation, Anne used a smartwatch for the first time for about an hour to get used to operating it. The study began by giving Anne a 10-minute introduction to Memento and the interactions needed to operate it. Anne was asked to pay particular attention to Grace during her rounds on this day. The researcher then shadowed Anne on her usual route through the care home, making notes on observations, and taking short videos of moments of intense interaction with a small video camera. The field study started with Anne approaching the residents’ common living area (B), from the stairway (A). There she met and talked with Grace. Anne then walked Grace to her apartment (D), via the corridor (C), and spent some time there talking. Anne and Grace then left the apartment and spent time together in the corridor leading to the common living area (E).
In the common living area (B), Anne chose the herbs (artefact 8) as a topic of conversation and used the information hint offered on her smartwatch about Grace’s passion for gardening. They continued this conversation on their way to Grace’s apartment (D). While passing the badminton racket (artefact 7) in the corridor on the way (E) Anne chose not to use the information hint offered about Grace’s active sports life. Inside Grace’s apartment, Anne used an information hint about the photo album (artefact 3) to talk about Grace and her husband and some of the events related to life on their farm. Leaving the apartment Anne chose to use the information hint related to the badminton racket (artefact 7) to talk to Grace about her love of sports and invite her to play a game of balloon badminton (see Figure 4). At the end of the visit, Anne then left Grace in the common living area and went to see other residents in the care home. Grace and Anne engaged in a spontaneous game of balloon badminton.
Data collection and analysis
The total observation took 2 hours of Anne’s 8-hour shift. Fifteen pages of observational field evaluation and post-study reflective notes and 20 minutes of videotape were collected. Anne was asked to write notes on observations and thoughts on her interactions with Grace during the study, when appropriate. After the evaluation, with Anne present, the researcher had an informal chat with Grace about how she was feeling and how she enjoyed her time with Anne that day. The researcher also conducted a 30-minute interview with Anne immediately after the study to collect her insights. Short 15-minute semi-structured interviews were also conducted with two other caregivers and the care home manager, to get their feedback on the system.
This research used reflexive thematic analysis41,42 incorporating six recursive phases combining transcripts of the interviews with the observational notes collected. The researcher used this method to familiarise with the data, code it to create initial themes, review, develop, refine, define and name themes that represented the participants’ lived experiences in the evaluation of the technology. The reflexive coding and theming was undertaken by the researcher that gathered data in the field visit, using a highly qualitative and inherently subjective approach. This inductive driven analysis and interpretive approach, captured the researcher’s deepening understanding of the data. A final refinement, using affinity diagramming 43 as a collaborative process between the whole research team familiar with the care home context, for feedback on the final themes. This process was done to identify evaluative outcomes thematically and to inform further design of the Memento concept.
Results and discussion
The caregivers and care home manager were all extremely enthusiastic about what the system could provide in terms of matching nearby residents with artefacts and sending life story hints to the caregiver. They were impressed that the system would make it possible to integrate spontaneous RT into their daily interactions with residents, and thereby have a positive impact on resident well-being in the care home. Through this study method that respected the privacy and self-esteem of the residents, we gained the trust of caregivers, residents, and the care home management. Grace, at 83 years old, was proud to be a part of our study and enjoyed sharing her reminiscences with us.
Reflecting on the design of Memento, and through thematic analysis, we identified the following understandings of the impact that Memento has on the everyday lives of people with dementia and their caregivers. Our findings are grouped into five overall themes: companionship through spontaneous meaningful conversations; increasing confidence through sense of identity; identifying shared interests amongst residents; preserving individual identities of residents; and improved access to residents’ stories. The following discusses these themes informing the design of Memento and its ability to successfully support dementia care and is followed by a brief discussion on the next stages from a research perspective and where this technology could have other applications. Quotes provided in this section were translated from Danish for this article.
Companionship through spontaneous meaningful conversations
During the study, Anne received numerous information hints on her smartphone and was able to choose amongst them without difficulty. Every time a life story connection was presented it proved relevant for activating memories that prompted Grace to engage in conversations she cared about. From Anne’s point of view, the interventions from Memento did not reduce the companionship in the conversation between herself and Grace, suggesting that Memento does not impact the naturalness of interactions between caregivers and residents.
As the care home manager said: “This method is new in the sense that we have the information readily at hand. […] It also means that although we know our residents really well, […] the here-and-now relation comes more into focus by using the information […] on this little watch.”
The subtle nature of the caregiver interaction with Memento, a vibration, and an information hint displayed on the smartwatch, helped support companionship while maintaining a focus on presence and natural social interaction between resident and caregiver. The use of barely visible proximity beacons attached to artefacts around the care home and integrated into the normal accessories of residents, such as bracelets, name badges, or necklaces, means that detection and matching between residents, artefacts, and stories happens in the background. While residents remain unaware of the system it is giving the caregiver immediate access to highly relevant and personal conversation topics. This supports spontaneous and natural RT integrated into everyday activities, allowing residents to avoid the kinds of problems associated with group reminiscence therapy sessions, such as feeling they are being tested or not wanting to participate in social groupings at fixed times and locations.
