
Abstract
A high-quality, sustained, health workforce contributes to a healthy population. However, a global reality is that rural health services, and the workforces that provide those services, are under unprecedented pressure. It is posited that improving a rural health practitioners’ capability could help to retain them working rurally for longer. Capability refers to skills and experience and the extent to which individuals can adapt to change, generate new knowledge and continue to improve their performance. With rapidly increasing access to, and use of, digital technology worldwide, there are new opportunities to build capability and leverage personal and professional support for those who are working rurally. In 2021, semi-structured interviews were conducted in rural Australia with thirteen General Practitioners and allied health professionals. Thematic analysis was adopted to analyse the data and map it to the Health Information Technology Acceptance Model. Whilst it could be assumed that low technology literacy would act as a barrier to the use of digital tools, the study demonstrated that this was not a significant impediment to participants’ willingness to adopt digital tools when social and professional networks weren't available face to face to address their capability challenges. The findings provide insight into the concept of health workforce capability and important considerations when designing capability support. This includes key features of health apps or digital tools to support the capability of the rural health workforce. Understanding the factors that make up a health professionals’ capability and the motivations or cues to act to build or maintain their capability may have a positive effect on their retention in a rural location.
Keywords
Introduction
Poor health outcomes in rural areas have been repeatedly and directly linked to poor access to, and retention of, appropriately skilled health services.1,2 The world rural population in 2020 was 3.4 billion, a 0.04% increase from 2019. 3 Around 7 million people—about 28% of the Australian population—live in rural and remote areas, which encompass diverse locations and communities. 4 The continuing maldistribution of the health workforce and primary care and tertiary health services in regional and rural Australia is well documented and this often compounds existing health inequalities between rural and urban areas.5,6 Despite efforts to address this disparity, it remains challenging to attract and retain health professionals motivated to work in rural locations in Australia and elsewhere.7,8
There is a significant amount of literature that suggests attraction, recruitment and retention of rural health professionals relies on factors other than clinical competence.9–11 Recent analyses posit that health professionals’ decisions to stay or leave a rural health position are complex and influenced by ‘a myriad of highly interactive dimensions within personal, organisational, social and spatial domains’. 12 In the literature, job satisfaction through having access to advanced work roles is strongly correlated with increased retention of rural health professionals. 13 Retention has also been found to be contingent on the extrinsic rewards provided by the employer (e.g. salary and work conditions) and the intrinsic rewards that come from within the individual, which are derived from the role and the work being performed (e.g. degree of autonomy and/or challenge). 14 For rural and remote allied health professionals, the most cited extrinsic factors to increase retention were professional development opportunities,15–17 reduced professional isolation and sufficient supervision,18,19 while the most cited intrinsic factors positively influencing retention were autonomy and community connectedness. 14 There is also a need to identify where improvements can be made to encourage an increased uptake in rural training, which is vital to addressing workforce maldistribution. 20
The literature indicates the solutions to address these challenges should be ‘bundled’ to ensure they closely target the combination of influential dimensions or factors.21,22 The NSW Rural Doctors Network (RDN), a 30-year-old independent, non-governmental organisation responsible for supporting the attraction, recruitment and retention of a primary health care workforce in figurerural NSW hypothesised that health workforce capability could be one of those influential factors. 23 Capability refers to skills and experience and takes into account factors such as values, commitment, creativity, intuition, integrity and other personal qualities, as well as context/environment. 24 It considers the extent to which individuals can adapt to change, generate new knowledge and continue to improve their performance. 25 The Capability Approach is an economic theory developed by Amartya Sen 26 that inspired the founding of the UN's Human Development Index (capturing capabilities in health, education and income). Sen proposed that metrics of wellbeing should focus directly on ‘what people can do or be’. 27 Sen's Capability Approach is being applied in different ways, and researchers have different interpretations of what it means to employ a capability perspective. Some researchers are applying the concept to the social and structural forces that contribute to convert individual capabilities into realised functioning's, 28 and the set of situations or conditions in the community and society that enable optimal health. 18 Likewise, in the rural health workforce context, while policies and programs to improve recruitment and retention often focus on the individual health professional (and their families), thinking about capability enables us to see the family, interpersonal, leadership and organisational environment as equally important to health workforce sustainability and quality of care in rural settings. 23 A focus on the social and structural elements of capability assists us to take a broader view of workforce performance in the rural setting. It encompasses the important factors and combinations of factors that facilitate functioning such as enjoying a rural lifestyle, finding work–life balance and engaging with community.
In Martiniuk et al., 23 RDN posit that helping to support a health professional be capable can help them to be adaptable, feel motivated and thus have resilience to stay through “tough times” which is necessary in a long career in rural health. Furthermore, if we can understand how to support health workforce capability, we may be able to improve the attraction, recruitment and retention of rural health professionals and in so doing enhance the sustainability of the rural health workforce. 23
In the last few years digital technologies have changed the health communication landscape with attention being paid to online tools for enhanced communication and consumer content. 29 This potentially enables rural health professionals to access support and training, where travel, cost and time barriers prevent or limit opportunities to gain support face to face.15,30 There has been an increase in health and fitness apps and research on their use in the areas of health promotion and disease management. 31 However, to our knowledge, there are no studies that have focused on the use of apps or digital tools by health practitioners where access to an app might increase their capability and positively impact on their retention.
