
Abstract
Objective
Since the 1990s, almost all healthcare organisations have had electronic health records (EHR) to organise and manage treatment, care and work routines. This article aims to understand how healthcare professionals (HCPs) make sense of digital documentation practice.
Methods
Based on a case study design, field observations and semi-structured interviews were conducted in a Danish municipality. A systematic analysis based on Karl Weick's sensemaking theory was applied to investigate what cues HCPs extract from timetables in the EHR and how institutional logics frame the enactment of documentation practice.
Results
The analysis uncovered three themes: making sense of planning, making sense of tasks and making sense of documentation. The themes illustrate that HCPs make sense of the digital documentation practice as a dominant managerial tool designed to control resources and work routines. This sensemaking leads to a task-oriented practice which centres on delivering fragmented tasks according to a timetable.
Conclusion
HCPs mitigate fragmentation by responding to a care professional logic, where they document to share information and carry out invisible work outside of timetables and scheduled tasks. However, HCPs are focused on solving specific tasks by the minute with the possible consequence that continuity and their overview of the service user's care and treatment disappear. In conclusion, the EHR system eliminates a holistic view of care trajectories, leaving it up to HCPs to collaborate in an effort to obtain continuity for the service user.
Keywords
Introduction
This article presents findings from a study on local sensemaking of digital documentation practice in municipal healthcare. We argue that digital documentation practice contributes to the fragmentation of care trajectories in municipal healthcare. However, healthcare professionals (HCPs) somewhat mitigate the effects of this fragmentation by enacting a documentation process framed by care professional logic and performing invisible work.
Background
Since the 1990s, almost all healthcare organisations in Denmark have had a digital system to organise information, treatment, care and finance1,2 making the electronic health record (EHR) a central digital component of healthcare practice. In Denmark, the implementation was driven by a political and managerial expectation that digitalisation would promote continuity in service users’ care trajectories. 3
The EHR is a digitised format of medical records, 4 focusing on longitudinal trajectories within care, treatment and nursing in municipal healthcare. The digitisation of the records is expected to achieve more efficiency in healthcare systems and gather, manage and share service user information to support clinical decision-making for HCPs and increase service user satisfaction.2,4 Although it is well recognised that EHR systems have the potential to improve clinical outcomes and efficiency,5–7 the benefit realisation awaits, partly due to organisational issues, such as workarounds in the HCPs’ digital documentation practice. 8 As such, digitising documentation and subsequent workflow does not come easy in healthcare systems. Østensen and colleagues 9 show that nurses’ information practice in municipal healthcare is highly complex, affecting how and when information is produced, written down and shared with others. Hansen and colleagues 10 suggest that HCPs have a negative attitude towards digitalisation due to changing power structures. The complexity of healthcare services is well known on a global scale; however, it remains unclear how HCPs, in general, make sense of digital documentation.
Furthermore, some studies indicate that the digital evolution of the EHR comes at the price of fragmenting information and tasks.11,12 Some studies show that the EHR ought to be a support but ends up being an obstacle,9,13 while Dahl 14 suggests that HCPs experience daily dilemmas and paradoxes, as new approaches such as ‘everyday rehabilitation’ are introduced with the paradigm of neoliberalism within elder care.
In a previous documents analysis, we showed that the digital documentation focused on the organisational management of health and described a potential task-orientated practice supplied by an anonymous HCP. 3 In this study, we focus on how HCPs make sense of the abstract political and managerial ideas in their concrete documentation practice. In doing so, we are inspired by Karl Weick's sensemaking theory. 15 Sensemaking comprises two parts, where the first part ‘sense’ refers to the meaning and the second part to ‘making’ refers to the process of construction. 16 Sensemaking occurs when incongruence, paradoxes or dilemmas appear in HPCs’ daily practices. 15 When situations become equivocal, people will try to make sense of and enact this sense back into their world of healthcare practices to establish order. Hence, organising and sensemaking are two sides of the same coin. 17
Digitalisation of healthcare
Recent studies indicate that digital solutions are often immersed in an uncritical discourse, with expectations that technology and digitalisation will reduce costs and expenses.18,19 Frequently, these expectations are ‘over-optimistic’ 20 and, according to Dahl, 19 are properly grounded in a fear of the care crisis in the Nordic welfare states, where demographic changes and lack of personnel threaten municipal healthcare. Kovalainen 18 argues that care is commodified, leading to a production logic within care work. For many years, New Public Management (NPM) has been the primary driver of management in healthcare, inspired by tools such as Lean, Total Quality Management (TQM) and scorecards. 21 Accordingly, Lenz 22 points out that the discourse on digital technologies fits perfectly in a modern society, where digital solutions are perceived as beneficial to all parties involved, even though there are some concerns regarding sustainability and data concentration within big tech companies.
