
Abstract
Health informatics applications reduce time intervals in acute coronary syndromes, but their impact on guideline adherence is unknown. This pre–post intervention study compared guideline adherence between telemedically supported (n = 101, April 2014–July 2015) and conventional on-scene care (n = 120, January 2014–March 2014) in acute coronary syndrome. A multivariate logistic regression was performed for dependent variables: adverse events 0 versus 0, p = NA; electrocardiogram 101 versus 120, p = NA; acetylic salicylic acid 91 versus 102, p = 0.21; heparin 92 versus 112, p = 0.99; morphine 96 versus 107, p = 0.33; oxygen 83 versus 102, p = 0.92; glyceroltrinitrate 55 versus 90, p = 0.038; correct destination: 100 versus 119, p = 1.0. The time from ambulance arrival to hospital arrival was prolonged with telemedicine: 48.7 ± 11 min versus 35.5 ± 8.1 min, p < 0.001. Guideline adherence showed no differences except for glyceroltrinitrate. Prolonged time requirements are critical, though explainable. However, this approach enables a timely and high-quality backup strategy if only paramedics are on-scene.
Background
Patients with acute coronary syndrome (ACS), especially those with ST-segment elevation myocardial infarction (STEMI), are at high risk of arrhythmic complications during the first hours after symptom onset.1–3 Therefore, ambulance personnel must be skilled in recognizing and treating such complications. 4 The time from symptom onset to reperfusion predicts the amount of salvaged myocardial cells, infarction size and the probability of congestive heart failure and long-term mortality.5,6 It is well known that telemedical approaches that transmit the 12-lead-ECG (electrocardiogram) from the prehospital setting to a cardiologist shorten the time interval to reperfusion.7,8 In a follow-up study by Sanchez-Ross et al., 9 the patient outcome was even improved if 12-lead-ECG transmission was performed. Current guidelines by the European Resuscitation Council and the European Society of Cardiology postulate early 12-lead-ECG interpretation and specific medications.4,10,11
Although it is not exactly known which medications can improve patient outcome if administered early in the prehospital phase, current guidelines recommend certain medications within the early phase after first medical contact.4,10,11 Modern emergency medical services (EMS) must ensure these strong recommendations and have to deliver guideline-adherent medications most early. In some European countries, a two-tiered EMS system is run with both physician and non-physician staffed ambulances. 12 In Germany, like in many other countries, paramedics have restricted competences in delivering intravenous medications. While the positive effects of telemetric pre-information of the hospital are already known, it is not known if telemedical support to ambulance personnel has an impact on guideline adherence in ACS. Furthermore, a telemedical concept might lead to earlier initiation of medical therapy in the prehospital phase because legal restrictions can be obviated by physician-based telemedical delegation.
Two prior research projects have evaluated telemedical support to EMS physicians and paramedics. Guideline adherence in ST-segment myocardial infarction was improved using real-time telemedical support in simulated scenarios. 13 Furthermore, telemedically supported paramedics produced quality of care that was at least as good as on-scene EMS physicians in simulated scenarios without the necessity for highly invasive procedures. 14 These results led to clinical evaluation of the concept in clinical studies. Feasibility, general safety, improved data transfer in acute stroke and analgesic quality above the required minimum standard were shown.15–18
The telemedical concept was also shown in ACS with a small sample size in a previous research project. 19 Due to these findings and the possibility of earlier initiation of intravenous prehospital therapy, a comprehensive telemedicine system for EMS was financed by German health insurance in a pilot region (Aachen, Germany) and implemented stepwise. Safety, guideline adherence and prehospital time requirements in ACS were compared between telemedically supported paramedics and a historical control group of conventional on-scene care delivered by EMS physicians.
Methods
Organizational setting
In the city of Aachen (253.945 residents, December 2015), the EMS is run by the fire department and three EMS agencies. Nine regular paramedic-staffed ambulances are run each day, and two additional ambulances can be staffed by firemen if necessary. To carry out advanced life support, two EMS physician units are run on a 24/7 basis. Starting in April 2014, a prehospital comprehensive telemedicine system was implemented into routine care in this EMS district. This lasted until March 2015. During this time, 11 ambulances were connected stepwise to the telemedicine system.
