
Abstract
Evidence highlights the intrinsic link between nurse staffing and expertise, and outcomes for service users of healthcare, and that workforce retention is linked to the clinical and organisational experiences of employees. However, this understanding is less well established in mental health. This study comprises a retrospective observational study carried out on routinely collected data from a large mental healthcare provider. Two databases comprising nurse staffing levels and adverse events were modelled using latent variable methods to account for the presence of multiple underlying behaviours. The analysis reveals a strong dependence of the rate of adverse events on the location and perceived clinical demand of the wards, and a reduction in adverse events where registered nurses exceed ‘clinically required levels’. In the first study of its kind, these findings present significant implications for nursing workforce policy and present an opportunity to not only improve safety but potentially impact nurse retention.
Introduction
Since the publication of To Err Is Human, 1 patient safety has received growing attention from researchers and policymakers worldwide. 2 The National Health Service (NHS) in England is no exception to this and remains the subject of numerous reports condemning the state of patient safety and highlighting insufficiencies that contribute to patient harm.3–5 Evidence suggests that one in 10 patients come to harm as a result of healthcare, and almost half are considered avoidable. 6 However, understanding of staff safety is far more limited. 7 Staff safety is pertinent in the current climate within the NHS, which is facing a growing shortage of overall staff,8,9 and registered nurses (RNs) in particular.10–13 Safety measures within healthcare have historically related to the patient. The collection of data on ‘violence and aggression’ in the Mental Health Safety Thermometer is a recognition of this being a common harm experienced in this care setting. 14 However, the metric does not distinguish between harm to other patients and harm to staff. There has been some qualitative work that highlights the concept of the absence of threat of harm to staff as being essential for nurses to be able to work effectively in the inpatient psychiatric setting, 15 but there is little published research quantifying staff harm and exploring its relationship with staffing.
Of the limited research that is available regarding staff harm and safety measures, it has been found that feelings of safety correlate with experiences of stress and burnout. Evidence suggests that concern for personal safety is a high stressor and can contribute to burnout. 16 Given that higher burnout has been linked with staff being more likely to view their work environment as ‘unsafe’ but reduces the likelihood of ‘near misses’ being reported, 17 staff wellbeing is important in ensuring both an adequate workforce and being able to accurately capture the state of safety in healthcare.
The NHS currently utilises a number of operational databases for adverse events reporting and management of staffing levels, which collate routine patient and operational data that could be used for such purposes. The inherent availability of large, routinely collected datasets,18,19 alongside the emerging power of machine learning and knowledge-driven decision-making tools, 20 has been championed as a promising area for improving healthcare services.21,22 Indeed, the overlap between patient safety and staffing has been well established utilising such datasets.23–27
This study utilises existing data from a large English mental healthcare provider of both acute and community services, focusing on the analysis of reported incidents to examine how such data can be used to monitor and predict where staff safety may be at risk. We examine the extent to which the perceived demand for RNs and unregistered nurses, as well as the variations from the ‘clinically required’ levels, is correlated with increases in staff adverse event reporting. By utilising the clinically perceived requirements in place of the pre-planned levels, the analysis better reflects the shift by shift requirements.
This study utilises anonymised, routinely collected administrative data and therefore was not subject to NHS ethical approval. HRA algorithm institutional ethical approval was sought and granted by the University and access was granted by the participating trust’s research and development department following protocol review.
Data selection criteria
Two databases were extracted from a large English mental healthcare provider in England providing both acute and community services – one containing safety incidents and one containing nurse staffing data. The nurse staffing dataset comprised a single data table detailing the ward-level nursing complement on each shift (early, late, and night) by nurse type (registered or unregistered) specifically for inpatient areas. In addition, the dataset comprised the ‘planned level’ and ‘clinically required level’ of nurse staffing. The planned level was determined annually in line with available budgets, whereas the clinically required level allowed clinical staff to report additional staff requirements in accordance with demand and clinical judgements for safe staffing. The incident reporting system is a commonly used system for reporting adverse events comprising a web-form for data capture and SQL engine for data storage. The data storage element comprised two key data tables – one detailing the incident (including location, severity, likelihood to repeat, and date) and the other detailing those involved (patient vs staff, victim vs perpetrator vs witness, age). The database was initially aggregated to day and ward level, pooling adverse events to find the total daily rate. This selection was then aligned with the trust’s staffing database by date and ward ID.
The co-variates of interest selected from the staffing database were the clinically required staffing level and the variation of actual staffing from the required levels for each of the three shifts (referred to as the
The variation from the clinically required staffing levels was used instead of the absolute staffing level to reduce the collinearity of the covariates. Where the level of staffing is less than the clinical demand, we can infer a situation in which staff members must optimise their time, with a greater risk of tasks going undone or work being rushed. Hence, where staffing levels are less than the demand requires, we could expect to see low priority tasks (such as the reporting of near misses) going undone.
The other confounding variable included for analysis was the geographical location of the ward. The data from this trust were tagged within the incident reporting database for one of 10 geographical locations, which have been pseudonymised for this analysis. A brief description of the specialties and characteristics of each location are supplied in Table 1.
Location descriptions.
