
Abstract
Providing the best possible nutritional care requires accurate and precise communication between healthcare professionals. Developing a Nutrition Minimum Data Set will inform professionals in primary healthcare of which core elements should be documented and facilitate a standardized approach to the documentation of nutritional care. A two-step methodological approach was utilized in this study: (1) a systematic scoping review was conducted to map evidence underpinning the development of a Minimum Data Set and (2) the datasources were categorized using the inductive content analysis approach. A total of 32 items were identified in the datasources. Five categories were inductively derived from the data: (1) physiologic measurements, (2) ability to eat, (3) intake, (4) stress factors and (5) factors which indirectly affect intake and needs. Organizing the documentation following the structure presented in this Minimum Data Set will contribute to a standardized terminology, which may lead to increased quality of documentation, increased continuity of care and improved health outcomes.
Background
The prevalence of malnutrition is in different studies estimated to be 40–90 per cent of patients in nursing homes and patients receiving home care.1–3 The consequences of malnutrition are costly both for the patients and the healthcare system. Patients’ functional capacity, health status and quality of life are reduced and mortality is increased fivefold. 4 Malnourished patients are more likely to suffer from concurrent infections, such as pneumonia,5–7 and have an increased hospitalization, readmission and rehabilitation rate.8–12 The annual healthcare costs for a malnourished patient are up to three to four times greater than those of a well-nourished patient.13–15 Primary healthcare professionals are challenged by the fact that nutritional care is complex and multifaceted and that many nutritional-related data and much information must be collected in order to provide high-quality care and ensure its continuity. 16 The phrase ‘one size does not fit all’ is often used to highlight the need for tailored and patient-targeted observations and interventions within nutritional care.17,18 Nutritional care encompasses a large variety of complex and less complex practices, ranging from assistance during meal times, calculating protein and calorie intake and providing nutritional advice and counselling. Nutritional issues or malnutrition do not occur and are not solved overnight, and regardless of the content, duration or type of nutritional care, the communication and collaboration among different healthcare professionals are of the outmost importance in order to ensure that patients receive coherent and coordinated nutritional care and treatment. Primary healthcare professionals often make decisions regarding nutritional observations or interventions alone, without any colleagues present; 19 hence, the requirement for a supportive, structured, accurate and updated healthcare record is indisputable.20–24 A survey of 20 European countries found that the nursing process is commonly used to structure the documentation within different healthcare settings. 25 In addition, within this frame, several standardized terminologies are being used, such as the VIPS model (Well-being, Integrity, Prevention and Safety), North American Nursing Diagnoses Association – International (NANDA-I), International Classification for Nursing Practice (ICNP), Nursing Interventions Classification (NIC) and Nursing Outcomes Classifications (NOC). 25 The different data structuring methods contain a standardized terminology with the overall purpose of encouraging a common understanding and interpretation of terms. 26 However, in spite of these existing structures and terminologies, several studies highlight the need for documentation systems that support and guide healthcare professionals in their observations and documentation in a more detailed manner.27,28 The term ‘nutrition’ is well-known and commonly used in patients’ healthcare records. Although the term indicates that it is relevant to observe and document about nutrition, the term does not adequately specify or guide healthcare professionals with regard to what to observe or document within the nutritional area. This could potentially cause healthcare professionals from the same district in a community setting to use different terms to document the same information and observations. It has been suggested that the lack of detailed standardized terms and ambiguous language to describe observations and interventions results in imprecise and unstructured documentation of the care and treatment delivered,29–31 consequently compromising the initiation, continuation and quality of therapeutic nutritional care and treatment.32–35 In fact, some documentation systems might even be counterproductive to safe and effective care. 27 Studies describe a lack of nutrition-related information in patients’ healthcare records.35,36 Healthcare professionals indicate that they do know that nutrition is important,37,38 but they have difficulties identifying what needs to be documented about patients’ nutritional care, what is relevant and what is important.37,39 Fundamental to any discussion of structured documentation is a recognition of the significant international work undertaken on Minimum Data Sets (MDS). MDS are one of the most notable structured documentation systems within patient care and consists of a minimum set of data with uniform definitions and categories within a specific aspect or dimension of the healthcare system.40,41 Within the primary healthcare setting, for example, the MDS for Long-term Care Version 3.0 exists and consists of 20 main categories to facilitate standardized assessment and documentation for nursing home residents, including nutrition. 42 Although studies have found various MDS to improve quality of documentation and consequently patient outcomes,34,43–46 studies have also found that many MDS lack sufficient detailed information and indicators to support clinical decision making within specific areas.47,48 Instead, the MDS act as an overall framework in which healthcare professionals themselves decide upon which variables and observations that are relevant to document based on their expertise and level of knowledge within the specific area. As there are no established detailed MDS for the nutritional area within primary healthcare, the aim of this study is to develop one.
