
Abstract
Many medical organizations have implemented electronic health record (EHR) and health information exchange (HIE) networks to improve medical decision-making. This study evaluated the contribution of EHR and HIE networks to physicians by investigating whether health information technology can lead to more efficient admission decisions by reducing redundant admissions in the stressful environment of emergency. Log-files were retrieved from an integrative and interoperable EHR that serves seven main Israeli hospitals. The analysis was restricted to a group of patients seen in the emergency departments who were administered a Creatinine test. The assessment of the contribution of EHR to admission decisions used various statistical analyses and track log-file analysis. We showed that using the EHR contributes to more efficient admission decisions and reduces the number of avoidable admissions. In particular, there was a reduction in readmissions when patient history was viewed. Using EHR can help respond to the international problem of avoidable hospital readmissions.
Keywords
Introduction
Interest in information technology (IT) in health care is intensifying rapidly. 1 The health-care sector has invested heavily in health information technology (HIT) in recent years 2 to improve medical decision-making and increase its efficiency through better medical processes and the integration of patients’ data. Jha et al. 3 stated that HIT has the potential to improve the efficiency and effectiveness of health-care providers. In recent years, both successful4,5 and unsuccessful implementations of medical information systems (IS) have been documented worldwide,6–9 involving vast amounts of money. Thus, it is no wonder that the debate over HIT cost-effectiveness has yet to be resolved.
This study investigated the clinical and economic implications of using HIT. We explored how accessing historical medical data provided by an electronic health record (EHR) and a health information exchange (HIE) network affects admission decisions in the high-stress environment of emergency departments (EDs). In addition, we explored the role of various sources of information, including local (documented at the same point of care) versus external (documented at other points of care), to assess the contribution of interoperable systems. Specifically, we explored the role that EHR and HIE can play in reducing the number of ED redundant general readmissions and single-day admissions. We suggest that a tiered approach is useful in determining whether HIT has the potential to save costs and in which instances it makes a worthwhile contribution.
The following sections provide a literature survey and an introduction to the focal EHR and HIE networks. Section “Data analysis and results” describes the methodology and section “Discussion” details the results of the study. The final sections discuss the implications of the results, provide a discussion, and examine the limitations of the study and avenues for future research.
Previous studies of medical informatics
The implications of using HIT at the point of care have been studied from a variety of perspectives. Yet despite the increasing use of these systems by clinicians, there has been little research documenting the clinical and economic implications of their use.10–12 This issue is a familiar one. The productivity paradox suggests that in some fields, the overall contribution of information technologies is not immediately apparent. 13 Nevertheless, it has been shown that a lack of information may result in lesser quality of care and unnecessary costs.4,14 This study aimed to fill this gap by examining the impact of online medical systems on the process of decision-making in the stressful ED environment.
IT can help achieve the goals of safer, more effective, patient-centered, timely, efficient, and equitable health care. HIT can decrease costs of health care while maintaining or improving quality. 15 Walker et al. 1 showed that the exchange of information from different sources (known as “interoperability”) between health-care providers enabled a computer-assisted reduction of redundant tests and led to positive financial returns. Ben-Assuli et al. 16 evaluated the contribution of EHR and HIE to improvement in medical decision-making processes and concluded that accessing the medical history of patients can lead to better decision-making and outcomes. Although clinicians express a high level of confidence after receiving information,17–20 the introduction of additional information and care options has been shown to increase decision complexity. 21 In the case of actual exploitation of information, physicians retrieve only a limited amount of relevant information even without time constraints 22 and use EHR systems for fewer tasks than the systems’ support. 23 Esquivel et al. 24 noted that medical IT is poorly adapted to the health-care social environment and proposed that flexibility in the referral process is necessary for effective system use by staff.
Sox et al. 25 emphasized the importance of medical history as a way to draw valid, reasonable conclusions regarding medical decisions. Walker et al. 1 argued that there is a relationship between the reviewing of medical history and improved medical care, including admission decisions. Goldman et al. 26 showed, for instance, that children with abdominal pain received more effective medical care (including better admission decisions) when the physician reviewed their medical history. It is likely that some single-day admissions are unnecessary and could easily be eliminated if physicians had access to proper medical history.
These conclusions and more general studies have shown that a clinical support system can efficiently triage patients in an ED using a limited amount of information27–29 and can result in both clinical and economic advantages. Nevertheless, they leave many basic questions unanswered, one of which is the role of EHR and HIE itself in medical decision-making. In addition, the health-care sector needs additional proven results regarding the effect of using HIT on advancing quality of care and improving patient safety. Hence, this study examined the impact of EHR systems and HIE networks as the source of medical history in EDs, rather than other traditional sources of medical information such as hard copies of patient records, physical examinations, or patient complaints.
The EHR IS and its environment
In Israel, every citizen is required by law to be a member of one of the four health maintenance organizations (HMOs) that currently exist in the country. This study focused on the largest HMO in the State of Israel, listed as one of the world’s five largest nongovernmental HMOs. This HMO is a nonprofit organization that serves over 3.8 million customers. Its annual budget is funded mostly by the State through National Health Insurance, but also through its customers. The HMO owns seven general hospitals (all surveyed in this study). Hospitals owned by the HMO care for patients insured by other HMOs as well.
