
Abstract
The main aim of this study is to review the literature to show how ideas around virtual communities of practice (VCoP) offer a model for supporting informal caregivers of Alzheimer’s patients (caregivers) to learn how to deal with caregiving demands. Caregivers are individuals who have a significant personal relationship with and provide a broad range of unpaid assistance to an older person or an adult with a chronic or disabling condition outside of a professional or formal framework. This review will examine the current evidence on the needs of caregivers, identify dimensions to be considered in VCoP design and suggest further directions of research. The investigation is an integrative review that builds a bridge between different areas of work. The outcome is eleven dimensions for the design of successful VCoPs for caregivers: Network Structure, Technology, Moderator, Scale, Alignment, Community Design, Sense of Trust, Knowledge Sharing, Sustainability, Ethics and Evaluation. In addition, we propose a Tree Metaphor to present our research results. Well-designed interventions based on VCoP principles have the potential of addressing caregivers’ needs.
Keywords
Introduction
Because of the ageing of the global population 1 there has been an increase in chronic disabling disorders that require a high level of care, such as dementia, including Alzheimer’s disease. 2 Caring for a person with Dementia creates a huge burden on their family and in many ways erodes the quality of life of caregivers. 3 In turn, poor informal caregiver quality of life increases the use of healthcare systems and the institutionalization of the patient. It follows, therefore, that attention to the needs of informal caregivers is a public health imperative. 4 Interventions are required to help them learn how to deal with care giving demands and to support them emotionally. 5
Informal caregivers are individuals who have a significant personal relationship with and provide a broad range of unpaid assistance to an older person or an adult with a chronic or disabling condition outside of a professional or formal framework. 6 Informal caregivers of Alzheimer’s patients (hereafter, “caregivers”) are the invisible second patients. 4 Research suggests that caregivers’ main needs are information and training about the disease, and support from others experiencing the same situation.7,8 Caregivers are also keen to learn skills for improving the daily life management of their relative. 9 Therefore, most interventions aim to improve information sharing, offer social support, and suggest coping strategies. 10 The most common intervention for caregivers is the face to face support group. 11 Support groups focus on building sympathetic relations among participants to discuss problems and feelings regarding care giving. 12 The well recognized value of this intervention is the emotional support, the useful information obtained from others and its social aspects. 12 Belonging to a support group makes caregivers feel understood as they become part of a community. 13
However, support groups differ in content, process and structure and it is unclear which groups produce a meaningful outcome for caregivers. 11 Furthermore, learning is not a primary focus in most models. 14 Critically, one of the main support group inconveniences is the time they take up and the need to travel to meet. 15
It is the argument of this paper, that some of the answers to delivering appropriate support to caregivers can be found in the literature of Communities of Practice (CoP). Originating in the field of social learning, but increasingly popular in applications within organizational studies and information systems, the literature around CoP is a fertile ground to search for evidence of how learning and information sharing can happen in a community context. “CoP are groups of people who share a concern, a set of problems or a passion about a topic, and who deepen their knowledge and expertise in this area through interacting on an ongoing basis.” 16 The concept captures the way that individuals’ desire to learn, share knowledge and support each other can be powerfully rooted in common daily practices and a common identity. 17 The health and social care fields are now showing a growing awareness of the potential of CoP as an approach to learning, identity and innovation. 18
ICT-based (Information, Communication and Technology-based) interventions with caregivers appear to be able to alleviate the burden of caring and prolong community living 19 as they can offer both information and social-support in scalable, convenient ways. 20 Moreover, Alzheimer’s M-health tools have been shown to be successful in improving awareness based on providing information for both, patients and caregivers. 21 In many senses the biggest challenge for a virtual community is the creation and sharing of knowledge. 22 The concept of VCoP again rooted in the CoP literature with its learning origins offers insights into how this can be accomplished. Many of the latest ICTs are well aligned with the peer-to-peer learning processes typical of a CoP. 23 The obvious benefit of such interventions is that they can usually be accessed at the caregiver’s convenience. Thus VCoPs offer a scalable way to deliver information and support from a diverse multidisciplinary team of practitioners to large groups of patients as well as their caregivers. 23
Methods
Overview
This study operates at the intersection of health and other fields of study, such as the theory of social learning, knowledge management and ICT. The researchers approached the investigation through an integrative review to build a bridge between these related areas of work. 24 This integrative review aims to summarize past empirical and theoretical literature to provide a more comprehensive understanding of how to address a health care problem. 25
The hypothesis is that a VCoP may offer an excellent model of how to help caregivers learn how to deal with caregiving demands, and to support their informational and emotional needs. Accordingly, this research was conducted to critically examine the current evidence relevant to VCoP for caregivers, identify dimensions to be considered in its design, and suggest further venues of research. A literature review of the needs of caregivers was used and a separate study of VCoPs was developed, with the aim of seeking to link the two.
