
Abstract
Nowadays, it is common for people to look for health care information on the internet. The eHealth Literacy Scale (eHEALS) is commonly used to measure eHealth literacy. As of the publication of this study, the Indonesian version for eHEALS has not been published even though eHealth literacy is necessary, especially in the current COVID-19 pandemic. We aimed to evaluate the validity and reliability of the Indonesian version of eHEALS (I-eHEALS). A total of 100 respondents in East Java were involved in this cross-sectional study. Pearson-product moment correlation method and construct validity were used to validate the results. The reliability was determined based on the Cronbach’s alpha internal consistency measurement and intraclass correlation coefficient (ICC). The Pearson correlation analysis results are significantly higher (r > 0.254, p < 0.01) compared to the critical value table. Single factors accounting for 57.66% variance in the scales exhibit a unidimensional latent structure. The internal consistency between items is excellent as shown by the Cronbach’s alpha coefficient (0.91). The ICC analysis shows an acceptable result (0.552, p < 0.01). The I-eHEALS is valid and reliable to be used for evaluating the eHealth literacy of the Indonesian population.
Introduction
Vast amount of information relating to health and medicine can be found easily throughout the internet nowadays. Internet use has become a standard practice for people looking for health care information. A study by the Pew Research Center Project claimed that approximately three-quarters of adults in the United States use the internet to seek for health information. 1 Around 31.5% of participants in a nationwide study conducted in Germany used the internet as the information source of choice for health-related questions. 2 However, not all health resources found through the internet are credible or certified by experts of each respective field. This statistic calls for the importance of health literacy among internet users. As a multidimensional concept, there are multiple changes to the definition of health literacy since its conception 50 years ago. The term used to focus only on a person’s ability to read and comprehend written information regarding health. Currently, the concept covers factors influencing people’s ability to access, understand, and utilize information regarding health from multiple sources. 3 One of the means of obtaining this information is through the internet. Based on currently published studies focusing on eHealth, there is an apparent inconsistency in the use of the term. A systematic review by Oh et al. 4 found 51 unique definitions of eHealth. In those definitions, technology was seen as an instrument to enable a service and as the embodiment of eHealth itself. It was portrayed as a means to assist or enhance human activities rather than a substitute for human beings. The definition proposed by Eysenbach is one of the most cited ones, in which the study described eHealth as an emerging field in the intersection of medical informatics, public health and business, referring to health services and information delivered or enhanced through the internet and related technologies. 5 To focus specifically on the literacy aspect of using eHealth, Norman and Skinner coined the term “eHealth literacy” describing the ability to seek for health information on the internet. eHealth literacy is essential for discerning high-quality health information from low quality ones. 1 One of the most commonly used instruments to measure literacy in eHealth that have been previously used is the eHealth Literacy Scale (eHEALS).6 –11 eHEALS is a self-reported health literacy measurement proposed by Norman and Skinner in 2006. The questionnaire was developed with the purpose of measuring the respondent’s knowledge and ability to find, evaluate, and apply health information taken from the internet. 12 To appropriately use the questionnaire in non-native English-speaking countries, it is necessary to have a translated and culturally adapted version according to each respective country. Currently, there are multiple versions of the instrument based on different purposes of use and languages.13 –16 As of the publication of this study, the Indonesian version for eHEALS has not been published even though in 2018 Indonesia was ranked as the fourth country with the highest number of internet users worldwide, measuring at 171 million users or 64.8% of the total population. 17 Additionally, not every information found on the internet is reliable. Baseless information or hoax are prominent problems plaguing the Indonesian web community. 18 The need for eHealth literacy evaluation in Indonesia is more common now more than ever since the outbreak of the 2019 novel coronavirus disease (COVID-19). 19 An understanding of the disease is necessary for citizens to accept major societal changes amid the pandemic by having an adequate understanding of the disease through reliable sources, one of which is through the internet. 20 One of the expected beneficial outcomes by being able to evaluate the eHealth literacy of the population is that it would allow the government to identify a variety of literacy levels among citizens with multiple sociodemographic backgrounds and generate a proper response accordingly. The current proposed strategy to contain the spread of the infection, one of which is by posting COVID-19 information in social media platforms, may not be effective if the diverse literacy levels of the population are not taken into account. Therefore, it is necessary to create an adapted Indonesian version of eHEALS according to the local language and cultural terms. In this study, we aimed to evaluate the validity and reliability of the Indonesian version of eHEALS or I-eHeals.
