
Abstract
Background:
Preeclampsia is a serious medical disorder affecting pregnancy. Screening in early pregnancy can identify women at risk and enable effective prophylactic treatment. Accurate blood pressure (BP) measurement is an important element of the screening algorithm. Automated self-screening, while attending the first trimester ultra sound scan, using a BP self-measurement (BPSM) station, could be a low-cost alternative to office BP measurements (OBPM) on both arms performed by clinical staff, if the measurement quality can be ensured.
Objectives:
The aim of this study was to compare automated BPSM using a self-measurement station on one arm, with OBPM performed by clinical staff on both arms. Primary outcome was the difference in mean arterial pressure (MAP) between the two methods and secondary outcomes were safety and practicality issues.
Methods:
Pregnant women attending ultrasound-examination at 12 weeks gestational age were recruited and randomized to start with having two OBPMs taken on both arms by staff, using two standard validated automatic upper arm BP devices, or self-measuring using an automated BPSM station following a crossover study design. The BPSM station consists of a validated blood pressure device, and an add-on sensor system capable of registering blood pressure values, rest-time, back-supported, legs-crossed, and ambient noise-levels respectively, and providing interactive guidance during the measurement process, for supporting the self-measurement process.
Results:
A total of 80 complete BP measurement sets were obtained, for a total of 240 BPSM measurements and 320 OBPM measurements. We found no significant difference between the OBPM and BPSM methods (p=0.86) for mean arterial pressure (MAP). However, erroneous measurements were observed frequently during the experiment, mainly during the first of the 3 BPSM measurements (6%), secondary during the second BPSM measurement (3%). Only one data set (1%) was excluded due to OBPM errors.
Conclusion:
No significant difference in MAP between the two methods was found. Means for detecting and repeating erroneous BP measurements should be implemented. Measurement errors was found in 9 % of the measurement sets which is not acceptable for clinical use. Thus, several measures have been identified in order to properly identify and recover from such measurement errors in the future.
Keywords
Introduction
Pre-eclampsia (PE) complicates approximately 2–8 per cent of all pregnancies 1 and is associated with an increased risk of foetal growth restriction, foetal death and maternal morbidity including generalized seizures, intracerebral haemorrhage and severe or lethal effects of multiple organ failure. 2 Most patients with PE have blood pressure (BP) values over 140/90 mm Hg.1,2
Recent studies have shown that screening of asymptomatic pregnant women in their first trimester of pregnancy for risk of development of PE in the second half of the pregnancy is clinically very relevant as prophylactic acetylic salicylic acid reduces their risk of developing severe PE significantly.3–7 Accurate BP measurement is an important part of this screening, and reliable BP measurements taken on both arms have been shown to be a major part of this.3,8 The method used for this is called ‘office blood pressure measurements’ (OBPMs), also sometimes called conventional BP measurements, and which implies a measurement taken by a healthcare professional at the ‘office’ (e.g. at an outpatient clinic) rather than in the home of the patient.9
In order to be reliable, a range of recommendations must be followed.9–12 These include calculation of mean arterial pressure (MAP) (((2 × diastolic BP) + systolic BP) / 3) from BP measurements taken simultaneously on both arms, performed twice for a total of four measurements, staying in a quiet setting before and during measurements, being rested for 5 min before first measurement, not moving or talking, being correctly seated, legs not crossed, back-supported, feet flat on the floor, arm supported at heart level, and finally correct cuff size and mounting.9,10 Thus, screening of pregnant women in their first trimester requires trained clinical staff to assist with performing the BP measurements in order to ensure the data-quality.
As an alternative to this, we have previously shown that blood pressure self-measurement (BPSM) stations could automate the measurement process, allowing the pregnant women to self-measure BP reliably.13,14 BPSM has also been shown to reduce the risk of white coat hypertension, which is a well-known source of bias in 20 per cent or more of patients visiting a clinic. 15 However, current BPSM stations only support measurements on one arm, rather than the two-arm approach recommended by Poon and colleagues.3,8 Thus, in order to be able to use the algorithms developed by Poon and colleagues3,8 for the early identification of PE, we need to investigate the differences between the OBPM two-arm and the automated BPSM one-arm approach.
