
Abstract
With the development of Web 2.0 technologies, an increasing number of websites are providing online healthcare services, and they have potential to alleviate problems of overloaded medical resources in China. However, some patients are reluctant to trust and continue using online healthcare services, partly due to the immature development of healthcare websites. Previous research has argued that online trust is significantly associated with the risk or benefit perceived by users. This study aims to extend prior research and examine how perceptual factors influence patients’ online trust and intention to continue using online healthcare services. We developed a model with the moderating role of purpose of use and tested it with data collected from 283 participants. The results support the validity of the model and most hypotheses. The moderating role of purpose of use between the perceived benefits/risks and patients’ online trust is also highlighted. Theoretical and practical implications are also discussed.
Keywords
Introduction
Consumers’ use of websites and online healthcare services has grown rapidly, attracting much attention. An increasing number of people use healthcare websites for healthcare information or consultations. 1 A survey in 2012 shows that 35 percent of adults in the United States have used the Internet for health consultation, 2 while in China, 39 percent of the netizens say they would search online for health-related information if they became ill. 3 In the Chinese market, online healthcare services have considerable potential to help people obtain information and access care, suggesting strong prospects for future market growth. As the most populous country in the world, China faces mounting costs of caring for an increasingly aging population. The number of older adults in China is expected to reach 243 million in 2020, comprising 18 percent of the population. 4 In addition, a growing number suffer from chronic diseases, leading to dramatic increases in medical expenses, and the heavy burden of providing healthcare will quickly become an urgent societal and policy concern. The increasing demands for healthcare as well as an overburdened supply of healthcare providers will fuel greater demand for online healthcare services. 5 Access to online health promises to bring benefits such as 24-h availability, no geographic restrictions, lower costs, and faster service. However, for the potential of this technology to be realized, people must trust it.
In the domain of health information, prior research has focused on the trust and quality of health websites. 6 Trust is important for users when they make decisions about whether to use online healthcare websites, which site to use, and for what purposes, and building trust relationships with health consumers is essential for online healthcare providers. 7 Online sources of information include health websites,8,9 forums, 10 and online health communities. 11 In a review of trust models in the online healthcare context, Khosrowjerdi 12 concluded that most studies focus on consumers seeking information with few studies explored continuous usage of online healthcare services.
Although researchers have done fairly extensive examinations of online trust, 13 little attention has been devoted to understanding why users trust online healthcare services and, more specifically, their continued adoption, suggesting the need for further exploration of the determinants of trust in these contexts. Since healthcare websites provide various types of services, such as health information, consultation, and appointments, trust may vary depending on the ways in which consumers use them. This study proposes an integrative model built around theories of perceived benefit/risk to understand both trust and continued adoption intention toward online healthcare services.
Online healthcare services
Health plays an important role in our daily life, and consumers have embraced the Internet to search for health-related information and making appointments with physicians, 14 as well as informational and emotional support from connecting to others with similar conditions. 15 Many platforms, such as online communities, forums, and websites have been built to serve these needs. 15
Three types of online healthcare services are available in China. The first type is information services, which are basic elements in all online health platforms, and they provide a variety of information to users. While they offer medical knowledge to medical professionals and students, including academic trends and literature, general information is also provided, such as information about hospitals and physicians, diseases, treatment options, and medications. From the perspective of general users (patients or potential patients), these online information services have become effective ways of acquiring knowledge about disease prevention and treatments for common diseases. The second type involves online consultation, which facilitates easy interaction with physicians without an appointment or office visit. Patients and users can ask questions or leave messages for physicians through websites or apps, and physicians may respond in their spare time. Patients with less serious illnesses may be attracted by services of this kind. The third type of service helps users set up appointments online. Before seeing a physician in the hospital, patients in China commonly set an appointment with the physician, and they book a reservation ticket from the hospital in advance. However, the number of tickets is limited, especially the tickets of well-regarded physicians, and hospitals frequently cannot meet the demand. These services are most helpful when patients already have a physician, and they can use the service to book appointments for return visits or follow-up visits after online consultation.
Patients’ online trust
Trust is a broad concept whose definition varies in different disciplines such as psychology, economics and philosophy. However, a commonly accepted definition regards trust as “a psychological state comprising the intention to accept vulnerability based upon positive expectations of the intentions or behavior of another (p. 395).16” In online environments, a new concept of trust emerges: online trust. In these settings, it is challenging for people to know who they are trusting, and making a precise definition of online trust is not easy. Corritore et al. 17 regard online trust as a form of expectation, and an individual assumes that his or her vulnerability would not be attacked in an online environment. While there is an abundance of research on online trust generally, few studies explore trust in the domain of e-health.17,18 This study aims to fill these gaps. As a relatively new form of commercial activity, online healthcare services involve many more uncertainties and risks than their traditional healthcare delivery.
Theoretical background and hypotheses
Trust toward behavioral intention
The concept of behavioral intention emerges from the theory of reasoned action (TRA) and theory of planned behavior (TPB), which refers to a measure of the strength about one’s intention to engage in a specified behavior. 19 Behavioral intention is generally used to describe the acceptance and continued use of systems or services. For example, Luarn and Lin 20 studied the adoption of online banking, while Swar et al. 21 explored the continued online healthcare information search. 9 In this study, behavioral intention refers to the possibility of users’ continued adoption of online health healthcare services.
