
Abstract
Mental illnesses are on the rise on campuses worldwide. There is a need for a scalable and economically sound innovation to address these mental health challenges. The aim of this study was to explore university students’ needs and concerns in relation to an online mental health virtual community. Eight focus groups (N = 72, 55.6% female) were conducted with university students aged 18–47 (mean = 23.38, SD = 5.82) years. Participants were asked about their views in relation to online mental health platform. Three major themes and subthemes emerged: (1) perceived concerns: potential loss of personal encounter and relationships, fear of cyber bullying, engagement challenge, and privacy and distraction; (2) perceived advantages: anonymity and privacy, convenience and flexibility, filling a gap, and togetherness; and (3) desired features: user-centered design, practical trustworthy support, and online moderation. The analysis informed design features for a mindfulness virtual community.
Keywords
Introduction
There is an alarming increase in mental illnesses on university campuses across North America, including Canada.1,2 In 2013, a national survey of students in 32 Canadian post-secondary institutions found high anxiety in 56.5 percent, hopelessness in 54 percent, seriously depressed mood in 37.5 percent, and overwhelming anger in 42 percent. Furthermore, 9.5 percent of students seriously considered suicide and 6.6 percent reported intentional self-abuse manifested in self-cutting, burning, bruising, or injuring self. Most tragically, 1.3 percent reported having attempted suicide. 3 The economic burden of mental health includes loss of generic productivity and reductions in health-related quality of life. 4 The mental health cost in Canada alone is estimated to be more than CAD $51 billion yearly, with 9.8 percent of that as direct medical cost, 16.6 percent as long-term work loss, 18.2 percent as short-term work loss, and 55.4 percent (CAD $28 billion) due to loss of health utilities (e.g. vision, hearing, speech, mobility, dexterity, emotion, cognition, and pain as assessed in the Health Utilities Index Mark 3 system). 5
However, face-to-face mental health support is expensive to implement and sustain over time. Such financial constrain is also evident in Canadian university campuses where counselors are overwhelmed with demand and lack of resources to care for large student bodies. 6 Others report long wait time for a counseling appointment in university campuses. 7 Approaches to improve mental well-being before the crisis ensues have become necessary. One such approach could be mindfulness practices.
Mindfulness is an emerging mental health approach and defined as “the awareness that emerges through paying attention on purpose, in the present, and non-judgmentally to the unfolding of experience moment by moment”; 8 mindfulness meditation is a practice that involves non-reactive awareness and acceptance of present experiences (e.g. emotions, sensation, and mind) coupled with breathing. Mindfulness-based interventions have been found to positively impact psychological health (e.g. decline in mood disturbance, reduction in psychological symptoms and emotional reactivity, improvement in behavioral regulation)9,10 and physical health (e.g. sensory pain and physical impairment) 11 in clinical and non-clinical populations.12–16 Hence, mindfulness techniques hold promise in addressing students’ mental health challenges on campuses. However, extensive mental health needs in the student population and the limited availability of mindfulness certified professionals set limits to a brick-and-mortar delivery model for mindfulness. Possibly, Internet-based tools could be employed to address these challenges. Evidence shows that health virtual communities are flourishing 17 and several scholars report positive health outcomes when patients are supported by such tools;18–21 however, none has used mindfulness techniques. Access to virtual communities enable and empower patients to become active participants in managing their own health conditions.22,23
In this context, our team embarked to develop a Mindfulness Virtual Community (MVC) for York University students.24–26 The key elements of this platform are peer-to-peer asynchronous online forum, mindfulness-based self-help modules, and group-based video conferencing with a psychologist. The overall aim of the multi-phased project is to generate robust evidence on effectiveness that could lead to uptake of such mindfulness initiative across several universities in Canada and internationally. Given the significance of user-centered designs for the success of an online community, 27 the first phase of the project aimed to understand the students’ needs, behaviors, and expectations from a mindfulness-based platform and conducted focus groups. In this article, we present the analysis of students’ requirements, motivators and challenges for engagement in a MVC, and the main components that they feel essential to include in its structure.
Methods
Study design
We opted to use qualitative research approach to elicit student perspectives. Qualitative methodologies28,29 offer important discovery tools to uncover a social phenomenon and have been widely used to explore user needs and to inform the development of e-health solutions, including virtual communities, 30 or even assess the feasibility and acceptability of e-health solutions.30–33 Therefore, to build student-centered evidence-based MVC, we conducted focus groups with students to uncover their mental health challenges, their online experiences, and their expectations and requirements in a mental health virtual community. For socially sensitive engagement of students, the groups were stratified as follows: two female-only and two male-only groups on the topic of general mental health; two mixed gender groups on the topic of stress and anxiety; and two mixed gender groups on the topic of mood and depression. The study was approved by the York University’s Ethics Review Board.
