
Abstract
Autism spectrum disorder is associated with significant healthcare costs, and early diagnosis can substantially reduce these. Unfortunately, waiting times for an autism spectrum disorder diagnosis are lengthy due to the fact that current diagnostic procedures are time-consuming and not cost-effective. Overall, the economic impact of autism and the increase in the number of autism spectrum disorder cases across the world reveal an urgent need for the development of easily implemented and effective screening methods. This article proposes a new mobile application to overcome the problem by offering users and the health community a friendly, time-efficient and accessible mobile-based autism spectrum disorder screening tool called ASDTests. The proposed ASDTests app can be used by health professionals to assist their practice or to inform individuals whether they should pursue formal clinical diagnosis. Unlike existing autism screening apps being tested, the proposed app covers a larger audience since it contains four different tests, one each for toddlers, children, adolescents and adults as well as being available in 11 different languages. More importantly, the proposed app is a vital tool for data collection related to autism spectrum disorder for toddlers, children, adolescent and adults since initially over 1400 instances of cases and controls have been collected. Feature and predictive analyses demonstrate small groups of autistic traits improving the efficiency and accuracy of screening processes. In addition, classifiers derived using machine learning algorithms report promising results with respect to sensitivity, specificity and accuracy rates.
Keywords
Introduction
Autism spectrum disorder (ASD) is a lifelong, complex, neurodevelopmental condition characterised by impairments in the development of socio-communicative skills and the presence of repetitive or restricted behaviours and interests.1,2 ASD is the fastest growing developmental disability, and prevalence rates continue to rise at an incredible rate. 3 Current estimates indicate that about 1.5 per cent of the world’s population is on the autism spectrum, and it is thought that a large number of people with ASD in the community remain undetected.4,5 Therefore, growing awareness of ASD has increased the demand for self-administered diagnostic services. 6 This is of great importance since receiving an ASD diagnosis is a ‘critical milestone’, enabling parents to better understand the needs of their child and to have access to crucial support (therapy and special education). ASD is associated with significant healthcare costs, and early diagnosis can significantly reduce these.7–9 Unfortunately, wait times for an ASD diagnosis are lengthy (e.g. average waiting time in the United Kingdom is 3.5 years) due to the fact that current diagnostic procedures are time-consuming and not cost-effective.10,11
The rapid growth in the number of ASD cases worldwide necessitates developing easily accessible and effective ASD screening tools. 12 In addition, datasets on the traits, characteristics, diagnoses and prognoses of autism are rare. 13 Presently, few autism datasets associated with clinical diagnostics are available. The clear majority of available data on autism concerns the genetics of the condition. Few examples on those are the Autism Genetic Resource Exchange (AGRE), 14 National Database of Autism Research (NDAR) 15 and Boston Autism Consortium (AC) 16 but no behaviour data for screening of ASD.
To overcome the above two challenges, an ASD screening mobile application is proposed. This application offers friendly, time-efficient and accessible autism tests for all age categories. The proposed app can be utilised by a variety of stakeholders including parents, caregivers and more importantly health professionals to advise potential cases for further clinical assessments. Moreover, this app was able to derive valuable primary datasets related to toddlers, children, adolescents and adults that can be utilised for descriptive and predictive analyses. A feature analysis based on wrapping methods that integrates Naïve Bayes classifier showed small yet effective groups of features that can represent current autism self-administered screening methods (section ‘Data collected and analysis’ gives further details). In addition, two machine learning algorithms (Naïve Bayes and Logistic Regression)17,18 have been applied to show the significance of the features collected.
In this article, an innovative and interactive app that contains evidence-based short ASD screening tools for toddlers, children, adolescents and adults using the Autism Quotient 10 (AQ) and Quantitative Checklist for Autism in Toddlers (Q-CHAT) methods is developed.19–21 There are limited studies that have been conducted on developing interactive mobile platform autism tests for different types of users interested in autism. Furthermore, most of the current screening methods (such as AQ and Social Communication Questionnaire SCQ) take considerable time to conduct and their short versions have not yet been integrated into a mobile environment in order to speed the screening and increase accessibility for the healthcare community.22,23 By developing an interactive mobile ASD screening tool that covers the entire population, it will result in several distinctive advantages:
Collecting valuable data related to ASD for all age categories with new sets of features such as age, gender, born with jaundice and ethnicity among others.
Speeding up the referral process of ASD cases for further clinical review when the app is used by health professionals, especially in busy medical clinics and by general practitioners (GPs).
Increasing accessibility to ASD screening diagnostic tools among the general healthcare community and their stakeholders including individuals, parents, day cares, schools and medical clinics among others.
The ASD screening app can be used to collect data related to cases and controls that can be utilised for further analysis. Thus, this app can serve as a primary means for data collection, especially if the data related to ASD being sought is rare.
Awareness about ASD, its diagnosis and its effects will be enhanced over a large portion of the world since the ASD app tests are developed in 11 languages.
There have been recent attempts to develop mobile-based apps for different Pervasive Developmental Disorders (PDD), such as Asperger Syndrome and autism. Examples of these apps are Autism & Beyond (AaB), 24 Autism and Developmental Disorder Screening (ANDDS), 25 Autism Test, Asperger Test (AT), 26 and ASDetect 27 among others. These ASD apps have helped the community to only cover part of the problem or a certain PDD category but are not fully comprehensive enough to cover the complete ASD population. For instance, the AT app covers only adults with a certain PDD and contains 50 questions based on the AQ-Adult screening tool, making it time-consuming and highly specific. In addition, the ASDetect app is designed for toddlers younger than 2.5 years and is a video-based app that parents can use to look for autistic traits related to their children. Therefore, ASDetect cannot serve children over 2.5 years of age, adolescents and adults. Comparably, the AaB app offers a video platform that enables parents to analyse their kids’ behaviour and emotion traits without covering other ASD groups. Section 2 below discusses in detail the existing autism testing apps and reveals their positive and negative traits with an in-depth critical analysis.
Overall, an ASD screening app has yet to be seen, which embraces all age categories (infant, child, adolescent and adult), serves larger communities (the majority of the aforementioned apps are only available in English) and are short in length (3–5 min). Therefore, the proposed ASDTests app is designed and implemented to fit all age categories and serve larger communities worldwide (across 11 languages) while maintaining brevity (10 questions per test).
This article is structured as follows: section ‘Literature review: common ASDTests mobile applications’ examines current autism testing apps through literature review and critically analyses their advantages and disadvantages. In section ‘The proposed ASD mobile application (ASDTests)’, the structure and components of the proposed ASDTests app are shown, and the theory behind each test is revealed. Section ‘Data collected and analysis’ is devoted to the data description along with the descriptive, predictive and feature analyses. Finally, conclusions and thoughts on future work are presented in section ‘Conclusion’.