The aim of this study was to compare automated BPSM using a self-measurement station on one arm, with OPBM performed by clinical staff on both arms. Primary outcome was the difference in MAP between the two methods, and secondary outcomes were safety and practicality issues.
Methods
Setting
The Department of Obstetrics and Gynaecology, Aarhus University Hospital, delivers around 5000 babies per year. The majority of the pregnancies are uneventful. Of these, around 200 to 800 develop PE. 16
Participants
We invited 112 pregnant women attending routine ultrasound, at gestational week 12, at the Department of Obstetrics and Gynaecology, Aarhus University Hospital, to participate in this study. Exclusion criteria were abnormal first trimester scan and twin pregnancy.
Equipment
We used two Microlife (MicroLife BP A2 Basic, MicroLife, USA), one for each arm, as well as the A&D TM-2655 BP Kiosk station (TM-2655, A&D Cooperation, Japan), combined with a touch screen computer utilizing an add-on sensor system capable of registering BP values, rest-time, back-supported, legs-crossed and ambient noise-levels, respectively, and providing interactive guidance during the BPSM process. We have previously shown this method to obtain reliable measurements.13,14
Study design
In order to avoid bias due to the order of measurement methods, a crossover design was used with participants randomized to either start with OBPM or BPSM. Participants were approached in the waiting room, before the scheduled scan. Randomization occurred after the participants had accepted. Verbal and written information regarding the study purpose and structure was given to all participants. Permission from the local ethical committee was obtained (VEK 1-10-72-81-14 and Data authority 2007-58-0016).
OBPM method