Procedure
Eight focus groups were conducted in March and April of 2016 at York University, Toronto, Canada. The study inclusion criteria were as follows: (1) being an undergraduate student enrolled at York University and (2) aged 18 years and above. There were no specific exclusion criteria other than not meeting the inclusion criteria.
Students were recruited through flyers, listserv, in-class announcements, and campus social media outlets. Students expressed interest in participating by contacting the study’s Gmail account. The research assistant (RA) responded to each inquiry with a request to complete a pre-screening questionnaire confirming: eligibility (i.e. meeting the inclusion criteria), self-identified gender, preference for one of the stratified groups (first, second, or third choice; no preference; or not willing), and meeting times per day. The RA then used this information to schedule the groups and achieve the desired stratification. A maximum of 12 students were scheduled to participate in each group. In total, 320 students contacted the RA, and 238 students completed the pre-screening questionnaire. Among them, 72 students were chosen using a purposeful sampling approach 34 and participated in eight focus groups; 24 students did not show to the scheduled focus group for personal reasons (e.g. conflicting schedules).
Each focus group began by providing study details and obtaining a written informed consent. Participants wore a name tag bearing any name they chose and were encouraged to choose pseudonyms; the pseudonyms were tracked and maintained in a master list. A trained moderator (C.M.) used a semi-structured interview guide with a set of open-ended questions developed by the research team to facilitate focus-group discussions (e.g. “what do you do, whether that’s online or offline, if you’re feeling stressed, anxious or down”). All discussions were audio-recorded. The moderator moved from general questions to more focused one, covering online activities, content and connectedness, psychological support sought, and finally, MVC-related questions and knowledge of mindfulness. The moderator used prompts to investigate statements and topics in more depth. At the end of 90 min, the moderator asked participants to complete an anonymous survey that included basic demographic information as well as the Patient Health Questionnaire-9 (PHQ-9) 35 and Beck Anxiety Inventory (BAI) 36 scales for depression and anxiety. These validated questionnaires have been widely used across various populations, including university students, and show consistent results. 37 All participants were given the choice between two forms of compensation: CAD $20 cash or 2 percent increase in the term mark for a course of a consenting professor.
Data management and analysis
All audio-recorded data were transcribed verbatim. The transcripts were imported into ATLAS.ti® for Windows (version 7.5.12; ATLAS.ti GmbH, Germany). 38 This dataset was analyzed employing a thematic description approach. 39 This approach suits very well our aims since we were not to build a theory or to interpret the meaning of an experience but rather to stay close to the data and get a thematic description of the participant perspectives. 40 The preliminary codes were developed by C.M. and two members of the research team (C.E.M. and F.A.) employed to the dataset independently, followed by joint discussion for refinement where coding disagreements were resolved through consensus.
The survey data were entered into SPSS 23.0 (IBM Corporation, USA). 41 Descriptive statistics were employed to describe the sample characteristics.
Results
Sample characteristics
Overall, 72 students participated in eight focus groups. Participants’ demographic characteristics are summarized in Table 1. The mean age was 23.38 (SD = 5.82) years, ranging from 18 to 47 years, and 55.6 percent (n = 40) of the participants were females which keeps the final views balanced and representative of both males and females. In terms of study year, the students who completed third and fourth year were more represented with rates at 25.0 percent (n = 18) and 26.4 percent (n = 19), respectively; students in fifth year or more were less represented at 9.7 percent (n = 7) as expected. Overall, 41 percent (n = 30) were not working; among the 59 percent working students, 30.6 percent (n = 22) were working for 10–20 h/week and 9.7 percent (n = 7) for more than 20 h/week. In terms of information technology and Internet connectivity, 94.4 percent (n = 68) of the participants reported they had access to a smartphone and 93.1 percent (n = 67) had access to laptop/PC at home. Also, 68.1 percent (n = 49) connected to the Internet for personal use through smartphones, 50.5 percent (n = 36) through a laptop; tablets and desktops were the least used with rates at 12.5 percent (n = 9) and 12.5 percent (n = 9), respectively.
Sample demographics (N = 72).