Baudin et al. 23 argue that there are quite different perceptions of technology in healthcare. The authors find a form of resistance among municipal HCPs, as they are often not directly involved in the processes during implementation, even though they have in-depth knowledge and practical, front-line experience with elder care. Schwennesen 24 examined how technology may be perceived as a digital stand-in for HCPs in physical rehabilitation but found that neither service users nor HCPs changed their usual work practices. Technological advances are extensively studied in relation to welfare technology, such as medication dispensers, 25 automation 26 and robotics.27,28 However, many of these studies indicate that it is necessary to direct attention to organisational and societal structures when examining the digital transformation of healthcare. Thus, it seems evident that digitalisation is changing municipal healthcare. However, how HCPs implement digital documentation systems in local contexts remains unexamined.
Focus and aim
Orlikowski 29 argues that human action can change technology in practice. Consequently, digital technologies in the form of the EHR have no fixed structure and no predetermined effect on HCPs’ practice. Instead, digital technologies are enacted into practice and have implications for the organisational outcomes. 30 Based on Weick's theory on local sensemaking, the aim was to understand how HCPs make sense of digital documentation practice in municipal healthcare.
Methods
Sensemaking, cues and institutional logics
According to Weick, 15 sensemaking is a reciprocal process with interacting actors who enact practices and their surroundings which are made meaningful by the extraction of cues in an ongoing cycle. This forces HCPs to enact the documentation process in a social context with various logics and extract cues from their surroundings, for example, from co-workers, management, service users and the EHR.
Processes of sensemaking consist of seven properties that can form the basis for the exploration of how organisations interpret and manage change. Weick
15
(p. 17) understands sensemaking as a process that is:
grounded in identity construction; retrospective; enactive of sensible environments; social; ongoing; focused on and by extracted cues; and driven by plausibility rather than accuracy.
According to Weick,
15
a cue is a simple, familiar structure that functions as a seed for a sense of what is going on. Thereby, a cue functions as a point of reference. Weick
17
argues that the faith in cues and the sustained use of these cues as reference points tie elements of sensemaking together when people enact practices as if the cues were real. What an extracted cue might become depends on the context in two ways: firstly, context frames the extraction of the cue. How and if people notice a cue is the first step; if a cue is not noticed, people will not make sense of it. Secondly, context affects interpretation, indicating that the interpretation of cues takes place in a social, institutional and cultural context.
15
We operationalise contextual framing as institutional logics. According to Thornton and Ocasio, institutional logics is ‘The socially constructed, historical patterns of cultural symbols and material practices, including assumptions, values and beliefs, by which individuals and organisations provide meaning to their daily activity, organise time and space and reproduce their lives and experiences’.
31
Thus, HCPs act in a field of expectations, norms and values. Research on institutional logic shows that HCPs apply a vast range of logics in daily practice.32–35 Inspired by Frederiksen and Beedholm,
36
we operationalise Weick's concept of cue framing in four salient institutional logics:
Public management logic Market logic Medical profession logic Care profession logic
The public management logic relates to public administration with a focus on legitimacy and policy. The market logic relates to finance and focuses on productivity and efficiency. The medical profession logic relates to medicine and focuses on cure and professional judgement. The care profession logic focuses on care and professional judgement. As such, we applied the perspective of institutional logics to specify salient contextual framing in the Danish healthcare context.
Case study design
The study was designed as a qualitative single-case study 28 conducted in a medium-sized Danish municipality with ∼44,000 residents. The issue for the case was digital documentation practice in municipal healthcare, structured by the documentation process of the common language platform (CLP). The municipality represented an ordinary municipality that did not differ from the majority of municipalities regarding size, organisation, devices or staff. 37
Denmark is divided into 98 municipalities. 38 The local authority of the municipality is responsible for elder care, home care, home nursing and rehabilitation services. Services are tax-financed and primarily delivered by HCPs, such as nurses, nursing assistants, social and healthcare helpers, occupational therapists and physiotherapists.39,40
Denmark has had a digital agenda for the public sector for quite some time, with the latest strategy opening on digital documentation with its main argument: ‘It should not fall on the individual patient or relative to carry information about treatment and medical history through the health system. Patients and relatives must be able to rightly expect that the healthcare professionals with whom they interact are familiar with the relevant information […] required for treatment and for ensuring peace of mind and an experience of a coherent health system.’ 41 This vision is operationalised with the CLP, a documentation method that is aimed at the fundamental structure of all EHR systems in Danish municipalities. As such, all HCPs in Denmark use the same documentation method, regardless of their roles, IT supplier, use of devices, local organisation, etc.
CLP was initiated in 1998 by Local Government Denmark. The first step consisted of a standardisation of healthcare services to ensure, for example, that HCPs working in the home care/nursing services use the same vocabulary and terminology in Danish municipalities. 42 From 2004, CLP was integrated in the digital development of the municipal EHR. 43 CLP was further developed by Local Government Denmark and operationalises current digital strategies, legislation and policy. The method is described in a Method Handbook, 44 developed to guide users on correct documentation practices in the municipalities. CLP is based on a generic process model, which specifies organisational steps in relation to the documentation process. The process is illustrated in Figure 1.

Common language platform.