Literature search and data evaluation
First, research on the community literature was gathered. We started our search in February 2017 and we included literature published from 1996 onwards, because that is when the concept in health was first used. 26 A conventional literature search was undertaken using the MESH terms (Medical Subject Headings): “Community Network” AND “Caregivers” AND “Alzheimer Disease” AND “Internet.” The databases searched were Scopus, PsycInfo and PubMed. The inclusion criteria were reports written in the English language on communities with informal caregivers of Alzheimer’s patients. The exclusion criteria were literature not published between 1996 and February 2017; not written in the English language; focused on the patients or on health professionals; not referencing CoP theory explicitly. More than 300 citations from the reference lists of research reports were found. After we analyzed the first 20 studies, it was found that none of the citations for “Community Network” explicitly used CoP theory. The authors chose to conduct additional searches specifying CoP which are the focus of our research.
Then a second conventional literature search was undertaken with the terms “online OR virtual OR web 2.0 based OR internet-based” AND “Community of Practice” AND “Alzheimer” AND “carer OR informal carer OR informal caregiver OR non-professional carer OR non-professional caregiver.” Again, the search was carried out through Scopus, PsycInfo, and PubMed. The same inclusion and exclusion criteria as in the first search were followed. Other relevant literature, specifically books and book chapters, were identified through an iterative process based on the journal papers found. The integrative review from this point follows the six steps of a “berrypicking” approach 27 : footnote chasing, citation searching, journal runs, area scanning, author searching, and subject searches in bibliographies and abstracting indexing services. Through footnote chasing and citation searching several authors were identified: Barnett, Wenger, Hara and Le May. Regarding journal runs, two types were identified related to the project: health sciences and information sciences journals. Accordingly, journals of both fields where identified: Health Informatics Journal, Journal Computer Mediated Communication, Journal of Innovation in Health Informatics, Journal of Medical Internet Research, Journal of Research in Nursing and Health and Journal Web Based Communities. Afterwards, an area scanning which included CoP in health and VCoP in health was conducted to check all the theoretical models. The search strategy is set out in the following PRISMA flow diagram (Figure 1):
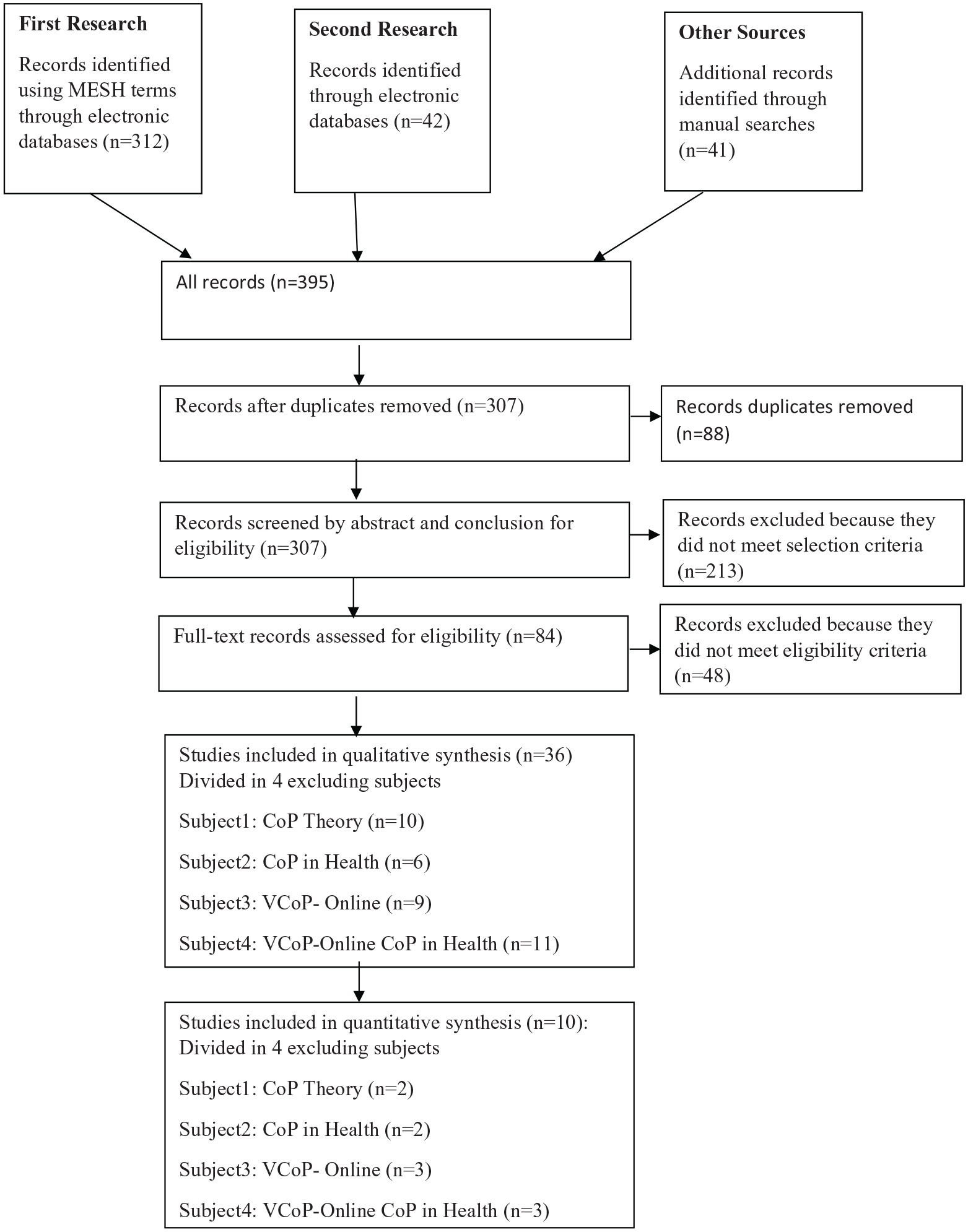
PRISMA Flow diagram outlining the search and review process.