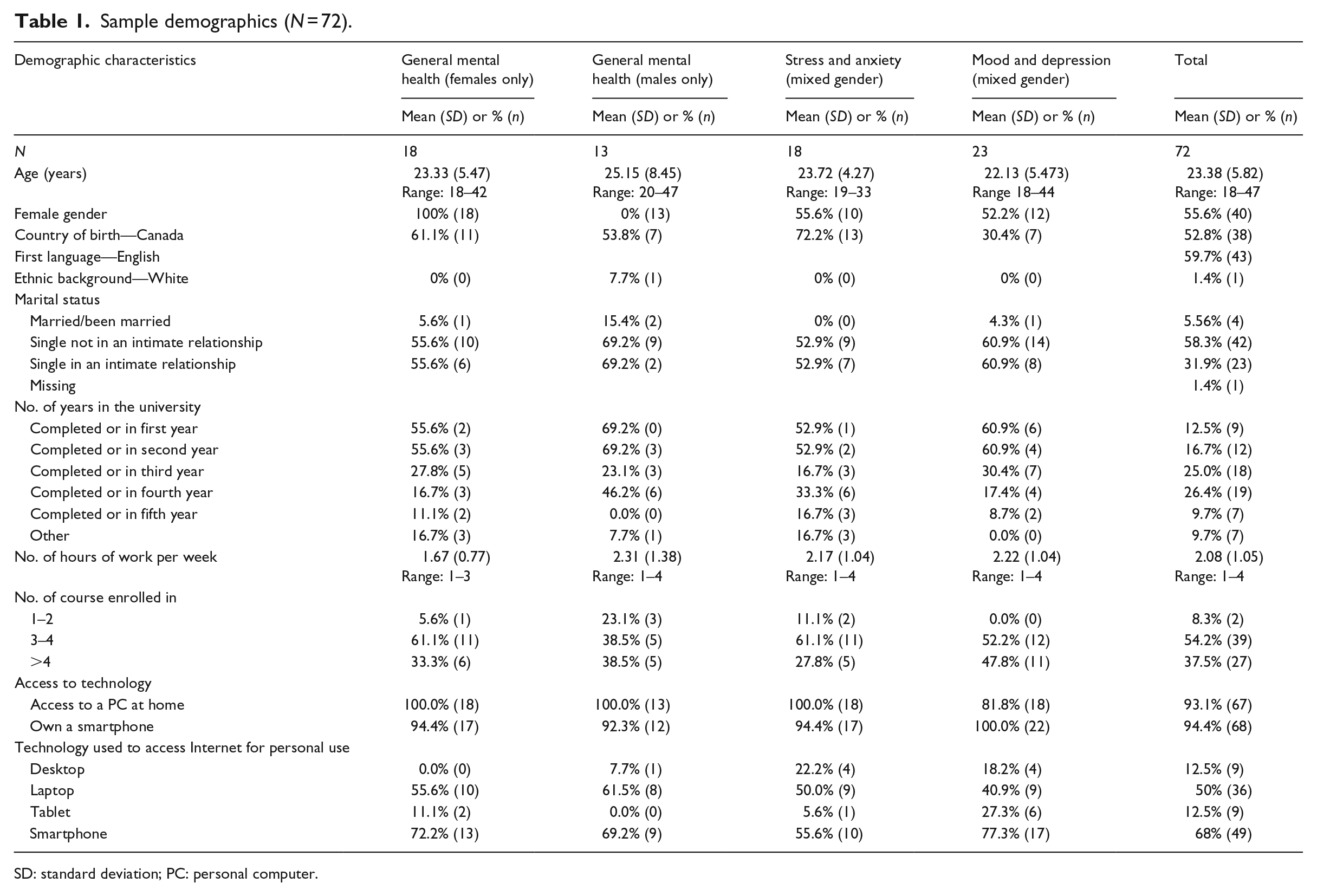
SD: standard deviation; PC: personal computer.
Qualitative findings
The focus-group qualitative data analyses uncovered three major themes pertaining to the MVC as identified by the students: (1) perceived concerns, (2) perceived advantages, and (3) desired features. Each theme consisted of subthemes. The following is a description of the main themes and subthemes.
Perceived concerns
Overall, the focal point of participants’ concerns was the potential impact of a virtual environment on the MVC members’ experience of social interaction. The potential loss of personal encounter was the most frequently reported concern. The second concern raised by students was the concern of online bullying. Students wanted to make sure that they can preserve a personal “touch” with others online as well as to ensure that the MVC is a safe space. The challenge of online engagement was the third major concern. Surprisingly, while privacy and risk of distraction were mentioned frequently in the context of other online activities, they were not significant concerns in the context of the MVC (see Table 2). We describe below each subtheme.
Number of participants who voiced concerns, advantages, and desired features.
