
Abstract
Following a decade of dissemination, particularly within the British National Health Service, electronic rostering systems were recently endorsed within the Carter Review. However, electronic rostering necessitates the formal codification of the roster process. This research investigates that codification through the lens of the ‘Roster Policy’, a formal document specifying the rules and procedures used to prepare staff rosters. This study is based upon analysis of 27 publicly available policies, each approved within a 4-year period from January 2010 to July 2014. This research finds that, at an executive level, codified knowledge is used as a proxy for the common language and experience otherwise acquired on a ward through everyday interaction, while at ward level, the nurse rostering problem continues to resist all efforts at simplification. Ultimately, it is imperative that executives recognise that electronic rostering is not a silver bullet and that information from such systems requires careful interpretation and circumspection.
Introduction
A key finding of the recent Carter Review 1 recommends that all UK National Health Service (NHS) trusts adopt electronic rostering (e-rostering) by October 2018. Despite a decade of growth of e-rostering implementations, 2 Carter criticises their use as ‘immature’ and notes that ‘few trusts are using its full functionality and benefiting fully from what it can do’ (p. 23). Subsequently, NHS Improvement has published ‘Good Practice Guide: Rostering’ 3 in order to systemise the roster process, principally in the form of the roster policy. The term ‘roster policy’ refers to a formal document that codifies which rules and procedures are to be used when preparing staff rosters. 4 From an optimisation perspective, the roster policy specifies which constraints are regarded as ‘hard’, which are ‘soft’ and how these constraints are to be applied. 5 As a public sector body, many NHS trusts have made their roster policies freely available online. This research uses 46 policies to examine the implications of codifying the roster process.
Background
Nurse rostering is a complex task with consequences for patient care, staff work/life balance and hospital budgets. Notwithstanding this importance, rostering has received limited attention within the healthcare management literature 6 although Operational Management (OM) research has a long history of modelling algorithms for nurse scheduling. 7 However, despite four decades of research, a single solution to the ‘Nurse Rostering Problem’ (NRP) has yet to emerge. 8 Consequently, the explicit codification of the roster process, as outlined in a roster policy, offers a unique opportunity for OM and healthcare management researchers to span this research gap.
The last decade has seen significant growth in the number of commercial e-rostering systems being deployed. 9 Today, e-rostering is increasingly regarded as the solution to producing cost-effective, safe, equitable work schedules.1,10–12 Traditionally, new Ward Managers have learned their manual rostering skills from an experienced Ward Manager 6 via the transfer of tacit-to-tacit knowledge or ‘socialization’. 13 Tacit knowledge is difficult to formalise, highly contextual and dependent upon the mental models, beliefs and perspectives of both individuals. This ‘personal’ knowledge, 14 while rich in content, is limited in value beyond a small team of individuals and can rarely be utilised by a hospital as a whole. 15 Consequently, e-rostering requires the codification of the roster process3,16 and hence the transformation of tacit-to-explicit knowledge. 13
Codification is a measure of the ease with which an element of know-how can be unambiguously allocated to agreed perceptual or conceptual categories. 16 Processes and procedures lend themselves more readily to codification than attitudes, skills and competencies which incur a higher cost of codification, and inevitably, the economics of codification often define what is considered codifiable. 17 Powerful stakeholders may define what is codified, sometimes to the detriment of other, less powerful, stakeholders. Thus, by enabling know-how to be utilised beyond a small team, 16 codification may also modify the balance of power between the stakeholders.17,18 For example, codification of the tacit knowledge required to roster a particular ward may shift power away from Ward Manager, possibly resulting in resistance to e-rostering systems. 5 Moreover, codification may render senior executives oblivious to the tacit knowledge required to craft a ‘fair’ roster, resulting in the e-rostering system being used, primarily as a governance tool aligned to management objectives. 19
The study
Aims
The complexity associated with workforce rostering is determined by the type and scope of constraints. Historically, these constraints were implicit and unstated. However, codification, in the form of a roster policy, is a prerequisite of all e-rostering systems. The aim of this research is to compare a sample of roster policies to examine the implications of the codification process for rostering practice.
