
Abstract
People with serious mental illness have reduced life expectancy compared with a control population, much of which is accounted for by significant physical comorbidity. Frontline clinical staff in mental health often lack confidence in recognition, assessment and management of such ‘medical’ problems. Simulation provides one way for staff to practise these skills in a safe setting. We produced a multidisciplinary simulation course around recognition and assessment of medical problems in psychiatric settings. We describe an audit of strategic and design aspects of the recognition and assessment of medical problems in psychiatric settings course, using the Department of Health’s ‘Framework for Technology Enhanced Learning’ as our audit standards. At the same time as highlighting areas where recognition and assessment of medical problems in psychiatric settings adheres to these identified principles, such as the strategic underpinning of the approach, and the means by which information is collected, reviewed and shared, it also helps us to identify areas where we can improve.
Keywords
Background
In mental health inpatient settings, the population that we work with often have significant physical comorbidities. 1 People with ‘serious mental illness’ (SMI) have been shown to face a ‘persistent and increasing’ risk of dying earlier than healthy controls. 2 In reports of mortality figures, the emphasis is often on death from ‘unnatural’ causes (such as suicide and homicide). However, the vast majority of people that we look after die from ‘natural’ causes, in particular circulatory and respiratory diseases. 3 Despite this, in mental health, the domain of physical health is one where doctors, 4 registered mental health nurses (RMNs) 5 and health-care assistants (HCAs) 6 can lack confidence in the requisite skills.
Recognising and assessing medical problems in psychiatric settings (RAMPPS): the RAMPPS course
In Yorkshire and the Humber in 2011, a collaborative project between each of the region’s mental health trusts, the postgraduate school of psychiatry and the clinical skills network was established to examine the possibilities for application of simulation in mental health. Significant regional investment in clinical simulation facilities meant that there was greater access to simulation than ever before. 7 However, mental health services were not making use of the technology. This has also been true of other specialties and regions, with the Department of Health’s ‘Framework for Technology Enhanced Learning’ (‘TEL framework’) 8 noting ‘significant variation in the provision and use of e-learning, simulation and newer technologies both geographically and between disciplines’. Whilst simulation is used in mental health in some areas of undergraduate9–11 and postgraduate 12 training, the authors are unaware of similar use in physical health-care training for multidisciplinary groups.
With a small repository of scenarios based upon investigated serious untoward incidents (SUIs) from around the region, and a number of interested consultant psychiatrists, senior nurses and clinical simulation educators to constitute a faculty, a pilot course was set up in Leeds. This was then developed and shared with each mental health trust in Yorkshire and the Humber, where local faculties were given the tools to deliver similar courses for their own teams, made up of core trainees in psychiatry, inpatient RMNs and HCAs. 13 The structure and content of the recognition and assessment of medical problems in psychiatric settings (RAMPPS) course will be explained further throughout this article.
Technology-enhanced learning
‘High-risk’ professions, such as the aviation industry and the military, have long embraced simulation to build confidence and competence. 14 In this setting, learning experiences can be standardised, and the needs of the learner can be allowed to be paramount. Medicine as a whole is making increasing use of simulation as a crucial part of training, with a growing evidence base of effectiveness in the teaching of procedural skills, teamwork and communication. 15 When things go wrong in the provision of health care, decision-making, situational awareness and other ‘human factors’ are frequently the problematic elements, 16 and simulation training can be a useful tool to examine and improve these areas.
Sir Liam Donaldson’s 2008 report, ‘Safer Medical Practice’ 17 made reference to high-profile examples where simulation had been of benefit in the aviation industry, and where it could have prevented tragedy in the health service. He highlighted the potential applications of simulation and stated that the technology ‘offers an important route to safer care for patients and needs to be more fully integrated into the health service’. This thread was picked up by Dame Sally Davies, Sir Liam’s successor to the role of Chief Medical Officer in the 2011 TEL framework. 8 The emphasis here was on informing ‘the decisions of providers and commissioners when considering what role technological approaches should play in equipping their workforce with the necessary capabilities across care pathways’. While simulation has an appeal on a naïve-intuitive level, the framework sets out key principles that underpin the value of this educational approach.
The TEL framework identifies 12 recommendations across six key domains as shown in Figure 1. In the course of this article, we will outline pertinent features of the RAMPPS course, by comparison of its features against the 12 recommendations set out in the TEL framework.