As online trust can reduce the uncertainty of a system and its processes, it helps maintain a stable condition for users and service providers. 22 Bart and Shankar 23 found that trust was a key element to affect behavioral intention. According to Chen and Dibb, 24 there is a significant predictive relationship between trust and behavioral intention. In the study of e-commerce, previous researchers have noted that online trust would influence behavioral intentions. 25 McKnight et al. 26 indicated that users tend to continue participating and trading with their providers when trust was formed in a website. Trust can be viewed as an antecedent that may create a positive attitude toward behavioral intentions. 27 For example, Pappas 28 suggested that trust could lead to purchase intention. Therefore, we present the following hypothesis:
H1. Patients’ online trust positively correlates with their continued adoption of online healthcare services.
Perceived risk
Perceived risk is a notion first proposed in the field of psychology. Bauer 29 introduced this concept to explore the behavior of consumers, suggesting that consumers could not ensure the results were always good, and perceived risk is a combination of uncertainty and serious outcome.
Perceived risk is closely related to the feeling of consumers and differs from the real one. Once consumers perceive a risk, they take appropriate actions to reduce it. In marketing research, various types of risks have been identified. Jacoby and Kaplan 30 classified perceived risk into five types: financial, performance, physical, psychological, and social risks; an additional factor was proposed by Peter and Tarpey, 31 which they named “time risk.” Since then, these six types of risks are widely accepted by researchers. In the domain of online service, the concept of perceived risk has evolved as the potential for loss in the pursuit of a desired outcome when using an e-service. 32 Our study specifies perceived risk as the possible uncertainties or negative consequences that users perceive from the utilization of online healthcare services.
In addition, the relationship between perceived risk and trust has received considerable attention. 33 Bansal et al. 34 examined three health websites and found a negative effect of risk on consumers’ trust in the website, suggesting that risk can be regarded as an antecedent to online trust in health information websites. 8 If consumers perceive a low risk of using online services or products, their sense of trust would increase. Therefore, we present the following hypothesis:
H2. Perceived risk negatively correlates with patients’ trust of online healthcare services.
While the research outlined above suggests that trust serves as a mediator between perceived risk and intention, other researchers have suggested direct links between these constructs. In the domain of e-commerce, perceived risk affects consumers’ attitude toward online purchasing, thereby eventually influencing their purchase intention. 35 For example, Kim et al. 36 proposed a model based on the assumption that perceived risk would directly affect decision-making, and Antony et al. 35 indicated that perceived risk significantly affected online purchasing intention. Thus, we present the following hypothesis:
H3. Perceived risk negatively correlates with continued adoption of online healthcare services.
Perceived benefit
Perceived risk and perceived benefit have been found to be inversely related. 37 Wilkie and Pessemier 38 believe that perceived benefit is a sensitive factor for consumption. Perceived benefit refers to the subjective feeling of receiving a reward or return. 39 In contrast to perceived risk which provides potential barriers to trust, perceived benefit provides incentive for users to trust. In this study, we define perceived benefit as users’ belief that their health condition would be improved using online healthcare services. If patients perceived the online healthcare services were beneficial, they are more likely to develop a high level of trust. Therefore, we propose the following hypothesis:
H4. Perceived benefit positively correlates with patients’ online trust.
Prior research has found significant associations between perceived benefit and behavioral intention. For example, perceived benefit was found as a significant predictor of accept intention to use e-payment systems. 40 For online shoppers, perceived benefit serves as an incentive to make a purchase. 36 Sirdeshmukh et al. 41 showed that the perceived benefit of consumers could help regulate their behavioral intention, and Lee 42 confirmed that the perceived benefit had a significant impact on the behavioral intention. Mou and Cohen 9 also reported a positive relationship between perceived benefit and behavioral intention. In the context of online healthcare, we posit that consumers will choose to continue using the services if they perceive more benefits compared with other forms of services. If patients perceive benefits can be gained from using online healthcare services, they will be more likely to continue using them. Hence, we propose the following hypothesis:
H5. Perceived benefit positively correlates patients’ continued adoption of online healthcare services.
Moderating effect
Moderating effects have attracted an emerging attention, and the introduction of moderating variables is crucial in theoretical development. 43 The moderating effect happens when the moderator affects the strength or direction of a relationship between two constructs. 44 Fang et al. 45 adopted perceived effectiveness as a moderate variable to test the trust and behavioral intention model of e-commerce. Different moderating factors can reflect various characteristics or perceptions.
In the context of online services, users’ characteristics such as gender, age, or experiences are associated with their perceptions of constructs like satisfaction and loyalty. 46 Many scholars are intrigued by the moderating role of users’ characteristics as they pertain to specific online trust. As for online healthcare services, purposes of users are relatively distinct, that is, seeking health information, making appointments with physicians, or consultations. We posit that variations in different purposes are associated with habits and preference, which will lead to a different level of perceived trust. For example, compared to making appointments and consultations, seeking health information online involves less risk because no personal health information is required and users are free to review all the health information on the websites without direct harm. In the case of making appointments and consultations, the latter demands a higher level of online trust since more interactions about personal health are involved, while online appointment services are relatively mature and already enjoy a high level of awareness and acceptance. If the patients have faith in the information provided on the website, and it can solve their problems, taking advantage of other services would be unnecessary for them. When patients trust online professionals and want to know the severity of their diseases, using consultation services would be a better choice. After patients decide to go to see specific physicians, the online appointment system would be convenient. Different purposes of use may indicate different personal situations and trust toward online healthcare services. Thus, we propose the following hypotheses:
H6a. Purpose of use in online healthcare services has a moderating effect on the relationship between perceived risk and patients’ online trust.
H6b. Purpose of use in online healthcare services has a moderating effect on the relationship between perceived benefit and patients’ online trust.
Based on theoretical background and hypotheses, we form a research model, as shown in Figure 1.