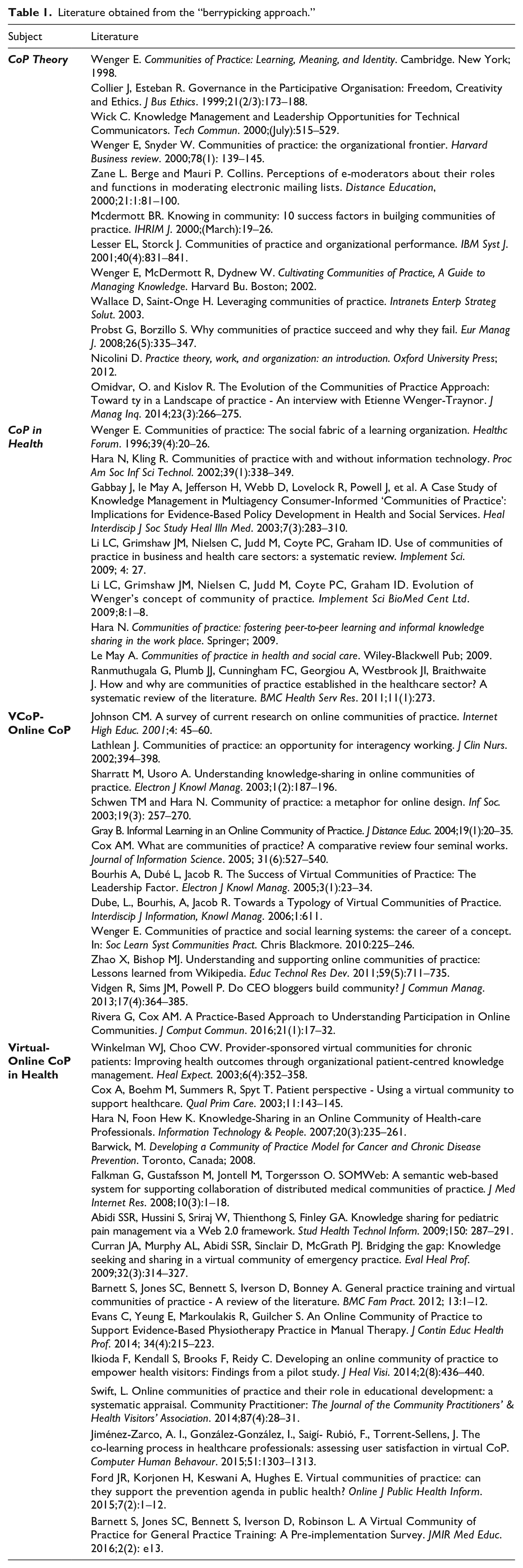
With the aim of gaining a holistic understanding of the possible adequacy of the VCoP as an intervention to respond to caregivers needs, literature was divided into four main subjects: CoP theory (12 records), CoP in heath (eight records), VCoP-online CoP (12 records) and Virtual-online CoP in health (14 records), (Table 1):
Literature obtained from the “berrypicking approach.”