There is no standard methodology for the development of MDS and several approaches have been used, among them work conferences (based on expert opinions and experiences) and formal consensus techniques (e.g. the Delphi consensus technique).49,50 By aggregating various sources of evidence, data from nutritional screening instruments, nutritional expert knowledge and patients’ perspectives, this study will develop an MDS within the nutritional area specifically for primary healthcare in order to develop a detailed framework for documentation of nutritional care by identifying items that may influence nutrition. This will provide a common terminology within the nutritional area, and thereby, it is hoped to increase the quality of documentation, promote continuity of nutritional care and enhance patient outcomes.
Objective
The objective is to identify data elements to be included in a Nutrition MDS specifically for primary healthcare in order to facilitate a standardized approach to the documentation of nutritional care.
Research questions
What items are included in validated nutritional screening instruments for adults in primary healthcare?
What do nutritional experts find appropriate to assess about adults’ nutritional status in primary healthcare?
What do patients and their relatives find appropriate to assess about adults nutritional status in primary healthcare?
Methods
Design
A two-step sequential methodological approach was utilized. First, a systematic scoping review using The Joanna Briggs Institute’s approach for the conduct of systematic scoping reviews was utilized to map the available evidence underpinning the development of an MDS.51,52 Second, the data included from the scoping review were analysed using the content analysis approach53–55 (see Figure 1).
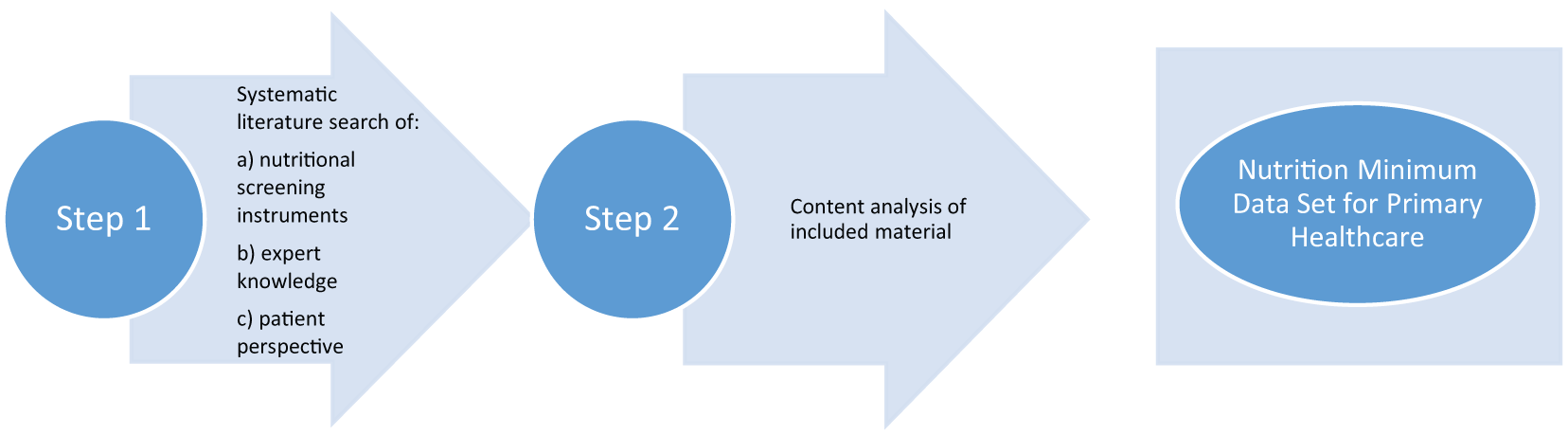
Process of developing a Nutrition Minimum Data Sets.