Although this qualitative research on capability is exploratory in nature, having a systematic framework helps guide the qualitative exploration and identify critical aspects of the research. A limited number of theoretical frameworks have been developed to assess the acceptance of technology implementation in healthcare. The Health Belief Model (HBM) is one of the most widely used models for understanding health behaviours and identifying health beliefs. 32 The Health Belief Model (HBM) posits that messages will achieve optimal behaviour change if they successfully target perceived barriers, benefits, self-efficacy, and threats. 33 Key concepts of the model have been integrated with those from models of technology acceptance. 34 The Health Information Technology Acceptance Model (HITAM) (Figure 1) is an example of this integration and explains how factors (such as health status and beliefs, subjective norms, technology reliability and self-efficacy) influence interactions with health information technology, such as apps, to form behavioural intention in health consumers. 35 This framework considers behavioural beliefs, normative beliefs and efficacy belief, leading to the concepts of perceived threat, usefulness and ease of use respectively. Kim and Park, 35 note that the model needs to be further developed to describe consumers behaviour when using various health information technologies. The HITAM framework has been adapted in a qualitative study relating to mobile phone applications in the self-management of Type 2 Diabetes Mellitus in rural Australia, 36 and a study that examined the willingness to use telemonitoring interventions in patients with type 2 diabetes and/or hypertension in the public primary healthcare setting in north-eastern Singapore. 37 Application of such a model to the concept of capability may enhance understanding of how interactions with information technology could similarly form behavioural intentions around capability in rural health workforce. Where health practitioners have limited professional support, access to apps that make them feel more capable in health behaviour or decision-making in rural practice may be extremely beneficial. Therefore, the current research attempts to systematically identify and classify health professionals’ views about important capability factors, the cues to action to build or maintain capability and benefits and barriers to using health apps or digital tools framed around the HITAM. Elements of the Framework have been adapted to reflect the findings of this study.

The health information technology acceptance model (HITAM).
Methods
Data collection
Participants were recruited either via the telephone, in person or through the Rural Health Pro newsletter in April 2021. Rural Health Pro is a popular digital platform that connects health professionals and organisations interested in rural health. Participants who saw the invitation in the newsletter contacted researchers to express interest in taking part in the study. A plain language statement and consent form were emailed to participants and on return of written consent, an interview time was established. All interviews were conducted by RR and SP by telephone in May 2021.
Participants
Thirteen rural health professionals (4 males, 9 females) responded to the invitation to participate in the study. They included 4 General Practitioners, a pain specialist, three nurses, two occupational therapists, a speech pathologist and a physiotherapist, with an age range of 39 to 65 years, and an average age of 51 years.
Interview guide
The interview guide was adapted from Anderson et al., 38 and Jeffrey et al. 36 (See Table 1). Further, definitions of persuasion strategies used in digital apps acted as prompts in the interview and were drawn from. 39 Additional questions were added to explore factors related to health workforce capability and another inquired: “What features would you want in an app to make it useful for you”. 40 Asking this question allowed the authors to gain more comprehensive insight into the features of a useful health workforce capability app as one option for providing support to rural health professionals. Interviews lasted between 30 min and two hours. Two participants requested a second interview because they had a lot to contribute.
Sample interview questions.

Ethics
Ethics approval to conduct the feasibility study was received from the Northern NSW Local Health District Human Research Ethics Committee (2020/ETH03020).
Data analysis
Firstly, the verbatim transcripts were coded manually using inductive thematic analysis. The first two recordings were coded separately by two authors (KP and RR). The remaining eleven interviews were coded primarily by authors KP and SP, but each of the authors were involved in coding transcripts. RR and AT meticulously verified the analysis by the other two researchers to ensure completeness.
Secondly, data were then analysed using deductive content analysis following Elo and Kyngas. 41 The authors of this paper tested the Health Information Technology Acceptance Model (HITAM). An initial structured analysis matrix was developed based on a modified version HITAM. The team came together to compare their codes and revise the codes in an iterative fashion to develop a set of themes that captured the essence of the interviews. Finally, the raw data were compared with the emerging theme labels and definitions, and further refined by merging, adding, and removing redundant themes. Subsequently, a number of more nuanced sub-categories were added into the initial matrix, to reflect the different factors associated with health workforce capability. The names of some codes were refined to better reflect the categories resulting in a final framework that underwent multiple iterations.