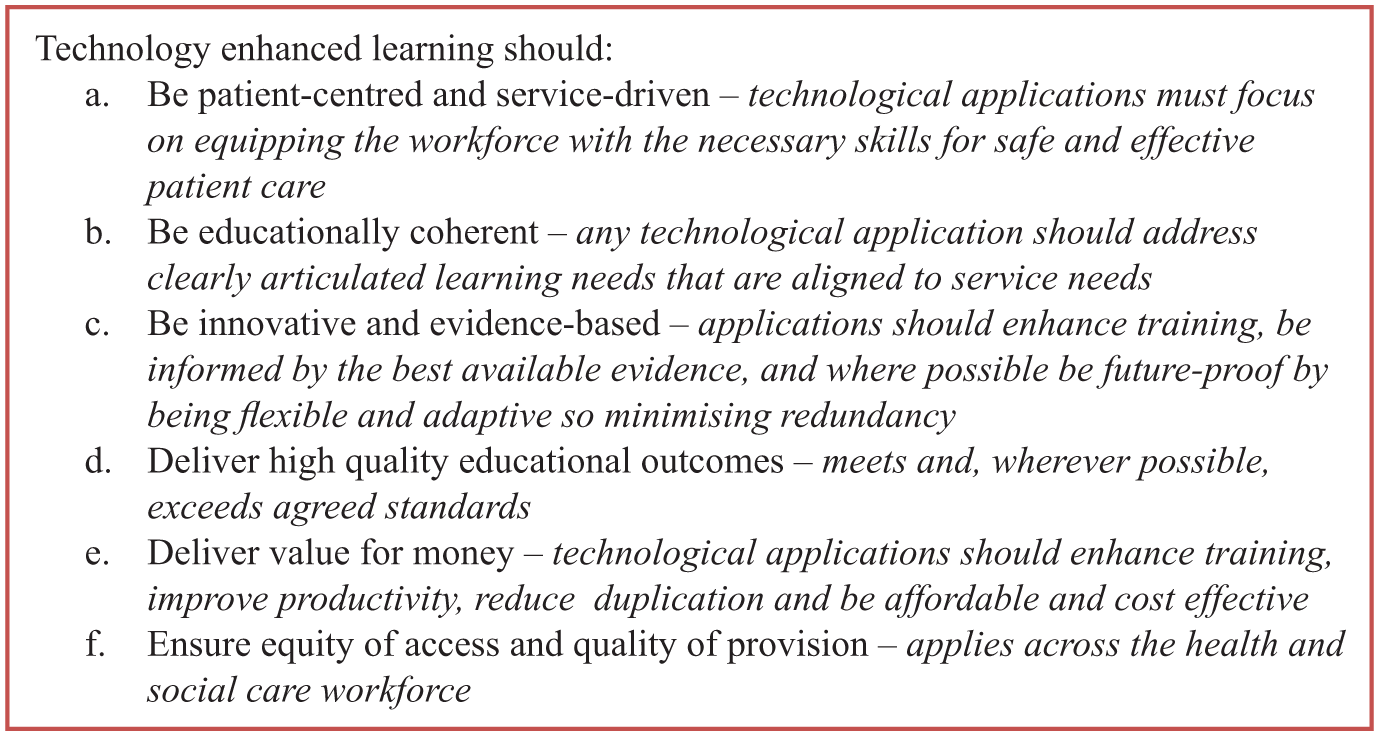
Six principles of technology-enhanced learning.
Patient centred and service driven
The first recommendation in the TEL framework is that ‘healthcare professionals should learn skills in a simulation environment … before undertaking them in clinical practice’. RAMPPS scenarios cover a number of common (e.g. hypoglycaemia) and significantly less common (e.g. neuroleptic malignant syndrome) clinical scenarios, allowing delegates to practise their approach in a safe setting where there is no risk of harm to patients. In the course of a simulated scenario, a doctor, nurse or HCA can take observations from, administer medications to and otherwise treat high-fidelity manikins. While the task at hand may be something that has been done before, it may be something borne of necessity by the urgency of a clinical situation, as can be the case in real life. Multidisciplinary teams are expected to work together, exactly as they would on a ward, sharing findings and escalating concerns as appropriate. ‘Learning skills’ clearly goes beyond practical tasks, particularly in a specialty like psychiatry, where access to investigations and treatments is more limited than it would be on a general medical ward. However, we have been using RAMPPS scenarios to teach the situation-background-assessment-recommendation (SBAR) communication tool, 18 and while some trusts in the region have some experience of this, 19 this is far from universal. As such, the security of the simulation suite provides a safe space to practise using a new approach to handover of information.
