
Abstract
Different accident analytical approaches have been utilised in safety-critical industries for analysing accidents and formulating safety recommendations. This study presents a ‘health informatics’ case incident of a patient adversely affected due to a medication dosing error resulting from a combination of contributing factors including those relating to the Computerised Order Provider Entry System. A comparative study was carried out using selected accident analytical approaches: Human Factors and Classification System, System-Theoretic Accident Modelling and Processes and Accident Modelling. Each resulting output was compared using the model characteristic criteria developed by Underwood and Waterson. Safety recommendations developed based on the outputs from the models/methods were also compared for any similar findings. It was acknowledged that while accident models incorporating ‘systems thinking’ can prove to be beneficial for healthcare in providing insight on systemic factors, there is a need for improving the reliability and validity of these models. This particularly applies to Rasmussen’s Accident Modelling approach to be considered useful in the healthcare domain.
Keywords
Introduction
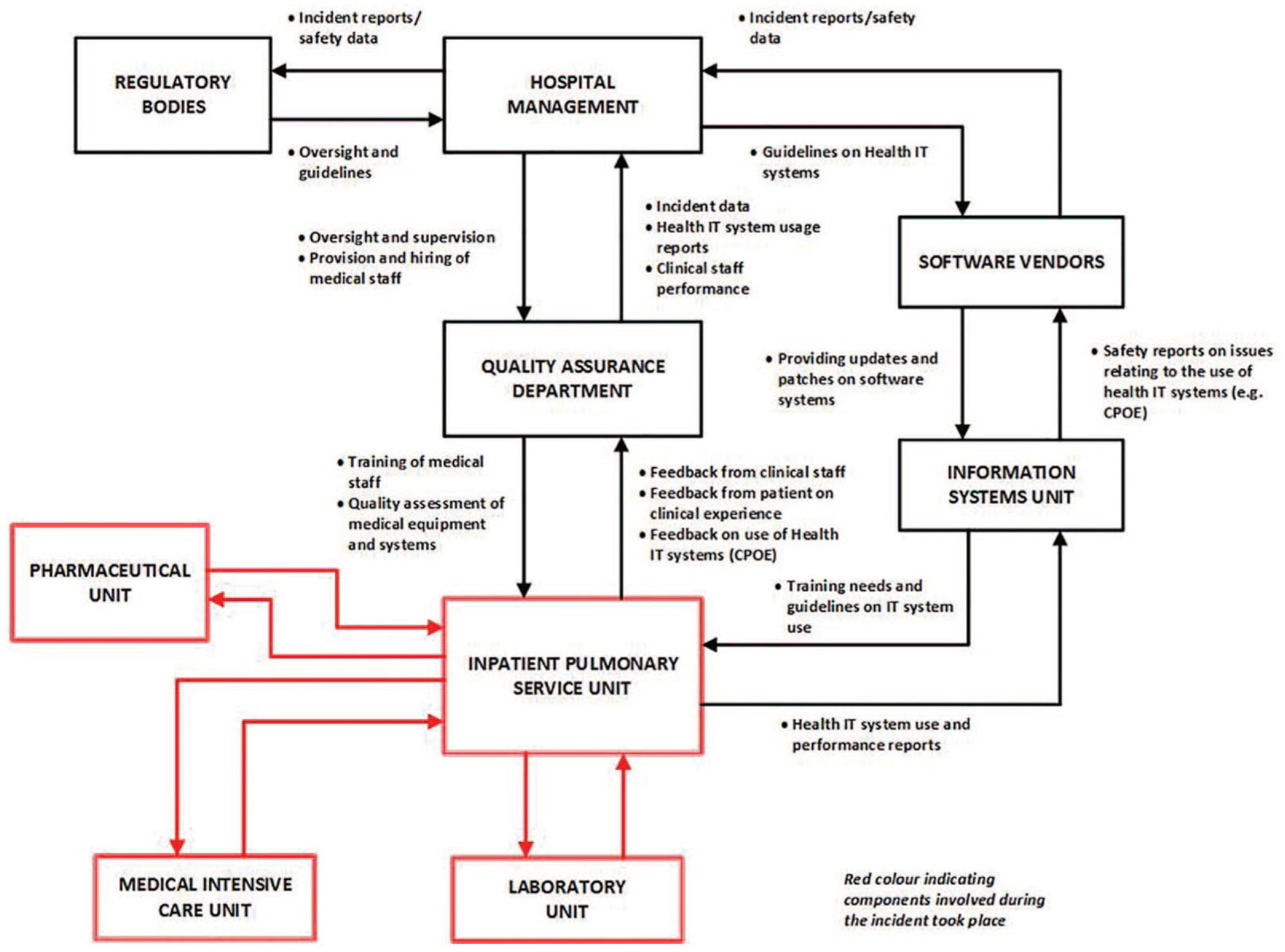
The healthcare system can be regarded both as a safety critical and a sociotechnical system consisting of the interconnection of people (users of health information technology (health IT) systems), technology (software/hardware), processes, organisation and the external environment (where policies are developed and enforced) 1 as shown in Figure 1.
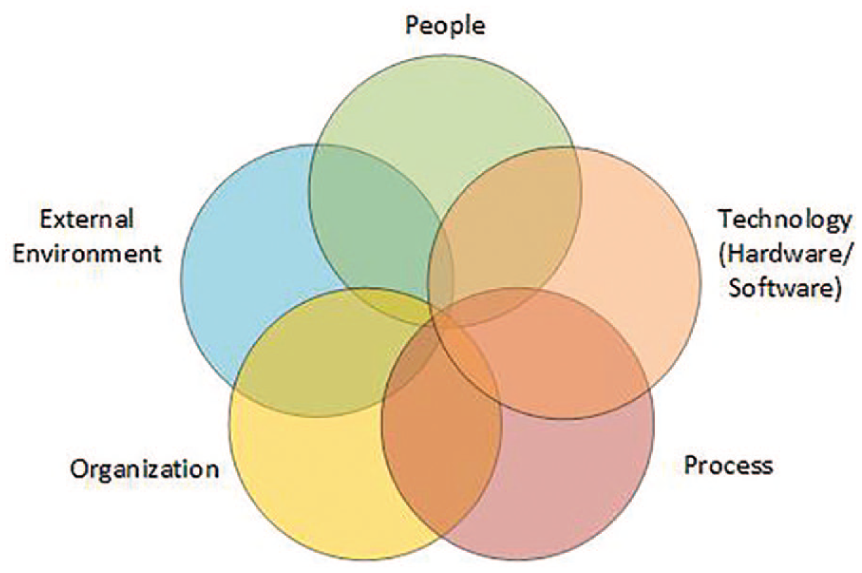
Sociotechnical system underlying health-IT related adverse events (adapted from Sittig and Singh 1 and Harrington et al., 2011).
Health IT broadly comprises of ‘all computer software used by health professionals and patients to support care’. 2 Its implementation has helped to reduce medical errors leading to patient harm and improve clinical processes, workflow and communication between clinicians for increased efficiency.3,4 Unfortunately, unintended consequences and new forms of errors resulting from using IT systems can adversely affect patient safety. 2 These consequences occur from interactions between operators and clinical IT systems contributing to the occurrence of such outcomes. Reasons behind any occurrences should not only focus on proximate causes but also existing latent conditions including design, use of health IT systems and existing policies within and outside the organisation. The Insititute of Medicine (IOM) also highlighted the need for improving patient safety by ensuring the safe use of health IT in the delivery of effective healthcare. 3
Different accident analytical approaches have been used in different safety-critical domains for investigating ‘why’ accidents occurred and developing effective countermeasures to improve safety.5,6 While approaches incorporating ‘systems thinking’ are considered the dominant paradigm for accident analysis, there has been a research gap in practically applying these approaches for incident analyses in healthcare systems. 6 Due to the growing awareness of the limitation of root cause analysis (RCA) techniques, there is a need for incorporating systemic approaches for accident analysis. This is especially very critical in being to investigate further into contributing factors relating to the use of health IT within a complex system like healthcare.
Objectives of study
The aim of this study was to determine which of the selected accident analytical approaches is the most practically suitable using a health IT–related case example. To achieve this, study objectives carried out include the following:
Comparing the resulting outputs from each accident causation model based on the usage characteristics criteria. 7
Comparing causes/contributing factors identified from the application of these approaches.
Comparing safety recommendations developed based on analyses.
Research methodology
A case study approach 8 was considered the appropriate approach in applying accident causation approaches and comparing findings (contributing factors and safety recommendations). Details of the incident were drawn from multiple sources.3,9 The aim of exploring this case incident was in understanding the role of Computerised Order Provider Entry System (CPOE) application in addition to other contributing factors that led to the patient receiving a high dose of potassium chloride (KCI).
Each accident causation approach was selected based on their theoretical underpinnings and methodology in analysing adverse events. The Events and Causal Factors (ECF) approach was selected based on its ability to provide ‘linear’ and simplistic evidence-based view of the accident by graphically presenting a chain of events leading to a failure. 10 The Human Factors and Classification System (HFACS) allows causes/contributing factors to be classified according to its taxonomy of failure categories which is based on Reason’s Swiss Cheese model. AcciMap (Accident Modelling) and STAMP (System-Theoretic Accident Modelling and Processes) were selected for being among the most utilised systemic approaches in safety-critical domains. 6 While the former allows contributing factors to be causally mapped according to the model’s abstract levels, 11 the latter allows for control flaws and inadequate constraints to be identified. 12
The application of the selected approaches was carried out by the principal author, and respective outcomes were reviewed by human factors specialists and experienced users of these techniques. The safety recommendations were also reviewed and validated. A usage evaluation framework used in previous comparative studies 7 forms the basis for discussing for comparing the application of the selected approaches.
Description of accident approaches
This section provides a brief description of the selected accident causation approaches.