Steps 1–3 cover the authority process, where HCPs who have trained to become care assessors open the case (1) and make an assessment of the service user's care and treatment needs and functional capabilities. The assessment is documented in the EHR in standardised fields entitled ‘Functional conditions’ and ‘Health conditions’ (2). The care assessors make decisions (3) on the health and care services that the individual service user should receive, how many minutes per day/week and for how long as well as the required qualification of the HCP providing the care. They forward this information to the planners (4), who plan visits in a planning module of the EHR on a daily basis for the HCPs visiting the service users in the particular municipality. HCPs receive this as a timetable in the EHR that shows a daily schedule from 7.00 to 15.00, listing the individual tasks they have to provide (5) at the particular service user's home. HCPs update information in the EHR with observations (notes), instructions relating to, for example, wound care, visiting plan and general information on the service user, next of kind or other relevant information. In addition, nurses and occupational therapists are required to follow up (6) on ‘Health conditions’ and ‘Functional conditions’.
In the municipality used for the case study, each organisational group represented separate steps of the documentation method. Care assessors had responsibility for steps 1–3; planners were responsible for step 4, and the different units were responsible for step 5. Step 6 was the joint responsibility of the parties involved.
Recruitment and sampling
The collection of contextual data17,45 took place between March and December 2021. Potential participants were informed about the study at a staff meeting and subsequently invited by managers via e-mail. It was voluntary for the HCPs to participate. In addition, we selected participants who represented the different organisational fields in size and function. To achieve a diverse sample of HCPs, we employed purposeful sampling as suggested by Campbell et al. 46 with the following inclusion criteria: qualified HCPs and non-manager, experienced in homecare and employed for an extended period of time.
Twenty-three HCPs (22 female and 1 male) participated in the study with different educational backgrounds: 6 nurses, 5 nursing assistants, 2 occupational therapists and 10 social and healthcare helpers (see Table 1). Before data collection, every participant was asked to re-read the information document and give written consent to participate. Approximately 124 h of field observations were conducted in the spring of 2021 over 17 weeks. Sixteen HCPs were shadowed during their daily work, and we conducted interviews with 15 HCPs during the autumn/winter of 2021. Ten HCPs are quoted in this paper under pseudonyms.
Participants.

Field observations. Based on Cato Wadel's 47 description of doing fieldwork in one's own culture, the first author took on the role as an apprentice 48 and accompanied HCPs during their shifts. The observation guide was based on Wadel's 47 principles of being relational, empty and elementary. As such, HCPs showed the first author their habits, routines and practices during their daily work. Accordingly, the observations took place in service users’ homes as well as in the municipal cars, driving from one service user to another. Field observations lasted between 5 and 8 h and corresponded with the HCP's shift from start to finish. In addition, a few staff meetings and service user conferences took place during the data collection. Field notes were hand-written on paper and transcribed into Word afterwards.
Interviews. Based on Kvale and Brinkmann's 49 methodological framework, interviews took place at HCPs’ local workplaces at the end of their shifts. Interview questions were based on existing literature on documentation practice and reflections on field observations. Interviews concerned participants’ experiences with documentation and how their practice played out in their daily encounters with service users, colleagues, technology and organisational factors (see Appendix – Interview guide). Every interview began with a short informal talk on function, professional background and length of service in the municipality. If the HCP had participated in field observations, the interview was initiated by exchanging reflections on the day. HCPs were then asked questions on how they applied the documentation system in their daily work routines and on their reflections on different aspects of the documentation processes, such as reading, writing and searching for information. Interviews had to fit in with participants’ work schedules and lasted between 55 and 95 min. Interviews were transcribed verbatim by the first author.
Data analysis
The concept of sensemaking in organisations allowed us to assess the HCPs when placed in a state of uncertainty related to the current digital strategy of documentation practice. The analysis of interview and field data was conducted in an interplay between theory and data. 50 We began with codes and categories emerging from data and then moved on to theoretical concepts to understand how HCPs made sense of the digital documentation system (see Figure 2). Firstly, we carried out a close reading of field notes, transcribed interviews and collected material. Secondly, we looked for contradictions, paradoxes, connections and surprises in the material. With Weick's theory of sensemaking as a theoretical lens, we identified general themes. As such, sensemaking theory served as an ‘observer's manual’ to identify findings. 15 During this phase, we searched for patterns in the material to identify relationships among the properties which indicated sensemaking processes. In the fourth phase, we established themes, presented as findings. For example, ‘time’ appeared to be a central cue for sensemaking in relation to framing the care work and documentation processes. For instance, the user interface of the EHR entailed that the timetable was always presented as the first information for the HCPs on their screens. As such, the timetables stood out as a particularly important provider of cues, initiating sensemaking processes for the HCPs.

Analysis process.
In the following sections, we will first describe the timetable as a technological artefact saturated with cues placed by management, politicians and so on. Then, we will present our findings as to which cues the HCPs notice, their interpretation of cues and how the cues are framed by logics, leading to the enactment of a certain kind of digital documentation practice.