In 2004, the HMO deployed an interoperable solution covering EHR IS and HIE networks (analyzed in this study). The HMO was the first in Israel and one of the early adopters, internationally, of this health-care IT. Their solution enables health-care organizations to share medical and health information between various points of care that belong to different health-care entities, creating a virtual patient record by logically connecting a group of care providers and organizations and thus eliminating the need to centralize the data or replace existing IS. The system aggregates the documented medical information from all points of care that individual patients visited in the past (including hospitals, community clinics, institutes, labs, etc.). It then performs a context-sensitive integration of the information. This results in a comprehensive, integrated, and real-time virtual patient record available at all points of care of the HMO. As a pure interoperable network, the system only needs a few seconds to gather historical patient data from the other health-care IS at the HMO’s various points of care. The data include patients’ demographics, chronic medication, adverse reactions, detailed lab and imaging results, past diagnoses, health-care procedures, and so on.
However, the hospitals studied here also serve patients insured by other HMOs, but their EHR IS and HIE network only provide full integrative information on patients belonging to the main HMO. Information regarding patients from other HMOs is partial and only includes data documented during previous admissions to the hospital for the current referral and does not include data from community clinic visits. This study also explored this dissimilarity in the nature of information as a function of HMO membership.
The Creatinine case study
In this study, we sampled a homogeneous group of patients who were more similar as regards their medical condition than the general public of patients. 4 We focused on the subset of ED referrals who had a Creatinine test during their visit. Two different groups were compared: those for whom information was viewed and those for whom information was not viewed.
The Creatinine test
Creatinine is a breakdown product of creatine phosphate in muscles and is usually produced at a fairly constant rate by the body (depending on muscle mass). Creatinine is mainly filtered by the kidneys, though a small amount is actively secreted. There is little to no tubular reabsorption of Creatinine. If the filtering by the kidneys is deficient, Creatinine in blood levels rise.
The Creatinine blood test is usually ordered along with a blood urea nitrogen (BUN) test to assess kidney function. Both are frequently ordered as part of a basic metabolic panel (BMP) or comprehensive metabolic panel (CMP), which are groups of tests performed to evaluate the function of the body’s major organs. BMP or CMP tests are performed on healthy people during routine physical exams and on acutely or chronically ill patients in the ED and hospitals. If the Creatinine and BUN tests are found to be abnormal or if the patient has an underlying disease, such as diabetes that is known to affect the kidneys, then these two tests may be used to monitor the progress of kidney dysfunction and the effectiveness of treatment. Blood Creatinine and BUN tests may also be ordered to evaluate kidney function prior to some procedures, such as a computerized tomography (CT) scan that may require the use of drugs that can damage the kidneys. Increased Creatinine levels in the blood point to possible diseases or conditions that affect kidney function. Low levels of Creatinine are not common and are not usually a reason for concern. They can be perceived as conditions that result in decreased muscle mass. The standard and normal values for the test range between 0.6 and 1.2 mg/dL.
Material and methods
Track log-file analysis
Log-files were retrieved from the main HMO for ED referrals from 2004 to 2007 (after the IS was adopted by all seven hospitals and the HIE was established). The log-file consisted of 340,804 admitted patients and 474,310 nonadmitted patients for whom a Creatinine test was conducted. The source of the log-file was seven main hospitals owned by the HMO that used the EHR IS and an interoperable HIE network to share medical information from distributed health suppliers electronically (including external medical clinics, imaging institutions, labs, and hospitals). Medical history was defined as the different types of patient medical histories (described above in the description of the focal IS) viewed by physicians.
Independent variables
Viewed medical history
The term “viewed medical history” refers to access to at least one of several medical history categories in the focal EHR IS. Due to lack of information on the number of specific components that were retrieved by the physicians for each case, this was measured as a dichotomous variable, indicating only whether the physician retrieved any information from the EHR IS (1 = history viewed; 0 = history not viewed).
Viewed local information
The variable “viewed local information” indicates an examination of medical information created locally within a specific hospital. We coded the variable “viewed local information” 1 if local information was viewed from the EHR IS and 0 if local information was not viewed.
Viewed external information (interoperability)
The variable “viewed external information” indicates the viewing of medical historical information created outside the specific hospital and provided online by certain health suppliers connected to the HIE network. External information concerned past and present main HMO–insured patients for whom both local and external types of information were available to a certain extent. Coding was 1 if external information was viewed from the EHR IS and 0 if it was not viewed.
Health insurance provider
To control for major discrepancies in the quality and the amount of medical information between the main HMO patients and other HMO patients, a dichotomous variable was created (1 = member of the main HMO (for whom full medical history was available via the IS); 0 = member of other HMOs (partial history available)).
ED department
This variable represented the specific type of unit where the patient was evaluated in the ED such as internal medicine or surgical. Internal medicine (71.71%), surgical, and pediatrics together amounted to more than 90 percent of the entire sample for which Creatinine test was ordered.
Hospital
This variable represented the specific hospital where the patient was evaluated. Each one of the seven hospitals had a different code represented by this variable.
Creatinine result
A continuous variable represented the result of the Creatinine test, namely, the level of Creatinine in the blood. This was the result of the Creatinine test ordered by the doctor to determine whether the result was “normal” or not. This variable was measured in milligrams per deciliter.
