
Abstract
Background
Gamification within eHealth services can increase eHealth adoption. However, little is known about factors affecting adoption of gamified eHealth among older adults. In this study, we sought to explain the (continued) use of a gamified eHealth service among older adults (55+).
Methods
Participants used a gamified eHealth service, focusing on falls prevention, for 4 weeks and completed a post-test questionnaire based on the Technology Acceptance Model. We used Partial Least Squares Structural Equation Modeling to analyse our data.
Results
Seventy-two older adults participated with a mean age of 65.1 years (SD = 7.0). Our results show that first, perceived ease of use affected use of the service (use duration: β = 0.303, R2 = 0.130, and use frequency: β = 0.304, R2 = 0.107). Second, perceived usefulness affected the intention to continue using the service (β = 0.754, R2 = 0.640). Third, use of the service did not predict the intention to continue using it. Furthermore, enjoyment affected perceived usefulness (β = 0.783, R2 = 0.563) and aesthetics affected perceived ease of use (β = 0.634, R2 = 0.652).
Conclusions
This study refutes the expected relation between use and intention to continue use a gamified eHealth service. Additionally, we learned that using theoretical approaches focusing on technology acceptance, are not suitable for explaining (continued) use of gamified eHealth services.
Introduction
Gamified eHealth services can be a means to improve users’ engagement with eHealth services.1–3 Since 2010, gamification (defined as “the use of game design elements in non-game contexts” 4 ) started to emerge in eHealth services. 1 Randomized Controlled Trials have shown that the target population used eHealth services more and dropped out less often when the eHealth service included gamified elements compared to non-gamified counterparts (e.g. Refs. 5 and 6). Furthermore, a recent meta-analysis showed that gamified eHealth services focusing on physical activity were more effective in improving one’s physical activity compared to non-gamified eHealth services. 7 These studies suggest that gamified eHealth services might be a solution to tackling the high drop-out rates among eHealth users, which could, in turn, could improve the effectiveness of the service.
For older adults, eHealth has great potential. It can be part of ensuring older adults to live longer at home, to manage their own health, and to increase their health literacy.8–13 Looking at gamified eHealth services for older adults, these are mostly used in their home environment, and most of these type of eHealth services focus on users’ physical health. 14 In rehabilitation care, it is very common to use gamified eHealth services. 15 A review study by Skjæret and colleagues 16 investigated the use of gamified eHealth in rehabilitation care for older adults. They found contrasting evidence towards the adherence to the therapy. In some studies, participants in the gamified group adhered better to the therapy compared to the control group (offline therapy), and in others they did not find a difference.
Looking more closely at literature focussing on gamified eHealth services, lots of studies report the design process of the service or explain the service itself (e.g. Refs. 3, 17 and 18). The amount of literature available about gamified eHealth service shows us that gamification within eHealth is an acceptable concept. However, to the best of our knowledge, no study is conducted to uncover antecedents of the intention to continue use a gamified eHealth service among older adults. Most of the studies involving older adults exploratively assess users’ opinions towards these services. For example, Minge and colleagues 19 conducted focus groups and concluded that older adults are positive towards gamified eHealth services. In other studies that looked at the feasibility of gamified eHealth, older adults were also positive towards the gamified eHealth service: they enjoyed using it.20,21 However, if such a service loses its seriousness (e.g. because of too many fun, useless elements), older adults consider these services as less helpful. 19 Investigating studies involving younger adults, we can hypothesize that ease of use, enjoyment, attitude 22 and social influence 23 positively affect the continued use of a gamified exercise service, and usefulness and playfulness indirectly affect the continued use (via attitude).
Knowing the antecedents of older adults’ intention to continue use a gamified eHealth service provides developers and researchers guidance when developing, evaluating and implementing gamified eHealth services. This allows for a better fit between the gamified eHealth service and older adults, which, in turn, leads to increased engagement with the service. 24 Building forth on the Technology Acceptance Model25,26 we conducted a study to identify these antecedents and to explain the use and the intention for continued use of a gamified eHealth service among older adults.
Method
Participants and Study Procedure
The study population consisted of older adults aging 55 years or older speaking Dutch, with access to a computer, laptop or tablet. We recruited participants through mass mailing, advertisements in local newspapers, physical therapists and snowball sampling. Older adults who wanted to participate, contacted the researcher, after which the researcher checked the inclusion criteria. After inclusion, participants completed a pre-test questionnaire consisting of demographics. Then, they received access to the gamified eHealth service from the researcher, and they used it for 4 weeks. The participants received a manual from the researcher (see Supplemental Material) with instructions how to use the service. Finally, they completed a post-test questionnaire consisting of the antecedents for adoption.
Intervention: a Gamified eHealth Service
The gamified eHealth service that the older adults used was called Stranded (see Figure 1). Stranded is an online environment in the form of a deserted island and consists of two parts: a falls prevention program and minigames. Older adults were involved during the development of this eHealth service.
27
When logging in into the eHealth service, the service shows the user how the protagonist ended up on a deserted island. The user plays with the protagonist and can help her to leave the island by performing physical exercises and completing minigames. When a user opens his/her training programme, a secondary window is opened in which the program is provided in the form of exercises shown via video, instructed via sound, and explained by text. The physical exercises are part of the OTAGO falls prevention Programme.
28
The program consists of three weekly sessions with a warming-up, training exercises, and a cooling-down. Previous studies evaluated the OTAGO programme positively,29,30 also in an online setting.