The timetable as a technological artefact
Orlikowski 29 describes that people draw on different properties in a technological artefact in addition to their embeddedness in the institutional context. Properties may be hardware, software, user interface, features, etc.
When the HCPs logged into the EHR on their different devices, the timetable was the first information presented to them. On a tablet, the timetable was supplied with information on team tasks and correspondence from GPs or the hospital. This information was not available on mobile phones. The headline on both devices was ‘My tasks’. The timetable was generated on the basis of the planner's work in the planning module of the EHR. The planners received the allocation of the service from the care assessor level and did the actual planning for a team of geographically organised HCPs. Timeslots on the timetable were allocated by planners, and the HCPs could not alter this but could make the visits in another order. Below, we illustrated a segment of a timetable from home care, which would normally run from 7.00 to 15.00. Figure 3 is an example of a timetable, inspired by field studies.
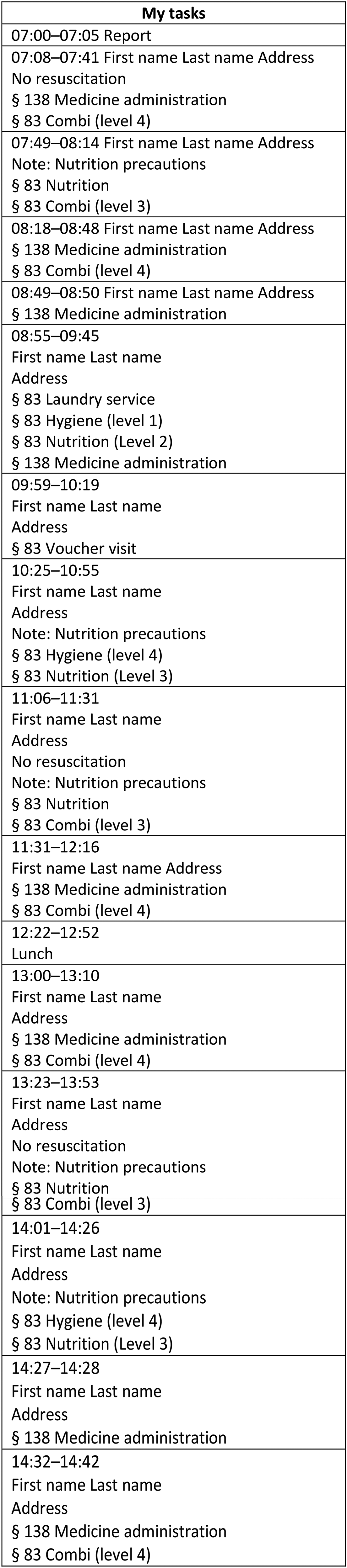
Timetable, home care.
When a visit was completed, the HCP would mark the visit as ‘delivered’ by pressing a green tick on the right-hand side of the timetable. Transport time between visits was automatically calculated by the EHR system. There was never any time in the timetable that was unaccounted for, as every timeslot had a headline. HCPs could only see their own timetable, not their colleagues’ timetables. Only the planners could see the timetables for the entire team. As a result, many teams used the workaround of taking pictures of the HCPs’ printed timetables and sending them to the HCPs at work that day. In general, services were labelled ‘tasks’, and when an HCP sent notes to another HCP in the EHR, it was also labelled as a ‘task’. The HCPs called the timetable their task list or driving list.
Findings
The analysis revealed three distinct themes within HCP documentation practice: making sense of time planning, making sense of tasks and making sense of recordkeeping.
Making sense of time planning
Planning time was a point of reference for planners and HCPs. For the planners, the main job function was managing time and planning timetables for the HCPs as efficiently as possible. Planners received timeslots in the planning module from the care assessment department. Initially, the module did not show background or additional information about the service, just a task and time allocation. When the planners worked with the timetables, the slots would appear on the screen as a small block in a calendar format, which they could move around on different timetables, named as geographical sites or with specific HCP names. Thus, the planner enacted a documentation practice, where they planned timeslots in the timetables for the municipality, divided by teams and HCPs.
Planners focused on planning timeslots in timetables. They had a narrow focus on the task's scale in minutes and not on the content of the task. Hereby, the planners’ interpretation of time was framed by the public management logic and market logic, as time allocation for services was closely connected to the efficient use of resources controlled by others. The planners did not have any power over the amount of time allocated. This was assessed and decided on by another organisational actor – the care assessment department. Thus, planners did not have any organisational insight into the rationale for assessing time for the tasks allocated by the care assessment department. Planners expressed frustration about the newly allocated timeslots but planned whatever came in on their lists. For instance, when a planner explained:
‘They [the care assessors] have also cut the time. Now we get seven minutes instead of fifteen’.
‘But that's very specific to have to assess the help as seven minutes. How do they do it?’
‘I don’t know. They probably have a catalogue’.
‘For the care visit?’
‘Yes’.
