
Abstract
The objective of this study was to perform a systematic review and meta-analysis comparing the effect of telehealth interventions to usual care for cancer survivors’ quality of life. A comprehensive search of four different databases was conducted. Manuscripts were included if they assessed telehealth interventions and usual care for adult cancer survivors and reported a measure of quality of life. Pooled random effects models were used to calculate overall mean effects for quality of life pre- and post-intervention. Eleven articles fit all systematic review and meta-analysis criteria. Initial analyses indicated that telehealth interventions demonstrated large improvements compared with usual care in quality of life measures (Δ = 0.750, p = 0.007), albeit with substantial heterogeneity. Upon further analysis and outlier removal, telehealth interventions demonstrated significant improvements in quality of life compared with usual care (Δ = 0.141–0.144, p < 0.05). The results of the systematic review with meta-analysis indicate that supplementary interventions through telehealth may have a positive impact on quality of life compared with in-person usual care.
Introduction
As of January 2016, there were an estimated 15.5 million cancer survivors in the United States and, for them, the transition from treatment to aftercare is a difficult process.1,2 Transition of care requires changes in the patient’s self-care, as well as continued coordination of ongoing medical care. 3 Advances in treatment delivery as well as the increasing proportion of the US population over the age of 65 years will increase the need for transitioning services and supportive care for cancer survivors.1,4,5
The diagnosis and treatment of cancer leads to psychological and physical side effects. 6 In conjunction with physical symptoms, psychological symptoms such as anxiety and depression can be a challenge for treating clinicians.2,6–9 Depression and anxiety are associated with decreased compliance with treatment, as well as low adherence to guidelines for healthy diet, nutrition, and physical activity.5,10 Likewise, cancer survivors suffer from increased nervousness and fear in addition to cognitive and functional impairments, leading to reduced quality of life (QOL).3–6,8 By providing patients with education and healthy lifestyle programs, clinicians can help cancer survivors decrease the uncertainty and physical and psychological distress associated with their disease.6,10
Cancer survivors post-treatment continue to have unmet needs, and despite evidence showing benefits from supportive care, referral rates are low.8,11 Cancer survivors may face significant barriers such as poor health and family responsibilities that prevent travel to centralized healthcare facilities. 12 For rural residents and remote communities, acquiring and retaining adequate workforce is a barrier for accessing health care for many patients. This is not only limited to rural areas, but workforce shortage areas in many urban areas. 13 One potential solution for gaining access to specialty care is through the use of telehealth technology.7,11–14
The terms “telehealth” or “telemedicine” are used interchangeably. Telemedicine predominantly refers to the diagnosis and monitoring technology used in provider-patient contacts, whereas telehealth may also include management, education, and other allied health care services. 15 Telehealth technologies, such as telephone, videoconferencing, and Internet-based interventions, have the capability of bringing services into the survivors’ home and bolster the management of symptoms without needing to have direct physical contact with hospital or clinic services.16,17 Telehealth facilitates transitioning of post-cancer treatment care from hospitals to the home and community and empowers survivors and their families or caregivers to play a more active role in managing their care.8,10,11,18
The purpose of this systematic review with meta-analysis was to examine the effect that telehealth interventions providing emotional support or self-management of symptoms have on cancer survivors’ QOL. Emotional support consisting of counseling or psychiatric consultations focused on relieving the psychological symptoms, that is, anxiety or depression. Self-management interventions relate to the physical and functional issues that maybe present after treatment. This systematic review examined the overall effect of telehealth technology to support cancer survivors in the management of their symptoms in comparison to in-person usual care (UC). We were interested in determining whether interventions utilizing telehealth-delivered support were more effective in improving QOL versus UC from baseline until the end of the intervention period.
Methods
This systematic review and meta-analysis were guided by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement. 19
Data acquisition
An electronic database search was conducted from inception to 31 October 2017 by two of the coauthors (J.L.L. and A.B.R.) using the following databases: National Library of Medicine Catalog (Medline/PubMed), the Cumulative Index to Nursing and Allied Health Literature (CINAHL), and Ebsco Health (Medline complete). The initial key-term search consisted of the following: “telehealth OR telemedicine OR videoconferencing OR email OR telephone OR web-based” AND “Cancer” AND “quality of life OR assessment.” After the initial search, article titles and abstracts were inspected for relevance to the inclusion and exclusion criteria, followed by obtaining full-texts for identified manuscripts. Manuscripts were then further inspected for inclusion and exclusion criteria post-retrieval. Reference lists of full-text manuscripts were then hand-searched and cross-referenced for potentially relevant papers. Another separate search on the Cochrane Library was conducted for systematic reviews containing similar content. Relevant systematic reviews were then obtained and cross-referenced for additional manuscripts missed during the original search. Consensus among all the authors was then sought for an article’s final inclusion in the meta-analysis.
Inclusion and exclusion criteria
All manuscripts included in the systematic review and meta-analysis must have been published in a peer-reviewed journal in English and met the following inclusion criteria: (1) cancer survivors post-initial cancer treatment included must have had any form of cancer and completed initial active treatment (i.e. not undergoing active chemotherapy and/or radiation, or post-surgery for initial cancer diagnosis); (2) survivors must have been adults, 18 years of age or older; (3) interventions must have used some form of telehealth/telemedicine, including but not limited to telephone calls and/or web-based interventions; (4) the focus of each intervention must have been on emotional support or self-management of symptoms through counseling, educational intervention, or tele-rehabilitation; (5) studies must have used a measurable global QOL scale or questionnaire; and (6) studies used a randomized control trial (RCT) methodology, controls receiving UC. Studies were excluded if (1) they assessed the efficacy of palliative care, (2) the patients were undergoing active cancer treatment, or (3) they combined in-person/mail and telehealth in the same intervention.