The emergency dispatch centre dispatched an ambulance and an EMS physician unit in all cases of clearly suspected ACS for legal reasons. Therefore, telemedicine was only used when the primary dispatch was only an ambulance due to a different description of the medical situation by the caller and the paramedics on-scene detected an ACS. If STEMI or cardiogenic shock was diagnosed by the tele-EMS physician, then an EMS physician unit had to be summoned but only if the arrival of this unit was estimated faster than the presumed hospital arrival time.
Also in the control group, the algorithm (standard operating procedure) was provided to the EMS physicians and paramedic in a paper-based booklet. This booklet was also provided to the EMS personnel from the start of teleconsultation system with identical content as the telemedicine software.
Telemedicine system
All ambulances were equipped with an audio- and data transmission unit (peeqBox, P3 telehealthcare, Aachen, Germany) and an In-Car-Computer. Both units were connected via WiFi and enabled encrypted and parallelized data transmission via up to five cellular networks (2G und 3G mobile networks). The following applications were integrated into the comprehensive telemedicine system: real-time audio and vital data transmission (numerical values and curves), 12-lead-ECG and still picture transmission as well as video streaming from inside the ambulance. The technical performance has already been described and can be judged as high. 20 Specially trained EMS physicians staffed a teleconsultation centre that was run 12.75 h daily initially and on a 24/7 basis from July 2014 on. In the centre, a context-sensitive software was run that provided checklists and algorithms based on current guidelines (Telemedical Documentation, P3 Telehealthcare, Aachen, Germany). An algorithm and checklist for ACS was displayed based on the current guidelines (Figure 1).11,21,22
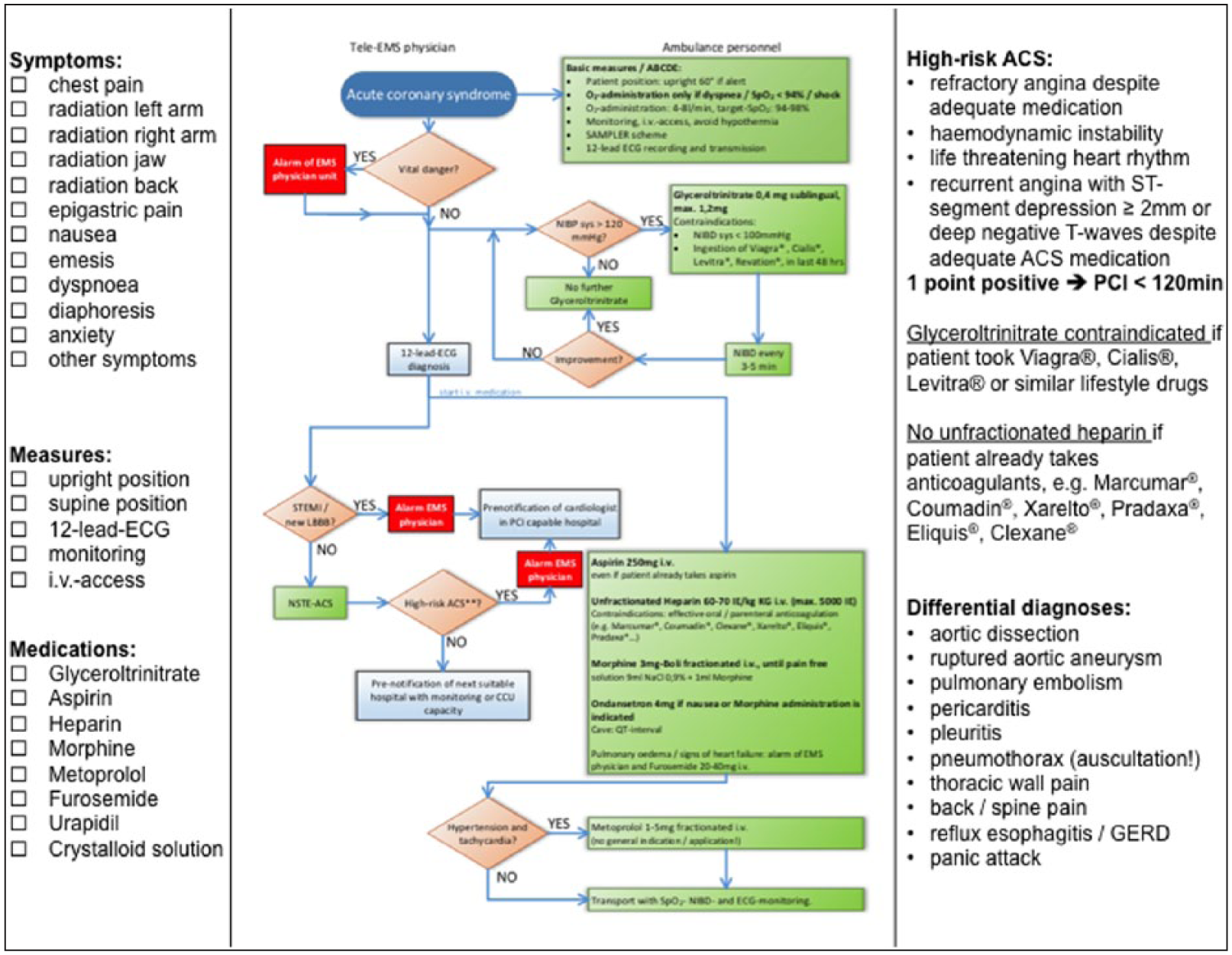
Schematic screenshot of ACS algorithm and checklist.
Qualification of physicians and EMS personnel
All EMS physicians in this EMS district had to have a minimum clinical experience of 3 years training in anaesthesia and critical care, had to be certified EMS physicians and had to run through an Advanced Life Support Course from the European Resuscitation Council (or equivalent) and a certified prehospital trauma course (Pre Hospital Trauma Life Support® or equivalent). Paramedics received a 2-year training and were