ECF
ECF charting provides a means of graphically presenting chains of events that lead to failure.13,14 It allows investigators to chart the sequence of events in a chronological or linear manner. 13 This method can be utilised as a standalone technique for representing events using different symbols from the ‘initiating event’ to the ‘accident’ and further into amelioration processes. Counterfactual reasoning is also applied by investigators to differentiate causal factors from influences relating to the incident. 15
HFACS
The HFACS method not only was initially developed for analysing accidents in the aviation industry but has also been adapted to the healthcare domain (Wiegmann and Shappell, 2003). 16 It is based on Reason’s Swiss Cheese Model comprising of unsafe acts, pre-conditions for unsafe acts, unsafe supervision, and organisational influences17,18 (see Figure 2). This model also provides qualitative and quantitative means of analysing multiple cases to determine patterns and trends to accident causations in the system as well as root causes.
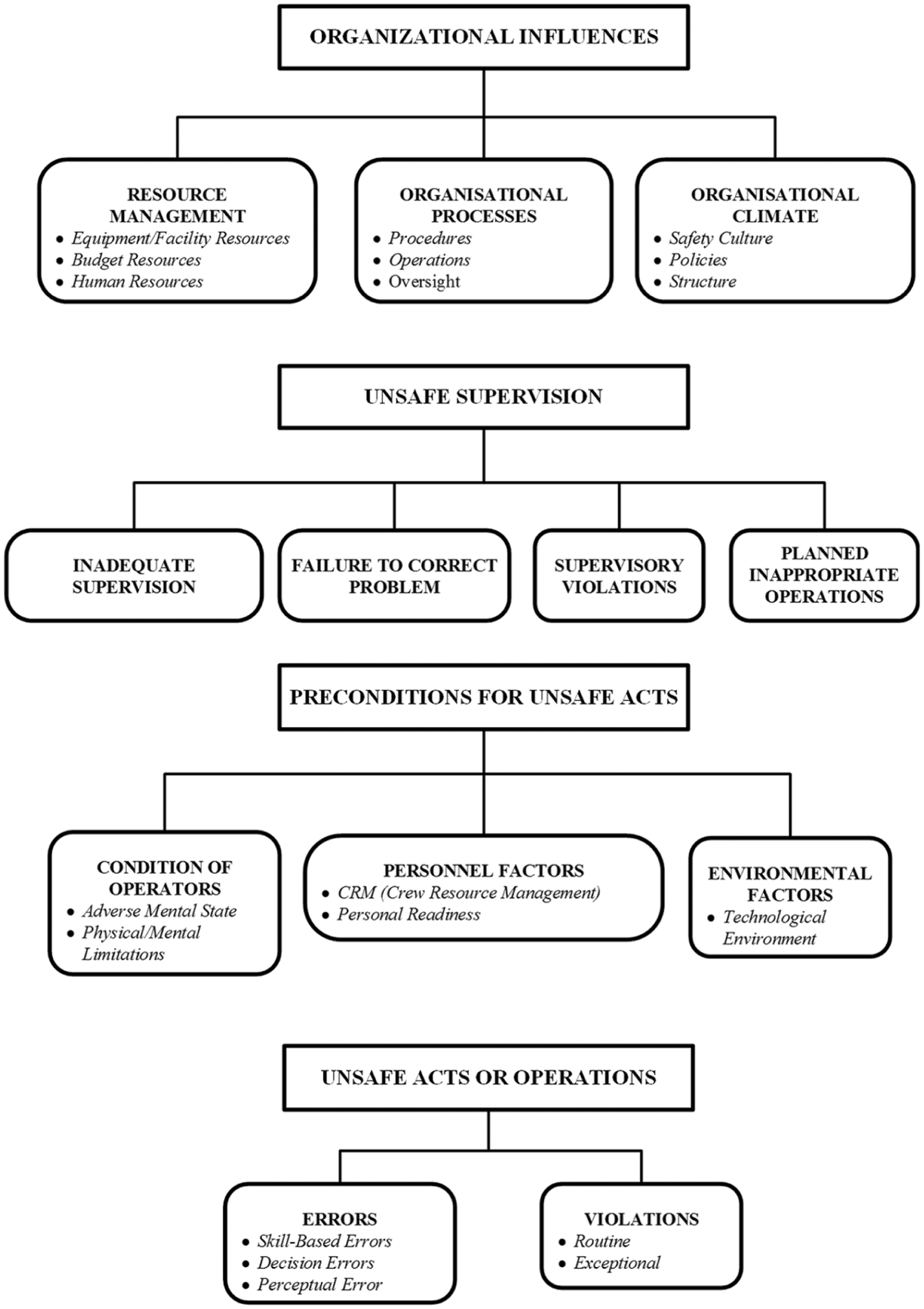
The Human Factors and Classification System (HFACS). 17
AcciMap
The AcciMap model provides a graphical multi-causal diagram for determining factors (events and decisions) that contributed to the accident19,20 (see Figure 3). This approach is also based on Rasmussen’s 21 theory of accident causation. Based on the AcciMap analysis, safety recommendations are formulated to prevent their future occurrence.22,23 The model can be used as a standalone and as part of a broader risk management framework (RMF) involving Actor maps, Info maps and Conflict maps. 19 This process is achieved by linking causal connections within and between different system levels.
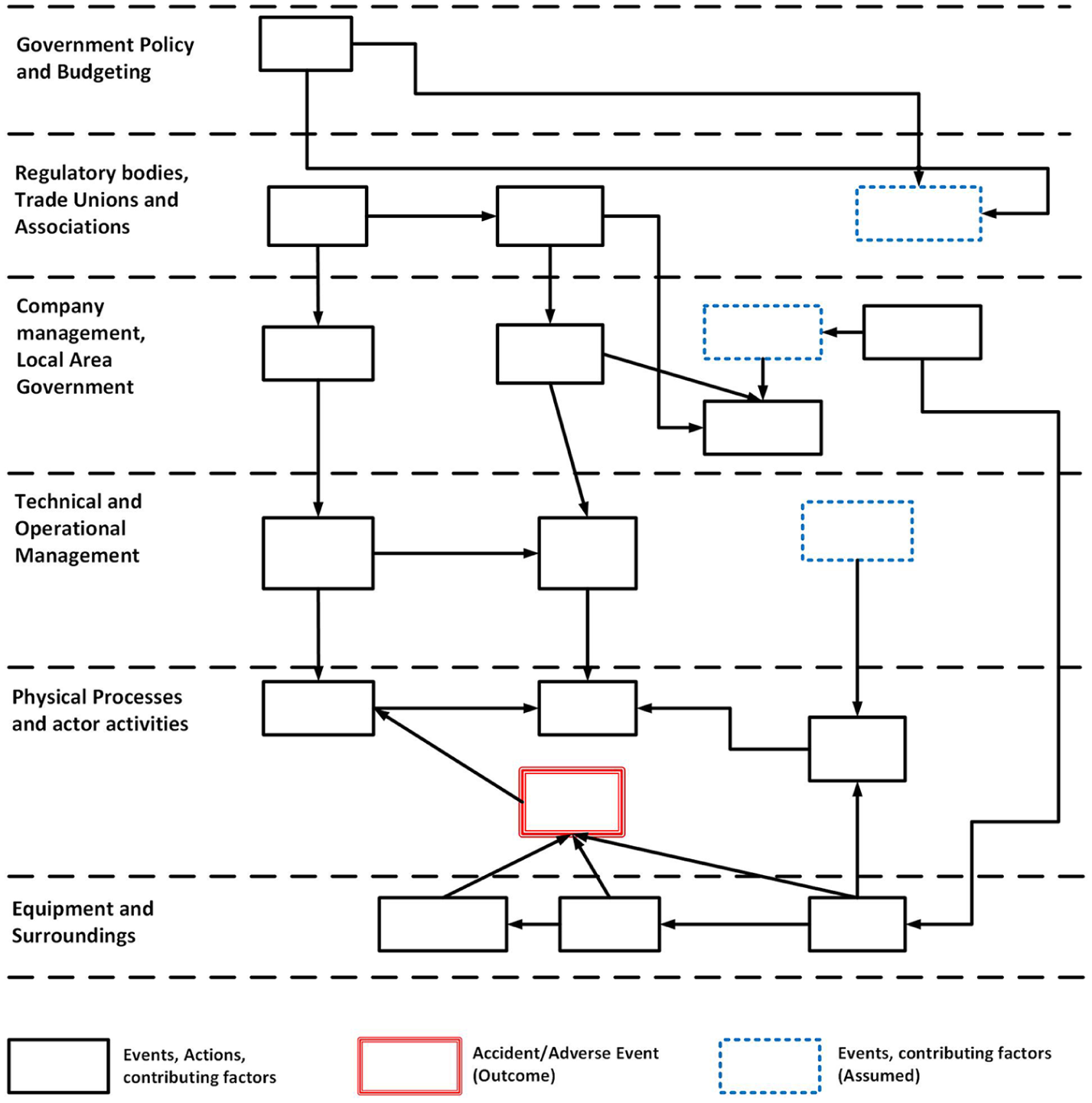
Skeletal AcciMap outline (adapted from Svedung and Rasmussen 11 ).
STAMP
The STAMP model is a systemic-based model developed by Leveson 12 for analysing adverse events in complex systems. It is based on systems and control theory where safety constraints between components are analysed for any disturbances that can affect system safety24,25 (see Figure 4).
