
Abstract
The COVID-19 pandemic has driven a greater reliance on telemedicine, yet rural access, use, and satisfaction with telemedicine and the role of eHealth literacy are unknown. Using a cross-sectional design, 279 (70.6% female) western rural Canadians completed an online survey. The majority of participants reported access to telemedicine, but nearly 1/5 lacked access to online or virtual mental health services. The majority of participants had used health care services following the declared COVID-19 pandemic in North America, and just under half had used telemedicine. Telemedicine satisfaction scores were higher among participants who had used video (M = 4.18) compared to those who used phone alone (M = 3.79) (p = 0.031). Telemedicine satisfaction and eHealth literacy were correlated (r = 0.26, p = 0.005). Participants did not want telemedicine to replace in-person consultations. Telemedicine practice requires that rural residents have the resources, ability and willingness to engage with remote care.
Background
Well known health and health care disparities characterize at-risk populations in rural settings. Poor mental health, unhealthy behaviors (e.g. smoking), obesity, chronic diseases (e.g. cardiovascular disease, diabetes), lower life expectancy, and potentially avoidable mortality are higher in rural and remote areas than urban areas. 1 Despite these greater needs, rural populations/communities face disparities in their access to health care such as physician (primary, specialist) shortages, lack of health care facilities, services and equipment, and inadequate infrastructure.2,3
Prior to the COVID-19 pandemic, telemedicine was touted as a promising solution to address these rural inequities and increase the quality and accessibility of health care. For our purposes, and following the World Health Organization, telemedicine is used interchangeably with telehealth and defined according to four elements: provides clinical support; connects users from different locations; uses information and communication technologies; and orients to health outcomes. 4 Developments in remote monitoring and sensor technology have further advanced telemedicine practice providing applications for diagnosis, disease surveillance and treatment support. 5 Indeed, the benefit of using technology in the delivery of mental health services to rural areas has been well documented. 6 So too, cloud-based solutions have been effectively used to link rural patients with medical consultants through intermediary health care and community clinic workers. 7
Despite its potential, pre-COVID-19 telemedicine uptake was slow and below expectation. 8 Pre-COVID-19 evidence indicates that rural residents have lowered amenability and preference for telehealth services when local services are available (e.g. hospitals, clinics).9–11 How COVID-19 imposed restrictions on access to these services, and disruptions in usual rural primary care with the abrupt switch to telemedicine, have influenced rural residents’ satisfaction with telemedicine is unknown.
Although rural uptake was low, pre-COVID-19 satisfaction with telemedicine has been found to be high among patients from rural and remote areas. 12 Orlando et al., 12 found high levels of satisfaction (system experience, information sharing, consumer focus and overall satisfaction) with telehealth videoconferencing among patients and caregivers living in rural and remote communities who had outpatient appointments from their local health care center with a health care provider at another center. Harkey et al. 13 found patients living in rural areas had high levels of satisfaction with telehealth services for occupational therapy, physical therapy or physiotherapy, and speech-language therapy compared to in-person care. These telemedicine uses were largely for specialist care and did not necessarily reflect the massive shift that occurred with the COVID-19 pandemic that catalyzed telemedicine into all areas of practice including primary care where it had not been routinely used.
It is important to understand rural citizens’ use of, and satisfaction with telemedicine during COVID-19, especially as some have projected that post-pandemic, telemedicine will become the new normal in health care delivery. 14 A recent survey suggested that patient satisfaction with telemedicine was high following COVID-19 15 ; however, this finding was not specific to rural communities who face different challenges than their urban counterparts. For example, reliance on telemedicine used to its full capacity (e.g. video) requires adequate broadband access, which is often limited in rural and underserved settings. 16 In urban Canadian communities high-speed internet doubled to 51.5 Mbps in 2020, while in rural communities it plateaued at 5.5 Mbps, 17 potentially impacting the type and quality of telemedicine care rural people receive and influencing their satisfaction with this care modality.
Another factor that impacts users’ ability to use, and satisfaction with, telemedicine is electronic health (eHealth) literacy (defined as the ability to find, use and apply health information from electronic sources 18 ). In their study of the eHealth literacy and communication technology use of remote Hawaiian community members, Witten and Humphry 19 found that the eHealth literacy of this population appeared insufficient for proper understanding and utilization of technology. Although not rural-centric, a systematic review of telemedicine adoption suggested that low eHealth and/or a lack of computer literacy prevailed as barriers to widespread implementation. 20 Indeed, eHealth literacy has largely been overlooked in the development of technology-based health interventions, limiting accessibility. 21 Despite the fact that the COVID-19 pandemic has driven a massive shift to telemedicine to decrease person-to-person contact, and slow the spread of the virus,22,23 no research could be found examining the association between eHealth literacy and telemedicine satisfaction among rural patients. Overall, more research is needed examining rural access, use of, and satisfaction with telemedicine during the COVID-19 pandemic, as well as exploring the role of e Health literacy in patient satisfaction with telemedicine.
The purpose of this study was to describe rural health service and telemedicine usage and satisfaction in rural communities during COVID-19 as well as to explore the role of eHealth literacy in telemedicine satisfaction and gather participants suggestions for improving rural telemedicine delivery.
Research questions
What proportion of rural community participants accessed health services, mental health services, and telemedicine during COVID-19?
How satisfied are rural community members with telemedicine?
How is telemedicine satisfaction related to eHealth literacy?
What suggestions do participants have for improving telemedicine in rural areas?
Methods
Study design and participant recruitment
This study employed a cross-sectional online survey from May 29 to July 8, 2020. Participation was open to all rural British Columbia community members community members; however, recruitment efforts targeted those communities where medical services were provided through one of the provincial health regions. The health authority covers a large geographical mass encompassing both urban and rural and remote communities. However, only adults (19 years or older) living in or near a community that would be considered rural or remote (e.g. population less than 12,000 i ) were included. Recruitment efforts involved social media posts (Kijiji, Facebook, Twitter), announcements in rural community association newsletters, advertisements on rural British Columbian websites, and email invitations sent through community networks. To promote participation, three CA$100 and one CA$400 draw prize incentives were advertised. Participants provided online informed consent before proceeding to the online survey. The survey used a combination of fixed and open responses. This study was reviewed and received ethics approval by the University of British Columbia Research Ethics Board (#H20-01166).