(Field note, Ulla, home care, planner)
In addition, the planners had to make sure that all requested services were planned. They needed to make sure that services were planned as tasks in the timetables, even when staff were off sick or there was a mismatch between supply and demand, which is illustrated in this fieldnote: When an HCP calls in sick, the planner moves the visits around in the planning module. She says she can’t book a substitute but will try to work it out. She moves visits around between the HCPs. Sometimes she moves the visit back again. She places the visits very close, thereby removing the time between visits. This is ‘transport time’ calculated by the system. It is the time allocated for the HCP to get from one service user to another. In addition, she opens a visit – a ‘voucher visit’ and removes ten minutes of the calculated time, so the visit (and the slot) becomes smaller. (Field note, Inge, home care, planner)
As such, it was not an option to leave out tasks if they ran out of personnel. In such cases, they altered standardised timeslots, adjusted assessment or circumvented the system's automatic calculation of transport time: In the office, the planner is moving the services around on the plans; she is unsure whether she should book a temp for the morning visits or whether she should cut timeslots and transport time. She says: ‘Sometimes it's cut a heel and chop a toe’ (Field note, Dorthe, home care, planner)
The planners made sense of the documentation practice as a planning practice by ensuring that all tasks were planned. They focused on allocating the tasks to the available timeslots, even if they had to alter and adjust the services that the service users had been assessed to require. They were never in a position where they could increase time, but they would often decrease the time per visit to get the puzzle to fit. They would never leave out a task, even if they actually did not have enough resources to meet the demands. Instead, they deliberately pressured HCPs by planning timetables that were obviously unrealistic, which ensured that all tasks were delivered ‘on paper’, even though the reality was inevitable service reductions for service users when tasks were reduced and a difficult working environment for HCPs when transport times were altered to zero minutes. As such, planners enacted a planning practice which framed the HCPs’ work as a special practice and zoomed in on delivering tasks on time. The planners made sense of the timetable as a task list that was unrealistic timewise for the HCPs, as there were no other options in the organisational context.
Making sense of tasks
HCPs had their time structured by the timetable. When an HCP finished a task and left the service user's home, she opened her timetable. In the timetable, there was a mark on the right-hand side of the designated task. The HCP swiped this mark, thereby marking the visit as delivered or ‘swiped’. All HCPs marked their visits. Marking the visits was a way of indicating that you were doing the tasks, as illustrated in this field note, where Lonnie, a nursing assistant, checks if she marked all her tasks: Lonnie has finished all the tasks for the day. Finally, she opens the timetable and goes through it. During the day, she marked all tasks as delivered. Therefore, every task is marked with a green circle to the right of the task. (Field note, Lonnie, nursing assistant)
As all the HCPs’ timetables were tightly planned, extra visits as a result of medical alerts or calls overlapped scheduled tasks. When HCPs were behind schedule, the HCPs extracted time as a cue framed by the efficiency demands embedded in the market logic. They solved this by simply ‘catching up’ by themselves. They never called the office or a colleague to ask for help but were intent on delivering care no matter how their own working environment was affected, thereby also drawing on the care profession logic framework, leading to daily dilemmas. The HCPs responded to service users’ needs when they assessed that this was necessary. In these situations, they decided to stay longer in the particular service user's home and hereby circumvented timeslots. However, they were very much aware that this practice could not be justified to the management: Rikke started to move faster to her car. She said: ‘Now we’re about a quarter of an hour behind. But I’m really bad at walking out when they need to talk’. (Field note, Rikke, social and healthcare helper)
As such, the HCP managed by operationalising the task list as precisely as possible. If they did not follow the designated timeslots, they simply began to move faster, drive faster and skip corners in order to finish the timetable on time. Often, they cancelled their own breaks or toilet visits. In many cases, HCPs compensated for the unrealistic timetables by preparing from home: But a lot of people do [read the EHR at home]. I don’t like to be unprepared. Umm… so when I […] eat my breakfast, I turn on my phone. Then I look at my task list. And that's not really right, as I don’t get paid for that, but I don’t care, because I would rather be well prepared. And then I just check quickly to see… if there's anything about any individual service user. (Interview, Birthe, social and healthcare helper)
As the quote indicates, HCPs from time to time acted in accordance with the care profession logic by for example doing work from home. However, as the market logic framed documentation practice as the overall condition, this led the HCP to mostly sticking to tasks and timeslots on their timetable. As such they continuously mediated between logics.
The task as a cue for actions in the service user's home led to a task-oriented documentation practice, where the HCPs swiped the visit or marked it as ‘delivered’ as their documentation. This enactment of documentation practice was performed when the HCPs made sense of the task as was expected by themselves and the care assessment – nothing more and nothing less.
Making sense of recordkeeping
From time to time, HCPs did not just swipe the visit but made the judgement that they needed to communicate with others. In such situations, they pressed the ‘ + ’ on the task list and chose to open an observation. Occasionally, they would also send this observation to someone else in the organisation. As such, HCPs enacted recordkeeping as a documentation practice, where they actively wrote health professional information in the EHR.