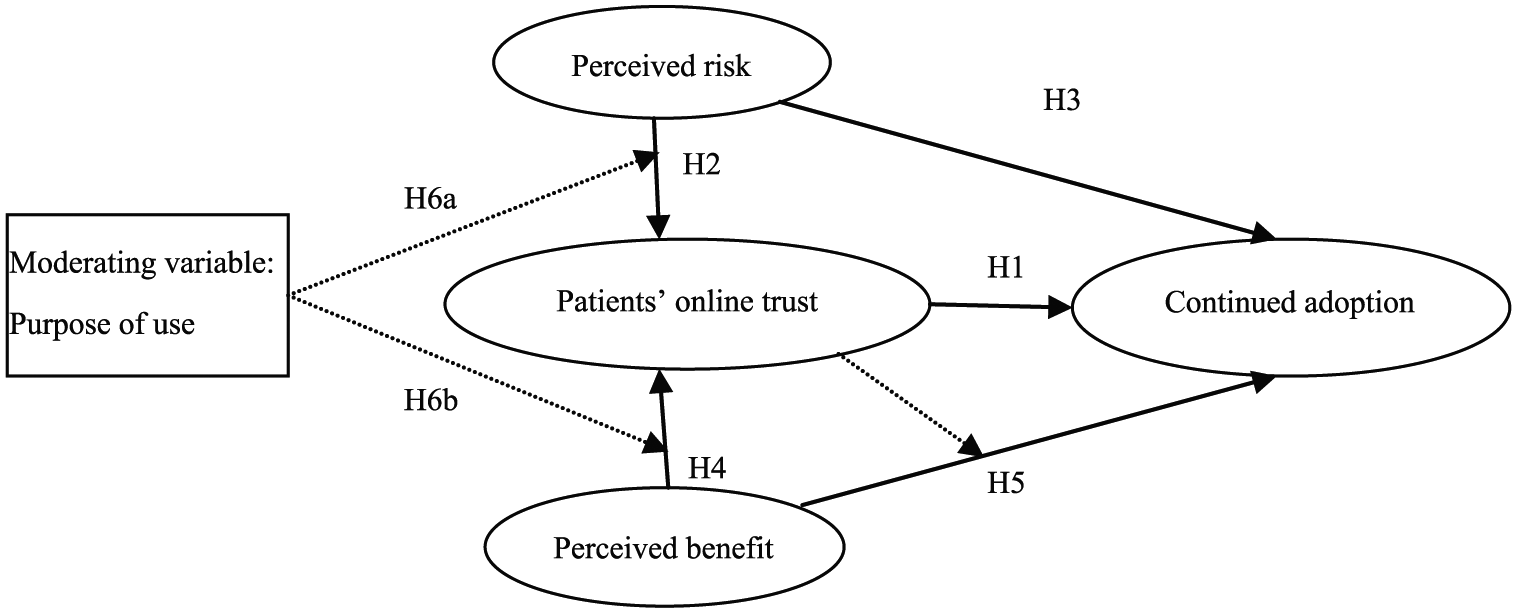
Research model.
Methodology
Measurement and questionnaire design
We conducted a survey to collect data. Two parts were included in the questionnaire. First, an information section gathered data about the characteristics of respondents, which include gender, age, education, and health condition (i.e. whether they have chronic diseases). Next, we asked the respondents about their main purpose for using online health services: whether to obtain health-related information, consult with physicians or other specialists, or setup an appointment. The answers were used to divide the respondents into three user groups: (1) information, (2) consultation, and (3) appointment. The next section included measures of trust, perceived risk, perceived benefit, and intention to use online healthcare services. Most of the items were adapted from prior studies where they had been tested and validated. The wording of some items was modified to make the survey fit for the context of online healthcare services. Perceived risk was measured from its six dimensions, and two items (time and function) were omitted after a pilot test. We used a four-item scale derived from Kim et al. 36 to measure perceived benefit. The items used to measure the patients’ online trust were adapted from the four dimensions of online trust presented in the study of Shankar et al. 47 Behavioral intention was measured by the items adapted from Liu et al. 48
After the preliminary questionnaire was completed, we conducted a pretest to refine the questionnaire. In the pilot survey, we consulted with 10 teachers and 25 postgraduate students in health informatics, as well as specialists in the field of medical information. The final constructs, operational definitions, and measurement items are listed in Table 2. All the constructs in the research were measured with a five-point Likert scale ranging from 5 (Strongly Agree) to 1 (Strongly Disagree).
Data collection and analysis
We formed a research group to collect data both online and offline. The questionnaire was either distributed via Questionnaire Star (one of the largest online survey company in China) or offline. Since our target participants were individuals who had used online healthcare services, we asked potential participants if they had used online healthcare services in the first place. The survey was continued only if the response was yes. We provided a gift (e.g. towel, soap, or lucky money) to encourage participation. The survey began in June 2016 and lasted for 1 month. We collected 298 questionnaires, and 283 responses were valid.
The structural equation modeling (SEM) was adopted to test the hypothetical model. We also followed a two-step procedure proposed by Anderson and Gerbing. 49 A confirmatory factor analysis (CFA) was conducted to test the convergent and discriminant validities of the constructs, and then, the structural model was tested to indicate the relationship among latent variables.