Measures
Demographic characteristics of participants
Demographic data collected from all participants included: age, gender, ethnicity/race, and education. We also asked the participants to indicate their community name, and categorized these based on the health authority responsible for health services.
Health care service use
To measure health care service use, participants were asked to answer whether they had a need for health services (e.g. hospital, family doctor, HealthLinkBC ii ) during the COVID 19 pandemic (i.e. since March 18). Those who responded affirmatively were then asked about the frequency of their communication with health care providers since March 18 based on a 5-point scale ranging from Far less often (1) to Far more often (5). Finally, the same group of participants were asked to indicate how they had communicated with their health care providers by checking all that apply: In person, telephone, email, text message, social media (Facebook), Telehealth/eHealth, HealthLinkBC, video-conference (e.g. Zoom, Skype), website, or “I have not communicated with doctors, health care providers or HealthLinkBC during the COVID-19 pandemic.”
Health service access and frequency of use
Participants were also asked a series of questions about which services they had access to such as: Telemedicine, online mental health programs, virtual or phone mental health services (e.g. connecting with someone). Additionally, they were asked how often they used these same services during, compared to before, the pandemic.
Telemedicine use and satisfaction
To understand participants’ engagement with telemedicine, participants were provided with a definition of telemedicine, and asked “Have you used telemedicine?” (yes/no). Those who indicated “Yes” were asked to complete an additional four-items from the Telemedicine Satisfaction Questionnaire (TSQ). 