
Abstract
Content produced by caregivers of stroke survivors on the online video-sharing platform YouTube may be a good source of knowledge regarding caregivers’ unmet needs. We aimed to examine the content, quantity and quality of YouTube videos that target and discuss the needs and concerns of caregivers of stroke survivors. YouTube was systematically searched using six search strings, and the first 20 videos retrieved from each search were screened against the inclusion criteria. A pre-determined coding schedule was used to report the rate of unmet needs in each video. Twenty-six videos were included in the analysis. In total, 291 unmet needs were reported by caregivers of stroke survivors, an average of 11.2 unmet needs per video. The most common unmet needs domain was ‘Impact of Caregiving on Daily Activities’ (44%). Most videos were developed in the United States (61.5%) and featured spouses of stroke survivors (65.47%). Content produced by caregivers of stroke survivors on YouTube may be used as a tool for caregivers to provide and receive support through online communication. YouTube videos offer insight into the unmet needs of caregivers of stroke survivors and may be used as an additional resource for stroke services to support caregivers.
Introduction
Stroke is the second leading cause of disability worldwide. 1 Stroke events often result in long-term negative health outcomes, such as cognitive and/or physical disability post-stroke, and increased risk of anxiety and depression. 2 Around 50% of people who have a stroke will require care, 3 and often this care is provided by family members or friends. As a result, stroke events deeply affect not only the stroke survivor, but often the quality of life and physical and psychological health of the caregivers,4,5 Internationally organisations, such as The International Alliance of Carer Organizations (IACO),6,7 support the need to identify the issues and concerns of caregivers of stroke survivors, in order to improve both stroke survivor and carer health and well-being.
Informal caregivers (defined as people who provide unpaid care and/or support to someone in need of care) may be family members or friends who provide day-to-day pragmatic, physical or emotional support to a stroke survivor. 8 Informal caregivers of stroke survivors are predominantly spouses of the stroke survivor 9 and often take on new and sometimes challenging roles post-stroke, in addition to providing daily living support to the stroke survivor. Many informal caregivers, such as spouses and children, wish to keep ‘caring within the family’ 10 which can create complex relationships between the stroke survivor, their caregiver(s) and other family members impacted by the stroke. The stroke survivors’ course of recovery can also heavily impact the caregiver, as the stroke survivor may improve and decline at unpredictable rates,11,12 As a result, the stroke caregiving trajectory fluctuates and is unique compared to other illnesses12–15 such as dementia, which shows a linear decline. 16 This is a particular challenge for caregivers of people who have had a stroke, as their caregiving roles and tasks may require immediate changes in response to the stroke survivors’ ongoing needs. Therefore, it is important for caregivers of stroke survivors to be able to readily access information and resources to meet their ongoing needs which change over time. 12
Unmet needs occur when support and services to address a person’s needs are not available and/or received. 17 Caregivers of stroke survivors often report a range of unmet needs, including inadequate resources and delivery of information,5,18–20 and difficulty in managing cognitive, behavioural, communication and emotional changes in stroke survivors. 21 Caregivers have reported feeling socially isolated post-stroke as providing care may prevent them from maintaining a satisfying social life and relationships with friends and family outside of the caregiving role,10,22–24 The Internet and social media have been identified as tools which caregivers use to seek health information related to the care of their relatives. 25 Hamm et al. 26 conducted a scoping review of how patients and caregivers use social media and identified that self-care was the most commonly reported use of social media, closely followed by posting and sharing experiences with peers. Therefore, caregivers of stroke survivors may turn to web-based platforms to connect with other caregivers in similar situations and to find stroke care-related information. 26
Little research has examined YouTube as a means of social support or information resource for caregivers. YouTube (https://www.youtube.com/) is a cost-free video-sharing social media platform, which allows users to view, generate and upload audio-visual content. 27 It is the second most accessed website worldwide 28 and has over 1 billion users – almost one-third of all people on the Internet. 29 In this study, we aim to conduct an online study and examine the quantitative and qualitative content, quantity and quality of YouTube videos that specifically target and discuss the needs and concerns of caregivers of stroke survivors. With this additional insight and information, the provision of care to this particular group across varying countries and healthcare systems by identifying areas of active need and interest on video-sharing social media.
Methods
Study design
An online study was conducted using the online YouTube search engine. The study received approval from the University of Newcastle Human Research Ethics Committee, Approval No. H-2017-0274.
Search strategy
Between September and October 2017, one member of the research team (A.M.J.D.) searched videos using the following search terms: ‘carers of stroke survivors’, ‘caregivers of stroke survivors’, ‘stroke carer’, ‘stroke caregiver’, ‘family of stroke survivors’ and ‘spouses of stroke survivors’ in the YouTube search engine. These search terms were developed to identify YouTube videos that capture a range of experiences of caregivers of stroke survivors and first-hand testimonials that may be produced by both professional organisations and carers themselves. The terms carer and caregiver were both used, as some organisations and caregivers themselves prefer to use one term over the other. The search terms ‘family of stroke survivors’ and ‘spouses of stroke survivors’ were included to capture the experiences of family caregivers of stroke survivor, who may not use the language of ‘caregiver’ or ‘carer’ to discuss their experiences providing care for a family member or friend who has experienced a stroke. Videos were sorted with the default ‘relevance’ setting to obtain the most relevant videos.
Methodology used in previous similar research was applied, whereby the first 20 videos obtained from each search were watched fully to identify relevant videos that fulfilled the eligibility criteria, including videos in the ‘up next’ section 30 – 31 .
Eligibility criteria
YouTube videos were included in analysis if they were produced and developed by either adult caregivers of stroke survivors and focused on carers’ needs and concerns, or professional organisations (such as the Stroke Foundation, which is in Australia) and depicted first-hand testimonials of the needs and concerns of caregivers of stroke survivors. Videos were excluded if they were (1) intended for caregivers of other populations such as people with dementia; (2) were intended for, and focused on, stroke survivors; (3) were developed and produced by professional organisations and provided information and/and or help guides; (4) were in languages other than English and (5) were duplicates of other videos already identified by the search strategy. There was no limit on the date for YouTube videos published.