Data collection
A comprehensive systematic literature search was performed to identify (1) all published nutritional screening instruments that have been developed and validated in the adult population in a primary healthcare setting, (2) evidence from the perspectives of nutritional experts within the nutritional care field as to what is viewed as appropriate to assess about adults’ nutritional care in primary healthcare and (3) perspectives and views of adult patients and their relatives regarding nutritional assessment and documentation were also sought. 52 The Joanna Briggs Institute’s approach for the conduct of systematic scoping reviews was utilized to map the available evidence underpinning the development of an MDS. The scoping review methodology was chosen due to its usefulness for addressing objectives broader than traditional systematic reviews and capturing a range of potentially relevant sources of evidence. 56 A detailed description of the search strategy, search questions and criteria for inclusion and exclusion can be found elsewhere. 52 All datasources were selected against pre-determined inclusion criteria consisting of detailed descriptions of the types of participants, the core concepts and the context. 51
Data material
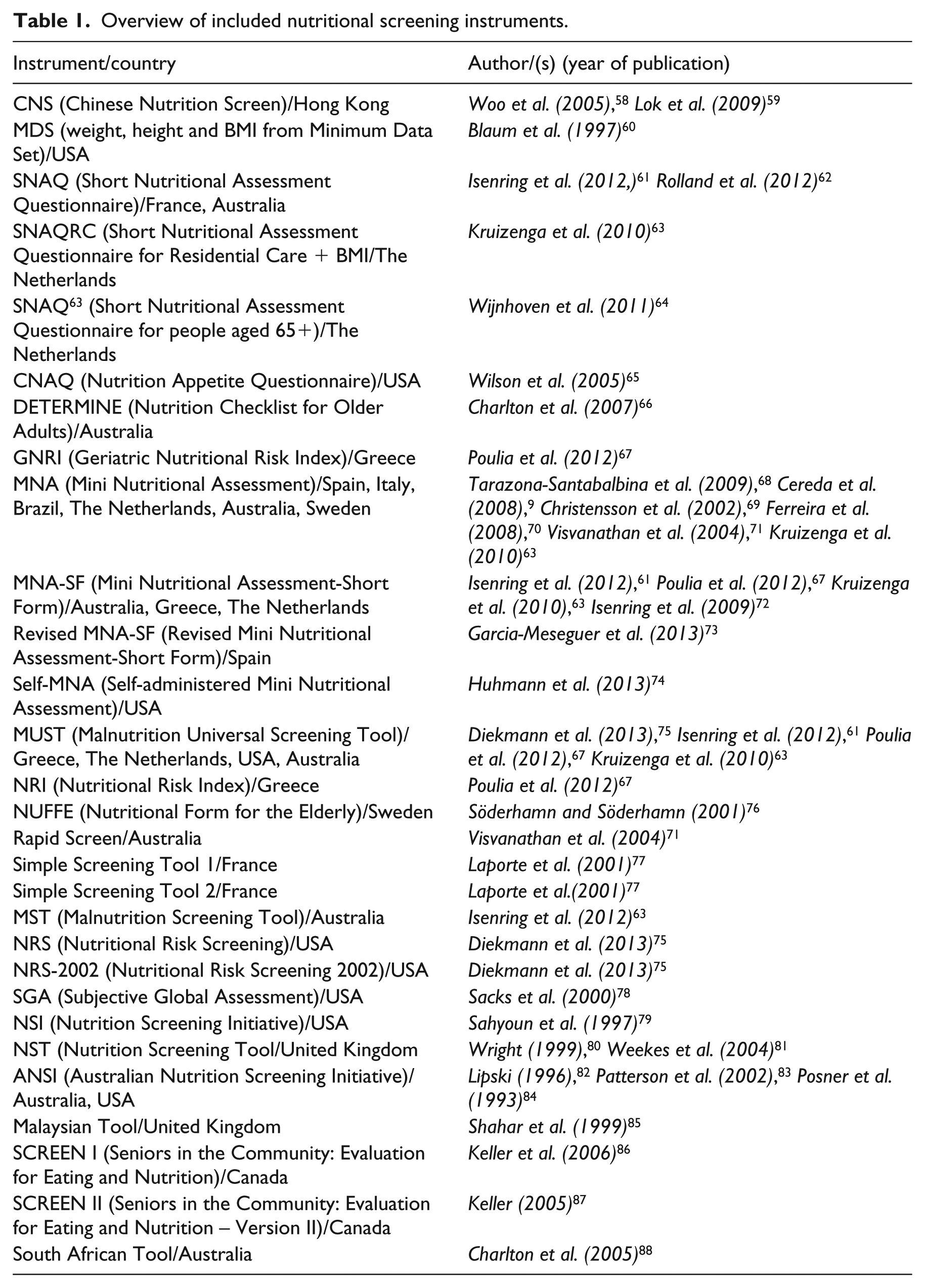
A total of 29 nutritional screening and assessment instruments that have been tested and validated within a primary care setting have been identified and were reported in a total number of 33 studies. The studies included were published between 1996 and 2013 (see Table 1).