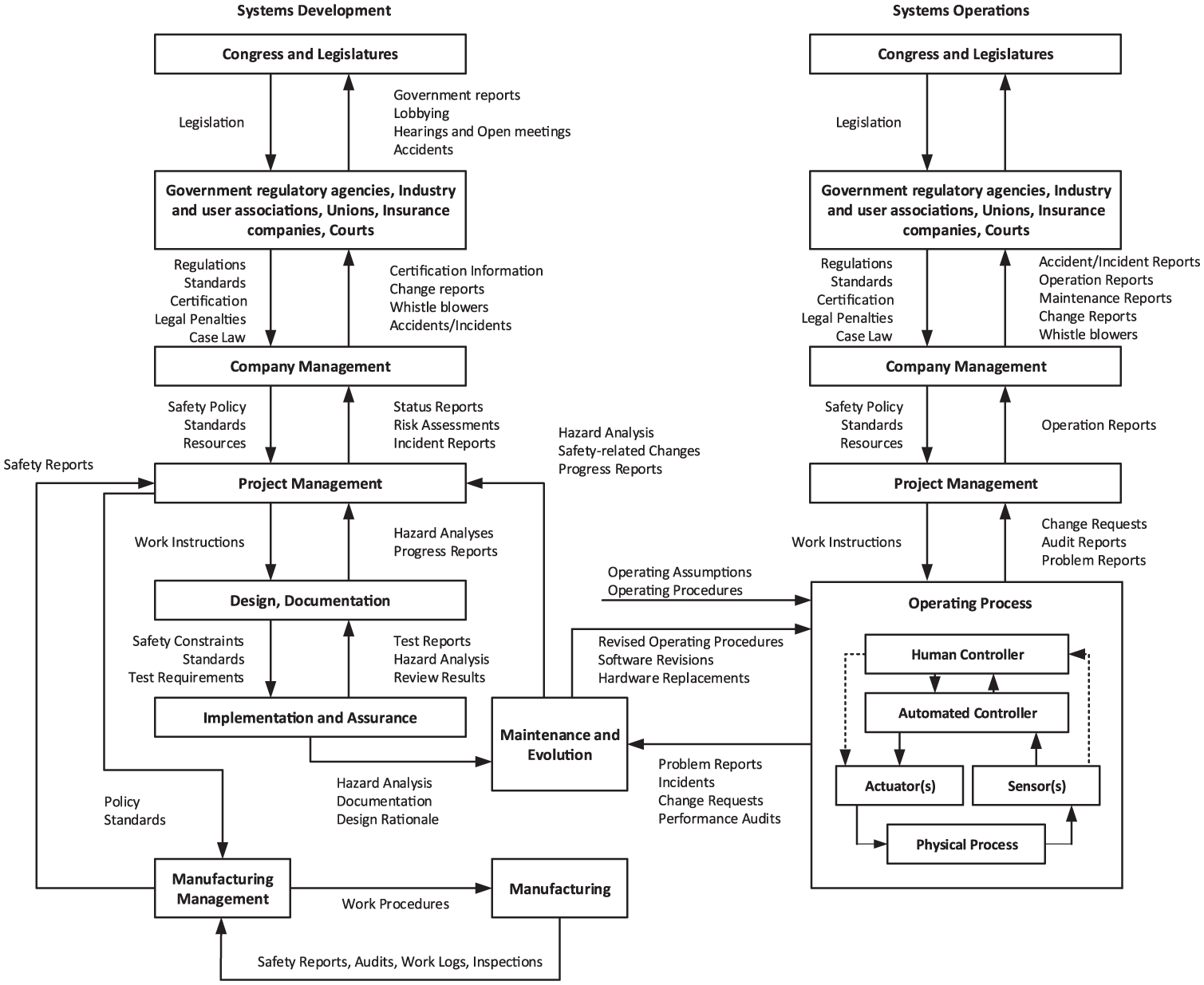
Generic complex sociotechnical safety control structure. 24
The STAMP model also comprises of two types of analysis: Systems Theoretic Process Analysis (STPA) and Causal Analysis using System Theory (CAST). The STPA is a STAMP-based hazard analysis on system engineering in defining accidents, system hazards and control structure. 24 The model’s architecture consists of a generic complex sociotechnical system safety control structure and a high-level taxonomy of safety constraints utilised for specific system hazards defined at the beginning of the analysis (see Table 1).
STAMP’s control failure taxonomy of control flaws leading to hazards. 12
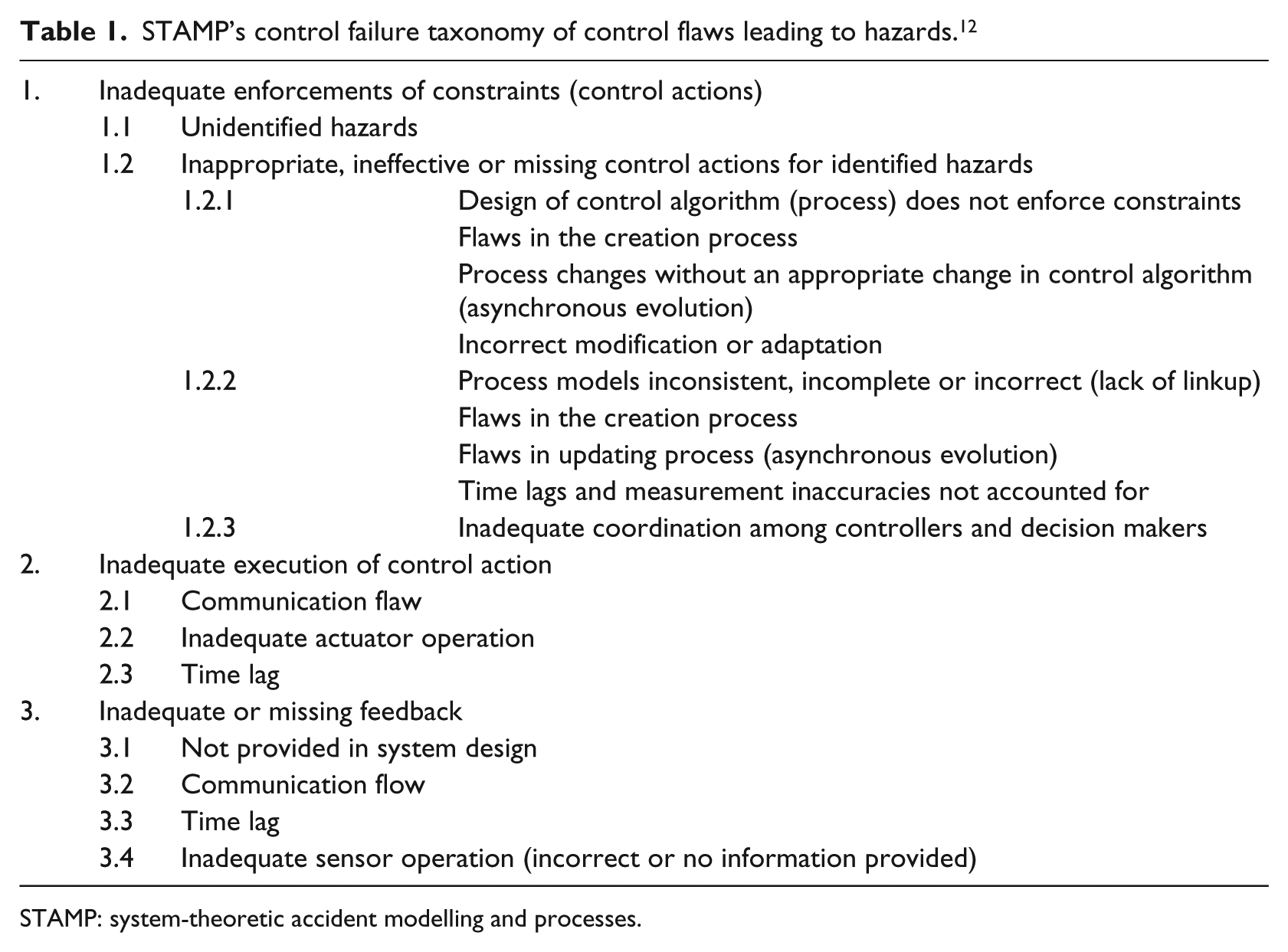
STAMP: system-theoretic accident modelling and processes.
Case incident synopsis
This incident involved a patient who was initially hypokalemic when admitted. Two providers (A and B) attended to the patient with the first administering KCI.3,9 Events leading up to the patient receiving a high dose of KCI took place within the space of 3 days (see Table 2). This incident was classified as an example of a ‘software-related’ or ‘health IT–related’ incident where the combination of factors relating to the technological product and how it was operated can increase the likelihood of the accident occurring.
Orders and actions by providers A and B over 2 days (adapted from Horsky et al. 9 ).
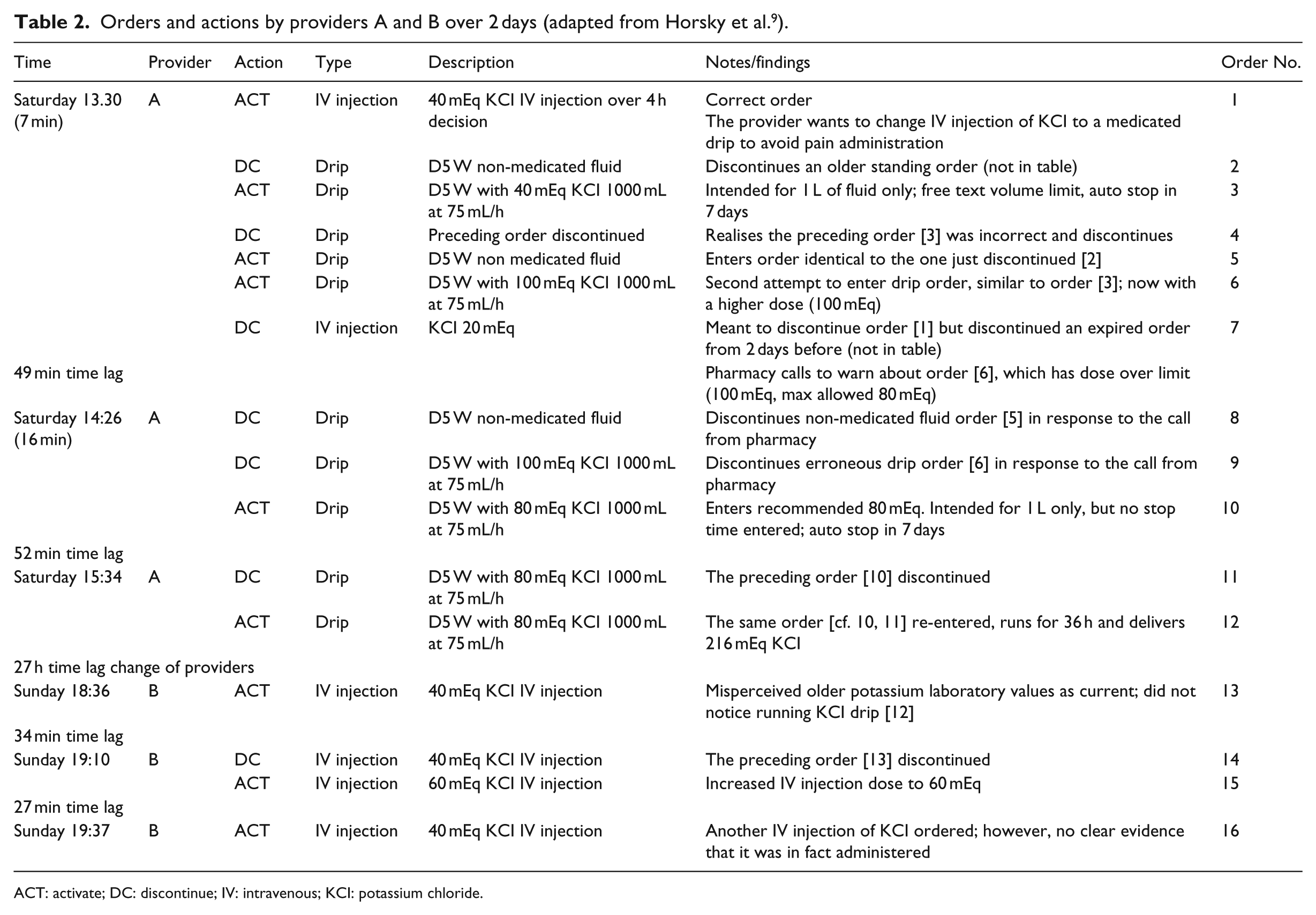
ACT: activate; DC: discontinue; IV: intravenous; KCI: potassium chloride.