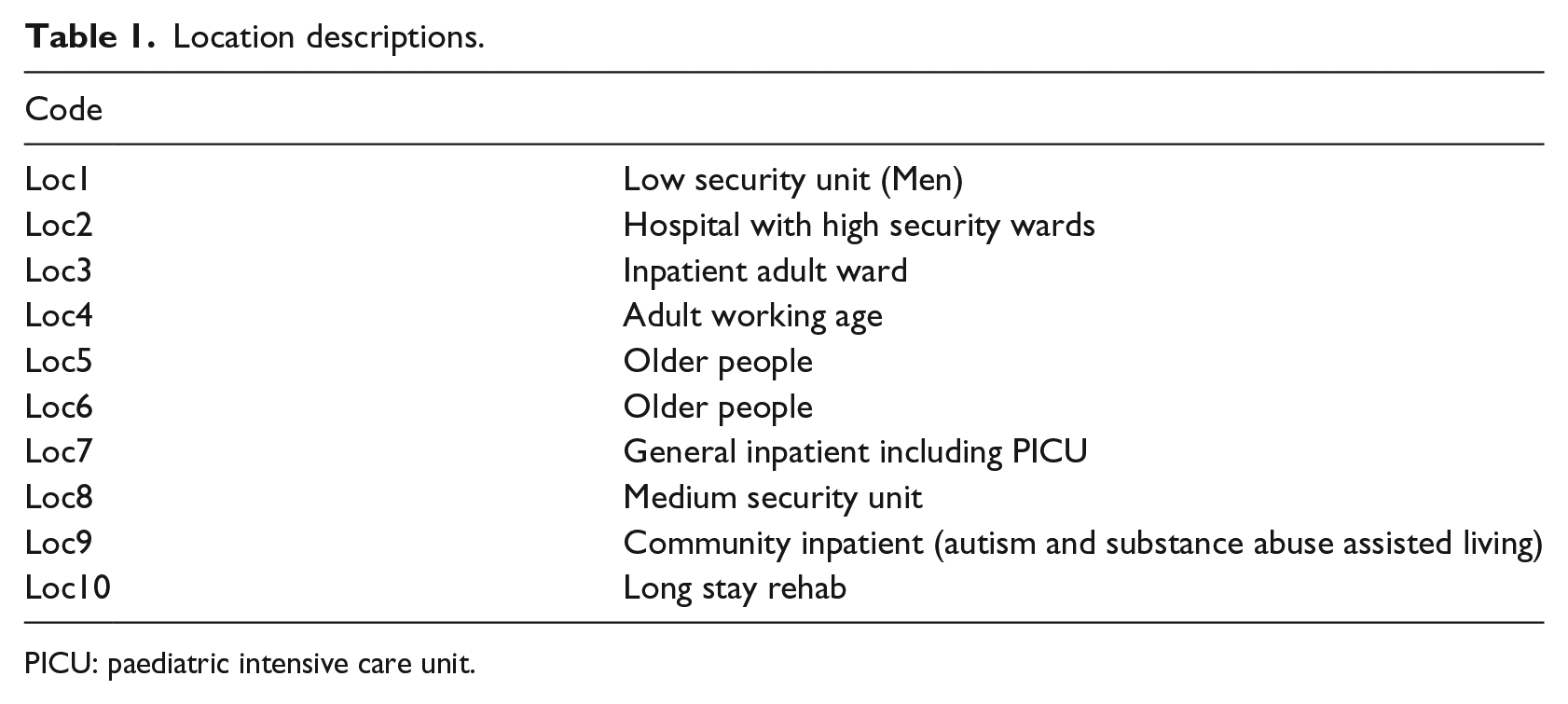
PICU: paediatric intensive care unit.
Each feature of the constructed dataset was inspected as histograms in order to remove extreme outliers, which were then classified as miss-entered data, constituting 1.2 per cent of the extracted data. The analysis subsequently addressed the relationship between the variation of nurse staffing (by shift) and perceived clinical demand on the rate at which members of staff were reported as victims of adverse events. The definition of ‘victim’ arises from the event reporting system where each individual is flagged for their involvement, for example, ‘victim’, ‘perpetrator’, or ‘witness’. To allow for variation in ward sizes, the rate of reports was corrected for the total number of nurses on shift for a given ward and day. The analysis hence models the number of staff reported as victims of an adverse event per nurse on shift as a function of perceived clinical demand, and variation in staffing from the perceived clinical demand with location ID serving as a proxy for safety and reporting culture.
Method
The data were analysed via a selection of count-based models including Poisson, zero-inflated Poisson, negative binomial, and hurdle regressions. 28 The Poisson regression is the typical form of general linear model to apply to count data, with the others dealing with variations from the basic Poisson distribution. The negative binomial regression is designed to model count data with over-dispersion (i.e. larger error variance than allowed for by Poisson regression), while the hurdle and zero-inflated regression models count data that contain more zeros than is typical of the Poisson process. Each analysis routine used the well-documented implementations in the R language in the PSCL 29 and MASS 30 packages. Model comparisons were made using the Bayesian information criteria (BIC) in which a smaller BIC score is indicative of a superior model. 31
Subset selection was carried out via LASSO-regularised regression routines,
32
in particular the Poisson and binomial-family glmnet algorithms implemented in R by the glmnet package.
33
The LASSO-regularisation approach aims to extract the smallest subset of features that explain the model without the reduced error bars inherent in stepwise selection.
34
The regularisation parameter λ was tuned via 10-fold cross validation (CV), and model coefficients are reported for the ‘one standard error’ λ term,
The Expectation–Maximisation (EM) algorithm36–38 used in the study makes use of the ‘emax.glm’ R implementation. The data analysis was limited to two competing Poisson regression models for simplicity, using 20 randomly selected starting conditions to perform early ending fits in order to explore the parameter space and check for an optimal starting point.