Overview of included nutritional screening instruments.
Two consensus documents regarding the views of nutritional experts were identified and included. The studies were published in 2012 88 and 2013, 89 respectively.
No studies including patients’ or relatives’ views or opinions about the assessment of adults’ nutritional status in primary healthcare were identified.
Data analysis
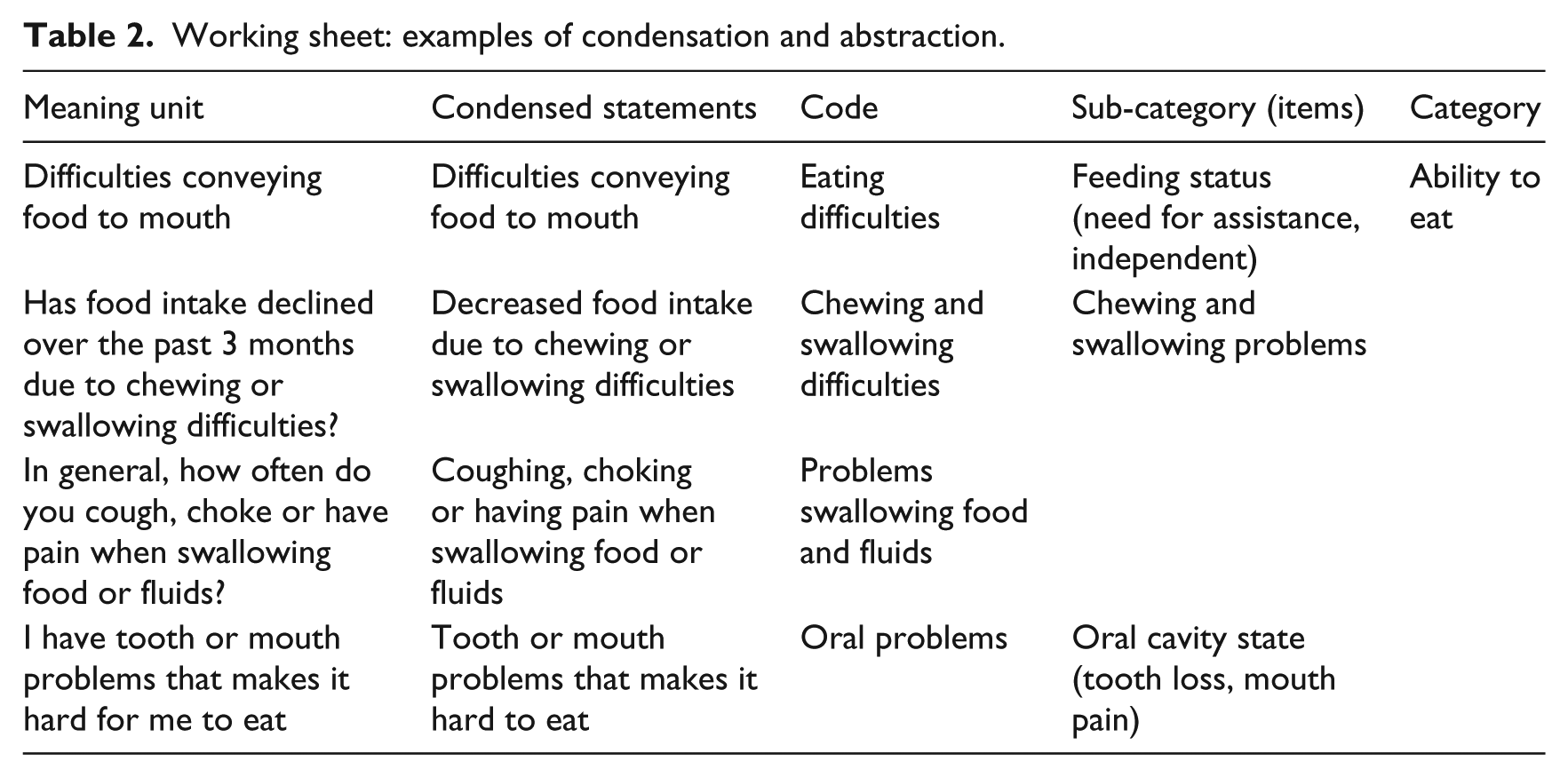
Data were analysed in a manner consistent with content analysis methodology in order to identify those minimum number of items that may have an impact on patients’ nutritional status in primary healthcare. The data included were analysed using inductive content analysis in three steps.53–55 First, relevant data were mapped and extracted in accordance with the three research questions. Second, the data were mapped in a draft dataset where the meaning of the original text related to nutrition was condensed. Where possible, the condensed text typically contained the full information from the original text in order to adequately represent the original meaning. If the original text contained several pieces of information, then a separate condensed statement was created for each piece of information. Information such as ‘Has food intake declined over the past 3 months due to loss of appetite, digestive problems, chewing or swallowing difficulties?’ was divided into three separate condensed statements: (1) Has food intake declined over the past 3 months due to loss of appetite? (2) Has food intake declined over the past 3 months due to digestive problems and (3) Has food intake declined over the past 3 months due to chewing or swallowing difficulties? To analyse and summarize the information about items that may influence nutrition, a coding scheme was inductively developed in group discussion based upon previous work on categorizing MDS. 90 The group consisted of S.J.H., M.B., P.U.P. and A.B. It was also agreed that condensed statements could be labelled by more than one code. Third, sub-categories (stated as items in the following sections and paragraphs) and categories were developed. The analysis was carried out by S.J.H. and thoroughly discussed with M.B. and P.U.P. in order to rule out misunderstandings and maximize validity.
Table 2 depicts a part of the process of comprehensively examining and inductively deriving data.