Literature review: common ASDTests mobile applications
This section highlights and critically analyses the available autism screening tests developed for the mobile environment. Any educational, awareness and non-screening apps are excluded from the literature review section. The functionalities of current autism apps are also briefly explained, and their strengths and weaknesses identified. To be exact, a table at the end of this section will provide all relevant details and functionalities of these apps.
AaB app
AaB is a video-based screening app developed in the United States by researchers from Duke University 24 and Apple in order to assist parents in identifying their children’s mental health challenges (anxiety or tantrums) that might relate to autism. Parents above the age of 18 years with children below the age of 6 years can use the AaB app. The app contains seven modules where three of which are questionnaires about family background, parental concerns and child’s temper tantrum. The seven modules consist of 50 questions plus four videos each approximately 30 s to detect the child’s emotions. The app is part of a study that has over 2600 participants and is only used to collect data related to the emotional behaviour of young children between the ages of 1 and 6 years. Even though AaB 28 has achieved 7 out of 10 ratings by users, it is limited in scope and does not cover a significant portion of ASD cases besides it cannot be used for instant screening. Moreover, user reviews revealed that the AaB app is time-consuming and not an adequate tool for screening all core ASD symptoms as, for example, RRBs. 24
Asperger Test app
The AT app was developed with the intention of providing a proper mechanism for adults to identify the possibility of Asperger or autism traits. While the AT app does not provide a formal diagnosis, it does provide guidance to users for understanding their socially related behaviours. Currently, two versions of the app are available: one for adults/adolescence and one for children. Each version contains 50 multiple-choice questions, which can be a hurdle for users, especially on a mobile platform such as smart phones. At the end of the test, users are given a score that denotes the chance of having autistic traits. 29 The AT app has obtained 3.9 ratings, and its user rate is higher than that of the AaB app. Most users found the AT 30 app useful, while a few users felt that the questions are somewhat forceful. In addition, the AT app has a wider scope than the AaB app, taking into account young children, adolescences and adults. Shorter versions of the app have been developed by Allison et al., 20 but have not been implemented in mobile environment.
Autism and Developmental Disorder Screening app (ANDDS)
ANDDS was developed to evaluate the risk of ASD and other progressive issues among toddlers aged from 6 months to children younger than 3 years. The app uses a series of Boolean (yes/no) questions that cover the child’s development behaviours at different age stages (i.e. 6, 12, 15, 18, 24 and 36 months). 25 Therefore, this app covers only a limited group and ignores a very large portion of the population (children >3 years, adolescent and adults). The questions developed for the ANDDS app were developed by behavioural scientists involved in ASD. The results of the app are displayed in three different coloured bands. Red is an indication for further medical evaluation, yellow denotes that parents should be more watchful of their child’s behavioural development and green shows that the child is in accord with their peers in terms of behavioural development. The ANDDS is not a popular screening test among users, however, as it has no rating.
Autism Test app
Autism Test Application (ATA) is a self-awareness app on autism and other related psychological challenges that can be taken by adults and in some cases by parents when conducting the test on behalf of a child. This app was developed for educational and research purposes to identify the common symptoms of autism in adults, and not for clinical diagnostic purposes. The app contains twenty questions, each with three possible alternatives (disagree, sometimes and absolutely), and it then generates a percentage of autism. One of the obvious major drawbacks of the ATA app is the quantification of autism in cases, as seen in the reviews given by users who have already taken the ATA test. For instance, feedback from individuals with a formal diagnosis of autism showed different scores when taking the test, making the result of the ATA questionable. ATA does not have specific questions that cover the complete range of ASD areas (stereotyped behaviour, communication, reciprocal and social interaction). Users have rated this app at 3.3, and a few have commented that the results generated by the app do not make any sense. 26 It is not clear what the methodology used to design the questions were and whether it is based on known, published, screening methods from behavioural scientists. The ATA app has a translated version in Arabic called Autism Test Light, which has a 2.5 rating and just two user reviews.
ASDetect app
ASDetect app uses a series of videos and non-videos combined with questionnaires for toddlers to evaluate the social and behavioural characteristics and can also be taken by parents and caregivers. At the end of each test, which takes approximately 20–30 min to complete, the app pinpoints the likelihood of the toddler possessing autistic traits. ASDetect app has three types of tests based on the toddlers age (12, 18 and 24 months). The app has been able to gain 4.5 ratings, the highest among other considered screening apps. 27 Research carried out by the app developers claims that the screening accuracy of the results generated by ASDetect is about 81 per cent when compared with export screening. Nevertheless, this has not been verified by independent researchers. Currently, there are 33 reviews of this app in which most were positive while some users commented about the comprehensiveness issue since the app only focused on the psychological behaviours of young children. Moreover, some reviews specified that the ASDetect app should cover a wider audience, especially for children older than 2 years, which has so far limited the use of the app among the health community for ASD screening.
Indian Scale for Assessment of Autism
One of the methods used to assess an individuals’ level of autism is the Indian Scale for Assessment of Autism (ISAA).31,32 An app based on the ISAA with English and Hindi versions was developed to help parents, particularly in India, to evaluate their child’s level of autism by answering 40 questions covering different autism areas. Each question has a number of alternatives and the user navigates through a large number of screens to receive their end score and its corresponding autism rate. Any score below 76 shows no autistic traits while any above 153 exemplify severe autistic traits. In-between scores exhibit differing autism levels. Currently, the app has 28 reviews with a 4.4 rating on Google store. No ratings or reviews are given on the ISAA app in the Apple store.
Naturalistic Observation Diagnostic Assessment app
Naturalistic Observation Diagnostic Assessment (NODA) is a medical research–based mobile app developed to provide parents with proper guidance on autism traits among children, and thus, the app is not a screening tool like the previous apps. 33 NODA uses a custom set of videos combined with the advice of experts to help parents understand the cognitive challenges of their children. To use the app, users must register and go through a verification process. They are then able to record and upload videos of their children on which experts can provide comments. Unfortunately, these processes (besides the technical skills needed to navigate through NODA) have limited its use among users and the health community. Currently, NODA has no reviews or ratings in either the Google or Apple stores. Finally, NODA generates a report for the user, so medical experts can use it during the diagnosis process later.
Table 1 shows a comparison between the previously discussed ASD mobile screening apps in terms of atypical features such as functionalities, coverage, rating, reviews and target users among others. Out of all of the autism testing apps considered, ASDetect and ISAA have been able to obtain good ratings with approximately 30+ user reviews. All the considered apps are using questionnaires to detect the autistic traits, and some such as AaB and ASDetect utilise videos. Apparently, questionnaires are more favourable to users than videos, as the apps that are using videos have gained little to no ratings from the users. According to user reviews, many believe video screening to be more time-consuming than taking a questionnaire-based test. In questionnaire tests such as AT, however, the number of questions made the screening process lengthy and users may lose interest in using the app over such time. The ISSA, AT and ATA apps seem to cover a larger segment of ASD users as they target both adults and children. Only a few apps are available in both Google play and Apple iTunes stores, making them accessible to both iPhone and Android users. The majority of the apps, however, offer their tests only in the English language and thus a larger audience is not able to make use of them. More importantly, no ASD testing apps have been found that cover toddlers, children, adolescents and adults collectively, making the available apps narrow in their scope of coverage.