Methods
Translation and cultural adaptation of the instrument
The original eHeals questionnaire consists of eight questions measured by a 5-point Likert scale (1: strongly disagree, 5: strongly agree), with a total score ranging from 8 to 40. A higher score naturally indicates a higher level of literacy. The instrument measures perceived knowledge, skills, and confidence in locating, evaluating, and using electronic health information to make health decisions. There are two additional questions, which assess the perception of the internet as a tool to assess health information and make decisions, that do not contribute to the total score. 12 Two translators with a high level of English language proficiency and medical background worked independently on translating the questionnaire before combining the end result. Twenty random participants were selected to test the pre-finalized version. Feedbacks from the partakers were taken into account and discussed by the two translators and additional input from other external parties with equal levels of proficiency. The completed outcome was assessed once again by the involved parties before being spread to the participants.
Study design and population
This is a cross-sectional study with a non-probability sampling involving a total of 100 consecutively selected individuals in East Java, Indonesia in March 2020. The sample size was based on previous studies that used a subject-to-item ratio ⩾2 or a sample size ⩾100 to validate a scale. 21 Due to the COVID-19 pandemic, the data collection was performed through an online survey spread among potential participants living in East Java. The province is appropriate for evaluating a research instrument on the Indonesian population as it is the second most populous province in the country, thus, the ethnic and cultural diversity of the nation is well-represented. Moreover, the Javanese ethnicity makes up approximately 40% of the nation’s population. 22 An informed consent was given by each participant before filling in the questionnaire. To ensure proper and appropriate answers, the basic purpose of the study was explained to the participants in the preface section.
Validity analysis
Descriptive statistics of the sociodemographic status were presented as the mean (±SD), amount (n), and percentage (%). Questionnaire results were separated into each function domain and tested for both validity and reliability. Pearson product moment correlation method was used to test the validity by evaluating the results using the critical value table of the Pearson Product-Moment Correlation Coefficient (r > 0.254). 23 Exploratory factor analysis was performed to ensure construct validity. 24 Kaiser-Meyer-Olkin value (>0.7) and data factorability was evaluated based on the Bartlett test of sphericity. The number of extracted factors were determined by scree plot and the eigenvalue (>1). 25