Results of analysis
Each of the results obtained from the use of ECF, HFACS, STAMP and AcciMap are highlighted in the following sub-sections.
ECF result
The output of the ECF analysis assumes linear sequences of events and associated conditions leading to the adverse event (patient becoming hyperkalemic) (see Figure 5). The event that ended with ‘the patient becoming hyperkalemic’ can be further analysed to include amelioration processes of ensuring that this adverse event does not occur again. In identifying root causes, there was evidence that there was miscommunication between providers A and B regarding the patient’s KCI levels which contributed to the provider B unintentionally increasing the KCI dose. Another root cause includes the interface design of the CPOE system which made it difficult for both the first provider and the attending nurse to place in the order.
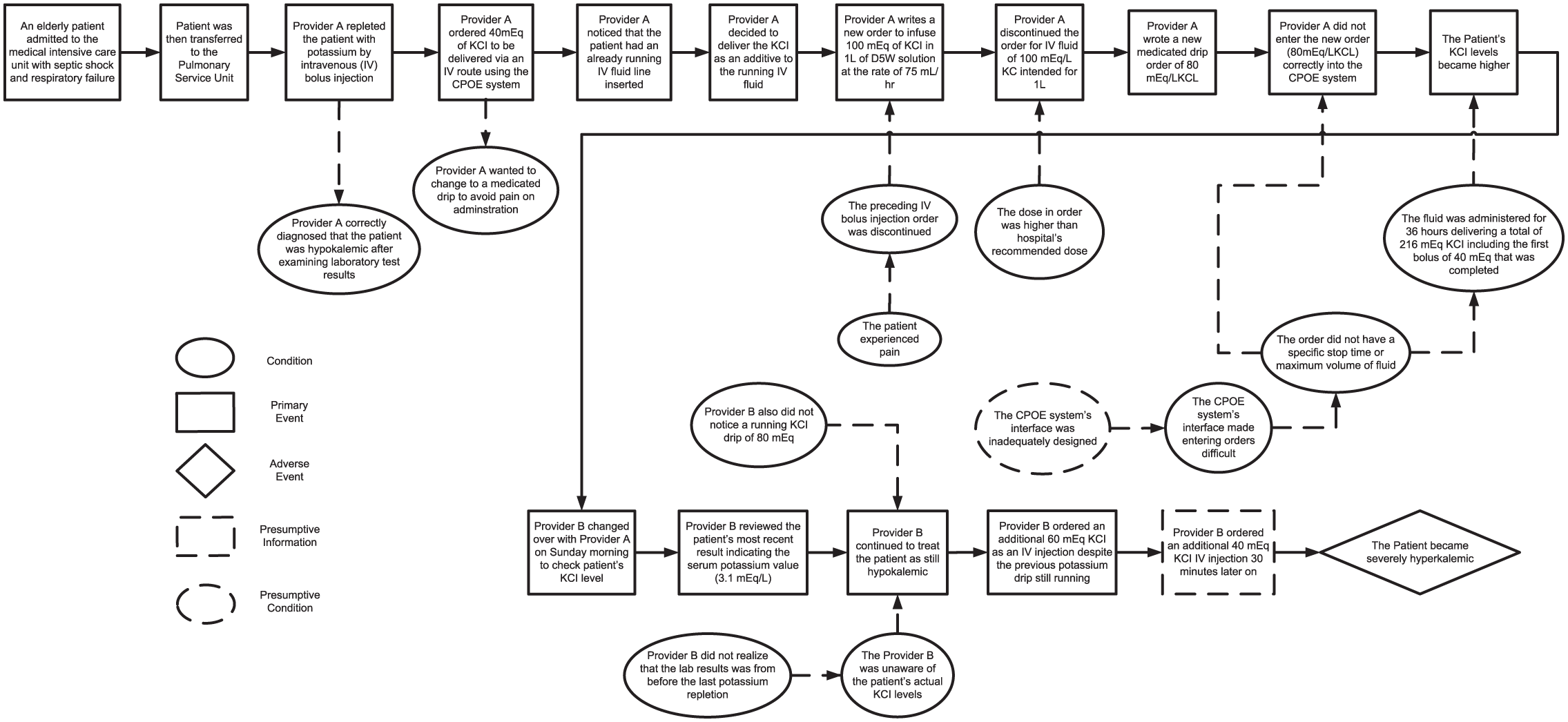
Events and causal factor (ECF) analysis of the case study over the course of 3 days.
HFACS result
The HFACS analysis allows the classification of failures into four levels relating to the medication and CPOE incident (Figure 6).
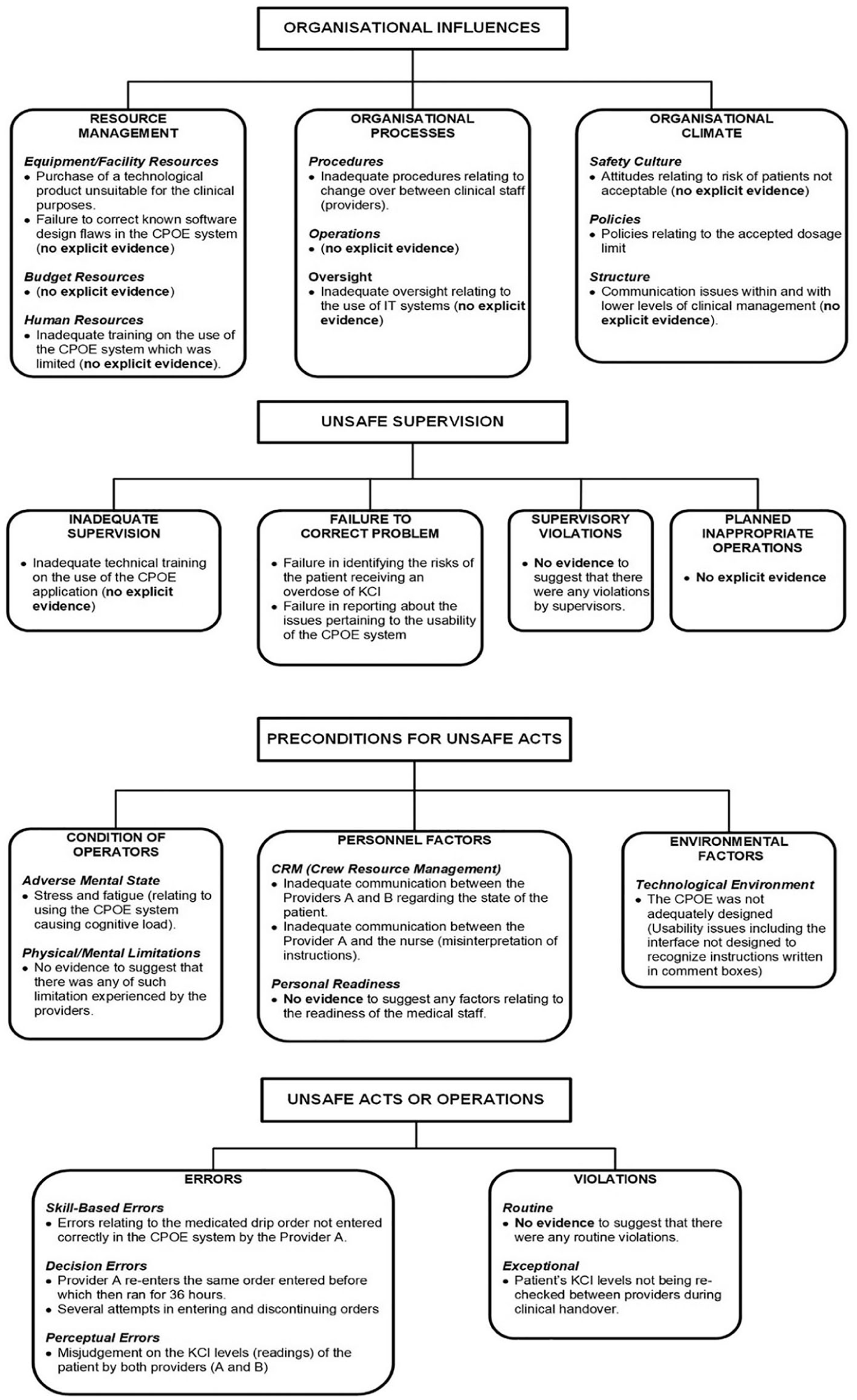
The application of the HFACS on the health-IT adverse event case study.