ASD screening Apps in terms of their features.
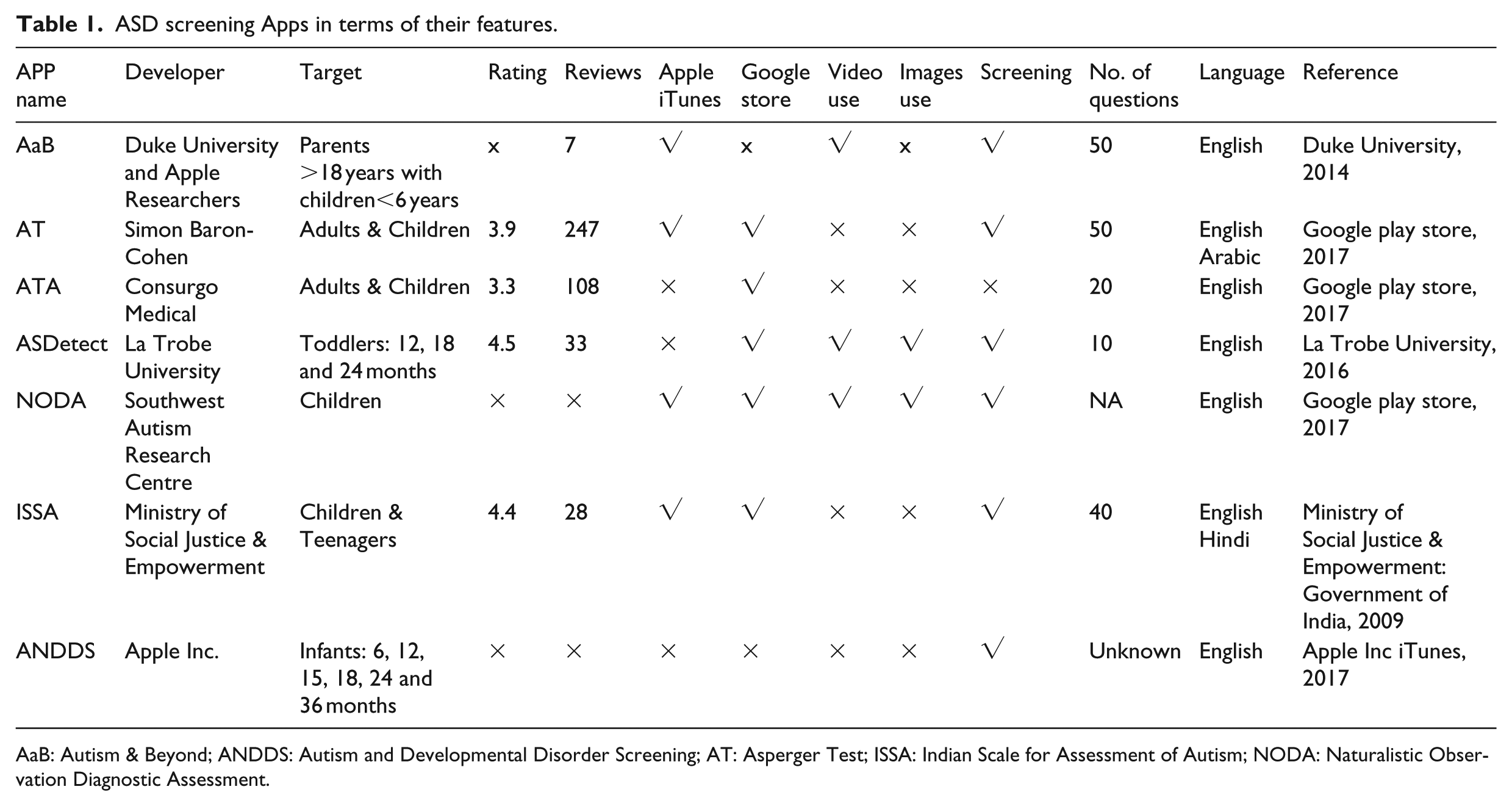
AaB: Autism & Beyond; ANDDS: Autism and Developmental Disorder Screening; AT: Asperger Test; ISSA: Indian Scale for Assessment of Autism; NODA: Naturalistic Observation Diagnostic Assessment.
The proposed ASD mobile application (ASDTests)
Designed for all user age categories, ASDTests app is based on two short versions of the AQ and Q-CHAT screening methods.20,34 It includes four key screening questionnaires, each of which contains 10 questions based on the user’s age category. To be exact, there is a questionnaire for infants (less than or equal to 36 months), children (4–11 years), adolescents (12–16 years) and adults (17 years and above) as displayed in Figure 1. Figure 1 shows the navigation diagram of the ASDTests app and on a higher level the key screens. In section ‘Key functionalities and data characteristics’, the functionalities, as well as the requirements of the proposed medical app, will be highlighted in detail.