Data extraction
Two researchers (A.M.J.D. and S.A.H.) independently reported the prevalence of unmet needs in the content of each included video according to a pre-determined coding schedule (Appendix 1) based on a literature review with caregivers of people who have cancer 17 and caregivers of stroke survivors,5,32 An example of this is a domain titled, ‘Emotional and Psychological’ with subdomains such as ‘Know How to Provide Emotional and/or Psychological Support for Stroke Survivor’ which is defined as ‘Caregiver expresses lack of knowledge on how to provide emotional or psychological support for the stroke survivor’. Unmet needs were reported at each instance they were mentioned by a caregiver of a stroke survivor; multiple unmet needs could be reported per video. For each video, information was collected on the country of origin, total number of views and comments, and number of ‘likes’ and ‘dislikes’, and video duration in minutes. The two reviewers met to discuss discrepancies in their decisions, and a third reviewer was consulted in case of disagreement. The quality of the video and audio track for each video was measured, following the methodology of Sorensen et al. 33
YouTube provides information on the content producer, including the username and profile photo. If the username of the YouTube content producer was associated with an organisation and was further supported by the branding of the organisation, this was determined to be an organisational or ‘professional’ YouTube account. YouTube accounts that did not have usernames or images associated with organisations were determined to be developed by ‘amateurs’ (defined as people who individually developed the videos without the licence from companies). The following information was reported about each video: if the video was developed by a professional organisation or an amateur, the population of people appearing in each video and the relationship of the caregiver to the stroke survivor were also recorded. As YouTube does not provide the country in which the videos were uploaded from, the Social Blade 34 analytics website was used to determine video country of origin where videos had five or more subscribers.
Analysis
Proportions were used to report the frequency of each unmet need domain or individual item in each video, compared overall and by country. Proportions were also used to report the country, developer, relationships of caregivers and the population (single caregivers, multiple caregivers, stroke survivors and healthcare professionals) of each video. Descriptive statistics were used to report the duration of the videos, views, number of ‘likes’, ‘dislikes’ and comments.
Representative quotes of the videos were transcribed verbatim by A.M.J.D. and were coded to unmet needs domains using the pre-determined coding schedule. Videos were also grouped according to general theme of the qualitative content of each video based on categories by Hamm et al. 26 where videos were also grouped according to the following themes on the content of the videos: Vlogs (video blogs diarising an experience), Providing Tips, Collaborative Projects with the Caregiver Community and Seeking Support. The audio quality and video quality of the videos were analysed using methodology by Sorensen et al. 33 in which videos are rated on a measure of ‘poor’, ‘fair’ and ‘good’.
Results
Of the videos identified through searching YouTube on the unmet needs and concerns of caregivers of stroke survivors, 26 were included in the final analysis. The majority of videos identified in our search were excluded as they either focused on stroke survivors or were developed by healthcare professionals. A flow chart of this process is shown in Figure 1.
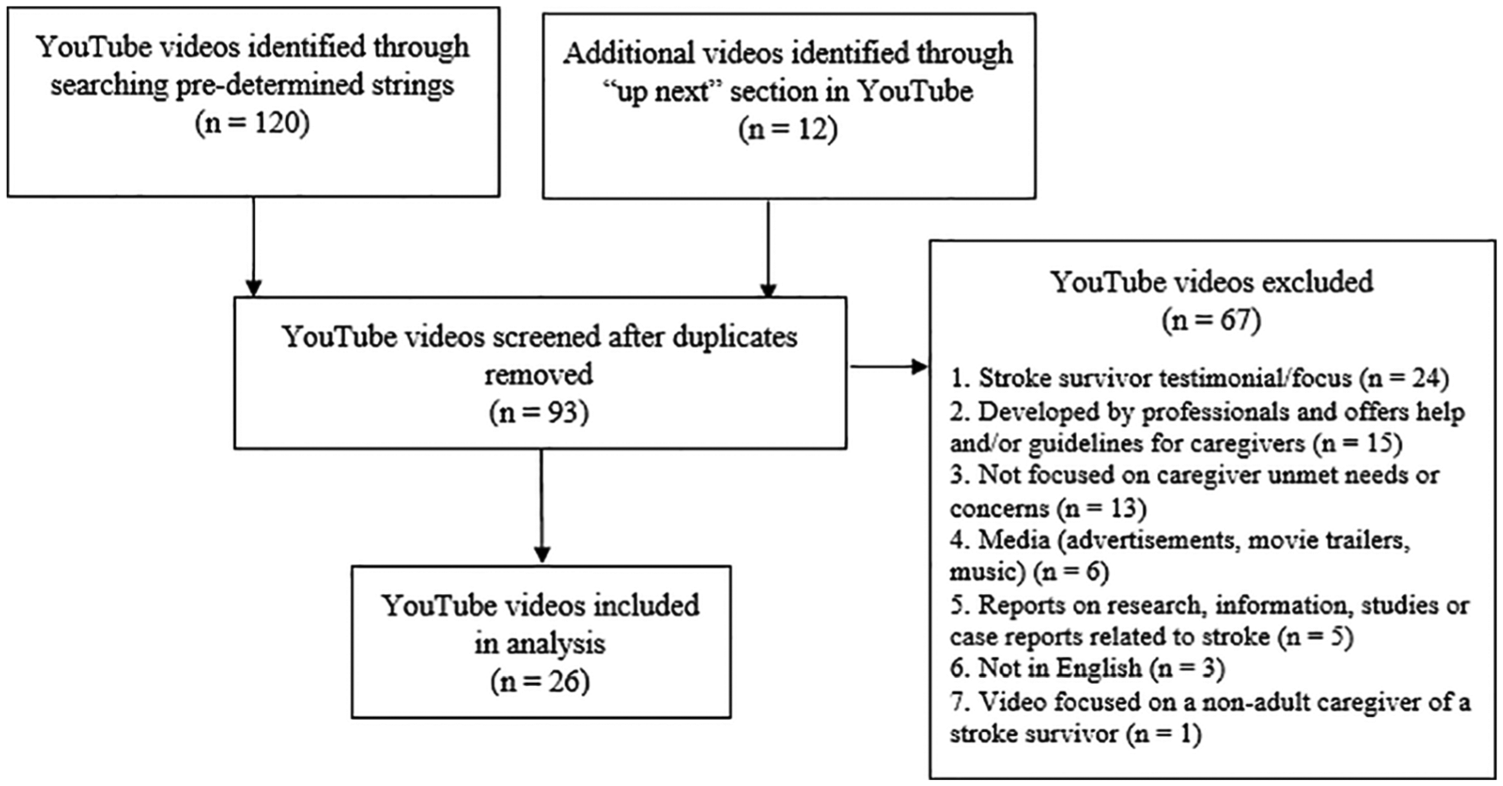
Flowchart of YouTube video screening process.
The search strings which identified the most relevant results were ‘Caregivers of stroke survivors’ and ‘Stroke caregivers’ which identified seven relevant videos in each search (35%). The least relevant search string was ‘Family of stroke survivors’ which identified no relevant videos. The majority of relevant videos were developed in the United States (61.5%), were developed by amateurs (57.7%) and featured spouses of stroke survivors (65.47%). Videos ranged from 1 min and 28 s to 19 min and 35 s. All videos developed in the United Kingdom were developed professionally, while 15 of the 16 videos developed in the United States were developed by individual caregivers. The single video developed in New Zealand was professionally developed. In total, there were 10 unique creators of videos, containing testimonials of 28 unique caregivers. The majority of caregivers were female spouses of the stroke survivor. Other video characteristics are reported in Table 1.
Characteristics of needs and concerns of caregivers of stroke survivors videos on YouTube (n = 26).