Unsafe acts
Under unsafe acts category, skill-based errors consist of provider A and the attending nurse incorrectly entering the order in the CPOE system. Decision errors consist of actions of provider A in discontinuing and reentering a similar order which ran for 36 h but with a higher dose. In the perceptual errors subcategory, there was evidence suggesting misjudgement when reading KCI of the patient particularly by provider B. In the violations subcategory (routine and exceptional), violation of the procedures regarding rechecking of the patient’s KCI levels during clinical handover between providers A and B increased the likelihood of the patient becoming more hyperkalemic.
Preconditions for unsafe acts
This level helps in understanding ‘latent conditions’ that facilitated unsafe acts by the staff involved in the incident. In the condition of operators subcategory (adverse mental state), provider A had to put in an amount of cognitive effort when operating with the CPOE system due to how the interface was designed which can cause stress. The personnel factors indicate inadequate communication between both providers during the changeover process. Provider A and the attending nurse regarded the misinterpretation of the order and between providers in communicating the actual result of the patient’s KCI level. The environmental factors, specifically ‘technological environment’, relate to CPOE system’s interfaces creating difficulties for providers due to the way it was designed (i.e. lacking an interface for allowing instructions to be written in comment boxes), and thus have usability issues. There was no additional evidence to suggest any contributing factors from the ‘physical environment’.
Unsafe supervision
Failures under the ‘inadequate supervision’ include not providing adequate technical training and guidelines on the use of the existing CPOE system. Failures can also potentially include not addressing issues regarding the use of the CPOE system as well as change-over processes. Also, under the subcategories ‘failure to correct problem’ and ‘supervisory violations’, failures here emanate from not identifying initial risks to the patient becoming hyperkalemic. In addition, issues relating to the usability of the CPOE system and failure to initiate corrective plans due to possible lack of investigation on ‘Health IT’-related events were not reported. However, there was not enough evidence that this will be considered a valid contributing factor.
Organisational influences level
Not all categories in this level could be used for classification. At the ‘organisational process’ category, procedures relating to changeover between providers was identified (procedures). Under the ‘resource management’ category, purchase of an unsuitable technological product (equipment/facility resources) and inadequate training in using the CPOE system (human resources) can only be inferred based on the unsafe events that took place and why it happened. However, more evidence will be needed to validate these factors.
STAMP/STPA result
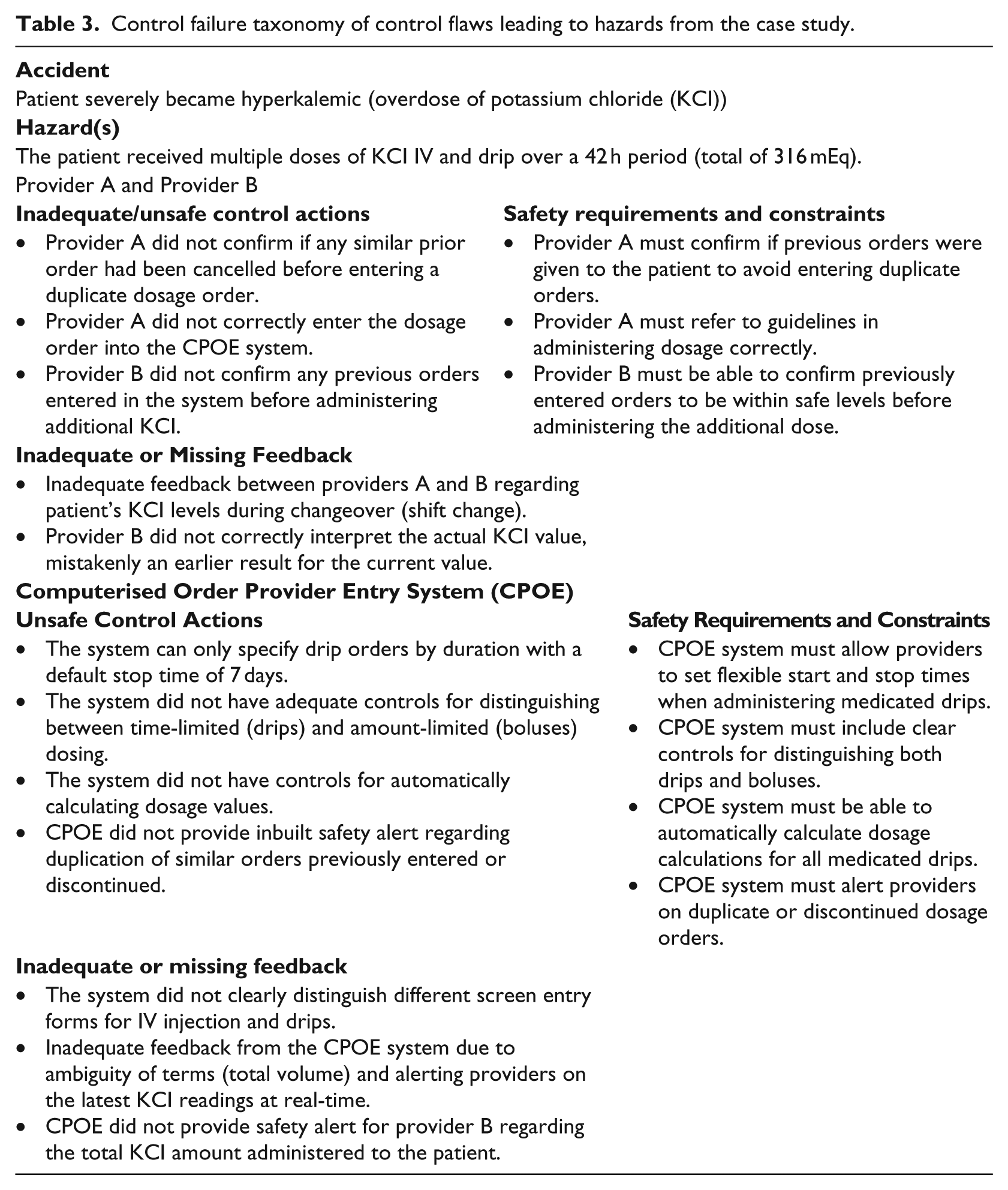
In applying causal analysis based on STAMP, a high-level safety control structure (see Figure 7) and a more focused control structure where the incident occurred were developed (see Figure 8). Using the STAMP taxonomy, interactions between the providers and the CPOE were analysed for identifying safety requirements and constraints, inadequate/missing feedback and inadequate/unsafe control actions (see Table 3). Some of the unsafe control actions relating to the providers include, for instance, the first provider not entering the dosage order in the system correctly. This is also in addition to provider B not confirming previous orders before ordering additional KCI dose. Some of the unsafe control actions relating to the CPOE system include the system not having controls for calculating dosage values automatically and the system only being able to specify drip orders with the default stop time of 7 days (see Table 3). There was also inadequate/missing feedback relating to changeover between providers and also for the CPOE system not differentiating different screen entry forms for drugs and IV injection.
The STAMP control structure of the CPOE medication error case study.
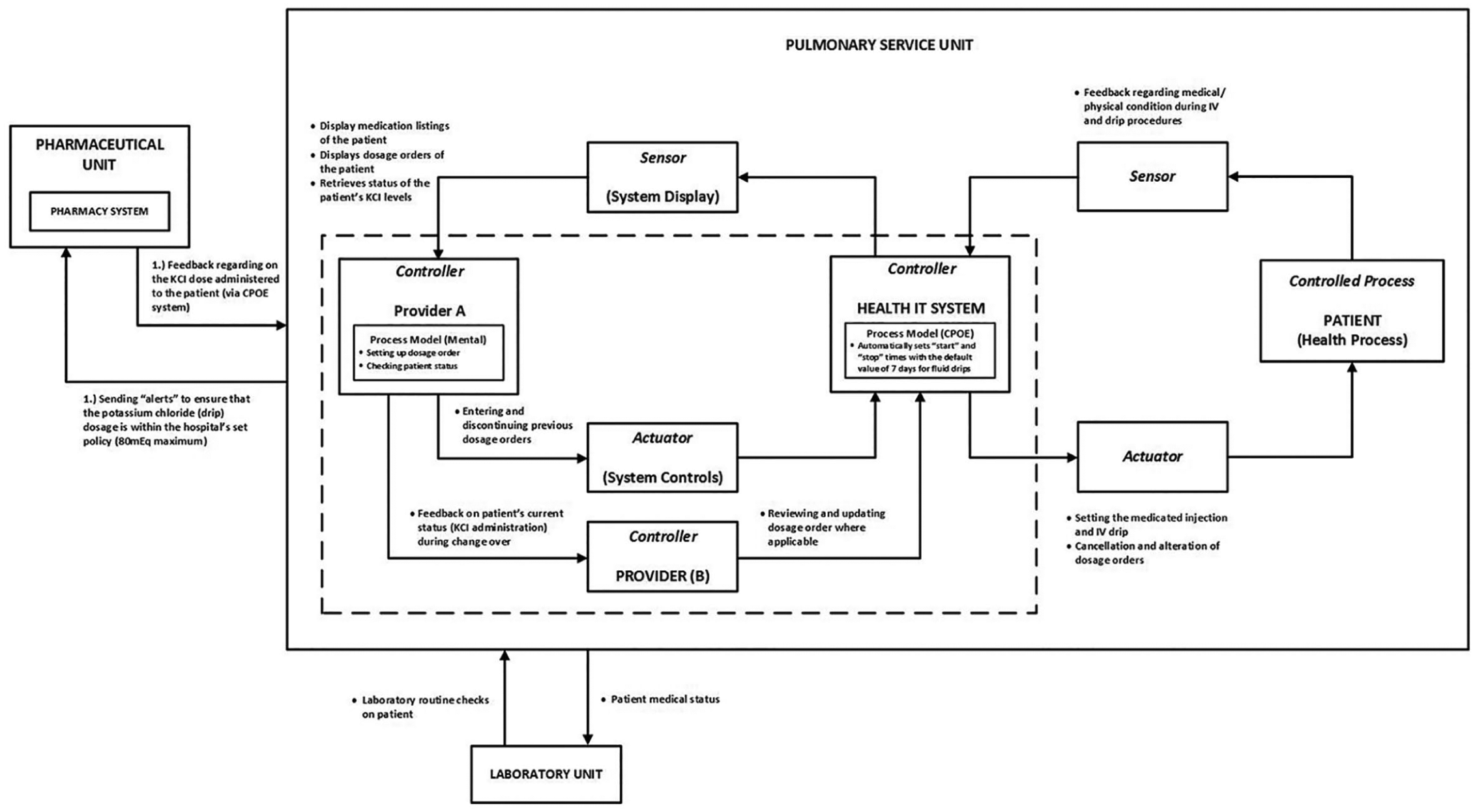
STAMP analysis of lower level system components (interaction between the providers and the clinical information system).
