
Abstract
There is a strong push towards standardisation of treatment approaches, care processes and documentation of clinical practice. However, confusion persists regarding terminology and description of many clinical care process specifications which this research seeks to resolve by developing a taxonomic characterisation of clinical care process specifications. Literature on clinical care process specifications was analysed, creating the starting point for identifying common characteristics and how each is constructed and used in the clinical setting. A taxonomy for clinical care process specifications is presented. The De Bleser approach to limited clinical care process specifications characterisation was extended and each clinical care process specification is successfully characterised in terms of purpose, core elements and relationship to the other clinical care process specification types. A case study on the diagnosis and treatment of Type 2 Diabetes in the United Kingdom was used to evaluate the taxonomy and demonstrate how the characterisation framework applies. Standardising clinical care process specifications ensures that the format and content are consistent with expectations, can be read more quickly and high-quality information can be recorded about the patient. Standardisation also enables computer interpretability, which is important in integrating Learning Health Systems into the modern clinical environment. The approach presented allows terminologies for clinical care process specifications that were widely used interchangeably to be easily distinguished, thus, eliminating the existing confusion.
Keywords
Introduction
Care process specification, also described as care process modelling, arose from a need to evaluate the quality of healthcare delivery.1,2 Documentation of care processes is said to result in healthcare quality improvement as it helps those involved in patient care to develop a shared understanding of care to be provided, and a reference point for identifying areas for future improvement.3–6 The intention is to ensure that services being provided to patients deliver the desired health outcomes consistent with current clinical knowledge. 2 Deviation from those quality standards established in the care process specification (described as variation), is the driving force making adaptation of change in any given care process specification necessary. 7
A wide range of terms exist for what we describe collectively here as clinical care process specification (CCPS) documents, each of whose remit could generally be described as the documentation of care processes for improving healthcare quality and outcomes. These terms include: clinical practice guidelines (CPG) 8 which are sometimes also known as consensus-based guidelines (CBG) 9 and local operating procedures (LOP),10,11 clinical decision rules (CDR), 12 clinical pathways, 13 care plans, 14 treatment protocols (TP) 15 and caremaps 16 which in their contemporary form share some similarities with clinical algorithms dating from the early 1980s. 17 A key issue limiting the effectiveness of these tools is lack of agreement on whether some of the titles described above represent distinct clinical documents,18–20 or are synonymous.18,21–23 Furthermore, standardisation of definitions, presentations and development processes for most types of clinical documentation have either been incomplete or only added to the confusion.16,18,24,25
The British Medical Association and Royal College of Nursing developed a joint guidance stating that use of standardised forms is beneficial in reducing variation in healthcare practice. 26 The use of different versions of the same clinical care specification in different units within the same care facility, and between different care facilities, may not previously have been seen as such an important issue. However, in this increasingly digital healthcare environment we are seeing greater amounts of data being generated and captured daily, including from diagnostic devices used, or sensors worn, by the patient while in the community. Any differences in the documentation approach or data recording method results in fragmented data, complicates the integration of data about the same patient from different sources and inhibits health information exchange (HIE).27,28
Even though standardisation of healthcare practice, procedure and tools can improve healthcare quality, outcomes and accountability, there remains significant resistance to its implementation.16,29,30 This is not surprising, as the issue of distinguishing these clinical tools persists. 16 We have sought to resolve the disagreement in the distinction between these terms using extensive literature review and input from a wide range of clinical experts to identify a taxonomy and characterisation, with specific attention focused on identifying differences and similarities for a range of common clinical document types. We address the problem of a lack of standardisation of terminology and formalisation of specifications of clinical care processes, and aims to investigate a taxonomy and a way to characterise CCPS documents to: (1) identify and formalise the definition, structure, content and in later works, development process for each and (2) contribute towards the standardisation of the terminologies used when referring to these documents. In addressing the problem and achieving the aim of this work, this article has the following three objectives:
Produce a taxonomy based on all of the terminologies that are used to represent CCPS documents, to aid in resolving the confusion observed in the literature regarding whether these terms are synonymous, similar or representation of distinct clinical specifications.
Characterise each CCPS, so that readers can identify that if a document has these properties, then it must be this type of CCPS. Specific questions associated with this objective are: What are they composed of? What are the common and unique elements? Can we develop a descriptive terminology, definition and demonstrate the structure of each based on our review of the literature, their individual domains and overall use case?
Evaluate the characterisation framework through application, for example, clinical artefacts from a hospital or clinical provider.
Background, context and problem
Why clinical documents were developed?
Many of the clinical documents, or tools, reviewed in this research were developed and refined during the 1980s and 1990s in response to a number of key needs, including the need to control costs and to improve the quality of patient care.31–33 Using project management (PM) and total quality management (TQM) tools more common to industry, hospital managers sought to reengineer the processes of hospital care to reduce clinical resources and error rates, and improve patient outcomes.20,33–35 However, clinical costs continued to increase, and error rates persisted with distressing frequency. 36
The move to standardisation
In the early 2000s, the focus of hospital management and clinical literature shifted towards the theme of standardisation. Researchers, politicians, those engaged in hospital governance and some clinicians recognised that standardisation should be considered to be of paramount importance. 37 They sought to achieve standardisation of such things as clinical decisions, diagnostic and therapeutic methods, evidence-based guidelines, care approaches, practice standards and clinical information.32,36–39 Standardisation in the name of quality care and outcomes would become the single-minded national focus of healthcare service delivery for entire countries.32,39 This type of standardisation has been promoted with such passion that multiple teams within the same country, or even within the same organisation, can be seen developing standardisation frameworks with some level of similarity and overlap.40–42 Overall, this drive towards standardisation has had little effect on the definition, development and structure of clinical documentation. As we approached the end of the first full decade of standardisation, calls for standardised clinical care documents continued to increase,16,39,43–45 and an unmet need was also identified in calls to resolve poorly standardised taxonomy and nomenclatures being used in developing and cataloguing some clinical documentation. 46 When disagreement persists in the literature resulting directly from the lack of standardisation in the nomenclature, definition and structure of these documents, efforts to standardise healthcare services using them will continue to fall short of expectation.
