
Abstract
The purpose of this article is to identify and assess service delivery issues within a hospital emergency department and propose an improved model to address them. Possible solutions and options to these issues are explored to determine the one that best fits the context. In this article, we have analysed the emergency department’s organizational models through i* strategic dependency and rational modelling technique before proposing updated models that could potentially drive business process efficiencies. The results produced by the models, framework and improved patient journey in the emergency department were evaluated against the statistical data revealed from a reputed government organization related to health, to ensure that the key elements of the issues such as wait time, stay time/throughput, workload and human resource are resolved. The result of the evaluation was taken as a basis to determine the success of the project. Based on these results, the article recommends implementing the concept on actual scenario, where a positive result is achievable.
Keywords
Introduction
Background
The emergency department (ED) has a busy and chaotic environment, where people’s lives are at risk. The flow of patients is high, with each patient having their own needs to be met. Maintenance and organization of the flow of patients along with service delivered to them are essential. 1 Service delivery in such an environment is very complex for medical staff, operational staff and executive management team. The motivation to deliver service comes from within the structural framework of the department, the management team, the business process and departmental framework. 2 Improvement of business process brings in the bucket of benefits to organization if conducted with an appropriate approach. The current business process for this project of ED has been adapted from the ideal ED patient journey presented by New South Wales (NSW) Health Ministry. 3 Furthermore, this article will be based on i* Organizational Modelling, which is an actor-oriented technique and provides relationship among actors in terms of goals, resources, tasks and sub-goals. The i* Organizational Modelling offers detail of organizational context and business process based on actor dependency. 4 The i* Organizational Model helps to model business both in as-is and to-be situations, where ‘as-is’ model represents how the business is at present, whereas ‘to-be’ model represents how the model will be in future.
Issues
Providing fast, effective and quality medical services is of top priority for any ED. At present, the time-management and bottom-line pressure has increased in all types of hospitals, as such it is obvious that speed and efficiency are of utmost importance than ever in ED. 5 A study on the inefficiency of ED in Queens Hospital states that 83 per cent of the patients are only seen on time and the waiting time for them is too long. 6
As per the Australian Hospital Statistics 2013–2014, the average wait time in NSW hospital is 15 min when 50 per cent of patients have commenced clinical (median wait time) care while 78 min when 90 per cent of patients have commenced clinical care (90th percentile wait time). The highest median wait time in Australian states was for Northern Territory at 34 min while Australian Capital Territory (ACT) has highest 90th percentile wait time at 152 min. Australian Health has stated that any median wait time more than 16 min is stated as longer than required while anything more than 40 min for 90th percentile wait time is long enough. 7
The average wait time for a patient to commence clinical care after entering ED for hospitals in NSW is 15 to 78 min; 15 min is average wait time when 50 per cent people commenced clinical care while 78 min is average wait time when 90 per cent people commenced clinical care.
The study also states that 50 per cent of efficiency is dependent on system issue and rest upon the staff and doctors on duty. 5 From the findings of the study, Wirth proved that the efficiency of the ED is mostly impaired by long wait time as well as workload on physicians and staff, as workload on staff lowers the quality of service to patient while long wait time itself is a measure of evaluating service delivery. It is identified that the key issues related to ED service delivery are in business process, workload staff, long wait time and stay time, as well as the unsatisfied patient over service provided.
Significance
Improvement of business process, allocation of more staff and application of advanced framework to business prospective are some of the solutions to address the issue of ED. This study will propose a new improved business process and service delivery framework (SDF) in response to issues identified. The development of improved business process and SDF is supported by i* Organizational Modelling of the current and proposed business modelling. Moreover, the key elements of the issue like inefficiency, wait time, stay time and workload need to be evaluated to make sure that they are eliminated. This project will address all these key elements while working towards improvement of business process using i* Organizational Modelling. Furthermore, this study will highlight the significance of i* Organizational Modelling used in service delivery innovation of an ED.
Aims
This project works on upgrading/restructuring the business process of an ED to provide a better and efficient service delivery to the patient. The aims of the project include the following:
To identify and assess service delivery issues within the hospital ED using i* Organizational Models;
To address the key issues such as workload, wait time, efficiency and the effect of workload causing service delivery issue in ED;
To reduce the wait time and stay time to a significant number;
To propose an innovated SDF for ED with an improved organizational model supported by efficient business processes;
To improve the current patient journey diagram.
The expected outcome of this project is the improved patient journey diagram and new SDF.