The framework advocates provision of ‘a lead to ensure that students, trainees and staff have appropriate access to technological applications to support their learning’, where there is appropriate use of technology to meet curricular, patient and service needs. For RAMPPS, this has taken a two-pronged approach: in 2008, the Yorkshire and Humber strategic health authority (SHA) set up a team of ‘clinical skills project workers’ (later rebranded as ‘strategic clinical skills advisors’ (SCSAs)) from a number of different nursing specialties, with a remit to oversee the implementation of a regional clinical skills and simulation strategy. 7 The SCSA mental health specialist has provided the role of nursing lead for the project across the region; similarly, the Yorkshire and Humber postgraduate deanery (now Health Education Yorkshire and the Humber) has supported the development of the role of ‘clinical simulation fellow’ in many medical specialties. The role within the school of psychiatry was established in 2012, and this constitutes a medical ‘lead’ for RAMPPS.
A second part of this recommendation highlights the need for ‘a strategic lead for technology-enhanced learning with responsibility for ensuring appropriate use, value for money, equity of access and demonstrable benefits to patients and services’. In the initial phases of the RAMPPS project, it was difficult to identify a clear mechanism for this. It appeared that this should be something separate to and overseeing the roles of the SCSA and the clinical simulation fellow. The route that we took was to form a regional steering committee. From the large number of involved consultant psychiatrists, senior nurses, clinical simulation educators, practice learning facilitators and resuscitation officers across the region, we appointed regional representatives and set up a biannual meeting to share areas of good practice, discuss problems, ratify newly submitted scenarios and otherwise provide overall direction to the project.
This steering committee also helps us to address recommendation 3, in which those purchasing technological solutions to support learning should undertake regular review to ensure that they continue to meet clearly defined patient and service need, support the health and social care workforce in their specific learning objectives, and provide value for money.
To date, actual purchase of technological solutions for the RAMPPS course per se has been minimal. Instead, the key has been to establish working relationships with existing simulation centres and local experts, rather than to imitate their work through purchase of our own equipment.
Nevertheless, there are costs that must be taken seriously, the most significant of which relates to ‘backfill’ of ward staff to allow them to attend a whole-day RAMPPS course in the first place. One role of the committee is to regularly review RAMPPS evaluation data: Participants are asked to rate their confidence in a number of domains taken from relevant professional curricula (the Royal College of Psychiatrists’ (RCPsych) 20 core training curriculum, the Nursing and Midwifery Council’s 21 essential skills clusters and the Royal College of Nursing’s 22 HCA ‘First Steps’ competencies checklist) before and after taking part in a RAMPPS course. Data from four courses that have been run so far have demonstrated improvements in confidence in a number of competencies across all professional groups. 13
At this relatively early stage in the project, it is difficult to demonstrate ‘value for money’. Our intention is that staff taking part in RAMPPS recognise deterioration in physical health at an earlier stage and escalate their concerns appropriately. Through this, we would expect a long-term reduction in the frequency and severity of SUIs related to physical health problems, which themselves are associated with resource costs 23 and potential litigation costs. 24
At present, RAMPPS has not produced a coherent solution to recommendation 4, in which ‘providers should provide appropriate access for all their students, staff and trainees to a system to manage, record and evaluate their learning’. Working with multidisciplinary groups adds significant value to the RAMPPS learning experience, but the support mechanisms in place for each of them to record and monitor their own learning are varied, if they exist at all. Core trainees in psychiatry have to maintain a portfolio 25 in which they record learning experiences and are encouraged to reflect upon significant training opportunities. However, access to personal development plans and similar tools to plan and record learning is variable in nursing disciplines. One way in which we intend to address this for RAMPPS is to contact delegates 3 months after taking part in RAMPPS. Here, we could collect further data about their confidence in the identified competencies, to see whether this persists or decays. We could also request a short reflective piece about ways in which delegates have used the approaches taught in RAMPPS in their clinical practice. The delegate would then be able to use this as part of their continuing professional development (CPD) to identify other training needs.