Working sheet: examples of condensation and abstraction.
Results
In all, 32 meaningful patterns representing variables and items that may have an impact or influence on patients’ nutritional status were identified. From these patterns, five categories were generated to establish the main content of a Nutrition MDS for primary healthcare.
The majority (72%) of the nutritional screening instruments were targeted at patients aged 65 years or older. Furthermore, a majority (62%) of the nutritional screening tools had been tested and validated in a nursing home care setting. Care facilities were typically characterized in the studies as a long-term care facility with multiple levels of care, with residents ranging from functional to very debilitate; 21 per cent of the nutritional screening tools had been tested in a community dwelling population. In these studies, the population had typically been recruited from a geriatrician’s clinic in a community or by other healthcare professionals either providing home care for the elderly or meeting the elderly in the local community centre. The remaining nutritional screening tools (17%) had been tested in care facilities and among elderly residents typically recruited using multiple sources such as facility databases, newspaper advertising or through local contacts. 51
The first consensus document describes characteristics for the identification and documentation of malnutrition in adults in all settings. It was conducted and published by the workgroup compromising people from Academy of Nutrition and Dietetics and American Society for Parenteral and Enteral Nutrition (ASPEN). 88
The second consensus document focuses on assessment and treatment of malnutrition in Dutch geriatric practice. 89 It is a consensus approach through a modified Delphi method, with the participation of 11 geriatricians with expertise within malnutrition. A nutritionist supervised the process and analysed the data from the Delphi study. In this case, they assessed specific actions towards geriatric patients.
The data material reported in total 32 items related to a minimum set of data within the nutritional area in primary healthcare. Five categories were inductively derived from the dataset: (1) physiologic measurements, (2) ability to eat, (3) intake, (4) stress factors and (5) factors which indirectly affect intake and needs.