Dependent variables
Admission decisions
Admission decision was defined as a dichotomous variable that described the decision whether or not to admit the patient to the ED (1 for admit decision and 0 for discharge decision). This measurement scale has been used in previous research. 30
Single-day admissions
This variable quantified whether a patient, as a result of the decision to admit, was admitted for a single day (coded 1) or for a longer period of time (coded 0). Previous observations showed that the proportion of single-day admissions changed when the patient’s medical history was consulted.4,16 It is likely that some single-day admissions are redundant and could be avoided if physicians had access to proper medical history. Existing scales have shown that such short-term admissions can be reduced.16,31 The measurement scale of single-day admissions filtered out patients who intentionally sought and received treatment involving a single-day admission.
Readmission within 7 days
This variable quantified whether a patient was readmitted to a hospital within 7 days since the previous discharge from the hospital (coded 1) or otherwise (coded 0). This measure is widely used as a means of monitoring the efficacy of critical care pathways. 32 Decreasing incidences of readmission have increasingly become a goal of caregivers, hospital administrators, and policy makers,33,34 to the point that recent policies seek to penalize doctors for high readmission rates. 35 An accepted notion is that the shorter the period between discharge and readmission, the more likely that the patient was discharged prematurely. 36 Nevertheless, readmission rates are also used as a proxy for quality of care rendered during the hospitalization.36,37 In addition, it reflects the level of patient safety as part of the whole health-care service.
Data analysis and results
Descriptive statistics
The first step in the analysis was to calculate the percentages of information viewed in terms of patient characteristics. Table 1 shows that patients’ historical information was viewed via the EHR IS (the majority of which resulted in an admit decision) in only 37.1 percent of all referrals to hospitals. In other words, 62.9 percent of all referrals did not involve any use of EHR. Additionally, physicians mostly used local information (created at the same hospital as the current referral) and made less use of external information (created at another distributed health-care provider), as can be seen in Table 1 (7% external information vs 30.1% local information).
Characteristics of the study sample and comparison between subjects with medical history viewed versus subjects with medical history not viewed.
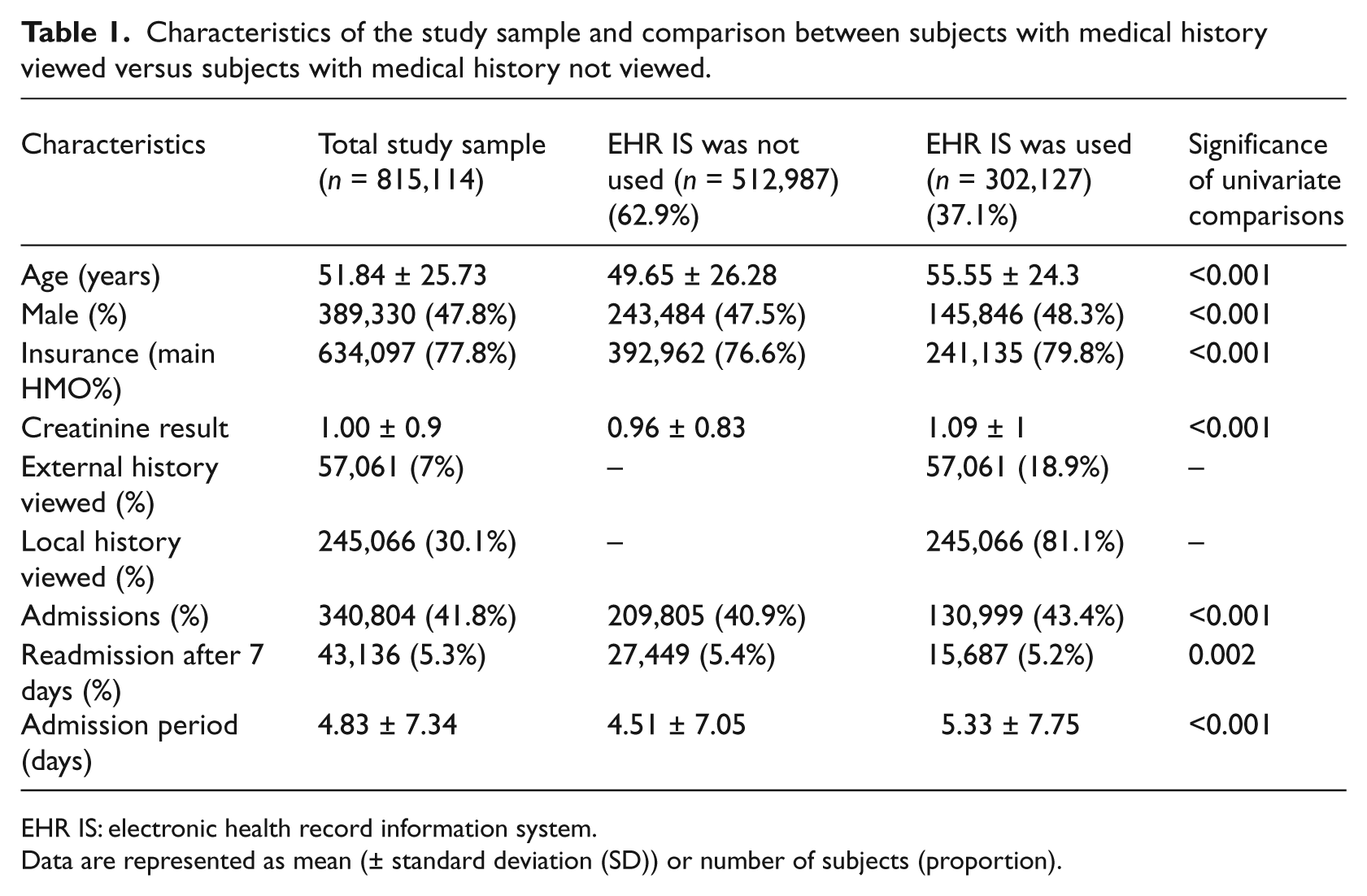
EHR IS: electronic health record information system.