Results
The aggregated dataset analysed comprised 40,123 observed days (total) divided between 51 wards and 10 locations (see Table 1 for descriptions). The data were recorded over 3 years as part of the routine function of the trust with the earliest observations taken from September 1, 2014, until March 31, 2017. Within the study, there were 10,119 events reported, accounting for 19,693 members of staff being the victim of an adverse event, inclusive of near misses and non-harm incidents. The events reported have a raw prevalence of 0.252 (±0.004) events reported per ward per day and 0.491 (±0.009) members of staff being a victim of an event per day per ward.
Prior to analysis, the rate of adverse events where staff were victims was first characterised before removing outliers. The majority of day–ward combinations resulted in no adverse events being reported, accounting for 84 per cent of the dataset. Where events were reported, each was tagged for an incident type. Aggregating by incident type, the most prevalent events were ‘Aggression by Patient on Staff or Other’ (6520 events reported with 12,138 members of staff as victims), ‘Inappropriate Behaviour’ (1762 events reported with 4058 members of staff as victims), ‘Self-Harm’ (429 events reported with 929 members of staff as victims), and ‘Sexual Incidents’ (298 events reported with 493 members of staff as victims).
Initial trials of the Poisson model (BIC = 74,295) demonstrated evidence of over-dispersion, with the deviance residuals showing non-normal behaviour on a Q-Q plot (see Figure 1(a)). The model dispersion was estimated at 3.07 via auxiliary ordinary least squares (OLS) regression (with an associated p value below numeric precision) implying over-dispersed errors. Trials of the dispersion-corrected count models showed an improvement in the BIC scores, with the negative binomial giving the optimal model (BIC = 52,726) compared to the zero-inflated (BIC = 56,928) and hurdle (BIC = 56,916) models. The negative binomial model resulted in a sizable reduction in the BIC score in comparison to the Poisson model, indicating that the reporting of adverse events is better explained by the negative binomial model.
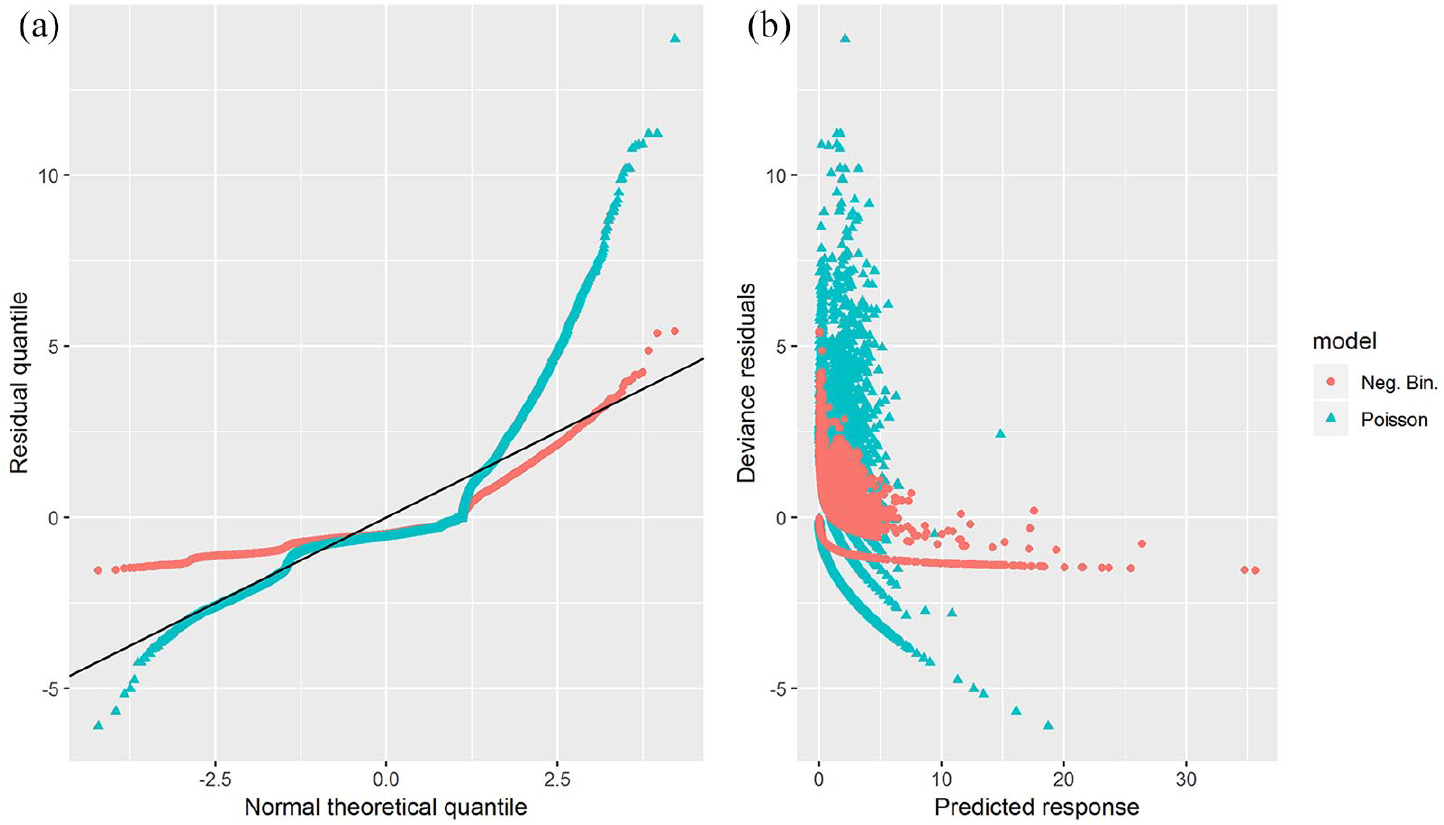
Comparison of residuals via a) QQ-plot and b) prediction-residual plot for the Poisson and negative-binomial regression models.