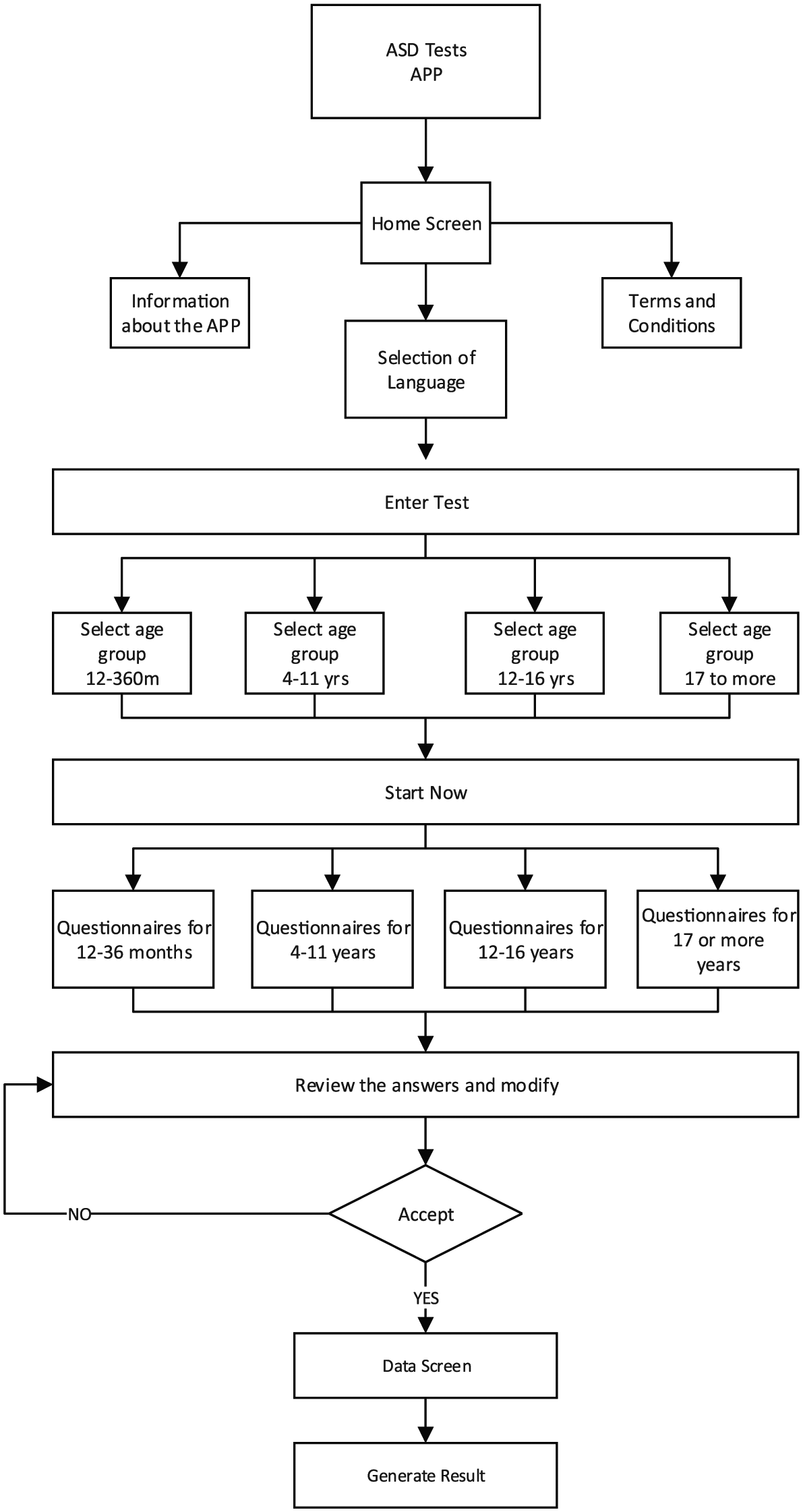
The proposed app (ASDTests) navigation diagram.
ASDTests Questionnaires
This section briefly describes the four autism questionnaires (modules) embedded within the proposed ASDTests app. In particular, the theory behind the screening tests that has been used for each age category in the app is highlighted.
The Toddlers Questionnaire (Q-CHAT)
The Checklist for Autism in Toddlers (CHAT) method was developed to detect autism in toddlers less than 18 months. Later, Robins et al. 34 enhanced the sensitivity of the original CHAT method and proposed the modified CHAT (M-CHAT). In both the CHAT and M-CHAT, there are over 20 questions that needed to be filled in order to assist healthcare specialists in differentiating cases from controls for further referrals. Recently, M-CHAT was shortened to just 10 questions by Allison et al., 20 in which the authors analysed the different versions of CHAT and AQ to reduce the time spent during screening by clinicians. The methodology adopted by the authors is to merely keep the most significant items during the screening based on computing a discrimination index. Evaluation using primary data collected consisting of cases and controls showed that the shorter version of M-CHAT was acceptable in terms of sensitivity and specificity rates. Allison et al. 20 illustrated the questions in the 10-Q-CHAT version along with possible alternatives and the way scores are computed.
AQ Test and Its Short Questionnaires (adult, adolescent, children)
The Autism Spectrum Quotient (AQ) is one of the early autism screening tools that was designed by behavioural scientists at the University of Cambridge to enable adults with an average IQ to detect autistic traits in a self-administered questionnaire. 19 Originally, the AQ test consisted of 50 questions that belonged to five areas related to autism’s cognitive strength (communication skills, imagination, attention to details and attention to switching and social skills). Later, slightly different versions of the AQ test were developed to cover children and adolescents.20,35,36 Each question in the AQ is associated with four possible alternatives (definitely agree, slightly agree, slightly disagree and definitely disagree) and is scored a point.
Allison et al. 20 proposed a simplified adult version of the original AQ test called AQ-10-Adult. The AQ-10-Adult test uses four choices per question (definitely agree, slightly agree, slightly disagree and definitely disagree) that the user should select during the screening process. Then, a handcrafted diagnostic rule is utilised to compute the score. Any individual who scores more than 6 is then referred for a full ASD diagnostic assessment. The screening rule often considers one point per question. To be exact, a point is assigned if the answer is either ‘Lightly Agree’ or ‘Definitely Agree’ for questions 1, 7, 8 and 10. In addition, a point is added if the user’s responses to questions 2, 3, 4, 5, 6 and 9 were either slightly or definitely disagree.
Finally, Baron-Cohen et al. 35 and Auyeung et al. 36 developed full AQ versions for adolescents and children, respectively. Then, Allison et al. 20 proposed shorter versions for the full adolescent and children AQ tests. Score calculations for the adolescent and child short versions are different from the AQ adult short version; however, details of the questions, and the scoring of the adolescent and children AQ short versions, can be found in Allison et al. 20
Key functionalities and data characteristics
Besides the landing, information and terms and conditions screens, the key function of the ASDTests app is to enable different types of user to measure ASD traits using four different modules (discussed in section ‘AQ Test and Its Short Questionnaires (Adult, Adolescent, Children)’). Initially, the user from the landing screen (Figure 2(a)) chooses the language from 11 available languages and then selects their test based on the age category screen (Figure 2(b)). Based on the age chosen, the user is relayed to the appropriate ASD screening test. Each test consists of 10 questions in a sequential order, and each is associated with an image to enable users to carefully select the appropriate answer. Users can use touch screens to navigate through the app, which can be run on smart phones (Android and IOS) as well as tablets. Figure 2(c) displays one sample question from the toddler test. Once the user completes the test (goes through the 10 questions), then a screen emerges to review the answer (Figure 2(d)). In this screen, the user can review their answers and amend any they wish. The screen serves as a quality assurance measure so that users can review and verify answers before progressing to the data input screen (Figure 2(e)).