24 These included: “I feel comfortable communicating with my health-care provider via telemedicine”; “I find telemedicine an acceptable way to receive health-care services”; “I will use telemedicine services again”; and “Overall, I am satisfied with the quality of service being provided via telemedicine.” Participants responded to each item on a scale ranging from Strongly disagree (1) to Strongly agree (5). An overall telemedicine satisfaction score was created by taking the mean of the four telemedicine satisfaction items. In previous research, the full 14-item TSQ has demonstrated preliminary validity and reliability. 24
eHealth literacy
Participants were asked to complete an 8-item (e.g. “I know what health resources are available on the internet”) electronic Health Literacy Scale (eHEALS). 18 The eHEALS is “a measure of eHealth literacy developed to measure combined knowledge, comfort, and perceived skills at finding, evaluating, and applying electronic health information to health problems” (p. 1). 18 Previous research using the eHEALS has demonstrated moderate test-retest reliability, good internal consistency and construct validity.18,25 Participants responded to items on a scale ranging from 1 (strongly disagree) to 5 (strongly agree). An eHealth literacy score was created by summing the eight eHEALS items (possible range 8–40).
Telemedicine experiences and suggestions
In addition to the quantitative measures, participants who responded that they had used telemedicine, were asked to respond to an open-ended question about their experiences with telemedicine. We also invited them to provide suggestions to improve telehealth services in rural communities.
Data analysis
Descriptive statistics (frequencies and means/SDs) were used to summarize the data. Pearson’s Chi-square tests, which evaluate whether categorical variables are related or independent by testing the goodness of fit between actual and expected frequencies on another categorical variable 26 were used to examine telemedicine use (yes/no) by gender (male/female). Independent samples t-tests, which examine statistically significant differences between the means of two unrelated groups, 27 were used to investigate age differences in use of telemedicine (yes/no), and whether telemedicine satisfaction differed by gender (male/female) or modality (telephone versus videoconference). Correlations were