OBPMs were conducted by clinical staff using two automated BP measurement devices (MicroLife BP A2 Basic, MicroLife, USA) following the approach suggested by Poon and colleagues3,8 and shown in Figure 1.
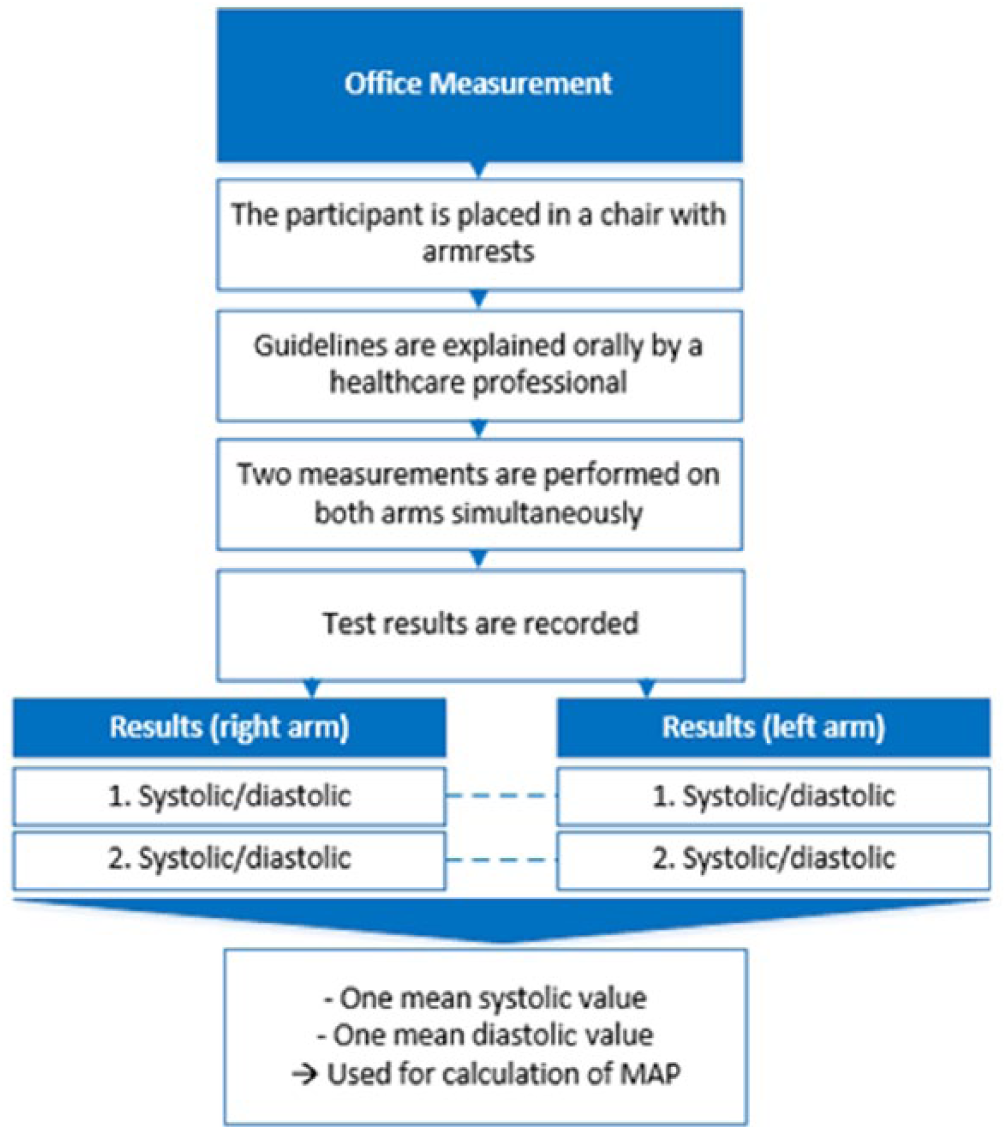
Overview of the OBPM method and the resulting data set.
Prior to the measurements, the participants were informed about the recommendations on correct BP measurements, including stance, waiting time, and how to behave during measurements,9,10 and compliance with these was constantly ensured by the clinical staff through observation. In accordance with Poon and colleagues,3,8 two measurements on each arm were performed simultaneously. Finally, the average of the systolic and diastolic pressures, respectively, for each pregnant woman was used to calculate the MAP.
BPSM method
BPSM was conducted by the participants themselves in a quiet room using a BPSM station consisting of a clinically approved BP device (A&D TM-2655P, A&D Cooperation, Japan) with a fully automatic cuff-system and an add-on sensor system capable of registering rest-time, back-supported, legs-crossed, recording participant adherence during the self-measurement process13,14 as shown in Figure 2. Data from the add-on sensor system were not used in this study.
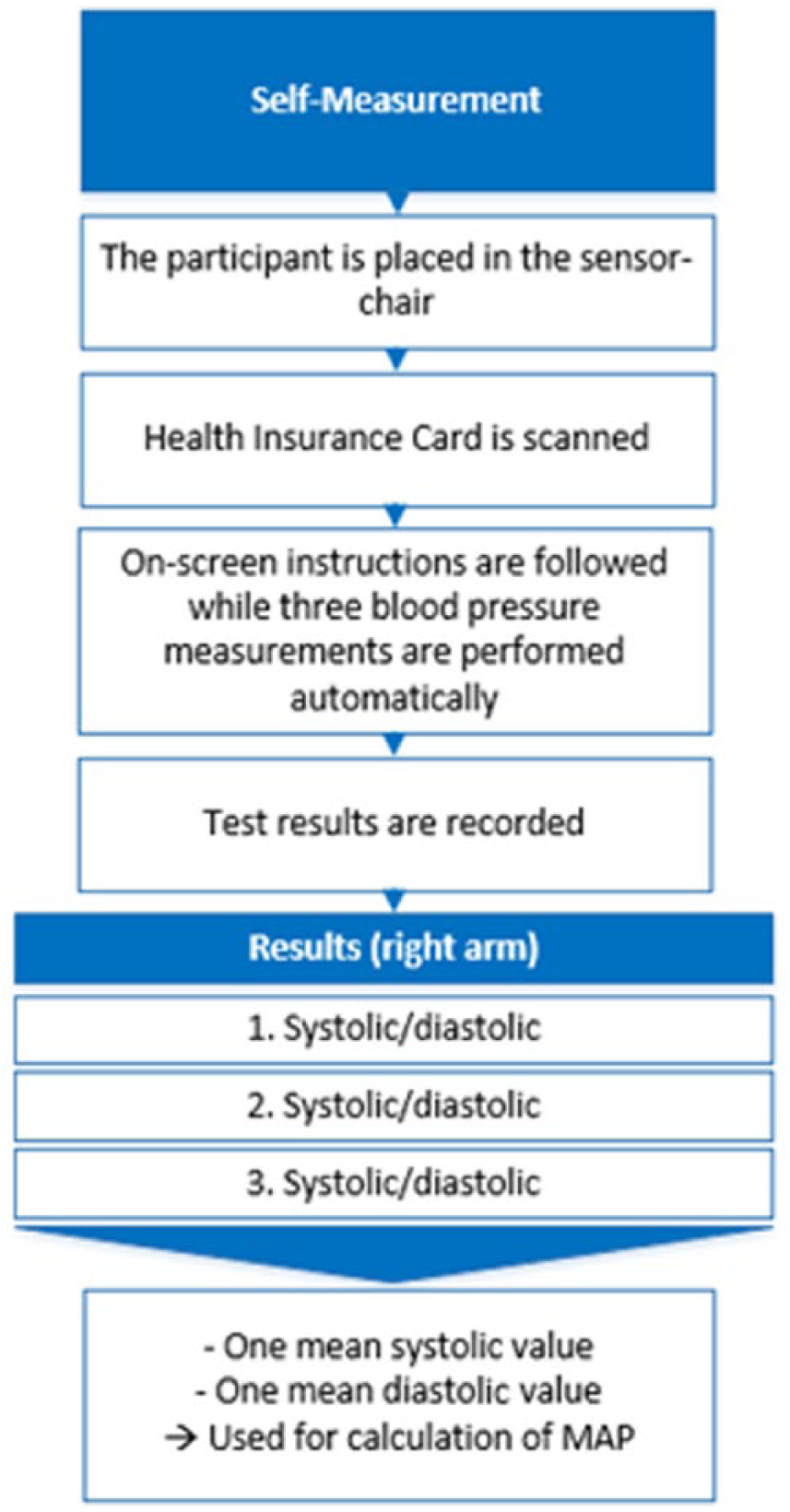
Overview of the BPSM method and the resulting data set.
The BPSM station guided the participants through three consecutive BP recordings, with 1-min rest between each recording following an initial 5 min of rest. After three measurements, the system calculated the average of the three BP measurements. The participants were not given instructions by staff prior to using the station. Instead, interactive and automated instructions were given on the station’s screen during the self-measurement process. If participants forgot to comply with any of the recommendations, they were automatically reminded to comply.