Data extraction and analysis
For the systematic review portion of this study, descriptive data were extracted from each of the included articles pertaining to their methodology and results. The Physiotherapy Evidence database (PEDro) scale was used to determine the quality of the articles, based on the reported study protocols and results.20,21 The PEDro scale is used for RCT studies to determine internal validity by utilizing a list of 11 methodological components that affect the quality of the methodology. 21 The higher the score, the greater the methodological quality.20,21
Numerical data extracted for the meta-analysis included sample sizes, QOL measures means and standard deviations (SDs) from baseline and post-intervention, as well as effect sizes for each study whenever data were available.
After the collection of study data, standardized mean differences between baseline and post-test for telehealth interventions versus UC were calculated while adjusting for small sample bias (Hedges g). 22 A random effects model was used to determine an overall mean effect size (∆). The random effects model was utilized due to the uncertainty of evaluating a homogeneous population. 23 Heterogeneity was assessed via I2 and Q-statistics. The fail-safe N was also analyzed to determine the impact of bias from unpublished studies on the mean effect size. 23 All effect-size data and heterogeneity statistics were calculated with the Comprehensive Meta-Analysis (V3.3.070, Biostat, Inc., Englewood, NJ, US) software package. Effect size data were interpreted as small = 0.1–0.3, moderate = 0.3–0.5, and large effects = >0.5. 24
Results
Figure 1 is a flow diagram of the article selection process and provides details of the comprehensive search completed as well as the articles included and excluded at each stage. Our initial search for articles using our search terms within the designated literature databases yielded a total of 8930 articles, 4583 of those were duplicates. Eleven articles (Table 1) ultimately fit all systematic review and meta-analysis criteria.
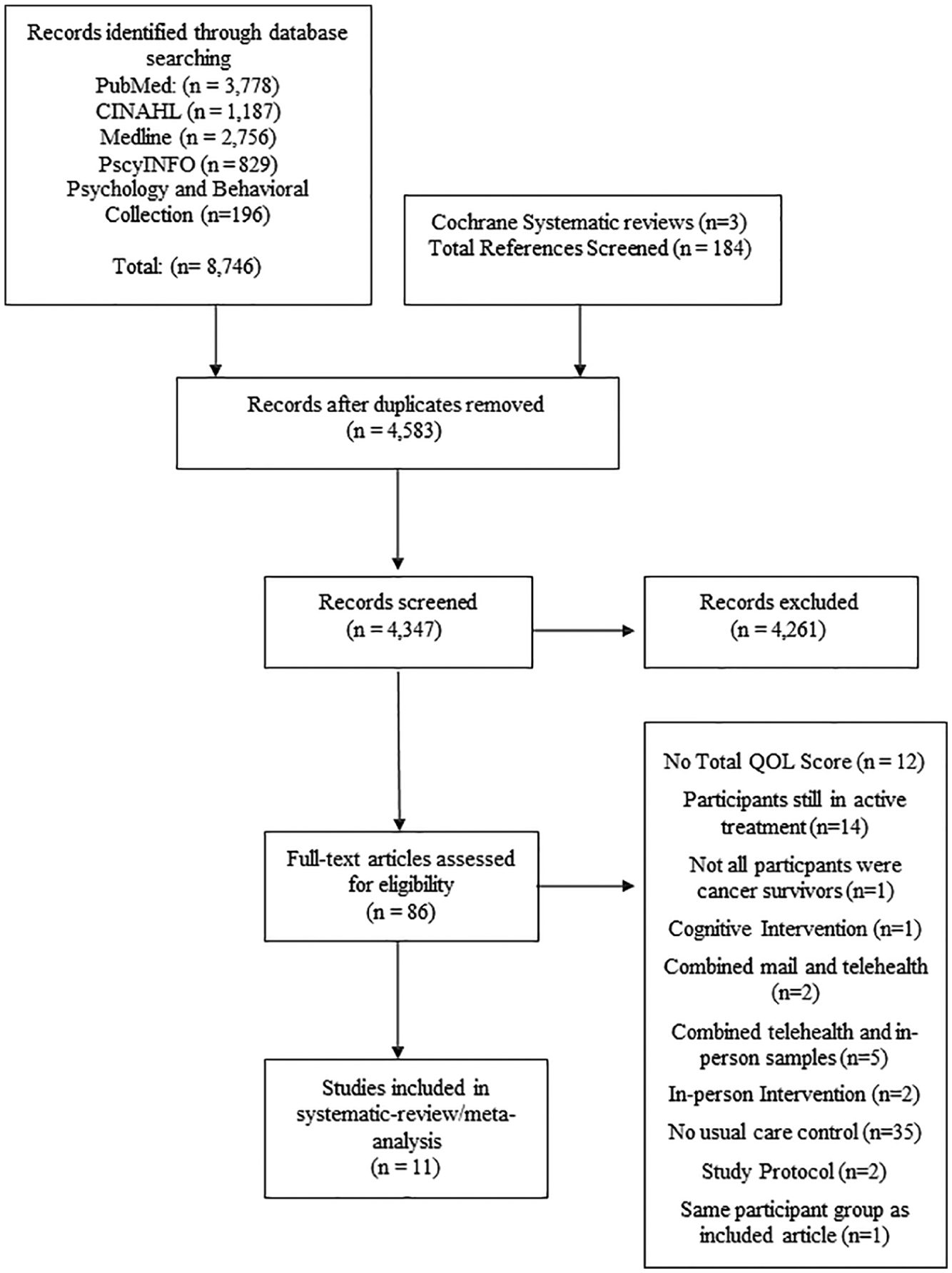
Article selection flow diagram and number of articles reviewed.
Summary of evidence for each individual study included resulting from systematic search of the literature.