31
The minigames within this eHealth service are cognitive minigames (i.e. mind games to activate the brain) and were unlocked after participants completed their exercises, as a reward. The first minigame unlocked after completing the first training session, and from the remaining minigames, each minigame unlocked after completing 3 training sessions. In this eHealth service, the following four motivational affordances
32
from the gamification movement are incorporated: A story (there is a story on how the protagonist ended up on a deserted island, and how the user can build a boat to leave the island), rewards (by completing the physical exercises, users can unlock minigames as a reward), levels (the minigames have difficulty levels), and progress (when completing minigames the user earns boat parts to leave the island). Screenshot of the homepage of Stranded.
Research Model and Questionnaire
The gamified elements included within Stranded, are subordinate to the physical exercise module. Therefore, we used the Technology Acceptance Model (TAM)25,26 to investigate the use and intention to continue use, rather than a model focusing on assessing the gaming experience (like the theory of Core Elements of the Gaming Experience 33 ). Furthermore, previous literature on the use of digital games with an educational meaning among older adults also showed that these applications need to be easy to use and useful, 34 which are included in the TAM as well. From the existing theoretical approaches which are being used in explaining eHealth acceptance, we decided to use the TAM due to pragmatic reasons: only three constructs and no sample size power issues. We did expand the TAM with some additional variables that predict the core variables ease of use and perceived usefulness, in order to increase the model’s explanatory power.