Design
This research employs qualitative thematic content analysis. 20 This method is often used ‘to answer questions such as what, why and how, and the common patterns in the data are searched for’ using a coherent set of codes to manage text with similar content (p. 138). 21 In this manner, meaning is created by developing summary themes from complex raw data. 22
Data collection
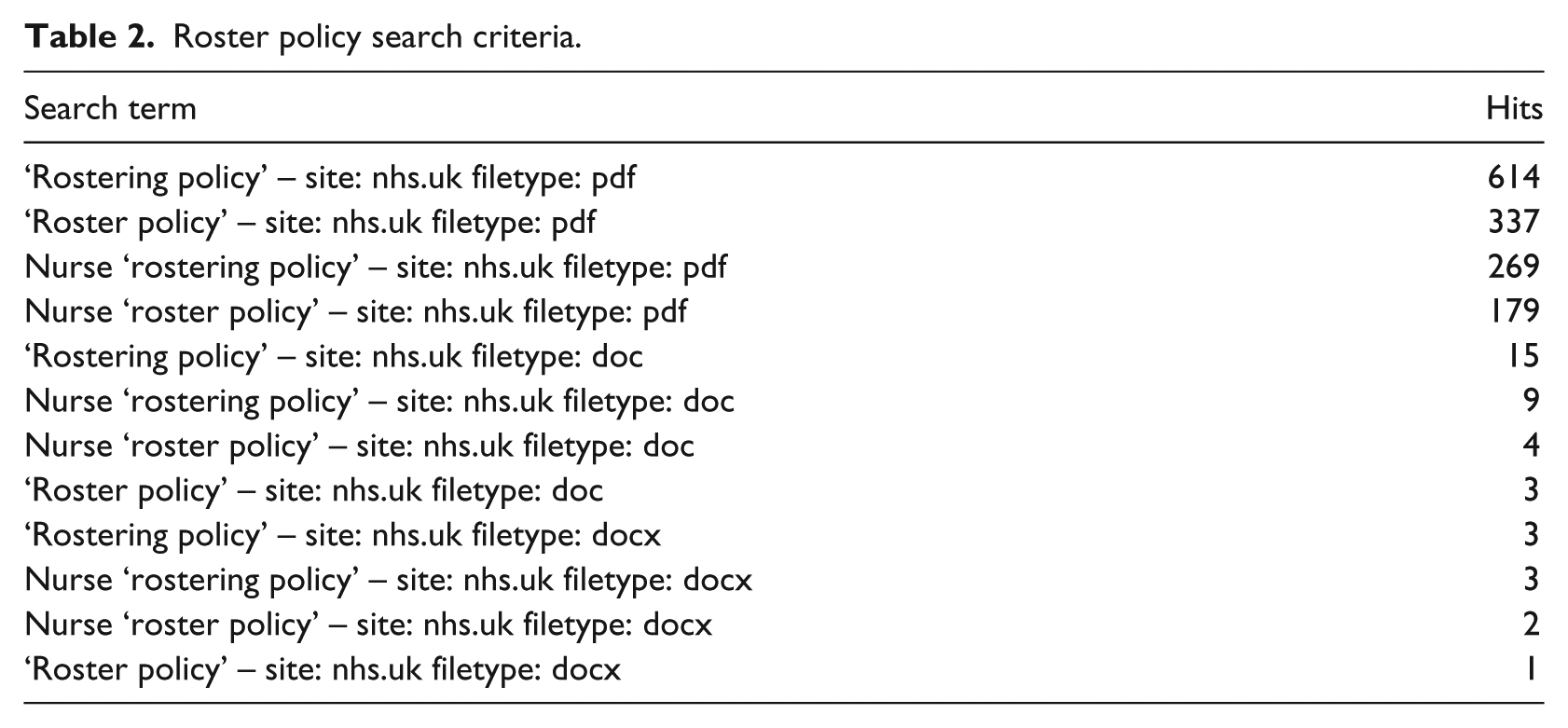
The study is based upon 46 publicly available roster policies (Table 1). Utilising the Google search engine, the data were collected during the period between 23 August 2015 and 12 March 2017. The search terms used and their results can be found in Table 2. These results were then screened to remove duplicate/older versions of policies and irrelevant documents such as agendas, minutes and newsletters in which roster polices were mentioned. A series of search terms excluding the .nhs.uk domain were then used to identify roster policies deployed in institutions outside the NHS and the UK. Unfortunately, only one relevant document was found – The Rostering Resource Manual from New South Wales Ministry of Health, Australia.