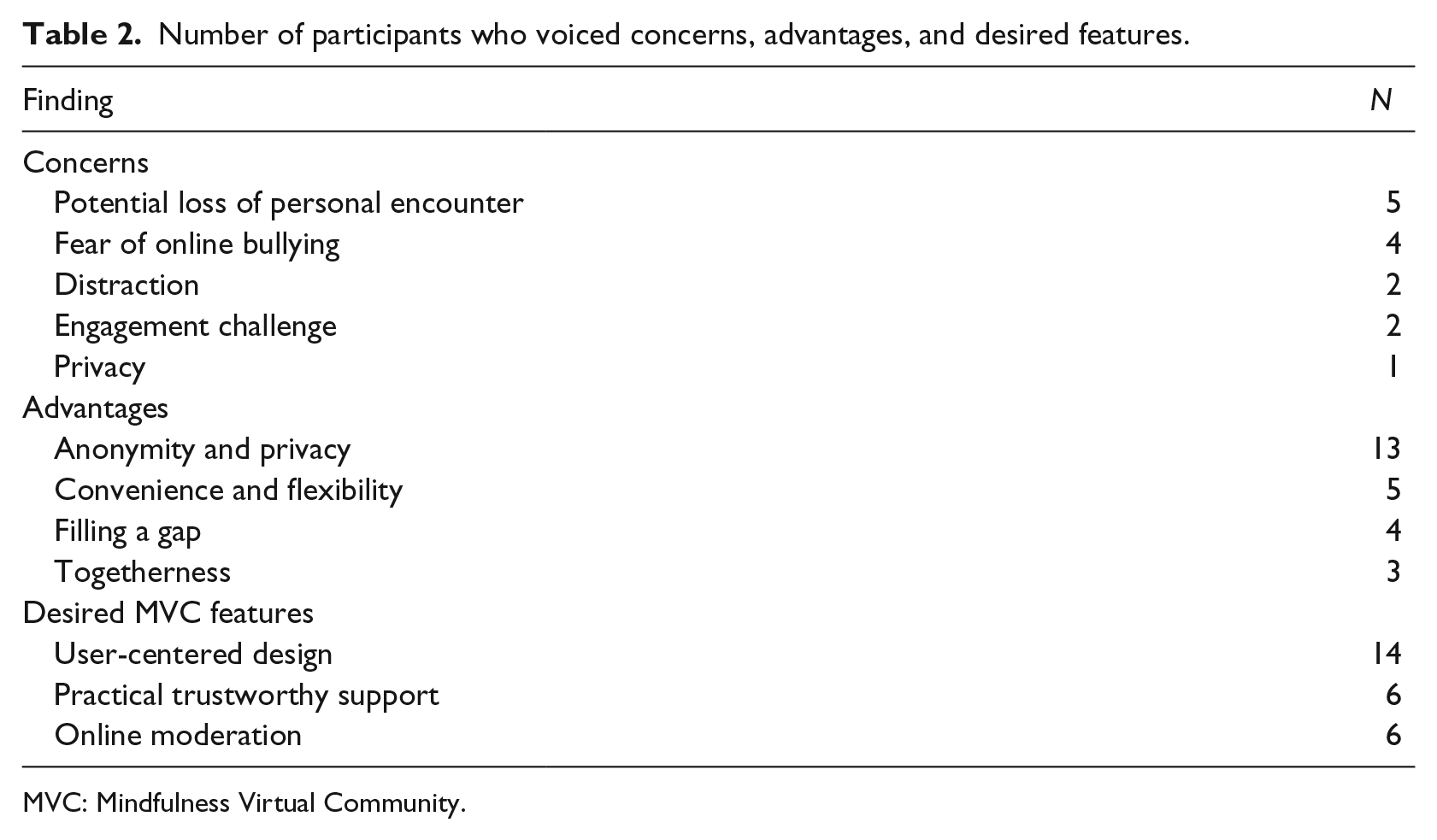
MVC: Mindfulness Virtual Community.
Potential loss of personal encounter and relationship building
Losing personal touch with others was the major concern expressed by participants, especially for online encounters related to mental health, where discussions are personal and intimate. Participants were worried about feeling in front of a “machine” not “a person”; they contrasted such a situation to a relationship with a friend since one goes to “friends because they are personal,” and therefore maybe there would be a need of “in-person meetings” to “eliminate that barrier” and build “long-term” community-like or friendship-like relationship: . . . but like I don’t know how personal this community could get, right? But like, you go to your friends because they’re personal, right? Like they can really understand your own life but then an online community like yeah, it can’t get that personal. (Male, aged 20, Canadian-born)
Fear of cyberbullying
Students had significant concerns about cyberbullying, given their lived experiences online. Their statements reflected anxiety about “nasty” comments, “negative” behavior, “rudeness,” and “bad” or “hurtful” comments. Students voiced their feelings of vulnerability in the face of cyberbullying, and the need to address cyberbullying in the MVC to ensure participants’ mental well-being: negative things behind anonymity, people will be trolling the boards and I feel like it’s always hurtful. And even if their privacy is maintained, just hearing those things from other people in an environment that you’ve made yourself vulnerable in, I feel like would be even more damaging. (Male, aged 24, Canadian-born)
Engagement challenge
Some students expressed a concern based on the idea that not everyone may want to engage with mental health online, either because they wish to avoid spending more time online or because of the lack of person-to-person encounters. Some raised the need for an awareness campaign to let students know about the existence of the MVC, noting that some students lack awareness of already existing resources. The quote below exemplifies this perceived engagement challenge: I feel like benefits even, on its own wouldn’t be a big enough push. Because, like, we know exercise is good, nutrition is good but how many of us actually do it, right? [. . .] I don’t understand how you would engage someone into joining such, like, a site. (Female, aged 21, Canadian-born)
Other concerns: privacy and distraction
Two additional concerns were raised tangentially as follows: privacy of the online discussion and the possibility that the MVC might add to an already existing experience of becoming distracted online. Online privacy and security of the medium of communication was a concern given the sensitive nature of the subject of discussion (i.e. mental health) that involves delving into personal and “big issues” of one’s experience at a certain period of life: . . . security issue. Privacy and I don’t know if they’re recording what I’m saying or—that is talking. But—and another thing about the texting—I also don’t feel it is secure. [. . .] I think that if it’s like a small issue, then it’s okay. But if it like—if it’s more like . . . [Facilitator: A big issue?] A big issues, then yeah, I’m not comfortable. (Female, aged 22, non-Canadian-born)
However, privacy seemed less of a concern in the context of the MVC than elsewhere online, and less of a concern than the opportunity to connect meaningfully with others.