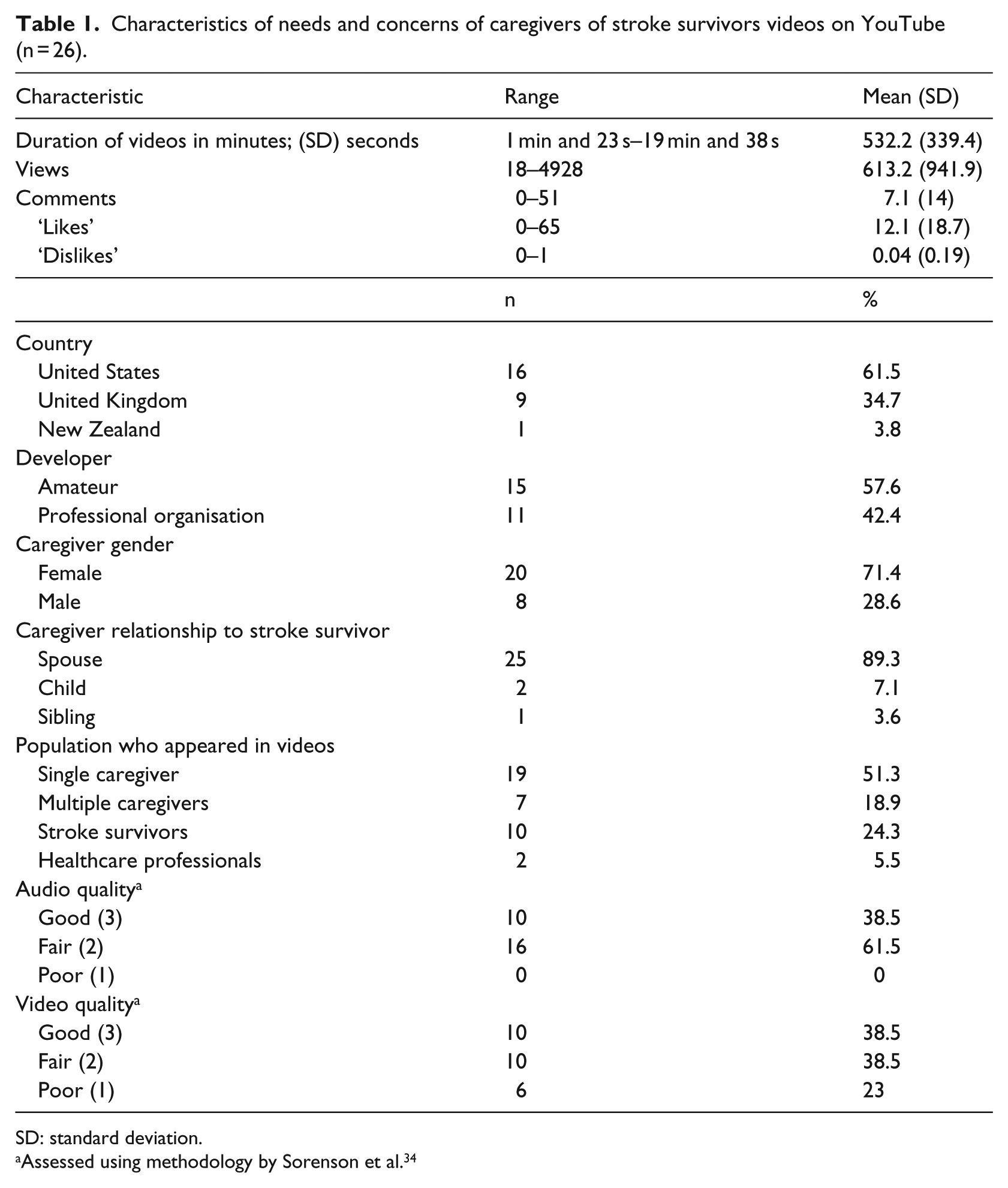
SD: standard deviation.
Assessed using methodology by Sorenson et al. 34
In total, there were 291 unmet needs reported by caregivers of stroke survivors over 26 videos, with an average of 11.2 unmet needs per video. Multiple unmet needs could appear in a single video. The most reported unmet needs domain by caregivers was Impact of Caregiving on Daily Activities, which made up almost half of reported unmet needs (44%). Table 2 reports the frequency of unmet needs of caregivers of stroke survivors appeared in each video.
Frequency of unmet needs of caregivers of stroke survivors which appeared in identified YouTube videos (n = 26).
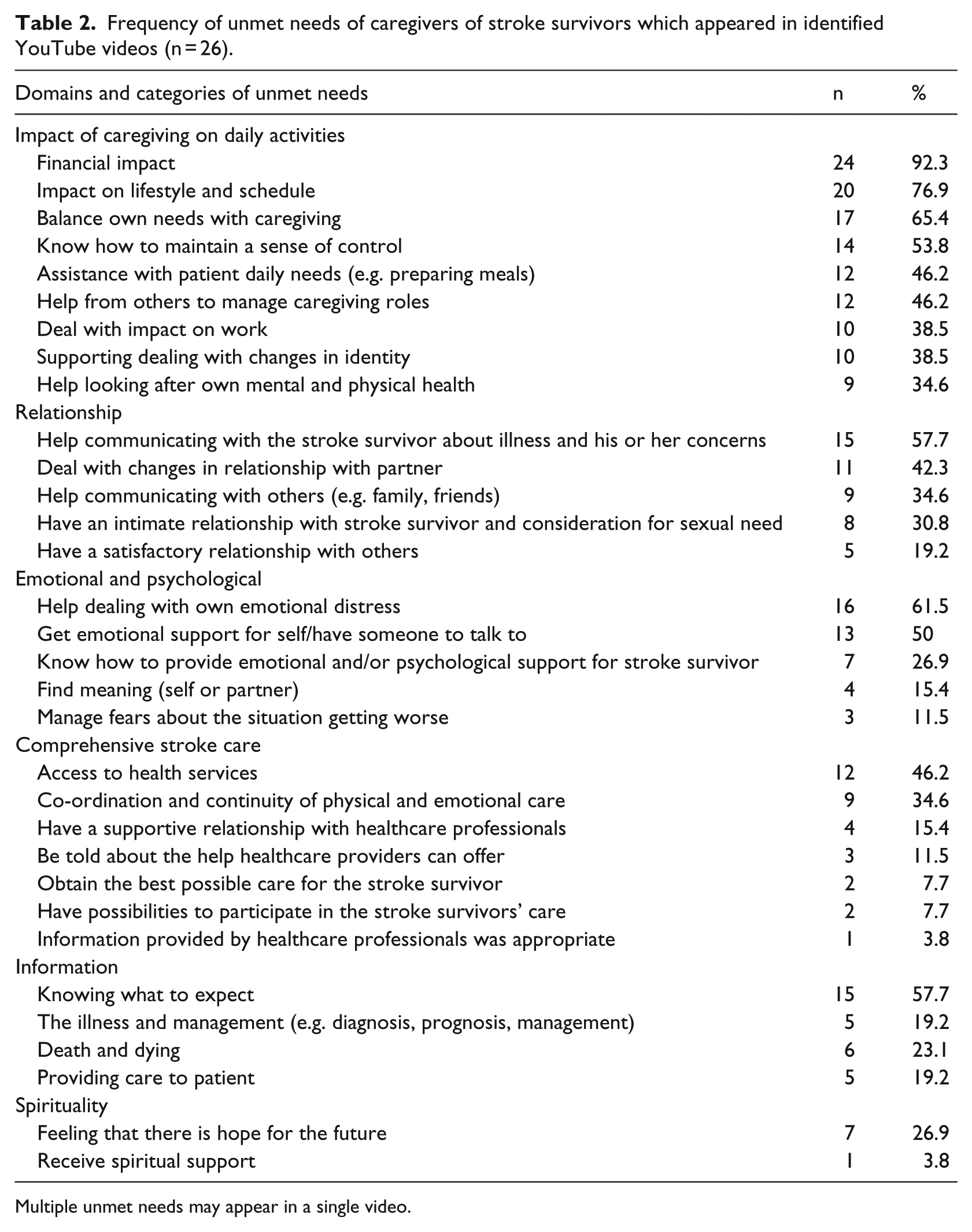
Multiple unmet needs may appear in a single video.