Control failure taxonomy of control flaws leading to hazards from the case study.
AcciMap result
Branford’s AcciMap model was applied on the case incident from the original documentation 9 as well as the additional abridged information from other sources 3 (see Figure 9).
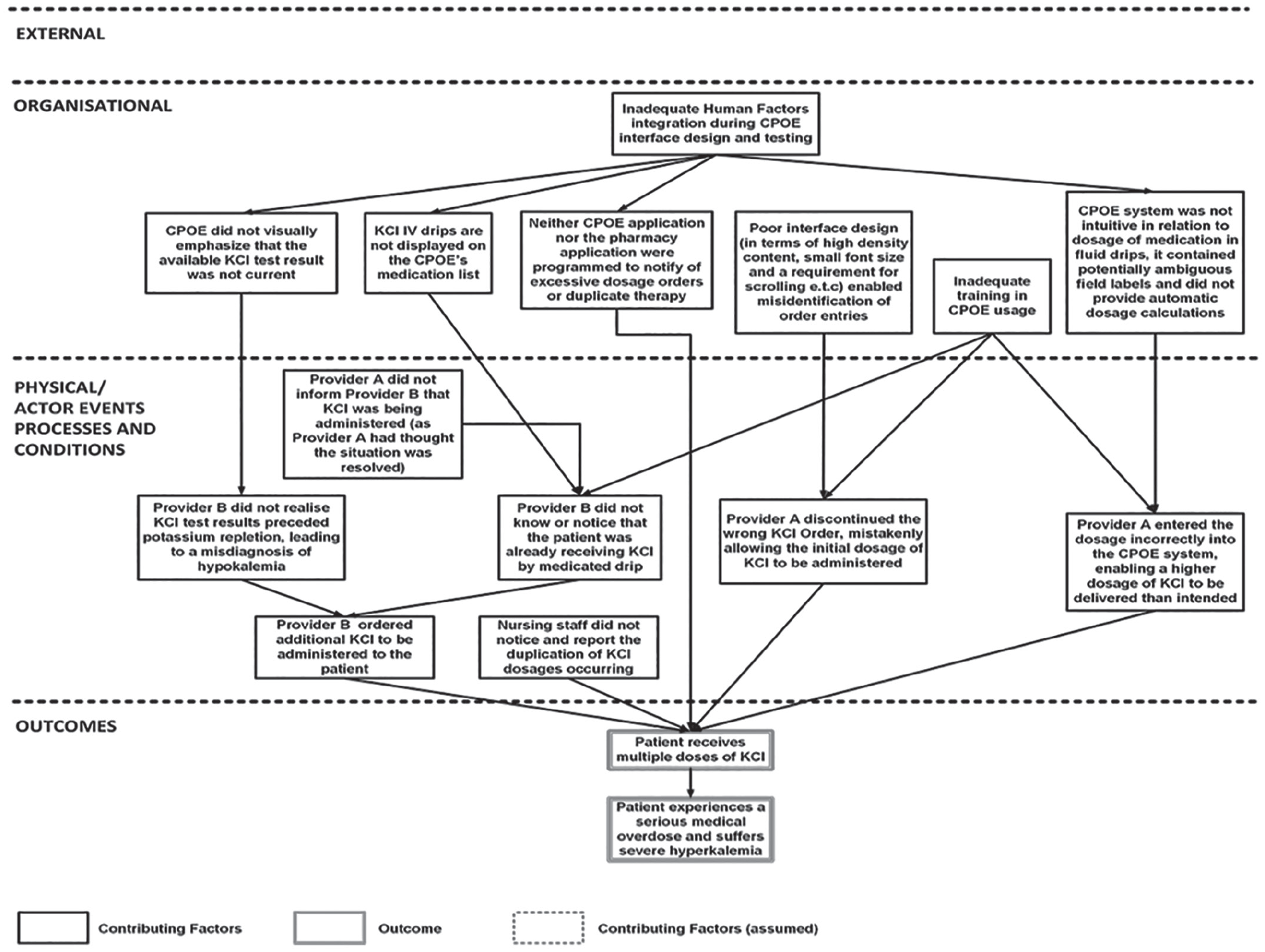
AcciMap analysis of the medication dosing error related to CPOE system (based on Branford’s standardised AcciMap format).
Based on the result obtained, the contributing factors identified are discussed below:
Outcome(s) of the case incident
This indicates the adverse outcome on the patient where he suffers severe hypokalaemia because of multiple doses of KCI.
Physical processes and actor activities
This level describes a combination of events carried out by different ‘actors’ that directly affected the patient including how the conditions may have affected them. The first provider (A) had given the patient a high dose of KCI than was originally intended because the order was not entered correctly into the CPOE system. Provider A also discontinued the wrong KCI order and mistakenly allowed an initial KCI dosage to be administered. During the changeover, provider A did not adequately inform provider B regarding the KCI dosage administered. This was due to the first provider assuming that the situation was resolved. This then led to provider B mistakenly taking an earlier result of the KCI as the current and then administering an additional KCI. Also, the nurse that was initially involved did not also notice the duplication of the dosage orders entered.
Organisational level
Contributing factors at this level include inadequate training in using the CPOE system and usability issues. These include the design of the interface including small fonts and clarity of safety-critical information. Another contributing factor was that neither the CPOE application nor the pharmacy system was programmed to notify excessive dosage or duplicate order entries. These factors stem due to inadequate human factors integration during the design and testing of the CPOE application.
External level
There was no explicit evidence to suggest that there were any external contributing factors that created the conditions for the accident to occur.
Usage characteristics of selected accident analytical approaches
The usage characteristics criteria were used to summarise the application of the selected approaches (see Table 4). However, three important characteristics, usability, validity and reliability, are further discussed.
Summary of usage characteristics comparison (adapted from Underwood and Waterson 7 ).
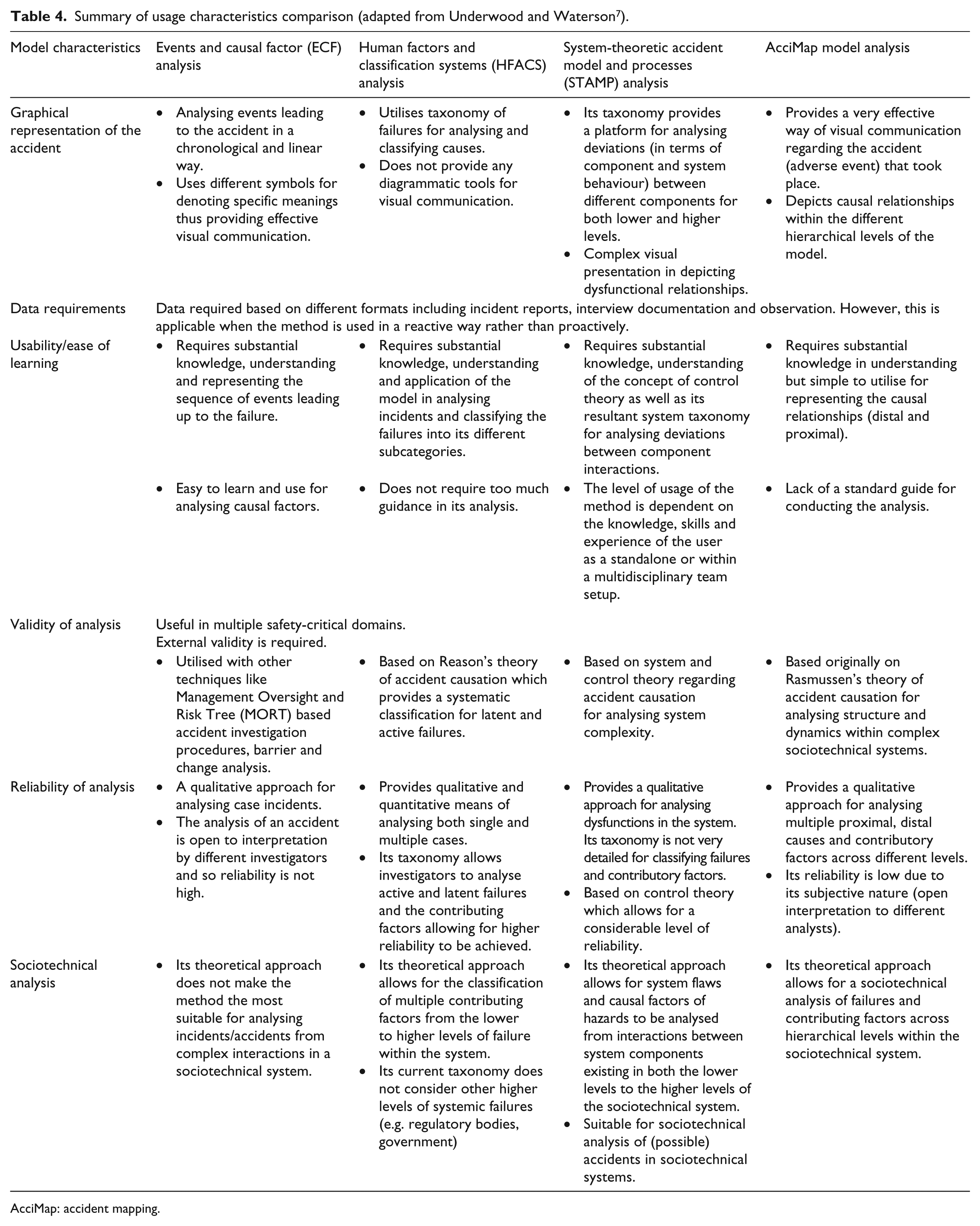
AcciMap: accident mapping.