The additional variables we included were enjoyment, aesthetics and control. It has been found that enjoyment of a digital game was a strong predictor for older adults to play a game (again).35–37 Multiple studies found that aesthetics of a serious game or gamified eHealth service influence older adults’ use of the technology.38,39 Khalili-Mahani and colleagues 38 found that aesthetics are important; too intense aesthetics (i.e. a confusing and distracting appearance) of a serious game, led to more frustrations among older adults during use of the game. Finally, control increases older adults belief to acquire the habit to play the serious game, which affects the adoption of the eHealth service. 40 All together, we think that enjoyment of a gamified eHealth positively influences its perceived usefulness, and aesthetics and control influence its perceived ease of use.
The factors mentioned above are all included in the research model defined (see Figure 2). Additionally, we included use of the gamified eHealth service in our causal model. A lot of studies using the TAM, assess the intention to use as proxy for use. As in our study older adults used the service for 4 weeks, we had access to use data and had the opportunity to include it in our model. There are two use constructs in our model, one measures the total duration in minutes older adults used Stranded, and the second one measures the frequency participants used Stranded, during the 4-week period. These use constructs are measured with system log data. The causal model defined.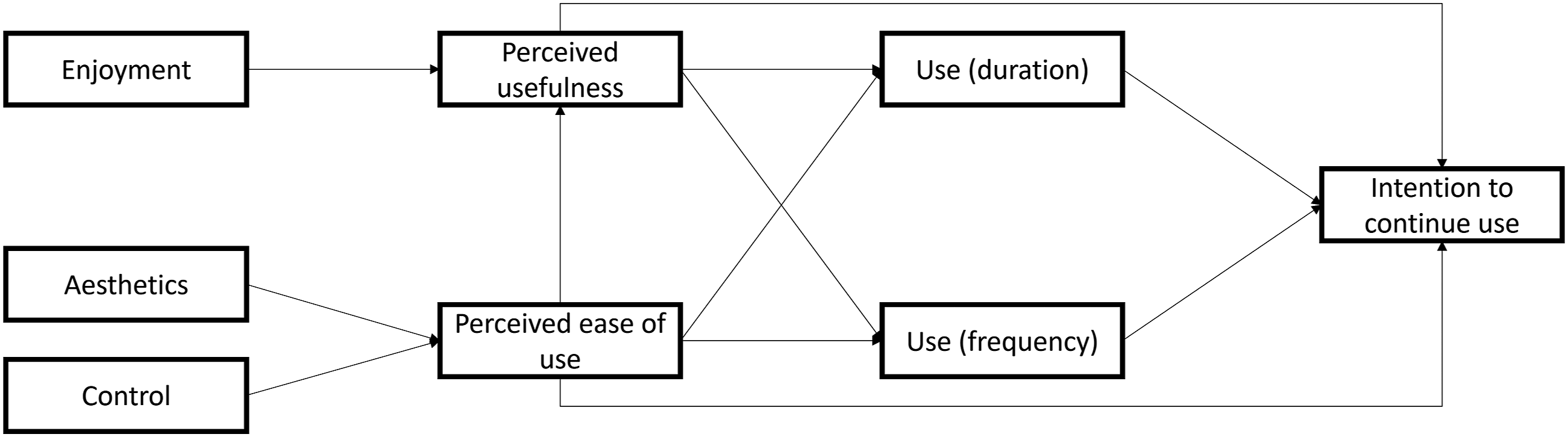