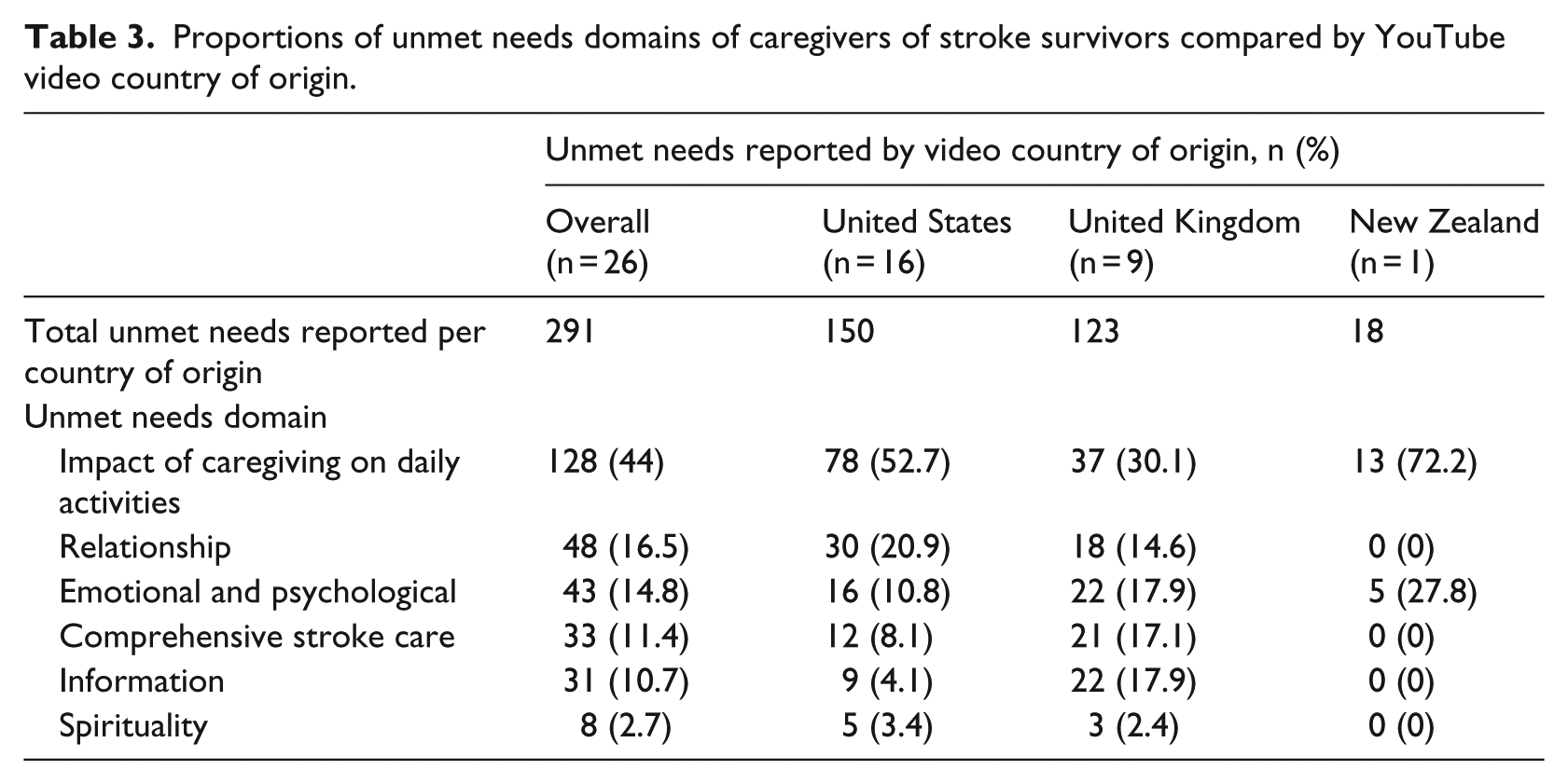
Comparisons of unmet needs domains by country are reported in Table 3.
Proportions of unmet needs domains of caregivers of stroke survivors compared by YouTube video country of origin.
Domains of unmet needs
Impact of caregiving on daily activities
The most commonly reported unmet needs domain was ‘Impact of Caregiving on Daily Activities’, which appeared 128 times in 26 videos, and made up 44% of the unmet needs reported. The highest reported subcategory in this domain was ‘Financial Impact’, which appeared 24 times in 26 videos (92.3%). Caregivers who appeared in YouTube videos developed in New Zealand reported the most ‘Impact of Caregiving on Daily Activities’ unmet needs (72.2%).
Relationship
Unmet ‘Relationship’ needs of caregivers of stroke survivors appeared 48 times in 26 videos and made up 16.5% of the unmet needs reported across YouTube videos. ‘Help Communicating with the Stroke Survivor About Illness and His/Her Concerns’ was the highest reported subcategory in this domain and appeared in over half of the YouTube videos that were analysed (n = 15, 57.7%). Caregivers who appeared in YouTube videos developed in the United States reported the most ‘Relationship’ unmet needs (20.9%).
Emotional and psychological
‘Emotional and Psychological’ unmet needs of caregivers of stroke survivors appeared 43 times in 26 videos, which made up 14.8% of the unmet needs reported. The most commonly reported category was ‘Help Dealing with Own Emotional Distress’ which appeared in 16 (61.5%) YouTube videos which met inclusion criteria. Caregivers who appeared in YouTube videos developed in New Zealand reported the most ‘Emotional and Psychological’ unmet needs (27.8%).