Perceived advantages in MVC
Participants perceived four main advantages of the MVC that would stimulate them to engage with it online. The perceived advantages were as follows: (1) providing a safe space (to overcome stigma or backlash and to get valid support); (2) convenience in terms of commute, access time, and ease of access; (3) overcoming barriers and filling a gap in the healthcare system; and (4) providing a feeling of community achieved by the experience of online togetherness.
Anonymity and privacy
By far, overcoming stigma and backlash was the main perceived advantage of the MVC. Online anonymity has been perceived as an advantage because it provides a way to seek mental health support without the knowledge of friends or family; thus, ensuring privacy and overcoming culturally based stigma and backlash. The MVC was described as a solution that ensures privacy through remote online access to online resources from “the privacy of your own home.” The following comments convey this perceived advantage: Like personally for me like in my background, . . . if you’re physically going to like a support group or something, if I were to admit that to my family they’d be like oh, like why do you want to? Why are you wasting your time like that? Why are you going to like these groups? Like you can just study, you’ll be fine. (Female, aged 21, Canadian-born) There’s no stigma because nobody knows I’m kind of going on there. (Female, aged 31, Canadian-born) That anonymity, that, you know, that sense that it’s anonymous. I just don’t want people to see me going through. (Male, aged 24, non-Canadian born)
Convenience and flexibility
Since the MVC would be accessed on a myriad of devices (e.g. personal computer, laptop, smartphone), participants have seen in it an added convenience, a comfortable and flexible way to gain access to mental health resources, overcoming geographic and time limitations: for me like most of the time, 99 percent of the time I’m on phone, right? . . . And if you do have a platform where it’s easy to just click the button or click on whatever and then it pops up you’ll be able to instantly just access through that, yeah. (Male, aged 27, non-Canadian-born) It seems like an online community would like—it takes away a lot of the excuses. Oh, I don’t want to go out today. Oh, I don’t have to. Oh, it doesn’t fit into my schedule. Well, hey, I can kind of go online, whenever I want. (Female, aged 31, Canadian-born)
Filling a gap
Participants expressed their feeling that the access to a clinical professional offered by the MVC would fill a gap in the current system where young people feel isolated and family physicians “only give a prescription [medication]” and mental health is “stigmatized” and you need to go to a specialized place. It was their view that the MVC will provide them with a space to access a professional more easily: it breaks down a lot of barriers in terms of—because like that’s something that currently like doesn’t exist right now like if you have to go a psychologist you have to go to a hospital psychology, you have to go counselling and disability services, you have to—there’s that kind of—it’s a gap that needs to be filled and like people—young people as well, like we’re always online, you know. So, I mean it’s good. Like an online support group seems to like fill in all those gaps. (Female, aged 31, Canadian-born)
Togetherness
Another important advantage of the MVC mentioned by participants is the opportunity to come together, as this togetherness provides support to act “with someone,” and having the experience of being “together” in a community. However, students were averse to the “support group” wording and expressed their wish not to use such wording: Well, I know—like, I personally have been going to counselling through York and I’ve been trying to observe mindfulness, and it can be, kind of, difficult to pick up on, if you’re not being coached through it, so I think that would be a really cool way to, like do it at your own pace, but have the support to do it with someone. (Female, aged 21, Canadian-born)
Desired MVC features
By far, the most significant theme that appeared in students’ comments related to user-centered design, including ease of use, non-judgmental content, and personalizable content. Looking at students’ concerns about “cyber bullying,” for example, and advantages of “filling a gap,” it is not surprising that “moderation” should emerge as a key feature of the MVC. Below are examples of participants’ comments regarding the features they perceived as needed in the MVC.