Results
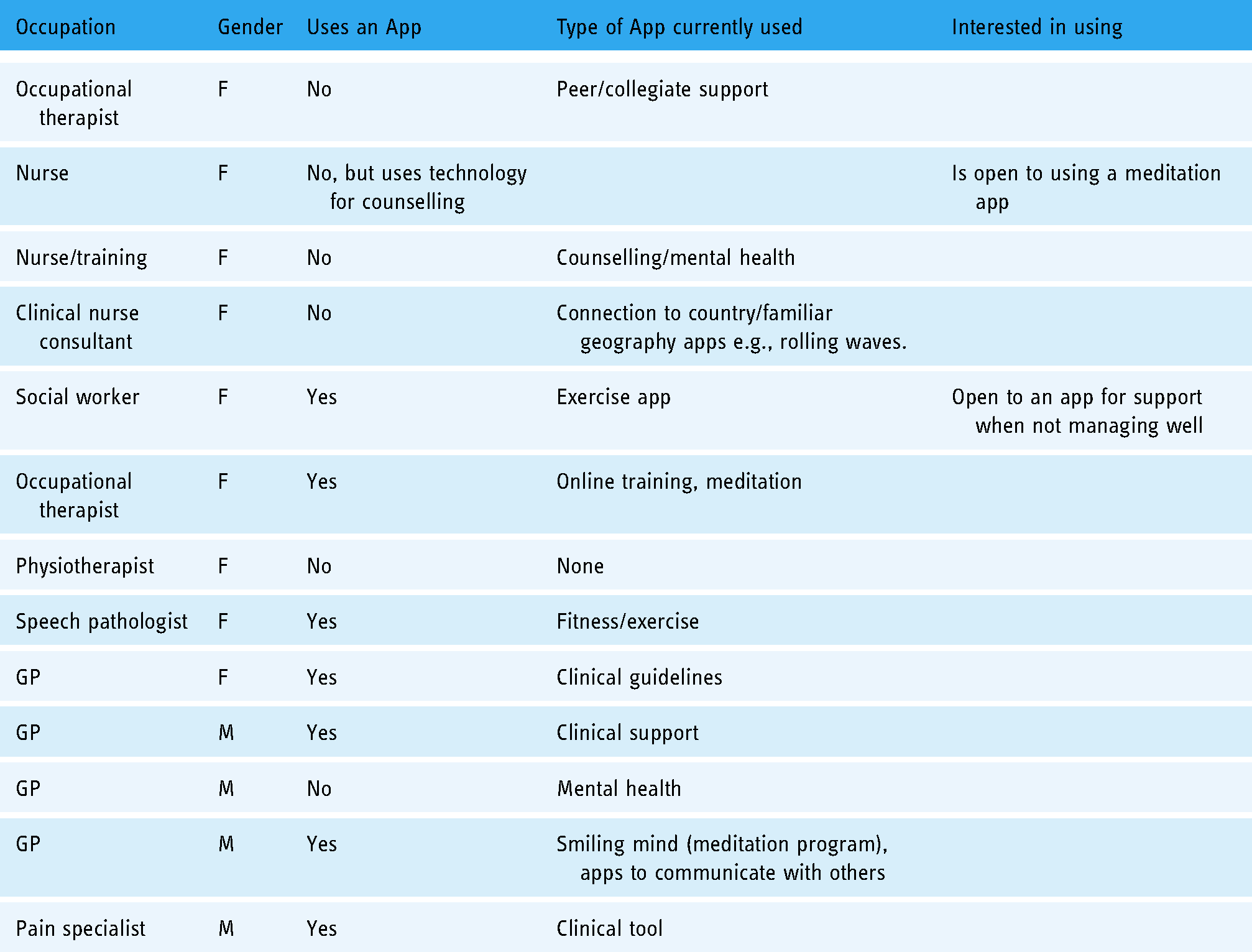
Of the thirteen participants, seven currently use apps. The type of apps used varied and included clinical support, health and fitness, meditation and communication apps. All but one participant was aware of some apps and had ideas about what apps or features would be useful. The following table describes the participants and summarises the findings in relation to the use of apps (Table 2).
Participants and app use.
Framework for building health workforce capability through using digital technology
The analysis supported the general applicability of the HITAM model in understanding capability amongst rural health professionals. Some of the elements of the original model were strongly represented in the data, particularly the broad areas signified by the three domains. However, in order to provide a more comprehensive reflection on the factors and dynamics that underpin a rural health professionals capability, the authors were required to create additional categories. These refinements to the original model enabled the authors to start to understand the key elements of capability in the rural health workforce context, in particular the specific personal and work-related factors that impact on capability.
The final matrix reflecting factors influencing capability and beliefs that impact on taking action about capability are summarised in Figure 2 which the authors have titled a ‘Framework for Building Health Workforce Capability using Digital Technology’ (the Framework). The Framework was broadly organised into three domains: Factors affecting capability, Modifying Factors and Likelihood of action. Nine main themes and 16 sub-categories are arranged within the three domains. The results section describes these themes and sub-categories with illustrative quotations.
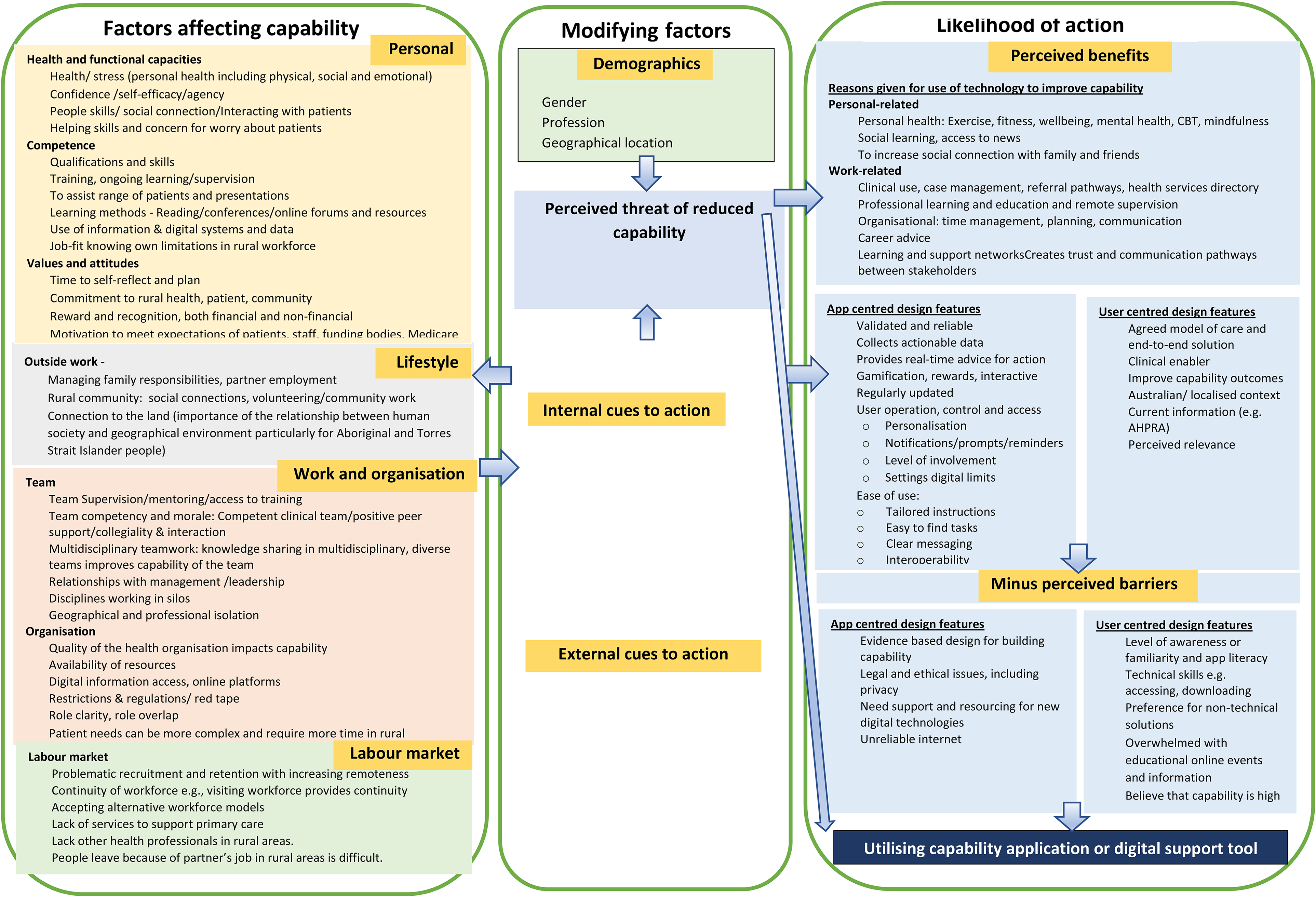
Framework for building health workforce capability using digital technology.
Domain 1: factors affecting capability
Within the three domains, nine key themes and sixteen sub-categories emerged from the deductive analysis using the HITAM model. In the first domain of the Framework, we consider the factors rural health practitioners identified as important to their capability. The most important aspects influencing capability fell into four major themes namely Personal, Lifestyle, Work and Organisation, and Labour Market. Each of the four themes were broken down into further sub-categories.
Theme: personal factors
Within this study the Personal factors that impacted on a participants capability included health and functional capacities, the degree of competence and their values and attitudes. Essential health and functional qualities identified were their personal health including mental health, their agency or self-efficacy, confidence, helping skills and concern for patients. Participant's exploration of their personal qualities was focused on how these impacted on their professional life, indicating the two are dynamically connected. As one GP relayed: So, capability in a particular practice sense, is having the capacity and the confidence and perhaps the compassion to work in an unsupported situation in general practice, which is a very broad-base science. And that can be a difficulty because keeping up to date, in this very broad basis, general practice, can be quite hard. (Interview 13, GP)
Personal health, encompassed physical, social and emotional health and was deemed to be important. In relation to this view of personal health, one participant noted: Because, if we aren't healthy spiritually, and social and emotionally, how are we going to help people here? How am I going to help the people here if I’m struggling? (Interview 3, nurse)
Of particular note was that seven out of 13 participants referred to their confidence, describing either feeling confident or lacking in confidence. Being confident was seen to be central to feeling capable in an isolated rural health position: I’ve also been encouraged by some recent training I’ve done which has helped my confidence. I see that I’ve actually got quite a lot of capability in my role, and I’ve been able to meet the challenges that I’ve been presented with which are many and varied each day. (Interview 9, physio)