Comprehensive stroke care
‘Comprehensive Stroke Care’ needs of caregivers of stroke survivors appeared 33 times in 26 videos, which attributed to 11.4% of the unmet needs reported. The most frequently reported category was ‘Access to Health Services’ which appeared in just under half of the videos analysed (n = 12, 46.2%). Caregivers who appeared in YouTube videos developed in the United Kingdom reported the most ‘Comprehensive Stroke Care’ unmet needs (17.2%).
Information
Unmet ‘Information’ needs of caregivers of stroke survivors appeared 31 times in 26 videos, which made up 10.7% of the unmet needs reported. The most commonly reported category was ‘Knowing What to Expect’ which appeared in over half of the YouTube videos which met inclusion criteria (n = 15, 57.7%). Caregivers who appeared in YouTube videos developed in the United Kingdom reported the most ‘Information’ unmet needs (17.9%).
Spirituality
Unmet ‘Spirituality’ needs were reported eight times in 26 YouTube videos, which made up 2.7% of the unmet needs reported. The most frequently reported category was ‘Feeling That There Is Hope For the Future’ which appeared in just over one-quarter of the YouTube videos that were analysed (n = 7, 26.9%). Caregivers who appeared in YouTube videos developed in the United States reported the most ‘Spirituality’ unmet needs (3.4%).
YouTube video qualitative content
The majority of the videos were Vlogs, in which the main content featured the caregiver(s) diarising their daily thoughts and feelings in Vlogs (n = 16, 48.5%), followed by Collaborative Projects with the Caregiver Community, which featured caregivers discussing a topic from a professional developer (n = 9, 27%). The next most reported category was Providing Tips, in which caregiver(s) offered support and ideas to other caregivers (n = 7, 21.5%) and the least reported theme was Seeking Support (n = 1, 3%).
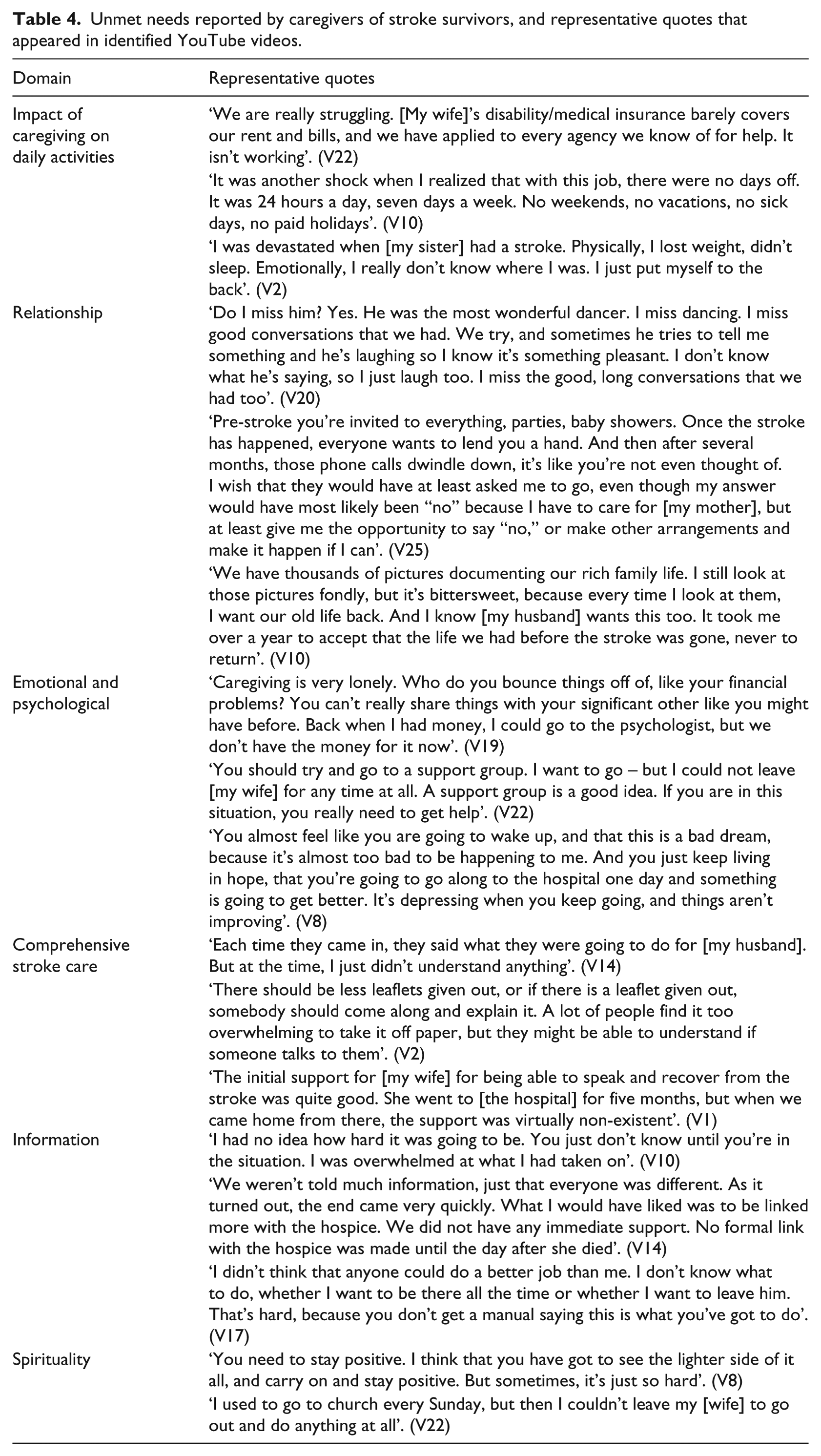
Two amateur caregivers of stroke survivors were responsible for producing half of the videos which met inclusion criteria (n = 13, 50%). These caregivers provided some information and insight on why they produced and developed the video series. This included documenting their lives as caregivers, offering support and/or advice to other caregivers, and to express frustration with the caregiving role. The first caregiver series containing five videos identified in the search documented the emotional burn-out of a caregiver over a period of 2 years (V19, V20, V21, V22, V23). This video series was a personal narrative recount of the caregiver’s experiences and needs and was treated more like a personal video journal to record his frustration and resentment. Another caregiver series containing eight YouTube videos focused on providing day-to-day strategies on time management, stroke-related products and the changing needs during the caregiving experience to inform and help other caregivers (V7, V11, V12, V15, V16, V24, V25, V26). Representative excerpts for each domain appear in Table 4.
Unmet needs reported by caregivers of stroke survivors, and representative quotes that appeared in identified YouTube videos.
Discussion
This study examined the content, quality and quantity of YouTube videos that feature first-hand testimonials of caregivers of stroke survivors. The findings of this study suggest that the majority of caregivers of stroke survivors are using YouTube to diarise their experiences, in which they explored their own experiences. Across the videos, it appeared that a proportion of the caregivers who uploaded videos were attempting to provide support to the online community of caregivers by providing tips and resources to assist with the caring role. This study highlights the unique additional information and insights provided by identifying areas of active need and interest by caregivers of stroke survivors who engage in this online community by uploading videos on YouTube, and those who watch the videos to connect with other carers.