Increasing confidence through feelings of competence
Being able to remember past activities, memories and past competencies are an important part of increasing self-confidence and sense of well-being for people with dementia. The frustrations of not being able to remember recent events can be counterbalanced by reminiscing. Memories about a past where the person had particular skills and competencies and reliving those moments through conversations about them can help increase personal confidence in people with dementia.
People living in their own homes and with family members have many daily opportunities to reflect on their past through familiar artefacts and places around them – and through conversations with loved ones who also remember their past histories. This becomes problematic in care homes, where the environment is new. With numerous residents and the changing shifts of caregivers, it is very difficult for them to know each resident’s individual stories and the artefacts in the care home that trigger those stories and boost feelings of confidence and competence. According to Anne, hints from Memento helped reinforce Grace’s competencies, she said, “Grace […] asked me time and again what year it is. She could not remember – but she was competent through her memories. She remembered details about when they got a new roof on their farmhouse. And still, she kept asking “what year is it?” So, this is also a reinforcement of her competence as a person – to […] be able to do things – to […] remember things.”
Memento positively helped the caregiver engage in conversations on topics dear to the resident. These conversations made Grace feel and act more confident because she could remember and relive past competencies and share them. Grace reported that talking about her past was highly enjoyable and gave her a renewed sense of self-confidence, to remember how she used to love sports and was an accomplished and active badminton player.
Identifying shared interests amongst residents
Part of the caregiver’s role is to identify residents with shared interests and connect them, seeding conversations about their shared interests. This takes the conversational load off of the caregivers, leaving them open to do other duties. It is also beneficial for residents, helping them find conversational points that can ease them into social connections with others, helping counteract feelings of isolation and loneliness, which are a problem in care homes. 44 As Anne shared,
“Having dementia makes you withdraw, in how you relate to other people, but when someone invites you to a conversation, you get an opportunity to reach out and engage in a dialogue that matters.”
In the past, this has been done by reading through the life stories of all residents and trying to find similarities in their stories or visually identifying matching items or subjects. This can be a difficult and imprecise method for finding common ground amongst residents.
Since caregivers have multiple people in their care Memento alleviates the problem of caregivers having difficulty remembering specific memory triggers for each individual. Memento was embraced by caregivers as a great mechanism for reducing the time spent repeatedly reading life stories to find residents with shared interests. They were especially pleased that the system was able to match artefacts in the common areas with several nearby residents and their life stories, making it possible and relatively easy to start conversations involving several residents around an artefact. Their experience with residents meant they could provide additional insights into the memories a shared artefact might evoke and add this into the conversation. They were then able to add this into the database of residents’ life stories to enrich future connections.
Alternatively, caregivers could find common interests among residents and use this knowledge to place relevant artefacts in common areas to facilitate spontaneous RT – both on individual and group levels. Conversations triggered by the use of Memento, through matching proximate artefacts to nearby residents, make the work of the caregiver both easier and more rewarding.
Preserving individual identities of residents
By engaging a person in conversations on topics that are dear to them, RT helps preserve the identity of that particular person and counteracts the “loss of self” that often accompanies the fading of recent memories. 45 It is important for individuals who are finding things and people difficult to identify and remember to have other ways of embracing their individuality that go beyond everyday activities and draws on remembering themselves through their histories.
Information hints from Memento supported the caregiver in involving residents, who otherwise tended to withdraw socially, into conversations about things they cared about, and which helped them identify with their past. As Anne said, “What matters most […] is the preservation of identity. [With Memento] We get an electronic tool that helps us […] focus on the person all the time.”
The care home manager also described the contribution of information hints from Memento, by saying,
“One problem for elderly in a place like this is to remember – but memory can be triggered by seeing things or hearing things. So, what we can do is to bring the life lived back into the resident’s present life much more than if we did not have these hints.”
Using Memento in their daily work made it possible for caregivers to help augment the resident’s sense of self, through small episodes and conversations based on personal memories and life stories. Such conversations with residents could be interwoven throughout their usual daily activities, giving many opportunities for spontaneous RT in the place where they live. In this way, RT, which has been shown to alleviate cognitive and memory decline in people who are living with dementia, can be a part of the resident’s and caregiver’s everyday interactions, occurring in places that feel comfortable and familiar, and help to preserve their identities while anchoring them to the here and now.
Improved access to residents’ stories
In follow-up interviews, Memento was very positively received by both Anne and the care home manager for helping them manage and make better use of the resident’s life stories. When made available in the places where daily activities take place, they became an invaluable asset in helping facilitate meaningful conversations between caregivers and residents. According to the care home manager, “They [the residents] cannot remember what happened yesterday, and sometimes they have difficulty knowing the present time and place, but they carry so many memories of the past with them, and when you talk about those, you get the feeling that they are engaged”.