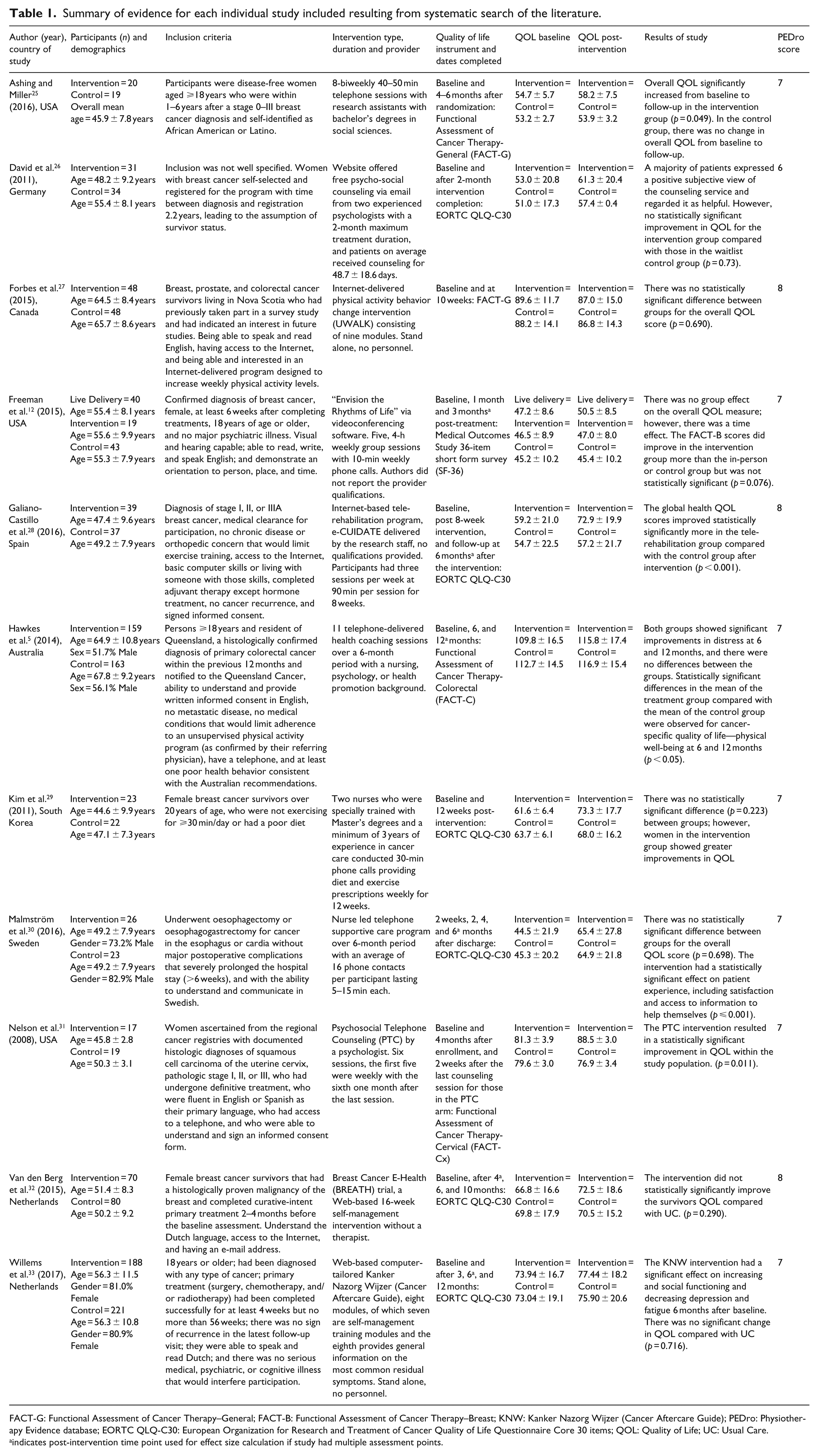
FACT-G: Functional Assessment of Cancer Therapy–General; FACT-B: Functional Assessment of Cancer Therapy–Breast; KNW: Kanker Nazorg Wijzer (Cancer Aftercare Guide); PEDro: Physiotherapy Evidence database; EORTC QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 items; QOL: Quality of Life; UC: Usual Care.
indicates post-intervention time point used for effect size calculation if study had multiple assessment points.
Of the eleven studies included, six (55%) were of breast cancer survivors, one (9%) oesophageal cancer survivors, one (9%) colorectal cancer survivors, one (9%) of cervical cancer survivors, and two (18%) included cancer survivors of multiple forms of cancer. Five of the eleven (45%) studies utilized telephone interventions, one (9%) a videoconferencing intervention technique, one (9%) an email-based counseling, three (27%) a web-based self-management intervention, and one (9%) an Internet-based tele-rehabilitation program. The length of time from baseline to the end of the intervention assessment ranged 2–12 months, with the majority (6/11) of the articles using 6 months or greater as the final assessment. The total patients from these studies were 1349 cancer survivors, with 709 survivors in the control arm of the study and 640 survivors in the intervention arm. The average age range was 46–66 years, with the overall average for the combined studies being 55 years. Due to 7/11 studies dealing with predominantly female cancer types (breast and cervical), the majority of the patients (75%) were female. The average PEDro score across studies was 7.0 ± 1.0, indicating moderate to high methodological quality across the included studies.
Eight of eleven articles did not show a statistically significant improvement in the QOL assessment scores for survivors in the intervention compared with the control groups from baseline to end of intervention. David et al. 26 found no significant differences in change of mean QOL between those who participated in the free psycho-social counseling email group and those who were on the waitlist control. Forbes et al. 27 saw decreases in overall QOL for both the web-based intervention and UC control groups, with no significant difference in change between the groups. Freeman et al. 12 did not find significant differences for the breast cancer survivors in the intervention arm compared with those in the wait list or live delivery arm. However, there were significant increases in QOL (⩾3 points) for both those in the videoconferencing telehealth and live delivery intervention groups compared with the control group. The telehealth delivered program showed the greatest improvement in QOL of 5.12 points, compared with the same program given in-person, which showed an increase of 3.55 points from baseline, and the waitlist had a slight increase of 2.4 points from baseline to the 3-month post-intervention assessment. 12 Freeman et al. 12 noted in their study limitations the differences between sample sizes in each group may have led to the variability in the increase in QOL scores, as the telemedicine delivery group was just under half the size as the in-person delivery and control groups.