Reliability analysis
Cronbach’s alpha was used to measure the internal consistency of the scale (α < 0.5, unacceptable; 0.5 ⩽ α < 0.6, poor; 0.6 ⩽ α < 0.7, questionable; 0.7 ⩽ α < 0.8, acceptable; 0.8 ⩽ α < 0.9, good; α ⩾ 0.9, excellent). 26 Intraclass correlation coefficient (ICC) is also measured as part of the reliability analysis (r < 0.4, poor; 0.4 ⩽ r < 0.75, satisfactory; r ⩾ 0.75, excellent). 27 IBM SPSS Version 24.0 software was used for the statistical analysis.
Results
Subjects’ characteristics
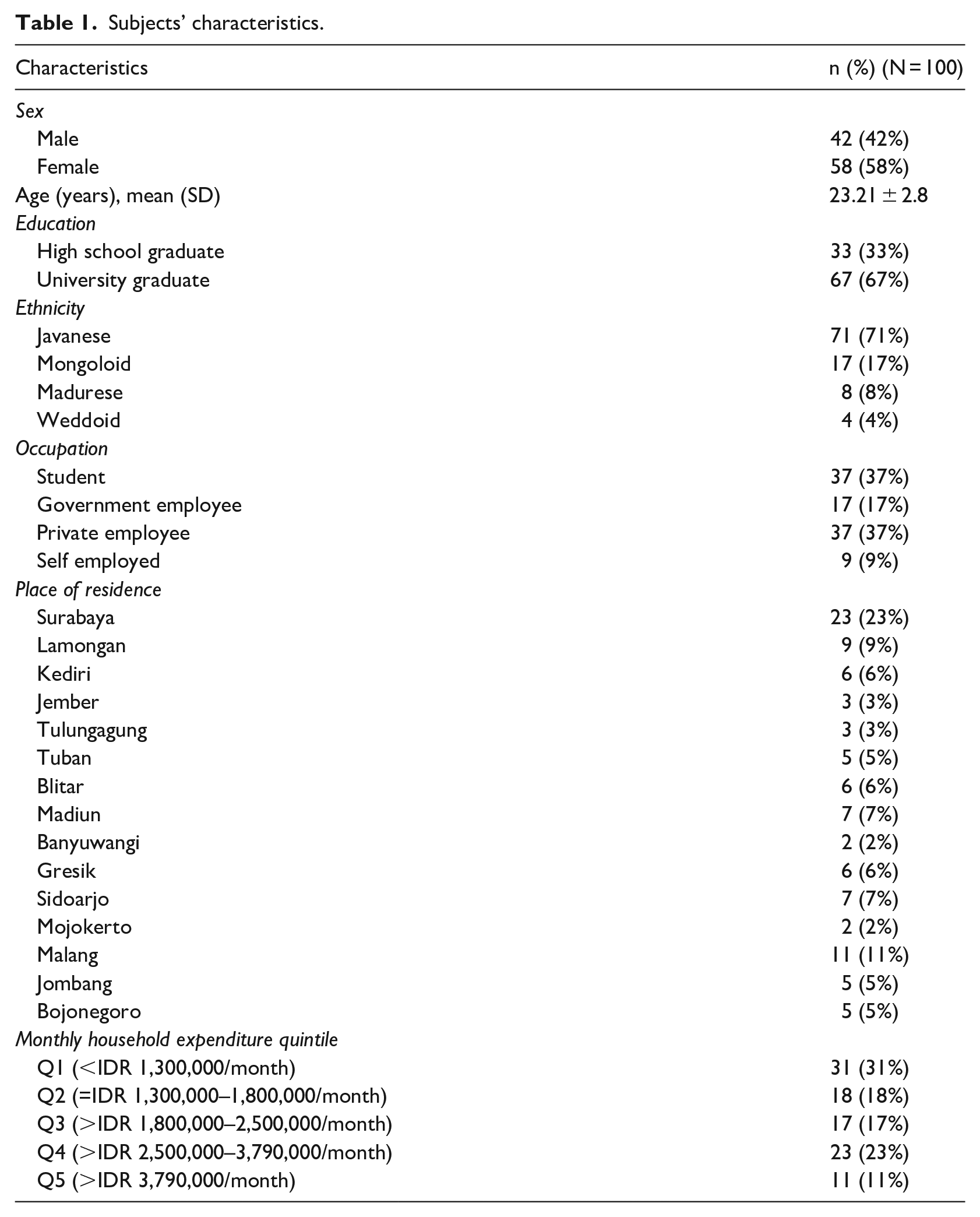
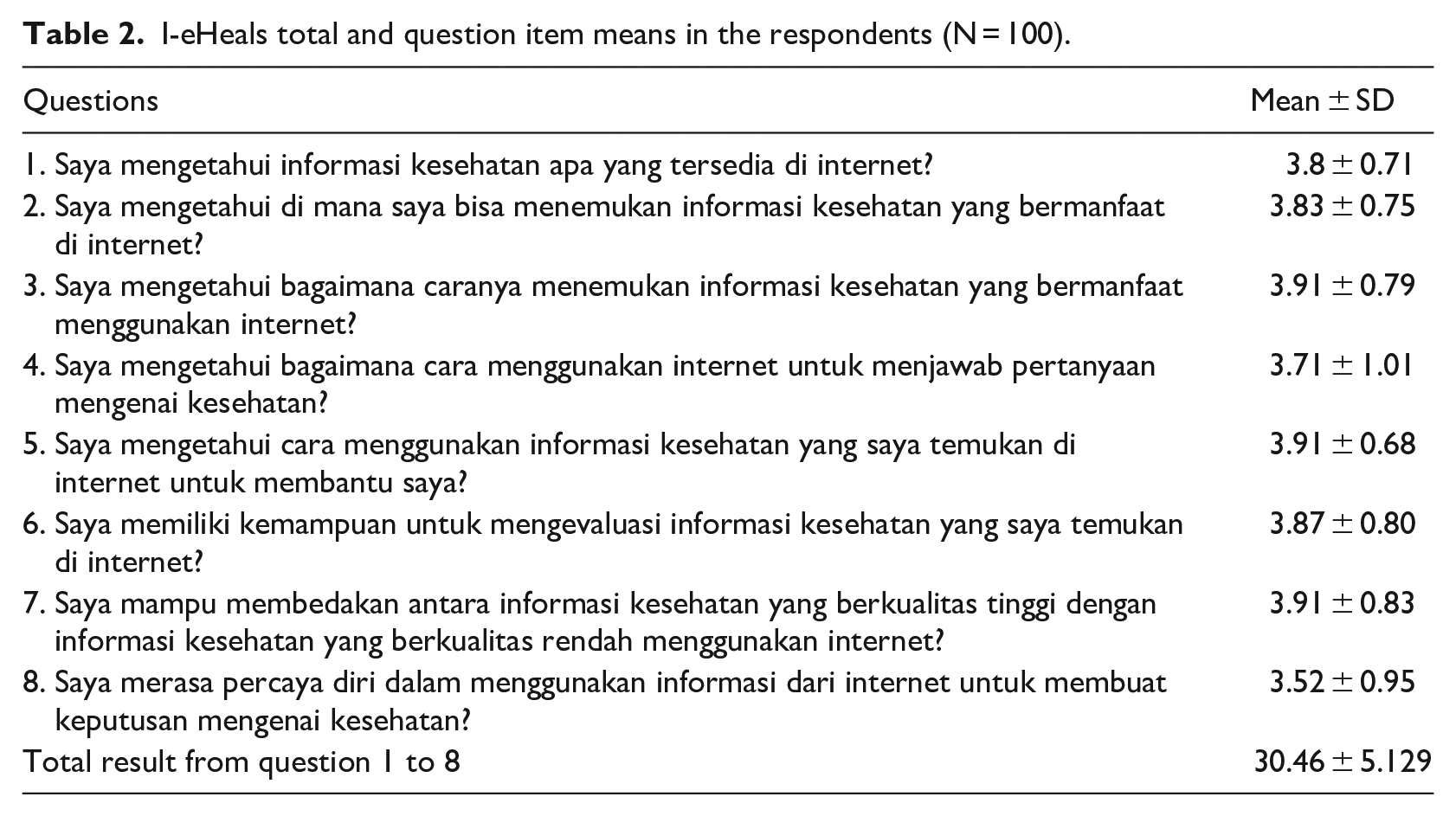
A total of 100 respondents were involved in the study. Table 1 shows that most participants are around 23 years old and were High School and University graduates. Javanese, Madurese, and Mongoloid are in the top five ethnicities that comprise Indonesian people, thus, the ethnicities of the respondents in this study adequately represent the population. Most of the samples reside in Surabaya and Malang. This is expected, since Surabaya is the largest and most densely populated city in East Java. Additionally, it is the second largest metropolitan city in the country behind Jakarta, which would the end result of the analysis more promising. The socioeconomic status of the respondents based on the monthly household expenditure also appropriately exhibit the overall status of Indonesian citizens. Table 2 displays the average result from each question item as well as the average result from the respondents (30.46 ± 5.129).