Educationally coherent
There are four parts to recommendation 5. The first relates to identification of a strategic lead for technology-enhanced learning, in a similar way to recommendation 2b. The second goes on to explain specific roles that the strategic lead (or leads) should fulfil; for example, ‘they should highlight and describe the opportunities for use of technology. They should indicate how to facilitate multidisciplinary and interprofessional learning in the delivery of their curricular or similar learning framework outcomes’. Given that simulation is an educational approach that is unfamiliar to many of those working in psychiatry, part of the role has been to explain the opportunities that it can bring. To do this, the strategic leads have met with groups of consultant psychiatrists, senior nurses and trust-level managers across the region to explain the RAMPPS approach. RAMPPS has been presented at trust, regional, national and international conferences, as a means of demonstrating the work that has been done so far, to invite comment and criticism and to recruit faculty members. Interprofessional learning is at the heart of RAMPPS, and the course provides a rare example of how this can work in psychiatry.
In initial drafts of the RAMPPS scenarios, learning objectives were laudable, but fell short of accepted standards. They were taken directly from relevant curricula, and as such, there were separate objectives for doctors, nurses and HCAs. Furthermore, taking isolated competencies meant that there were many that appeared to be appropriate. The result was a list of between 10 and 14 learning objectives, per profession, per scenario. This was unworkable and as such was extensively reviewed after the initial courses, taking the lead from local experts in simulation. Following review, the number of specific objectives has been reduced to no more than six, shared by all delegates, but still mapped to specific areas of the relevant curricula. They now conform to Heinich’s 26 ‘audience, behaviour, condition, degree’ (ABCD) principle of learning objectives (e.g. In the simulated scenario (C), the doctor, nurse or HCA (A) will be able to use SBAR when handing over information (B) in a manner expected at their level of training (D)).
The domain of educational coherence concludes with the message that simulation is not an end in itself but rather should be ‘appropriately integrated in a blended approach to learning and implemented to address specific learning or clinical needs’. At present, RAMPPS is a standalone course. However, the simulation is a relatively small part of the learning. Debriefing is a crucial component of effective learning and has been shown to be integral to the effectiveness of simulation, 27 helping individual learners to monitor their own progress and slowing the ‘decay in skills over time’. Issenberg et al. comment that ‘educational feedback to learners is a principal feature of simulation-based medical education’, and good debriefing pays close attention to the learning objectives. 28
In a whole-day course, simulation is likely to last no longer than 100–120 min in total. The learning takes place in the debriefing afterwards, with opportunity to review (including through the use of video playback) and reflect upon one’s own actions and the actions of others. There are plans to further develop RAMPPS over the next 12 months such that it is preceded and followed by a short e-learning package, where the first element acts as a ‘refresher’ or provides a basic grounding in the airway-breathing-circulation-disability-exposure (ABCDE) approach to assessment of a patient 29 and the SBAR and average value per user alert-responding to voice-responding to pain-unresponsive (AVPU) models, while the second reinforces the e-learning and the simulation experience.
Innovative and evidence based
The TEL framework advocates aspiration to ‘educational excellence by encouraging innovation, evaluation and the dissemination and adoption of evidence-based, good practice’. Simulation training around physical health in psychiatry is innovative, and while there are pockets of similar work elsewhere, 12 RAMPPS is innovative in combination of these principles with a truly interprofessional approach. Through sharing of successes and challenges, as well as our own evaluation data, we aim to contribute to a growing evidence base.
High-quality educational outcomes
Recommendation 7 echoes elements of recommendation 5c, highlighting clarity about ‘the purpose of the facility, equipment or content identifying the target groups(s), expected learning outcomes and, where appropriate, guidance on its use’. We do this in two main ways. First, before arranging a RAMPPS course in a given trust, we deliver what has come to be known as a ‘RAMPPS faculty development day’. This provides an opportunity to talk to a group of interested consultant psychiatrists, senior nurses, resuscitation officers and others, who may or may not have heard about the RAMPPS course before, about the core concepts and aspects of delivery. Through sharing of the development journey, video from the pilot and subsequent courses, and an opportunity to take part in scenarios as if they were delegates, those attending gain an understanding of the nature of the approach and the role of a facilitator within that. This is reinforced by a RAMPPS handbook, which contains scripts, equipment lists and physiological flow charts for each scenario, alongside clearly identified learning objectives and a set of debriefing tools.