used to examine relationships between telemedicine satisfaction and age, as well as telemedicine satisfaction, and eHealth literacy. Spearman’s Rho coefficients were reported because the telemedicine and digital literacy response scale were ordinal. Open-ended responses were coded, and thematic analysis was used to determine themes. Quantitative data were analyzed using IBM SPSS Statistics 26 and NVivo 12 was used to analyze the qualitative data.
Results
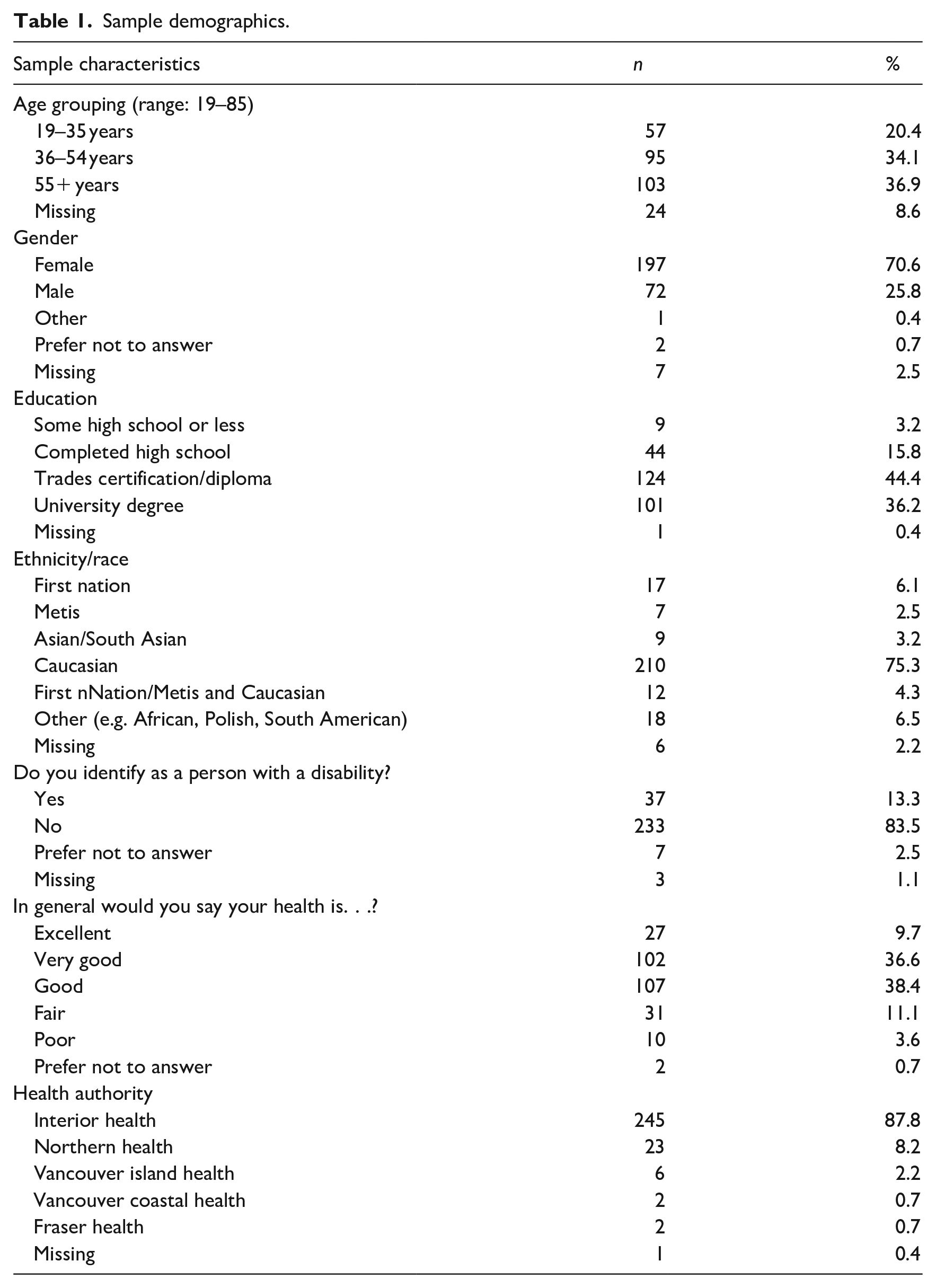
Online surveys were completed by 279 participants (70.6% female) between May 29-July 8, 2020 (6 weeks). The mean participant age was 49.45 years (SD = 14.66). The majority of our participants were middle-age and older adults (71%), Caucasian (75%), with trade certification/diploma or a university degree, (>80%), and self-reported good to excellent health (85%). See Table 1 for a summary of participant characteristics.
Sample demographics.
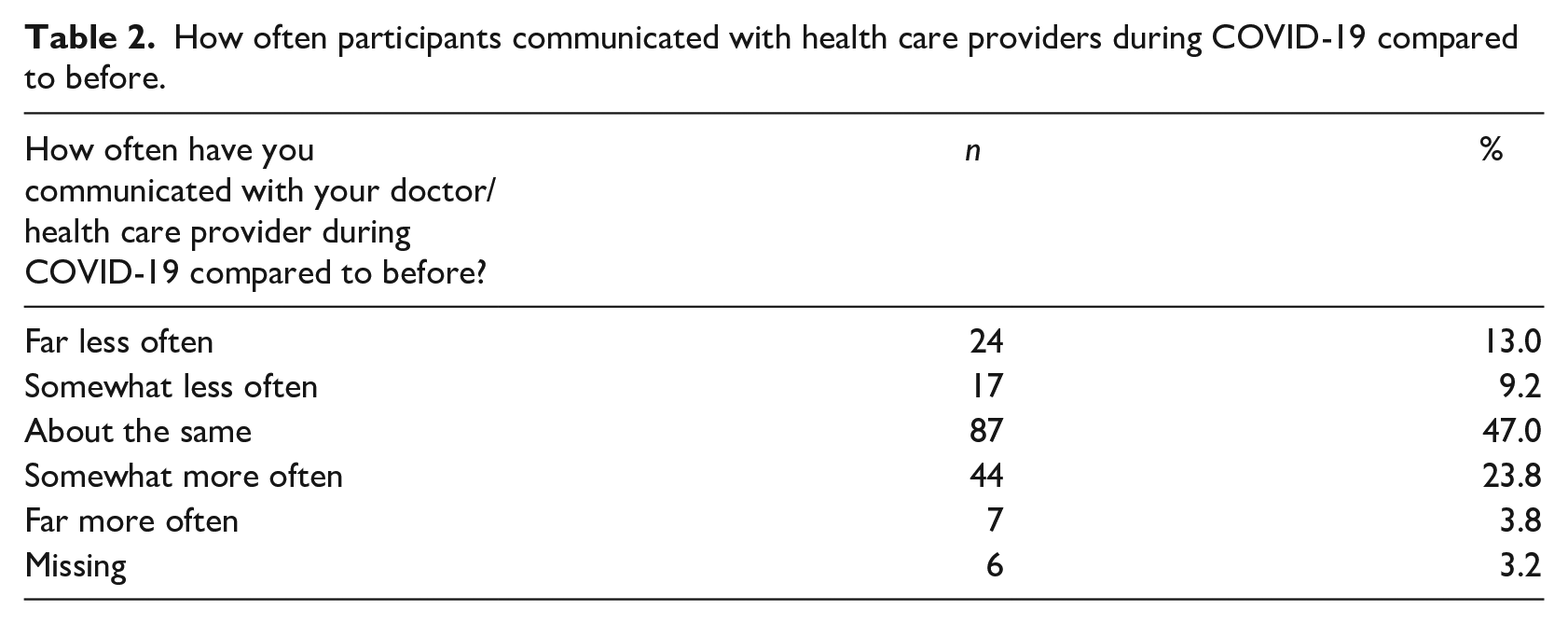
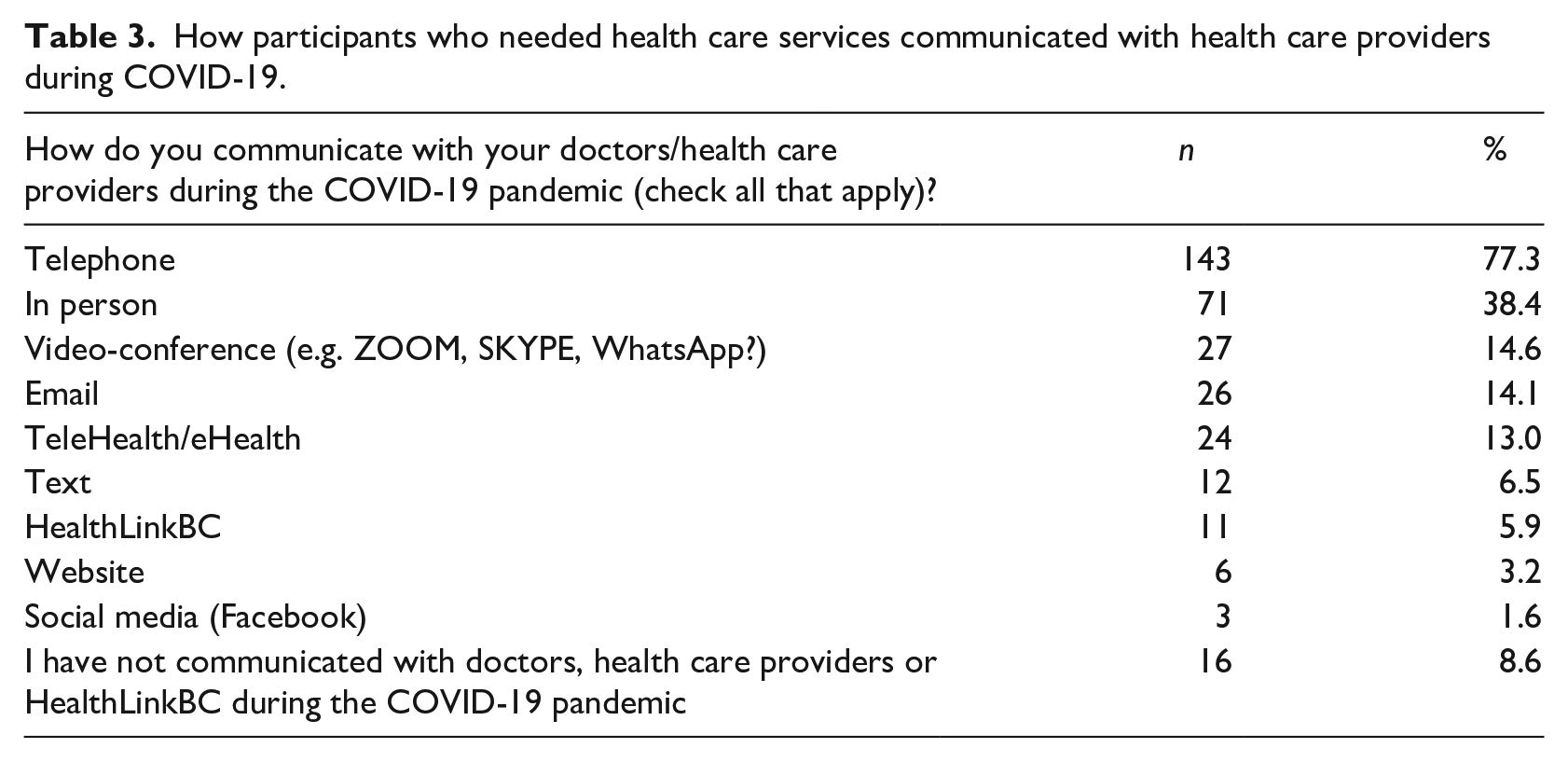
In total, 185 (66.3%) responded “yes” they had needed health care services during the COVID-19 pandemic. Approximately half of these participants indicated that their frequency of communication with health care providers was “about the same” during COVID-19 compared to before (see Table 2). Twenty-two percent of participants had communicated somewhat/far less often, and in some cases, this reduced frequency carried over into pressing issues such as a “lump in my breast because I feel I won’t have access to a mammogram right now.” In contrast, 27.6% of participants had communicated somewhat/far more often during COVID-19 than before. The most frequent mode of communication with health care providers during COVID-19 was telephone, followed by in-person, and video-conference (See Table 3). Despite the fact that this question was only answered by participants who had indicated a need for health care services during the COVID-19 pandemic, 8.6%, had not communicated with health care providers.
How often participants communicated with health care providers during COVID-19 compared to before.