Despite the improvement in BIC score, inspection of the negative binomial deviance residuals reveals a distinct structure. Notably, the model shows a bias to under-estimating larger values (Figure 1(b)) and a strong discontinuity in the Q-Q plot (see Figure 1(a)). This behaviour may well be explained by having two competing processes – one driving the inflated zero counts and the other the expected Poisson behaviour.
Two competing behaviours are relatively common, and should, in theory, be well modelled via the hurdle or zero-inflated models. However, if the variables being modelled do not account for which of the two behaviours dominate, these models will have only limited performance. As an alternative, we turn now to consider how well a latent variable model, such as the EM algorithm, explains the data.
Having fit the EM algorithm, the data were found to be well divided between the two models. Dividing the data at a model-probability of 0.5, the two models show remarkably different average rates of adverse events per nurse on the ward of 0.175 (±0.002) and 0.00087 (±0.00004) for 5908 and 34,079 observations, respectively. With these values in mind, it appears that the system is divided between adverse events being reported at a moderate rate and at a low rate. We, hence, adopt the term ‘Moderate Reporting Model’ (MRM) and ‘Low Reporting Model’ (LRM) to describe the two competing scenarios.
To explore how well we can predict which model applies to a new observation, the LRM probabilities arising from the EM algorithm were fit using LASSO-logistic regression. By aggregating the data into two groups, LRM versus MRM, the regression becomes a binomial regression problem and is hence referred to as the Binomial Model (BM). The initial BM, performed using the same variables as the EM algorithm, showed some predictive power (‘receiver operator curve – area under curve’ score (roc-auc) = 0.7474). The roc-auc score takes values between 0.5 (unable to predict the correct model) and 1 (perfect prediction of the correct model), with a value of 0.75 suggesting only moderate predictive power.
To improve the predictive power of the BM, the covariates were expanded to include the last reported rate of adverse event on each ward. The addition of the extra term dramatically improved the roc-auc score (0.9983, near perfect prediction). This suggests that the model division learnt through the EM algorithm may be well predicted for new observations, not merely learnt retrospectively, and is highly dependent on the previous reporting rate. The parameter values for the optimal BM are given in Table 2, and the odds ratio and confidence intervals for the staffing parameters are included in Figure 2 where a positive parameter value indicates a preference for the LRM.
Location parameters for the three models (with 95% confidence intervals and significance level).
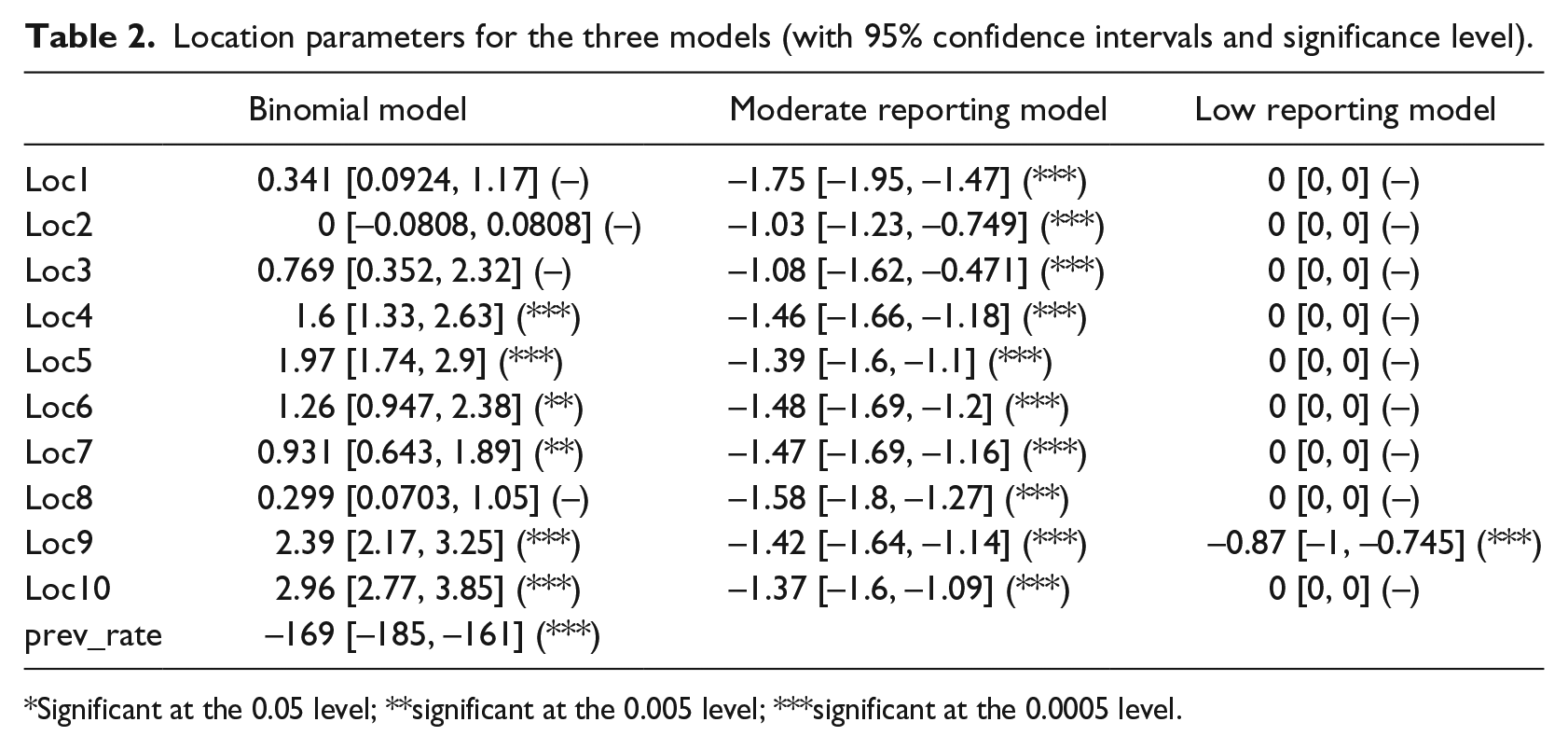
Significant at the 0.05 level; **significant at the 0.005 level; ***significant at the 0.0005 level.