This enactment was framed by three logics, which independently framed the documentation practice with different nuances. HCPs often knew the service users very well. They sometimes visited the service users several times a day over the course of many years. HCPs enacted a documentation practice where they wrote information in the EHR in order to share this knowledge with other HCPs. They extracted the task as a cue, interpreting it as a ‘deviation’ and labelled it as such, framed by the care professional logic, the public management logic and the medical profession logic. The logics framed the specific kind of documentation that the HCPs recorded in the EHR.
The public management logic framed the documentation practice on account of the close connection between health professional authority and political attention in respect of the EHR as a source of quality assessment. HCPs who held an authority registration were aware that they were legally obliged to document their actions in the EHR. During an interview, a nurse stated that she sometimes opened the EHR at home in her leisure time. When asked why, she explained: Because you have to cover your own ass, you know? Because if something goes wrong, then I must have documented that this particular service user was given this and that medication. (Interview, Annika, nurse)
This indicates that within the public management framing, the HCPs extracted the task as a cue, which they interpreted into legally based documentation for the purpose of justifying their actions in the trajectory.
As described above, the HCPs labelled certain situations as a ‘deviation’. A deviation was interpreted as a situation that was different from the one the HCPs had expected, for example, when the service user's treatment did not have the expected effect, when the service user's mood was low or when the service user did not drink or eat sufficiently. The deviation was a justification for documenting beyond the swipe: I only write a note when I notice a deviation […] we write far too much, and I have done so myself, and it has really helped to remember that I should only write a note, if there is a deviation, because I used to write several notes every day. (Interview, Sofie, social and healthcare helper)
This indicates that documentation was considered a time-consuming task, which did not necessarily lead to value for the service user. This suggests that the HCPs were mindful of a deviation from what was expected when they assessed the situation in the home as a whole. They focused on the service user's trajectory, and when a deviation from the expected occurred, they documented it by ‘opening an observation’ (writing a note in the EHR). Thus, the label ‘deviation’ was a justification for spending time on documentation.
The care professional logic framed the second type of documentation practice within this theme. During the field studies, it was clear that the relationship between HCPs and the service users was characterised by shared experiences framed by the care professional logic. The HCPs had knowledge of the service users and their entire situation at home. They regarded the task as a cue to what to expect, framed by the care professional logic. In this example, Rikke draws on her knowledge to asses if the situation at the service user's home matches the task: We enter the home, and Rikke is greeted by a married couple who are very friendly welcoming her and seem pleased to see her. Rikke greets them back in the same manner; they know each other from before as members of the same association. She follows the service user down the corridor and sits on a low stool in front of a footstool by an armchair. Rikke asks questions while helping the service user. She looks around and talks to the service user while helping to put on the socks. She strokes the legs up and down, checking for any folds – it looks as if she does not even think about it. (Field note, Rikke, social and healthcare helper)
HCPs interpreted the task as a broad indicator of the situation at the service user's home. As such, the specific task was one point in the overall picture, which the HCPs knew from previous experience in the home. HCPs documented their observations to pass on information to other HCPs on the service user's trajectory. All HCPs articulated this rationale for documentation; here stated by Anne Sofie: [I write notes] to avoid service users having to repeat themselves many times about their current situation, but also to ensure that my colleagues have the best possible basis for meeting the service user in the best possible way. And thus get the best possible trajectories. And make sure that the service user feels heard and seen …and feels there is continuity and that we remember to talk to each other across professional groups and work areas. (Interview, Anne Sofie, nurse)
If the HCPs did not know the service user, they searched the EHR for information. This indicates that if the HCPs did not have knowledge of the service user and the situation, the task was an ‘empty’ cue, leading them to search for information. HCPs felt obliged to obtain information before entering the home and to share knowledge with each other. During interviews, JDJ asked the HCPs when they would write in the EHR. Marianne, a nurse, stated: …Well, whenever I think there is some information that needs to be passed on. I am not documenting just to be safe, you might say. Because, if it's described in the instructions what to do and I think that's what I’ve done, then I just swipe. (Interview, Marianne, nurse)
Marianne's statement is an indication that providing information is important, because it might be relevant to other HCPs that take part in the service user's trajectory. Many HCPs articulated that writing notes in the EHR were related to sharing information on the trajectory to benefit the service user: It's for the sake of the service user that we document. And, of course, for colleagues, too. You know, I have to write stuff, so it can be understood…and yes… That's what I think is the most important thing. (Interview, Birthe, social and healthcare helper)
Birthe states that information needs to be written down in such a manner that her colleagues understand and can base their actions on this information.
The medical profession logic framed the third type of documentation practice within this theme. HCPs documented in a traditional health professional manner on specific treatments. The HCPs extracted the task with the extra layer of the legal basis for the service. When this was within the Danish Health Act, HCPs would often document in relation to the specific treatment. When they documented medication services, the HCPs always documented all actions, and the documentation practice was standardised in specific fields and with the use of ticks in the system. When HCPs documented on, for example, wound care, they would describe the treatment with health professional terms and language. For example, Anna documents on a visit about wound care: She creates an observation ‘Wound treatment’. Here she uses predefined options. She structures her text according to the ‘TIME’ model. It is a professional description of the wound.