This study found that self-efficacy reflects confidence in a health professionals’ ability to exert control over their own motivation, actions and social environment. Therefore, participants capability was impacted on by their self-efficacy. Confident health professionals felt they had more control over their ability to manage a situation and this enhanced their beliefs about their capability: …once you’ve done your three years of perseverance and being patient in building up your confidence and competencies, you realise that, “Wow, I can just pull my hand to anything, plus I get a rural lifestyle”, which is, personally, phenomenally better than you could ever get in – well, again, that's my personal experience – a metropolitan area (Interview 17, occupational therapist).
Confidence was also said to underpin the second personal factor in the framework, a health professionals’ competence. A health professionals’ competence was largely impacted on by their qualifications and existing skills, their ability to access training, ongoing professional learning and supervision to build further knowledge and skills, access to information and technology, their adaptability, and suitability for their role. Remoteness continued to provide challenges with access to training and supervision. So, you know, you need to be able to adapt to whatever comes through the door. But it's hard to maintain that skill and knowledge across a broad range. (Interview 16, nurse, training)
Participant's confidence was also linked with their values and attitudes which centred around their commitment to rural health, caring for their clients and making a difference to the health outcomes of members of their community. As one pain specialist commented: Well, I think it's sort of a confidence within yourself that I can help people. Then you’re feeling like you’re making a difference personally. So that sense of ability and confidence to help people and feel that what you do is right. So, I think that's important. (Interview 7, pain specialist)
One health professional kept her promise to return to her community out of concern for her patients and because it enriched her professional and personal life: And I promised the people of [place name] that I would be back one day, and I came back five years ago, just in time for my best friend, [name of patient], one of my best friends. She was 80. Every time I’d sit next to her, she’d hold my hand. And when she held my hand, all this stuff run through my body, this goodness, and it made me feel so loved and cared for. (Interview 3, nurse)
Reward and recognition were mentioned three times, in relation to the fact that capability isn't recognised by appropriate grading or renumeration: But from an award perspective, it's not reflective of what I’ve been asked to do. I’m still a level 2, which is just your stock standard new grad level, and that job description doesn't actually reflect what the demands are on me now as a senior therapist But there's no opportunity for personal re-grade. There's no acknowledgement of that, basically. (Interview 17, occupational therapist)
Theme: lifestyle factors
The second tier of the factors affecting capability related to lifestyle outside of work. These factors included managing family responsibilities, the nature of the rural community, connection to the land and partner employment. However, most comments received were in relation to community. Often health professionals are recognised members of the community which was generally found to have a positive impact on their work capability, with intrinsic reward. But when you go into a rural community, their sense of belonging is phenomenally better than you would ever experience in a metropolitan. Just looking after you, looking out for you. People knowing who you are. (Interview 17, occupational therapist)
The rural community in which the health professionals lived had a direct impact on their capability as indicted by a nurse, “But there's times there – And this community is really so resilient, like they’re a lot like me. That's probably why I fit in here”. The sense of place and belonging to a community appeared to encourage health professionals to remain for longer, despite some of their challenges. No one suggested close ties with community had a negative impact due to a lack of anonymity or high expectations.