Methodology and approach
A search was conducted using Scopia, Science Direct, PubMed, EBSCOhost, DOAJ and Elsevier for literature discussing the definition, development or use of a range of clinical document types including: caremaps (caremap, care map and CareMap), pathways (care, clinical and critical pathways), guidelines (CPG), plans (care plans), rules (CDR), and protocols (care protocol). In each case literature was sought where authors had attempted to: (1) define the document type, (2) detail the inputs used in development (evidence, literature, team composition, etc.), (3) identify the intended patients, conditions and audience, (4) detail the aim, goals and intended outcomes and (5) highlight potential benefits and barriers encountered during development and operationalisation of the document. The literature was used in partnership with several different but compatible research methodologies to meet the objectives shown in Table 1.
Mapping methodologies to deliverables and objectives.
Content and thematic analyses
Concept analysis (CA) and thematic analysis (TA) are separate but interrelated qualitative approaches for descriptive data analysis with low levels of interpretation. 47 CA is an accepted systematic coding and categorisation method for investigating texts and resolving quantitative description of the features.47,48 CA first establishes categories and then records the instances in which that category is evident or can be inferred from within the collected texts being analysed. 48 TA is a more qualitative method used to identify, analyse and report patterns, or themes, that emerge as being important within the material being analysed.47,48 TA provides the systematic element characteristic of CA, and can also combine analysis of frequency with analysis of in context meaning, therefore providing a more truly qualitative analysis. 48 CA and TA are established methodologies regularly used in clinical, nursing and other healthcare research contexts.47–50
The literature review resulted in spreadsheets with the details and a brief description of each article. CA was then used to data mine the literature to inductively develop a list of concepts that were used either in discussion of the particular CCPS document, or which were a structural component of examples provided or included by the authors. These concepts were used to populate the spreadsheets in the format of formal CA charts.51–53 TA extended these with context, collecting together examples of where different authors represented the same general idea in a variety of ways or with differing language, and thus making each concept of interest identified in the literature more generic by describing it based on its underlying theme.
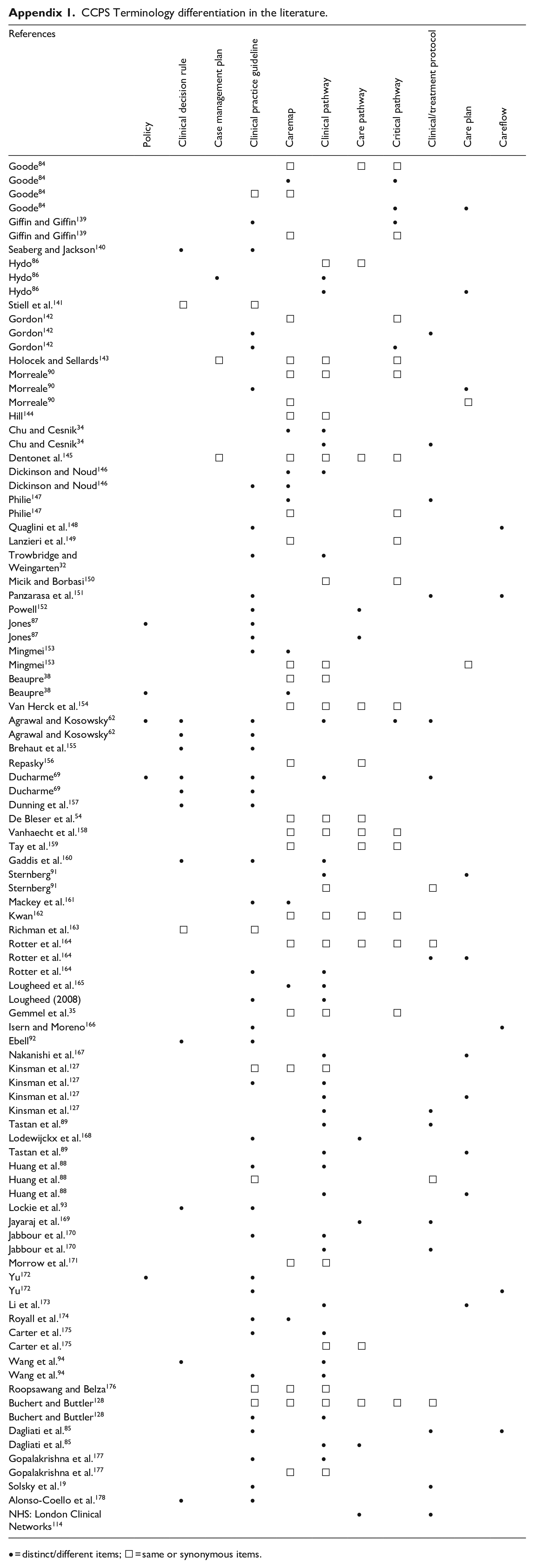
To identify the scope of author positions on whether CCPS documents were the same or distinct, we collected data on how authors described and discussed them in this context as shown in Appendix 1. Where authors described a document type as also known by, or was the same as another, these were indicated with an unfilled square. Where they provided narrative that differentiated or distinguished different types, this is indicated with a filled circle. Separate rows are used to record subsequent instances identified in the same text being reviewed. In our primary spreadsheet we also collected any definitions authors provided for each document type, as well as descriptions of input materials, goals, uses and whether they provided an exemplar document for the reader.
The expanded De Bleser approach
As part of our methodology, we viewed CCPS documents as consisting of elements that can be represented along continuums describing either their (1) degree of prescriptiveness or (2) input to healthcare quality improvement. De Bleser et al. 54 identified both the continuum and their elements which they applied in development of a characterisation framework for clinical pathways only. The continuums and their elements were presented on two axes: an y-axis with elements describing levels from current practice to healthcare quality improvement, and the x-axis ranking elements from descriptive to prescriptive.
Drawing on De Bleser et al’s framework, we extended De Bleser’s coordinate system approach for use in describing CCPS documents’ evidential and practical application, that is, the addition of an hierarchy of CCPS based on the strength of systematically developed evidence contained within the document along a virtual z-axis describing how applicable the document is to the conduct of patient care, as illustrated in Figure 1.