Data are represented as mean (± standard deviation (SD)) or number of subjects (proportion).
Relationships between the main variables
This section presents the statistical analyses of relationships between the dependent variables and the main independent variables: admission decisions, single-day admissions, and 7-day readmissions by comparing proportions of independent populations (not exposed to medical information vs exposed to such information). We show these relationships and create a background for the multivariate logistic regressions by determining the inner relationships between the variables.
As seen in Table 2, when medical history was viewed via the EHR IS, there was an increase of 6.11 percent in the rate of admissions. Thus, medical history was more frequently viewed in medical cases that tended to be more severe or urgent. Among the main HMO patients, there was an increase of 5.76 percent in the rate of admissions when medical history was viewed. Among patients of other HMOs, this increase was 5.22 percent. However, viewing the medical history via the EHR IS significantly reduced both rates of single-day admissions and 7-day readmissions. For both the main HMO patients and the non-HMO patients, there was a considerable decrease of more than 23 percent in the rate of single-day admissions. When medical history via the EHR IS was viewed, for the main HMO patients, there was a significant decrease of 3.51 percent in the rate of readmissions, but for the other HMO patients, the decrease was statistically insignificant.
The impact of using EHR IS on decision to admit, by type of insurance.
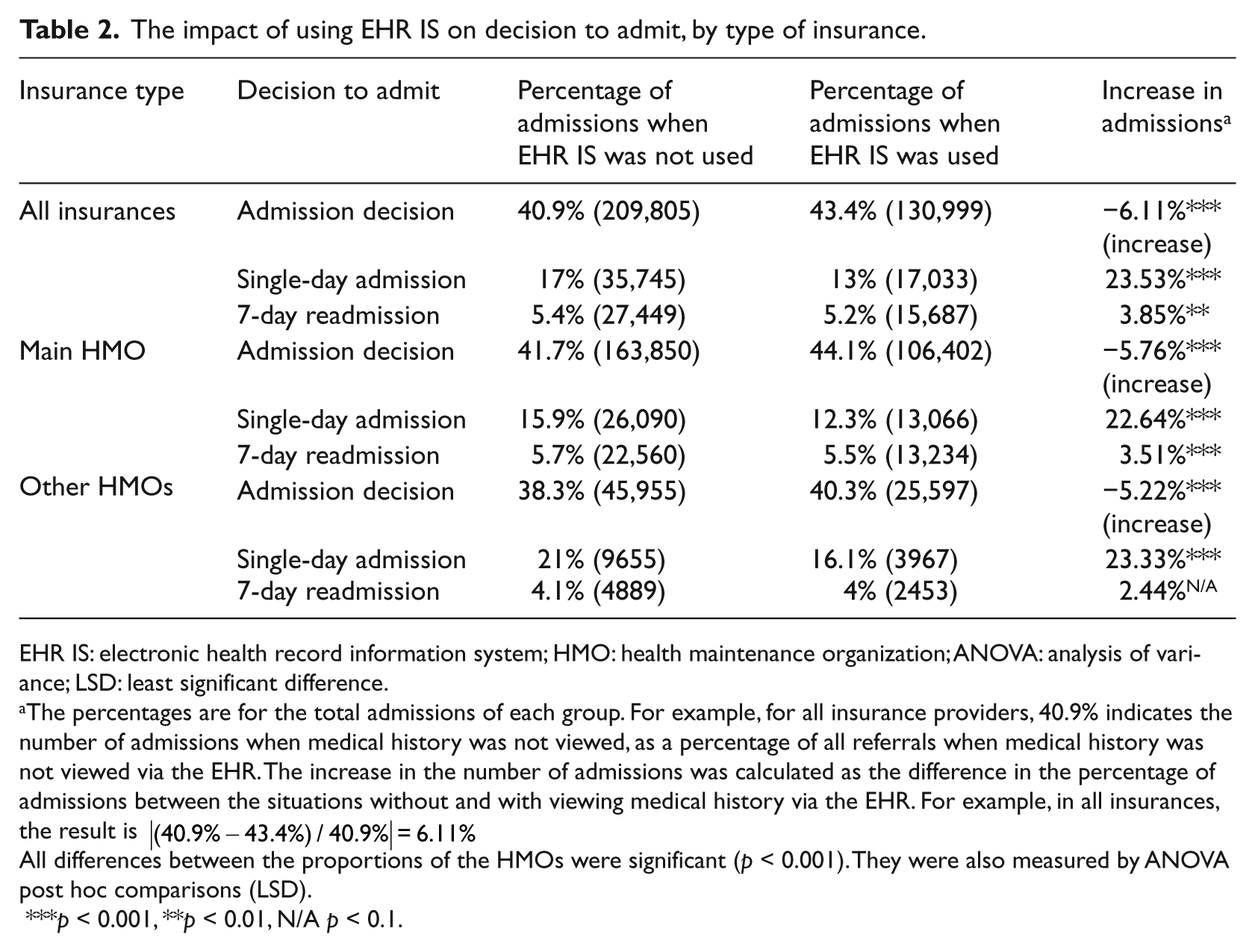
EHR IS: electronic health record information system; HMO: health maintenance organization; ANOVA: analysis of variance; LSD: least significant difference.