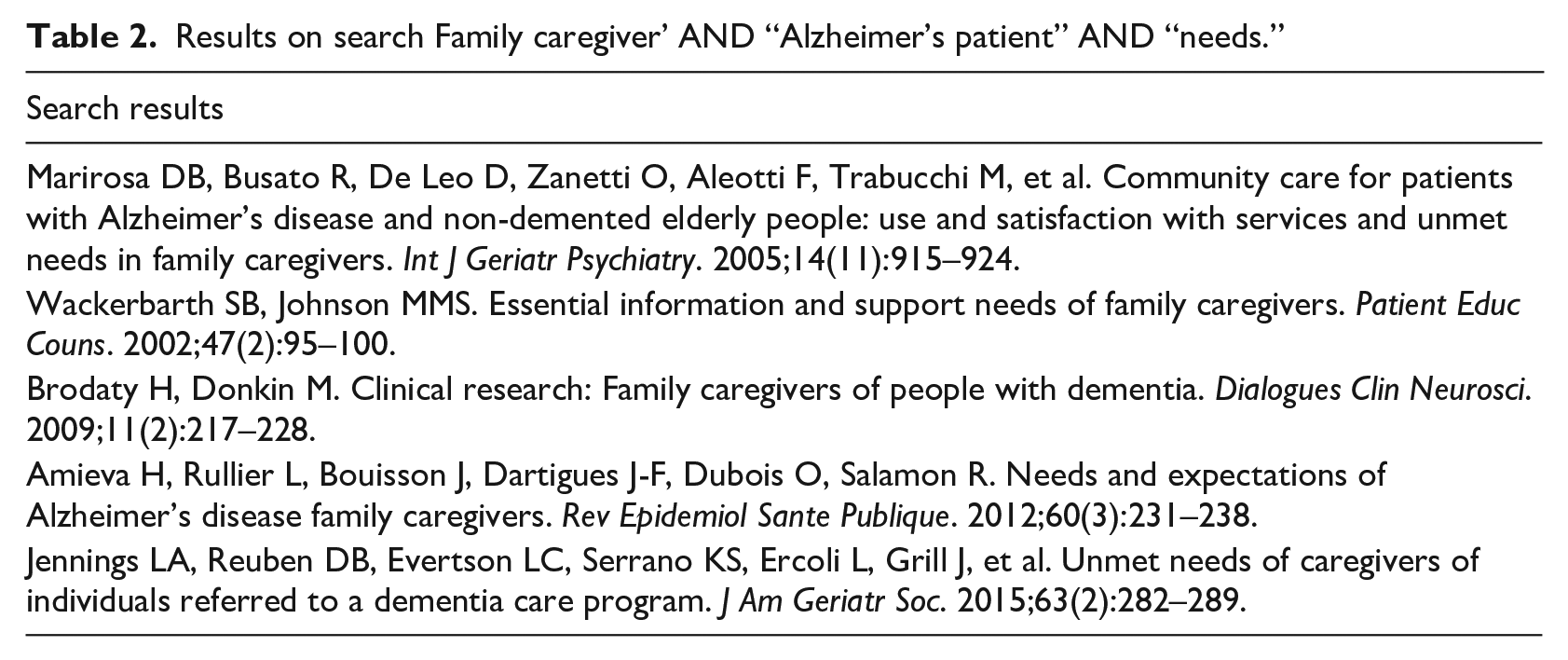
Separately a search on caregivers’ needs was undertaken using the terms “Family caregiver” AND “Alzheimer’s patient” AND “needs.” The search gained 51 results of which five met the inclusion criteria which was that items had to be literature regarding the needs of Informal caregivers of Alzheimer’s patients. Exclusion criteria was research focused on Alzheimer’s patient own needs and formal caregivers’ issues. Then, 46 results were excluded. None of the articles referred to VCoPs, indicating a gap in the literature which the study is able to fill. Results are shown in the following table (Table 2):
Results on search Family caregiver’ AND “Alzheimer’s patient” AND “needs.”