Data analysis
The primary outcome was the difference in MAP between the two methods. Normality testing was performed using qq-plots and histograms, and the difference in MAP was assessed using paired t-tests. All data analysis was done with STATA, and further visualized using box plots. Also, Bland–Altman plot was used to illustrate the differences between the MAP averages of the two methods. Measurements with systolic BP measurements below 70 mm Hg or diastolic BP below 40 mm Hg were considered as measurement errors and excluded from the study, and only complete measurement sets were used.
Results
A total of 112 participants were included in the study, resulting in an equal number of BP measurement data sets, each of which consisted of three BP measurements from the BPSM station, and four BP measurements measured by staff. A total of 32 resulting BP measurement data sets were excluded from the study, 13 of which were due to a calibration error found in the TM-2655 device. A further 10 data sets were excluded due to physical differences in the study setup, specifically differences in the position of the height of the measurement arm relative to the height of the seat, which lead to systematic differences during measurement. One participant fainted during office measurements and did not proceed to the self-measurement station. Data sets from a further eight of the remaining 88 data sets (9%) were excluded due to having one or more measurements below 70 mm Hg systolic or 40 mm Hg diastolic. Of these, seven were data from the BPSM station and one from the OBPM session. Also, five of the seven erroneous BPSM data sets occurred during the first of the three measurements of the patient, while two of seven erroneous measurements occurred during the second measurement. No errors were found during the third measurement of the BPSM sessions.