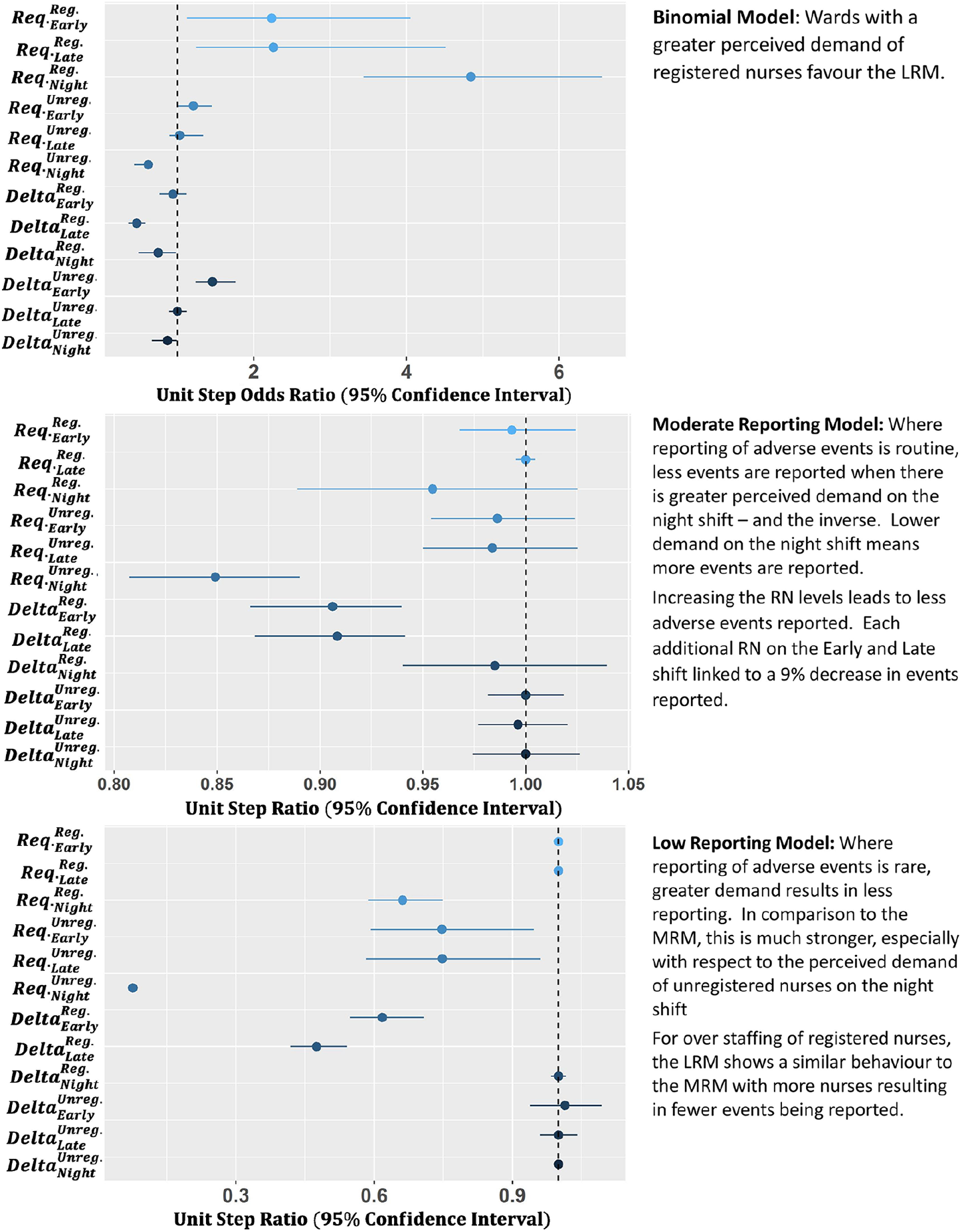
Bootstrapped 95 per cent confidence intervals for the staffing parameters across the BM, MRM, and LRM.