Publicly available roster policies used.

NHS: National Health Service.
Roster policy search criteria.
Ethical considerations
The roster policies used in this research were all available in the public domain and readily accessible on the internet.
Data analysis
A preliminary inspection of the roster policies revealed that there were several areas of duplication between policies. To quantify this, the policies were analysed using the commercially available text-matching tool, Turnitin™. The ‘Originality Check’ facility of the software used a matching algorithm to find strings of words within a specific policy that were identical to those within its general repository. Of 46 policies examined, 12 shared 50 per cent or more of their content with other policies in the sample, while 6 shared 10 per cent or less (Table 1). For example, Southern Health NHS Foundation Trust shared
65 per cent with Hampshire Community Health Care;
42 per cent with Aintree University Hospital NHS Foundation Trust;
42 per cent with South Staffordshire and Shropshire Healthcare NHS Foundation Trust.
Consequently, there were numerous common phrases and expressions, such as the following statement which occurred on 12 policies, ‘[Trust] recognises the value of its workforce and is committed to supporting staff to provide high quality patient care’.
Using thematic analysis, the content of the policies was then coded using QSR NVivo11 software. An initial set of categories were developed based upon the explicitly stated objectives of each policy. 23 These categories were then translated into nodes. The body of each policy was then examined. Relevant content was allocated to the initial ‘objective’ nodes and emergent themes used to construct new nodes as they arose. The Rostering Resource Manual from New South Wales Ministry of Health was also coded in order to provide a comparison to the NHS policies. After three iterations, similar themes were combined into meta-themes.
Validity and reliability/rigour
Reliability in content analysis requires two distinct factors: that the coded data set produced from the analysis is consistent and that the coding instrument is dependable. 24 The first is often met using multiple coders and eliminating the discrepancies between them, and the second by ensuring well-defined decision categories and well-specified decision rules. Verifying the integrity of the coding tool reduces the necessity for multiple coders. 25 In this instance, while the coding was undertaken by the author alone, the initial categories were taken from the explicit objectives of each policy, thereby providing the well-defined decision categories required.
Results
The stated objectives of the roster policies code into five major themes described as follows:
‘Fair but safe’ (46 policies).
‘Efficiency by utilisation’ (33 policies).
‘Staffing for care’ (31 policies).
‘Agency/bank minimisation’ (28 policies).
‘Payment processing’ (11 policies).
The ‘Fair but safe’ objective
All 46 policies examined included an objective associated with roster fairness. In 35 policies, this was qualified with the need for safe staffing and often expressed as ‘Ensure safe and appropriate staffing using fair, consistent rosters’. Conversely, while the NSW policy had the most references to fairness, it also had the lowest references to safety. 26 While none of the policies explicitly defined ‘fairness’, 18 referred to ‘fair and equitable rosters’. To achieve equity, the procedures for allocation of requests, annual leave, flexible working and study leave were explicit in all policies. For example, the shift request process in most policies was highly codified and typically specified:
The mandatory use of the e-rostering system for requests.
The period during which requests could be made, prior to the roster being created.
The maximum number of requests allowed.
The indicators used to monitor roster fairness.
The responsibility for approving requests and reviewing the fairness of requests.
The procedure for requesting annual leave was also highly codified, particularly with regard to the allocation of school holidays and festivities such as Christmas. However, the process for flexible working was less specific and in 34 policies referred to a separate document.
Interestingly, although 23 policies included ‘Definitions’ sections, none defined what the terms ‘fairness’ or ‘safety’ meant in terms of rostering. Moreover, despite fairness being the most common objective, a consistent framework for how this was to be achieved was not provided. Indeed, explicit measures of fairness could only be found in 15 policies these included as follows:
Number of approved shift requests as a percentage of total shifts worked.
Number of approved requests per person.
Number of shifts breaking rules as a percentage of total shifts worked.
Number of Christmas shifts worked per person.