(T = Tissue, I = Infection/ inflammation, M = Moisture (moisture/ secretion), E = Edge (wound edges)
(Fieldnote, Anna, nurse)
HCPs always had to justify the time spent on documentation, leading to labelling most recordkeeping activities as ‘deviations’ framed by the public management logic. In addition, they based the rationale for documentation in the care professional logic when they extracted the task in the timetable as one point in the trajectory, indicating that they had to share information with each other to ensure the service user's experience of continuity. Within the framing of the medical profession logic, documentation was characterised by treatment, such as wound care. HCPs extracted the task as a cue to medical treatment and interpreted this as a part of the professional trajectory with the object of curing the condition.
Documenting healthcare
Sensemaking processes of documentation practice are intertwined and occur in a daily flow. Our analysis shows three distinct themes associated with sensemaking processes of documentation practice, as illustrated in Figure 4.

Sensemaking processes: overview.
Combined, the themes illustrate that HCPs make sense of the digital documentation practice as a dominant managerial tool designed to control resources and work routines. This leads to a task-oriented practice which centres on delivering tasks according to a timetable. As the HCPs are also driven by medical and care professional logics, they respond to service users’ needs and professional judgements, hereby enacting a traditional documentation practice that centres on sharing information on treatment and care trajectories with colleagues. When this occurs, they justify spending time on documentation by labelling it a ‘deviation’.
Discussion
According to Weick, sensemaking is best seen when there are dilemmas on the line. 15 The results show that HCPs extract several cues when they try to make sense of a documentation practice characterised by dilemmas.
An obvious dilemma for the HCPs seems to be between the HCPs’ norms on sharing information and the user interface in the EHR. As described in the findings, HCPs extracted cues from tasks and time in the timetable and labelled it a ‘deviation’. The deviation was a label applied to justify spending time on documentation, which they reasoned that they needed to share with other HCPs engaged in the trajectory. This sensemaking was framed by several logics, namely, the market logic, the medical profession logic and the care profession logic. It seems that the HCP's initial urge to write a note in the EHR stemmed from the care profession logic and the medical profession logic. This draws back to the notion of recordkeeping as an information-sharing practice among HCPs, much in line with suggestions made in previous research by Petrakaki et al. 2 and Eklöf. 51 Over time, the term ‘recordkeeping’ has been replaced by the term ‘documentation’ to define the process of submitting written information between HCPs. 3 As such, ‘documentation’ is a broader activity, which also includes data production for managerial purposes. Still, the rationale for recordkeeping (writing a note) is that healthcare information in the EHR increases the quality of treatment and underpins the relationship between the HCP and the service user. When documentation becomes a ‘deviation’, the cue is framed in a market logic. This draws from the rationale that time is a resource, and resources need to be spent efficiently. Within this logic, documentation is a potential waste of time, as it is time spent away from direct treatment or care.
As sense is dependent on several properties, research implies that it is possible to engage in strategic sensegiving, where an actor attempts to influence other actors’ sensemaking processes. For example, Bansal 52 has examined how sensemaking and sensegiving are intertwined during acquisitions. Other research has examined sensegiving among managers at different levels and how it is possible to achieve strategic sense in an organisation.53,54 Consequently, it is possible to view the user interface of the EHR and timetable as a strategic action taken to imply certain sensegiving processes inherent in the documentation practice. The user interface in the EHR and the technological structure of the timetable can be viewed as a strategic action from the political level. Hereby, the technological artefacts function as a means to exclude HCPs as a ‘human error’ in municipal healthcare, not unlike autopilot systems in aeroplanes, which potentially reduce pilots to ‘sense-less’ actors. 55
Davina Allen has done substantial work on organising practices within care work.56–60 She has developed the care trajectory framework, which offers a conceptual and theoretical foundation for organising care work.57,61 Allen argues 61 that nurses have an important role as ‘glue’ in the healthcare system, as they make sure different elements are aligned in trajectories. This was examined in a Danish context by Norlyk et al. 62 They argue that care trajectory management is an undervalued part of care practice. Similarly, we find that HCPs make sense of documentation activities as an activity that takes time from direct care and thus have no value in care work. Our findings indicate that for all HCPs, making sense of documentation practice is characterised by invisible work, which remains unaccounted for in an otherwise data-driven organisation. It appeared that the deletion of transport time was a common practice among planners and accepted among HCPs. In general, HCPs started their work at home and skipped breaks in order to fit everything in. This practice was invisible in the timetable. Accordingly, time spent on coordination activities, such as information on treatment, general state or concrete care activities, had to be justified by using the label ‘deviation’ and was largely ‘funded’ by HCPs giving up their free time, breaks and transport time. Our study supplements the results by Norlyk et al. 62 on the invisibility of trajectory management work in home care by demonstrating that HCPs perform both invisible and unpaid work.