Finally, the nature of the community itself can influence the type of work a health professional undertakes. As one occupational therapist indicated: And that's what's happened with this hand therapy, as in I’ve seen a need, the community has embraced the need. The doctors from metropolitan areas and surrounds have also been very happy because of course it's increasing referrals. (Interview 17, occupational therapist)
Theme: work and organisation
The Work and organisation level capability factors included work factors such as personal isolation and team work as well as organisational level factors such as the availability of resources to support education, training and supervision, clarity of roles and access to technology and digital information. Eight of the thirteen interviews referred to professional isolation. This was largely due to the fact that they worked in a solo or small health service or practice without professional peers, or the relationship with the appropriate professionals was not deemed to be functional: I went and sought out networks, and I found that really reassuring, to be able to just talk through the struggles that I was facing and knowing that I wasn't alone in that position. (Interview 17, occupational therapist)
Most health professionals discussed the need to have access to peer support. This was said to help them feel less isolated in dealing with the challenges of practicing rurally. But having somebody that can listen I think, and be able to just respond, I think, in an understanding way. And maybe have some ideas of putting something in place, or something to do. (Interview 5, social worker)
One interviewee referred specifically to the importance of having a work team for building their capability: I was just thinking about the value of having a team around you and that team can sometimes make up very different types of professions…. it's about tapping into all the other team members for support and capability building. I know that I’ve benefited heaps from that over the years working in rural, and I’ve learnt so much just from other professionals in terms of growing my patient care abilities as well (Interview 9, physiotherapist).
Not having access to a person to provide clinical leadership through supervision or management to debrief with was also an important barrier to working rurally. Having a supervisor or key contact with whom to share work challenges played an important role in individuals’ capability. Two interviewees noted that deficits in leadership led to unhealthy workplace culture and missed opportunities for training. The dearth of good supervision was partly related to a lack of renumeration for undertaking the role: I think having an outlet to be able to debrief. I found it very, very hard getting a supervisor to do supervision, out here. I’m a level three. Also, our practitioners here –our social workers are level three, which means you’ve got to have somebody at a higher grade. There are apparently only two-level fours within our total area, which means you’ve got to source somebody external, and that's been a real issue for me as well. So, supervision, or some form of being able to debrief and do that regularly is a big one. (Interview 5, social worker)
Training was considered to be very important in building capability. Having access to digital technology has improved rural health professional's access to education and training. It also reduced the time spent in travelling to large regional or metropolitan areas to access training. Most participants who used appsthat support capability development stated that what they liked most was their ability to provide information, which they would not access otherwise. Some of the information they referred to was provided directly by the app such as clinical information and some of the information was generated by other users and shared on the app. I think it will be ensuring proper training in that area. Yes. So, that would include training, perhaps updating training in counselling and also in chronic disease management. (Interview 13, GP)
Five participants identified issues around lack of organisational resources to support their capability. This included staff resources and convenient access to technology and technical support when needed. I think having the appropriate or enough resources. And that's dependent obviously on other services a lot of the time, because we are limited out here (Interview 5, social workers)
Theme: labour market
The final section of the first domain relates to the labour market. The study identified a number of labour market or system issues that impacted on a rural health professionals’ capability. It includes factors such as increased difficulty in recruiting GPs, allied health professionals and specialities as the degree of remoteness increased, the lack of continuity of the workforce and the lack of alternative models to help address the workforce challenges. …. there's a big problem, trying to attract people to work in rural and remote areas (Interview 7, pain specialist)
Continuity of workforce and the lack of options to replace people were of concern and impacted on health professionals’ sense of capability: ….at the moment, our allied health and nursing vacant positions, are huge and difficult, which means that we have to carry more roles. We lost our palliative care nurse a few months ago, and we lost a wound care nurse and we lost our several other nurses all at the site all within a month. (Interview 18, nurse)
Domain 2: modifying factors
The second domain of the Framework explores internal and external cues to action. A number of internal cues to action make up capability including perceived capability, motivation, low morale, technical competence and resources. Cues to action are motivating factors or stimulus that trigger the decision to take action to support or build one's capability. These can be internal motivations such as feeling depressed or having low morale or external motivations such as availability of counselling support. The internal cues or motivations were most likely to create action to support their capability using technology as stated by one GP, “I feel that at the moment, I could do with a bit of help in motivation.”