Subjects’ characteristics.
I-eHeals total and question item means in the respondents (N = 100).
Validity analysis
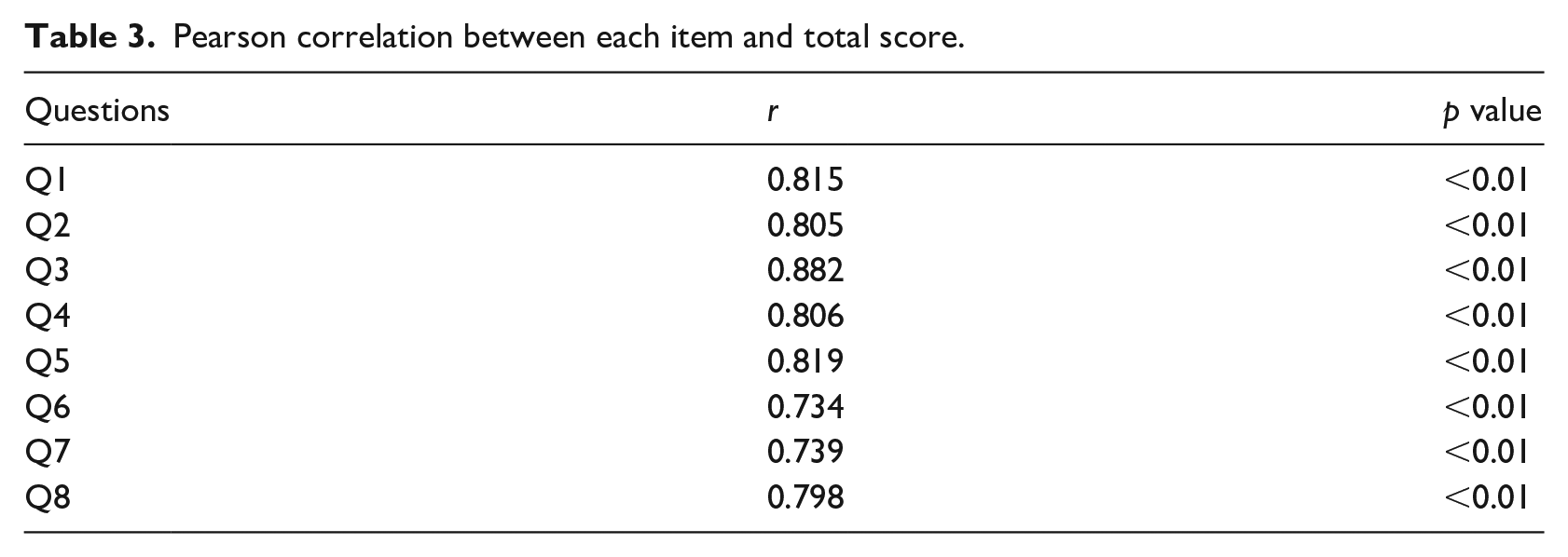
Based on the Pearson correlation analysis as seen in Table 3, the r value is significantly higher (r > 0.254, p < 0.01) compared to the critical value table of the Pearson Product-Moment Correlation Coefficient. The magnitudes of the intercorrelation between the question items and the total score are mostly ranged from high (r = 0.70–0.90) to very high (r = 0.90–1.00). These results exhibit an excellent level of validity of the I-eHEALS. Moreover, the construct validity analysis also shows promising results. The Bartlett test of sphericity (x228 = 508.46, p < 0.01) suggests the factorability of the correlation matrix. The Kaiser-Meyer-Olkin test (0.875) demonstrate an adequate sampling relative to the number of question items. A single factor model is kept based on the initial eigenvalue (5.00) and a unidimensional latent structure of the scree plot shown in Figure 1. The factor loadings and score coefficients shown in Table 4. The extraction sum of the squared loadings is 4.61 with a 57.66% variance.
Pearson correlation between each item and total score.
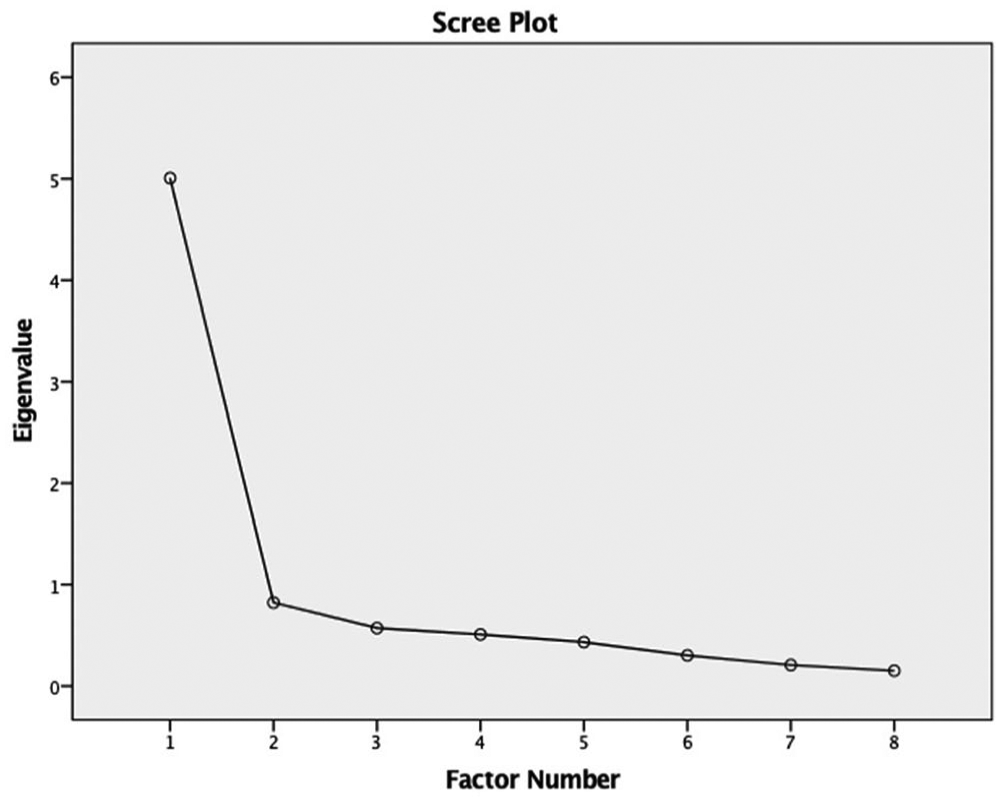
I-eHEALS scree plot.