How participants who needed health care services communicated with health care providers during COVID-19.
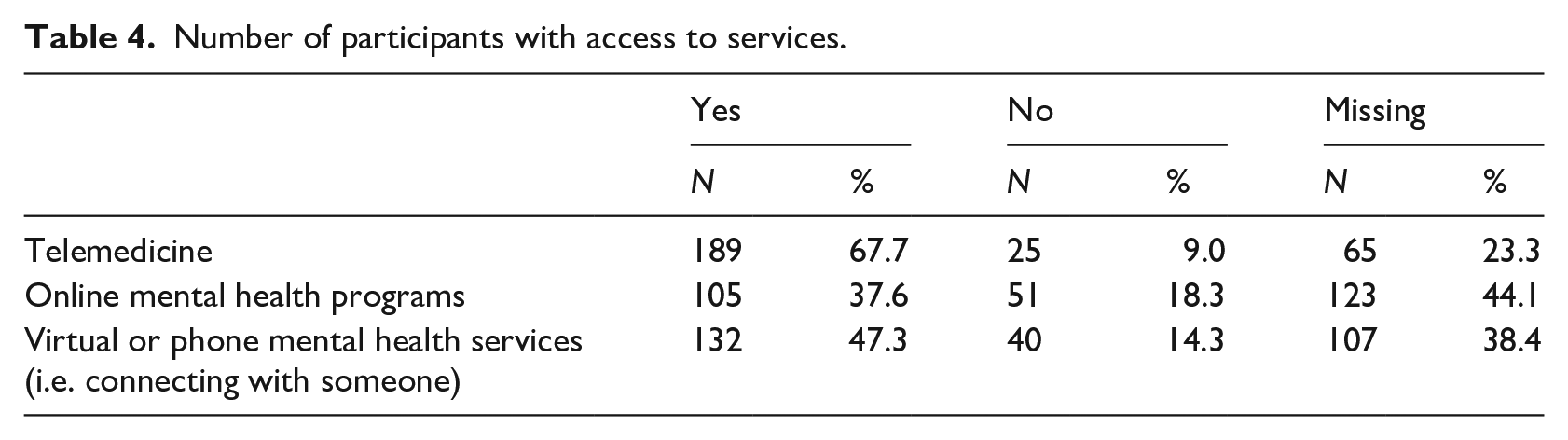
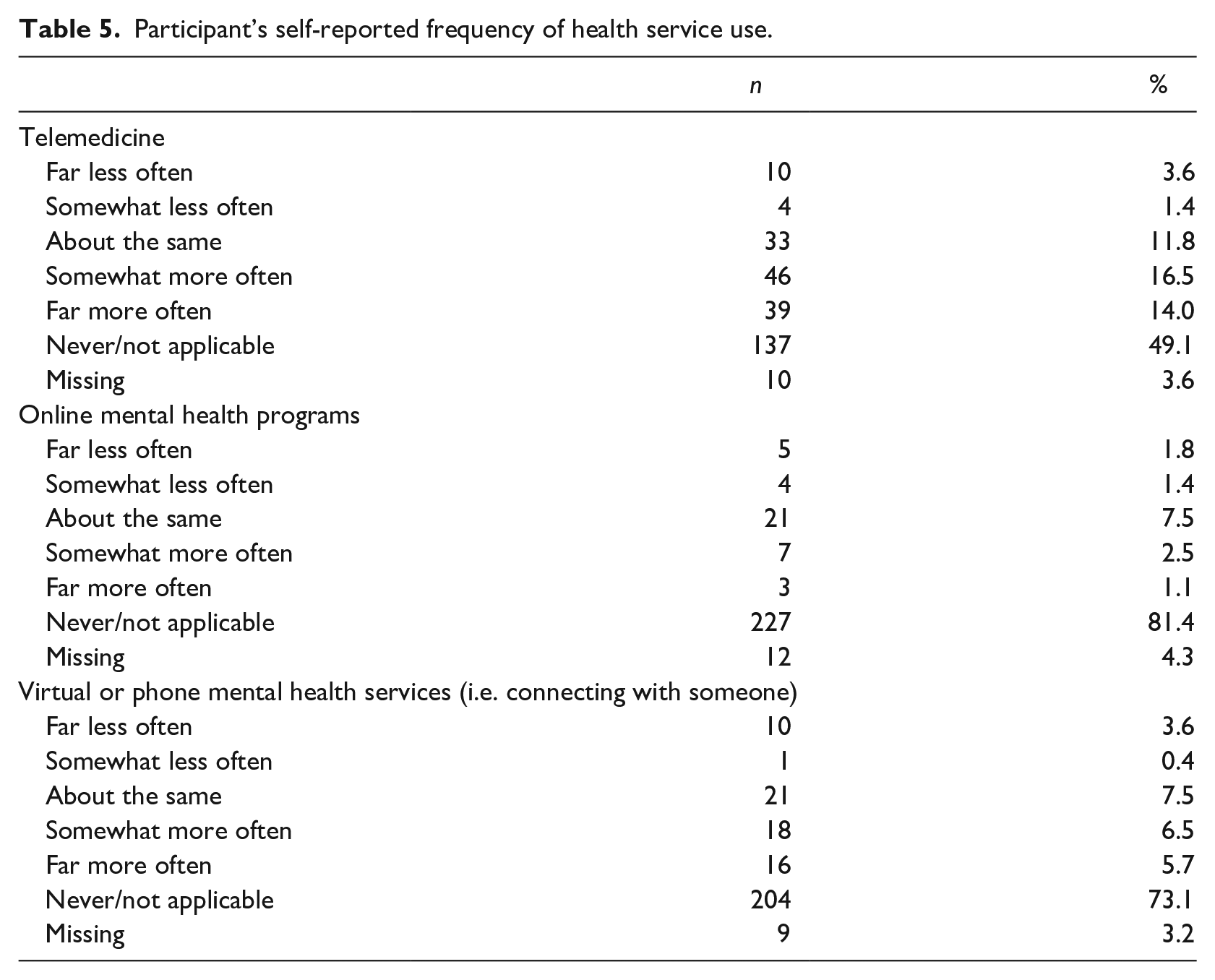
The majority of participants reported having access to telemedicine (See Table 4). Although 18% reported they did not have access to online mental health programming, and 14% did not have access to virtual or phone mental health services, it is important to note that 38% and 44% did not respond either yes or no to these two questions, respectively (see Table 4). In total, 120 (44.1%) of participants responded “yes” they had used telemedicine. The proportion of males (45%) who had used telemedicine was not significantly different from the proportion of females (43%) who had used telemedicine, χ2 = 0.87, p = 0.834. Age did not differ among those who had used telemedicine (M = 51.15 years) and those who had not (M = 48.38 years), t(247) = 1.49, p = 0.138. In terms of frequency of use, 31% of participants reported using telemedicine somewhat and far more often since the start of COVID-19; likewise, 3.6% and 12.2% of participants reported using online or virtual mental health services somewhat more or far more often since COVID-19, respectively (See Table 5).
Number of participants with access to services.
Participant’s self-reported frequency of health service use.
Two-thirds of participants reported that telemedicine was an acceptable service model and were satisfied with the quality. Three quarters of participants felt comfortable using telemedicine and nearly 90% would use telemedicine again (See Figure 1). When the four satisfaction items were summed, 74 (62.7%) of the participants scored a four or higher (i.e. agreed, or strongly agreed). There was no difference in total telemedicine satisfaction scores between men (M = 3.79) and women (M = 3.90), t(111) = 0.51, p = 0.613 and satisfaction was unrelated to age (Spearman’s Rho r = −0.04, p = 0.71). Satisfaction scores were higher for the 24 participants who had used video/video and phone (M = 4.18) compared to the 69 participants who used phone alone (M = 3.79), t(69) = 2.2, p = 0.031.