Complete data sets from 80 participants were used for the data analysis, including 320 OBPMs and 240 BPSMs. Data were found to follow a normal distribution based on the histogram and qq-plot tests. In Figure 3, the MAP value for each of the 80 included data sets is shown as a Bland–Altman plot, including the differences between the averages of the two methods.
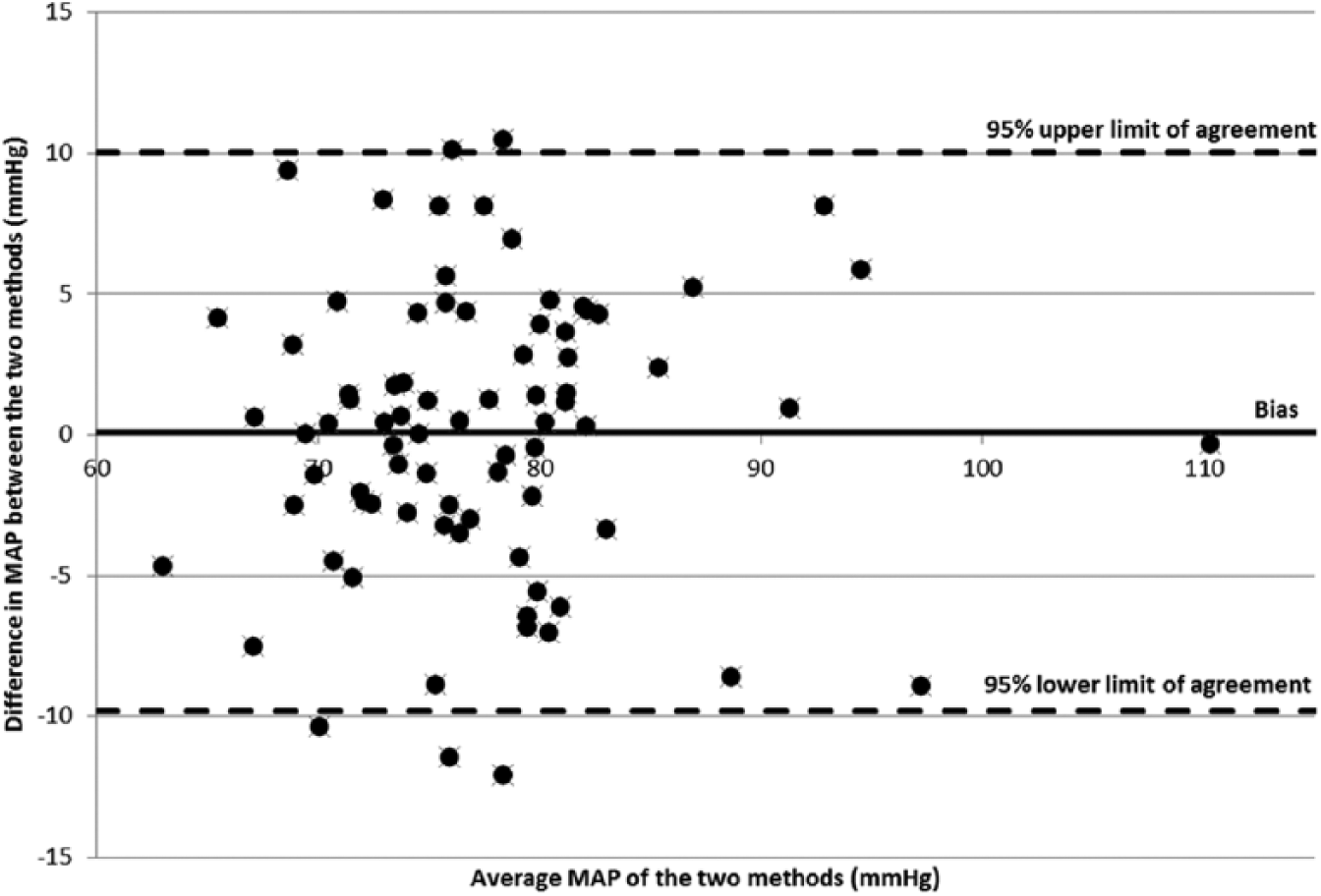
Bland–Altman plot illustrating the differences in MAP (in mm Hg) based on the mean MAP of the two methods BPSM and OBPM (x-axis) and the differences between the two (OBPM – BPSM) on the y-axis, including the 95 per cent lower and upper limits of agreement.