The most frequently reported unmet needs domain was ‘Impact of Caregiving on Daily Activities’, in which ‘Financial Impact’ was the most frequently reported sub-domain. In recent research, information-related needs such as inadequate information delivery are generally the most commonly reported unmet needs,19,20,35 Additionally, previous studies have commonly used surveys, qualitative interviews and self-report measures as data collection methods to collect data to identify unmet needs. The current study captured behaviour in an unscripted video format as opposed to prescriptive videos developed by healthcare professionals for caregivers of stroke survivors. These unscripted videos offer a perspective from a phenomenological research approach. Therefore, these findings provide rich insight into the first-hand lived experiences of caregivers of stroke survivors, which can be used in addition to current research approaches to identify the unmet needs of caregivers of stroke survivors to develop support services and resources to assist them.
The patterns observed in ‘Financial Impact’ might also reflect the differing healthcare systems of the countries in which the videos were produced. Universal healthcare is available in countries such as in the United Kingdom and New Zealand; however, patients in the United States are often expected to pay for their treatment. Godwin et al. 36 systematically reviewed the cost associated with stroke in outpatient rehabilitative services and medicine in the first year following the stroke event. They found that in the first year, services such as rehabilitation cost US$17,081 and medicines cost US$5392. Therefore, the unmet needs of caregivers in the United States may be more focused on the financial impact compared to other countries.
The ‘Financial Impact’ of caregiving and aspects of lifestyle such as health, well-being and social are connected. Often family members give up their jobs to provide care, leaving them without financial support to engage in and maintain previously enjoyed social activities. 4 Therefore, the financial impact of providing care may affect the well-being of the caregiver by limiting their ability to engage in their usual hobbies, access supportive services and maintain a consistent working schedule. Caregivers of stroke survivors are not receiving the support they need through available social services, and it is possible that they are turning to online communities for support and information.
Caregivers express difficulty in separating and managing their own needs from caregiving, such as managing their mental and physical health, or a need for respite and time off from caregiving.5,37–39 Categories that can be considered health and well-being of the caregiver such as ‘Impact on Lifestyle and Schedule’ (n = 20, 76.9%), ‘Balance Own Needs with Caregiving’ (n = 17, 65.4%), ‘Access to Health Services’ (n = 12, 46.2%) and ‘Help Looking After Own Mental and Physical Health’ (n = 9, 34.6%) were all highly reported unmet needs across videos. These findings indicate that health services are failing to provide caregivers with the support that targets their health and well-being outcomes. Caregivers may be turning to online platforms such as YouTube to seek information on how to support themselves and provide support to other caregivers of stroke survivors.
The findings of Al-Busaidi et al. 40 were also consistent with our results, in which caregiver strain was a major factor. ‘Emotional and Psychological’ unmet needs were reported 43 times in 27 videos, with the highest subcategory as ‘Help Dealing with Own Emotional Stress’. These results are also consistent with Hamm et al. 26 who identified self-care as the main use of social media for patients and caregivers. Caregivers and the general population are increasingly using social media and web-based platforms as an acceptable way to access healthcare and self-care information/support. Using an easily accessible platform like YouTube to develop content and share experiences with other caregivers may provide caregivers with a tool to cope with stress and connect with other caregivers in similar situations.
There were numerous unmet needs reported by caregivers of stroke survivors across YouTube videos. In our search strategy, only 26 videos of 132 viewed (19.7%) featured content where caregivers of stroke survivors discussed their unmet needs and concerns. This percentage of relevant videos is much lower than in other fields of previous research using YouTube41–43 and suggests that it is difficult to find content that specifically addresses the unmet needs of caregivers of stroke survivors, even when search terms that target this population are used.
These findings suggest that the few caregivers of stroke survivors who create YouTube videos are willing to discuss their unmet needs. The YouTube videos that met our inclusion criteria ranged from 0 to 65 likes (M = 12.1, SD = 18.7) and a very small proportion of dislikes ranging from 0 to 1 (M = 0.4, SD = .19). This information suggests that the few people who are viewing these videos are noting them as positive. However, the range of views 18–4928 (M = 613.2, SD = 941.9) is vastly different from the number of comments (M = 7.1, SD = 14) and likes/dislikes. This indicates that while many people are watching the videos, a very small number of people are commenting on them. It is possible that the people who viewed the video contacted the creator of the video to connect with them, but it is not possible to determine if such contact occurred. As the likes/dislikes of the videos were largely positive, it would seem that YouTube could provide caregivers of stroke survivors with an opportunity to have their voices be heard and reach out to other caregivers to give and receive support.
Implications for policy
Views on each video varied greatly, ranging from 18 to 4928 views. Caregiving organisations worldwide including the International Alliance of Caregiver Organizations 7 may consider increasing their efforts to raise awareness through their other online and social media platforms to disseminate videos which feature first-hand testimonials of caregivers of stroke survivors. This would increase the reach of this information and make the needs of caregivers of stroke survivors more readily available to caregivers who seek to connect with other caregivers across the globe. Development of YouTube videos tailored to country and healthcare systems would be beneficial for caregivers to access country-specific information about how to access services, where to seek support and resources, and where to buy care products which may be helpful for caregivers seeking assistance. For researchers, YouTube videos allow the identification of unmet needs and preferences for service delivery would help address the lacunae in continuum of care, resulting in the development of support and services to address these needs.
YouTube videos may also be used in addition to clinical support to increase awareness of caregivers’ unmet needs and platforms to connect with other caregivers. Videos which feature first-hand testimonials of caregivers of stroke survivors may provide new caregivers with lived experience, information provision and a sense of belonging to a community. For example, when caregivers discuss their experiences, they may provide new caregivers with insight into questions for health providers that they may not have considered, knowledge of assistance and services available to them, and the possible life changes which they may experience as a family member of a stroke survivor. Provision of videos featuring first-hand testimonials from healthcare providers to new caregivers has the potential to decrease feelings of anxiety and isolation reported often by caregivers of stroke survivors, and increase preparedness for taking on the caregiving role.
Given that the majority of the videos were developed in the United States and the United Kingdom, efforts can be made to produce videos which are locally relevant worldwide. For example, there were no videos outlining experiences of Australian or Canadian caregivers. Organisations such as The Australian Stroke Foundation and the Heart and Stroke Foundation Canada could develop YouTube content as an addition to information and resources for stroke services, as this information delivery could greatly benefit caregivers who are struggling to navigate the Australian healthcare system and access relevant resources and services within Australia. Therefore, the addition of YouTube videos as a resource may increase caregiver well-being by (1) making caregivers’ experiences more accessible, and increasing connectivity to other caregivers and (2) making relevant information about available services and support more readily available.