Usability/ease of learning
Substantial knowledge, especially for first-time users, is required to model in using these approaches. From this experience, each of the models presented contrasting challenges. The utilisation of ECF requires following guidelines in representing the chronological sequence of events. An understanding of human error, as well as Reason’s Swiss Cheese Model 26 which the taxonomy is built on, is at the very least a basic requirement. While using all the approaches require a considerable amount of time, cognitive effort and knowledge of the domain, ECF, HFACS and AcciMap were less challenging in its application and more intuitive than STAMP.
Modelling the accident using the STAMP model requires a thorough understanding of system and control theory concepts to be able to effectively analyse accidents. This in addition to understanding how to apply the model’s taxonomy for identifying unsafe controls and safety constraints within a complex sociotechnical system took a great deal of time. Despite AcciMap being relatively easier to apply than STAMP, it still requires following a set of guidelines in correctly identifying valid contributing factors, placing them in the right level and setting logical causal relationships between them. Of the approaches, ECF provides a simplified way of modelling and describing the events leading to the accident. While this may be the case, counterfactual reasoning was required in determining the necessary events needed to have caused the accident.
Validity of analysis
Formal validity measurements were not carried out in this study, but validation with experienced analysts (human factors specialists) was required for outputs of the analyses. Each of them is based on a recognised theory of accident causation and has been applied across multiple safety-critical domains for accident analysis (Salmon et al., 2012). 7 To formally measure the validity of each approach used, a study will need to be taken that involves comparing outcomes and safety recommendations taken by multiple analysts and experienced/expert opinion. 22
While each model presents different methodological approaches for analysing accidents, AcciMap and STAMP allows users to determine why accidents occurred using systems thinking and looking at the entire sociotechnical system. The classification scheme of the HFACS model provides guidance in data collection and analysis of singular and multiple incidents. However, HFACS overall is limited because of the restrictive nature of its classification scheme in addition to not considering contributing factors at the external level.
Reliability of analysis
No formal reliability measurements were carried out in this study. However, HFACS’s taxonomy can potentially enable multiple analysts to produce similar results from the case study. This is because of its reliability when classifying human errors27,28 and is considered moderately higher in comparison to AcciMap and STAMP models.6,7 While the methodological approach regarding the use of AcciMap allows analysts to construct multiple causal relationships, the reliability of the AcciMap model has been mixed with past studies considering it to be low. 7 Its outcomes can vary between multiple investigators due to lack of a classification scheme. 28
A similar conclusion on potential variations if undertaken by multiple investigators can be applied to the ECF charting approach. The STAMP’s generic taxonomy should allow for some considerable levels of reliability. Ideally, results from the use of these approaches would need to be re-evaluated from other analysts using both intra- and inter-reliability measurements to determine if similar outcomes and recommendations will be produced.
Discussion
Contributing factors from the analyses
Based on the results, each approach produced a set of contributing factors/control flaws based on its underlying methodology (see Table 5). This can potentially influence the development of safety recommendations for mitigating and preventing its reoccurrence. Common themes regarding contributing factors identified from these approaches include ‘inadequate communication’ between providers (A and B) and usability of the CPOE application. In the case of the ECF output, ‘lack of/or poor communication’ between providers A and B played a role in the latter not knowing the patient’s true KCI levels. However, the question that will be asked will be ‘why’ there was a miscommunication. In this case, provider A may have assumed that the CPOE system would emphasise the current KCI value for provider B to access.
Contributing factors (ECF, HFACS and AcciMap) and control flaws (STAMP) from case incident.
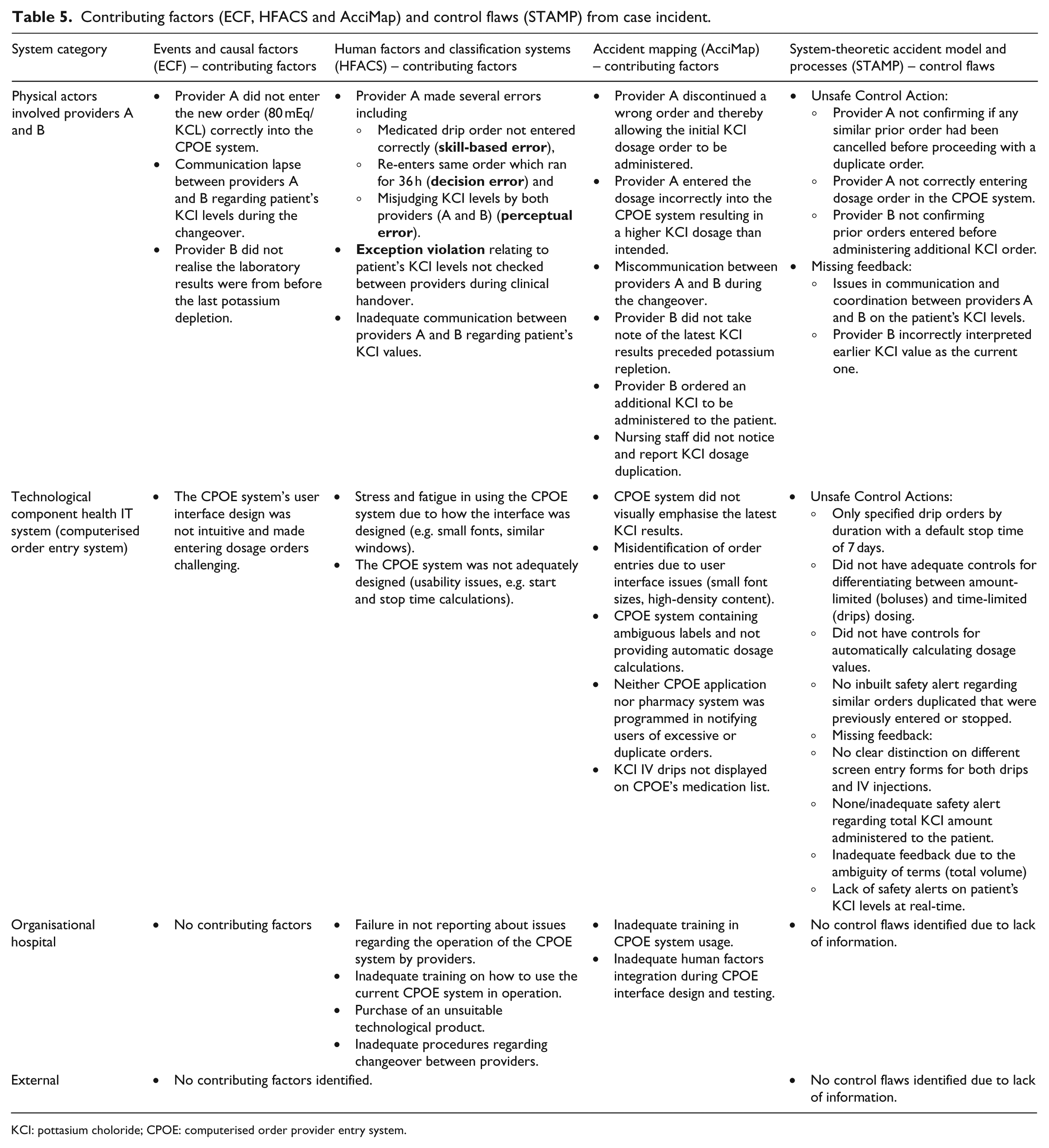
KCI: pottasium choloride; CPOE: computerised order provider entry system.
On further examining the ECF result, it can be deduced that the dosage order was not entered correctly due to design issues of the CPOE system. These design flaws would be considered another necessary cause for provider A’s difficulty in entering the dosage order. Applying counterfactual reasoning to the ECF analysis, it can be argued that if provider A had properly informed provider B about the patient’s KCI status, then the likelihood of the patient receiving a higher dosage of KCI would have been reduced or prevented. Another counterfactual claim would be that if the CPOE interface was designed to have clarity in the labels indicated on the interface and a comment box to allow the first provider and nurse to easily enter the dosage order, then the chance of an error in inputting the dosage order would have been reduced. In the case of the incident between the nurse and the first physician (provider A), if the nurse had reconfirmed the order that was given by the provider, the value would have been entered incorrectly into the CPOE interface.
From the HFACS result, the categories defined allow for contributing factors to be classified but more importantly to determine the nature of unsafe acts, pre-conditions to these acts and any organisational influences. Several factors similarly identified in ECF include errors (skill, decision and perception) committed by both providers. Other factors include communication flow between both providers and the CPOE system having usability issues due to design flaws. Other contributing factors classified included issues relating to inadequate technical training on the use of the current CPOE application (unsafe supervision) as well as factors relating to procedures (handover) and purchase of the system not very suitable for this clinical purpose.
Contributing factors identified using the AcciMap approach produced similar factors with additional ones relating to the CPOE system. These include both CPOE and pharmacy systems not being programmed to notify providers on duplicate orders and drips not being displayed on the medication list. All these stem from the lack of human factors integration into the design of the CPOE which was identified at the organisational level. The STAMP model differs from AcciMap, HFACS and ECF due to its focus on violations in safety from interacting system components rather than from an initiating event. From the STAMP/STPA analysis, unsafe control actions and missing/inadequate feedbacks regarding providers (A and B) and the clinical IT system (CPOE) are identified as well as safety constraints. These include provider A not confirming if similar orders were cancelled, and provider B not confirming orders entered previously by provider A. Unsafe control actions relating to the CPOE include not having safety controls for alerting on similar or duplicate orders previously entered, and only having a default setting of 7 days duration for drip orders.