Results
Demographics
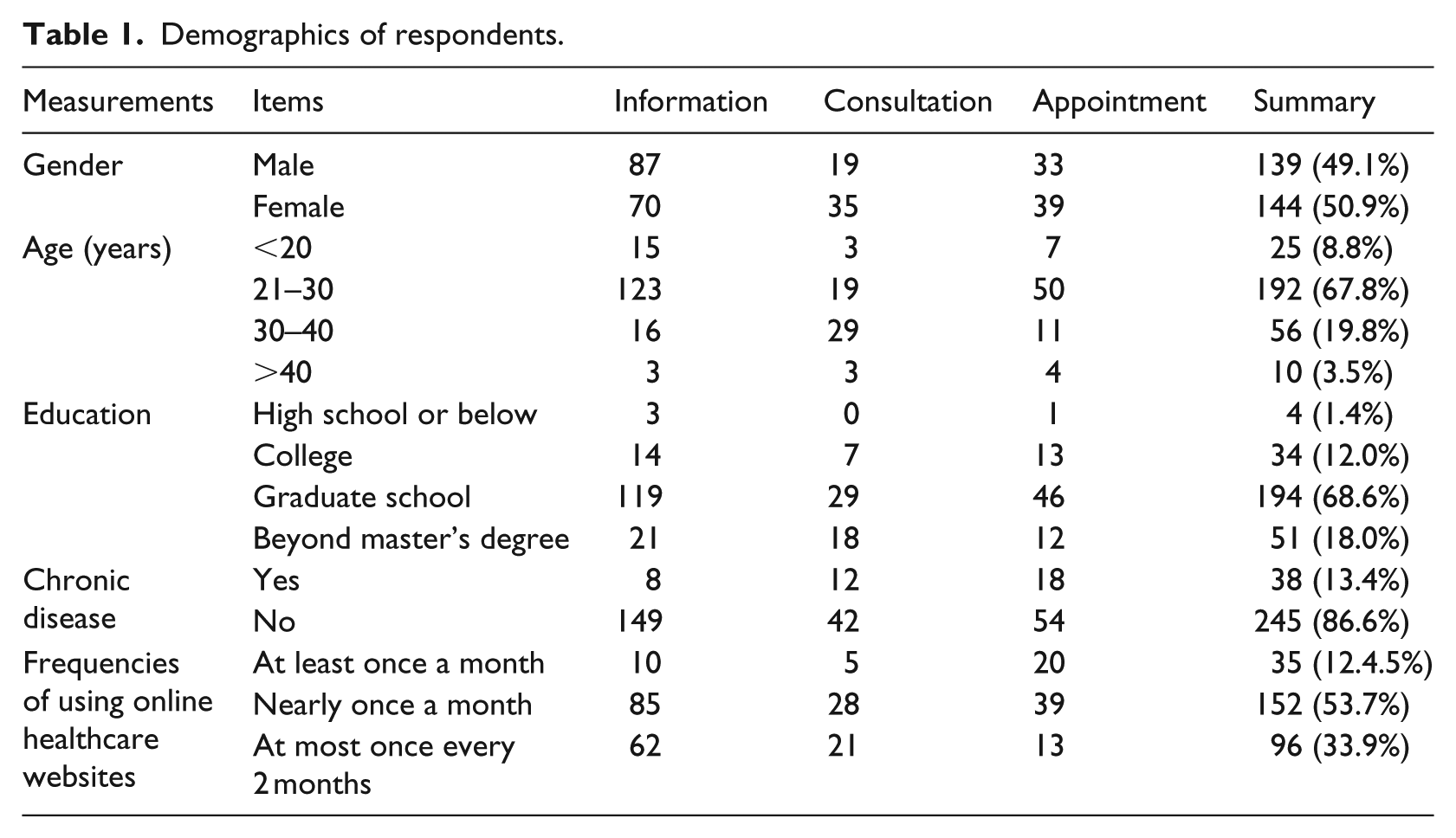
The descriptive statistics of the sample is presented in Table 1. The proportion of information group (N = 157, 55.5%) is larger than that of other groups (consultation, N = 54, 19.1%; appointment, N = 72, 25.4%). Among the respondents, 76.6 percent of them are under age of 30 years, and 86.6 percent of them have at least a bachelor’s degree.
Demographics of respondents.
Chi-square test
The chi-square test was used to explore the relation between demographics of respondents and their different adoption strategies. Results showed that respondents’ choice of online service (chi-square = 15.28, p < 0.05) varied by gender. Males were more likely to choose information than consultation services (odds ratio (OR) = 2.29, p < 0.05) but they were just as likely as females to use online appointment services. Reasons for using online health services also varied significantly by age: respondents between 20 and 30 years preferred information services (Fisher’s exact test = 47.16, p < 0.01), whereas most respondents between 30 and 40 years selected consultation services. Different education levels (Fisher’s exact test = 15.28, p < 0.05), health conditions (chronic diseases) (chi-square = 7.00, p < 0.05), and frequencies of using online healthcare websites groups (chi-square = 26.03, p < 0.05) showed significant difference in services selection. In general, gender, age, educational level, having a chronic disease or not, and frequency of health website use were significantly associated with type of service selected.
Reliability and validity
To evaluate the measurement scales, the results of the CFA, including factor loading (FL), construct reliability (CR), average variance extracted (AVE), and Cronbach’s α, are presented in Table 2. The results indicate that all FL values are higher than the 0.5 benchmark.50,51 The composite reliability scores for all the constructs are higher than 0.70,50,51 implying that the variables demonstrated reasonably high internal consistencies. In addition, Cronbach’s α values for all the constructs are higher than the minimum cutoff score of 0.70 and considered adequate. 51 All the AVE values of the constructs used to measure the variance are higher than the threshold of 0.50, indicating a sufficient convergent validity.
Construct definition and validity.