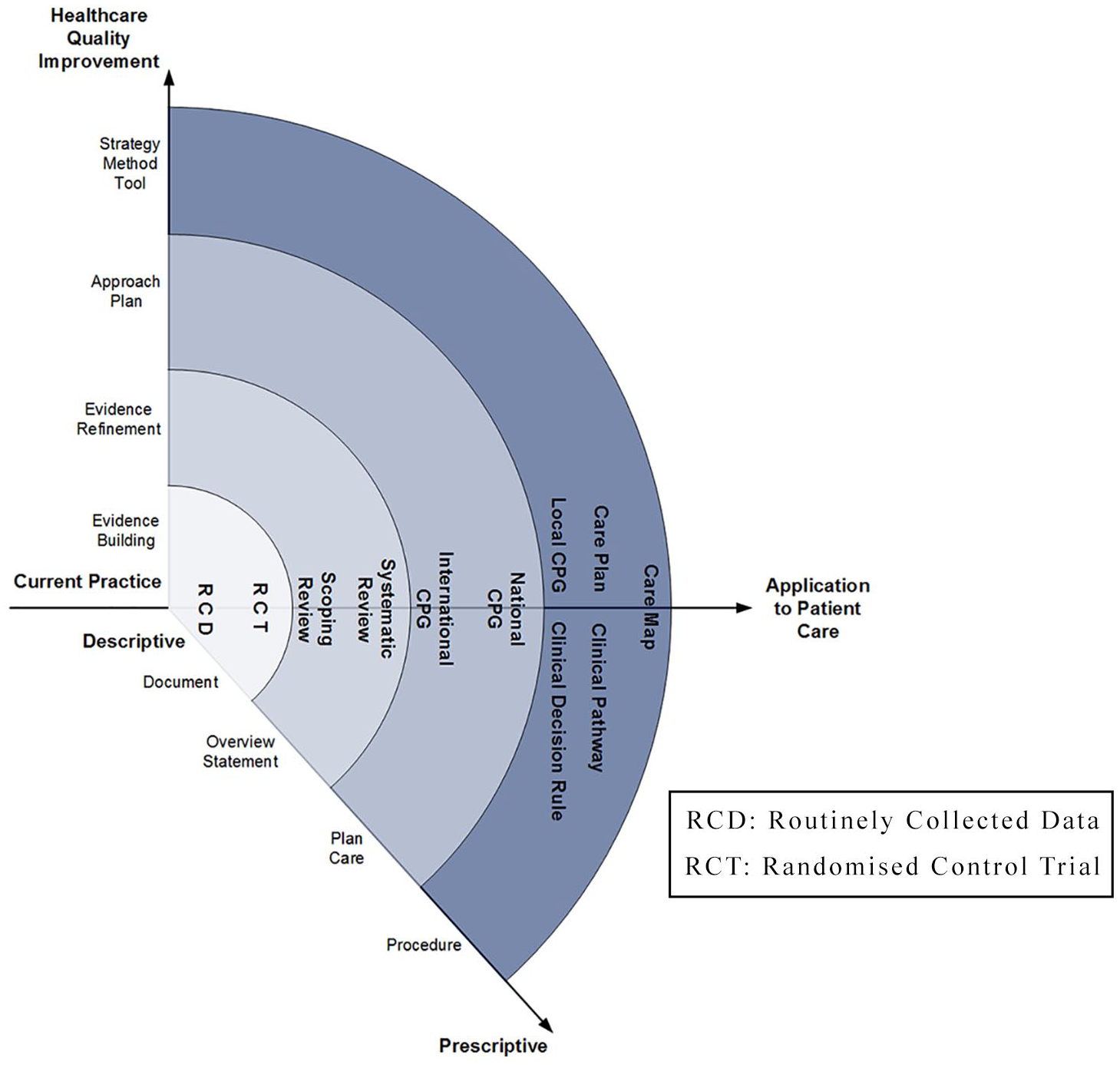
The expanded De Bleser approach.
Evaluative case study
The taxonomy and CCPS document characteristics through a case study using specifications for diabetes care. The case study approach provides a real-life perspective on observed interactions and is regularly used in information sciences.55–58 Case studies are considered as developed and tested as any other scientific method and are a valid method where more rigid approaches to experimental research cannot or do not apply.59–61
Results
The taxonomy for evidence-based clinical care processes
In developing the taxonomy shown in Figure 2, we considered all instances identified in the table in Appendix 1, along with authors’ definitions and descriptions of each document type and input from our clinical experts. The taxonomy identifies the categories of clinical documents we determined from our review as being unique or distinct, as well as a hierarchy for how authors described each as being derived from, dependant on, or acting as a component of another. A solid connecting line, or arc, represents where a strong and direct, almost, parent–child relationship was resolved from the literature. A dashed connecting arc represents those instances where an indirect relationship was inferred from authors’ narratives. Each document type and their described interrelationships are discussed in the following section.