The percentages are for the total admissions of each group. For example, for all insurance providers, 40.9% indicates the number of admissions when medical history was not viewed, as a percentage of all referrals when medical history was not viewed via the EHR. The increase in the number of admissions was calculated as the difference in the percentage of admissions between the situations without and with viewing medical history via the EHR. For example, in all insurances, the result is |(40.9%−43.4%)/40.9%|=6.11%
All differences between the proportions of the HMOs were significant (p < 0.001). They were also measured by ANOVA post hoc comparisons (LSD).
p < 0.001, **p < 0.01, N/A p < 0.1.
Table 2 reveals certain differences between the patients insured by the main HMO and other HMOs. In the following section, we study the effect of viewing medical history via the EHR using multivariate logistic regressions, after controlling for various independent variables.
Regression analysis
We ran the logistic regression using three blocks of variables: “treatment variables” (EHR IS used, age, insurance provider, gender, and Creatinine result), “control variables for type of department” (e.g. internal medicine and surgical), and “control variables for different hospitals” (due to various differences such as policies). Block 2, control for type of department, and Block 3, control for type of hospital, are not shown here, but were included in these regressions. Tables 3 to 5 present the outcomes of the logistic regression for the impact of the variable “history viewed” and other variables on the admission decision, on the rate of single-day admissions, and on the rate of 7-day readmissions.
A logistic regression on decision to admit for the EHR IS used.
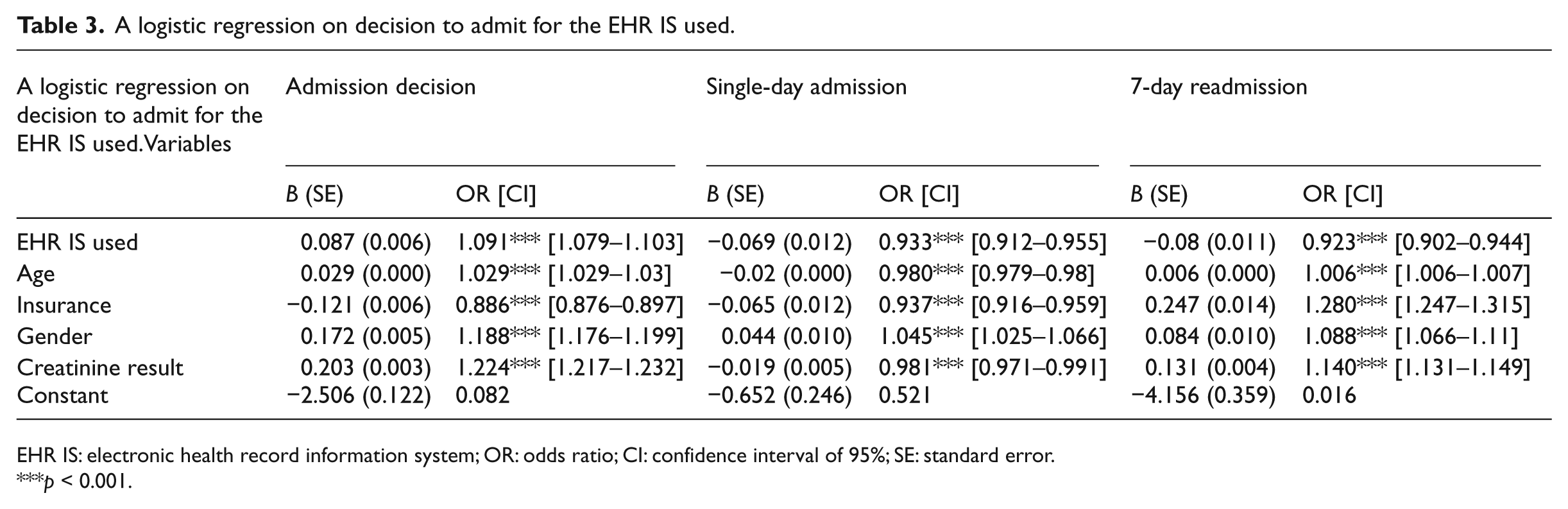
EHR IS: electronic health record information system; OR: odds ratio; CI: confidence interval of 95%; SE: standard error.
p < 0.001.
A logistic regression on decision to admit, for locally created information.