Participants were most concerned about professional isolation and three participants identified technology as a way of accessing support to build capability: I’m thinking probably through a mobile phone app, because I’m thinking of some younger clinicians that are working in really remote places that I’m conscious we will want to be looking out for but I’m not able to track them daily. I think of that generation where the mobile phone is probably very much a part of their lives. (Interview 9, Physiotherapist)
This was most likely to occur when they felt their capability was low. This motivated them to take action. Some participants identified low morale signalled the need to take action to address this: And I don't think I’ve ever suffered from depression, and I’d hate to, because I know on some of my down days, it's pretty crappy, so I’d hate to have depression. But I think, just acknowledging how things are a bit tough, or what can we do here? How can we make you feel better or get you out of this slump? (Interview 5, social worker)
The issue of technology literacy and how a person learns best could impact on whether they use technology to access support. For some participants simplicity and convenience was central to use. The availability of technical support or the time and opportunities to learn the skills needed to utilise technology had a direct impact on technology use. So, resources is a really, really big one. I’m not very tech lit, and I struggle with how I learn, how I take information is having somebody sitting with me and physically doing it. (Interview 5, social worker)
Geographical and professional isolation in rural areas restricts mentoring, networks, and collaborations; access to infrastructure; training; and mentors and these can be calls to take action to access support via digital means. There are aspects where I’m miserably lacking capability, which are usually about internet teaching and Zoom teaching and all of that kind of thing. (Interview 13, GP)
The need for mental health support was a motivating factor that could influence a health professional to take action. The availability of counselling was the most commonly named external cue to action. One participant indicated that an app that could gauge your mood would motivate them to act to build capability: And I think around the mental health stuff, or if you’re talking about something that's going to – where someone's going to pick up and gauge, you know that they’re not happy, well to me, it's that's really useful. (Interview 5, social worker)
Domain 3: likelihood of action to use a capability application or digital support tool
The third domain of the Framework relates specifically to technology use and represents the benefits and barriers of using a health app or digital solution to build health professionals capability.
Theme: perceived benefits of using technology to improve capability
The additional benefits of using a mobile app or digital tool for capability identified in this study were important factors in acceptance. Perceived benefits of using relevant apps were divided between person-related elements, work-related elements and design features. Person-related elements included improvements in personal health such as mental health, wellbeing, mindfulness and fitness; for social learning or to increase social connection with family or friends; to enhance clinical practice; to document health services and referral pathways; and, to improve access to education, training and supervision. Increased social connection to address mental health and wellbeing was the most commonly cited benefit of using apps for rural health professionals: And in my experience, across the board, one of the biggest things seems to be the psychosocial aspects such as depression, anxiety, stress and poor management of those things. I see so many people who’ve got severe depression and it hasn't been touched. Or if it has been touched, a psychologist has just seen them every now and then and thinking they’re doing fine. (Interview 7, pain specialist)
Work-related reasons for using an app or digital tools to build capability included for clinical use and professional learning, education and remote supervision. In relation to clinical use health professionals stated digital technology enabled them to read, listen or watch content that was useful to their jobs. The [name of app] is pretty good, because that gives you the clinical aspect but it also gives you referral pathways, and I think those are really good. (Interview 13, GP)
In addition, it enabled them to get information at the time it is needed allowing them to answer client's questions. So, it's the same idea, use that technology to fast access to many services, specialists’ opinion, registrars’ opinion, don't need to wait for hours or whatever to get an opinion or to help that person out. We might be able to be protecting them immediately, or at least they can get access to our data or the patient records immediately and they can have a quicker view of that and they will support us, help us with the decision sometimes. Because it's a life, we are not talking about a car or a building or something, it's a life of a person. (Interview 2, GP).
The most notable beneficial features of the design were comprised of app and user-related factors. The app centred design features included the ability to track the user's activity. Most participants liked having the tracking feature in their apps because this type of self-monitoring increases their awareness. Another common feature, liked by most participants, was the reminder. Reminders were found to be particularly useful for busy individuals. Somewhat related was that they appreciated getting real time advice for action and then feedback on their goals. Many users mentioned that having personalised information and services would also support long-term engagement. They could be tailored to each specific user, thus eliminating the cognitive burden of dealing with information overload. Ease of use includes some of the features like automation, clear messages and tailored instructions. …maybe an application, just let's say about something to organise your time more. I’m not sure what exactly, but let's say roughly I’m thinking of when you plan for a break for yourself, like four weeks or six weeks or eight weeks, how to plan that. How to organise your patients, or maybe add - without the names, add the cases, the important cases you need to follow up and chase, whether you need to leave them for a week or two when you have this holiday. (Interview 17, occupational therapist)
In relation to capability, one respondent suggested that some capability coaching would be a good purpose for an app or digital tool. …. if you could put a link to something that you could go - say for example, “You’re more capable when you’re relaxed. Here's a two-minute relaxation period,” whatever it is. Use two minutes of a relaxation tape. (Interview 16, nurse).