During initial design investigations, we realized that the existing registration procedure for documenting life stories of new residents was fairly ad hoc and reliant on manual registration and storing of their life stories into a set of separate text documents, filled in during induction. This suggested that a user-friendly interface integrated into Memento would assist staff in adding information about new and current residents, which in turn would enhance the capabilities of the system. Especially when keywords can be generated automatically. Hence, we designed a data entry registration form with meaningful fields, linked to the Memento system and database. The care manager commented that this interface would be an improvement in information gathering, as the format would serve as a checklist and help staff ask relevant questions and register important information in life stories as new residents arrive.
Limitations of the study
Memento received very positive feedback from the staff members involved in its development and use, as well as the resident that participated in the field evaluation of the system, but it is also important here to discuss possible limitations and disadvantages of the system.
Although a key benefit of Memento is the use of everyday technologies, such as a smartwatch and smartphone, it does require that caregivers who want to participate in spontaneous reminiscence therapy do wear a smartwatch, carry their mobile phone, and are so familiar with their use that they can do so discretely and quickly recognise the nearby object prompts, without drawing attention to their interactions with the system. This ensures that the conversation feels natural to the resident with dementia and that it can integrate seamlessly with the usual care activities. If the use of personal phones is discouraged during work shifts, then the question of a work-provided smartphone needs to be addressed. Similarly, not everyone has a smartwatch, as they are still quite a significant personal expense. The system would still work if the care home provided this hardware to be checked in and out and used during the caregiver’s shift, but this then takes additional administrative overhead.
For the system to work, the person with dementia needs to be wearing their name tag that has the embedded lightweight beacon. Although we were assured by the care home management that all residents were encouraged to wear their name badges at all times, it is quite conceivable that they may forget to do this, or may have misplaced it. In this case, caregivers have the added duty of ensuring that all residents wear their specially tagged name badges for the system to be effective in both one-on-one therapy and group conversations. A more robust design might be to give residents a choice of form factors for the personal beacon, such as a watch, necklace, key fob, or even integrated into their clothing.
This leads to another consideration, and that is giving the person with dementia the choice to wear the beacon and hence be part of the system, although in this context the residents were already carrying this beacon. In a care context, there are proven benefits for participating in reminiscence therapy, but individuals should still have the right to engage or not. Further research is required to understand how people with dementia feel about being always available or having their stories shared, and whether carrying the beacon or deliberately not carrying the beacon would be an indicator of their current openness for personal conversations. It is probably worth noting that the histories of residents that are in the system have been compiled with the knowledge and permission of the person with dementia and their families.
The presented study is inherently limited in terms of its generalizability. As the study only involved one resident using Memento, and the prototype has so-far only been deployed and studied in the context of one care home, our findings are purely qualitative and only indicative beyond the specific case study. In terms of bias from the participants, however, we have no reason to suspect this as neither the care home, nor the interview participants, were stakeholders in the technical project, or would gain from its continued development.
Extending memento
Given the high level of praise and acceptance of the Memento system by the care home stakeholders, it is evident that smartphone and smartwatch technologies represent an opportunity to develop systems that both support and extend caregivers’ capabilities in their everyday work. Additionally, the positive experience of relevant conversations reported by the resident indicates that these technologies also enable residents with dementia to have an improved quality of life. A worthwhile extension to this research would be a longitudinal study of Memento in use in the full care home situation, with multiple caregivers and residents. This would require the development of the system to be robust and able to run independently with minimal researcher intervention, easy resident and artefact tagging, reliable and comprehensive digitizing of resident histories by staff, and automatic logging mechanisms for collecting data about system interactions. It would also be interesting to look at adapting Memento to an at-home setting, using the same user-centred iterative design method. This could facilitate older adults staying in their own homes for longer by supporting itinerant caregivers in the community. Memento could enhance the quality of care in any situation where caregivers are unfamiliar with their clients by simply and subtly receiving information about the client’s history on their smartphone.
Conclusion
By taking human values into account, and using a sensitive approach to design, the design of Memento contributes to research understanding in the area of improving quality of life for people living with dementia in care homes. Our research produced a prototype technology design solution that makes it easy and convenient for caregivers to connect residents with real stories from their past and engage these residents in meaningful conversations that make them feel competent, and invite them to reminisce on past skills, knowledge, and experiences that belong to them. This novel integration of readily available and affordable proximity-aware digital technologies makes it possible for caregivers to naturally and spontaneously engage residents in meaningful conversations without interrupting the flow of daily activities. This is achieved by structuring life story information in such a way that relevant snippets can be matched to artefacts in a resident’s proximate environment and information hints sent to a caregiver’s smartwatch.
Our research opens up opportunities for technology to support caregivers in providing spontaneous conversational prompts on topics of relevance to people with dementia, renewing their sense of self-confidence, self-esteem and well-being.
Footnotes
Acknowledgements
We would like to gratefully acknowledge the willing participation and input from the staff and residents of the Farsøhthus Care Home in Djursland, Denmark.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.