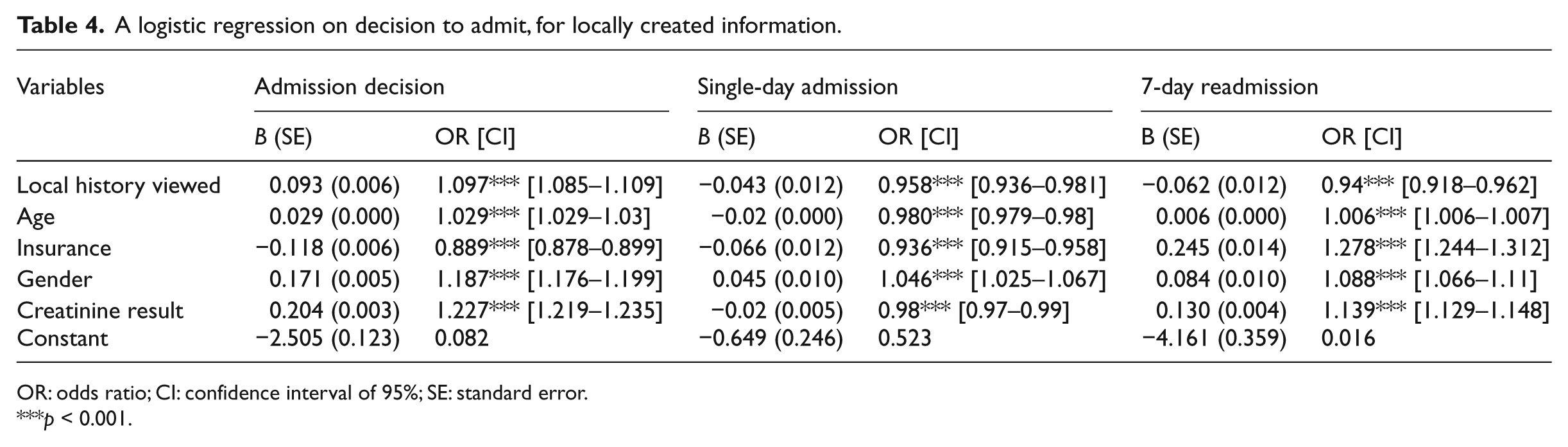
OR: odds ratio; CI: confidence interval of 95%; SE: standard error.
p < 0.001.
A logistic regression on decision to admit for externally created information.
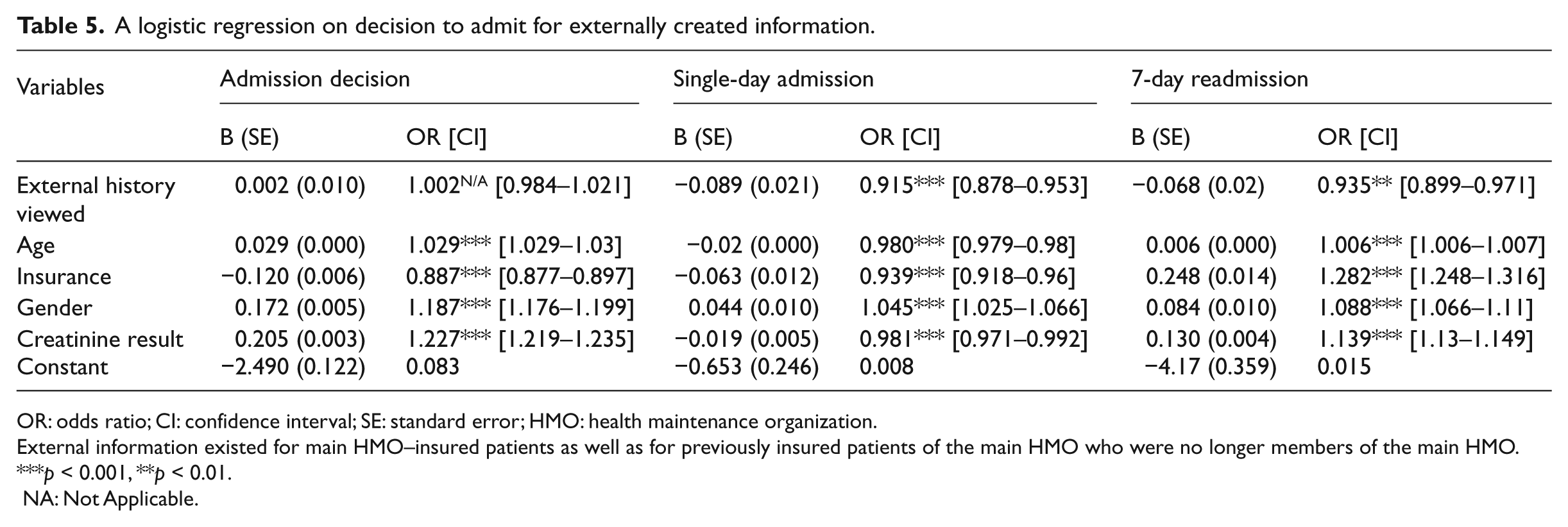
OR: odds ratio; CI: confidence interval; SE: standard error; HMO: health maintenance organization.
External information existed for main HMO–insured patients as well as for previously insured patients of the main HMO who were no longer members of the main HMO.
p < 0.001, **p < 0.01.