Kim et al. 29 did not find a statistically significant difference (p = 0.223) in QOL between participants in a telephone intervention group and a UC control group. Although not statistically significant, the intervention group had a larger increase of 11.7 units compared with a 4.3 units for the control. 29 Similarly, Malmström et al. 30 did not find a significant difference (p = 0.698) in QOL between the change in means of the intervention and control oesophageal cancer survivor groups. This study utilized a nurse-led telephone supportive care program with the final assessment at 6 months after starting the intervention. The intervention did have significant effects on the survivors’ experience in the intervention group compared with the control group, including information about “things to do to help yourself” (p = 0.001), written information (p < 0.001), and the global information score (p < 0.001). 30 Hawkes et al. 5 also found no significant change in QOL for colorectal survivors when comparing those in UC to those in a telephone health coaching program. Although both groups showed improvement in QOL over time, there was no difference between the two groups at 6 months or 12 months. However, there were significant increases in the differences of the mean of the treatment group compared with the mean of the control group in the physical well-being category of the QOL assessment (p < 0.05) at both assessment time points from baseline. 5
In a study using the Breast Cancer E-Health (BREATH) trial, a web-based self-management intervention, Van den Berg et al. 32 determined there was no significant difference (p = 0.290) in the effect of the intervention on the mean QOL scores when comparing those who received the intervention compared with those receiving UC. Willems et al. 33 utilized a web-based self-management intervention which consisted of informational modules. Although overall QOL was not significantly improved (p = 0.716), there were significant improvements in the intervention participants emotional functioning, social functioning, depression, and fatigue when compared with their UC control counterparts. 33
Three of eleven studies found significant changes in the mean score of the QOL of those within a telehealth intervention compared with those in UC. Nelson et al. 31 utilized telephone counseling as the intervention for uterine cervix cancer survivors and compared that to UC, measuring mean QOL at baseline and 2 weeks after the last counseling session. The intervention group of cancer survivors saw an average increase in their overall QOL score of 6.7 points, while the control group had no improvement. The difference in the baseline mean QOL to the mean QOL post-intervention was significant (p = 0.011) comparing those in the intervention group to those in the control group. 31 Ashing and Miller 25 found a significant difference in overall QOL from baseline to end of intervention timeframe (4–6 months) for breast cancer survivors in their telephone intervention compared with those in UC (p = 0.049). Galiano-Castillo et al. utilized an Internet-based tele-rehabilitation program called e-CUIDATE and assessed patients QOL at baseline and follow-up at 6 months after intervention. The change in overall health QOL was statistically significant when comparing the UC control with those in the program (p < 0.001). 28
In total, 11 individual effect sizes were calculated for the mean differences in QOL from baseline to post-intervention comparing telehealth intervention group to UC control. The distribution for all unweighted effect sizes calculated are displayed on the upper forest plot in Figure 2.
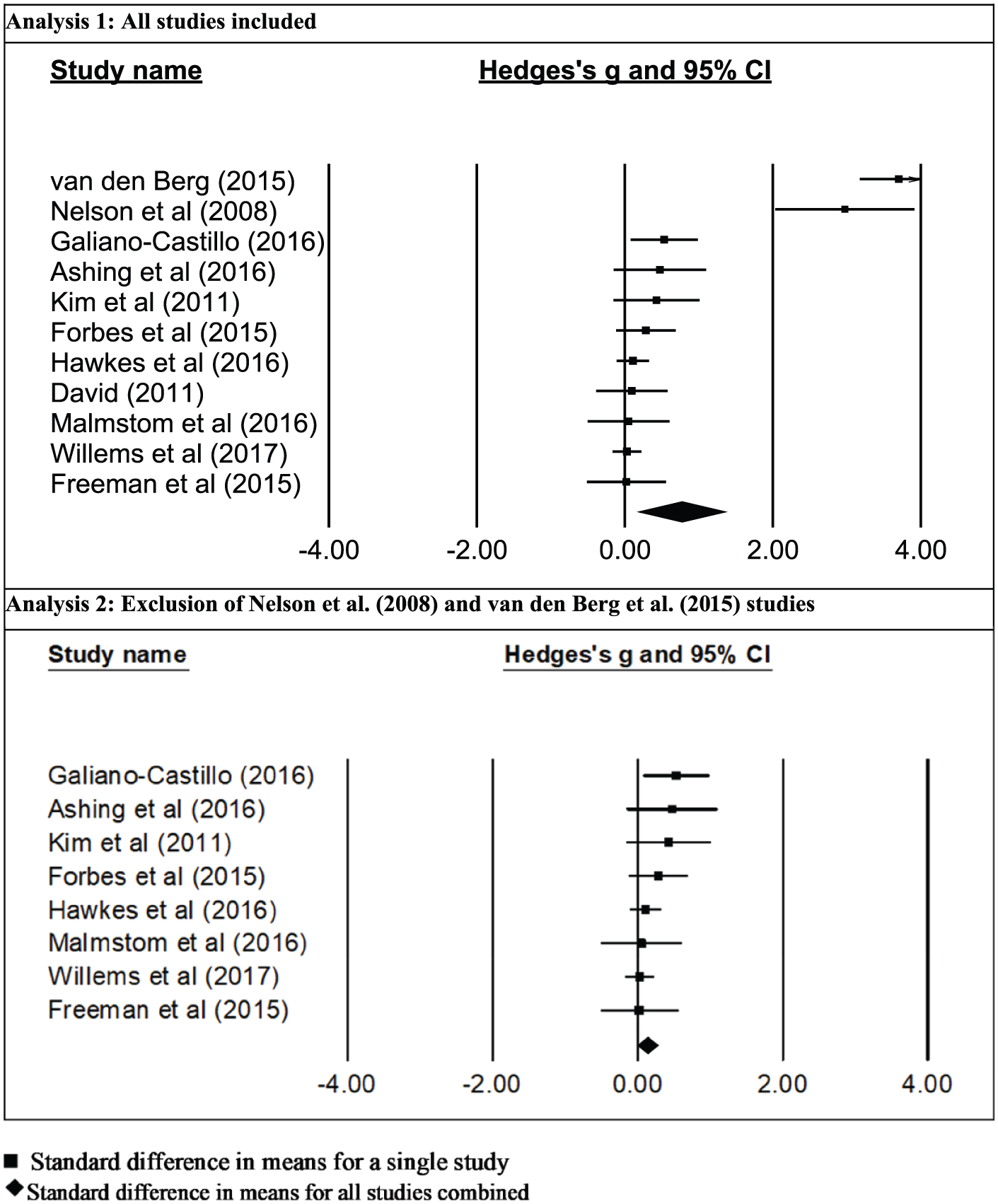
Forrest plot of Hedge’s g and the 95% confidence interval (CI) by name of study. The symbol “■” denotes standard difference in means for a single study and “◆” denotes standard difference in means for all studies combined.