allowed to perform intravenous (in general) as well as intraosseous access (in cardiac arrest); they could use supraglottic airways as well as defibrillation. With the exception of a small amount of lifesaving medications (crystalloids, epinephrine, glucose, inhalative bronchodilators, nasal midazolam and rectal diazepam), no other intravenous medications could be administered without advice from an EMS physician (delegation).
In the new function as a ‘tele-EMS physician’, only experienced EMS physicians (>500 emergency missions, >4 years of training in anaesthesia and critical care or board certification) who underwent a specific standardized 5-day training programme for telemedical support were employed.
Study design, data sources and outcome parameters
All data were collected prospectively for quality management purposes and analysed retrospectively. In the study group (telemedically supported paramedics), all printed teleconsultation protocols of one consecutive year between April 2014 and July 2015 were screened for the inclusion criteria. To compare this group with conventional on-scene EMS physician care, a historical control group was searched backwards from March 2014 to January 2014 in the paper-based EMS protocols. This way, only cases from a historical phase where no telemedical support was available were included. Inclusion criteria: Every patient with the diagnosis of non-ST-segment elevation ACS (non-STEMI-ACS) or STEMI/new left bundle branch block was included.
The following parameters were analysed between both groups: rate of adverse events (respiratory/circulatory insufficiency, allergic reaction, cardiac arrest), correct transport destination (PCI capable hospital in STEMI or high-risk non-STEMI-ACS11,21,22), guideline adherence in the prehospital phase (parameters displayed in Table 2) and time interval from first medical contact (paramedic/EMS physician) to hospital arrival.
Ethics and data privacy
The study was registered at clinicaltrials.gov (NCT03132935), and data collection was started after approval by the local ethics committee (University Hospital RWTH Aachen, EK 109/15). To ensure data privacy, all cases were pseudonymized for analysis. In the teleconsultation centre, personalized user profiles were used for strict data privacy. All data transmission occurred encrypted and was initiated only after verbal (alert patients) or presumed consent (impaired consciousness). All procedures were in accordance with national law.