BM interpretation
The BM, which describes the likelihood of an observation belonging to the LRM, shows a strong dependency on the location. Four locations (1, 2, 3, and 8) have no significant parameter, implying a baseline 50 per cent probability of being in either model, if demand is not considered. Of the other locations, there is a steadily growing likelihood of the ward following the LRM with Locations 6 and 7 having the lowest chance (75%), and Locations 9 and 10 the highest (93%).
Across the trust, the best predictor for which model will dominate (LRM or MRM) is the rate at which adverse events were previously reported. In general, the more the events are reported by a ward on the previous day, the greater the probability the ward will remain in the MRM. The level of reporting needed varies, with Location 10 requiring 0.017 events reported per nurse on shift to give even odds of either model. To put this into context, across the dataset, the average rate of reporting is 0.0265 (±0.0005) events reported per nurse, so each location can attain the MRM scenario.
The clinically required staffing levels show a marked effect on the BM as well. As the clinically required levels of RNs increase (i.e. as the demand for more clinical nursing skills increases), there is a growing preference for the LRM. Hence, a greater RN demand appears indicative of a decrease in adverse events being reported. Considering this dataset includes near misses, this is not overly surprising. As workload increases, there is a distinct possibility that staff will prioritise delivering care over reporting near misses or adverse events. The exception to this is the night shift for unregistered nurses, where a greater perceived demand leads to a preference for the MRM.
The delta staffing variables (variation from ‘clinically required levels’) suggest a shift to the MRM when the number of RNs exceeds the clinically required levels on the late and night shifts, and a shift to the LRM when the number of unregistered nurses exceeds the clinically required levels on the early shift. The increase in reporting with more RNs is unsurprising, considering that the more staff members that are present, the easier it is for events to be observed and reported. The lower reporting with more unregistered nurses than required may be due to the division in responsibilities between registered and unregistered nursing staff – it is not merely a question of higher headcount but the nurse’s professional practice and education as well.
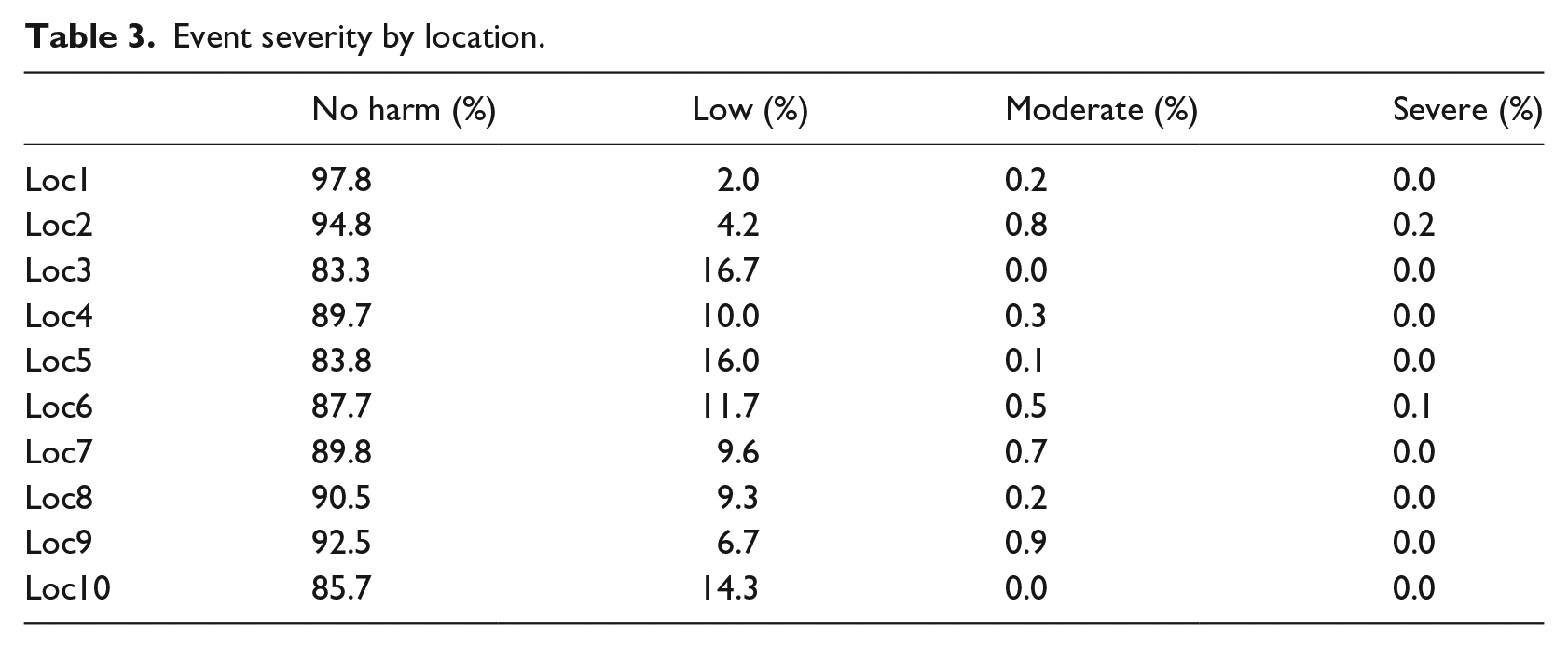
The strong dependency of the BM on location and previous rate of reporting suggests there is a cultural aspect to the divide between the MRM and LRM scenarios. Interpreting what a low reporting of adverse events and near misses means is complex, and we consider two competing hypotheses – a reduction occurs either because of less adverse events occurring or because fewer adverse events are reported. If the later of these is true, and the variation in reporting is due to changes in reporting culture, we would expect these locations to be biased towards reporting higher severity incidents. The result of this would be a decrease in the relative proportion of ‘near miss’ and ‘no harm’ events compared to higher severity incidents. Table 3 summarises the relative event severity across the 10 locations, and we observe that 3 of the 4 locations with the highest rate of ‘no harm’ events reported (Locations 1, 2, and 8) are among the 3 locations most favouring the MRM. It appears that a higher rate of reporting, as implied by favouring the MRM, is linked to a better reporting culture, as implied by the increase in ‘no harm’ events, and hence, the MRM should be considered the preferred behaviour we wish to instil on a ward.