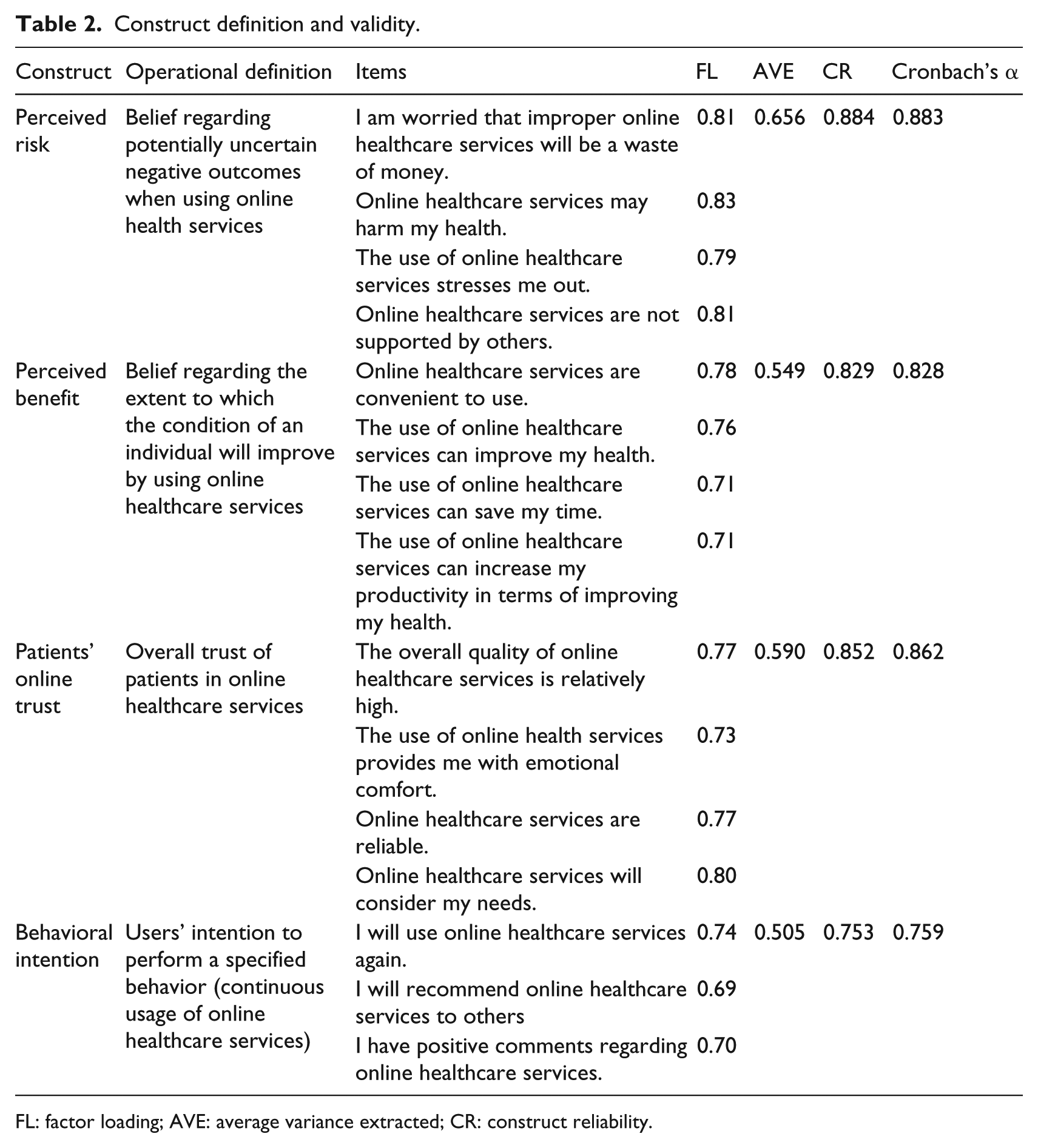
FL: factor loading; AVE: average variance extracted; CR: construct reliability.
Fornell and Larcker 50 asserted that AVE could also be used to evaluate discriminant validity, in which the square root of AVE should be larger than the variance shared between the construct and other variables in the model. Table 3 shows that all the square roots of each AVE value are greater than the inter-construct correlations, which indicates discriminant validity among the variables. Thus, the reliability and validity are considered adequate.
Correlation of latent variables and square roots of AVE values.
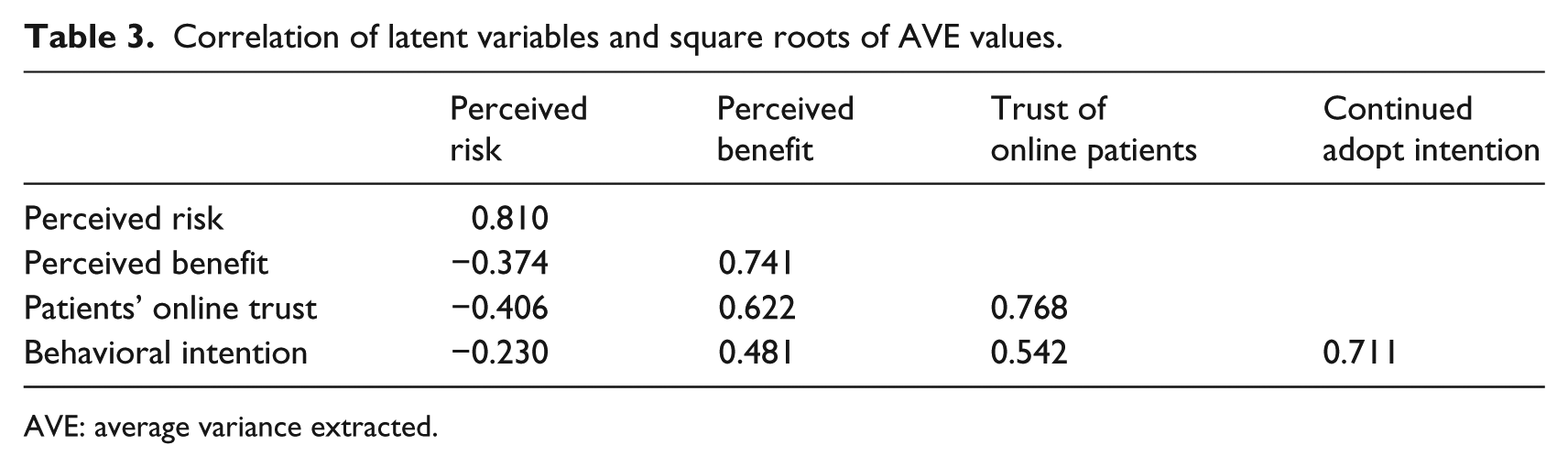
AVE: average variance extracted.