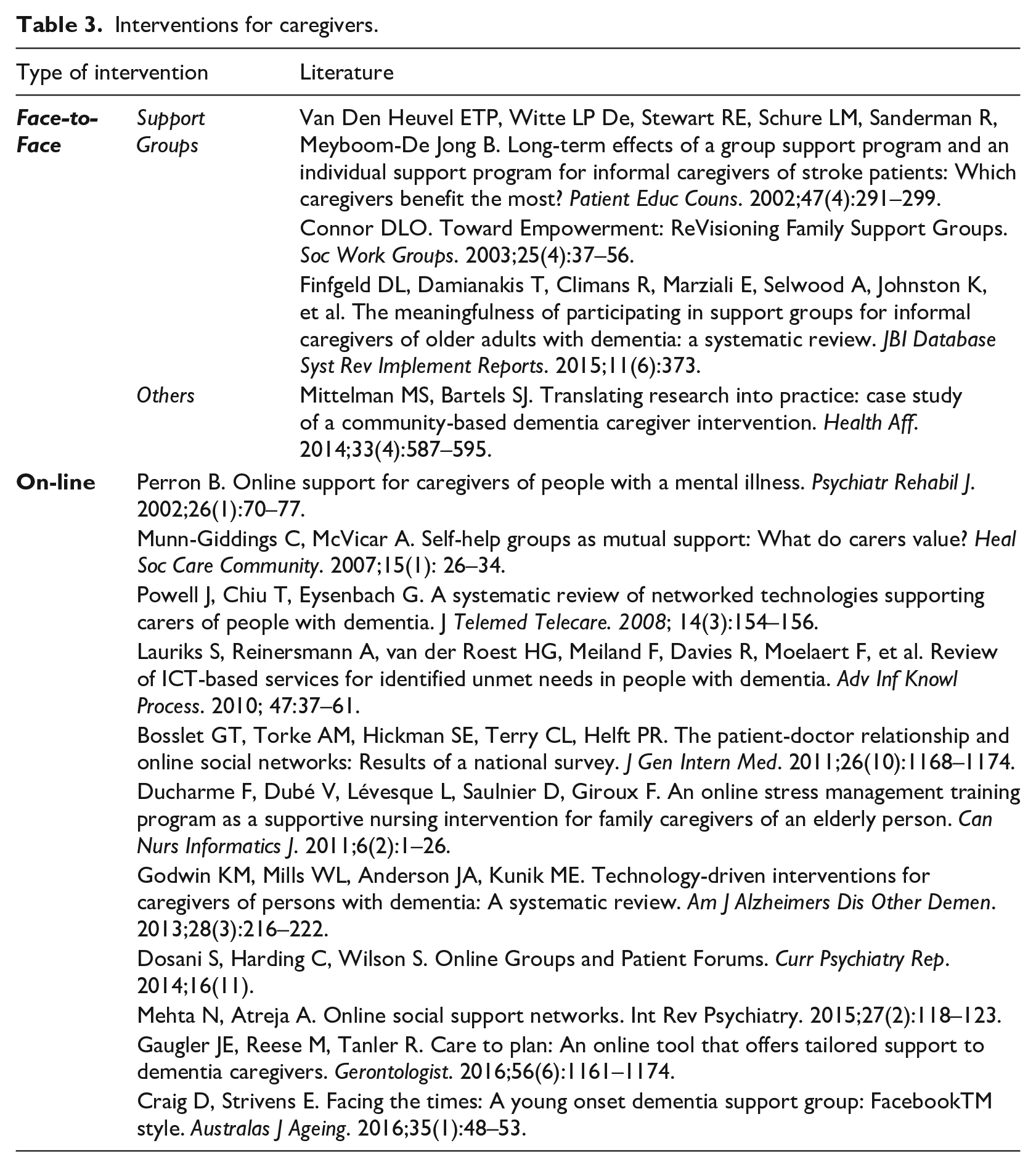
At that time, a search based on the terms “Intervention” AND “family caregivers” AND “Alzheimer’s” was launched. We obtained 81 results, from which 66 interventions focused on patients were excluded. The most common intervention was support groups. The 15 results were divided into face to face and online interventions (Table 3):
Interventions for caregivers.
Data analysis and presentation
All literature found in the course of the search, was critically reviewed. Through the exploration authors realised, besides the presence of several CoP definitions from 1991 to today, there are some models of VCoP in health since 1996. Researchers used Barnett’s proposed framework for VCoP in health 28 as a starting point to identify evidence-based principles to be considered in VcoP of caregivers design. Specifically, four dimensions out of seven were taken from this author’s model. Barnett’s framework has been shown to be effective in improving knowledge sharing, thus reducing isolation. 29 However, the full research suggested that the framework for VCoP for caregivers is a process more than a normative tool that encapsulates issues. 30 Moreover, in a recent study related to health and social care, new concerns appeared suggesting privacy and trust, 31 which were not mentioned in previous literature so concretely. These issues were then taken into consideration as part of the framework to achieve a successful health VCoP.
The literature of VCoP was analysed together with the information obtained caregivers’ needs and current interventions. Caregivers need to have support of their peers, get information and training about the disease. Furthermore, they are keen on improving the daily life management of their relative. We read the VCoP literature through the lens of these needs to identify key features of VCoPs. At the end of this process of integrative review are eleven dimensions for successful VCoPs of caregivers: Network Structure, Technology, Moderator, Scale, Alignment, Community Design, Sense of Trust, Knowledge Sharing, Sustainability, Ethics and Evaluation.
Results
Our analysis seeks to show the ways in which the interdisciplinary literature on CoPs and VCoPs can inform the process of building communities to address caregivers’ needs. The authors have identified eleven evidence-based dimensions of a VCoP which need to be considered in the caregiver context. The eleven dimensions are presented below sequentially but they should be seen as profoundly inter-related.