User-centered design
Four needs emerged from the participants’ comments: (1) non-patronizing, non-judgemental content, (2) personalized content, (3) engaging content, and (4) ease of use.
Non-judgemental and non-patronizing content
Participants clearly expressed their need to have content that is not “patronizing” and is “non-judgemental,” avoiding the “you should do” stance: Yeah, because I do find that in psychological help that no matter how helpful you try to be the [with wording] wording or whatever can come off [is] really patronizing. It’s like oh, you should maybe do “x” instead of “y.” But you know, I might enjoy doing “y” instead of “x.” (Male, aged 22, non-Canadian-born) Like the nonjudgmental part, more like the tips. So more like actually trying to make you feel better instead of like—we already know we’re depressed, we get it, but—[Laughter] at the end of the day we want to feel better, right. (Male, aged 20, Canadian-born)
Personalizable content
Another feature noted in the focus groups was to have the content personalized to individual needs. This personalization referred to “mindfulness exercises,” “pace,” and access (anytime), and to avoiding a one-solution-fits-all mind-set: Well, one of my roommates and I, like we both are trying to get into meditation, but we have very different styles. Like, for me, I prefer like a guided meditation that talks about sensation, . . . whereas she prefers more like, a visualisation, like imagine yourself on a beach, kind of thing . . . so having, again, those options. (Female, aged 21, Canadian-born) I think that would be a really cool way to, like do it at your own pace. (Female, aged 21, Canadian-born)
Easy to understand
Some students expressed a preference for concise (not “10 pages of words”), simple to understand and not “complicated” content: I kind of don’t want it to be like a chore, like. I want to go through it and feel at ease. I don’t want to be having to read like five, 10 pages of words. And especially grammar is too complicated, I don’t want to be taking out a dictionary and looking that up. I want it to be very easy, simple. (Female, aged 18, Canadian-born)
Practical trustworthy support
Participants went into details of their need to have access to a professional to talk to, a help system providing practical trustworthy information and tips. Having access through the MVC to practical support mechanisms “at hand,” to someone who “could help to understand,” a “specialist” to help in the personal issues, was seen as important: Someone like that was a professional that I could talk to that could help me to understand what was happening, why I was feeling this way, why I was crying a lot, why I was so stressed, and why I couldn’t focus anymore, all that kind of stuff. (Female, aged 27, non-Canadian born)
Online moderation
Finally, students emphasized the need of a moderator that plays a key role in maintaining the “safety” and decorum of the peer-support discussion boards and to avoid “jerks” from hurting others, as participants in online discussion forums can become “mean,” “negative,” “hurtful,” and “rude.” Some also found that a moderator would be helpful to facilitate contributions from MVC members: I just know in discussion boards and stuff, like there’s people who will say mean, negative things behind anonymity . . . I think the moderator is a good idea and maybe like screening posts before they go up, like someone has to approve it before it can be visible on the site or the app. (Male, aged 24, Canadian-born)
The following table summarizes the number of students who mentioned the different concerns, advantages, and features.
Discussion
Many studies have examined online interventions for mental health;42–52 however, to the best of our knowledge, this is the first focus-group study that explores the needs and expectations of undergraduate students about an online mental health virtual community. This study provides valuable insight into undergraduate students’ concerns for any online approach to mental health; it describes the advantages they perceive in such an approach as well as their platform feature requirements. Therefore, this study provides valuable information regarding factors to consider when developing an online mental health platform for students on Canadian campuses.
We have identified three major themes in students’ discussions: (1) perceived concerns, (2) perceived challenges, and (3) desired platform features. Under these three themes, many major subthemes were uncovered.
The potential loss of personal contact was understandably a main concern; research indicates that isolation among primary and secondary school children 53 as well as mothers and adolescents 54 leads to greater mental health difficulties.
The students’ worries regarding loss of personal contact seems a healthy one and conforms with existing research showing that contact among people with mental health illness is associated with more inclusive behavior and less critical attitudes toward mental illness. 55 The demand for personal contact would be expected to enhance inclusiveness.
However, cyberbullying is a major challenge on the Internet;56–58 it is experienced and practiced by males and females,59,60 adolescents, 61 and university students 60 and can have a huge impact on personal well-being. 62 In our study, students expressed fear of online bullying aligns with the general reported experiences of cyberbullying, and this creates a tension with the desire for personal contact, particularly in the context of mental health. Finally, maintaining engagement in an MVC is an expected challenge; engagement has been reported to be a challenge in many studies, and online engagement is a well-known topic in online mental health approaches.63–66
Seeking anonymity and privacy online has been omnipresent in different research areas, including health,67–70 especially with the proliferation of social media.71–73
Health information sharing raises concerns about a sensitive part of human life, especially when information relates to a stigmatized issue, such as mental health, where safety becomes a concern. 74 It was no surprise that participants perceived anonymity as a tool to protect privacy.