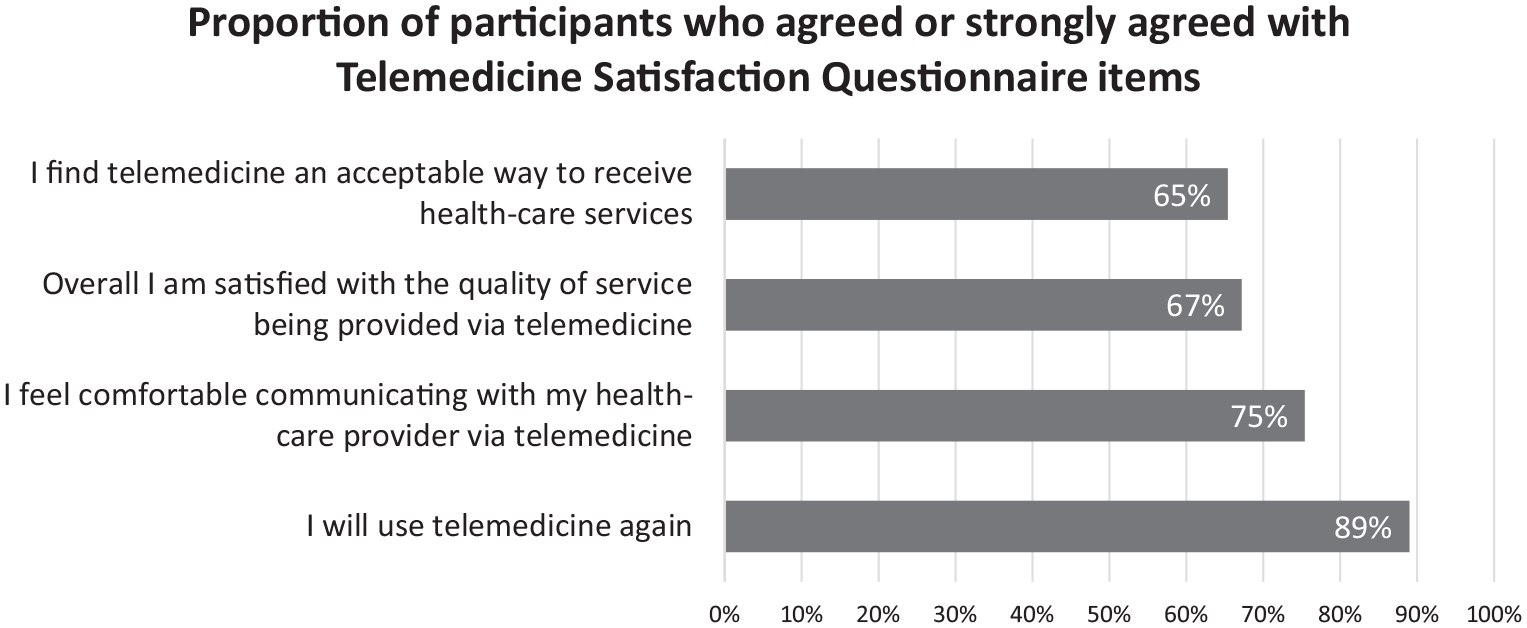
Proportion of participants who agreed or strongly agreed to each of the Telemedicine Satisfaction Questionnaire items.
eHealth literacy and telemedicine satisfaction
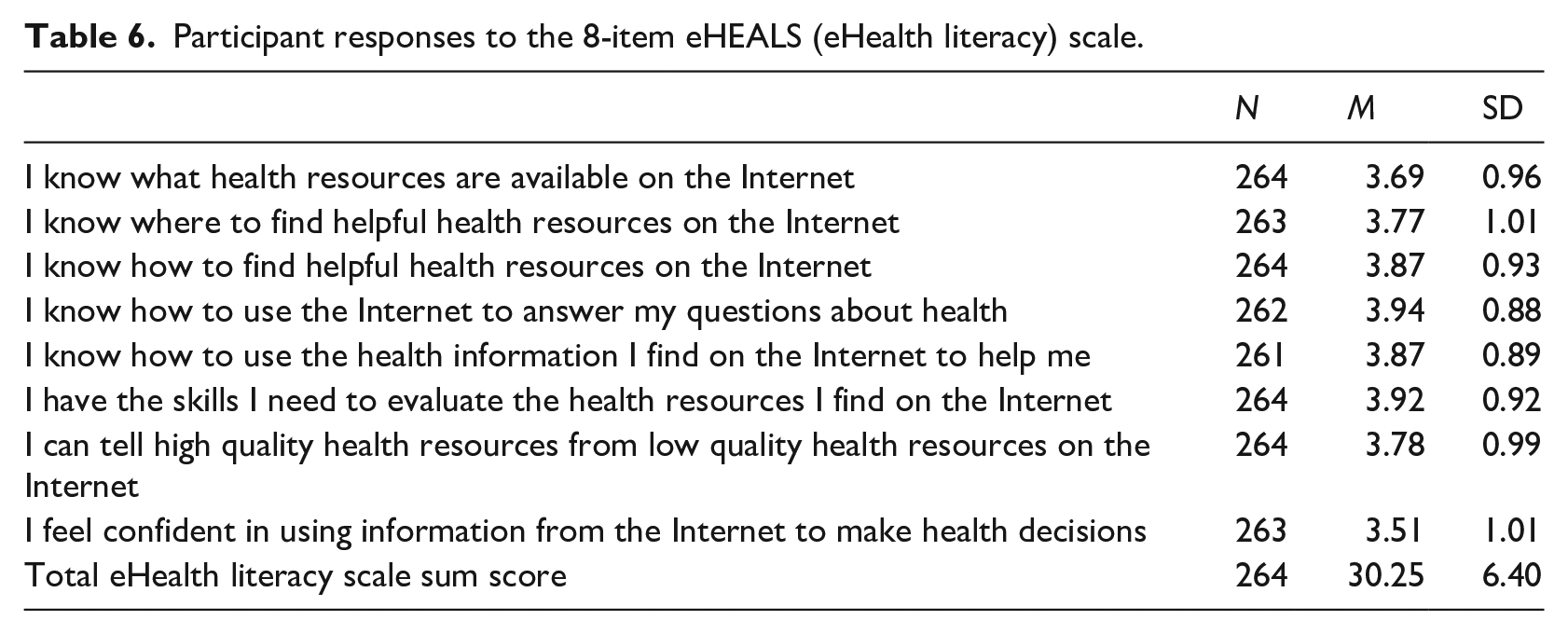
Overall, participants’ eHealth literacy scores were relatively high (See Table 6). Age was unrelated to eHealth literacy (r = 0.018, p = 0.779). Women (M = 30.9) had higher eHealth literacy scores compared to men (M = 28.4), t(100.7) = 2.53, p = 0.013 (mean difference = 2.53, 95% bootstrapped CI .55, 4.41). eHealth literacy scores were higher among those who had used telemedicine (M = 31.09) compared to those who had not (M = 29.53), though this did not reach significance, t(259) = 1.95, p = 0.052. Telemedicine satisfaction was positively correlated with total eHealth literacy scores (Spearman’s Rho r = 0.26, p = 0.005).