The summary statistics for the mean effect sizes for telehealth and UC with their 95 percent confidence intervals, heterogeneity statistics, and fail-safe N calculations are reported in Table 2 as Analysis 1. There was a statistically significant large mean effect compared with baseline across the included studies (Δ = 0.750, p = 0.007). However, when assessing publication bias, there were several outliers in the homogeneity of studies (Figure 3). The two articles leading to increased heterogeneity of the mean effect were Nelson et al. 31 and Van den Berg et al.
Summary statistics for telehealth intervention and usual care across all included studies.
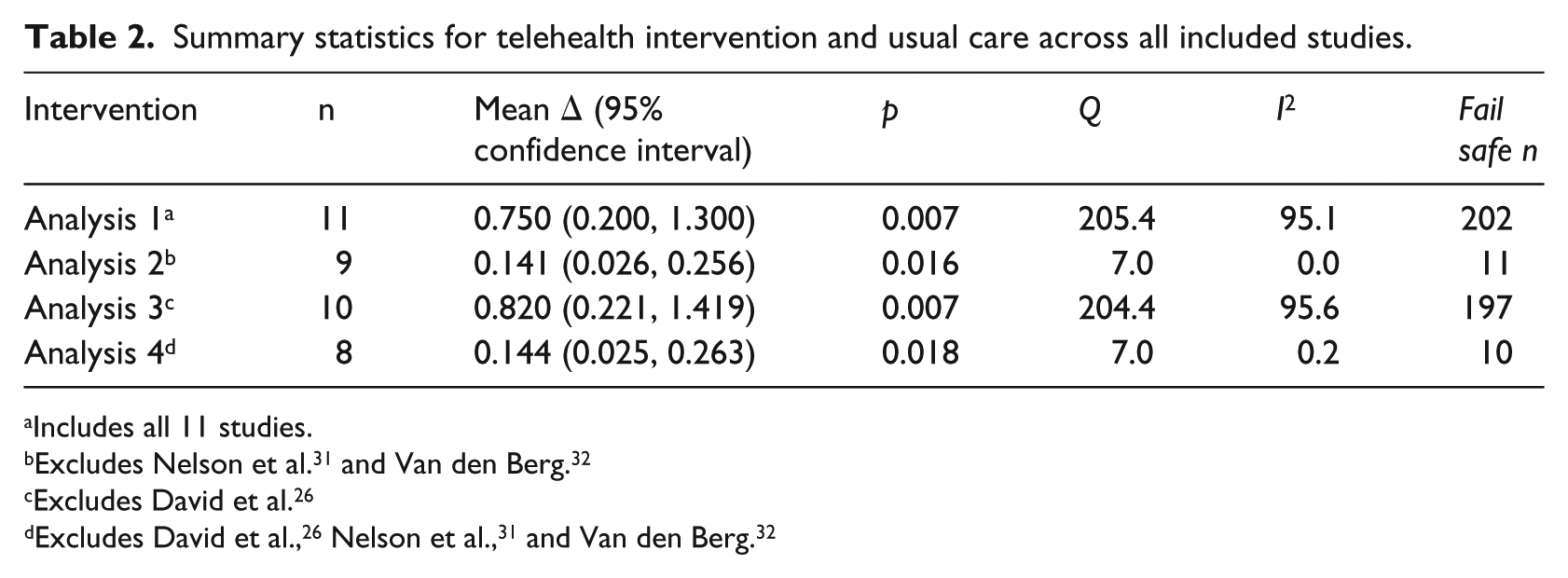
Includes all 11 studies.