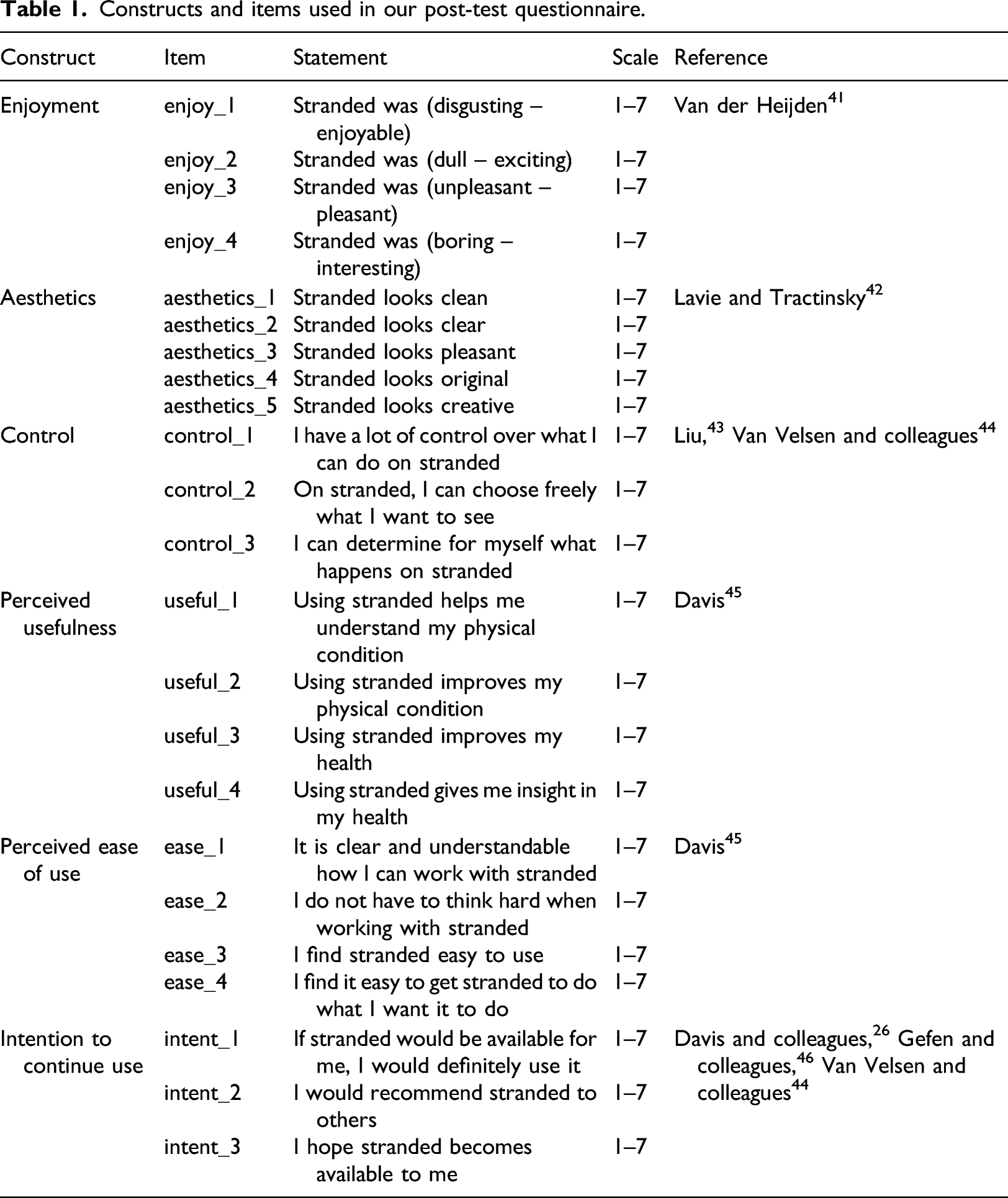
Constructs and items used in our post-test questionnaire.
Data Analyses
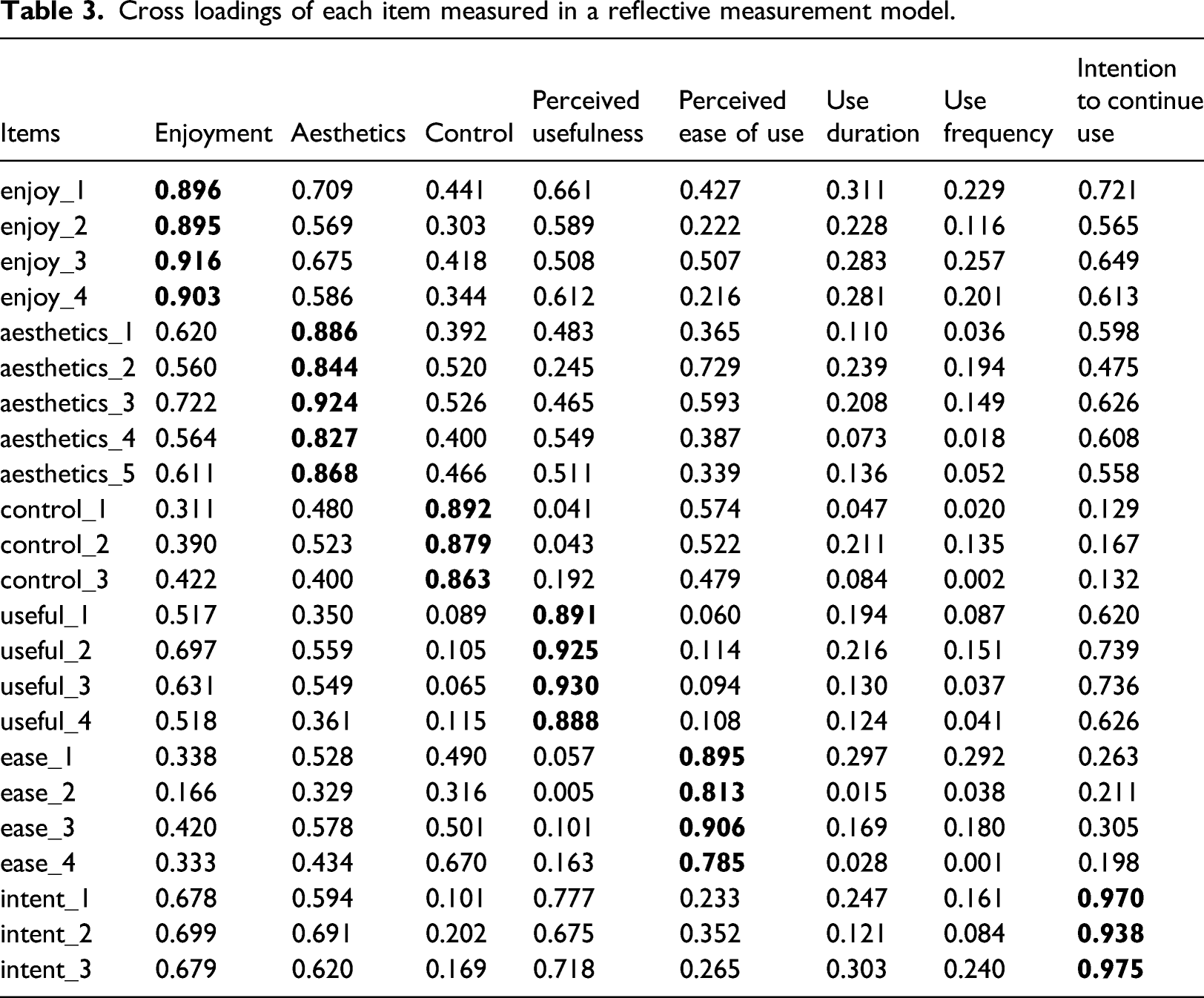
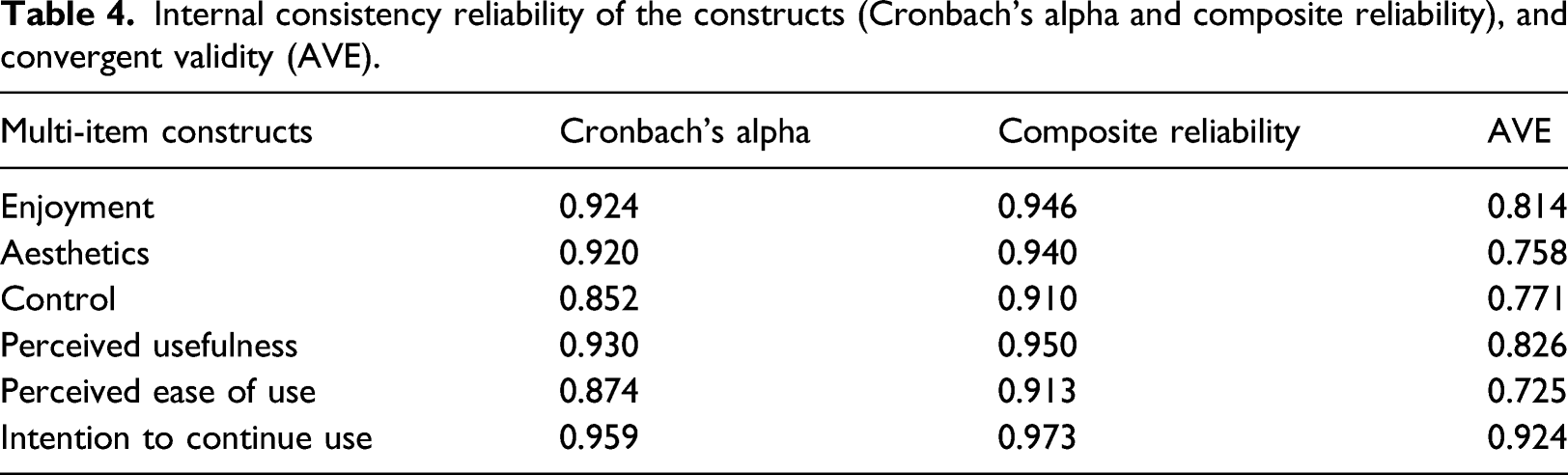
Descriptives were calculated for participant demographics, use of Stranded, and questionnaire constructs (means, standard deviations) in SPSS (version 19). We used Partial Least Squares Structural Equation Modeling (PLS-SEM) in SmartPLS 3.0 47 to test the research model. The maximum number of constructs influencing another construct is 4. So, the minimum sample size needed for analysing our model is 41 participants, based on a statistical power of 80%, significance level of 5% and a minimum R2 of 0.25. 48 For the model validation we used reflective and formative measurement models to optimize and assess the quality of our model. We started with the reflective measurement model. With this we assessed the indicator reliability (outer loadings) and discriminant validity (cross loadings) of the items, the internal consistency reliability of the constructs (Cronbach’s alpha and composite reliability), and the convergent validity (Average Variance Extracted (AVE)). Then we continued with the formative measurement model to assess the level of collinearity between items (Variance Inflation Factor (VIF) values), relative importance of indicators (outer weights), and absolute importance of indicators (outer loadings). After these steps, we determined our formative causal model, with which we determined the path coefficients (β), the model’s predictive power (R2), and effect sizes (f2). For all bootstrapping procedures we used 5000 subsamples.