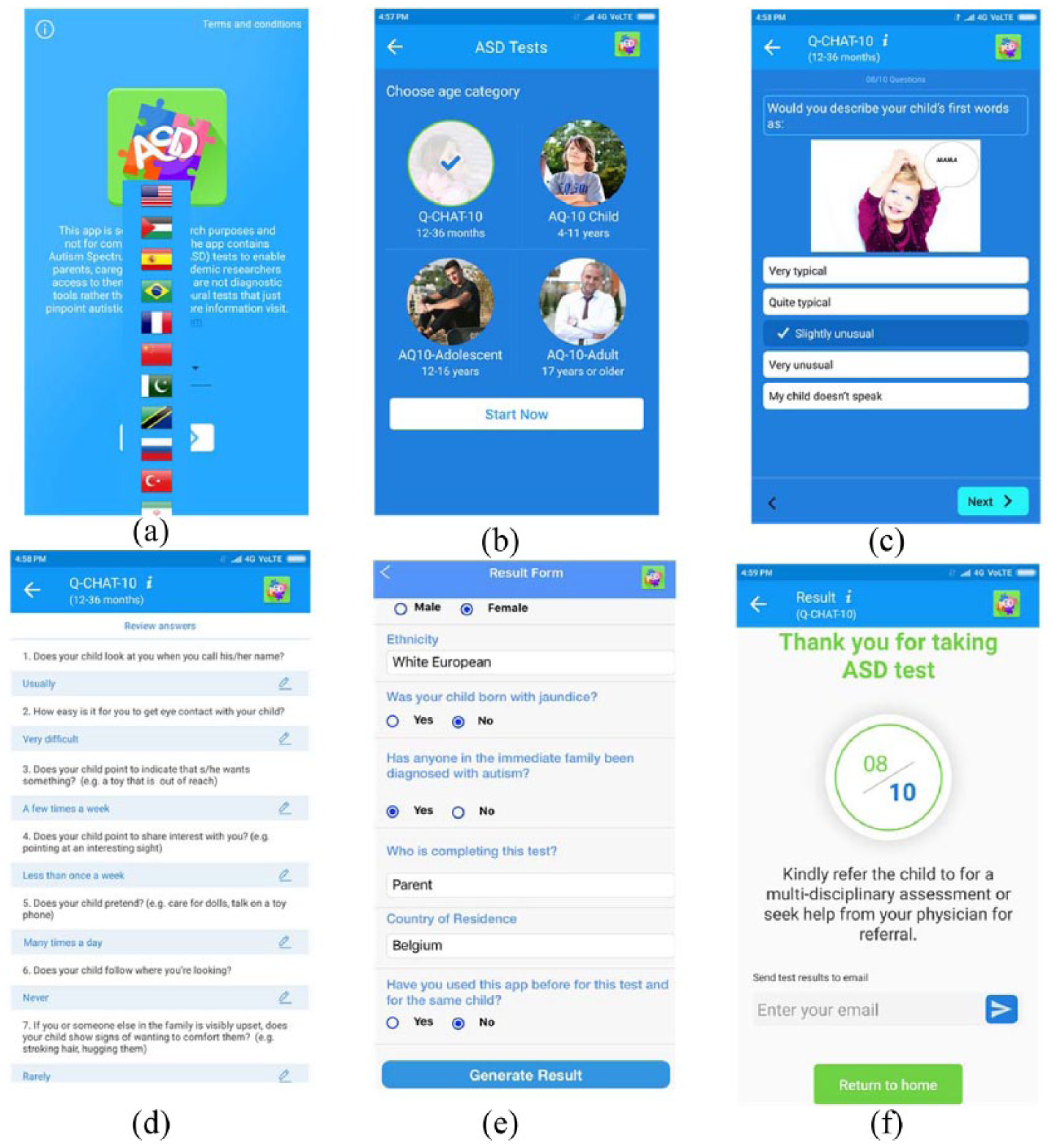
(a) Landing screen, (b) age selection screen, (c) a sample question: toddler’s test, (d) answer review screen, (e) data collection screen and (f) results screen.
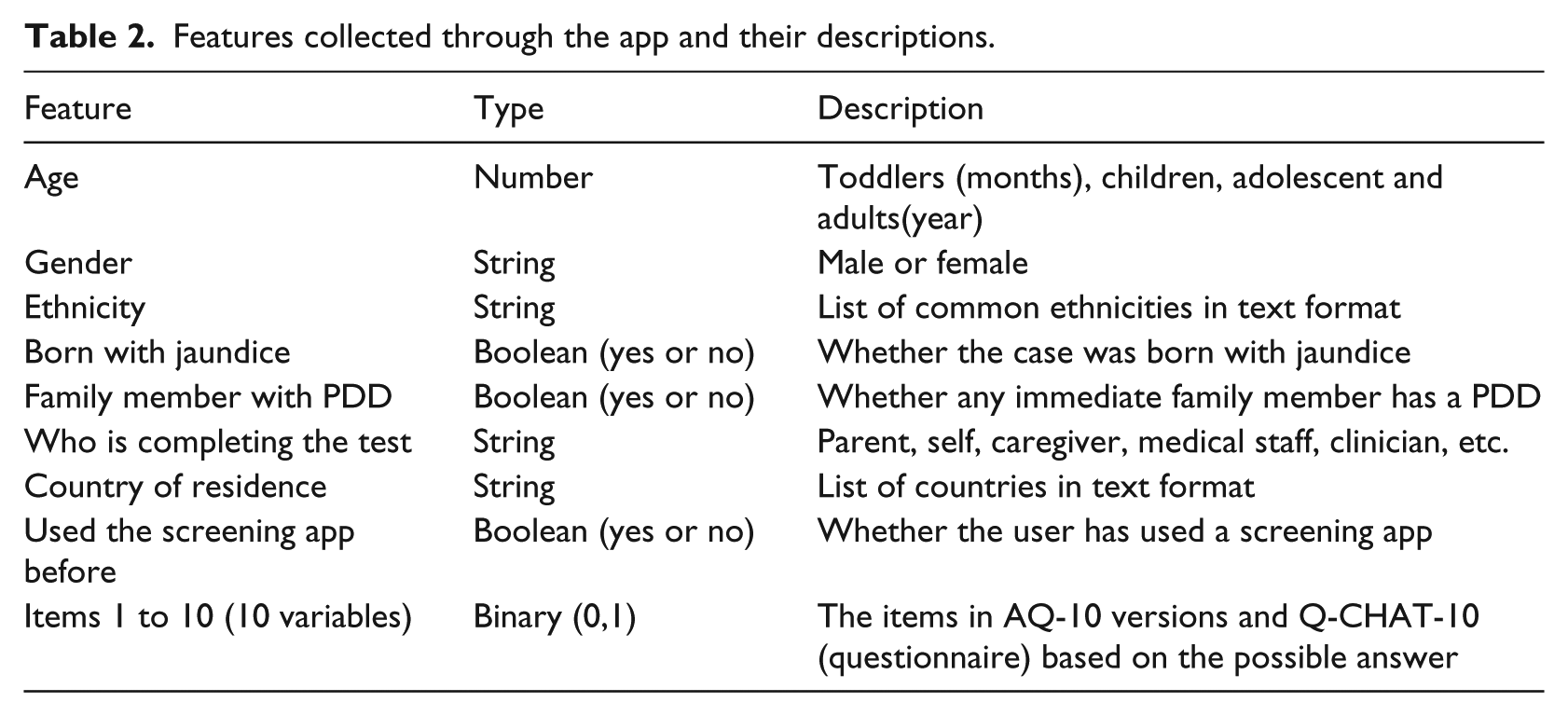
The key functionality of the data input screen is to collect relevant useful data about the case undergoing the screening. In particular, the features shown in Table 2 are collected. These features are stored in an MYSQL database and can be used for further data analysis later on to understand key features that may influence ASD diagnosis from a behavioural science perspective. One possible way to conduct data analysis is using computational intelligence and machine learning, as was utilised here.37–39
Features collected through the app and their descriptions.