NA: Not Applicable.
Table 3 reveals that compared to a situation where history was not viewed, when history was viewed via the EHR IS, there was an increase of 9.1 percent (p < 0.001, adjusted odds ratio (OR) = 1.091) in the probability of admitting the patient and a decrease of 6.7 percent in the probability of single-day admissions (p < 0.001, adjusted OR = 0.933). Furthermore, the probability of 7-day readmission decreased by 7.7 percent (p < 0.001, adjusted OR = 0.923). The above results were obtained after controlling for key characteristics of the patients’ data. These results are consistent with the findings presented in Table 3.
Moreover, when the age of the patients increased by an additional year, the probability of admissions increased by 3 percent (p < 0.001, adjusted OR = 1.029), the probability of single-day admissions decreased by 2 percent (p < 0.001, adjusted OR = 0.980), and the probability of 7-day readmissions increased by 0.6 percent (p < 0.001, adjusted OR = 1.006). This result suggests that older age, which is typically associated with deteriorated medical conditions, brings about additional admissions as well as readmissions. On the other hand, age was negatively correlated with single-day admissions, suggesting that a short admission term of a single day usually relates to less severe or urgent medical conditions.
Type of insurance also played a significant role. When the patients insured by the main HMO were compared to the patients insured by other HMOs, the probability of admissions decreased by 11.4 percent (p < 0.001, adjusted OR = 0.886), the probability of single-day admissions also decreased by 6.3 percent (p < 0.001, adjusted OR = 0.937), whereas the probability of 7-day readmissions increased by 28 percent (p < 0.001, adjusted OR = 1.280). The reduced probability of admissions for the main HMO members suggests that the additional patient data (mainly based on interoperability) available on the main HMO members may increase physicians’ efficiency in making admission decisions for their patients. We also ran all these regressions separately for each type of HMO and obtained almost identical findings.
We also explored the effect of gender and found that for male patients, the probability of being admitted was higher by 18.8 percent compared to female patients (p < 0.001, adjusted OR = 1.188), there was a higher probability of single-day admissions (an additional 4.5%; p < 0.001, adjusted OR = 1.045), and the probability of 7-day readmissions increased by 8.8 percent (p < 0.001, adjusted OR = 1.088).
Finally, we explored the Creatinine test’s impact on the results. We found that when the result of the Creatinine test increased by one unit, the probability of admission increased by 22.4 percent (p < 0.001, adjusted OR = 1.224), the probability of single-day admissions decreased by 1.9 percent (p < 0.001, adjusted OR = 0.981), and the probability of 7-day readmissions increased by 14 percent (p < 0.001, adjusted OR = 1.140).
To sum up, the results show that viewing medical history was associated with increased admission decisions, and at the same time, it contributed to better and more efficient admission decisions in terms of a reduced rate of single-day admissions and 7-day readmissions (adjusted for all remaining variables).
Contribution of the locality of information to admission decisions
Tables 4 and 5 show the results of the regressions for the locality of information. It illustrates the effect of interoperability. Table 4 presents the outcomes when local patient information was viewed, and Table 5 shows external information.
Table 4 reveals that compared to a situation where no medical history was viewed, when local medical history was viewed via the EHR IS, the probability of admissions increased by 9.7 percent (p < 0.001, adjusted OR = 1.097), the probability of single-day admissions decreased by 4.2 percent (p < 0.001, adjusted OR = 0.958), and the probability of 7-day readmission decreased as well by 6.0 percent (p < 0.001, adjusted OR = 0.94). The effects of age, gender, insurance type, and Creatinine test results were all significant, and they were almost the same as those presented in Table 3.
To sum up, Table 4 shows that viewing local medical history via the EHR was associated with decisions to admit and contributed to more efficient admission decision with a reduced probability of single-day admissions and 7-day readmissions. Compared to the results of Table 3, the magnitude of the effect on single-day admissions and 7-day readmissions was slightly smaller.
Table 5 shows that compared to a situation where medical history was not viewed, when external historical information was viewed via the EHR IS, the probability of single-day admissions decreased by 9.5 percent (p < 0.001, adjusted OR = 0.915) and the probability of 7-day readmissions decreased by 6.5 percent (p < 0.001, adjusted OR = 0.94). The effect of external historical information on admission decisions was minimal and not significant. The effects of age, gender, insurance type, and Creatinine test results were all significant, and again, they were almost the same as those presented in Table 3.
Unlike the earlier results, viewing external medical history via the EHR was not associated with increased admission decisions; however, it was associated with a reduced number of single-day admissions and 7-day readmissions, thus suggesting more efficient decision-making. The impact on single-day admissions was considerably greater than in the case of viewing local information.
Discussion
In recent years, there has been an ongoing debate about the efficacy of HIT in improving medical care, patient safety, physicians’ outcomes, and efficiency. Experts consider HIT a key to improving efficiency and quality of health care. 38 Our study focused on the ED and addressed one of the most important decisions of whether to admit or discharge a patient. 34 The current findings show that viewing medical historical information using EHR IS and HIE networks contributes to better and more efficient medical decisions in the stressful environment of the ED. Specifically, viewing medical historical information via the EHR IS clearly relates to a reduced number of single-day admissions as well as short-term readmissions. This association was substantial, supporting the claim that EHR IS and HIE networks can help avoid redundant admission costs. 14 As opposed to previous studies,4,16 these findings pertain to a rather specific homogeneous group of patients. These results suggest that if a Creatinine test is ordered, using EHR IS via an HIE network may lead to improved admission decisions.