Network Structure is the first dimension. CoPs have a “bottom-up” social structure that facilitates learning through interactions and relationships with others who share a common practice. 16 This mirrors the way that caregiving occurs in a social relational context. 15 Contact with other caregivers give rise to real effects on the perception of self-efficacy and decreased stress, depression and burden on the caregiver.32,33 Furthermore, contact with other caregivers reduces feelings of isolation 34 as they meet their needs for social support and experience less stress. 35 Network structure may start with an already existing carer support organization in order to create the social structure of the group. 36
The second dimension is Technology as it plays a critical role in supporting a community. The VCoP literature attests to the importance of selecting technologies that align to the feel of a particular practice. 37 Virtuality frees members from constraints of time and space20,35,38 and it facilitates timely acquisition of information, 39 which caregivers need. It provides strategies promoting caregivers’ health behaviour by increasing knowledge.20,35,40 Technology contributes to answer caregivers’ demand for social support and helps them experience less stress. 41 Caregivers want to share information so need quick ways to communicate (as with chat tools) and perhaps also to store and organise shared knowledge which could support quality assurance. But they also want to tell complex stories of experience and need to build trust and learn from each other. Hence, there must be functions to support some level of sharing of individual identity, like self-profiling.
The Moderator, as a community coordinator, is the third dimension. The CoP literature is replete with wisdom about defining the leadership role of a group member who helps the community focus on its domain, maintain its relationships and develop practices. 16 He/she plays an integral role in enhancing the functioning of the community and facilitating learning. 42 For caregivers, the role of moderator could be taken by health professionals or by an expert caregiver, but it could also be a peer. The moderator will have the role of facilitator of information sharing, will help to activate knowledge sharing and give support to all the members both within the caring context and the technological one.40,43
The fourth dimension is Scale. In CoPs the membership size is not fixed, but it is recognised that the size of the group is a critical dimension to its success. 44 In communities for chronic patients, the smaller, more controlled size of the private community render it more sustainable as a social structure. 36 Scale needs to be controlled as caregivers require social support because stronger ties enable sharing difficulties about coping with the diagnosis and the day to day experience of caregiving. 45
The fifth dimension is Alignment. Within CoP theory it is recognised that a community is driven by the value members get from it. 46 This value comes from the alignment of three related concepts: domain (common ground), community (social structure) and practice (specific knowledge the community shares, develops and maintains). 16 In addition, individuals’ collective and organisational motivations must be aligned. 47 If these two alignments are achieved, then members gain many advantages. For caregivers, alignment provides benefits such as help with practical challenges, access to expertise, 43 better ability to contribute to the group, confidence in one’s approach to problems, fun from being with peers, more meaningful participation to more sense of belonging. 16 All these mentioned benefits would help caregivers to satisfying their needs.
The sixth dimension is Community Design. CoP as a perspective recognises the evolving nature of community. The focus of a community develops and shifts. It has cycles of energy and quietness. In the early stages trust needs to be built. Higher level functions such as successively information sharing, knowledge-sharing and creation come later. These reflections resonate with the pattern of caregiving, with its highs and lows. It is the catalyst for community growth and development as it concentrates in emerging participation. 16 As the community grows, it develops a systematic body of knowledge. Caregivers, having sense of community, would realise their involvement with the community is translated into something useful as better caring for the patient, a better carer-patient relationship and better perception of their own role. 48
The seventh dimension is Sense of Trust. The most fundamental insight of CoP theory is that common experiences arising from a common context, help people to relate to each other. It is the common mundane experiences of caregiving that make them a potential community. Further, working towards a common vision for a community enables participants to build trust and relationships. 49 As a VCoP forms, it creates a sense of belonging for community members, and they develop the habit of consulting each other for help. 50 VCoP of caregivers’ members would develop norms of trust, reciprocity and cooperation that support knowledge sharing. As a consequence, caregivers are encouraged to use their real names and create authentic profiles to reinforce the sense of trust. 51