Physiologic measurements: body measurement of the human individual
Five items have been categorized under ‘physiologic measurements’, as they refer to body measurements of the human individual. Physiologic measurements is a common technique to assess the presence of malnutrition and is frequently represented in the datasources.
Items that have been categorized under ‘Physiologic measurements’: (1) biochemistry (e.g. serum albumin), (2) muscle and fat mass, (3) body mass index (BMI) (weight/height), (4) weight gain/weight loss and (5) nutritional status (both objective and subjective view of nutritional status).
Ability to eat: eating dependency, oral and nutritional health
‘Ability to eat’ encompasses three parameters that can affect patients’ nutritional status. Items that have been categorized under ‘Ability to eat’: (1) feeding status (need for assistance, independent) and need for assistance in self-care, (2) oral cavity state (tooth loss, mouth pain) and (3) chewing and swallowing problems. These can be considered possible barriers to patients meeting their nutritional needs if problems occur with them; hence, a thorough nursing anamnesis seems reasonable.
Intake: quality, quantity and type of food intake
‘Intake’ and the five items included in this category are related to the documentation and observation of quality and quantity of food intake as well as the type of food consumed (diabetic, etc.), which in a large number of the included datasources are considered to be an important part of the management and treatment of nutritional issues.
Items that have been categorized under ‘Intake’ are as follows: (1) types of diet/food avoidances/use of meal replacements, (2) number of daily meals consumed, (3) changes in food intake (reduced/increased intake), (4) daily consumptions of medicine and (5) daily consumption of liquid (including alcohol consumption).
Stress factors: physical and psychological state
For the immune system to function optimally, adequate nutrients must be available. A well-nourished body will not be ravaged by infections the way a poorly nourished body would be. Furthermore, stress (both physiological and psychological) has been considered to have a serious impact on nutritional status.
Items that have been categorized under ‘Stress factors’ are as follows: (1) mental condition/physiological state (state of happiness, mood); (2) medical condition (diagnosis); (3) metabolic stress (presence of pressure ulcer, inflamed skin or skin ulcer); (4) disease presence/co-morbidity and (5) age (>70 years).
Factors which indirectly affect intake and needs: nutrition during particular times in the life cycle, social and interpersonal factors
‘Factors which indirectly affect intake and needs’ has a total of 14 items. These items are a group of factors which may not have a direct impact on patients’ nutritional status, but may indirectly affect intake and needs. For example, the possibility of obtaining food products is not a factor which will independently have a direct effect on patients’ nutritional status, but it may, since patients might not be able to buy food products and rely on other people’s help, hence contributing to poor nutritional status.
Items that have been categorized under ‘Factors which indirectly affect intake and needs’ are as follows: (1) self-rated health status; (2) level of activity (mobility); (3) taste and smell of food and beverages; (4) appetite status (loss of appetite); (5) feelings when eating (feel full, hardly ever full; (6) feeling hungry (rarely, most of the time); (7) eating habits; (8) gastrointestinal symptoms; (9) gastrointestinal functions; (10) living alone, (11) company at meals; (12) reduced social contact/social isolation; (13) possibility of obtaining food products (transport) and access to groceries and meal preparation and (14) economic hardship (economic issues hindering food purchase). Figure 2 reflects how the categories were derived and mapped from the items reported in the data material.