Theme: perceived barriers to using technology to improve capability
The third domain of the Framework also explored barriers to use of health apps or digital supports in two categories: app-centred design and user-centred design. There were few app-centred barriers noted. One health professional indicated they weren't aware of any evidence-based capability apps and would consider their credibility before using them. Another focussed on internet issues that impacted on access. … I have increased speed and access, because the internet connection makes it really frustrating and it drops out in some rural areas, even regional sometimes. (Interview 9, occupational therapist)
Legal and ethical issues were noted by three participants, but these were mainly focussed on the question of liability associated with recommending the use of apps to clients. Ultimately, it was perceived that patient privacy could be upheld, that the benefits outweigh the costs, or that opt-out options could be used. And I don't think for people's health care it should be an issue, really. If they don't want to that's their prerogative. But I think most people would, wouldn't they, if they see value in it? They say, “Yeah, if it gets me better.” Most people want to be better, don't they? (Interview 7, pain specialist)
Perceptions of privacy associated with digital solutions was also noted, with a recognition that concerns about the level of privacy offered could be a barrier to App use. However, most stated they felt comfortable sharing with small groups in order to access the support they needed: As long as there's a privacy umbrella over it, that's acceptable. (Interview 7, pain specialist)
The notion that it is too late to do anything about the privacy concerns resulting from a lack of boundaries when it comes to digital technology was raised: But we’re just so enmeshed in it that it's like it's too late. So I feel like what's the point of worrying about it, it's just another thing to worry about. (Interview 6, occupational therapist)
There was also concern about needing to use a health professional's personal digital technology in the work context and the patient privacy concerns this raised. I use it [personal phone] to show and demonstrate stuff to patients. I use it to take photos. But the thing that I don't like is, firstly, it's my personal phone. If this technology is something that the healthcare system really wants to introduce, they really need to actually, again, set up systems that have it more in the work realms rather than the personal realms. (Interview 17, occupational therapist)
This highlights the issue raised about the need for adequate support and resourcing of digital technologies in the workplace. It was perceived health professionals may take the initiative, or seek to, utilise digital technologies to support capability but that there is a lack of organisational resourcing and support for this. There's been a lot of initiative from other clinicians in my region who have wanted to use telehealth or technology for training and also professional support in regard to home visits, so things outside of the hospital environment when you’re geographically isolated. But, again, as I’ve mentioned before, that was clinician-driven and dependent. It wasn't supported or funded by management, and it hasn't gone anywhere. (Interview 17, occupational therapist)
Digital capability support was noted to also be impaired at times by unreliable internet connectivity. This was noted by three participants: No, I don't tend to use mobile phone because it's unreliable usually. I find if I’m travelling particularly, I haven't always got network connection. (Interview 9, Physiotherapist)
Most of the user-centred barriers included low awareness and a lack of app literacy. Lack of app literacy centred on a lack of familiarity or awareness of apps often bought about by not enough time to search for them, which meant participants weren't sure which ones were available or appropriate and how to use them. I think just a familiarity with them and know which ones are really useful. I think it would be a useful exercise, if somebody worked out which were the best ones for GPs in a working situation. (Interview 13, GP)
This sometimes led to a preference for non-technical solutions. However, a number of participants felt that there is an overwhelming amount of information and educational events online and they were unable to choose which was most suitable and reliable. This suggests participants were looking for ways to manage information and that a one stop amount of shop or trusted source of information would be beneficial.
Discussion
Our findings are significant in identifying specific capability factors valued by rural health professionals and how to build capability for rural retention, which have previously not been investigated.
Kim and Park, 35 suggest theories and models help explain consumers’ health behaviour and guide the development of more effective ways to influence and change their behaviour. Our results demonstrate that a modified HITAM framework incorporating the HBM and additional sub-categories can be utilised to identify the factors affecting rural health workforce capability, the modifying cues to action to build and maintain capability, and the benefits and barriers to using apps or digital. This in turn informs the design of programs to achieve positive changes in health behaviour. In building on the HITAM model, the authors found that the additional sub-categories were required to fully explain important capability factors, identify the motivating factors and understand the role of technology in supporting a rural health professionals’ capability. We discuss three domains and nine themes related to rural health capability and capability support: factors affecting capability (Personal, Lifestyle, Work and organisation and Labour market factors); modifying factors (demographics, internal and external cues to action); and the likelihood of action to address capability issues using digital technology (perceived benefits and perceived barriers).
The most influential factors impacting on health workforce capability in the first domain of the Framework included physical and mental health, confidence and competence, self-efficacy, connection to community, connection to peers and education and training. Further, we identified the linkage between geographic isolation and personal, lifestyle, professional and health system interfaces. In particular, for our participants, engagement with peers and their rural locale shaped their professional identity and personal and professional satisfaction. We know from previous literature that community connectedness has a positive impact on retention.14,17,42 The importance of connection to others to build capability is also consistent with the findings of Harandi et al., 43 who noted that availability of social support bolstered participants ability to cope with challenges, providing an avenue for emotional expression and building or retaining their capability. 29
Our participants often did not have access to face-to-face education, training and continuing professional development and this was identified as a major factor impacting on their capability. This is significant because the most cited factors that negatively influence health professional's retention in rural and remote areas include lack of access to professional development, feelings of professional isolation and psychosocial and personal factors.9,15,18,23,44 A lack of access to a social or professional network face-to-face led most of our participants to consider a technology solution. With rapidly increasing access to, and use of, digital technology worldwide, there are new opportunities to leverage training and support for those who are working in rural and remote areas.30,45,46 Further, the online environment has become more multidirectional in its communication characterised by participation, collaboration and openness 47 and allows health practitioners to create health-focused groups to communicate with peers.48,49
The most important cues to action were found to be internal cues including isolation, perceived level of self-efficacy, and capability, motivation and technical literacy or technical competence. Like Bandura 50 this study found that self-efficacy reflects confidence in the ability to exert control over one's own motivation, behaviour, and social environment. Expanding on Bandura's self-efficacy concept to explore capability, this study found that where internal cues to action were strong and local options to attend to these cues were absent, participants tended to consider apps or digital tools to support their capability. Previous research by Jeffrey et al., 36 found that those with good technological literacy were more likely to consider and continue using apps. In our study, it was also those whose circumstances prevented them from accessing support face-to-face.
The last domain identifies a number of reasons why rural health professionals use digital technology to improve their capability, confirming that rural health workforce capability is a complex and multifactorial concept. The most commonly cited personal benefit from using a digital tool or app was increased access to support or social connection to address one's mental health and wellbeing. The most commonly cited work-related benefits of using digital tools or apps for rural health professionals were clinical support and professional learning, education and supervision. Both personal and work-related perceptions of benefits as well as the features of the apps and characteristics of the user, are important factors in the use of technology to build capability. Like previous research into the use of online tools and health apps for improving health behaviour, the authors of this study also found that perceived usefulness of, and positive interaction with, technology may ultimately increase behavioural intention.31,35,36 By identifying the core benefits and the app-centred design and user-centred factors as listed in the Framework, it is possible to design a digital solution that resonates with health professionals and in doing so address their various capability needs.