The eighth dimension is Knowledge Sharing. In the CoP perspective this is one of the main objectives of a community. Practice related knowledge is the specific form of knowledge the community shares, develops and maintains. 52 In the caregiving context, this would be everyday knowledge of how to offer care, how to deal with the patients’ varying condition, and other practical wisdom about living with dementia. VCoP is a very suitable framework to share and learn for caregivers where the domain, the caring of Alzheimer patients, creates the common ground and outlines the boundaries that enables them to decide what is worth sharing and how to present their ideas. 16 Acquiring and sharing knowledge, caregivers will have more information about the own patient’s illness, and about the use of resources and services which are the main caregivers demands. 53 In the case of the VCoP of caregivers including health care professionals as moderators, they would contribute mainly introducing evidence-based practice knowledge. Caregivers, from their side, would collaborate sharing their own experience and learning skills for improving daily life management of their relative which is one of their biggest concern. 9
The ninth dimension is Sustainability. In order to sustain a CoP, members have to remain motivated in their quest to highlight and share good practice with peers. 54 If caregivers realise that they can reach their needs within the VCoP they will keep engaged. Sustainability provides caregivers serenity, tranquility and psychological well-being and freedom helping caregivers meeting their needs. 55 Finally, VCoP of caregivers integration with an already existing patient/carer support organization may render it more effective as a social structure. 36
Ethics is the 10th dimension. CoP theory carries with it a particular sense of ethics of participation. Within a CoP or VCoP, everybody is viewed as an equal. 56 Furthermore, participating in a VCoP is voluntary. In respect of caregivers, this self-selection inside a non-competitive environment offered by the VCoP provides serenity and tranquillity to them matching their demands. 55 A VCoP of caregivers should prioritise patients’ privacy. Moreover, the moderator has a key role in ensuring confidentiality and patient’s data protection. If a moderator is a health professional, caring for patients/clients in practice reflects the ethics of the health professional and could create a motivating crucible for the renegotiation of boundaries. 57 Finally, there is a concern about a possible over reliance or even technology addiction from the caregivers perspective. 58
The 11th and last dimension is Evaluation. Communities need measures to capture and celebrate their achievements and to guide ongoing efforts to become more vibrant and effective. A CoP’s value may be measured through its activity. 16 Periodically, it is necessary to analyse if the results obtained by the CoP coincide with the results expected. The CoP literature proposes assessing the value of a CoP qualitatively, for example by collecting stories about its benefits. Telling stories not only helps individuals to develop an identity, but also serves to reconstruct the identity of the collective community on ongoing basis. 16 Furthermore, to measure the usability of the technology is a key issue. 59 Applied to VCoP of caregivers, validation of one’s practice with others who share a similar situation may affect one’s own life orientation satisfying their needs. 52 This process could be completed either by asking to members about their satisfaction with the community through surveys or suggesting them to tell stories which might help both to construct identity as an individual (caregiver) and to reconstruct the identity of the collective community of caregivers. Finally, in a VCoP evaluation by caregivers of the technology should be performed using usability tests. The results given by the different analyses should be contrasted with the expected results of caregivers. 59
Discussion
The current study suggests well-designed interventions based on VCoP principles have the potential of addressing caregivers’ needs confirming the research hypothesis. Eleven dimensions have been identified to be considered in the design of this VCoP: Network Structure, Technology, Moderator, Scale, Alignment, Community Design, Sense of Trust, Knowledge Sharing, Sustainability, Ethics and Evaluation. Reflecting the organic, dynamic and living sense of the caregivers’ VCoP, having in mind the analogy made between cultivating a plant and establishing a CoP 16 and, acknowledging there is a growing awareness of the importance of metaphors in theory development, 60 we propose a Tree Metaphor to present our research (Figure 2). A tree has roots, trunk, branches and crown. This tree has five roots which will grow up consecutively one by one starting from Network Structure, then Technology, Moderator is the third one, later Scale and, finally, Alignment. These five roots will form a strong basis for the tree allowing it to grow a strong trunk, the Community Design. Hence, roots are the five pillars for the trunk. The trunk should develop three branches representing first, Sense of Trust, then, Knowledge Sharing and finally, Sustainability. The tree crown, which will protect and make it brighter, will be the Ethics and Evaluation concepts.