Statistical methods
The categorical data are presented as frequencies and percentages. The frequencies of categorical baseline characteristics were compared between groups using a chi-square test with Yates correction or Fisher’s exact test where applicable. Continuous variables are expressed as the mean values ± standard deviation (SD). Differences in continuous baseline characteristics between groups were analysed via a two-sided t-test assuming unequal variances. Baseline variables with significant differences (p < 0.05) were selected as prognostic factors for multivariate logistic regression on the categorical outcome parameters (e.g. given medications). A firth bias correction was used to account for quasi complete separation (logistf).
For the univariate analysis of the categorical outcome variables, a chi-square test with Yates correction was used. All tests were conducted at the 5 per cent significance level. Because of the exploratory nature of the study, no adjustment to the significance level to account for multiple testing was made. Statistical analyses were performed using R (R Core Team (2016), R version 3.3.0).
Results
Initially, 137 patients received telemedically guided emergency care. In 21 of them, the patient was handed over to a conventional EMS physician shortly after initiation of teleconsultation because the EMS physician was already alarmed or STEMI was diagnosed initially and a conventional EMS physician was summoned. After exclusion, 101 patients were included (study group) to compare solely telemedical and solely conventional EMS physician-based emergency care (Figure 2). These cases were compared to 120 patients in the historical control period (Figure 2). Patient demographics and characteristics are summarized in Table 1. Patient