In Figure 4, a box plot is shown, illustrating the central tendency and spread of the data for the BPSM and the OBPM methods, respectively.
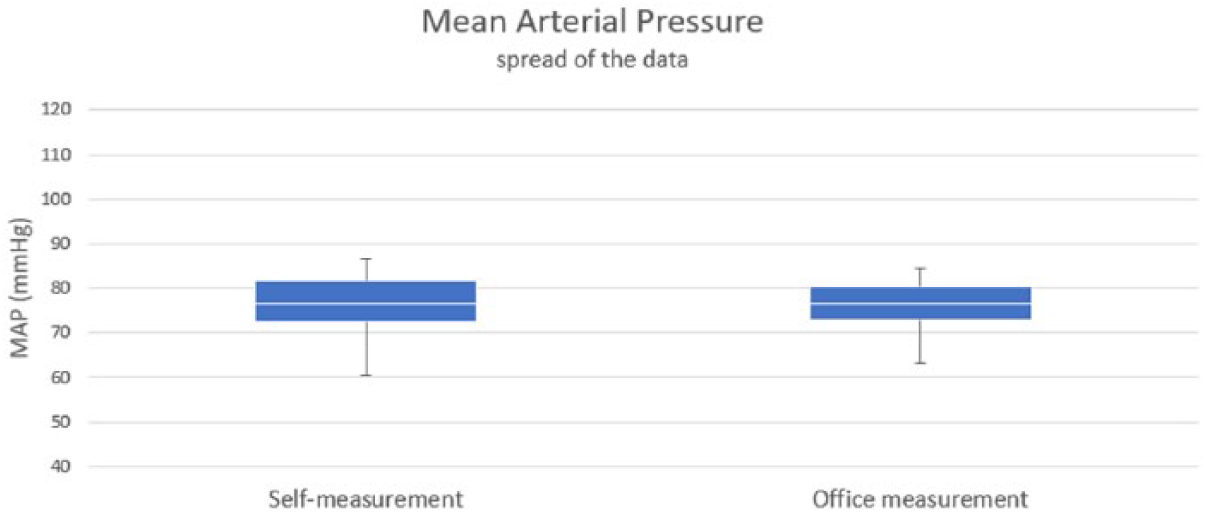
Comparative box plot of the 80 MAP values for BPSM and OBPM office-measurement methods.
Finally, in Table 1, the result of the paired t-test is shown. The table contains comparative data for BPSMs versus OBPMs including systolic, diastolic and MAP.
Mean difference, SD and p values for differences between BPSMs and OBPMs.