Comparison of safety recommendations
Safety recommendations formulated from the outcomes also produced some similar measures (see Table 6). These include redesigning of user interfaces incorporating best practices for system usability (ECF, AcciMap, HFACS, STAMP) and implementation of safety alerts on the CPOE (STAMP). Also included is the application of human factors in designing IT systems (AcciMap) and improving existing feedback protocols during the changeover between providers (ECF, HFACS, AcciMap, STAMP). Other safety measures not considered from the analyses include, for example, creating policies of simulated testing of health IT systems which can also serve as a way of training staff in using them. Also, the amount and type of alerts will need to be considered to avoid scenarios where providers will be bombarded with may alerts which could lead to alert fatigue. This can potentially pose a risk of ignoring important alerts that could act as a safety barrier.
Safety recommendations from the accident analytical approaches.
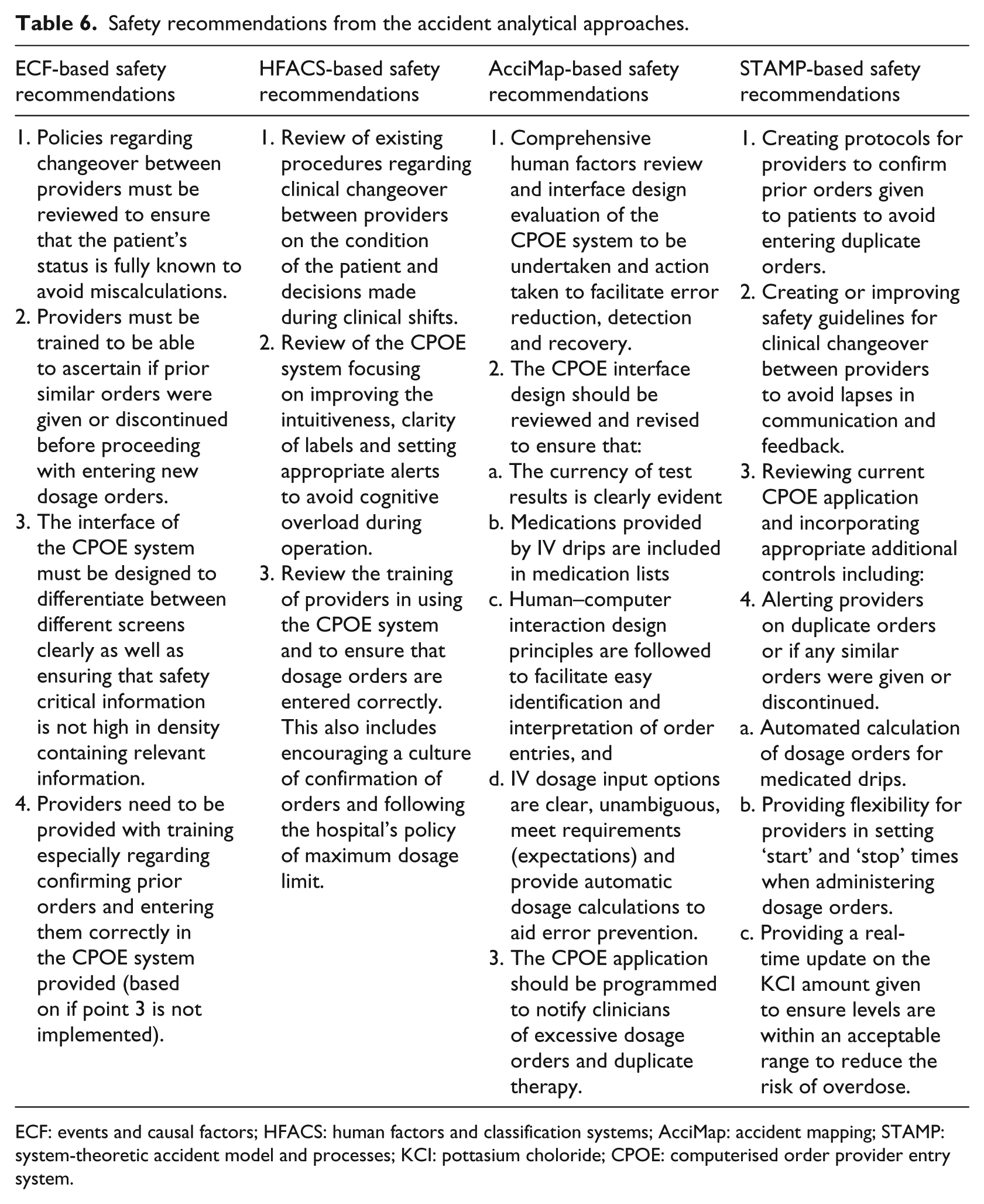
ECF: events and causal factors; HFACS: human factors and classification systems; AcciMap: accident mapping; STAMP: system-theoretic accident model and processes; KCI: pottasium choloride; CPOE: computerised order provider entry system.
Experiences in the application of selected accident analytical approaches
Applying each approach in analysing the incident presents different ways of analysing why the adverse event occurred. While ECF, HFACS and AcciMap generally employ a traditional approach of analysing accidents by extracting contributing factors, the STAMP approach focuses on determining unsafe control actions and constraints that were violated. Based on the usage characteristics criteria used to summarise differences of each accident approach, it is also very important to determine which of these approaches provide an overall benefit when carrying incident analysis in healthcare systems. Based on experience using these approaches, the ECF would be considered to be the most straightforward, intuitive and less time-consuming approach compared to the others. However, due to its linear approach in plotting sequences of events, it will be considered limited when modelling multiple causal interactions that typify complex sociotechnical systems. When considering the HFACS approach, with its classification scheme built upon a recognised theory of accident causation, categories defined will need to be specific to considering causal factors related to healthcare to make it more practically useful. In using this approach, some of the categories could not be used due in part to lack or no information to support evidence. The HFACS approach also does not have categories to consider external factors.
Similar to ECF, applying the AcciMap model did not require much effort in understanding how it is applied especially when following Branford’s guidelines. Key aspects include identifying valid contributing factors, placing them at the appropriate system level and inserting causal links between these factors. This gives an overall picture of how these multiple interactions proceeded to the accident. However, this ‘freedom’ of analysis introduces issues relating to subjective results based on analysts’ perception and understanding of the incident. A major criticism of the AcciMap approach is its reliability ranging from low to mixed. 7 The STAMP model certainly provides an alternative way of analysing accidents and can be used in conjunction with other approaches to provide a deeper understanding of the loss of control. STAMP’s theoretical underpinning can create challenges in classifying human and organisational failures within its taxonomy. 28 As powerful as the STAMP approach is, it is the least intuitive and the most time-consuming approach compared to the others.
Overall, in terms of being able to identify and graphically present multiple causal relationships in complex sociotechnical systems, AcciMap would be considered the most suitable of the approaches used in this study. However, its reliability and validity will need to be further improved to be considered a valuable tool for accident investigation and analysis in healthcare systems.
Limitation of study
The approaches applied to this type of incident not only presented different ways of analysing what went wrong but also presented challenges. There is the challenge of having different forms of bias when investigating and analysing why the accident occurred including hindsight and outcome bias. This was reduced by trying to analyse the case with the information extracted from multiple sources without using the original outcomes and recommendations.
It would have been more ideal to have access to additional information particularly from sources like interview transcripts of clinicians who were involved. This would have allowed for comparison with the previous author’s findings for similarities or differences. In addition, analyses and results from the application of these approaches were carried out by the principal author and reviewed by experienced practitioners. This approach was taken to ensure that results obtained were valid in the absence of no formal reliability and validity measurements that could be used for this study.
These issues can potentially determine how effective and practical safety recommendations developed can prevent reoccurrence. Another limitation in this study was that it was not extended to compare with the original recommendations from the incident. If this study was to be repeated, it will need to be applied to major cases with substantial supporting information to gain further insight into systemic issues. Also, for reliability and validity testing, each of the approaches can be analysed by multiple experienced investigators. Their findings can then be assessed for the reliability of the model as well as validating safety recommendations formulated from their analyses.
Contribution to knowledge
This study demonstrated the application of different accident analytical approaches in an example case incident. It was also important to determine which of them will be considered the most practically suitable for determining contributing factors including systemic factors in healthcare systems. However, while there is an acknowledgement of the strengths and limitations of each approach, it is important to consider crucial characteristics in determining which accident analytical approach to use. These include its ability to depict complex interactions, how intuitive and easy it is to apply and how much time it takes to learn and understand how they are applied.
Conclusion
The comparison of different accident approaches for investigating health IT–related safety risks demonstrates the strengths and limitations of their respective methodological approach. Despite each of their respective benefits, AcciMap and STAMP approaches generally provide a ‘systems thinking’ perspective when investigating and analysing incidents in complex systems. However, to be able to effectively apply these approaches, their theoretical foundations and guidelines need to be understood and applied correctly to obtain reliable and valid results. This will allow effective safety recommendations to be developed.
There is also the current challenge of how existing accident analytical approaches like the AcciMap’s reliability and validity can be further improved and hence be more practically useful in healthcare organisations. According to Salmon et al’.s 29 study, a domain-specific classification scheme like the HFACS approach can be developed and synthesised within the AcciMap methodology. This methodology can be similarly applied within the healthcare context for analysing health IT–related accidents. To achieve this, grounded taxonomies will need to be examined to develop a health-specific classification scheme of contributing factors incorporated within the AcciMap model.
Footnotes
Acknowledgements
Analyses and results obtained from the case study were reviewed by Dr Kate Branford, a human factors specialist with the railway industry, Australia and Clear Thinking consultant Dr Suzanne Shale and HFACS taxonomy specialist. Further acknowledgement also goes to Dr Maria Mikela Chatzimichailidou, Systems Engineer of the Imperial College, London, and Mr Iain Bishop, an e-Health Pharmacy Adviser, Information Technology of the National Services Scotland (NSS).
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.