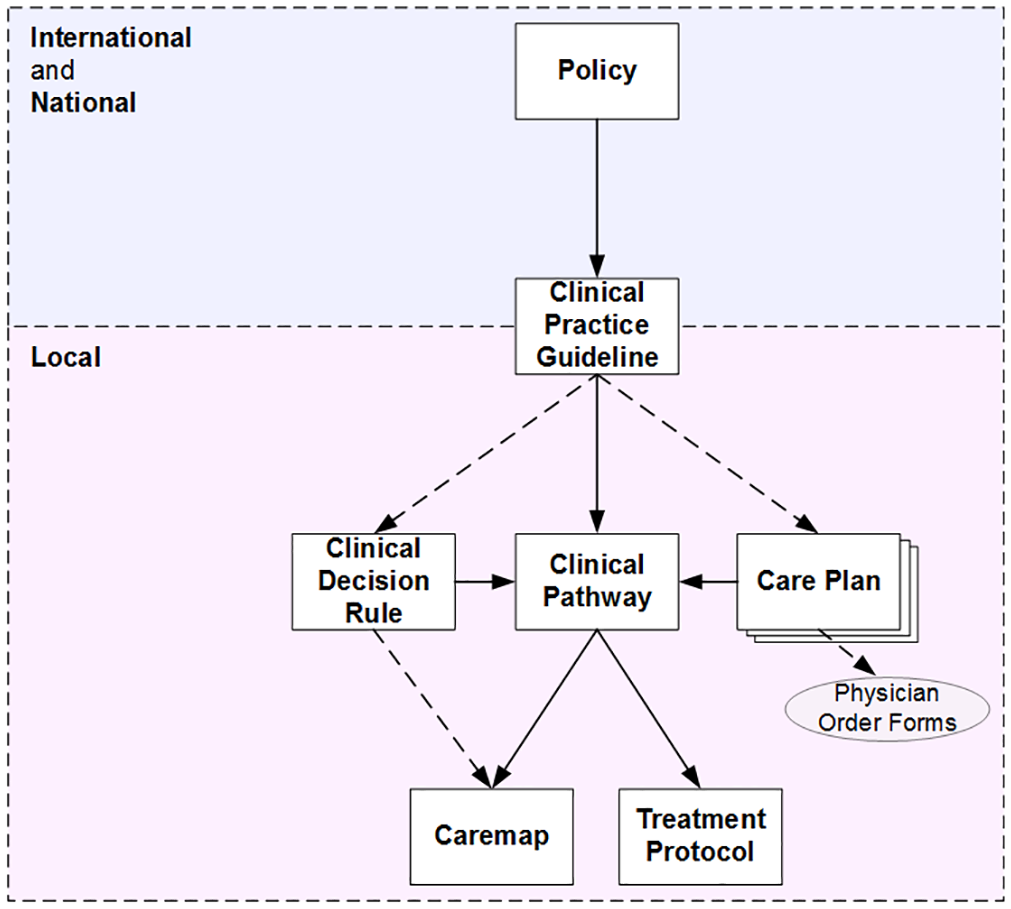
Taxonomy and hierarchy for clinical care process specification documents.
There is a notable relationship between this taxonomy and the expanded De Bleser model in Figure 1, especially in the hierarchy of systematically developed evidence described on the z-axis. In both cases, the clinical care specifications naturally fall in order of clinical, or operational, usability.
Policy
Policy was the most fundamental and formative document identified. Because policymaking can be driven or impeded by highly charged and competitive political ideologies and value systems, the resulting policies are not always based on clear and convincing scientific evidence.62,63 International and national organisations can also give rise to health policy.64–66 Policy can be applied at both a national and local level, with local policies often being representative of aspects of national or regional policy made relevant to specific local populations, whether based on ethnicity, age or disease criteria.66,67 Policy can directly determine a population’s health and health outcomes, especially where it is used to guide regulation of the distribution of specific types of health service in terms of human and material resources, how those healthcare services are funded, and the accessibility of those services for patients.66,68
CPG
It is generally accepted that CPG are systematically developed statements based on critical assessment of scientific evidence, experience and consensus and are intended to aid in decision making about appropriate care for patients in specific clinical circumstances.62,69–71 CPGs seek to provide clinicians with a vital shortcut to identifying the underlying science that informs particular clinical decisions. 70 Our review identified a hierarchy for CPG: (1) global, (2) national, (3) regional and (4) local. We also established other possible perspectives such as that of levels of customisation in which one guideline may exist at each level as a customised instance of a version at another level. Furthermore, in such a view, a CPG may originate at any level such that customisation may occur as a generalisation or a specialisation process to suit a population or an individual, respectively. Thus, a health facility–based CPG may become regionalised or nationalised or globalised while global CPG may be nationalised or regionalised or localised at a healthcare facility through customisation, that is, generalisation or specialisation, respectively. A key point to note here is that as you move from global, through national and regional, to local, the patient population for which the CPG applies reduces and becomes less heterogeneous while the guideline becomes more specific as a result of customisation.
Global guidelines are international guidelines published by organisations such as the World Health Organization (WHO)72,73 and World Federation of Haemophilia (WFH) 74 and multinational guidelines, sometimes described as CBG or consensus statements from groups like the European Society of Cardiologists (ESC). 75 International and multinational guidelines tend towards general or globally applicable recommendations for the diagnosis or management of specific conditions or clinical presentations.
In combination with local synthesis of evidence, global guidelines are regularly used in the production of national guidelines, which are endorsed for and intended to inform consistent clinical care across entire countries or health sectors.76–78 Given that there are a limited number of countries with sufficient infrastructure and financial resources to support committees and organisations that develop national guidelines, it is not unusual to observe the national guidelines of countries like the United Kingdom or Canada being used to support production of local guidelines in small countries like New Zealand.
Regional guidelines draw on health policy and national guidelines in the production of a more operationalised form of CPG dealing with demographic population needs in specific states, counties or municipalities. 79
Local guidelines is the term we are using to represent those CPG (recently termed LOP) in some Australian and American hospitals) that are developed and used directly in hospitals, general practice clinics and other patient-facing locations. They provide operationalised and instantiated evidence and clinical knowledge drawn from regional, national and global guidelines and are targeted to support and improve clinical decision-making and care delivered directly at the patient’s bedside; 79 they may also consider the cost of treatment in relation to the local budget for health implementation. Patients with the same condition sometimes receive different treatment at different hospitals, as different healthcare providers may disagree on what the best evidence may be in a given situation. 80 For this reason facility, or local, guidelines may also reflect particular elements of organisational culture, and it is not unknown for hospitals to amend guideline diagnostic or treatment threshold values either (1) to make the guideline more approachable to clinicians and increase adherence, (2) as a response to elements identified from previous clinical errors, (3) where based on past experience, senior consultants feel it may aid in the avoidance of future poor patient outcomes and potential litigation79–82 or (4) for local health economic considerations.