By contrast, a perceived advantage of the MVC platform was the ability to meet other people, to be together, and overcome isolation. Togetherness has received attention in psychology since the mid-1940s;75–78 emphasizing togetherness in MVC is in line with research findings that showed that even though togetherness is a challenging experience, especially with challenging life experiences, 79 it helps construct meaning. 80 Research has also shown that greater contact between persons with mental illness and their healthcare providers is associated with lower provider stigma and higher expectations of patient adherence. 81
One can surmise that a virtual community that facilitates togetherness might lead to lower stigma and higher expectations of adherence to mindfulness among the members of the MVC. Others report reduction in both loneliness and depressive symptoms is associated with higher perceived emotional togetherness in social interaction. 82 We anticipate that an enhancement in perceived togetherness would have a positive effect on MVC participants’ mental health. Given the lack of responsiveness of the current healthcare system in Canada to mental health crises, especially on campuses, it is understandable that focus-group participants perceived an MVC as an outlet that might bridge the current gap in access to mental health tools.
We expected many user-centered design requirements related to the user-centered design paradigm83–86 to emerge in the discussion. We have planned for the inclusion of participants’ preferred features because adapting the MVC to students’ needs is paramount to its adoption and success. 87 Meeting these needs is essential, given the short attention span (around 8 s) 88 reported in online browsing.
Some participants were very vocal against patronizing content and style. Patronizing language has been found to affect performance on a cognitive task, 89 and self-judgment behavior is known to hinder mindfulness; 90 therefore, it is imperative to ensure that the content and style of the MVC does not add a judgmental or patronizing atmosphere.
Content that is easy to understand is an absolute necessity, especially among non-native English speakers; language has been found to be a major barrier in communication, even when language assistance regulations are in place. 91 Exacerbating language challenges for persons already facing mental health challenges would set a program to failure. Finally, participants’ insistence regarding moderation of the online discussions correlates with the perceived challenges related to cyberbullying.
It is worthy to note that, despite student concerns about the potential loss of personal encounter, the anonymity and privacy were the most perceived advantages of the MVC while concern about privacy was mentioned by only one student. Such results indicate that asking about perceived advantages is important to reveal implicit concerns. User-centered design was understandably the most prominent required feature.
Design implications
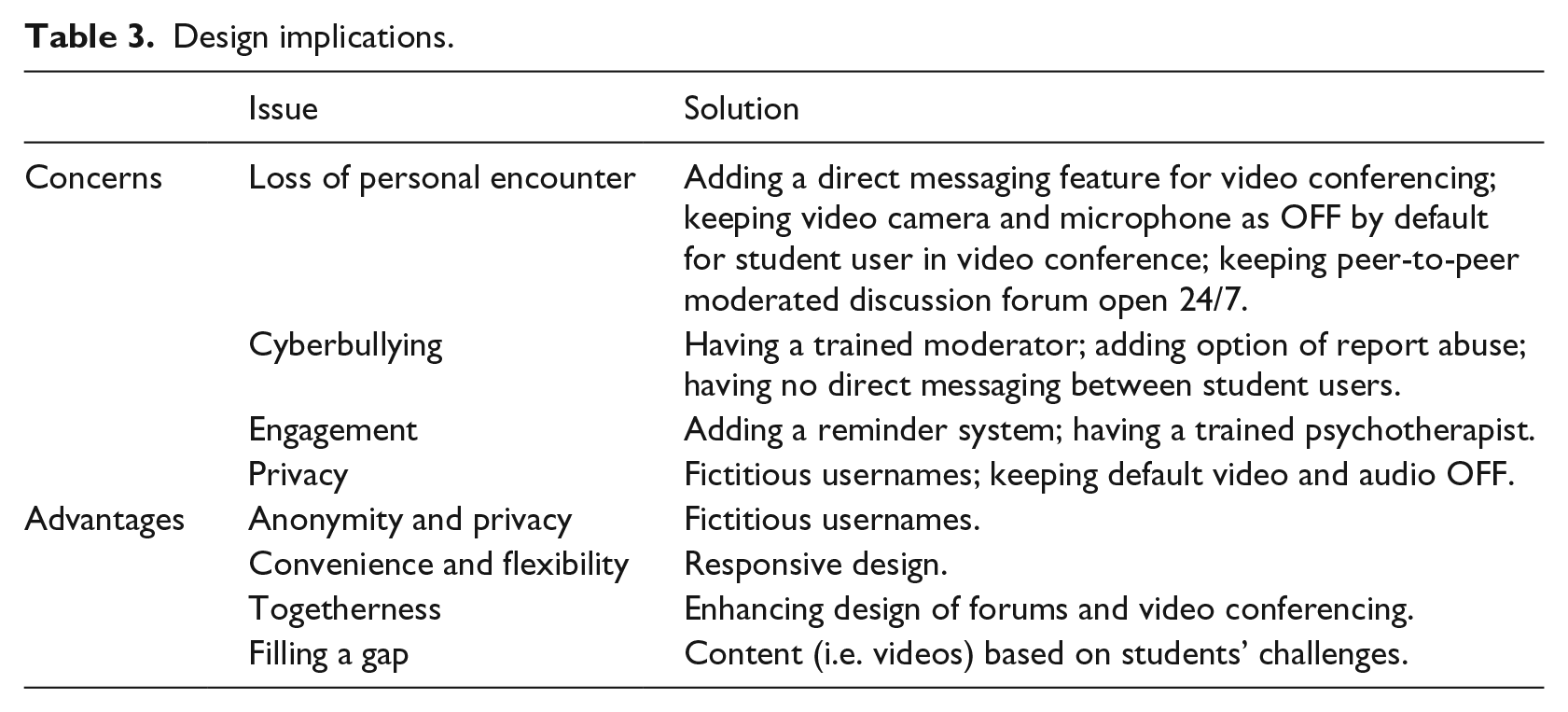
The above analysis led us to several design implications and we included those (summarized in Table 3) in the MVC developed for the randomized control study.