Excludes David et al. 26
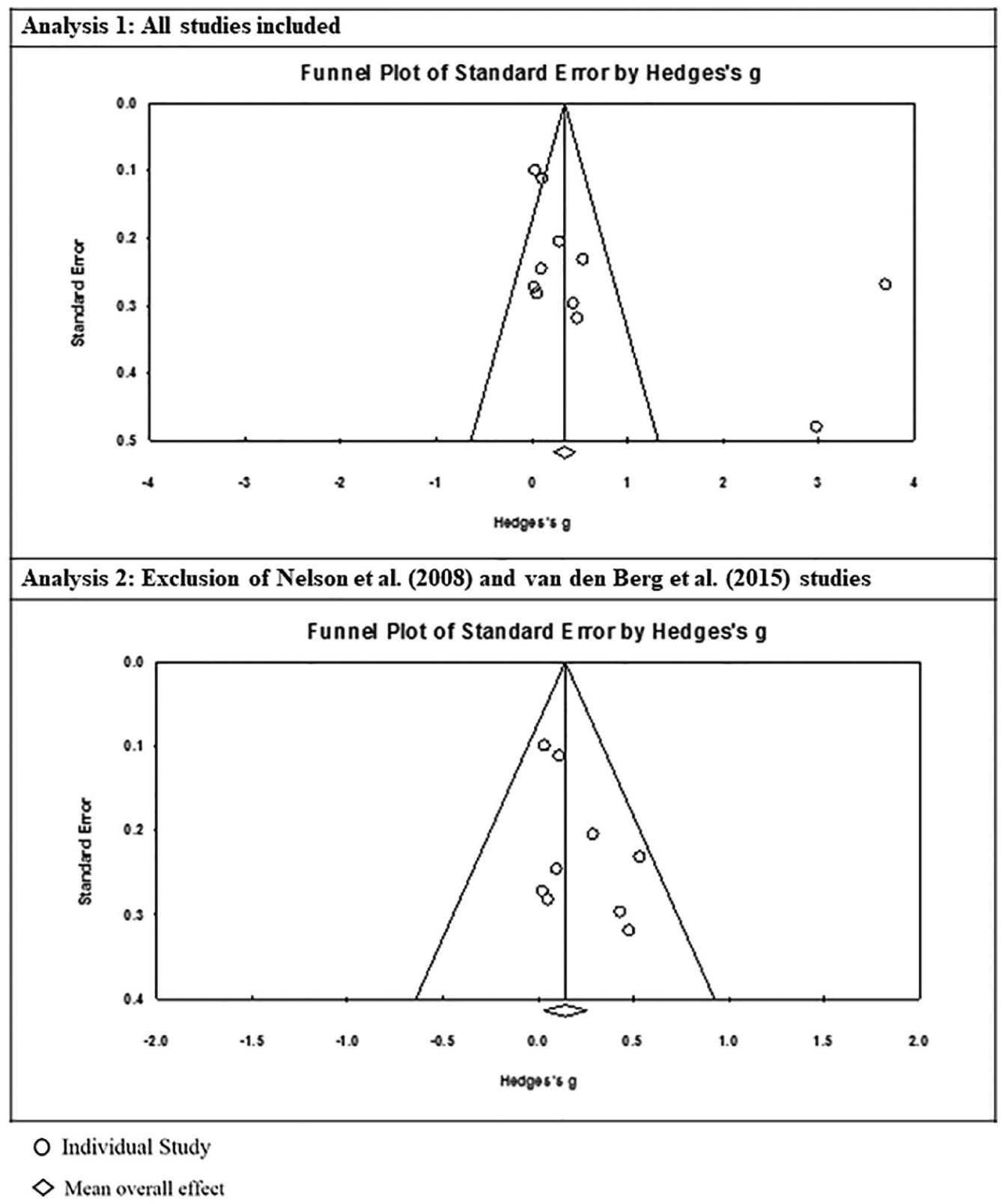
Funnel plots of the individual study effect sizes plotted against the standard error. The symbol “○” denotes individual study and “◇” denotes mean overall effect.
In the lower half of Figure 2, the distribution for all unweighted effect sizes calculated are displayed in a forest plot, excluding the Nelson et al. 31 and Van den Berg et al. articles. The mean effect was still significant (p = 0.016) but the effect size was much smaller than in the first model (Δ = 0.141). The summary statistics are reported in Table 2 as Analysis 2. Figure 3 shows the reassessment of publication bias and the overall homogeneity of the studies after exclusion of the outlier.
Both analysis models described above were run without the David et al. articles, due to a vague description of the population included in this study. This additional analysis was to determine if this study had a major effect on the intervention compared with UC. With all 10 articles in the analysis, excluding David et al., there was a statistically significant large, mean effect (Δ
Six of the articles focused on breast cancer and five on other forms of cancer or a mix of cancer types. A sub-analysis demonstrated significant differences between the two groups mean effect with cancers other than breast cancer showing a statistically significant moderate effect (breast cancer Δ = 0.876, p = 0.159; other cancer Δ = 0.475, p = 0.047). In the case of this analysis, cancer type does appear to be a factor affecting the mean effect outcome.
Another sub-analysis by technology type was conducted where we compared the five telephone-based studies to the seven studies using web-based technology. The web-based programs did not have a significant mean effect (mean ∆= 0.769, p = 0.107), but those in the telephone group (mean ∆= 0.703, p = 0.044) had a large mean effect that was significant in the change of QOL in telehealth intervention compared with UC. Technology type in the case of survivor programs does appear to be a significant factor in influencing outcomes.
Four of the articles used Functional Assessment of Cancer Therapy (FACT) assessments of QOL and six articles used the European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 items (EORTC-Q30) survey. Sub-analysis of these groups yielded similar results to the previous sub-analyses. The FACT assessment group had statistically significant large mean effect, where the EORTC-QLQ-C30 assessment group did not. The FACT assessment group had a mean effect size of 0.711 (p = 0.054) and the EORTC-QLQ-C30 group had a mean effect size of 0.801 (p = 0.115). This leads to the conclusion that the type of QOL assessment used could affect the outcome of this analysis. All statistics of the three sub-analyses are provided in Table 3, including mean effect, 95 percent confidence intervals, and p-values.
Summary statistics for sub-analysis of telehealth intervention versus usual care across all included studies.