Clinical pathway
Although CPGs and clinical pathways both provide a defined approach for a specific medical condition or treatment process, clinical pathways were a separate care process specification applied to healthcare practice in the 1980s with an additional focus on (1) the use of benchmarked outcomes, (2) cost containment through efficient resource use and (3) management of patient care within a structured hospitalisation period and reduced length-of-stay (LOS).83,69
Our work revealed that clinical pathways were the term most often described as being the same or synonymous with others studied in this review, predominantly with caremaps. They were also the term most often distinguished as different from others, especially CPGs. We also identified an issue of confusion within the literature as to whether clinical pathways, critical pathways and care pathways represented the same22,54,84 or distinct62,85 specifications. As part of the work on this article, an attempt at analysis of the various definitions was made. Given significant variance in defining elements used across the literature pool, the resulting definition was not probative and had potential to increase the confusion. Although some works provided simple and direct statements on the format, describing their particular pathway as a paper-based document or blueprint,34,86,87 others gave more comprehensive descriptions discussing systematic use of clinical evidence, the types of clinical staff and motivations driving the development and use of pathways.35,54,88
There was very limited evidence from which to infer the existence of minor operational differences between the three. In our analysis, the term critical pathways was observed more often in situations where the care is short, intervention- or event-based and relatively urgent, that is, in emergency medicine, surgical or intensive care domains. 84 The term care pathways was observed more often in the nursing domain to describe the day-to-day routine of care provided for patients. And clinical pathways appeared to be more broadly applicable, in that they often sought to address a wider range of patient issues than just this particular illness or clinical presentation and were observed across a range of care domains including: nursing, oncology, community-based care and mental health. Despite potential for these minor operational distinctions we believe it could be disingenuous to identify pathways as three separate objects. De Bleser et al. 54 also investigated the nomenclature issue for pathways, determining that while critical pathways was the internationally accepted term, more than half of all authors in their study had shown a preference for clinical pathway. For all these reasons our taxonomy treats them as a single term, clinical pathway.
Care plan
Care plans are an organised multidisciplinary day-by-day lists of care activities with intermediate outcome-based goals that healthcare providers will undertake to support identified patient problems.84,89 A clinical unit may have a care plan specified for patients with particular medical problem, for example, caesarean section, 84 community-acquired pneumonia 90 or stroke. 86 However, as care plans are specific to the patient they can only become prescriptive once the nurse or clinician has assessed that patient’s particular deficits and needs. 88 An implied relationship exists whereby the care plan may draw knowledge of the condition from the CPG, as indicated in Figure 1 by the dashed line. However, in practice care plans include no supporting literature or knowledge gained from retrospective chart or patient record reviews that would justify the practices used as part of the plan. 90 Care plans are a constituent component of the clinical pathway,84,89,91 and due to their prescriptive and scheduled nature, are credited as the component used to achieve reduced LOS. 90
Clinical decision rule
CDR help clinicians in their decision-making role by providing a link between published and clinical evidence, best practice and the diagnosis or clinical outcome under consideration.62,92,93 CDRs draw on evidence from guidelines to provide operationalised and efficient approaches to assessing probabilities for diagnostic, treatment and prognostic decisions integrated into the clinical pathway.69,92–94 The rules help to establish pretest probability, provide simple screening tests for common problems and estimate risk.62,95
Caremap
Caremaps have undergone a number of transformations since their inception in the mid-1980s. Traditional caremaps of the 1980s and early 1990s were heavily text-based holistic documents that, similar to clinical pathways, were concerned with restoring the entire patient to normality. 16 Transitional caremaps of the late 1990s and early 2000s were text with some early diagrammatic examples of the flow of care but narrowed their focus to the patient’s primary condition and entire hospital stay event while focusing on cost containment and resource consumption. 16 And the contemporary caremaps of today present as informative flow diagrams that present the sequence of activities and potential outcome paths for a single diagnostic, screening and/or intervention event. 16 Versions of clinical algorithm that are more alike contemporary caremap diagrams 96 are often observed appended to CPGs and clinical pathways, providing clinicians with a simple diagrammatic flow of the clinical decision paths evidenced within the main document.
Treatment protocol
Known variously as clinical, care or TP, these are standard descriptors of clinical care activities developed on the basis of guideline-based evidence, and usually found incorporated into clinical pathways and described against a timeline.34,97 Examples of TPs for severe acute respiratory syndrome, 98 post-resuscitation care, 99 lung donor treatment 100 and rhabdomyolysis-based renal failure 97 show the structure of these to treatment steps arranged in sequence for a particular clinical presentation. Some also include outcome assessment factors for evaluating the success of protocol application or for consideration of whether to move the patient onto more aggressive treatment options.98,99 Given the structure and presentation of TPs, many have potential for description using the graphical formalisation of the caremap.