Once the user clicks the submit button on the data screen, they will be automatically redirected to the results screen (Figure 2(f)). This screen contains the results and their translation based on the test type. On the back end, a function is built to compute the score and then corresponds each score with the appropriate text that the users will see in the results screen. For instance, say a parent is taking the ASD test for toddlers and the score obtain was 8. This indicates that the toddler should be referred to a health professional for clinical assessment of ASD. In the toddler test of our app (Q-CHAT-10), a score greater than 3 denotes a clinical assessment being necessary, otherwise no autistic traits are found. 20 The computations of the scores for the four modules (tests) in the app have been coded to enable users to obtain the score as well as its interpretation in a facilitative way. Moreover, the user can also email the results using the email functionality (Figure 2(f)) where a professional grade Portable Document Format (PDF) file that contains the necessary information about the case under consideration (case features, answers given, screening results, disclaimer, etc.) is constructed and emailed to the user (Figure 3). Finally, at any time during the ASDtests app, the user can terminate the test and return to the main screen.

The generated report by the ASDTests app.
The ASDtests app is available for download on iTunes and Google Play stores since 12 September 2017. Currently, it has over 900 downloads overall and a rating of 4.8 out of 5 on the Google play store with 111 user reviews. 40
Data collected and analysis
Table 3 shows 20 sample data instances that have been collected based on the AQ-10 Child assessment. In Table 3, A1–A10 are the questions in the screening methods embedded within the ASDTests app. The values (0, 1) are assigned to features A1–A10 by the app based on the answers given by the participant. For example, if the screening method is for adult, that is, AQ-10-Adult, 1 is assigned to A1, A7, A8 and A10 when the answer is either Definitely or Slightly Agree, otherwise 0 is assigned. For A2–A6, 1 is given for Definitely or Slightly Disagree, otherwise 0 is assigned to these features. More details on the scoring of features for adolescent and child can be obtained from Allison et al. 20 Any final score of more than 6 indicates autistic and therefore the dependant variable (target class) will be assigned ‘Yes’ (see last column in Table 3). However, when the score is 6 or smaller, then the target class will be assigned ‘No’. These assignments are done automatically by the ASDTests app.
Sample 20 data instances collected for children using ASDTests app based on AQ-10 child screening method.
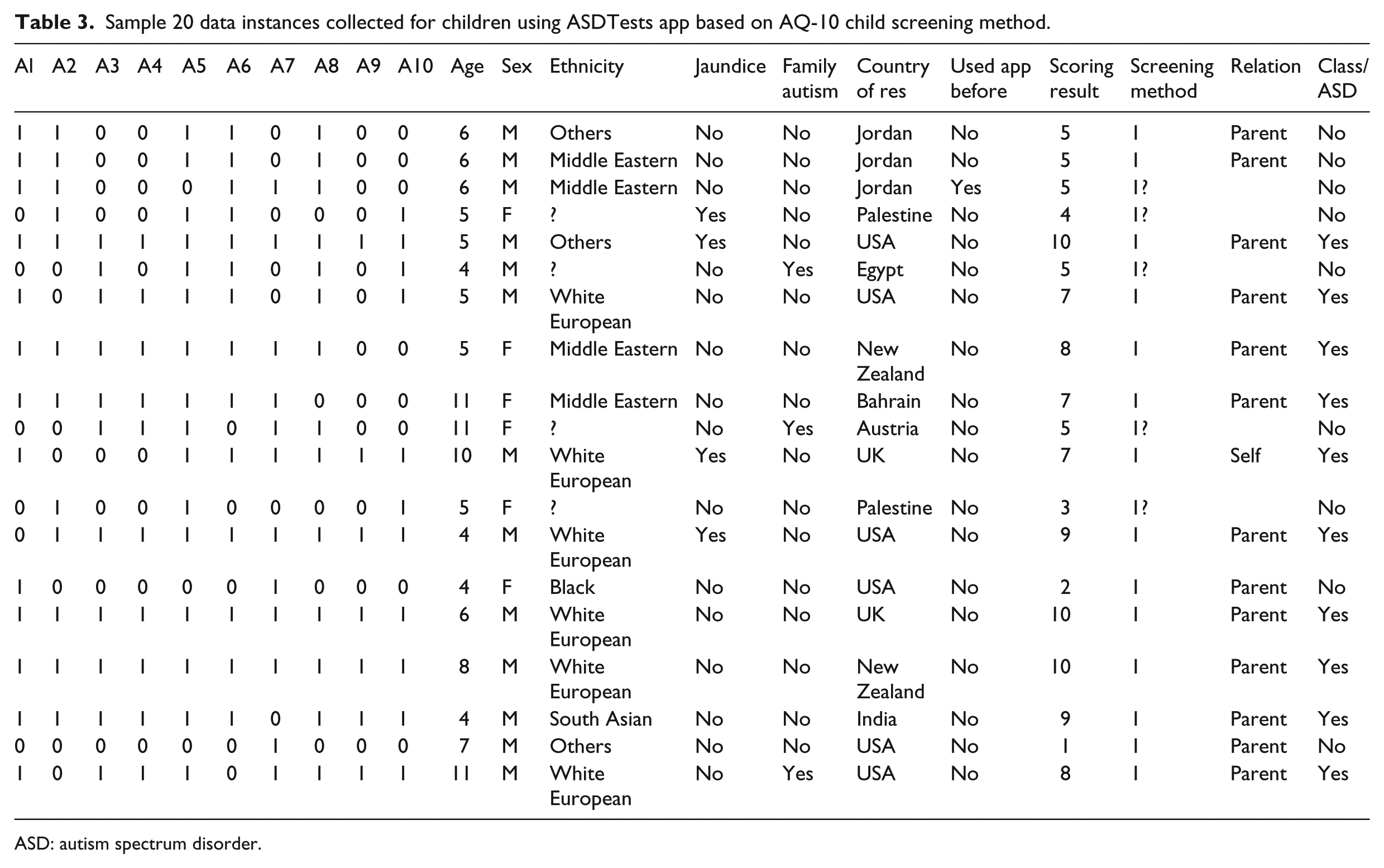
ASD: autism spectrum disorder.