In total, 16 policies placed responsibility for fairness with Ward Managers, though some trusts had expressly designated roles for e-rostering, such as Roster Creator (5 policies) and Roster Approver (3 policies). Ward Managers were expected to fulfil this responsibility by resolving issues around
Annual leave;
Study leave;
Shift requests;
Work patterns.
The ‘efficiency by utilisation’ objective
This was commonly expressed as ‘To provide effective management of the staffing establishments, thereby driving efficiencies in the workforce’ (18 policies) or ‘To enable the effective utilisation of the workforce through efficient rostering’ (8 policies). The key aspects of the efficiency objective included the following:
Utilisation of staff (34 policies).
Redeployment of staff (19 policies).
Responsibility for efficiency (5 policies).
Of the 34 policies highlighting staff utilisation, 12 included the following statement, ‘All rosters should be composed to adequately cover 24 hours, where appropriate, utilising permanent staff proportionally across all shifts’. However, none of these policies offered procedures defining how this would be achieved. In 10 of these policies, this was the only statement regarding efficiency. Other metrics assigned to the efficient utilisation of staff included percentage additional duties (24 policies) and percentage lost contracted hours (20 policies). No policy offered any procedures or metrics associated with the redeployment of staff though 12 policies stated that ‘During staff shortages it is accepted that staff may be required to work in other clinical areas to provide a safe and efficient service’.
The responsibility for achieving the efficiency objective differed across the policies. Most frequently, Ward Managers were charged with the responsibility for minimising lost contract hours while Matrons were responsible for staff redeployment, use of bank/agency staff and justification of additional shifts. The setting of efficiency indicators was usually the purview of the finance/accountancy staff, though in some policies responsibility lay with Roster Administrators, the e-rostering team, the e-rostering manager or the e-roster Project Support Officer.
The ‘staffing for care’ objective
This objective was concerned with the management of staffing levels and skill mix to ‘maximise the quality of patient of care’ (17 policies). Policies that did not include this as an explicit objective often implied it within the ‘fairness objective’, the term ‘appropriate staffing’ and ‘quality of care’ being commonplace within both objectives. Many policies focused on how often establishment numbers were reviewed (19 policies) and the responsibilities of staff regarding establishments (36 policies), for example: ‘skill mix and establishment should be reviewed at least annually, with the budget setting and workforce planning process. Skill mix and establishment reviews may happen more frequently if a need/risk is identified’ (11 policies). Typical establishment objective indicators were as follows:
Percentage of bank staff requested.
Post vacancies Whole Time Equivalent (required posts – actual staff-in-post).
Redeployed people hours.
Percentage staff with working restrictions.
Generally, the Ward Manager and/or Matron were responsible for setting the establishment but these then had to be agreed with the Director of Nursing before being signed off by the Directorate Management Accountant and/or the Director of Finance (27 policies).
The ‘bank/agency minimisation’ objective
Specified in 28 policies, this objective targets a reduction of nurse bank/agency spending. In total, 23 policies included detailed procedures for the assignment, deployment and monitoring of temporary staff. In total, 12 policies stated this objective as ‘reduce band and agency spend by giving [staff] clear visibility of contracted hours’. However, other policies only included metrics for measuring agency spend in headline key performance indicators (KPIs).
The ‘payment processing’ objective
This objective, commonly expressed as ‘to facilitate the payment of staff through data being entered at source’, was concerned with integrating the e-rostering system with the trust payroll system in order to minimise administrative errors and reduce the estimated £30.5 million overpayment of staff. The significance of payroll closing was most commonly accentuated as ‘all updates to the roster must be made as soon as practically possible after occurrence, taking into consideration Payroll deadlines’ (11 policies).
Rostering rules and localisation
While the policies examined were developed at trust level, local ownership of the roster was also evident. In total, 40 policies contained references to ‘local, ward-based’ sub-policies. The key areas of proposed localisation were as follows:
Staffing levels and skill mix.
Processes for managing additional demand.
Rostering of holidays and requests.
Flexible working arrangements.