Design implications.
Forums and video conferencing
To address students’ concern of loss of personal encounter, we enhanced the interactive features of MVC planned components of peer-to-peer discussion forums and the video conferencing with a mental health professional. For example, we added “direct messaging” feature in MVC so that student users could directly communicate with the moderator—a trained psychotherapist—during a live session if they felt uncomfortable articulating a question or comment verbally. For a video-conferencing session, we decided to set the “default” of the camera and microphone as OFF for the student users and ON for the moderator to enhance the comfort of student users and minimize concerns about losing personal touch. For the same reason, the opportunity to have peer-to-peer discussions via the offered discussion forum was kept “open 24/7” while the psychotherapist read the comments and moderated if needed.
Moderator
The forums we have developed were moderated to avoid cyberbullying. The students, members of the mental health virtual community, have a “report abuse” button that sends an immediate message to the moderator who would take corrective actions (e.g. delete the abusive message if needed, contact the abuser). We also decided to disable any direct online communication between the virtual community members to avoid bullying as it could go unchecked by the moderator.
Reminders and professional psychologist
To address engagement, we have embedded a “reminders” feature in the design of our platform to send students necessary reminders about online activities (e.g. video-conferencing sessions) and a decision was made to have a psychotherapist as the moderator.
Usernames
A decision was made to hide the real name of the students by assigning fictitious usernames to them when enrolling them in the platform; this would add to privacy and ensure anonymity of the virtual community members.
Responsive design
To answer the students’ concern about flexibility and convenience of the platform, we have ensured a responsive design 92 that adapt to the type of device the users have (e.g. tablet, smartphone, laptop). Students wanted to access the platform from the privacy of their environment, having a responsive design that enables them to use the type of device convenient in their environment; this would ensure flexibility in the program delivery.
Content based on students’ challenges
To ensure that the program responds to the students’ needs and fills the gaps they have identified in their experience of mental health challenges, we have built mindfulness videos that address the topics they identified as challenging in their daily lives. The videos topics covered study, intimate relation, discrimination, and other types of challenges students relayed to researchers during the focus groups.
Limitations of the study
This study involves some limitations worth mentioning. All participants in this focus group were recruited from one university. While students experience similar conditions across universities in Canada, we should be cautious in generalizing these findings to the whole student population in Canada or worldwide. The participants were all recruited from a university where most students do not live on campus but commute, many for over an hour each way; findings of this study may not be representative of students living in other settings.
Conclusion
The study participants were from an urban Canadian University of an age ranging from 18 to 47 years, Canadian-born and new immigrant, having a wide range of mental health challenges, and have participated in eight focus groups. They showed high interest in a moderated MVC that allows post-secondary students to access mental health resources online, from the privacy and convenience of their homes, in a manner perceived safe as it maintains their privacy and allows them to overcome stigma and social pressure. They expect moderation to reduce cyberbullying and provide a safe space for togetherness in a non-judgmental, non-patronizing environment, using understandable language. The overall experience could allow students to overcome the potential loss of personal encounter, barriers to engagement, and gaps in the current healthcare system setup for mental health.
This study can help researchers to understand undergraduate students’ needs, aspirations, and expectations in terms of mental health on campus. The results of the focus group have informed the development of a student-centered Mental Health Virtual Community dedicated to students in higher education. A randomized control trial is underway to test its effectiveness.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by the Canadian Institutes for Health Research (CIHR), eHealth Innovation Partnership Program (eHIPP; Grant No. EH1-143553).