It is common that HCPs establish workarounds to coordinate care work, such as communicate by telephone instead of the EHR to ensure cross-sectorial trajectories. 63 Many studies have confirmed that workarounds are a common feature of documenting in EHRs.64–66 It seems that the establishment of a workaround is often related to organisational issues, such as the distribution of responsibilities and tasks. In healthcare, workarounds are persistent practices performed by HCPs to get things done in a system short of resources. 67 During the case study, we noted that a particular group did not answer to the same management practices as the rest of the organisation. The rehabilitation team, which consisted of occupational therapists and physiotherapists, made their own care assessments and timetables. They had an increased amount of time allocated to read the EHR before visits, wrote a larger amount of text in the EHR and had fewer and broader standardised fields in the EHR. The rehabilitation team expressed the same rationale for writing information as other HCPs but had a very different organisational setup. As such, the market logic did not frame the rehabilitation team's sensemaking. This is probably due to a political prioritisation of rehabilitation plans as a means to achieve healthy ageing and self-help. 68 However, as all groups of HCPs had tasks in the longitudinal trajectories, thorough documentation on rehabilitation plans and strategies was often left unread in the EHR, as nurses, nursing assistants and social and healthcare helpers focused on delivering specific tasks by the minute with the possible consequence that continuity and their overview of the service user's care and treatment disappeared.
Strengths and limitations
Karl Weick's authorship on sensemaking has evolved from a cognitivist approach in The Social Psychology of Organizing 69 to a more constructionist approach with Sensemaking in Organizations. 15 As such, the focus has shifted to actively ‘making’ sense in a never-ending process of organising. Sandberg and Tsoukas argue 70 that large, macro contexts are often ignored in sensemaking analysis. This is a point that Weick agrees with. 17 We applied the concept of institutional logics from Beedholm and Frederiksen, 36 which served to identify dominating logics. These logics illustrate the social, institutional and cultural framing of documentation and allowed us to analyse HCPs’ sensemaking of documentation in a macro context.
As a final note, sensemaking is not a process with an event as a starting point and achievement of sense as an endpoint; sensemaking is an ‘an ongoing cycle’ 70 that can easily end in sense, actions, non-sense or non-action. Our results imply that the outcome of a sensemaking process can be permanent disruption, as new political focus areas, digitalisation strategies and management approaches continue to reform the healthcare system.
Therefore, our study is a snapshot of sensemaking processes by a group of HCPs. Still, it can inform policymakers, HCPs and managers of how the EHR must be viewed in a broader sense than merely as an HCP tool, which ultimately affects service user trajectories in municipal healthcare. Organising activities, which include knowledge of trajectories and forward-looking plans on treatment and care, is at risk of disappearing in an EHR infrastructure framed by achieving efficiency over trajectory awareness.
Conclusion
Our study reveals three themes within sensemaking processes of documentation practice: (1) making sense of planning, (2) making sense of tasks and (3) making sense of recordkeeping. The combination of the EHR as a technological artefact and the domination of the market logic and public management logic as contextual framing for documentation practice contribute to fragmentation and sub-optimisation of care trajectories in municipal healthcare. HCPs mitigate fragmentation by also responding to a care professional logic, where they carry out invisible work outside of timetables and scheduled tasks.
Even though the EHR and recordkeeping have a long history as health professional activity to support treatment and care activities, the EHR system in the Danish welfare system has transformed into a managerial system designed to control financial resources and optimise organisational routines. The design of the user interface of the EHR system omits a holistic view of care trajectories and collaboration among HCPs, leaving it to HCPs to obtain continuity despite the EHR rather than because of it.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231180521 - Supplemental material for Fragmented care trajectories in municipal healthcare: Local sensemaking of digital documentation
Supplemental material, sj-docx-1-dhj-10.1177_20552076231180521 for Fragmented care trajectories in municipal healthcare: Local sensemaking of digital documentation by Julie Duval Jensen, Loni Ledderer, Raymond Kolbæk and Kirsten Beedholm in DIGITAL HEALTH
Footnotes
Acknowledgements
We would like to thank all the participants for their contribution to the study.
Contributorship
JDJ conceptualised the study and conducted data collection and analysis with support from KB, LL and RK. JDJ drafted and wrote the original manuscript, and KB, LL and RK were involved in reviewing and editing it. All authors have read and approved the final wording of the manuscript.
Data availability
Data sharing not applicable to this article as no data sets were generated or analysed during the current study
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
According to Danish law, formal ethical approval of this study was not required, and ethical considerations followed the basic principles for research given in the Helsinki Declaration (World Medical Association, 2013). The participants received verbal and written information about the purpose of the study, their right to withdraw and the confidentiality of the data provided. Furthermore, the study was approved by the Danish Data Protection Agency [ID no: 2016-051-000001].
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Health Foundation (Helsefonden) and The Municipal Quality Development Foundation (Den Kommunale Kvalitetsudviklingspulje), Municipality of Syddjurs, Denmark. This study was kindly funded by the Local Authority of Syddjurs, Helsefonden and Local Government Denmark/The Danish Health Confederation.
Guarantorship
JDJ
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.