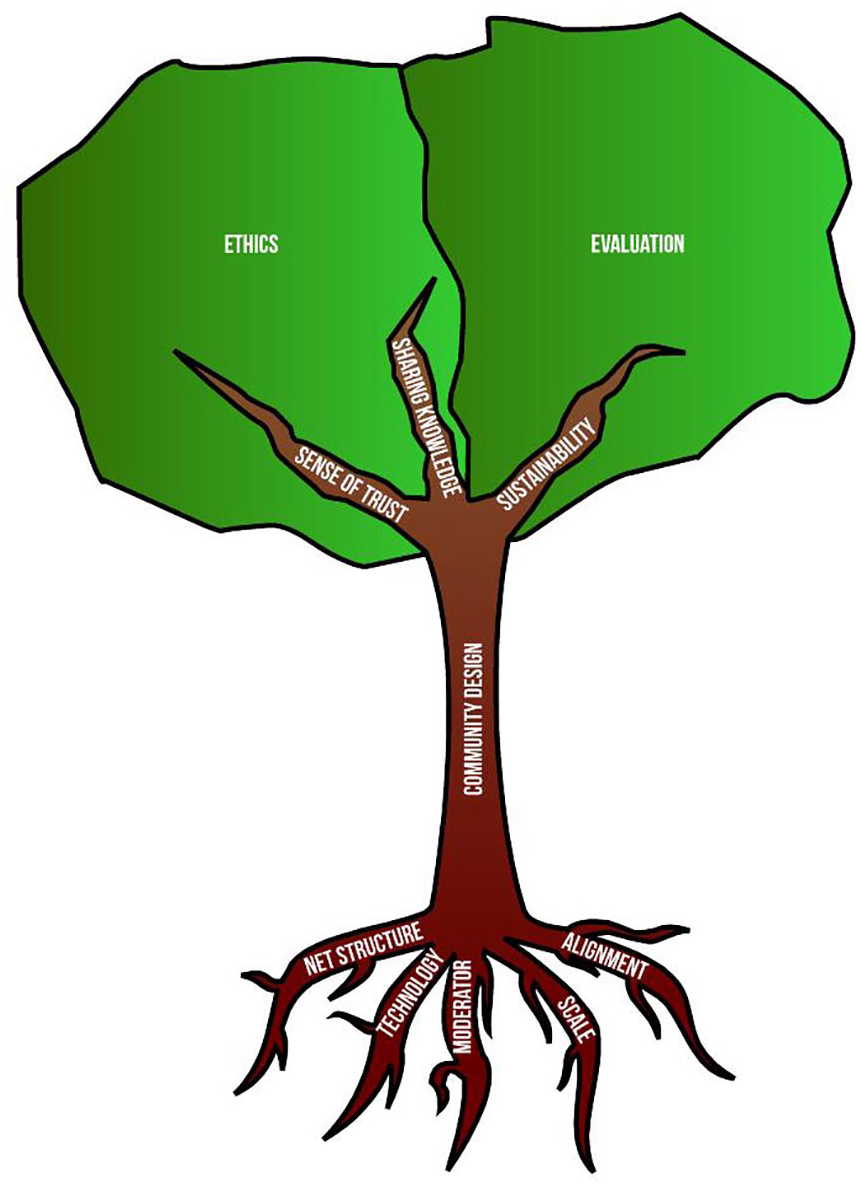
Tree Metaphor.
Cultivating VCoP to improve healthcare performance requires a greater understanding of how to establish and support VCoPs to maximise their potential to enhance healthcare. 18 Therefore, once the tree has been grown, it needs to be watered by the institution from whom depends the community, if it is the case, and from its own moderators and members. Members of the community are part of the tree and they will water it themselves giving value to the community through their own practice. Likewise, health professionals will water the VCoP prescribing it to caregivers and disseminating the VCoP of caregivers with other colleagues. In so far as the tree is duly watered, roots underpin it and the tree will continuously grow (trunk and branches) and having the crown green which means the tree is in good health. The main goal is to have a healthy and strong tree. However, not only watering the tree is important, weather may impact positive or negatively to the tree life. Community interaction with outside may be at two levels: individual or collective. Therefore, favourable and unfavourable weather may come from health and social policies, health and social institutions and professionals, non-members caregivers, caregivers’ members and non-members friends or relatives, and other cases too. Weather may influence the tree differently depending on the tree’s state of health.
Conclusion
Through this research we critically examined the current evidence relevant to CoP and VCoP and we identified eleven dimensions to be considered in the design for a VCoP for caregivers. We may conclude that even though the VCoP concept has not previously been used to design online interventions for caregivers, it seems that it could answer caregivers’ demands.
A VCoP of caregivers can accomplish three objectives that would make them superior to face to face support groups. 11 First, a VCoP of caregivers would be a long-term group, which was open to new members and could be led by fellow caregivers instead of professionals. Secondly, it is an intervention focused on the personal objectives for the caregiver regarding themselves and the relative they take care of. Thirdly, the VCoP of caregivers’ purpose is to create, expand, and exchange knowledge, and to develop individual capabilities. Hence, participating in a VCoP is a caregiver’s own choice based on the way it provides access to expertise, help with challenges, confidence in one’s approach to the problem, sense of belonging, fun of being with colleagues and more meaningful participation, covering their demands. 11
This analysis offers a useful contribution to the literature as several protocols and principles previously emerged regarding to VCoP61,50 and, specifically focused in health, 28 were mainly for professionals and sometimes patients, however not for caregivers. Naturally, it remains to be tested empirically how decisions about these dimensions might shape the character of a VCoP for caregivers.
Future research should consider the implementation process for a VCoP of caregivers. Furthermore, virtual reality (VR) is another technology to be explored. VR is now being used for older adults and cognitive rehabilitation.62,63 However, at present, informal caregivers still have many technological barriers as digital skills and bandwidth, and so these issues should be taken into account for future VR based applications. Ultimately, given that the way that caring affects caregivers’ quality of life, 3 the VCoP could be evaluated by its impact on their well-being.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.