Factor loadings and score coefficients with single extracted factor.
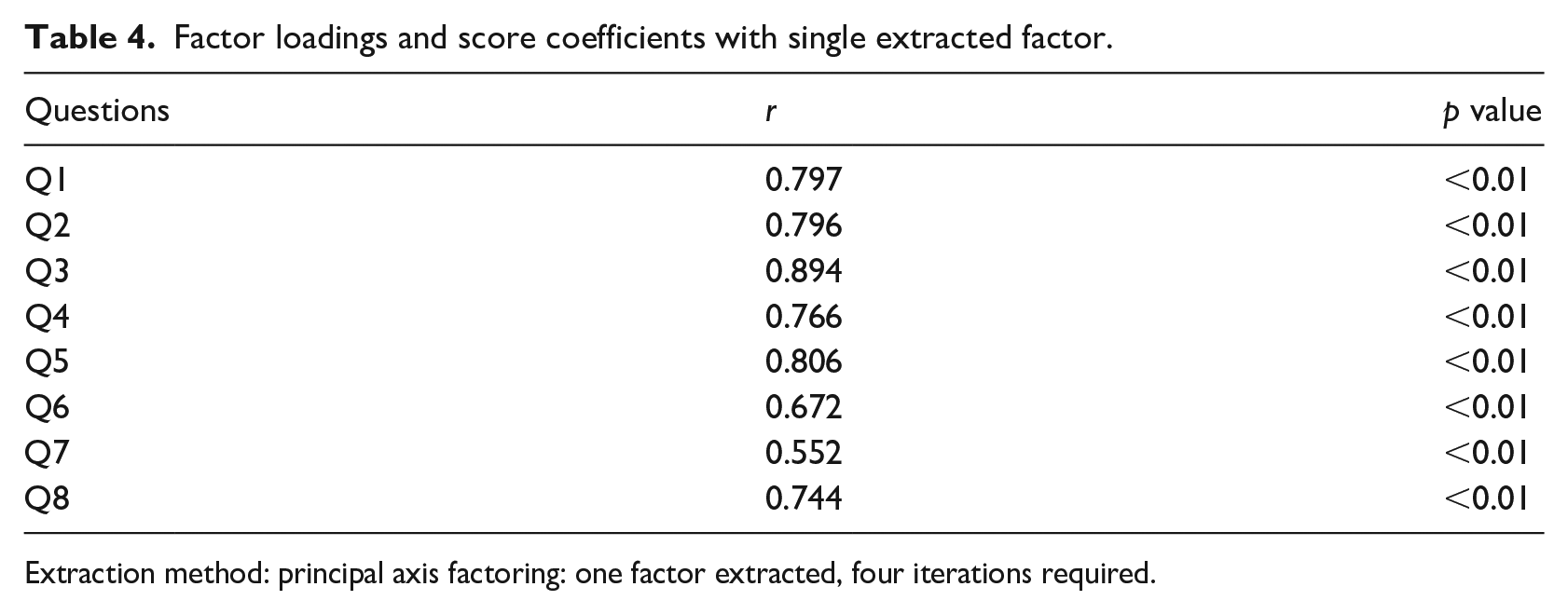
Extraction method: principal axis factoring: one factor extracted, four iterations required.
Reliability analysis
Table 5 display excellent internal consistency between items as indicated by the Cronbach’s alpha coefficient (0.91). The ICC analysis show an acceptable result (0.552, p < 0.01).
Internal consistency and intraclass correlation coefficient (ICC).