Study limitations
This study only examined the quality, quantity and content of the unmet needs of caregivers of stroke survivors on YouTube. Therefore, findings from this study should not be generalised to other social media platforms such as Facebook. Furthermore, as most of the videos were produced in the United States and the United Kingdom, these findings may not be generalisable to countries with differing healthcare systems, including Australia and Canada.
Although the search through the YouTube search engine was developed to capture a representative sample of caregivers of stroke survivors, the majority of videos were developed by two amateur caregivers of stroke survivors. However, the sample of 28 unique caregivers who were female, male, spouses, children and siblings provided a range of rich insights into the caregiving role through the unique perspectives and relationships between the caregiver and stroke survivor. In addition, it is possible that some relevant videos were missed. For example, as the search criteria were limited to videos in English, it is possible that these findings may not be generalisable to non-English speaking populations in which there may be differing cultural unmet needs of caregivers of stroke survivors.
Implications for future research
Further research into other popular web-based platforms such as Google, Facebook and Reddit (rated as the first, third and sixth most accessed websites on the web respectively) 28 and other video streaming platforms such as Vimeo 44 may also be useful to review to further identify the unmet needs of caregivers of stroke survivors. Furthermore, YouTube has been recognised as a popular platform for disseminating health information 45 with the potential to be a cost-effective and wide-reaching modality for health and support interventions and services. The development of a service or intervention using YouTube to disseminate information and support to caregivers of stroke survivors to meet their needs should be considered. Reviewing YouTube as a resource to address unmet needs may also be beneficial to caregivers of other people, such as those of people with dementia and people with cancer, as it will offer insight into their unique needs alongside varying healthcare systems and countries.
For researchers, online spaces like YouTube are of research interest because they provide insights and first-hand testimonials that are produced by target populations and hard-to-reach groups which are free of research-influence and can also raise awareness to resources available to consumers to meet their needs. Understanding what happens in these online spaces can have value across a range of disciplines by providing further understanding to the unmet needs of groups of interest, and a consideration of these online platforms as a mode of delivery for interventions and services. From reviewing first-hand testimonials of the caregiving experience, this information could be used to inform and develop services, interventions and trustworthy, accessible information for caregivers internationally.
Conclusion
This study aimed to identify and report the prevalence of unmet needs of caregivers of stroke survivors, and to evaluate YouTube as a resource for addressing these unmet needs. This study found that YouTube videos offer useful insight into the needs of caregivers of stroke survivors across varying countries and healthcare systems. Researchers and health services should engage with caregivers to ask how to best develop the use of YouTube as a consumer on how this platform could raise awareness. YouTube may provide a platform for mutual support independent from health services from caregiver communities who can connect through YouTube. YouTube videos may be used to raise awareness as a source of information of the unmet needs of caregivers of stroke survivors when developing support services and resources to assist caregivers of stroke survivors.
Footnotes
Appendix
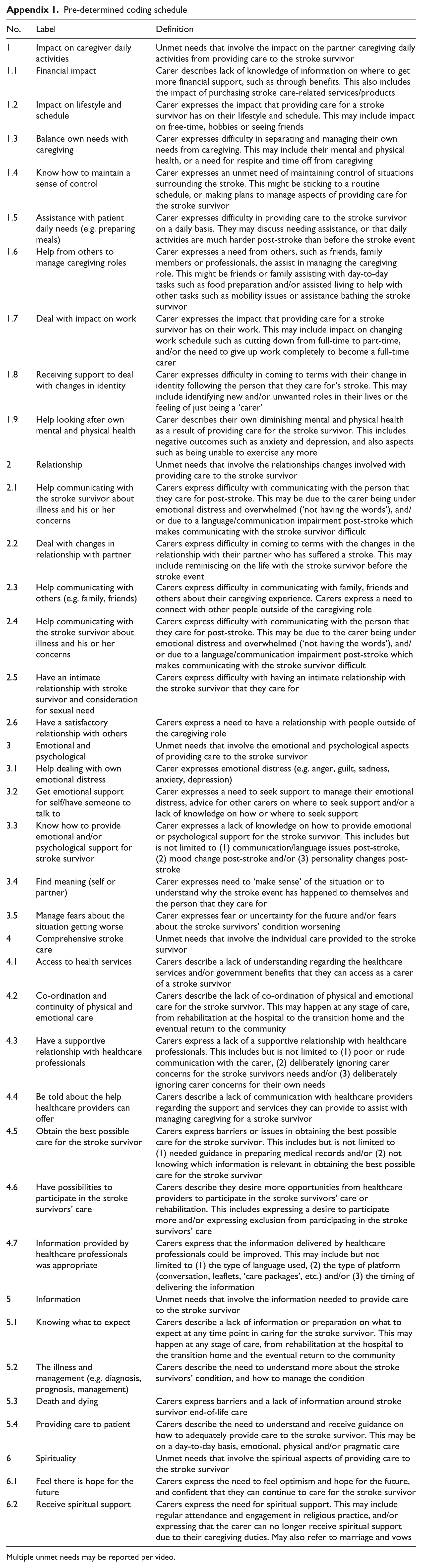
Pre-determined coding schedule
| No. | Label | Definition |
|---|---|---|
| 1 | Impact on caregiver daily activities | Unmet needs that involve the impact on the partner caregiving daily activities from providing care to the stroke survivor |
| 1.1 | Financial impact | Carer describes lack of knowledge of information on where to get more financial support, such as through benefits. This also includes the impact of purchasing stroke care-related services/products |
| 1.2 | Impact on lifestyle and schedule | Carer expresses the impact that providing care for a stroke survivor has on their lifestyle and schedule. This may include impact on free-time, hobbies or seeing friends |
| 1.3 | Balance own needs with caregiving | Carer expresses difficulty in separating and managing their own needs from caregiving. This may include their mental and physical health, or a need for respite and time off from caregiving |
| 1.4 | Know how to maintain a sense of control | Carer expresses an unmet need of maintaining control of situations surrounding the stroke. This might be sticking to a routine schedule, or making plans to manage aspects of providing care for the stroke survivor |
| 1.5 | Assistance with patient daily needs (e.g. preparing meals) | Carer expresses difficulty in providing care to the stroke survivor on a daily basis. They may discuss needing assistance, or that daily activities are much harder post-stroke than before the stroke event |
| 1.6 | Help from others to manage caregiving roles | Carer expresses a need from others, such as friends, family members or professionals, the assist in managing the caregiving role. This might be friends or family assisting with day-to-day tasks such as food preparation and/or assisted living to help with other tasks such as mobility issues or assistance bathing the stroke survivor |
| 1.7 | Deal with impact on work | Carer expresses the impact that providing care for a stroke survivor has on their work. This may include impact on changing work schedule such as cutting down from full-time to part-time, and/or the need to give up work completely to become a full-time carer |
| 1.8 | Receiving support to deal with changes in identity | Carer expresses difficulty in coming to terms with their change in identity following the person that they care for’s stroke. This may include identifying new and/or unwanted roles in their lives or the feeling of just being a ‘carer’ |
| 1.9 | Help looking after own mental and physical health | Carer describes their own diminishing mental and physical health as a result of providing care for the stroke survivor. This includes negative outcomes such as anxiety and depression, and also aspects such as being unable to exercise any more |
| 2 | Relationship | Unmet needs that involve the relationships changes involved with providing care to the stroke survivor |
| 2.1 | Help communicating with the stroke survivor about illness and his or her concerns | Carers express difficulty with communicating with the person that they care for post-stroke. This may be due to the carer being under emotional distress and overwhelmed (‘not having the words’), and/or due to a language/communication impairment post-stroke which makes communicating with the stroke survivor difficult |