Participant responses to the 8-item eHEALS (eHealth literacy) scale.
Telemedicine experiences and suggestions
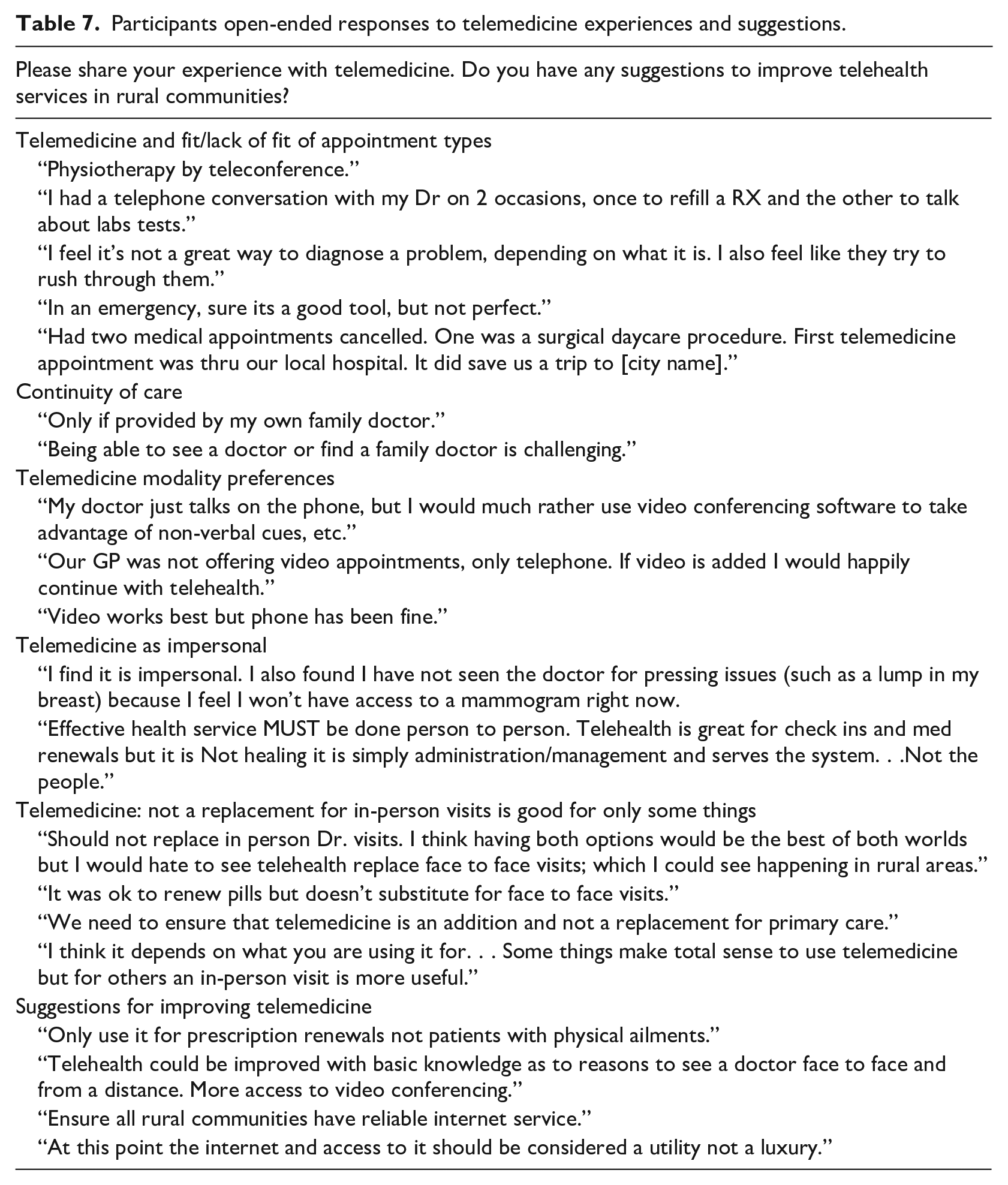
Six themes were identified from the open-ended responses from 79 participants who shared their experiences and suggestions about telemedicine (see Table 7). Participants expressed preferences for seeing their own family doctor, using video over telephone, and some found telemedicine impersonal. In addition, participants suggested that telemedicine should supplement, not replace, in person visits, and that reliable internet access for rural residents was needed.
Participants open-ended responses to telemedicine experiences and suggestions.
Discussion
The purpose of this study was to understand how adult rural citizens were using health care services, specifically telemedicine, during the first 4 months of the COVID-19 pandemic and their overall satisfaction with these services. Two-thirds (66.3%) of participants indicated they needed health care during the pandemic. Although nearly half (47%) of participants had communicated with their physician/health care providers with about the same frequency during, as before, COVID-19, the 22% of participants that had communicated somewhat/far less during than before COVID-19 may be cause for concern. Whether this had consequences for participants is unknown, but evidence from a rural US survey suggested negative consequences when people were unable to get health care. 28 Open-ended responses (to a question about telemedicine experiences) suggested that in some cases participants had delayed accessing services - perceiving them to be either too risky or unavailable - and in other cases participants noted that their appointments and even surgeries had been cancelled to relieve pressure on the healthcare system. The effects of delayed care, whether patient or system initiated, cannot be underestimated. In some Canadian jurisdictions non-urgent procedures and elective surgeries have been postponed for months. 29 The extent and impact of delayed care in Canada is unknown owing to suboptimal health data infrastructure and reporting system for both managing the pandemic and for ensuring everyone’s health-care needs are met. 29 Ensuring that people remain engaged in their health care with the shift to telemedicine is paramount. Findings from this study suggest that access to telemedicine, satisfaction with telemedicine, and e-health literacy may play important roles.