The faculty development day, delivered by local RAMPPS leads and supported by the strategic leads, ensures that facilitators are competent to run the debriefing. However, our working relationships with resuscitation officers, clinical simulation educators, consultant anaesthetists and others more regularly involved in simulation have meant that we have stopped short of training all facilitators extensively in use of simulation facilities or other technology tools, as stated in recommendation 8. Part of this is related to pressures of time and an intention to ‘play to the strengths’ of recruited consultant psychiatrists and senior nurses. Another part is more pragmatic; as we are not intending to purchase large amounts of simulation technology ourselves, it appears likely that facilities that we use will have a variety of equipment, from a number of different manufacturers. As such, training in any specific piece of equipment may well be fruitless.
Deliver value for money
We intend to provide value for money through the dissemination of this work across the whole of Yorkshire and the Humber in the first instance and then to other regions. There has been significant collaborative work between different agencies, and some of the main functions of the SCSAs and the regional clinical skills network have been facilitation of sharing of resources, maximisation of purchasing power and increases in ‘opportunities for multidisciplinary and interprofessional training across the entire care pathway’. By demonstrating the journey that we have taken in the design and development of RAMPPS, we hope to save other regions and trusts significant time, effort and expenditure.
Recommendation 10a suggests that ‘a national register covering e-learning modules, simulation scenarios and toolkits should be maintained to provide the facility to search for existing tools or projects in development’. There is a national register of e-learning projects 30 but at present not a similar facility for simulation projects (although such resources do exist in other countries 31 ). This would be likely to be an extremely useful facility and would undoubtedly help us to spread the message about our work further, as well as making our work and/or the work of others more efficient. In keeping with recommendation 10b, this is certainly something that we would have accessed. Our closest approximation, a literature search, yielded the aforementioned psychiatry simulation project in London, 12 alongside other innovative uses of simulation in undergraduate nurse training.9,32
Equity of access and quality of provision
The final domain, that of equity of access and quality of provision, underpins all of the others. As far as recommendation 11 is concerned, the ensuring of easy access to e-learning across different learning management systems (including different computer/mobile platforms) is something that has been written into draft proposals for our allied e-learning programme. Once this has been produced, this will warrant its own detailed consideration against the standard identified in the TEL framework.
Recommendation 12 is of more relevance to work on the RAMPPS course so far. Establishment of a local educational governance mechanism was an early priority. As mentioned, initial selection of relevant competencies from each of the professional curricula produced learning objectives that were unusable in practice. However, by mapping these competencies to our refined learning objectives, we were able to use them as a means of evaluation. The list of competencies was turned into a list of statements of confidence (e.g. ‘I am confident in my demonstration of respect for the skills, contributions and opinions of others’), and delegates were asked to rate their accordance with these statements across a 9-point Likert item. They were given the same questionnaire after taking part in RAMPPS, and questionnaires were paired, to gain greater statistical power. Detailed discussion of these data is beyond the remit of this article but is available elsewhere. 13 Alongside these quantitative data, we also asked for qualitative feedback about elements of RAMPPS that worked well or could be improved.
Conclusion
The RAMPPS course has emerged as part of a solution to the problem of difficulties in management of the physical health of inpatients on psychiatric wards. By providing a safe space for the practice of skills related to recognition, assessment and treatment of physical health problems, mental health inpatient staff can gain confidence in key competencies and provide better, safer care. The TEL framework provides a practical set of standards which can be used to audit innovations in learning that utilise technology in this way. At the same time, as highlighting areas where RAMPPS adheres to these identified principles, such as the strategic underpinning of the approach, and the means by which information is collected, reviewed and shared, it also helps us to identify areas where we can improve.
Long-term data will be important for a number of reasons. We believe that knowledge gained via this educational approach will be more resistant to decay than would learning from more traditional means, but at present, we have not demonstrated this. This long-term retention of knowledge is clearly something that key stakeholders will have an interest in. We aim to use the addition of e-learning to solve this and some of the other issues: Addition of an e-learning element would produce a more blended learning package, catering for adults with a wider array of learning styles; it could realistically link to relevant learning management systems, such as the RCPsych’s training portfolio or a mental health trust’s own management platform, and would also provide a conduit for long-term follow-up data, reflective work and post-course e-learning. As identified above, this would itself require careful audit with a tool such as the TEL framework.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.