The most notable barrier to app use was a general lack of familiarity with specific apps as healthcare tools to support capability. Participants were also unaware of the evidence to support the efficacy of apps in maintaining or building their capability. Previous research identified perceived barriers as a significant predictor of behaviour.35,51 A qualitative study of user perceptions of mobile health apps by Peng et al., 31 p 8 found ‘low app awareness and low app literacy are two factors leading to non-adoption’. The present study is consistent with this finding in terms of identifying technological literacy as a barrier, but the perceived barriers did not appear to have as great an impact on intention to use apps or digital tools. This may be because in the rural health workforce context there are other factors at play (e.g. isolation) and fewer options, which increase motivation to use a digital solution to support their capability. Further, we propose that individuals with other personal qualities such as a high level of competence may not see the barriers as insurmountable. Significantly, no participants were averse to the idea of using apps. Given that the challenges of retaining health professionals rurally persist,2,8 additional insights into addressing these barriers are important. Digital tools can play a particularly valuable role where traditional face-to-face modes of providing capability support are not available to rural health professionals.
Our research aimed to develop a robust foundation for future rural health capability research and to link this with our deepening understanding of technological solutions. This was achieved through the further development of the HITAM model. The Framework produced as part of this work possesses real-life applicability that can be further trialled in the sector and may serve to guide health workforce planners, human resource professionals, policy makers, and app designers in developing technical solutions. Our findings indicate that a one-size-fits all approach is unlikely to satisfy all needs and wants of users, which emphasises the need to consider individual lifestyles and preferences when designing digital interventions. Expanding our knowledge of important capabilities, the factors that build health workforce capability, the motivations to act to improve capability and the strategies relevant to the development of apps or digital tools presents. This is key, given the suggestion that retaining the expertise of health professionals with rural experience helps achieve better quality and more efficient health care delivery. 52 Whilst several studies have been conducted to investigate retention factors in rural Australia,2,10,11,17 the concept of health workforce capability has only recently emerged as a rural retention strategy, 23 RDN proposed that supporting the capability of the rural health workforce is important for improving the attraction, retention and sustainability of rural health services. 23 Because the rural workforce is often subject to heavy demands and stretched to the extremes of their capability, understanding and enhancing rural health professionals’ approach to personal and professional capability is paramount to improving the resilience and thus retention of the rural workforce.
Strengths, limitations and further research
A strength of the study is that it is the first qualitative study to report the attitudes and experiences of health professionals working in rural Australia regarding the use of apps or digital tools to improve capability. We purposively selected a wide range of health professionals because it is important that the model applies across rural health professionals given that rural health care relies increasingly on interprofessional collaboration, teamwork and education to deliver high quality patient care. However, we need to be cognisant of some limitations. Firstly, while we have identified a range of Work and organisational factors that were found to impact on health workforce capability, organisational factors may differ according to the resources, structure, work culture, policy etc. of the particular organisation.
The recruitment process for this study was largely implemented through Rural Health Pro. This may have resulted in a bias of self-selecting, technology literate health professionals. Although there was representation from the major groups of health professionals, the group size of each professional group was small and also unequal. Thus, further studies need to be carried out to determine if there are differences across gender and health profession.
There are a number of items we did not explore but could be considered for future research. The study explored relative contributions of each of the Framework success factors and barriers. However, with small numbers further study would be needed to delineate the relative contributions of Framework factors. Further study would also be needed to examine the applicability and success of the Framework itself or could focus on the users of apps that support capability development and any changes in user experience.
Conclusion
Some found it difficult to address the barriers of geographic isolation and lack of resources to live and work rurally and to perform to their best in situ. This is the first study that has explored the HITAM models in relation to maintaining or building capability. In our study we tested whether the Framework for Building Health Workforce Capability using digital technology we developed based on this model lent itself to exploring factors which influence rural health professional's capability. It was found that personal health and wellbeing, clinical confidence and competence, ongoing education and training, values and beliefs, extended social networks, commitment to and connection with community were important aspects of capability that did not form part of the original models or developments made through other studies that related to the use of health apps. Rural health professionals were encouraged to consider the possibility of technology as an anchor to build capability. A notable conclusion is the importance of rural health professionals being aware of the potential of apps as a self-management tool when their rural circumstances prevent other forms of support. Understanding the factors that make up a health professionals’ capability and the motivations or cues to act to build or maintain their capability through using digital tools may have a positive effect on their retention in a rural location. As such these findings may guide health workforce planners, HR professionals, policy makers, and app designers in developing technical solutions.
Recommendations
That a digital or technology solution to help rural health professionals build or maintain their capability should:
Apply the Framework for improving Health Workforce Capability through using digital technologies when developing new applications or considering areas to provide support to rural health workforce. Provide professional support to overcome a sense of isolation. Build skills to maintain clinical competence and facilitate access to education and training. Incorporate app centred and user centred features in the design of the digital app or platform such as alerts and customisation. Be user friendly and accessible Enable learning from other users’ experiences through the creation of a team or community of practice to work on a shared capability building activity. Protect user privacy
Footnotes
Contributorship
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
Ethics approval to conduct the feasibility study was received from the Northern NSW Local Health District Human Research Ethics Committee (2020/ETH03020).
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Guarantor
RR