Structural model
Amos 24.0 (IBM SPSS Version 24.0) was used to test our structural model. We test the significance of each hypothesis in estimating all the specified paths, as well as the standard errors and test statistics for each path. The assessment of the proposed research model included estimating the path coefficients and R2, which indicated the performance of the model. 52 Figure 2 shows the results.
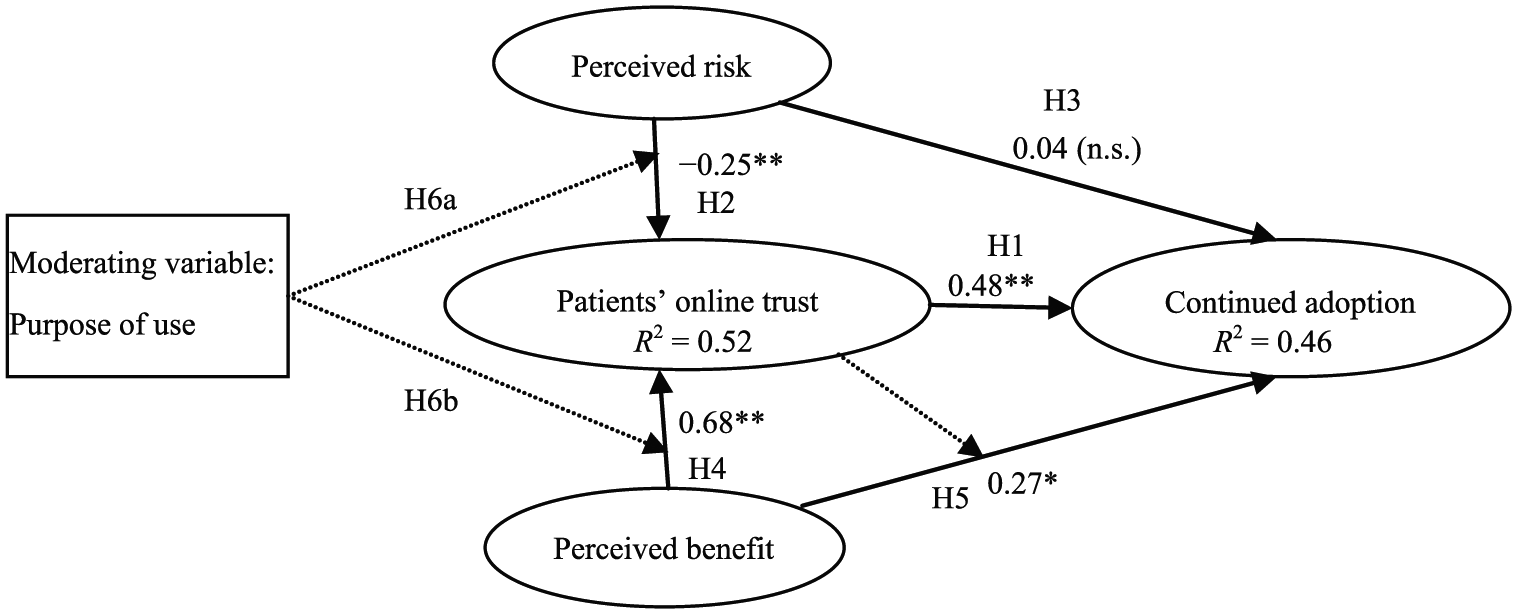
Standardized path coefficients and significance levels.
The R2 result of 0.52 indicates that 52 percent of the variation in the trust of online patients is attributed to perceived benefit and perceived risk, and 46 percent of the variation in continued adoption intention is associated with the trust and perceived benefit of online patients. The structural findings indicate that H1, H2, H4, and H5 are supported. As shown in Figure 2, the trust of online patients positively predicts behavioral intention and the path coefficient is 0.48 (H1: β = 0.48, t = 4.287, p < 0.01). As expected, perceived benefit and perceived risk both predict the patients’ online trust and their effects are opposite. The effect of perceived benefit is positive (H4: β = 0.68, t = 9.156, p < 0.01), whereas that of perceived risk is negative (H2: β =-0.25, t =-4.374, p < 0.01). Perceived benefit significantly affects continued adoption intention (H5: β = 0.27, t = 2.576, p < 0.05). By contrast, perceived risk does not directly affect continued adoption intention, and H3 is not supported. In the research model, the patients’ online trust can be regarded as a mediator between perceived benefit and continued adoption intention.
We further tested the mediating effects of patients’ online trust following the three-step method proposed by Baron and Kenny. 53 The results are shown in Table 4. The first and second conditions for mediating effect are satisfied as the relationship between independent variable (perceived benefit) and moderator (patients’ online trust), and the correlation between independent variable (perceived benefit) and dependent variable (behavioral intention) is significant. Then, the coefficient of perceived benefit and patients’ online trust is smaller than that of online trust and behavioral intention. Hence, the effect of perceived benefit on behavioral intention can be partially mediated by the patients’ online trust.
Result of mediating effects.