Characterisation of evidence-based clinical care processes
Table 2 provides a characterisation for CCPS based on their presentation, structure, the population they effect and their clinical intention. It also positions each document with reference to De Bleser et al.’s continuums or axes: the x-axis (descriptive/prescriptive) and the y-axis (healthcare quality improvement). And finally, it aligns the six clinical CCPS on a continuum in order of operational usability.
Characterisation framework of clinical care process specification documents.
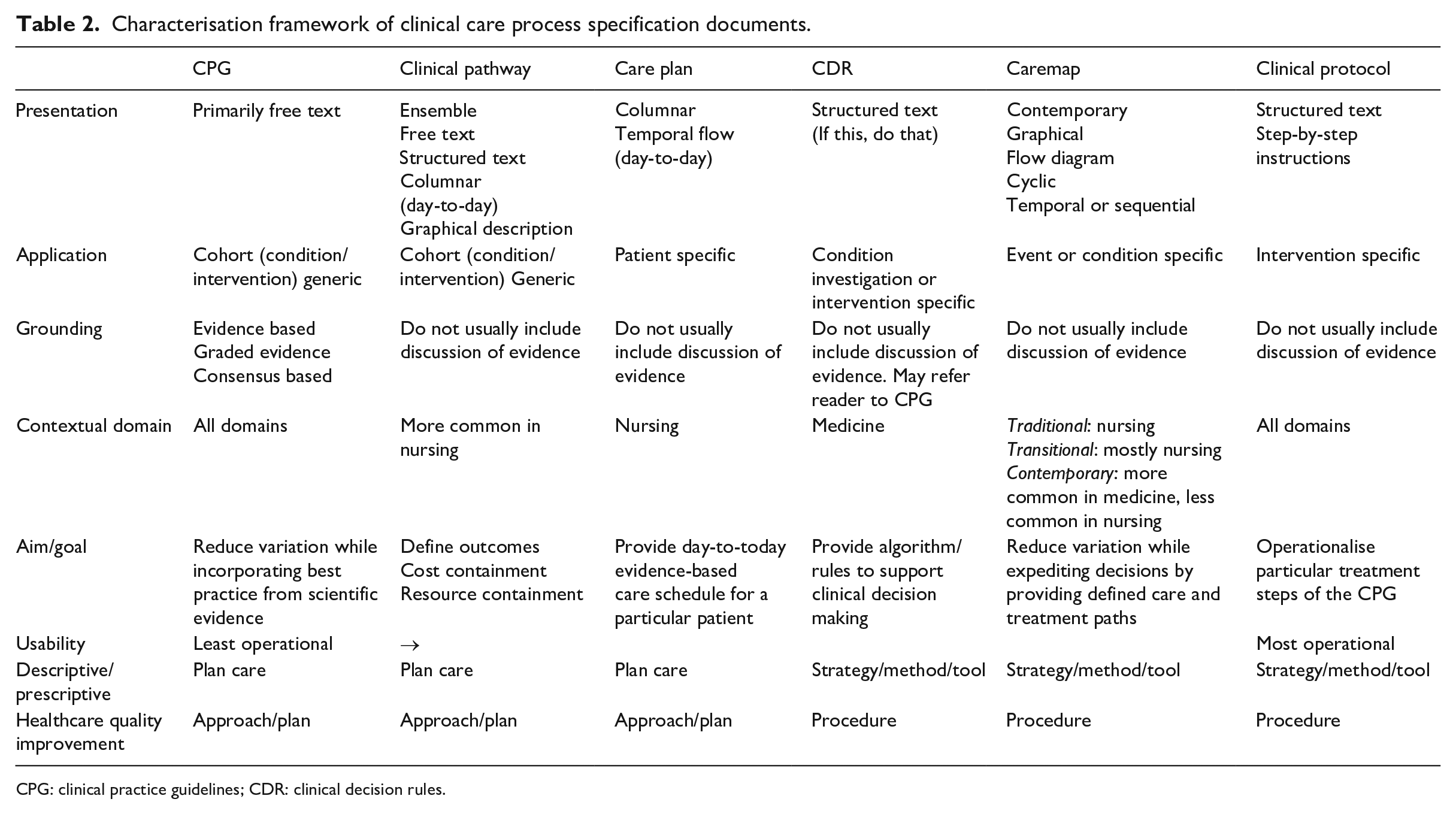
CPG: clinical practice guidelines; CDR: clinical decision rules.
This characterisation is robust in the sense that in addition to De Blesser’s elements it also incorporates aspects that allow CCPS to be analysed more comprehensively in terms of their content, structure and target patient cohort. This table would be useful in tasks seeking to identify or design particular CCPS documentation and ensure that it covers all of the aspects incorporated in Table 2.
Case study: Type 2 Diabetes and diabetes in pregnancy CCPSs in England
This section applies the taxonomy and characterisation to clinical documentation from England on the topic of Type 2 Diabetes (T2D) and diabetes in pregnancy. In each of the following, any reference to a section identifies a section so labelled within the particular clinical care specification document being described. Each of the specifications cited includes a URL in the reference so that the reader may access the document.
Policy
We identified three related documents that describe policy regarding diabetes, and more specifically T2D, namely:

Government policies generally open by expounding on the scope and scale of a public health issue. This information, which centres around the community and resource impact of the medical condition tends to be followed by messages to the lay public that are over-simplified such that they lose the proper meaning and efficacy they are intended to convey. In effect, they miss their goal and become more like promotional material intended for the media, as seen in the example of Figure 3, with claims based on a very small subset of cherry-picked and highly motivated volunteers.

Clinical practice guidelines for Type 2 Diabetes. 101
One component of this same policy which has become enshrined in UK taxation legislation, is the laudable challenge to remove 20 per cent of the caloric content comprised by sugar from all products produced across the food and drinks industry. While put in holistic context, this caloric-reduction policy carries over in Section 4 of the identified National Health Policy. However, this policy approach has resulted in manufacturers finding it necessary to replace sugar primarily with artificial sweeteners like aspartame and saccharin. Both these non-nutritive sweeteners have received sufficient research to suggest that the health dangers of frequent or daily use may also be harmful.104–106 This example demonstrates our claims regarding policy that it is: (1) politically motivated, (2) often not based on established scientific evidence and (3) it tends towards having been constructed by politicians from many small sound bites seeking air time to expound the virtues of their policy and elicit support from the ordinary citizen.
CPG
A selection of CPG relevant to T2D and diabetes in pregnancy are shown in Table 3.
Clinical practice guidelines for Type 2 Diabetes.
CPG: clinical practice guidelines; IDF: International Diabetes Federation; ADA: American Diabetes Association; EASD: European Association for the Study of Diabetes; NHS: National Health Services.
Similar to the government policy which claimed it had, or would, deliver weight loss, the international guideline at Section 1.2 recommends weight loss as the key tool for preventing T2D.
The international guideline at Section 1.3 also provides for a regimen of testing and thresholds to be used in diagnosing the diabetic patient. In this case the International Diabetes Federation (IDF) guideline follows a diagnostic standard from another international guideline, that of the WHO. Similar diagnostic testing and threshold recommendations carry through in the national CPG at Section 1.6 and local CPG at Section 4.3.
At each level, the recommendations in CPGs become more applicable to patient care. The international and national guidelines present the perfect scenario or perfect model for treatment, while local guidelines recognise that there are non-compliant patients and not everything will go according to plan.
Clinical decision rule
In many cases, CDR can be identified and isolated from within the content of local CPGs. For example, from within the Barts Health National Health Services (NHS) Trust local CPG described above, comes a diagnostic threshold rule for glycaemic control in pregnancy for diabetic mothers who were treated only with diet control: 10.1 Monitor blood glucose 4 hourly. If blood glucose >7.0 mmol/L on 2 consecutive occasions, start IV insulin/glucose infusion. If the woman requires a Caesarean section and the blood glucose >7.0 mmol/L, start IV insulin/glucose regime.
Clinical pathway
Two English diabetes clinical pathways are:
Each presents an approach to screening and patient assessment, care planning, patient support and education that includes for lifestyle changes in diet, weight, exercise and insulin/glucose control. Each also makes reference to, and recommendations regarding, potential complications that may arise in future for these patients and advises the signs and symptoms that clinicians and patients should be mindful of. These pathways present as a generic blueprint for care of patients with diabetes.