Ethical Considerations
We conducted this study according to the principles of the Declaration of Helsinki (64th WMA General Assembly, Fortaleza, Brazil, October 2013). For this study, we did not require formal medical ethical approval according to the Medical Ethical Committee Arnhem-Nijmegen (file number: 2019–5296). Each participant signed an informed consent form beforehand.
Results
Demographics
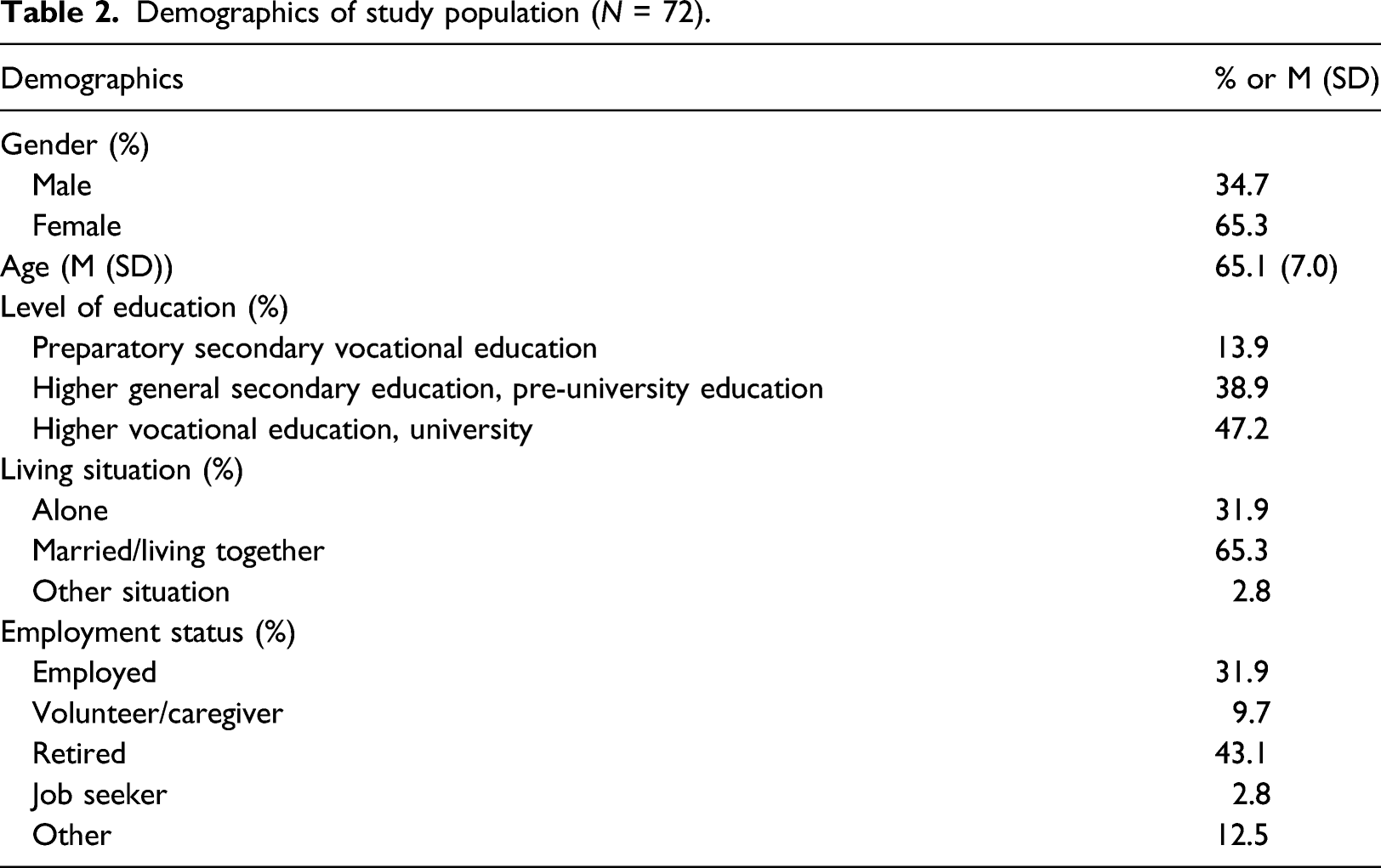
Demographics of study population (N = 72).