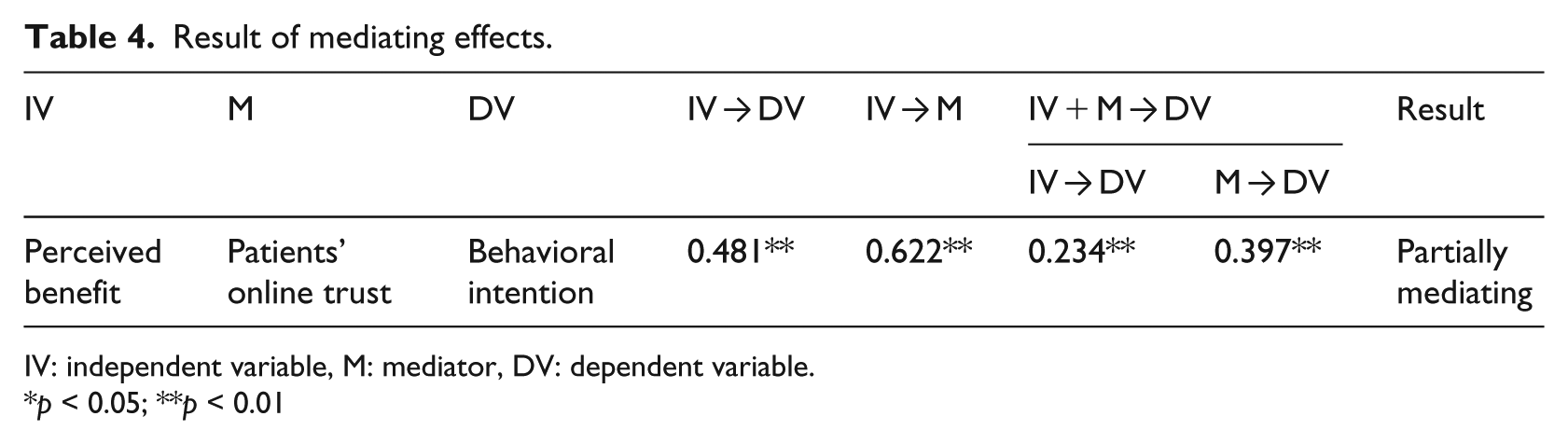
IV: independent variable, M: mediator, DV: dependent variable.
p < 0.05; **p < 0.01
The result of moderating effect of different purpose of use is as follows. The comparisons of path coefficients and R2 are shown in Table 5. The three groups have different R2 and path coefficient values, the correlation between perceived risk and patients’ online trust varies in different groups, the coefficient in consultation and information group are −0.82 and −0.30 while the correlation in appointment group is not significant. The coefficient between perceived benefit and patients’ online trust also varies among three groups; the consultation group shows a higher coefficient than other two, thus supporting H6a and H6b.
Result of moderating effects.
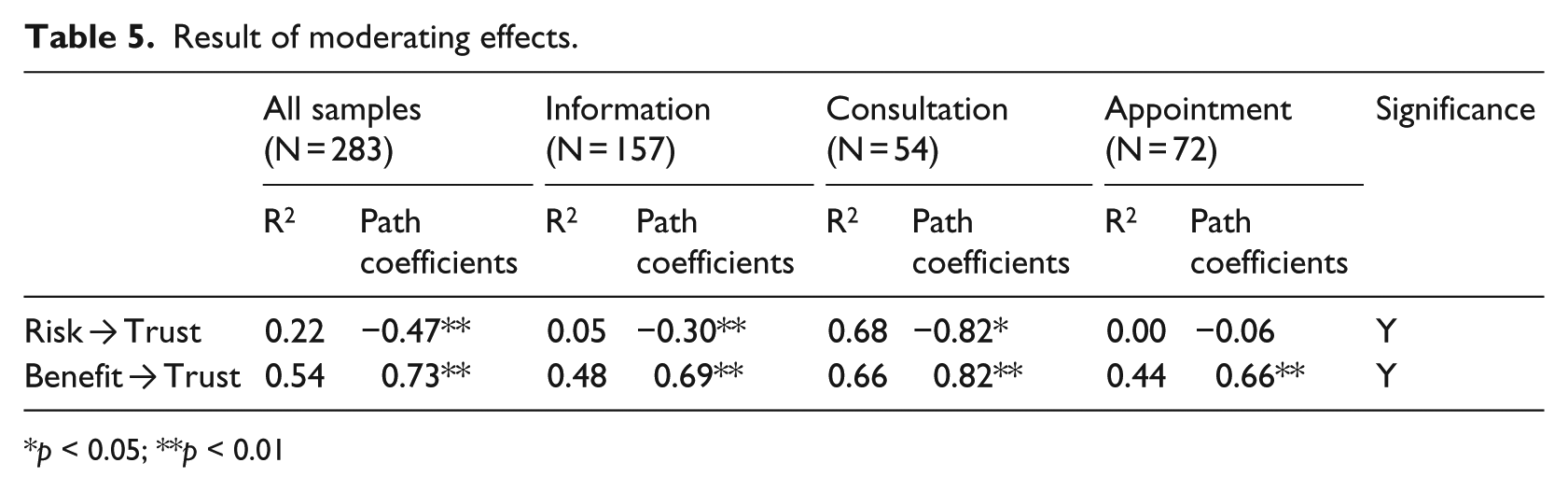
p < 0.05; **p < 0.01
Discussion
Trust plays a significant role when users make use of online healthcare services. Among the three services we tested in our study, seeking and using information does not require a high level of trust, whereas using online appointment services requires a moderate level of trust and online consultation requires the highest. Users have varying needs for using these three different services, leading to differences and continuous usage. The study of patients’ online trust is important for the development of online healthcare services. People would not choose to adopt them without trust, and building a high level of trust could also help retaining users. The study expands the understanding of various purposes of use in the relationship between perceived risk/benefit and patients’ online trust. Several key findings are generalized as follows.