| 2.2 | Deal with changes in relationship with partner | Carers express difficulty in coming to terms with the changes in the relationship with their partner who has suffered a stroke. This may include reminiscing on the life with the stroke survivor before the stroke event |
| 2.3 | Help communicating with others (e.g. family, friends) | Carers express difficulty in communicating with family, friends and others about their caregiving experience. Carers express a need to connect with other people outside of the caregiving role |
| 2.4 | Help communicating with the stroke survivor about illness and his or her concerns | Carers express difficulty with communicating with the person that they care for post-stroke. This may be due to the carer being under emotional distress and overwhelmed (‘not having the words’), and/or due to a language/communication impairment post-stroke which makes communicating with the stroke survivor difficult |
| 2.5 | Have an intimate relationship with stroke survivor and consideration for sexual need | Carers express difficulty with having an intimate relationship with the stroke survivor that they care for |
| 2.6 | Have a satisfactory relationship with others | Carers express a need to have a relationship with people outside of the caregiving role |
| 3 | Emotional and psychological | Unmet needs that involve the emotional and psychological aspects of providing care to the stroke survivor |
| 3.1 | Help dealing with own emotional distress | Carer expresses emotional distress (e.g. anger, guilt, sadness, anxiety, depression) |
| 3.2 | Get emotional support for self/have someone to talk to | Carer expresses a need to seek support to manage their emotional distress, advice for other carers on where to seek support and/or a lack of knowledge on how or where to seek support |
| 3.3 | Know how to provide emotional and/or psychological support for stroke survivor | Carer expresses a lack of knowledge on how to provide emotional or psychological support for the stroke survivor. This includes but is not limited to (1) communication/language issues post-stroke, (2) mood change post-stroke and/or (3) personality changes post-stroke |
| 3.4 | Find meaning (self or partner) | Carer expresses need to ‘make sense’ of the situation or to understand why the stroke event has happened to themselves and the person that they care for |
| 3.5 | Manage fears about the situation getting worse | Carer expresses fear or uncertainty for the future and/or fears about the stroke survivors’ condition worsening |
| 4 | Comprehensive stroke care | Unmet needs that involve the individual care provided to the stroke survivor |
| 4.1 | Access to health services | Carers describe a lack of understanding regarding the healthcare services and/or government benefits that they can access as a carer of a stroke survivor |
| 4.2 | Co-ordination and continuity of physical and emotional care | Carers describe the lack of co-ordination of physical and emotional care for the stroke survivor. This may happen at any stage of care, from rehabilitation at the hospital to the transition home and the eventual return to the community |
| 4.3 | Have a supportive relationship with healthcare professionals | Carers express a lack of a supportive relationship with healthcare professionals. This includes but is not limited to (1) poor or rude communication with the carer, (2) deliberately ignoring carer concerns for the stroke survivors needs and/or (3) deliberately ignoring carer concerns for their own needs |
| 4.4 | Be told about the help healthcare providers can offer | Carers describe a lack of communication with healthcare providers regarding the support and services they can provide to assist with managing caregiving for a stroke survivor |
| 4.5 | Obtain the best possible care for the stroke survivor | Carers express barriers or issues in obtaining the best possible care for the stroke survivor. This includes but is not limited to (1) needed guidance in preparing medical records and/or (2) not knowing which information is relevant in obtaining the best possible care for the stroke survivor |
| 4.6 | Have possibilities to participate in the stroke survivors’ care | Carers describe they desire more opportunities from healthcare providers to participate in the stroke survivors’ care or rehabilitation. This includes expressing a desire to participate more and/or expressing exclusion from participating in the stroke survivors’ care |
| 4.7 | Information provided by healthcare professionals was appropriate | Carers express that the information delivered by healthcare professionals could be improved. This may include but not limited to (1) the type of language used, (2) the type of platform (conversation, leaflets, ‘care packages’, etc.) and/or (3) the timing of delivering the information |
| 5 | Information | Unmet needs that involve the information needed to provide care to the stroke survivor |
| 5.1 | Knowing what to expect | Carers describe a lack of information or preparation on what to expect at any time point in caring for the stroke survivor. This may happen at any stage of care, from rehabilitation at the hospital to the transition home and the eventual return to the community |
| 5.2 | The illness and management (e.g. diagnosis, prognosis, management) | Carers describe the need to understand more about the stroke survivors’ condition, and how to manage the condition |
| 5.3 | Death and dying | Carers express barriers and a lack of information around stroke survivor end-of-life care |
| 5.4 | Providing care to patient | Carers describe the need to understand and receive guidance on how to adequately provide care to the stroke survivor. This may be on a day-to-day basis, emotional, physical and/or pragmatic care |
| 6 | Spirituality | Unmet needs that involve the spiritual aspects of providing care to the stroke survivor |
| 6.1 | Feel there is hope for the future | Carers express the need to feel optimism and hope for the future, and confident that they can continue to care for the stroke survivor |
| 6.2 | Receive spiritual support | Carers express the need for spiritual support. This may include regular attendance and engagement in religious practice, and/or expressing that the carer can no longer receive spiritual support due to their caregiving duties. May also refer to marriage and vows |
Multiple unmet needs may be reported per video.
Author’s note
Ratika Kumar is now affiliated with University of Newcastle, Callaghan, NSW, Australia and Neil J Spratt is also affiliated with Priority Research Centre for Stroke and Brain Injury, Hunter Medical Research Institute, New Lambton Heights, NSW, Australia and Department of Neurology, John Hunter Hospital, Hunter New England Local Health District, New Lambton Heights, NSW, Australia.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: A.M.J.D. is supported by the Research Training Program (RTP), University of Newcastle PhD Scholarship and Hunter Medical Research Institute/Emlyn and Jennie Thomas Postgraduate Medical Research Scholarship. A.L.B. is supported by the NHMRC Senior Research Fellowship Grant. N.J.S. was the recipient of a co-funded National Health and Medical Research Council/National Heart Foundation Career Development/Future Leader Fellowship (APPS1110629/100827). R.K. is funded by the Australian Government Research Training Program (RTP) scholarship. B.B. is supported by the University of Newcastle, Faculty of Health and Medicine Gladys M Brawn Career Development Fellowship.