User Experience
Regarding the post-test questionnaire, all constructs scored above the average. Participants were most positive about Stranded’s aesthetics (M = 4.7, SD = 1.3, N = 72). In the box plot of Figure 3 we see that in all constructs there is a wide range in the distribution of participants’ user experience with Stranded, and the medians of the constructs lie between 4.0 and 5.0. Box plot user experience domains measured on a scale from 1 (negative) to 7 (positive) (N = 72).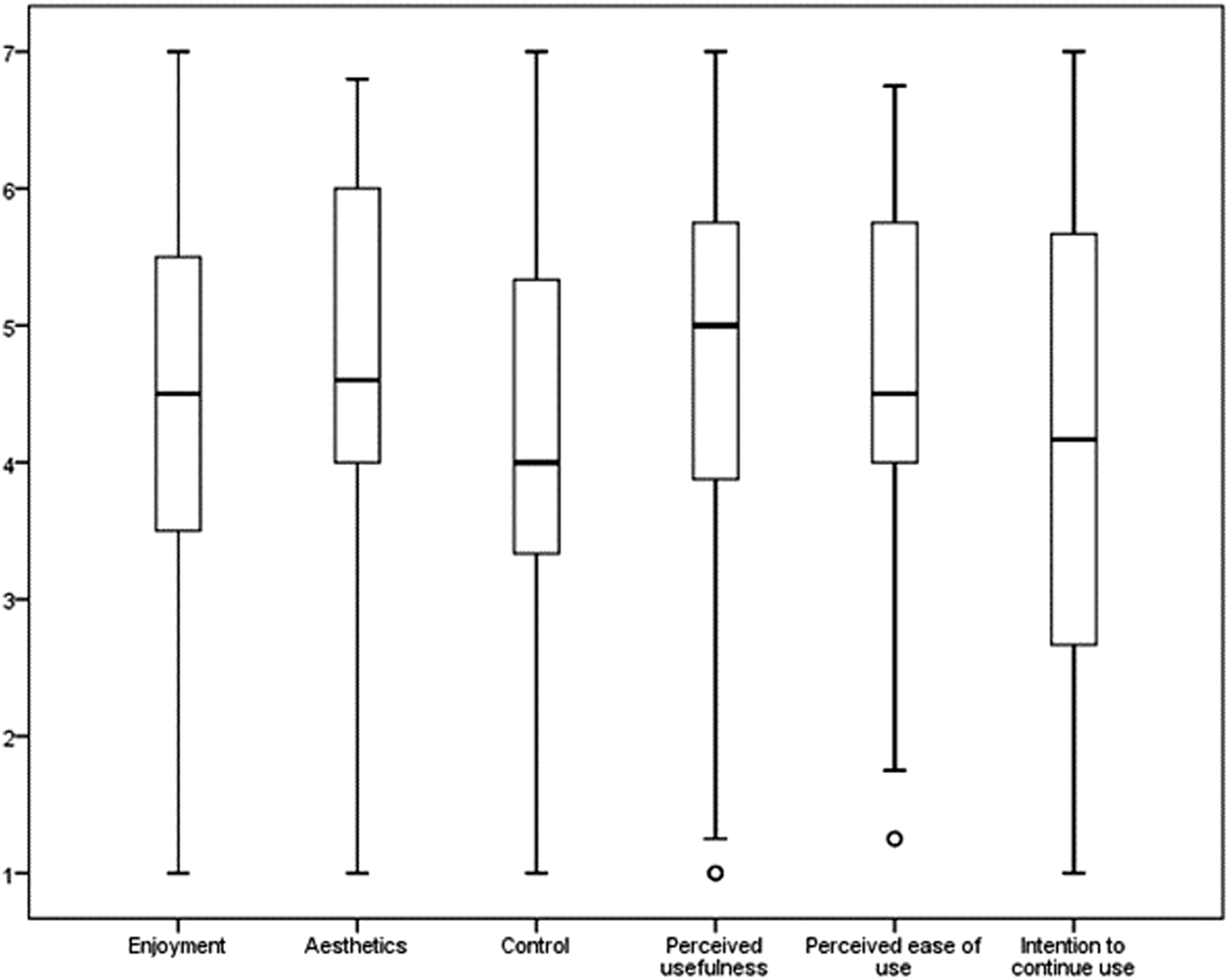
Use Data
During the first week of the study, 72 older adults used Stranded, and in the last week 51. On average, participants used Stranded 17.1 times (SD = 12.9) during the study period, with a range from 1 time to 74 times. The mean duration participants spent on the Stranded platform was 764 min and 52 s (SD = 678 min and 47 s). The minimum duration spent on the platform was 5 min, and the maximum was 3463 min (57 h, 43 min). On average, one session lasted 42 min and 22 s (SD = 20 min and 43 s).
Model Validation
Cross loadings of each item measured in a reflective measurement model.
Internal consistency reliability of the constructs (Cronbach’s alpha and composite reliability), and convergent validity (AVE).
We then switched from a reflective measurement model to a formative measurement model to further assess and optimize the model. By assessing the VIF values, we checked for multicollinearity. A VIF value of 5.00 or higher, indicates multicollinearity. Five items had an outer VIF value higher than 5.00. First of all, item 3 of the aesthetics construct had an outer VIF value of 5.147. The question belonging to this item (“Stranded looks pleasant”), is equivalent to item 3 of the enjoyment construct (“Stranded was [unpleasant – pleasant]”), so we deleted item 3 of the aesthetics construct. Two items (item 2 and 3) belonging to the perceived usefulness construct had an outer VIF value of 5.907 and 6.22 resp. The questions of these items are “Using Stranded improves my physical condition” (item 2), and “Using Stranded improves my health” (item 3). These questions resemble each other, but because the VIF values are still beneath 10.00, so still acceptable, 49 we did not delete these. The same applies for item 1 (“If Stranded would be available for me, I would definitely use it”) and item 3 (“I hope Stranded becomes available to me”) of the intention to continue use construct, that had outer VIF values of 8.794 and 9.847 resp. Looking at the inner VIF values, no values were above 5.00.
The last step in assessing our model and before determining the causal model, is assessing the significance and relevance of the formative items, with outer weights and outer loadings. To assess this, we ran a complete bootstrap procedure with 5000 subsamples. Four outer weights were significant (p < .05) and stayed in the model. All other items did not have a significant outer weight, but looking at the outer loadings, all items, except for one (item 2 of perceived ease of use), had a loading of 0.5 or higher. So these items were absolutely important, even though they were not relatively important, and could stay in the model. Item 2 of perceived ease of use had an outer loading of 0.472, but the p-value showed that it was significant (p = .015). So we also retained this item in the model.