Care plan
Two relevant care plans are:
My personal diabetes health care plan and record 115
My personal diabetes handheld record and care plan 117
Each contains information and contact details for services the patient may require. More importantly however, each provides space and tables for recording the day-to-day condition, treatment and care recommendations specific to that patient.
Caremaps
Caremaps provide a visual roadmap of care for a specific condition or treatment process. Caremaps can aid in treatment selection, understanding of disease progression, and can also provide the base knowledge that together with clinical expertise can be used in health research and development of Learning Health System (LHS). The PamBayesian project 118 has developed the following caremaps for diabetes in pregnancy as part of a project to develop clinical decision support LHS for use by clinicians and patients:
Midwifery Booking Visit GDM Booking Visit
Diagnostic Caremap GDM Diagnostic Decisions 2.0
Management Caremap GDM Management Decisions 2.0
Standardisation before computerisation
CCPS computerisation
Various types of CCPS such as caremaps, CPG and clinical protocols are increasingly becoming the subject of computerization. 119 For computerisation to be easily achievable, CCPS need to be formalised to make them computer-interpretable. 120 Formalisation of CCPS refers to specification using precise and unambiguous terms and structures, usually using computational or mathematical formalisms, making the resulting CCPS as computer interpretable.
Standardisation as a prerequisite to computerization
CCPS computerisation is enabled by CCPS formalisation which in turn is enabled by CCPS standardisation. Consequently, computerising CCPS that have not first been standardised creates more problems than it solves, or as one group of authors put it, that a mess computerised is a computerised mess. 121 While this research has referred to the need to standardise the structure and presentation of CCPS, there is also a need to standardise the content captured within the CCPS by standardising the underlying language. This is crucial to the challenge of formalisation to attain computer interpretability and hence computerisation.
Role of data and information standardisation in CCPS computerization
Data standardisation is needed to resolve the Data Triple-I issues of integrity, integration and interoperability identified in a 2019 literature review as significant barriers to adoption of health information technology. 122 The use of standardised clinical terminology and approaches to eliciting and reporting routine clinical data is necessary to improving clinical practice and communication and enabling accurate computerisation of health record data. 123 In our experience there are many existing healthcare provider projects in the United Kingdom, Australia and New Zealand that seek to standardise information that has already been captured, or to standardise coding of data as it is captured. The issue observed is that they do this more often without considering whether the underlying clinical document or form was standardised first. Where standards are considered there tends to be disagreement as to which underlying methodology, terminology, data standard or data exchange protocol should prevail: SNOMED, ICD-10, METeOR, FHIR or others.
The benefits of standardisation in the context of CCPS computerization
Standardisation of clinical documents has been observed to improve data collection, data quality, and to enable automated coding and analysis.124,125 Standardisation of CCPS using approaches that include: (1) defined data definitions and (2) attention to built-in computer interpretability 126 supports data standardisation, mitigating the Data Triple-I issues and increasing the chances for successful creation and adoption of LHS.
Discussion and related works
The confusion arising out of the absence of standardised definitions and nomenclature for clinical documents has been known since at least 2006.18,54,127,128 As a result of this lack of standard terminology and taxonomy, successive and discordant attempts at defining and describing a structure and development process for some have only served to intensify the issue.54,127,128 It is further intensified when we observe examples of authors who identified multiple document types as synonymous in name or structure,18,34,84,128 only to differentiate them in the same research by describing one as a single or multi-component item of the other,34,84 or a translation of the other represented in different structural form. 128 In earlier research, 16 our team identified examples where authors described a clinical document in-text using one label listed in the ‘Introduction’ of this article, only to find that the included clinical document was titled or described itself using another.129,130 Such instances exemplify this issue and its potential to create lasting confusion.
Authors have sought to define or present approaches to develop different CCPS during the last two decades, yet significant variance in the complexity level, design approach, content and representational structures for those discussed here has persisted.16,24 This lack of standard and formal care process specifications, differences in communication and information transfer between clinicians providing caring for the same patient can affect the quality of care and introduce additional risk of harm for as much as 25 per cent of all patients.131,132 Error reporting documentation also tends towards not being standardised. However, even where some effort has been made to standardise, clinical decision and treatment errors remain underreported. Although clinicians and clinical researchers are encouraged to be honest and transparent in such situations, we can never be certain whether reported error figures quoted are representative of the entire scope of the problem.133–136
Standardised approaches, especially in clinical documentation, ensure that each time a healthcare provider approaches that type of document, the format and content are consistent with expectation. 16 Standardised documentation ensures sufficient higher quality information is recorded and reported, enabling documents to be read quicker and content within to be better retained, all with the effect of improving overall patient safety and outcomes.16,131,137,138
Summary and conclusion
Since the early 2000s there has been a significant shift towards standardisation of healthcare and healthcare practice. Efforts to standardise healthcare can be held back by many things, one of which may be the lack of consistent nomenclature and definitions for CCPS documents, many of which are used every day in hospitals and general practice clinics. We have addressed the challenge by: (1) presenting a four-layer taxonomy for CCPS documents that begins with those documents that are least-able to be applied in clinical care and moves towards those which are most capable of use in the clinical setting and (2) drawing upon previous efforts to standardise the definition and structure of one type of CCPS document, expanding that method to apply to all documents included in the taxonomy. We evaluated our approach through a case study looking at a range of CCPS documents from the United Kingdom concerning diagnosis and treatment of patients with T2D and diabetes in pregnancy. We hope that the results and discussion will stimulate those in healthcare and healthcare service management to consider the potential benefits of standardising clinical documentation in the same way that evidence-based medicine aims to standardise healthcare. Standardising the way patient care is documented and reported will reduce significant data integration and interoperability issues as national health services continue to move towards implementing centralised electronic shared care records.