First, patients’ demographic characteristics affect the choice of services. Females are more likely to choose online consultation services than males. We found significant associations between intention to use online services and gender, age, educational level, health condition (chronic diseases), and frequency of using health websites. This suggests that online health providers can create different interfaces to attract users of different demographic groups or create publicity plans that appeal to specific demographic segments. Second, while both the perceived benefit and patients’ online trust show positive effects on the continued adoption intention as hypothesized, the effect of perceived risk is not significant. The patients’ online trust exerts greater effect on continued adoption intention than perceived benefit. If patients showed a high level of trust when using online health services, they are more likely to continue their usage behavior. Perceived benefit is an important determinant of behavioral intention, and the effect of perceived risk is insignificant. The result of the relationship between perceived risk and behavioral intention is not in accordance with the result of the research of Mou and Cohen. 9 This discrepancy may possibly be attributed to the fact that users in China are familiar with online healthcare services and may be confident using these services. Meanwhile, since the two studies are conducted in different locations, that is, one of China and the other of South Africa, 9 the differences in local culture may also be important, such as people’s risk perceptions and their risk aversion.
Third, both the perceived risk and perceived benefit significantly affect the patients’ online trust. The influence of perceived benefit is positive, whereas that of perceived risk is negative. The result is consistent with Yi et al. 33 and Wilkie and Pessemier. 38 Perceived benefit also exerts a higher level of effect than perceived risk. Thus, raising the perceived benefit of patients may be more likely to encourage use of online health services than reducing perceived risk, if providers aimed to improve the patients’ online trust. In addition, perceived benefit has both direct and indirect effects on behavioral intention, while perceived risk affects behavioral intention indirectly. The results of the path coefficient and the meditating effect demonstrate that perceived benefit can both directly and indirectly affect behavioral intention.
Fourth, the moderating effect of purpose of use indicates that different purposes may vary in perceptions on the relationship between the patients’ online trust and its determinants. Users with different purposes for accessing health services online demonstrate varying requirements for perceived risk and perceived benefit. The correlation between perceived risk/benefit and patients’ online trust is significant for the three types of purposes of use. Using online services for consultation with providers was associated with higher path coefficients than making appointments or obtaining information. This finding indicates that if patients use an online healthcare website to consult a provider directly, their perceived benefit and perceived risk are highly related to their online trust. Users of online services for provider consulting are also more sensitive to perceived risk than perceived benefit, as demonstrated by a higher path coefficient between perceived risk and patients’ online trust, compared to those who use online services to simply obtain information or make appointments. These findings suggest the characteristics of online consultation, where more personal interaction is involved, carry more risk for consumers. Patients who choose to communicate with physicians online may be experiencing more severe health problem and so they may be more sensitive to risks. Furthermore, the process of consultation is also more complex than obtaining information or making appointments; patients need to register, find a suitable physician, indicate their problem, and communicate with the physician. In contrast, since online appointment making has been provided by many hospitals and websites, it has been widely accepted, and patients are likely to perceive less risk.
Conclusion
This study has both theoretical and practical implications. From the theoretical perspective, the established research model provides a novel perspective of patients’ online trust and their continued adoption of online healthcare services. The constructs of perceived risk and perceived benefit are merged into the model, which can be helpful for later behavioral research regarding on these two variables. From the practical perspective, this research is particularly important for healthcare suppliers as it provides insights on retaining users. First, different forms of service attract different users. Identifying the influential factors can help service providers focus on different services and target users. Second, patients’ online trust positively affects behavioral intention. It indicates that the continued adoption intention of online healthcare services could be influenced by trust. Therefore, building a high level of trust environment is vital. The healthcare service providers and website developers can raise the level of trust by increasing the perceived benefit or lowering the perceived risk. For example, healthcare organizations could make their websites more user-friendly and reduce users’ concerns by publishing feedback from other consumers who have used them to obtain information, make appointments, or consult with providers. Third, the results show that perceived benefit is more influential, implying that providing benefits is more efficient to retain users than controlling the risk of online healthcare services. Under a resource limited scenario, creating more benefits for users is more effective for online healthcare service providers. Fourth, patients with various purposes of use differ in their perception of risk, benefit, and trust, and so, the organization’s strategy should be more personalization with a special focus on targeted groups.
Our study has several limitations. First, healthcare services differ from common consumer products and services. For example, online healthcare services cannot be seen and touched in the real world, and their actual usage may vary according to people’s health conditions. Further studies are needed to explore the special characteristics of online healthcare services. Second, we only examine the moderating effect of purpose of use on patients’ online trust, other factors such as gender, health conditions, or Internet experience may also have similar moderating effects. For example, although online healthcare services are helpful for older users, they may not think the services are safe. The perceived risk of older users may be higher than that of younger generations. In addition, people’s decisions to continue using online healthcare services may vary across ages or different levels of Internet experience.
In this study, we propose a research model based on perceptions of trust and theories of perceived risk/benefit. We also analyze the antecedents and the results of patients’ online trust and the moderating effect of purpose of use. Our findings indicate the trust is a predictor for the continued using intention of online healthcare services in China. The factors and results identified in this research may shed light on improving outreach strategies for providers of online healthcare services.
Footnotes
Acknowledgements
The authors sincerely thank the editor and the anonymous referees for the constructive reviews. In particular, the authors would like to sincerely appreciate John Huppertz for his great support and editing proof work for this paper.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by grant from the National Natural Science Foundation of China under grant no. 71671073.