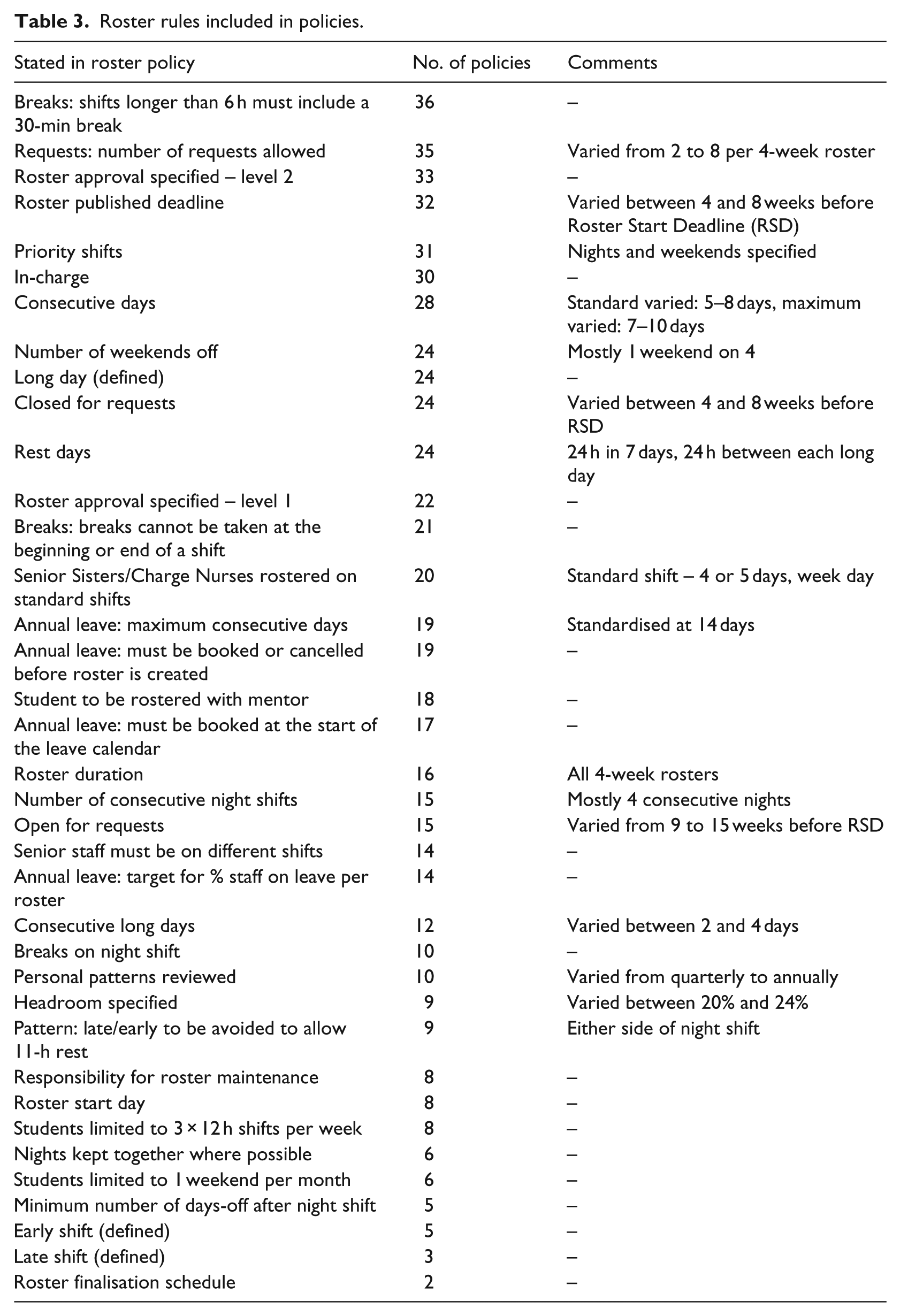
However, while the governance aspects of the roster were quite specific and increasingly codified as KPIs, the rules used to design the rosters, the actual ‘hard’ and ‘soft’ constraints were less specific (Table 3). No constraint was common to all policies in the sample and few were common to any. Where specified, roster rules varied significantly from trust to trust, with the most common associated with breaks, requests, roster approval and consecutive shifts. Interestingly, the NSW policy contained no specific constraints whatsoever. Instead, it explicitly stated that ‘there remains scope within the guidelines for managers to develop local variations relevant to their agree unit requirement’ (p. 3). 26
Roster rules included in policies.