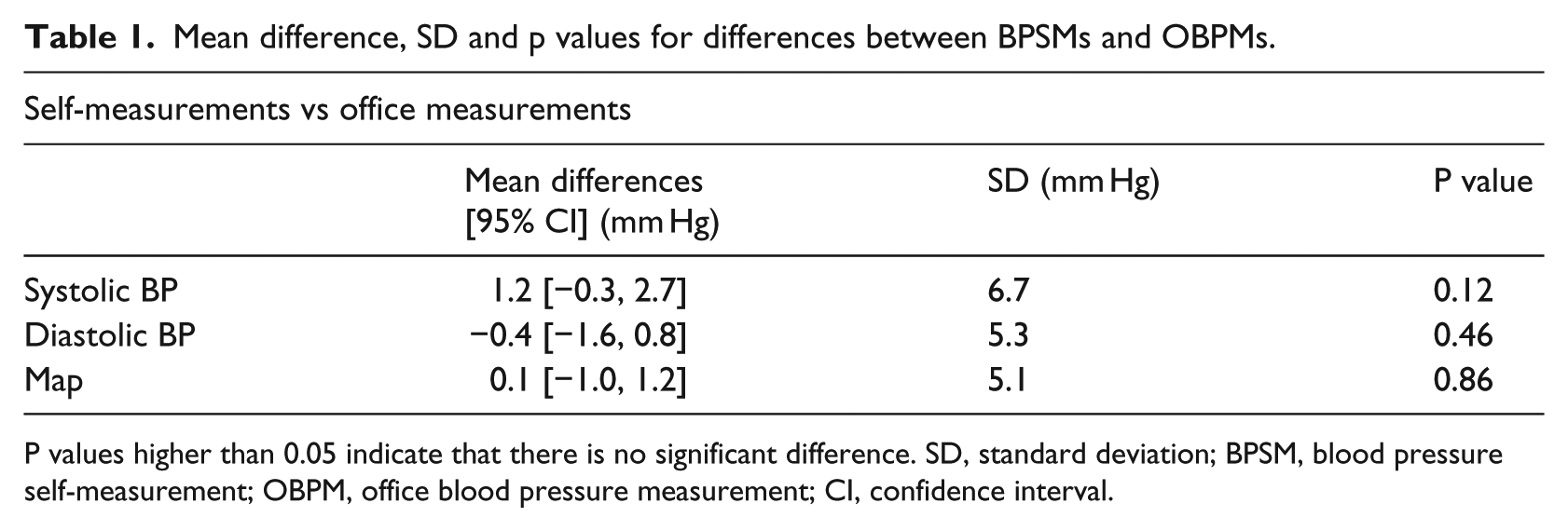
P values higher than 0.05 indicate that there is no significant difference. SD, standard deviation; BPSM, blood pressure self-measurement; OBPM, office blood pressure measurement; CI, confidence interval.
Discussion
Main findings
As Table 1 indicates, the resulting averages of BPSMs and OBPMs are comparable. No significant differences in MAP between the two methods BPSM and OBPM was found (p = 0.86). This is further supported by the Bland–Altman plot (Figure 3), where the points are uniformly scattered between the limits of agreement, which suggests good agreement between the two methods of measurement. Also, the box plot (Figure 4) shows good agreement between the two methods, especially in the interquartile range. A difference in BP measurements up to 5 mm Hg is not considered clinically relevant, while a difference between 5 and 10 mm Hg only is clinically relevant for patients who are borderline hypertensive and where a measurement error of 10 mm Hg could shift them from the normotensive to the hypertensive group.
From the sample of 80 pregnant women, we found that BP was in the very low end of the normal range with an average of 104/64 mm Hg (MAP: 77 mm Hg) for self-measurements and 103/65 mm Hg (MAP: 77 mm Hg) for office measurements compared to the normal range of 100/60–140/90 mm Hg (corresponds to normal MAP range = 70–105). However, it is normal for pregnant women in their first trimester to have low BP. 17
Measurement errors
A total of 8 participants out of 88 were removed due to measurement errors. Seven of these were due to measurement errors during the BPSM method, while 1 was during the OBPM method. Such erroneous measurements are typically attributed to physical factors such as underweight or arm circumference; however, no correlations between participants having low BP measurements and, for example, weight, height or arm circumference could be identified. The measurement errors could also be due to technical or procedural factors. Thus, five out of the seven erroneous data sets originated from the first out of three measurement sets for the participants in question, and only two of the seven erroneous measurements arrived during the second measurement set. No measurement errors were found during the third BP measurement. Thus, a possible explanation could be that the participants are more likely to make mistakes during the first measurement. In order to remedy these issues, a range of features for the automatic identification and correction of measurement errors needs to be implemented. These remedies include the automatic detection of deviations between BP measurements, for example, that two systolic measurement values from the same session differs 10 mm Hg or more, or two diastolic values differ 6 mm Hg or more. Such differences in a sequence of BP measurements could likely indicate a measurement error, either technical or by the participant, for example, movement artefacts or wrong arm placement during a measurement. To address this, the automated BPSM station could be equipped with an additional algorithm which could monitor the sequence of BP values obtained and simply discard any measurements deemed as outliers, as discussed in the section of future work.