Discussion
As of the creation of the eHEALS, this is the first attempt to translate the questionnaire into Indonesian. Previously the questionnaire has been translated into Arabic, 16 Chinese, 28 Iran, 29 Italy, 30 Korean, 31 Persian, 32 Spanish, 33 and Swedish, 16 among many others. Even though Indonesia is ranked as the fourth country with the highest number of internet users in the world, there has not been any accessible eHealth literacy measurement for the Indonesian population. 34 Apart from the literal English language comprehension barrier in several populations, it is also important to note that certain terms could have different meanings in other languages. The translation process necessitate a knowledge of the local terms to help respondent assimilate the questions as well as preventing potential misunderstandings. For example, the translators did not find the direct Indonesian translation of the term “health resources” suitable for the context of the question, thus, we changed it into the term closely-related to “health information” instead. The content and meaning of each item represent the original question items well. Several wordings of the sentences need to be adapted to the target language to ensure adequate understanding by respondents with different levels of education and health literacy. The decision to collect participants from East Java benefited the authenticity of the results as the respondents make up the dominant ethnicities representing the country. 35
Validity analysis
Excellent level of validity are shown by the Pearson correlation results based on the significantly higher r score (r > 0.254, p < 0.01) compared to the critical value table of Pearson Product-Moment Correlation Coefficient. 23 The construct validity results in this study are in line with the findings in the Korean and Spanish studies.31,33 Similar to the K-eHEALS, the I-eHEALS also displayed a monofactorial unidimensional structure and elucidated the variance. The 57.66% variance in this study that yielded a single factor solution is supported by previous Korean (50.3%), Spanish (52.6%), and Iranian (70.5%) versions.29,31,33
Reliability analysis
The internal consistency of the I-eHEALS is considered to be highly reliable and internally consistent based on the Cronbach alpha analysis (r = 0.908) and an acceptable ICC result (0.552, p < 0.01). The high measure for Cronbach alpha is usually attributed to questionnaires with large number of items, since Cronbach alpha is directly dependent on the number of items in a questionnaire. Internal consistency of the Indonesian version is comparable to the Korean (r = 0.88), Turkish (r = 0.78), Japanese (r = 0.93), and Swedish (r = 0.94) versions indicating an excellent reliability of the instrument.31,36 –38
Overall interpretation of findings
Apart from the statistical results, the feedbacks that we receive from respondents indicate that the questions were easy to understand and answer without any lost meaning or purpose. An adequate understanding of the question items would help future studies to evaluate the eHealth literacy of Indonesian citizens since, as mentioned previously, the country has the fourth largest internet users. 17 The US Office of Disease Prevention and Health Promotion elaborated on the need for increased health literacy, access to internet, and use of health information technologies to promote health of the public. 39 Studies aiming at measuring and understanding eHealth literacy is needed to develop effective interventions promoting the health of the public. As of now, there is not yet any national initiative to promote the significance of eHealth literacy in Indonesia. Due to the current pandemic situation, an adequate eHealth literacy is necessary for people to easily access information regarding COVID-19. An understanding of the disease would encourage people to follow regulations by performing physical distancing and staying at home. Measuring eHealth literacy is at its best a first step against the pandemic, however, the ability to do so would allow the government to produce informative and educational online materials regarding COVID-19 based on the diverse literacy levels among Indonesian citizens. The next probable step would be to conduct a strategy responding to different health literacy needs. Hopefully, the publication of I-eHEALS would propel future studies focusing on the eHealth literacy of Indonesian citizens.
Study limitation
The main limitation of our study is that the respondents involved were around 20–30 years of age and were either high school or university graduates. For the time being, this is expected as older Indonesian people with lower than high school degrees are not avid internet users. According to the United Nations Educational, Scientific and Cultural Organization (UNESCO), the current literacy rate for the Indonesian people is 95.66% for citizens with the age of 15 years and older. However, the rate is much lower for the geriatric population with the age of 65 years and older (74.34%). 40 Taking this data into account, a face-to-face survey may be needed in the future as the proportion of elderly internet users increases to conduct a complete and proper evaluation of the eHEALS specifically on the elderly population. Hopefully, the language comprehension of the much older population to understand the question items should not be a problem as they were written according to the national standard of formal Indonesian language. In this study, test-retest reliability was not performed due to time and financial constraints of the research team.
Conclusion
The Indonesian version of eHEALS (I-eHEALS) is valid and reliable to be used for studies evaluating the eHealth literacy of the young and middle-aged adult population in Indonesia.
Footnotes
Acknowledgements
The authors thank Putu Ayu Intan Cahaya Dewi, S.I.Kom, Dio Atmando, B.A., Illona Okvita, M.D., and Rafaela Andira Ledyastatin, M.D.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed consent
Informed consent was given by every respondent before being involved in the study.
Ethical approval
The study was approved by the ethical committee of “Rumah Sakit Orthopedi dan Traumatologi Surabaya.”