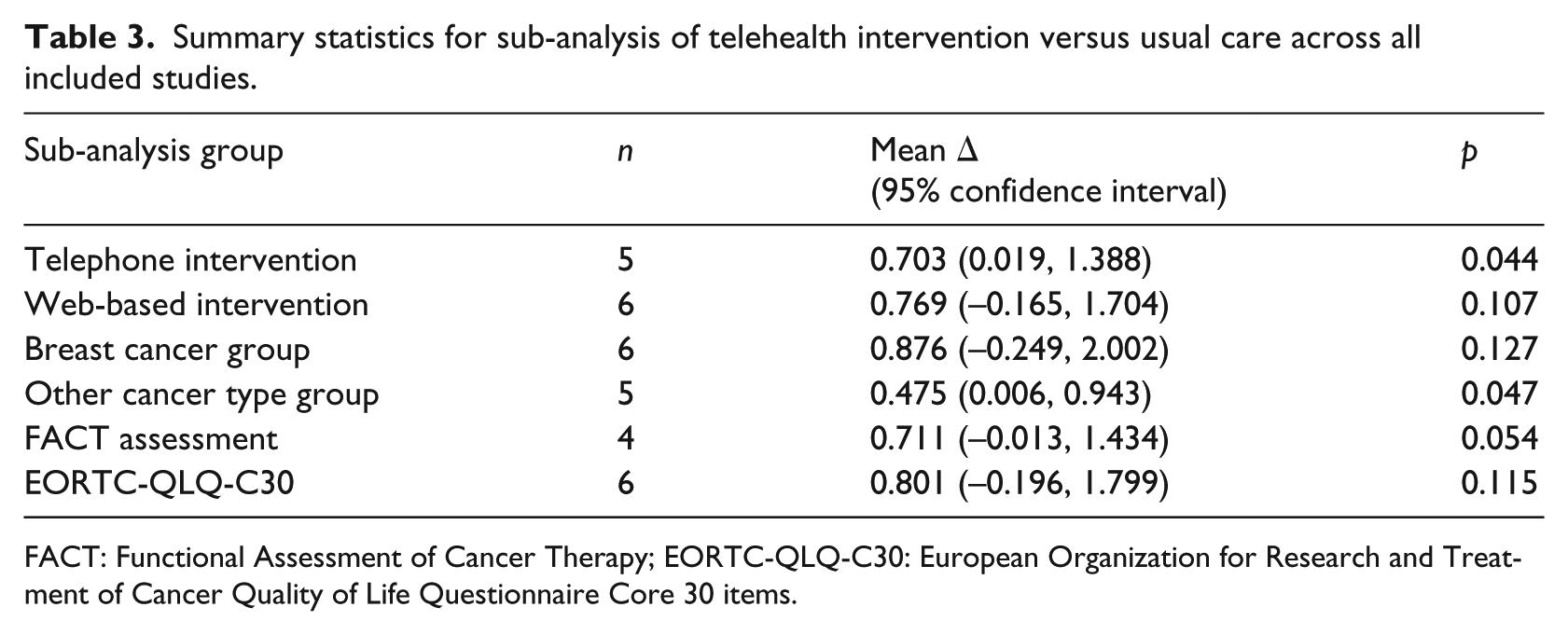
FACT: Functional Assessment of Cancer Therapy; EORTC-QLQ-C30: European Organization for Research and Treatment of Cancer Quality of Life Questionnaire Core 30 items.
Discussion
Our study performed a systematic review and meta-analysis of peer-reviewed studies that utilized telehealth interventions to improve the emotional support or self-management of symptoms of cancer survivors. Our analyses of included articles demonstrated a statistically significant, large effect of telehealth interventions on increasing survivors’ QOL compared with UC. Telehealth interventions that utilize additional support for cancer survivors appear to improve their QOL compared with the standard UC.
The studies in our meta-analysis and systematic review were relatively homogeneous as demonstrated by the funnel plots (Figure 3). Nelson et al. 31 was one of the outliers showing significantly improved effectiveness of telehealth versus UC, with survivors in the control group showing a decrease in QOL, the only study to show this effect. This was the only study analyzing patients with cervical cancer and had the youngest average age. 31 Van den Berg et al. was the second outlier, also showing a significant increase of telehealth intervention survivors’ QOL compared with less than a 10th of a point increase in QOL of UC survivors. However, the Van den Berg et al. 32 article was one of several breast cancer studies. These two studies use different telehealth technology (telephone and web-based), are differing cancer types, and are similar in age or gender to the majority of the other studies. It is possible that telehealth-based psychosocial treatments would vary in effectiveness across cancer diagnoses, age groups, and modality of delivery. Unfortunately, there has been insufficient research to demonstrate this.
These findings are somewhat in contrast to a systematic review and meta-analysis of cancer patients undergoing treatment that did not show significant effect of telehealth support interventions on patients’ QOL compared with UC. 34 This may be due to the differences in survivors compared with their counterparts still receiving cancer therapies, which effect each patient differently and can cause multiple issues, including physical, functional, and psychosocial symptoms and complications.16,35–39 Patients may have differing physical and psychological symptoms while in treatment compared with after completing active treatment. We also chose to focus on overall QOL compared with more specific elements of QOL, because, as our health care system transforms from an enterprise of “sick care” to one that emphasizes overall health and prevention, we sought to take a holistic approach. 40
Our inclusion criteria stated that all articles must have an overall QOL measurement. Of the 11 studies in our systematic review, the majority used the EORTC-QLQ-C30 survey. The European Organization for Research and Treatment of Cancer Quality of Life Questionnaire (EORTC QLQ-C30) is an integrated system for assessing the QOL of cancer patients participating in clinical trials and other types of research in which patient-reported outcomes are collected.41,42 The EORTC QLQ-C30 includes 9 multi-item scales, including functional, symptom, and global health scales. There are 5 functional scales and six single symptom measures.41,42 All of the scales and single-item measures range in score from 0 to 100. A high scale score represents a higher global health status score equating to a higher QOL.41,42
Four articles utilized the FACT instrument, either the general or cancer-specific FACT instrument. Functional Assessment of Cancer Therapy–General (FACT-G) is a 27-item instrument that has subscale scores for physical, functional, social, emotional well-being, and satisfaction with treatment.43–46 Cancer-specific FACT scales include those questions that are in the FACT-G but have additional questions that are cancer specific, such as for colorectal cancer (Functional Assessment of Cancer Therapy-Colorectal (FACT-C)) and cervical cancer (Functional Assessment of Cancer Therapy-Cervical (FACT-Cx)). Freeman et al. 12 used the Medical Outcomes Study 36-item short form survey (SF-36). The SF-36 includes one multi-item scale that assesses eight health concepts: limitations in physical and social activities due to physical or emotional problems, limitations in usual role activities due to physical or emotional problems, bodily pain, general mental health (psychological distress and well-being), vitality (energy and fatigue), and general health perceptions. 47 Like the other QOL assessments in this meta-analysis, the SF-36 correlates higher scores with higher QOL.