Event severity by location.
MRM interpretation
Assuming that a ward’s event reporting follows the MRM, the rate at which events are reported is reasonably consistent across locations. The only exceptions are Location 1, which shows the lowest baseline rate, and Locations 2 and 3, which show the highest. Considering this model is consistent with a good reporting culture, we can assume that the shift in rate is due to shifts in prevalence of adverse events. Location 1 being a low security location while Location 2 being a high security location could be the reason for this shift in inherent safety of the location.
In the MRM scenario, the rate of reporting appears to be weakly linked to the clinically required staffing levels. The only significant parameter is the required level of unregistered nurses on the night shift, where each extra unregistered nurse required reduces the rate of incidents reported by 15 per cent. Fewer events being reported as the perceived demand grows implies more events reported at the lowest perceived demand. Considering that the night shifts generally run with the fewest staff members (between one to two RNs and zero to six unregistered nurses) where perceived demand is lowest, the risk of very low numbers of staff on shift would inherently increase. It appears that even a small increase in unregistered nurses on the late shift above what clinical staff perceive as being required can result in a strong increase in staff safety.
The reporting of adverse events in the MRM scenario also appears to be only weakly linked to variation in staffing. The only two significant terms show a reduction in adverse events on staff being reported as the levels of RNs on the early and late shifts exceed the clinically required levels. Given the assumption that these observations arise from wards with a good reporting culture, the remaining explanation is that more RNs result in a safer environment for staff.
LRM interpretation
Assuming that a ward’s event reporting follows the LRM, the rate at which events are reported is relatively consistent across locations, with only Location 9 showing a strong decrease in rate (58% decrease) compared to the others.
The LRM has the majority of its behaviour arising from the staffing parameters, with a strong link between increasing demand and decreased reporting on the night shift for RN staffing, and all shifts for unregistered nurses, though the signal arising from the night shift is by far the strongest. This supports the idea that as wards increase in demand, event reporting becomes increasingly rare, with staff members likely more focussed on the delivery of care than filling out near misses. However, the marked increase in signal for the night shift suggests that this may be in addition to the signal suggested for the MRM. A decrease in events being reported with more perceived demand means far more events reported when demand is low. Where the level of unregistered nurses on the night shift is low, the risk of low staffing levels would be enhanced, and more obvious accidents occur (e.g. of a higher severity than near miss).
The reporting of adverse events in the LRM scenario shows a similar link to variation in staffing as the MRM. The only two significant terms show a reduction in staff adverse events being reported as levels of RNs on the early and late shifts exceed the clinically required levels. Whether this is a result of improved safety culture or indicative of something else is hard to say.
Discussion
The marked improvement in BIC as the model moves from the standard count behaviours to the mixed Poisson behaviour suggests that the reporting of staff adverse events is relatively complex. There is strong evidence that the trust’s rate of staff being victims of adverse events is not continuous across the locations operated, with some locations reporting far fewer incidents than others. This variation in reporting appears to go hand in hand with an improved culture of reporting ‘no harm’ events where a greater number of incidents are reported, and suggests that of the two models extracted, the MRM represents a desirable culture.
Across all locations, there is strong evidence that the clinically required level of unregistered nurses on the night shift is inversely proportional to the rate at which staff members are reported as the victims of adverse events. Both LRM and MRM scenarios suggest that as the clinically required staffing levels of unregistered nurses decrease, the rate at which staff members are recipients of adverse events increases. The extent to which ward staffing varies from these required levels is relatively small, in general falling between 1 over or under the required level, and hence, a low required level is indicative of a greater risk of very low staffing levels, which could explain why the number of adverse events on staff increases where the locations have a lower clinically required level of staffing.
Considering the majority of adverse events suffered by staff members arise from aggressive/inappropriate behaviour, and sexual incidents, the combination of low clinical demand and a greater risk of very low staffing levels establishes a clear image of a high-risk environment for staff members. Such a risk is becoming increasingly well-understood as the growing demands on community nursing lead to higher lone working; 39 however, the safeguarding needs may be unlikely to transport easily across disciplines.