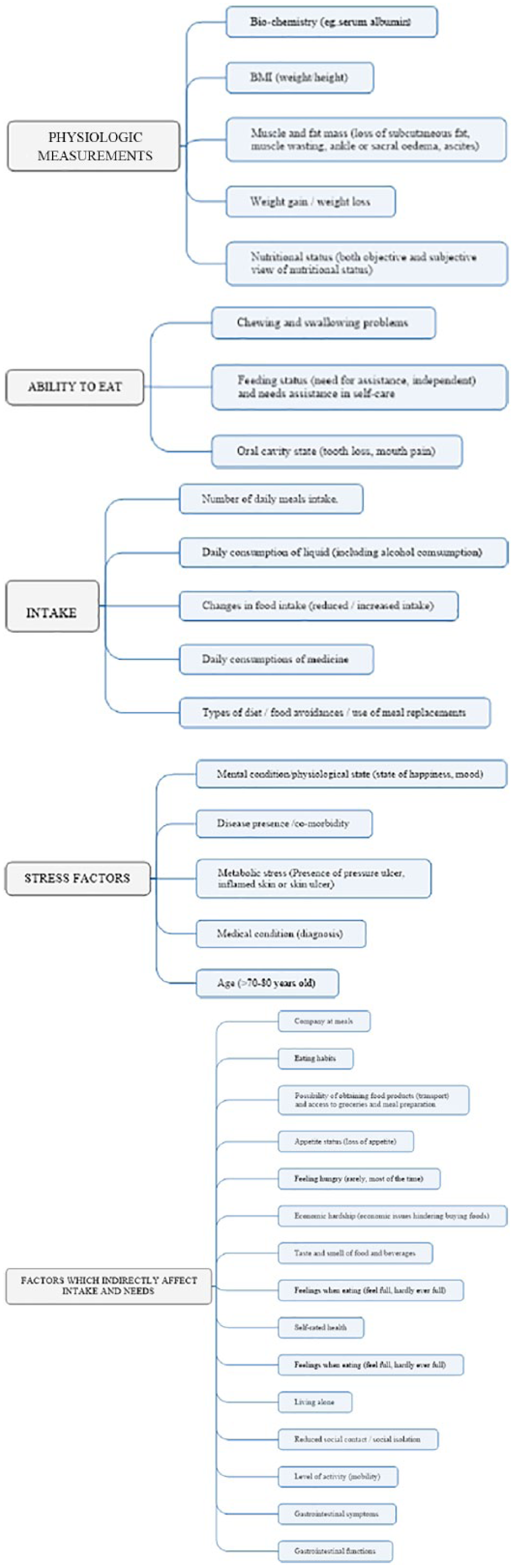
From items to categories.
Discussion
This study reports the analysis of 32 items originally identified using a systematic search of the literature including validated nutritional screening instruments, experts’ opinion and patients’ preferences. Through the development of this Nutrition MDS, it is possible to address some of the concerns regarding inadequate and poor nutritional care practice leading to high malnutrition rates in primary healthcare by providing an overall detailed framework upon which healthcare professionals can base their documentation. The designed MDS is anticipated to drive improvements in the recognition of malnutrition as it contains core data elements that all have a direct or indirect influence on patients’ nutritional status. This set of data differs from existing sets of frameworks in several areas. Primary healthcare professionals have for many years documented the care and treatment they provide using individual and cultural-/context-specific approaches; consequently, there is a wide range of terminology to describe the same nutritional care.91–93 The VIPS model is a Swedish initiative designed to make improvements within this area. 94 It has been translated and implemented in several European countries and has been shown to improve quality of documentation.94,95 This MDS supplements existing frameworks such as the VIPS model, by providing a more detailed common terminology and structure for the documentation of nutritional care. A clinical language and terminology have been developed for it and it may therefore guide healthcare professionals to document their work more accurately and precisely as they will use the same terms to describe the same type of observations, care and treatment. The use of a standard terminology within documentation not only provides guidance and support to healthcare professionals but also allows for the reuse of the data for administrative and research purposes. Several standard terminologies and clinical languages have been developed with the main goal to reuse data and it make comparable,24,96 and several studies have also shown the benefit of these on both quality of documentation and patient outcomes. 24 The high malnutrition rates indicate that only a small proportion of patients who in fact are at risk of malnutrition or even malnourished are identified and have relevant interventions implemented. Several studies support these findings and suggest that nutritional issues remain unrecognized to a high degree. 97 Adams et al. 20 found that 97 per cent were either malnourished or at risk of malnutrition in a sample of older adults. However, only 19 per cent of the older adults were identified by healthcare professionals as malnourished or at risk of malnutrition. 20 This present Nutrition MDS provides a structure based on specified terms, categories and headings. Categories such as ‘Ability to eat’ and ‘Intake’ lead healthcare professionals’ attention and awareness towards potential factors that can have a negative impact on patients’ nutritional status. It therefore expected to not only increase healthcare professionals’ knowledge regarding variables that may influence nutrition but also drive improvements towards the recognition of nutrition problems and support the selection of correct diagnosis and the subsequent planning of nutritional care and treatment and evaluation. Studies have investigated the effects of structured data documentation and found that it led to more comprehensive and multidisciplinary communication regarding patients’ needs and also more detailed information about interventions and actions plans.24,98,89 According to the Donabedian Model, improvements in the structure of care (e.g. a Nutrition MDS) should lead to improvements in clinical processes that should in turn improve patient outcomes. 100 Several studies support these associations and have found a positive effect of MDS on both the processes such as the quality of documentation 101 and subsequent impact on continuity of care and patient-related outcomes.42,102 This study seeks to meet the requirements of other studies stressing the need for a focus on increasing accuracy of documentation and facilitating precise communication among different healthcare professionals in primary healthcare.103,104
Strength and weakness of the study