age, the fraction of STEMI patients, initial pulseoxymetry values and pain scales differed significantly (Table 1). No adverse events occurred in the prehospital phase in either group: 0/101 versus 0/120, p = NA. The different procedures and medications according to the valid guidelines during the study phases are displayed in Table 2 in comparison between both groups.11,21–23 In the multivariate analysis, no significant differences were detected in guideline adherence of performing 12-lead-ECG, administration of aspirin, heparin, morphine, oxygen administration and transport destination (Table 2). Glyceroltrinitrate was significantly more often waived (although indicated) with the telemedical approach (Table 2). The out of hospital time intervals were significantly longer in the telemedicine group. For telemedicine group versus control group, ‘first medical contact to hospital arrival’: 48.7 ± 11 min versus 35.5 ± 8.1 min, p < 0.001, and on-scene time: 36.7 ± 11.3 min versus 25.4 ± 7.4 min, p < 0.001. The active time of the respective physician also differed with shorter net time requirement using the telemedical approach: 35.8 ± 13.6 min versus 53.5 ± 14.3 min, p < 0.001. Although technical evaluations were not outcomes of this study, there was no technical drop out that led to a termination of teleconsultation.
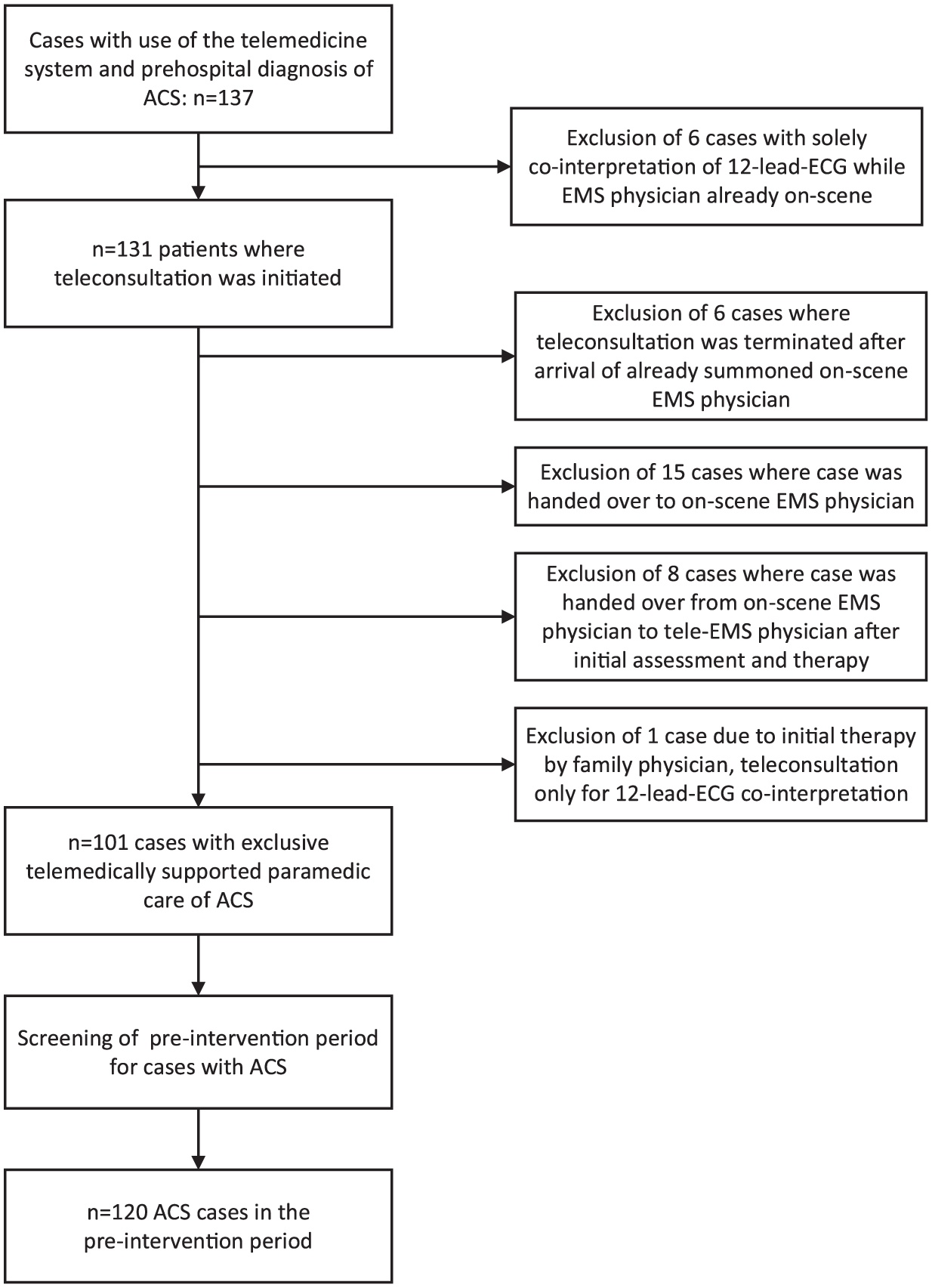
Study flowchart.
Patient demographics and characteristics.
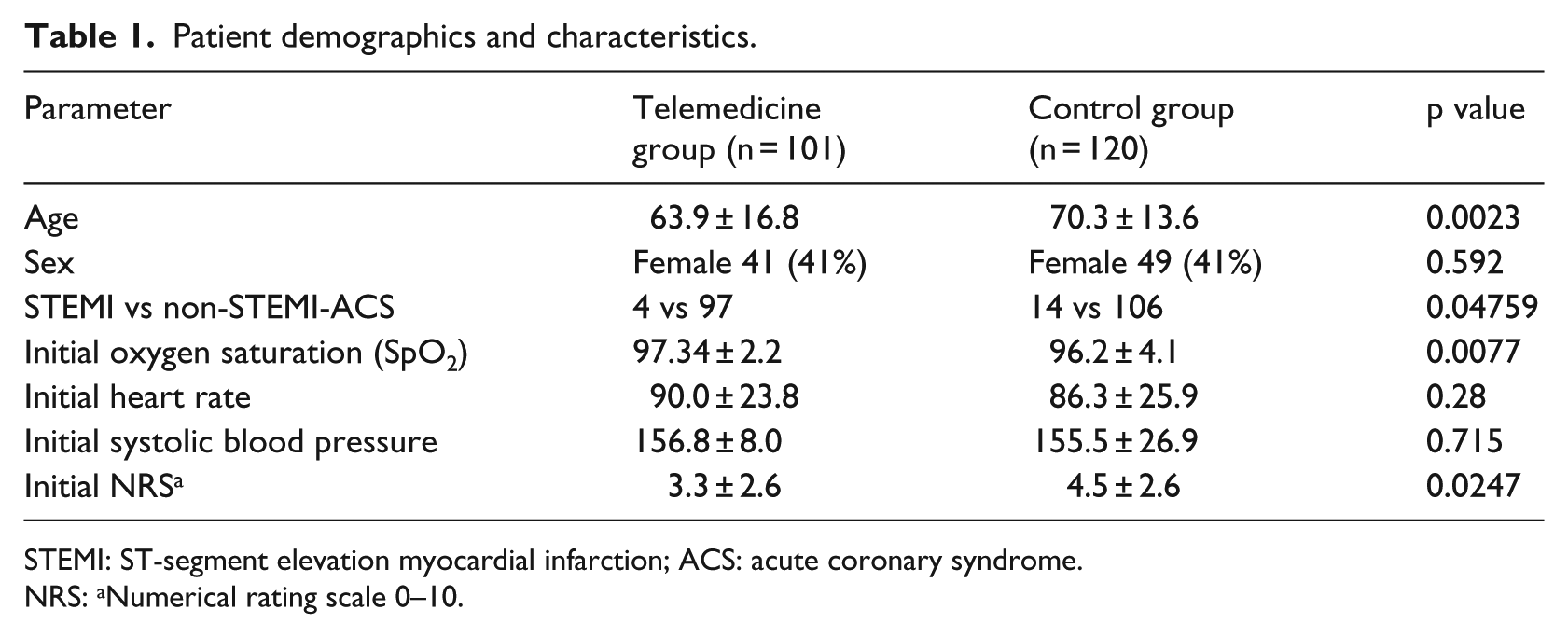
STEMI: ST-segment elevation myocardial infarction; ACS: acute coronary syndrome.
NRS: aNumerical rating scale 0–10.
Guideline adherence and quality outcomes.
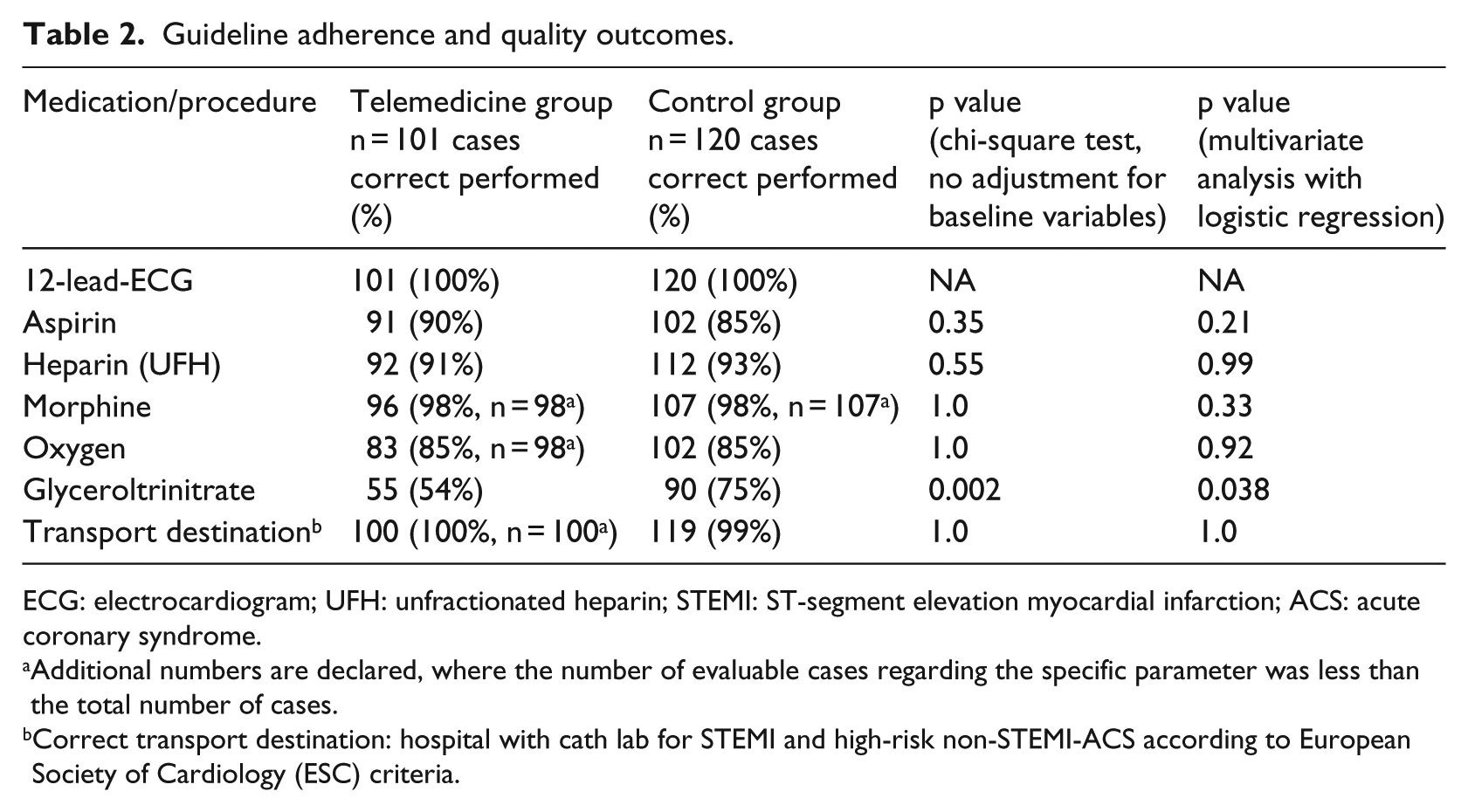
ECG: electrocardiogram; UFH: unfractionated heparin; STEMI: ST-segment elevation myocardial infarction; ACS: acute coronary syndrome.