Our sub-analysis of grouping studies based on differing characteristics yielded statistically significant results regarding the change in QOL of those in the intervention groups compared with those in the UC groups. Telephone-based interventions had a significant mean effect unlike the web-based programs. This could be associated with the ease of use with telephone over web-based interventions, and that the telephone interventions were usually more tailored to individual patient needs. Several of the web-based interventions (Forbes et al., 27 Van den Berg et al., 32 and Willems et al. 33 ) were stand-alone modules that were not tailored to the individual. Interventions that include more one on one interaction may be preferred by cancer survivors.
Although the majority of the studies evaluated telehealth interventions for breast cancer survivors, our sub-analysis did not find a significant effect of telehealth interventions on QOL compared with UC for breast cancer survivors. However, for the sub-analysis group which pooled the other forms of cancer there was a significant moderate effect. This suggests that telehealth interventions may provide better emotional and symptom support to specific cancer type survivors. This is important when creating telehealth programs and interventions for cancer survivors and who would benefit most from these types of interventions. It is critical to understand what works and for whom.
Our study found similar results to a recent meta-analysis of cancer patients in treatment that found the QOL assessment used made a significant difference in the mean effect of those in the telehealth intervention compared with those in UC. 34 Our study showed that the mean effect for the FACT assessment study group was significant, whereas using the EORTC-QLQ-C30 assessment did not yield a statistically significant effect on cancer survivors QOL. 34 The assessments were used with a variety of technology types and forms of cancer. This is interesting when attempting to compare studies using slightly different assessment techniques and if they are comparable given differences in measurements. There may need to be more research into the best form of assessing telehealth interventions for cancer survivors.
It is also important to note that there is a difference in statistically significant changes as opposed to clinical significance. Many of the studies included in this systematic review and meta-analysis did not show statistical significance in the overall QOL assessment; however, other study outcomes were significant such as satisfaction with care and physical-wellbeing perceptions. Hawkes et al. 5 found a statistically significant difference in the mean of the intervention group compared with control for the QOL subset physical well-being, but not overall QOL. David et al. 26 determined that, although there was no statistical difference in control and intervention groups, the survivors in the intervention found the counseling service helpful and regarded it as a positive in their lives. Similarly, Malmström et al. 30 found a statistically significant effect of telephone supportive care on patient experience, including satisfaction and access to information. Therefore, although some studies may not show a statistically significant effect in overall QOL, there are areas of a survivors’ life that are improved through the use of telehealth support programs. Likewise, studies have been conducted on the significance of a positive increase of overall QOL scores compared with negative and the meaning that has for cancer survivors. Survivors put larger weight on small positive gains in QOL and smaller weight to larger negative losses.48,49 Some research has attempted to determine a cut-off point for what is considered clinically significant change for QOL measures. Some suggest ranges of 5–10 for EORTC QLQ-C30 50 and 6.5 points for FACT-G. 51 Several have suggested proportions of change49,52 or 0.5 SD change as statistically significant.53,54 The general clinical significant is truly dependent on the patient’s perspective and the clinical benefit perceived by the patient and provider.48,52,55,56
We utilized the PEDro scale to determine the quality of the RCT studies, as noted in Table 1. All the studies fell in the range of 6–8 out of a total of 11 points. The majority were 7 points, with all studies unable or not providing information on blinding subjects, therapists, or assessors. Forbes et al., 27 Galiano-Castillo et al., 28 and Van den Berg et al. 32 were assessed slightly higher at 8 points, as these studies had concealed allocation, whereas the other six articles did not report this factor. David et al. 26 had the lowest quality score of 6, as the authors did not state thoroughly who was being included and excluded and for what reasons, contributing to the study’s relatively low PEDro score.
Conclusion
Study limitations
Our study should be interpreted in the context of certain limitations. Our meta-analysis had a small sample size of manuscripts and patient pools, and was limited to those published in English; therefore, we were unable to perform a complete moderator analysis to determine if alternative factors influenced the effectiveness of treatment delivery. Similarly, different cancers, stage of cancer, and treatment protocols may have varying impacts on QOL, which we were unable to fully explore due to the limited number of studies. Although we attempted to correct the heterogeneity of articles by excluding outliers, it did significantly affect the mean effect size. However, there was still significant effect in every analysis and some differences related to factors in the sub-analysis of differing groups.
Clinical implications
Our systematic review with meta-analysis demonstrated that supplementary interventions through telehealth might have a statistically significant positive impact on QOL scores relative to in-person UC. Some of the studies in this meta-analysis did see improvements in other areas such as depression, anxiety, and emotional, social, and physical well-being, even when overall QOL was not statistically significantly improved. The additional benefits of telehealth are increased access for rural patients and those who may struggle to get to in-person resources, as well as improving patient satisfaction.26,30,57,58 Our findings suggest more studies need to be conducted on the impact of telehealth interventions across different cancer diagnoses and delivery modalities, to gain better insight into the effectiveness these interventions may have on QOL for cancer survivors in all phases of survivorship.
Footnotes
Author’s note
Fernando A Wilson is now affiliated with University of Utah in Salt Lake City.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.