Although the majority of rural participants had access to telemedicine, under half (44%) had used it during the pandemic. This finding is comparable to a United States survey in which 46% of rural households reported using telemedicine for advice/treatment with their doctor or other health care professional by phone, smartphone, tablet, or computer. 28 That close to half of participants reported using telemedicine, may be linked to the older age range of the sample and the possibly of more with chronic conditions, as nearly 15% of participants rated their health as fair to poor. It is well known that rural communities are home to a larger proportion of older adults. In the province where this study was conducted, 25%–50% of the rural populations are 55 years and older. 30
In the current study, telephone was the most common mode of communication, followed by videoconference, texting, and email. Participants who reported using videoconference to connect with health care providers were more satisfied than those who used telephone alone. Open-ended responses were aligned with these quantitative results, with many participants preferring use of video but it was not always an option their physicians offered. Prior work has shown that the video component significantly contributes to quality and satisfaction of the visit. 31 In their retrospective cohort urban-based study, Ramaswamy et al. 32 reported significantly higher satisfaction scores for video visits than in-person visits during COVID-19. Often telephone is the only option in rural communities where the lack of high-speed broad band internet is a major barrier to the use of video-consultations, which have been found to be as effective as in-person care. 33
All participants within the context of this Canadian study have access to free mental health services, which is consistent with their relatively high self-reported access to online mental health programs and virtual services. It is of concern that nearly one fifth of participants reported lack of access to virtual mental health services at a time when there has been a well-documented increase in the need for these services. 34 For rural participants it is quite likely they did not have access to minimum broadband speed; only 37% of rural households in the province where the study was conducted had access to the minimum broadband speed necessary to support high quality video conferencing or online learning in 2017. 35 Despite Provincial government commitment to a Digital Health Strategy and investment expanding high speed internet to more rural communities in recent years, 36 performance testing conducted by the Canadian Internet Registration Authority in July 2020 suggested that rural internet speeds have plateaued at 5.5 Mbps (compared to 51.5 Mbps in urban areas) since the start of the COVID-19 pandemic. 17 However, it is also possible participants lacked awareness of the mental health services available despite provincial and federal investments in mental health resources. 34 That between 38% and 44% left the access to mental health services questions blank could suggest a lack of knowledge about these services. These participants may also not have needed the services and therefore were not aware of them. The vast majority did not use the services but a sizeable number used them more during than before COVID-19 (3.6%–12.2%). This usage resonates with a national survey that found that 50% of Canadians reported worsening mental health since the pandemic with 10% reporting a worsening of their mental health by ‘a lot’ as a result of COVID-19. 37
Rural participants in the current study had relatively high levels of satisfaction with telemedicine. Similarly, 88% of rural households in the United States reported wide satisfaction with telemedicine visits and the most recent advice or treatment they had received. 28 Similar to the current findings, Kruse et al. 20 identified the effectiveness and efficiency of telemedicine in contributing to patient satisfaction. However, a third of participants in the current study were not satisfied with the acceptability and quality of telemedicine care. Open-ended responses centered around ensuring telemedicine is a supplement, not replacement for, in-person care. The mixed findings reflect the need for providers to integrate telemedicine into their usual practices where appropriate while balancing the need to maintain the personal and human touch that study participants found challenging with telemedicine.
It is possible that individuals with higher eHealth literacy are more willing to use telemedicine. Our results suggest this pattern, with those having used telemedicine having higher levels of eHealth literacy, however, this did not reach significance. A unique and important finding from this study is the positive relationship between telemedicine satisfaction and e-health literacy. As COVID-19 has catapulted us into greater reliance on telemedicine, it is imperative that rural citizens possess the knowledge, comfort and abilities to find and use information and digital tools. Indeed, the digital divide encompasses more than just access to broadband connectivity, but also the tools, ability, and willingness to engage with virtual solutions. 38 Building rural residents’ capacity to understand and have personal and technical comfort with the receipt of health care through technology will need to involve telemedicine literacy training and support. 38
Limitations and future research directions
Responses were from participants who completed an online survey, excluding the perspectives of those without internet access or tools to access the internet (both hardware or ability). Telemedicine use may differ for those without access to broadband connection, which even for many who used the services was not stable and reliable. The survey was administered during the summer months when there was some respite from COVID-19. 39 The Provincial re-start plan (currently on pause with Province-wide restrictions in place) meant more people were returning to work, restrictions were being loosened, and provider practices opened for more in-person visits, 40 perhaps influencing responses. The primarily white, female, and well-educated sample with good to excellent self-reported health may not reflect the broader rural demographic. Thus, eHealth literacy scores may not generalize to other rural community members. Information about the satisfaction of those who did not access telemedicine was not obtained, limiting insights into unmet needs.
Future research could focus on the impact of the digital divide41,42 on rural health equity during and after the COVID-19 pandemic. Survey participants were rural citizens in general but future research might target “at-risk” populations such as those with chronic diseases, mobility issues, mental health challenges, and substance use, known to be more prevalent in rural communities. 43 As COVID-19 has intensified mental health needs in general, 37 it would be valuable to explore rural residents need for these services relative to their knowledge of and access to services. This will allow researchers and health care providers to better understand the discrepancies between access and usage of telemedicine relative to population needs in rural settings. The importance of e-literacy to telemedicine satisfaction warrants further research, particularly interventions to train and build capacity especially for those where e-literacy is low.
Conclusion
In conclusion, during the COVID-19 pandemic, two thirds of rural residents in a Canadian western province self-reported having a health care need, the majority had access to telemedicine, and just under half had used it. Compared to pre-COVID-19, self-reported telemedicine use had increased during COVID-19 as had use of mental health online programs and virtual services. E-Health literacy was positively associated with satisfaction with telemedicine. Yet, rural citizens also experienced challenges with telemedicine access due to unreliable/unstable internet and found the service impersonal. The lack of digital infrastructure is an ongoing concern for rural communities if they are to experience health care equity comparable to their urban counterparts. If telemedicine is to be incorporated into practice during and following COVID-19, it is important to ensure that rural residents have the support needed to engage with this form of remote care.
Footnotes
Acknowledgements
The authors want to thank the rural community participants who participated in the survey.
Declaration of conflicting interests
The authors declare no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the University of British Columbia Okanagan’s Eminence Program [GR015968, 2019]; and the Regional Socio-Economic Development Institute of Canada Fund [62R34654, 2020]. The funders were not involved in the design or write-up of this study.