Previous and current MDS have primarily been developed based on expert opinions by applying different kinds of formal consensus techniques, such as the Delphi Consensus Technique.105,106 This study incorporates different sources of information, and to date, such an approach has not been used as the foundation of a Nutrition MDS in primary healthcare. By using various validated nutritional screening tools as a part of the foundation of the MDS, it encompasses both patient-specific items as well as aggregated data. This Nutrition MDS should not, however, be mistaken for being a nutrition screening tool or being suitable to replace such tools. This MDS should instead be regarded as an overall framework that can guide healthcare professionals to choose, for example, a relevant screening tool that assesses the risk of dysphagia based on the observations done in regard to the patients’ ability to eat. Another strength is the ongoing publication of the different steps in the process of the development of this Nutrition MDS, which enhances its credibility and transparency.
A weakness of this study is that it was not possible to identify any documents on patients’ or relatives’ opinions about the assessment of adults’ nutritional status in primary healthcare. Hence, the patients’ perspective and voices are directly missing from this MDS. Capturing the patients’ perspectives in the documentation and therefore in their own care is an essential part of nutritional care and documentation. 107 Several studies support the fact that healthcare professionals need to implement and use patients’ preferences more systematically in their planning of care and treatment, as patients and healthcare professionals often have different views of the prioritization and severity of problems.29,108 Another weakness is that this generic MDS is based on variables identified in nutritional screening tools where the majority targeted is people aged >65 years. This may be a limitation for the generalizability of the variables identified in the Nutrition MDS and should be assessed with caution.
Implications for practice and research
Sustainability for this study and the results can, however, only be ensured by communicating the results with relevant stakeholders, such as nurses, dieticians, general practitioners and the management in primary healthcare. It is essential that the terminology used within this Nutrition MDS be translated to a clinical language that is understandable and manageable for end users (nurses, nursing aids, dieticians, management). The terminology used to describe the present Nutrition MDS in primary healthcare should be regarded as a scientific approach to developing a generic MDS and be viewed as a theoretical frame for further work within the Nutrition MDS in a clinical setting. Several studies have outlined the difficulties with implementing evidence-based practice, in part due to the terminology used lacking a thorough translation process.39,109,110 Thus, further refinement and development of this Nutrition MDS, for example, by using workshop methodologies with end users and experts within the field, is required. Research that investigates the effect of implementing a Nutrition MDS in a primary healthcare setting is also encouraged.
Conclusion
An MDS within the nutritional area in primary healthcare has been developed using different types of evidence, such as nutritional screening tools, experts’ opinions and patients’ perspectives. In all, 32 items and five categories have been identified and derived, and they appear to be meaningful and comprehensive in the assessment and reporting of adult patients’ nutritional status in a primary healthcare setting. Organizing the documentation in line with the structure presented in this MDS contributes to standardized clinical language and terminology, presumably leading to increased quality of patient documentation, increased continuity of care and improved health outcomes within the nutritional area.
Footnotes
Acknowledgements
Sasja Jul Håkonsen, Preben U. Pedersen, Micah DJ Peters, Ann Bygholm and Merete Bjerrum contributed to conception and design of the study. Sasja Jul Håkonsen involved in acquisition of data. Sasja Jul Håkonsen, Preben U. Pedersen and Merete Bjerrum analysed and interpreted data. Sasja Jul Håkonsen, Preben U. Pedersen, Micah DJ Peters, Ann Bygholm and Merete Bjerrum drafted the manuscript. Sasja Jul Håkonsen, Preben U. Pedersen, Micah DJ Peters, Ann Bygholm and Merete Bjerrum approved the version of the manuscript to be published.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.