Causal Model
Figure 4 shows our causal model. Five path coefficients were significant. Of these significant relations, we determined the effect sizes (f2). The effect size of the relation between perceived usefulness and intention to continue use was 1.498 (large effect size), between enjoyment and perceived usefulness was 1.25 (large effect size), between aesthetics and perceived ease of use was 0.794 (large effect size), between perceived ease of use and use in duration was 0.104 (small effect size), and between perceived ease of use and use in frequency was 0.102 (small effect size). Causal model.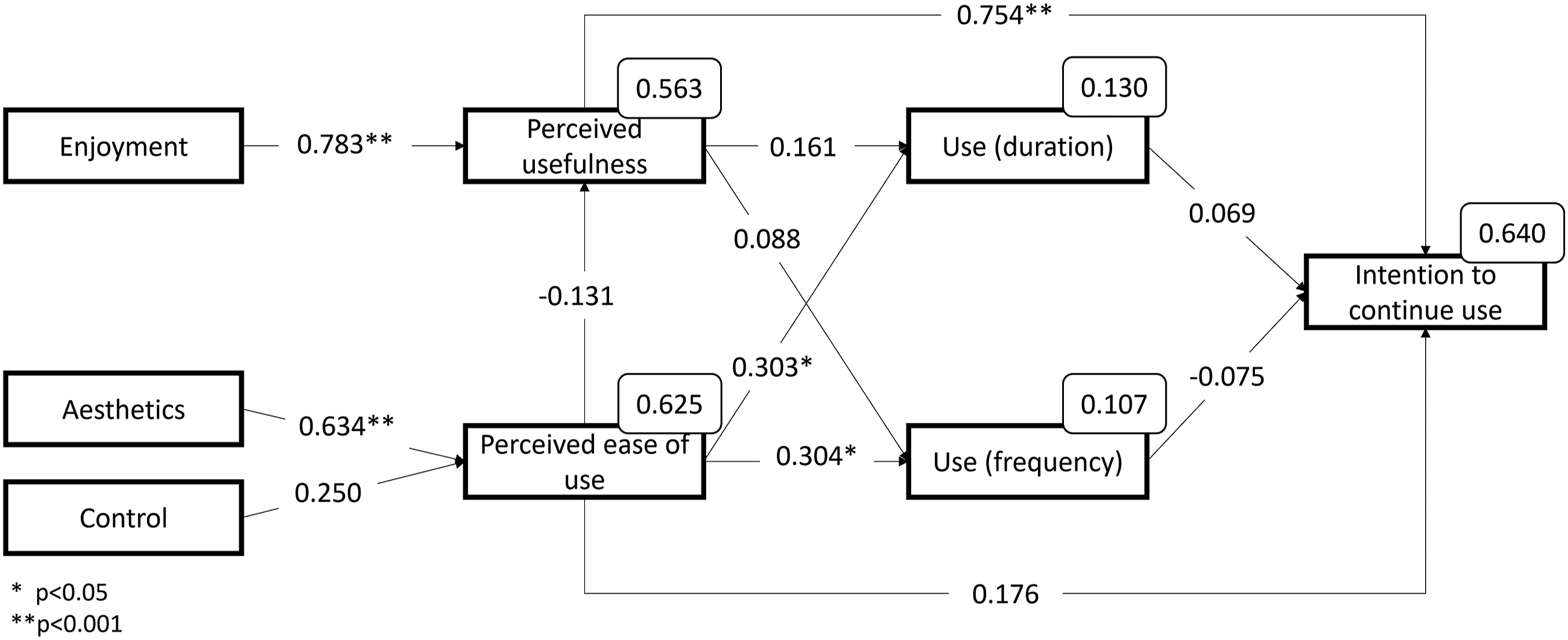
Despite those five significant path coefficients, our model also shows six insignificant path coefficients, which were not expected. Especially the following findings: perceived usefulness did not affect use, perceived ease of use did not affect intention to continue use, and use did not affect intention to continue use. These path coefficients and effect sizes were really small (β from −0.075 until 0.176, and f2 from 0.004 until 0.076), so even if they were significant, the effects of these factors would be low.
Discussion
With this study we aimed to explain the use of and intention to continue using a gamified eHealth service for older adults (in this study, a gamified falls prevention program, supplemented by cognitive minigames: Stranded). The majority of the older adults used the eHealth service for a period of 4 weeks and multiple times per week. A striking finding is that how often and how long older adults used Stranded did not affect their intention to continue using it. For this type of eHealth, aesthetics affect the perceived ease of use, while control does not. Enjoyment affects the perceived usefulness. Use, in terms of duration and the number of log ins, is predicted only by perceived ease of use. Our model has a high explanatory power for the intention to continue using the service.