Discussion
Codification and the roster policy
While codified knowledge is central to many healthcare systems used to enhance quality and accountability, 27 historically, there has been no universally accepted policy that nurse managers could use to allocate nursing resources efficiently. 28 Silvestro and Silvestro 6 note that the ‘specifications of rostering systems are rarely formally documented, despite their complexity and intricacy’ (p. 97). Increasingly, however, with the advent of e-rostering, processes and procedures are being codified and it is this ‘complexity and intricacy’ that poses the greatest challenge.
Resolution of the NRP has defied the efforts of OM experts for almost half a century. 5 During that time, many solutions have been proposed using abstract models that codify the intricacies, ostensibly reducing the need to grasp complexity 16 and bringing the illusion of transparency to the NRP. Unfortunately, information losses during codification have rendered those solutions non-generalisable, undefined and ambiguous. For transparency to be realised, stakeholders require a common language, set of rules and the capacity to interpret the code. This is the role of the roster policy.
The ‘fair but safe’ objective
Arguably, e-rostering produces fairer schedules2,3 and the term ‘fair’ is the most common used across the policies examined (11 times in each, on average). Despite this, the term remains undefined in any policy. ‘Fairness’ is multi-faceted and may be codified in several ways. Fairness may mean ‘sameness’ (equality of outcome), ‘deservedness’ (individual freedom) or ‘need’ (social justice). The evidence of this work suggests that fairness in roster policies is interpreted as equality of outcome. For example, the need for ‘equitable’ allocation of requests (36 policies), annual leave (23 policies), flexible working (14 policies) and study leave (12 policies) were all expressed explicitly. However, equity is a comparative measure, yet none of the policies specified boundaries within which these rules should apply. Consequently, policies may promote equality within a ward, 6 while exacerbating inequality between wards, between staff of the same grade or between hospitals within a trust.
Moreover, the use of rules to mandate equality offers only a superficial perspective of fairness within a tight-knit clinical team. In practice, fairness is engrained in ward culture and may be a fusion of ‘sameness’, ‘deservedness’ and ‘need’. Consequently, what is considered fair on one ward may be perceived as unfair on another. 29 In developing the roster, Ward Managers, with intimate knowledge of their staff, often attempt to balance all aspects of ‘fairness’ while maintaining safe staffing levels. However, as policy is increasingly developed in terms of procedural instructions and governance, their ability to act as autonomous professionals may become diminished. 30
Governance: the meta-objective
The role of governance is to ‘consolidate, codify, and universalise often fragmented and far from clear policies and approaches’. 31 E-rostering promises transparent, trust-wide, governance 3 and objectives such as ‘efficiency by utilisation’, ‘staffing for care’ and ‘payment processing’, may be regarded as different perspectives of that governance structure. For example, the ‘agency/bank minimisation’ objective is clearly aimed at controlling costs following a record £3.3 billion NHS spend on agency staff in the financial year 2014/2015. 32 Moreover, this research suggests that each of these objectives already has highly codified procedures with explicit performance indicators. Indeed, while the Carter Review 1 notes, ‘For clinical staff we observed variation … in policies and practices such as rostering’ (p. 7), this study illustrates that, even prior to Carter, trusts that had implemented e-rostering were, albeit at different speeds, beginning to converge around a common governance structure founded upon operational efficiency and safe, cost-effective staffing levels. Consequently, as McIntyre 3 seeks to standardise policies further, a single NHS governance structure for rostering, similar to that prepared for the 220 hospitals of NSW Health, is achievable.
However, beyond procedural governance, rostering is accomplished locally within each ward, using a series of constraints. These constraints or ‘rules’ vary significantly between wards and may depend upon ward size, clinical specialism, the range of ward activities and team/management arrangement within the ward. 6 Indeed, as Drake 5 notes, ‘the inclusion of a constraint itself, appears to be determined, to a large extent, by the Ward Manager preparing the roster’ (p. 807). This is tacitly acknowledged within the NSW Health policy by the absence of explicit rostering rules. However, selected NHS policies attempt to mandate some of the more common rules (Table 3) in order to impose consistency at a more codified governance level. Unfortunately, given the uniqueness of constraints on each ward, this is likely to lead to sub-optimal rosters as codification enforces a ‘one-size fits all’ policy to quite different ward environments.