Additional numbers are declared, where the number of evaluable cases regarding the specific parameter was less than the total number of cases.
Correct transport destination: hospital with cath lab for STEMI and high-risk non-STEMI-ACS according to European Society of Cardiology (ESC) criteria.
Discussion
Care guided by a telemedic physician led to no significant differences in guideline adherence except for the administration of glyceroltrinitrate, which was administered more correctly (if indicated) with conventional on-scene care. Both approaches were safe with no observed adverse events. In the telemedicine group, the time from first medical contact to hospital arrival was significantly longer with shorter net physician time requirements.
This is the first study to compare guideline adherence between telemedically supported prehospital care and conventional on-scene EMS physician care in routine care for ACS. The groups showed a comparable collective for the analysed measures because the recommended measures and medications are not age dependent, and the statistical model accounted for differences of baseline variables. Both groups demonstrated a high guideline adherence except for the management of glyceroltrinitrate.
Compared to other studies, both groups showed guideline-adherent administration of acetyl salicylic acid. In a recent evaluation of the US EMS system, only 45 per cent of patients received acetyl salicylic acid from the EMS. 24 Zeymer et al. 25 reported that only 33–45 per cent received antithrombotic agents in non-STEMI ACS and STEMI compared to 85–93 per cent in our study. Although both groups and especially the telemedicine group showed some weakness regarding the administration of glyceroltrinitrate, even this measure was above the administration rates reported by Francis et al. 26 All other measures and medications had a guideline adherence between 85 and 100 per cent, which is high relative to the published results of the other authors.24–26
One possible reason for the restrained use of glyceroltrinitrate may be that this medication should only be administered after ruling out right ventricular infarction, which requires a 12-lead-ECG interpretation. In the first phase of teleconsultation (prior to 12-lead-ECG registration, transmission and interpretation), acetyl salicylic acid, heparin and morphine can be delegated solely on the reported situation and the medical history. In some cases, the administration of glyceroltrinitrate can be forgotten or intentionally waived after symptom relief by morphine administration without an explanatory documentation. Unfortunately, we could not differentiate the omission of glyceroltrinitrate, and therefore the omission was considered ‘incorrect’ if no contraindications were documented. Nevertheless, current guidelines recommend glyceroltrinitrate after ruling out right ventricular infarction but only for ongoing chest pain. There is the possibility that some of the cases were considered ‘incorrect’ regarding glyceroltrinitrate, and these were assessed incorrectly due to symptom relief after morphine. However, this weakness is seen in both groups. Altogether, future efforts are needed to improve guideline adherence regarding this measure – especially with the telemedical approach. However, no evidence for improved patient outcome exists after the use of glyceroltrinitrate in the prehospital phase.4,10,27 Metrics indicated of improved outcome were seen in 85–100 per cent of patients in both groups without significant differences.