Does automated BPSM compare with OBPM?
Self-measured BP following the BPSM method and using the TM2655 device is a reliable alternative to the traditional staff-guided and dual arm OBPM method, which has been recommended for the screening of PE.
However, with measurement errors in 9 per cent of the measurement sets, steps must be taken to properly identify and recover from measurement error. A simple approach could be to request a further BP measurement when a measurement error is detected during BPSM. In our case, this would mean that 6 per cent of the 88 participants would have to take one additional measurement for a total of four measurements, while 2 per cent would have to take a total of five measurements. As a practicality consideration, adding potentially two extra measurements prolongs the BPSM process with 2–3 min, which reduces the overall practicality and feasibility of the BPSM process.
Related work
A range of studies have found that up to 50 per cent of self-reported BP measurements does not match the data stored in the BP device’s memory,18–20 and that measurement and reporting errors occur frequently when patients are doing self-measurements. 21 Also, it is well-known that self-measurements not following the given recommendations and guidelines leads to measurement errors.11,12 Thus, self-measurement systems without proper means of validating the self-measurement process for securing reliable and high-quality data measurements appear to be vulnerable to user-errors. In a previous study, we found indications that the measurement quality improves when using active and context-aware adherence aids;13,14 however, more work is needed in this area. Also, OBPM has shown to be vulnerable to user-induced errors. A Danish study involving nurses, indicate that time, knowledge and physical environment are the main reasons that recommendations are not always followed during OBPM with personal guidance from clinical staff. 22
A recent study involving 100 pregnant women attending routine obstetrical ultrasound scanning at an outpatient clinic found that the difference between BP measurements performed by hospital staff (OBPM) on both arms and self-measurements performed with the same equipment immediately after were within acceptable international standards, in terms of systolic, diastolic and MAP values. 23 Also, 76 per cent of the participants followed the guidelines correctly during self-measurement, which lead the authors to conclude self-measurement with the BP monitor used in the study to be a safe way to achieve routine BP control during pregnancy. 23
Future work
A number of improvements are necessary prior to introducing BPSM stations for use in the screening for PE in the clinical setting. These include (1) the automatic identification and correction of measurement errors, (2) introduction of an automatic recruitment system to maintain the flow automatically without requiring staff intervention, (3) automated steps to safeguard the hygiene and functionality of the self-measurement station, (4) support and safety measures (e.g. identifying if a patient faints during measurement) and (5) automated transfer of data and possible risk stratification of the results.
Finally, the use of automated self-measurement stations relying on a combination of context and medical sensors could be extended to other areas, including in the telemedicine and ambient assisted living settings.24,25
Conclusion
No significant differences in MAP between the two methods was found (p = 0.86). Thus, BPSM on one arm using the A&D TM-2655 BP device with interactive guidance and a sensor add-on system is a reliable alternative to OBPM performed on two arms by clinical staff. Means for detecting erroneous BP measurements should be implemented before the BPSM method is safe and feasible to use.
Footnotes
Acknowledgements
Louise Holm, Tone Stucke-Brander, Stefan Wagner, Puk Sandager, and Niels Uldbjerg jointly conceived and designed the experiments; Stefan Wagner, Louise Holm, and Tone Stucke-Brander built and validated the research prototype; Louise Holm, Tone Stucke-Brander, Stefan Wagner, Puk Sandager, Jacob Schlütter, Camilla Lindahl, and Niels Uldbjerg analysed the data; Louise Holm, Tone Stucke-Brander and Stefan Wagner performed the experiments; Louise Holm, Tone Stucke-Brander, Stefan Wagner, Puk Sandager, Jacob Schlütter, Camilla Lindahl, and Niels Uldbjerg jointly wrote the paper, with Louise Holm, Tone Stucke-Brander, Stefan Wagner, Puk Sandager, and Niels Uldbjerg acting as main contributors, and Louise Holm, Tone Stucke-Brander, Stefan Wagner, and Puk Sandager as first authors.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: This work was supported by a Danish national government grant from the Ministry of Higher Education and Science Grant Number: 1234-12345B_VK.