A total of 1452 instances that belong to toddlers, children, adolescents and adults were collected over a period of 4 months using the ASDTests app and based on Q-CHAT-10, AQ-10 Child, AQ-10 Adolescent and the AQ-10 Adult screening methods, respectively. After an initial investigation on the collected instances, it was clear that the vast majority of the instances that belong to toddlers and infants have been associated with a ‘no ASD’ class label, making such a group of data completely imbalanced. To be exact, 96 per cent of the cases who took the test for the Q-CHAT-10 (toddlers) have not been associated with ASD, and therefore, the toddlers’ instances are separated from other instances linked with children, adolescents and adults. This left 1100 instances that belonged to three target audiences (children, adolescents and adults). Figure 4(a) shows the instances of distribution with respect to age, and Figure 4(b) shows the class distribution per age category. It is clear from Figure 4(a) and (b) that there are more adult instances than adolescent and children, as well as more instances associated with the ‘No ASD’ class label. A basic explanation for more none ASD cases is that the population normally contains a much higher quantity of individuals with no ASD traits than those with ASD markers. Moreover, Figure 2(b) reveals that child instances are somewhat balanced with respect to class labels when compared with adult and adolescent instances.
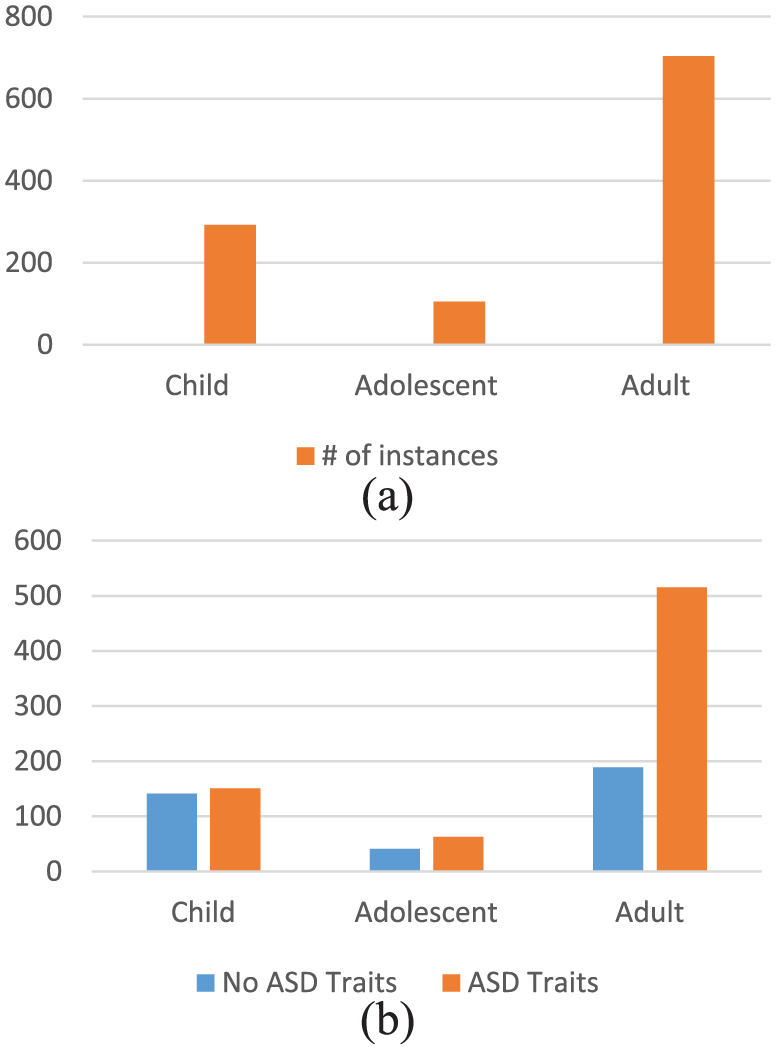
(a) The distribution of instances per age group (screening method target audience) and (b) the distribution of age instances per class label.
The average age in years for children, adolescents and adults in the three subsets based on the screening methods used are 6.3, 14.1, and 29.7 years, respectively. More male instances have occurred than female, as the number of instances for male and female in the three subsets (1100 total instances) are 625 and 475, respectively. The top ethnicities which participated in the data collection were Caucasian-European, Asian, Middle Eastern, South Asian and African/African-American with 381, 185, 128 and 65 respectively. In the three subsets of data, there were 707 and 393 instances linked with the ‘ASD trait’ and ‘No ASD trait’ class labels. More of the tests for adults have expectedly been taken by the individuals themselves, while many tests for the child category have been taken by parents, teachers or caregivers. Among the gathered instances, there were 194 cases with family members diagnosed with ASD and 165 cases of individuals born with jaundice. Finally, some values were missing in variables such as ethnicity and who is taken the test.
A feature analysis was conducted on the adults, adolescents and children datasets using wrapping filtering along with Naïve Bayes probabilistic classifier. 41 In the wrapping method, all combinations of feature(s) class will be tested with Naïve Bayes to select the set of features that maximises the predictive accuracy on the ASD classification problem. The aim of this analysis is to determine what influential features exist among the features collected and hence reducing the screening process of ASD. The classifiers obtained against the adult dataset using the wrapping method show that there are 12 influential variables from the set of all variables in the adult dataset (items 1 to 10 in the AQ-10-Adult questionnaire plus gender and ‘used the app before’). For the adolescent dataset, the wrapping method selected only 8 variables out of 21 (gender, born with jaundice, used the app before and items 2, 5, 9 and 10 in the AQ-10-Adolescent questionnaire).
Continuing, the results obtained by the wrapping method against the children dataset revealed that there are 4 effective variables selected from the 21 variables in the children dataset (items 1, 4, 8 and 10 from the AQ-10-Child screening questionnaire). The results obtained from the wrapping method that embeds a Naïve Bayes classifier demonstrate the influential features in each screening method based on the instances collected by the ASDTests app. These results clearly pinpoint that at least the self-administered screening methods of autism can be reduced in terms of the number of items/features required in a questionnaire, hence improving accessibility and efficiency. Furthermore, patients, clinicians, parents and other healthcare users can understand the concise set of autistic traits that designate ASD at least from behaviour science perspective, which helps improve the understanding of the screening process.
Table 4 shows the predictive analysis results derived by two machine learning algorithms (Naïve Bayes and Logistic Regression). The classification systems’ performance derived from the adolescent, adult and child datasets by Naïve Bayes and Logistic Regression algorithms with respect to predictive accuracy, sensitivity and specificity rates are shown in Table 3. Accuracy is a common metric in classification that computes the number of test data that were correctly classified from the total number of test data. Whereas sensitivity denotes the percentage of the test cases that are truly positive (with ASD class) and specificity represents the percentage of the test cases that are truly negative (cases with no ASD).