Moreover, while Hockley and Boyle 2 claim that e-rostering reduces the administrative load of Ward Managers, at ward level, roster requirements change regularly due to variations in staff, patient acuity and demand. This requires staff that are well-versed in changing the parameters of the e-rostering system, aware of when this is necessary and permitted the time required to do so. If this is the case, then the administrative burden is simply transferred, from manually maintaining the roster to maintaining the e-rostering system. Such challenges are regularly found in the information system failure literature.33–35
Consequently, when McIntyre 3 notes that rostering ownership should lie across the functions of nursing, finance and human resources, this requires that the codified knowledge of the roster policy be a proxy for the common language and experience acquired on a ward through everyday interaction. Subsequently, it is assumed that this ward-level knowledge may then be consolidated and re-packaged for the use of managers and executives. 19 However, these users may be oblivious to the following complexities:
‘Fairness’ remains undefined and its codification is likely to extend far beyond the equitable allocation of approved request shifts specified by most of the policies examined.
Rostering remains a representation of a series of non-deterministic polynomial-time (NP)-hard combinatorial optimisation problems that continue to challenge computational complexity theory due to its multiple complex constraints. 36
Roster constraints change regularly, casting doubt on the veracity of time-based comparisons.
Different wards often use a unique set of rules/constraints in developing their rosters, making inter-ward comparisons dubious.
There is then the potential for managers and executives to interpret this consolidated codified knowledge incorrectly. 19 For example, an important KPI used in a number of policies is the percentage of roster rules broken during a roster period. However, this metric may vary from unit to unit for a number of reasons given that
As Drake 5 notes, at ward level, the inclusion of a rule is often decided by the Ward Manager and that, ‘rules appeared to be applied (or disregarded) arbitrarily to certain individuals or groups of staff’ (p. 806).
Other than differentiating between a ‘hard’ constraint (an inviolable rule) and a ‘soft’ constraint (a ‘warning only’ rule), the e-rostering system cannot discern the ‘significance’ of rules, thereby allowing roster creators to discount rules they feel are unimportant. 9
Complex units such as operating theatres often require significantly more roster rules than general nursing wards.
Thus, while Carter 1 demands ‘policies and procedures that are swift and simple’ (p. 18), this research suggests that this is well underway with the ongoing consolidation of existing roster policies. Indeed, there is scope for the NHS to develop a service-wide process and procedures manual similar to that recently introduced in NSW 26 such that trusts are not continually ‘re-inventing the wheel’. However, when Carter calls for ‘a single version of the truth’ (pp. 4, 8, 9, 58, 86), at ward level at least, there needs to be a recognition that the NRP continues to resist all efforts at simplification and consequently the notion of a single truth is pure abstraction. 16 Consequently, executive and managerial users need to be aware of the limitations arising from the codification and normalisation of this consolidated, ward-based data.
Conclusion
The last decade has seen the rapid growth of e-rostering systems across the NHS. Indeed, the Carter Review explicitly endorses such systems, suggesting that they produce a fair and transparent working environment while reducing the dependency on expensive bank and agency staff. It is, therefore, reasonable to assume that the dashboard-type information arising from such systems can be gainfully exploited by senior managers across nursing, human resource (HR) and finance functions. On the contrary, this research, while recognising the apparent benefits of e-rostering, raises a note of caution. As seductive as they may appear to executives, information on rostering dashboards remain abstractions from the original data through a process of selective codification.
The roster policies examined represent a codified governance structure designed to bring clarity to the workforce planning process. Unfortunately, increasing convergence on a common roster development procedure may also leave executive users oblivious to the implicit complexities and trade-offs, associated with rostering. While e-rostering involves convoluted algorithms, Byzantine rules and substantial computing power, manual rostering addresses multi-faceted concepts such as fairness (as opposed to equality), trust and team dynamics. Unfortunately, neither method provides an ideal solution, and it could be argued that while manual rostering defies governance to the benefit of the ward staff, e-rostering neglects the ever-changing needs of staff in favour of hierarchical governance. In the push for transparency, it is imperative that executives recognise that e-rostering is not a silver bullet and the information from such systems requires careful interpretation and circumspection.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.