Remarkably, the EHR IS was used in the minority of the cases (about 30% and 7% for local and external patient information, respectively), even for a population in which the Creatinine test was ordered. It is therefore plausible to assume that the system is most valuable to doctors (and thus most used) when the medical cases are more complex and where uncertainty is greater. 17 Evidently, both admission rates and length of stay were significantly higher for patients whose medical data were viewed via the EHR IS, indicating the complexity of these medical cases. Nevertheless, according to the results, cases in which the system was viewed were characterized by more efficient outcomes in terms of single-day admissions and short-term readmissions; therefore, it is reasonable to assume that the use of an EHR IS via an HIE network in less complex instances would yield at least the same efficiency as in the complex cases. Normatively, complex cases should not lead to fewer short-term readmissions and single-day admissions than less severe and complex cases. It is also important to note that in light of the factors that affect decision-making outlined here, our results, although significant, do not imply causality. An inference of causality requires further analyses.
Furthermore, we explored the advantages linked to interoperability in establishing and using HIE networks, and we scrutinized both local and external historical information separately. Both information sources were associated with greater efficiency in terms of a reduced number of single-day admissions and 7-day readmissions. We suggest that external information, which was only rarely consulted by doctors (in only about a fifth of the cases in which the EHR IS was viewed), was examined in cases that were more complex. Notably, the effect of external medical history was greater than that of local medical history, again hinting that the use of additional information in the less complex cases may lead to increased efficiency as well. The interoperability analysis implies that the viewing of additional information (whether external or local) may yield increased decision efficiency. The results suggest that EHR IS contributes to a decrease in decision complexity. 21
Finally, when we examined the effect of viewing medical history on the main HMO patients versus other HMO patients, we found that viewing medical history was associated with increased admissions and decreased single-day admissions for both groups; however, there was a drop in 7-day readmissions only for the main HMO patients, possibly due to the smaller sample size for the other HMO patients. We also found that demographics such as age, gender, insurance type, and medical condition were all significantly associated with the decision made in the ED’s point of care. These associations were the same whether local or external or no information was examined.
Contribution and future research
The main purpose of this study was to provide additional insights into the field of medical informatics. Specifically, the motivation was to contribute to the assessment of the efficacy of HIT to improve the quality of health care. First, we focused on the stressful point of care of the ED and used a unique database containing an entire population of patients (815,114 referrals to the ED). The Creatinine sample was used to compare two groups of patients who were administered Creatinine tests, and thus were controlled somewhat for their medical condition as compared to the general heterogeneous public of patients, while still controlling for all other research variables. Second, we examined the use of local and external integrative and interoperable real-time medical information from decentralized medical caregivers. Finally, we shed light on the positive impact of using medical historical information via an EHR IS and an HIE network on the efficiency of medical procedures.
This study also had a number of limitations. First, different hospitals have different policies and practices regarding the use of the EHR. The hospital characteristics (including type of management, policy makers, admission policy,) have influence on a hospital’s ability to actualize the potential and utilize a new EHR IS to the maximum. It was suggested that such differences demonstrate potential policy opportunities for improving efficiency as well as quality of care. 39 We partially controlled for these dissimilarities using regressions with controls on fixed effects from the hospitals’ representative variables.
Second, to protect patient privacy, the log-files do not contain explicit information on the medical condition of any patient. However, they contain useful variables that implicitly represent some information on the medical condition of the patient including age, gender, type of department, and type of hospital. To partially overcome this lack of specificity, we narrowed our examination to those who were administered a Creatinine test.
Third, we did not have enough information regarding the physicians’ characteristics. We only knew their medical specialization. More information about their experience with technology and especially their attitudes toward technology could help to better analyze the physicians’ clinical decisions and use of HIT.
Future works should opt for a more detailed look at various medical conditions in terms of the association between EHR IS viewing and decision-making efficiency. Specific information components may be examined, as well as different levels of complexity. Another point worth investigating in the future is the impact of different features of the patient’s complaint (such as severity) on physicians’ decisions whether to use the EHR IS and the role of these features in mediating the effects found in this study. Future works should also address the issue of effect sizes and attempt to determine whether using EHR IS is cost-effective even when dealing with relatively small effects. The assessment of EHR IS could be expanded to other points of care such as community health centers. Data mining could be used as a predictive tool. We examined the value of information, rather than developing a prediction model for the future behavior of decision-makers or extracting patterns from the data.
Also, it would be worthwhile examining additional strategies that could increase admission efficiency and reduce avoidable admission costs. For instance, conducting additional patient follow-ups may lead to admission screenings outside the ED environment. Such contacts may involve only high-risk admissions or more general segments of the population. 40 Likewise, primary care quality management and tracking of family practices can also lead to fewer hospitalizations and life-threatening events. 41
Footnotes
Funding
This work was partially supported by the Research Center of Ono Academic College.