The greater risk of harm that may be associated with very low staffing levels may also be countermanded by an increase in RN staffing. The analysis shows that RN levels exceeding those recommended by clinical judgement on the early and late shift were linked to a decrease in adverse events on staff. Interestingly, equivalent behaviour on the night shift was not observed, although this may be due to the relatively low variation in RN staffing on the night shift in the dataset (83% of shifts running at the correct level with 12% running one under and 4% running one over). Alternatively, the increase in RN levels on the previous shifts may result in fewer tasks going undone and reducing the pressure on the night shift, resulting in a safer environment. 40
An increase in RN numbers has already been linked to improved patient outcomes;26,41 however, the effect of increased nursing levels may also lead to greater nurse retention. Considering the reported links between increased nurse stress with poor retention 42 and a poor perceived safety culture with burnout, 17 it is foreseeable that staffing above the level set from clinical demand may have compounded benefits. If the wards considered to have the lowest clinical-requirements received just a small increase in RN levels, it may lead to not only fewer staff members experiencing harm, but potentially reduce staff turnover and improve the safety culture. Clinical judgement is clearly of use in determining staffing levels; however, it needs to be complimented with operational considerations. Increasing the use of RNs is a growing ‘silver bullet’ by which we can fix the pressures faced by the NHS, but increasing demand does not fix the issue of supply.43,44
Although the findings of this study suggest that increased staffing could improve staff safety, in reality, the system is far more complex than this. Consideration needs to be given to optimal improvements in the context of budget and resource constraints. It is intriguing that shifts in unregistered nurse levels showed a far weaker link to the rate of events reported, suggesting that this is not a ‘bodies on the ground’ problem but rather something to do with the attributes of the RN. The dynamics involved in the skill mix of a workforce are not linear, and safety cannot be improved by simply increasing the proportion of the unregistered workforce. Furthermore, increasing staffing indefinitely does not yield respective increases in safety indicating other factors are at play. Griffiths et al. 44 highlighted that wider leadership and environment factors played a significant role, alongside having the right numbers of staff. The absence of real-terms increases in healthcare budgets in the context of growing demand, during a time of austerity and government instability, compounds the issue of growing demand, both in volume and complexity, and a solution to this is not imminent.
The exploration of this incident reporting system for staff harms is novel; traditionally, research in this area focuses on harm to patients. However, to not consider the implication of more than 10,000 reported incidents, resulting in nearly 20,000 staff victims over 32 months in the context of nurse retention would be a missed opportunity. Data warehoused in incident reporting systems are rarely considered in aggregate form, where the scale of incidents can be truly understood and, therefore, actioned. Instead, organisations tend to deploy root cause analysis techniques to individual events that meet a particular threshold (typically severity), and this threshold may or may not include harm to staff. Given that it is known that poor staff safety is linked to burnout 16 and that there is a cyclical effect of burnout on perceived poor safety, 17 it is important for organisations to reflect on the available intelligence housed in their data warehouses to ensure safe working environments for their staff.
Finally, when considering the usefulness of this analysis and the underlying role of routinely collected data within healthcare as a whole, we should reflect on the human factor. It has been shown that transparency within an organisation, when it comes to decision making, is known to have a positive impact on reducing staff absenteeism, and increasing staff retention rates. The databases that underpin this analysis have analogues in all NHS trusts, of varying quantity and quality, which have often remained as isolated silos of knowledge, and yet, it is feasible to mine them for insight. The data may contain inherent biases and validity issues, which will only become clear as the data are explored, 45 but it is only as the value of the data to patient care is demonstrated to frontline staff that we can expect compliance to improve.
There are opportunities in other methodologies to explore the reasons behind the behaviours exhibited in these datasets, such as qualitative research methods. This sort of research could help generate hypotheses for areas of improvement, which could then be subjected to experimental design interventions to improve staff harm.
Conclusion
This study demonstrates a method for modelling routinely collected data from a single mental health care provider in the NHS to explore the extent to which clinical judgement of demand, and more notably variations from these clinically required levels, align with adverse event reporting. There appears to be a consistent theme of reporting adverse events across the trust’s separate geographic locations, with different lessons to be learnt depending on location, ward acuity, and shift.
The models suggest that the greatest risk to staff is present when night shift staffing levels are at their lowest, possibly as a result of very low staffing levels. This risk might be balanced by the addition of an RN, but does point to a limitation of clinical judgement. The required level to deliver care may be less than that required to protect staff. Establishing a good safety culture is inherently difficult; however, the reporting of no harm events does appear to be a key marker of culture. Once staff members have the resources to deal with the recognised clinical demand, they appear to have better confidence in taking the time to report events, allowing for a trust to learn from near misses before they grow to actual harm.
The variation in unregistered nurse levels from the clinically required levels showed the least effect on the adverse event rate, yet the inherent rate at which these staff members are required is linked. It appears that clinical staff recognise the task required of unregistered nurses, but the wards show high resilience to under-staffing, while over-staffing gives little benefit. It is not only a question of increased headcount, but of the skill-set and expertise they bring to the environment.
Finally, the way in which we value healthcare staff has been brought to light here. Traditionally, the concept of safety is prepositioned by ‘patient’, and so, safety in healthcare is conceptualised as patient safety; little consideration is given to the safety of the staff delivering care. In a time where workforce retention is proving difficult and the quality and safety of care to patients is compromised, greater efforts should be made to improve staff safety, which might improve retention and simultaneously patient safety.
The methods presented represent a flexible approach to mobilise knowledge from the growing silos of routinely collected data in order to shape local safe staffing practices. They demonstrate that the analysis of such data via the application of data mining techniques represents a currently untapped opportunity to improve staff safety in healthcare.
Data are not currently available in a suitable format for open access. If you would like to request access to the data, please contact the named authors directly.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was supported by NHS Improvement.