However, only a few studies have researched prehospital guideline adherence in ACS. Most critically, the prehospital time interval was prolonged in the telemedicine group. It is critical to remember that we compared a group with two paramedics each (telemedicine group) to a four-member team (one EMS physician, three paramedics). Practical tasks like transferring the patient from the apartment to the ambulance are much more time-consuming with a two-member team. Also, the recommended medications had to be prepared and administered by only two persons. This study was done in an urban setting, and the increased prehospital time interval was probably due to the two-member teams on-scene. However, two-member EMS teams are current practice in many countries.
Additional studies are needed to evaluate if the additional time in the two-member teams affects patient outcomes. In rural areas where no conventional EMS physician is rapidly available, the telemedical approach enables a specific therapy beyond the competences and legal regulations for paramedics in many countries. The above average performance metrics are not solely explicable by the telemedical approach but also due to the high training level of physicians in both groups. In many German states, only 1.5 years of clinical experience and an 80-h course is needed for certification as an EMS physician. Both groups were clearly above this minimum standard. Although in-hospital time intervals could not be evaluated here due to data privacy regulations, every patient in the telemedicine group was pre-notified in the emergency room for low-risk non-STEMI-ACS. A pre-existing heart cath lab hotline including 12-lead ECG fax transmission to a cardiologist on demand was used for high-risk non-STEMI-ACS and STEMI to enable rapid percutaneous coronary intervention. Pre-notification including 12-lead-ECG transmission is well known to improve in-hospital time intervals and outcome.7–9 Telemedical STEMI networks are also established in some regions to enable a quick link between the prehospital and inpatient care.28,29 However, none of these studies offer real-time telemedical support by a remote physician for the ambulance team. If telemedical support and networks should prove their benefit in the future, barriers to widespread implementation have to be taken into consideration. Organizational models of telemedicine centres seem to be important to ensure implementation into routine care. 30
Limitations
Our study has some limitations. Although all parameters were collected prospectively for quality management purposes, analyses were performed retrospectively. In-hospital intervals were not addressed, because pseudonymization would not be possible at early stage. While the telemedical software had exact timestamps for every medication and measure, the control group only offered only cumulative documentation of the prehospital phase via paper-based protocols. Therefore, we could not determine if certain measures were performed earlier in one of the groups, although studying the time point of the 12-lead-ECG interpretation would have been especially interesting due to the recommendation of interpretation in <10 min after first medical contact.11,21 However, in case of a temporary shortage of highly qualified EMS personnel trained in 12-lead-ECG interpretation, especially in rural areas, telemedicine facilitates this interpretation within the recommended time frame. Overall, it has to be considered that this study was not powered as non-inferiority trial due to lack of pre-existing data regarding this comparison in routine care. A non-inferiority trial should be conducted to confirm the findings.
Conclusion
Telemedically supported paramedic care for ACS in an urban setting led to an above average guideline adherence as in the control group with on-scene EMS physicians except for the administration of glyceroltrinitrate. Both concepts were shown to be safe but in a context of small case numbers. The prehospital time interval was prolonged in the telemedicine group and was judged as critical. However, this telemedicine concept allows for earlier prehospital advanced therapy under supervision of an experienced physician if no physician is on the scene. The concept might provide early and resource-efficient emergency care – especially in underserved areas where four-member teams including a highly qualified EMS physician are not rapidly available or at night when helicopter physician teams are mostly unavailable.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.B., S.K.B., D.U. and M.M. declare no conflict of interest. R.R. and J.C.B. are shareholders of the docs-in-cloud company that provides consulting about telemedicine concepts.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.