We did not expect the lack of a relation between the use parameters and the intention to continue using the gamified eHealth service. On the contrary, given the literature on this topic,50,51 we expected that short-term use of a gamified eHealth service would be the main predictor for the intention to continue use. Upon reflecting on this issue, we think there are several possible explanations for this lack. First, a methodological explanation. In this study, we looked at two realities. One being the study context in which participants were asked to use the eHealth service and answer questions about its characteristics (e.g. aesthetics, perceived usefulness, etc.), and one being the hypothetical situation in which they would use the technology for their own good beyond the study (i.e. intention to continue use). We think that there is a possibility that a part of the participants were using the eHealth service to, among other reasons, also please the evaluators. The second explanation could be that participants indicated they did not want to continue using the service, because of a lack of novelty, or boredom. The gamified eHealth service does have difficulty levels in the falls prevention programme, and different minigames that can be unlocked. However, eventually, users will not have new content anymore, as the storytelling comes to an end: Building all boat parts, and being able to leave the island. In our study, we merged the use data from the 4-week period in two parameters: the frequency they used it in total, and the minutes they spend interacting with the eHealth service. A previous meta-analysis showed that eHealth apps focusing on improving physical activity is more effective in short-term use. In this meta-analysis, the authors are talking about a period shorter than 3 months. 52 However, it could also be the case that in our study the novelty and excitement were mostly present in the first 2 weeks. Mazeas and colleagues 7 also suggest that users benefit more from short-term use, compared to long-term use. When assessing the influence of previous use on intention to continue use, we propose future research to focus on the evolution of eHealth use over the different weeks, instead of including use parameters which only show the total duration/frequency over all weeks together.
Furthermore, we found that the use of a gamified eHealth service among older adults was only affected by perceived ease of use and not by perceived usefulness. This is in contrast with previous studies on eHealth in general (e.g.53–57), and studies on the use of technology and games among older adults in general (e.g. Refs. 34, 35 and 58–60). Khalili-Mahani and colleagues 37 found that if the cognitive game is being perceived as enjoyable and useful, older adults are more willing to play the game again, independent of the difficulty. As a result of these studies, we expected that both perceived ease of use and perceived usefulness would influence the use of the eHealth service. An explanation for this could be that the use of a gamified eHealth service among older adults is being influenced by other antecedents than those we expected and included in our model. Looking at our causal model, we see that the influence of perceived ease of use on use is weak, and the predictive powers of use in our model confirm this, which are both weak. As said previously, we think that use in our study was influenced by the fact the older adults were participants of a study. D’Haeseleer and colleagues 61 found that older adults perceive a self-management eHealth service useful, but not for themselves. Perhaps this was also the case in our study, which explains why we found no relation between perceived usefulness and the use parameters, and a weak relation between perceived ease of use and the use parameters. To confirm this, we recommend that future research should focus on reasons why older adults use gamified eHealth services within a study setting, and why they use it beyond the study.
Based on our results, we would like to raise the question whether theoretical approaches, such as TAM25,26 are suitable for measuring gamified eHealth use and intention to continue use gamified eHealth. The TAM is frequently being used in studies focusing on this topic (e.g. Refs. 62–65), even though this approach is developed outside the healthcare setting to measure acceptance of general technology. However, as we found multiple relationships lacking (e.g. between perceived usefulness and use, between perceived ease of use and intention to continue use), we place a critical note on the use of this approach. In our opinion, this approach is too simple to address the complexity of eHealth use and intention to continue use eHealth. This shortcoming is also discussed in other papers.66,67 Therefore we recommend researchers to be cautious when drawing conclusions upon use of and intention to continue use eHealth based on the TAM. This model can be used as a first starting point in studying the use of and intention to continue use the eHealth service that is in development, but should not be used to reach a final conclusion on these topics.
Strengths and Limitations
Our study is, to the best of our knowledge, the first in explaining antecedents for use and for intention to continue use a gamified eHealth service among older adults. By uncovering these antecedents, researchers and gamified eHealth developers can increase the fit of the service to the users to increase eHealth use and adoption. Furthermore, the predictive power of our research model to identify the antecedents of intention to continue use was substantial. Besides these strengths, this study also has some limitations. First of all, we used self-enrolment to recruit participants; if one was interested in using Stranded, (s)he contacted the researcher. This could have resulted in selection bias and as a result, participants might have been more committed to using the gamified eHealth service. Another limitation of this study is the use of only one gamified eHealth service, which can affect the generalisability of our results. The findings of this study can be generalised to older adults aging 55 years or older using a gamified eHealth service focusing on falls prevention. However, for being able to generalise our results to gamified eHealth services among older adults in general, more research is needed in which the study population uses different gamified eHealth services focusing on other aspects of health (e.g. mental health, nutritional habits). Finally, a sensible and interesting addition to the research model would be the inclusion of end-user motivation, as for example explained by the Self Determination Theory. 68 Previous research has shown that motivation can be linked to persuasive features in eHealth technology, 69 and thus, it would be a valuable direction for future research.
Concluding remarks
Our intention of this study was to get a better understanding about participants’ use of and intention to continue using a gamified eHealth service, and therefore enriching the TAM as a tool to for assessing gamified eHealth acceptance. Instead, we learned that TAM is not the perfect fit for explaining gamified eHealth use and intention to continue use, as the relation between use and intention to continue use is more complex than envisioned beforehand. This disagreement with literature might be caused by our inclusion of system use data. Based on our results, we recommend researchers in the field of gamified eHealth use to focus on ‘perceived ease of use’ to explain short-term use of a gamified eHealth service, and to focus on ‘perceived usefulness’ to explain long-term use of a gamified eHealth service.
Supplemental Material
sj-pdf-1-jhi-10.1177_14604582221106008 – Supplemental Material for Game not over: Explaining older adults’ use and intention to continue using a gamified eHealth service
Supplemental Material, sj-pdf-1-jhi-10.1177_14604582221106008 for Game not over: Explaining older adults’ use and intention to continue using a gamified eHealth service by Marian ZM Hurmuz, Stephanie M Jansen-Kosterink, Hermie J Hermens and Lex van Velsen in Health Informatics Journal
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Eurostars-2 Programme (10824).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.