Footnotes
Appendix
| References | Policy | Clinical decision rule | Case management plan | Clinical practice guideline | Caremap | Clinical pathway | Care pathway | Critical pathway | Clinical/treatment protocol | Care plan | Careflow |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Goode 84 | □ | □ | □ | ||||||||
| Goode 84 | • | • | |||||||||
| Goode 84 | □ | □ | |||||||||
| Goode 84 | • | • | |||||||||
| Giffin and Giffin 139 | • | • | |||||||||
| Giffin and Giffin 139 | □ | □ | |||||||||
| Seaberg and Jackson 140 | • | • | |||||||||
| Hydo 86 | □ | □ | |||||||||
| Hydo 86 | • | • | |||||||||
| Hydo 86 | • | • | |||||||||
| Stiell et al. 141 | □ | □ | |||||||||
| Gordon 142 | □ | □ | |||||||||
| Gordon 142 | • | • | |||||||||
| Gordon 142 | • | • | |||||||||
| Holocek and Sellards 143 | □ | □ | □ | □ | |||||||
| Morreale 90 | □ | □ | □ | ||||||||
| Morreale 90 | • | • | |||||||||
| Morreale 90 | □ | □ | |||||||||
| Hill 144 | □ | □ | |||||||||
| Chu and Cesnik 34 | • | • | |||||||||
| Chu and Cesnik 34 | • | • | |||||||||
| Dentonet al. 145 | □ | □ | □ | □ | □ | ||||||
| Dickinson and Noud 146 | • | • | |||||||||
| Dickinson and Noud 146 | • | • | |||||||||
| Philie 147 | • | • | |||||||||
| Philie 147 | □ | □ | |||||||||
| Quaglini et al. 148 | • | • | |||||||||
| Lanzieri et al. 149 | □ | □ | |||||||||
| Trowbridge and Weingarten 32 | • | • | |||||||||
| Micik and Borbasi 150 | □ | □ | |||||||||
| Panzarasa et al. 151 | • | • | • | ||||||||
| Powell 152 | • | • | |||||||||
| Jones 87 | • | • | |||||||||
| Jones 87 | • | • | |||||||||
| Mingmei 153 | • | • | |||||||||
| Mingmei 153 | □ | □ | □ | ||||||||
| Beaupre 38 | □ | □ | |||||||||
| Beaupre 38 | • | • | |||||||||
| Van Herck et al. 154 | □ | □ | □ | □ | |||||||
| Agrawal and Kosowsky 62 | • | • | • | • | • | • | |||||
| Agrawal and Kosowsky 62 | • | • | |||||||||
| Brehaut et al. 155 | • | • | |||||||||
| Repasky 156 | □ | □ | |||||||||
| Ducharme 69 | • | • | • | • | • | ||||||
| Ducharme 69 | • | • | |||||||||
| Dunning et al. 157 | • | • | |||||||||
| De Bleser et al. 54 | □ | □ | □ | ||||||||
| Vanhaecht et al. 158 | □ | □ | □ | □ | |||||||
| Tay et al. 159 | □ | □ | □ | ||||||||
| Gaddis et al. 160 | • | • | • | ||||||||
| Sternberg 91 | • | • | |||||||||
| Sternberg 91 | □ | □ | |||||||||
| Mackey et al. 161 | • | • | |||||||||
| Kwan 162 | □ | □ | □ | □ | |||||||
| Richman et al. 163 | □ | □ | |||||||||
| Rotter et al. 164 | □ | □ | □ | □ | □ | ||||||
| Rotter et al. 164 | • | • | |||||||||
| Rotter et al. 164 | • | • | |||||||||
| Lougheed et al. 165 | • | • | |||||||||
| Lougheed (2008) | • | • | |||||||||
| Gemmel et al. 35 | □ | □ | □ | ||||||||
| Isern and Moreno 166 | • | • | |||||||||
| Ebell 92 | • | • | |||||||||
| Nakanishi et al. 167 | • | • | |||||||||
| Kinsman et al. 127 | □ | □ | □ | ||||||||
| Kinsman et al. 127 | • | • | |||||||||
| Kinsman et al. 127 | • | • | |||||||||
| Kinsman et al. 127 | • | • | |||||||||
| Tastan et al. 89 | • | • | |||||||||
| Lodewijckx et al. 168 | • | • | |||||||||
| Tastan et al. 89 | • | • | |||||||||
| Huang et al. 88 | • | • | |||||||||
| Huang et al. 88 | □ | □ | |||||||||
| Huang et al. 88 | • | • | |||||||||
| Lockie et al. 93 | • | • | |||||||||
| Jayaraj et al. 169 | • | • | |||||||||
| Jabbour et al. 170 | • | • | |||||||||
| Jabbour et al. 170 | • | • | |||||||||
| Morrow et al. 171 | □ | □ | |||||||||
| Yu 172 | • | • | |||||||||
| Yu 172 | • | • | |||||||||
| Li et al. 173 | • | • | |||||||||
| Royall et al. 174 | • | • | |||||||||
| Carter et al. 175 | • | • | |||||||||
| Carter et al. 175 | □ | □ | |||||||||
| Wang et al. 94 | • | • | |||||||||
| Wang et al. 94 | • | • | |||||||||
| Roopsawang and Belza 176 | □ | □ | □ | ||||||||
| Buchert and Buttler 128 | □ | □ | □ | □ | □ | □ | |||||
| Buchert and Buttler 128 | • | • | |||||||||
| Dagliati et al. 85 | • | • | • | ||||||||
| Dagliati et al. 85 | • | • | |||||||||
| Gopalakrishna et al. 177 | • | • | |||||||||
| Gopalakrishna et al. 177 | □ | □ | |||||||||
| Solsky et al. 19 | • | • | |||||||||
| Alonso-Coello et al. 178 | • | • | |||||||||
| NHS: London Clinical Networks 114 | • | • |
• = distinct/different items; □ = same or synonymous items.
Acknowledgements
The authors thank Anokunda, Danika, Thomas, Liam and James.
Authors Note
The ORCID for the co-authors are as follow, Norman E Fenton: 0000-0003-2924-0510, Kudakwashe Dube: 0000-0002-2829-8481, Evangelia Kyrimi: 0000-0001-6727-2279, Graham A Hitman: 0000-0002-6637-9004
Contributors
S.M. performed the primary research and prepared the first draft. S.M. proposed the basis for the taxonomy and expanded De Bleser approach, which was refined by E.K. and K.D. J.S. and G.H. provided clinical input and review. K.D. and N.F. supervised the research. All authors contributed, commented and approved the final draft.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: S.M., N.F., G.H. and E.K. acknowledge support from the EPSRC under project EP/P009964/1: PAMBAYESIAN: patient managed decision-support using Bayes Networks. K.D. acknowledges financial support from Massey University for his study sabbatical with the PamBayesian team.