Accuracy, sensitivity and specificity rates of classifiers generated by Naïve Bayes and simple logistic regression.
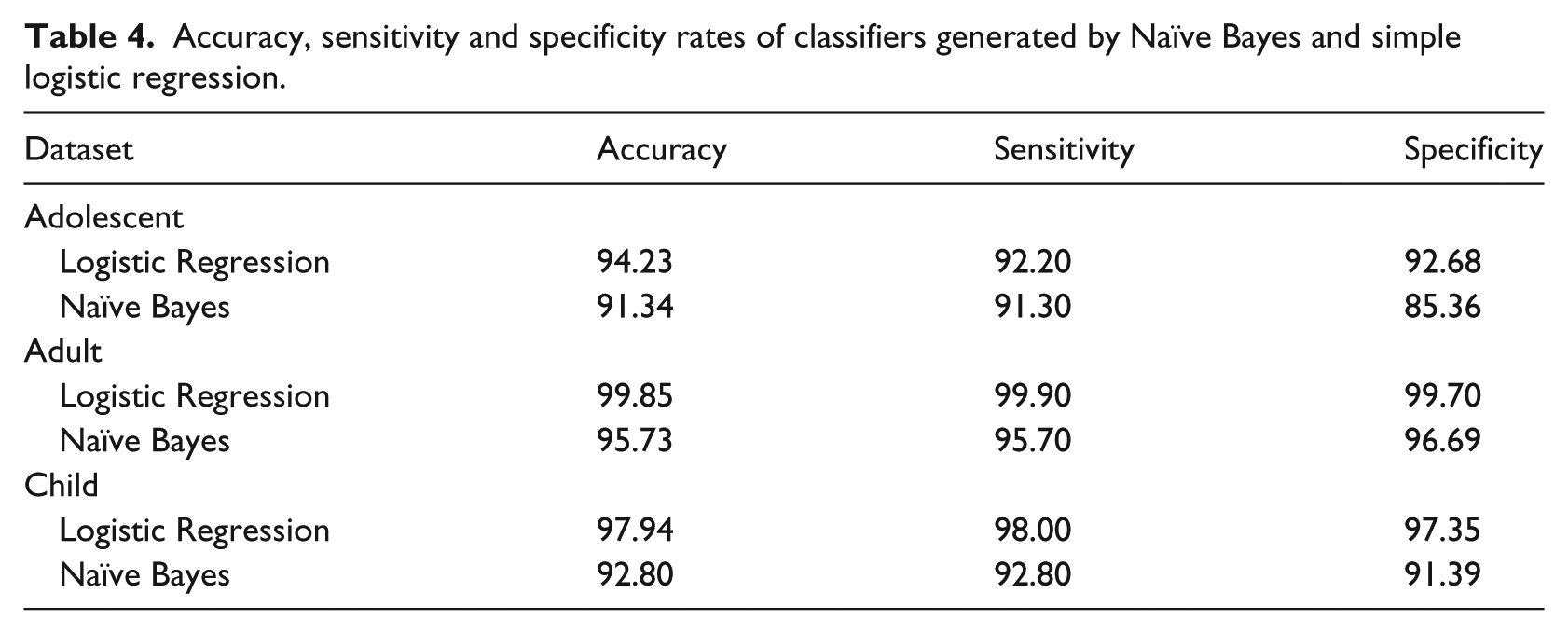
The results clearly show that the features collected by the ASD app are influential in detecting the dependant variable (class label). The results also pinpoint that machine learning algorithms are promising tools that indeed may enhance the performance of ASD screening and possibly diagnosis as well. 42 This can be attributed to the learning mechanisms employed by these intelligent algorithms in discovering hidden useful patterns for decision making and prediction. Logistic Regression showed superiority in detecting autistic traits over probabilistic classifiers derived by Naïve Bayes. Nevertheless, both algorithms revealed good rates of sensitivity, specificity and accuracy in screening autism. Higher rates have been derived on the adult dataset due to the fact that it has more instances than the child and adolescent datasets. Finally, machine learning reveals how the correlations among autistic traits can help clinicians, parents and caregivers improve the performance of ASD screening and possibly in the near future can replace the handcrafted rules and the scoring functions currently in use within classic screening tools such as AQ.
Conclusion
Since diagnostic services are normally busy, a general practitioner spends only a short time reviewing a patient. Therefore, a self-, caregiver- or parent-administered ASD screening method is advantageous, especially if accessible via easy mobile platforms or tablets. Most of the existing self-administered autism screening tools contain a large number of questions and are unavailable via mobile platforms, thus making them time-consuming and inaccessible by many health community users. And the ones that are available focus only on specific user groups (in particular, toddlers, children or adults) and come primarily in English. These therefore lack large coverage of existing ASD cases and are not accessible by most communities worldwide. This article has proposed a new mobile ASD screening tool called ASDTests to be offered in both Android and IOS versions containing four different modules and to come in 11 languages. Each module covers a specific age range (toddlers, children, adolescents and adults) and contains 10 questions linked to images, so the entire user population can utilise the proposed ASD screening app. The new app is vital for pre-diagnosing ASD since it increases user accessibility in an easy and time-efficient platform as well as being accessible to a wide range of users, including caregivers, parents, clinicians and health professionals among others.
Since ASD data are rare, the proposed app contains an important module for data collection of user features upon finishing a test and thus establishes a vital data repository related to autism that can be exploited for further analysis by behaviour and computational intelligence scientists. Features analysis using wrapping method that embeds Naïve Bayes classifier showed clusters of influential features for the adults, adolescents and children datasets that potentially can enhance the understanding of correlated autistic traits. A significant reduction of features was observed on the adolescents and children dataset based on the feature analysis conducted. This feature analysis was not possible without the ASDTest app’s data collection module. In addition, two machine learning algorithms (Naïve Bayes and Logistic Regression) have been used to show the significance of the features collected. Classifiers generated by the machine learning algorithms showed high sensitivity, specificity and accuracy rates. These results strongly indicate that we should replace existing scoring functions and handcrafted rules within screening tools with more intelligent machine learning models.
Fortunately, the rapid development in smart phone technology has provided new opportunities for us to create the ASDTests screening app. Cases, controls and their stakeholders as well as the healthcare community are now able to access this autism screening tool using smart phones and thus receive instant results along with a detailed report. This opens the door for ASD diagnosis cases to obtain faster medical referral and thus access to health, education and social support services. Quickened access may eventually help minimise further inappropriate developments in behaviour, communication and social interactions.
In the near future, it is intended to enhance screening of ASD by replacing the conventional diagnosis process of the handcrafted rules with automated machine learning technology.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.