Literature review on service delivery innovation of ED
Service delivery and issues in EDs
Service delivery is a critical aspect of every department of hospital. In an ED, the service delivery plays a vital role on treatment of life-threatening diseases. Development of service delivery system enhances quality of service and benefits service providers. 8 The service delivery innovation is described as aligning the business strategy/process, the service concept and the design of service delivery system. 9 In other words, in our case, it is simply putting together all business rules, practices, workflow and process of hospital into a concept of providing service to patients and designing a SDF or procedure. The overcrowding and its associated problems in an ED has been highlighted since late 1980s. 10 It has potential consequences that compromise access to care and quality of service provided. The EDs with poor service are described as high-risk areas with medical errors and pose a threat to patient safety. 11 The speed and efficiency of service in ED are slowed down by bottom-line pressure and time management. The main hindrance to service delivery in ED includes long wait time in waiting room, long overall stay time in ED, workload on staff and lack of efficiency in business process. 6
Business process modelling and ED
Business process modelling (BPM) is a structural representation or deception of a diagram which specifies the flow of activity in a specific organization/business part. 12 BPM is used to map the flow of work in an organization, so that analysis, understanding and improvements in the process can be made. 13 Business modelling is a concept which deals with structuring a business from different aspects of processes. The business model must provide an integrated view of all relevant information, functions, organizations and workflow. 14 The BPM has different techniques, out of which Business Process Modelling Notation (BPMN), Unified Modeling Language (UML) diagrams, 15 Flow Charts, Data Flow Diagrams, Object-Oriented Methods, Workflow Diagrams and i* Organizational Modelling are common. These different techniques represent a system in terms of object, attributes, operations and relationship, which helps to model a system. 13 A journal by Rojo et al. 16 had used BPMN to model an Anatomic Pathology Process. Yarmohammadian et al. 17 published an article on ongoing improvement of the hospital process through business process management. In 2008, Bhattacharyya et al. 18 conducted a technical article for low- and middle-income countries, which highlighted the use of process improvement and medical process reforming in order to develop an innovative health service delivery. Service delivery improvement through the usage of organizational model has been proposed in literature in other domains, including judicial services. 19 In analysis and study of business process innovation for health industry, we found that ED is technically linked to BPM in terms of understanding a process and developing better system and improvement of service delivery, which at the end of the day applies to provide better clinical care. However, we argue there is a need to analyse organizational models, actors’ dependencies and rationale to drive efficient operational processes.
Existing solution to the issues with efficiency in service delivery of ED
To solve the problem of wait time and improve efficiency for the non-acute patient in ED, hospitals around Australia use Fast Track Service Delivery Model which allocates patients into alternate streams within ED where patients are given care rather than waiting. This benefits service delivery in ED when it is crowded and is under pressure to free up ED beds in order to reduce complaints about waiting time and patients’ frustration. 20 After the implementation of Fast Track in ED, the wait time, overall stay time, workload and efficiency of service have significantly dropped but remain high, which need to be controlled and improved. 7 The key elements to the ED service issues need to be addressed to produce a positive solution. Improvement of business process, allocation of staff and use of advanced ED framework on business process prospective are found to be some of the possible solutions from the study. The incorporation of Fast Track and ongoing treatment in the ED as a business process improvement is a key towards improving service delivery. However, research analysis and static data from Australian Institute of Health and Welfare (2014) suggest that there is still ground for improvement in terms of wait time and overall stay in ED. 7 From the study, analysis and research of different case, papers and solutions available on service delivery within health domain, the project suggests that upgrading of business process will be an effective solution.
Current business process of service delivery of ED
Service delivery reforming is a complicated task in any existing scenario. If a business process for a new service delivery system/model is developed, life will become much easier as the scope will gain flexibility/elasticity. However, in this project case, the flexibility is not obtained to develop a completely new SDF but modification of a preexisting business process model that is providing service to patients in ED. In this article, the consideration is on different factors, cases and actors, working together to provide an Emergency Service to patient.
From the preexisting model presented below, it will be possible to explore the different levels and then propose the model. Finally, a proposed framework will be presented on the basis of different levels and versions of i* Organizational Models developed while reforming the business process and structure for service delivery in ED.
Existing service delivery process in ED
Understanding of existing service system of ED is essential in order to start developing any idea or concept. The basic idea of current business process and steps is adopted from the report of NSW Health Ministry. 3 The project is being worked on and models are developed around the basic ideas gained from ‘The Ideal Emergency Department Patient Journey’ of NSW Health Ministry Report. Although this report is based on NSW hospitals and Australian Health Standards, it also closely depicts the basic ED process followed all around the world.
Figure 1 identifies different roles, process and attributes of ED in a hospital. The present process/life cycle of ED is presented and shows how a patient who enters an ED will be accessed and provided with medicines. First, to start designing the framework, it is essential to understand the background. The understanding is needed on how things are conducted in ED, who is involved/responsible and what is the current model/approach followed in ED in hospitals. Figure 1 clearly describes all the phases, major tasks, departments and roles that are present in current EDs. The emphasis of the journey is to stream patients into the most appropriate Model of Care (MOC) for them as early as possible.
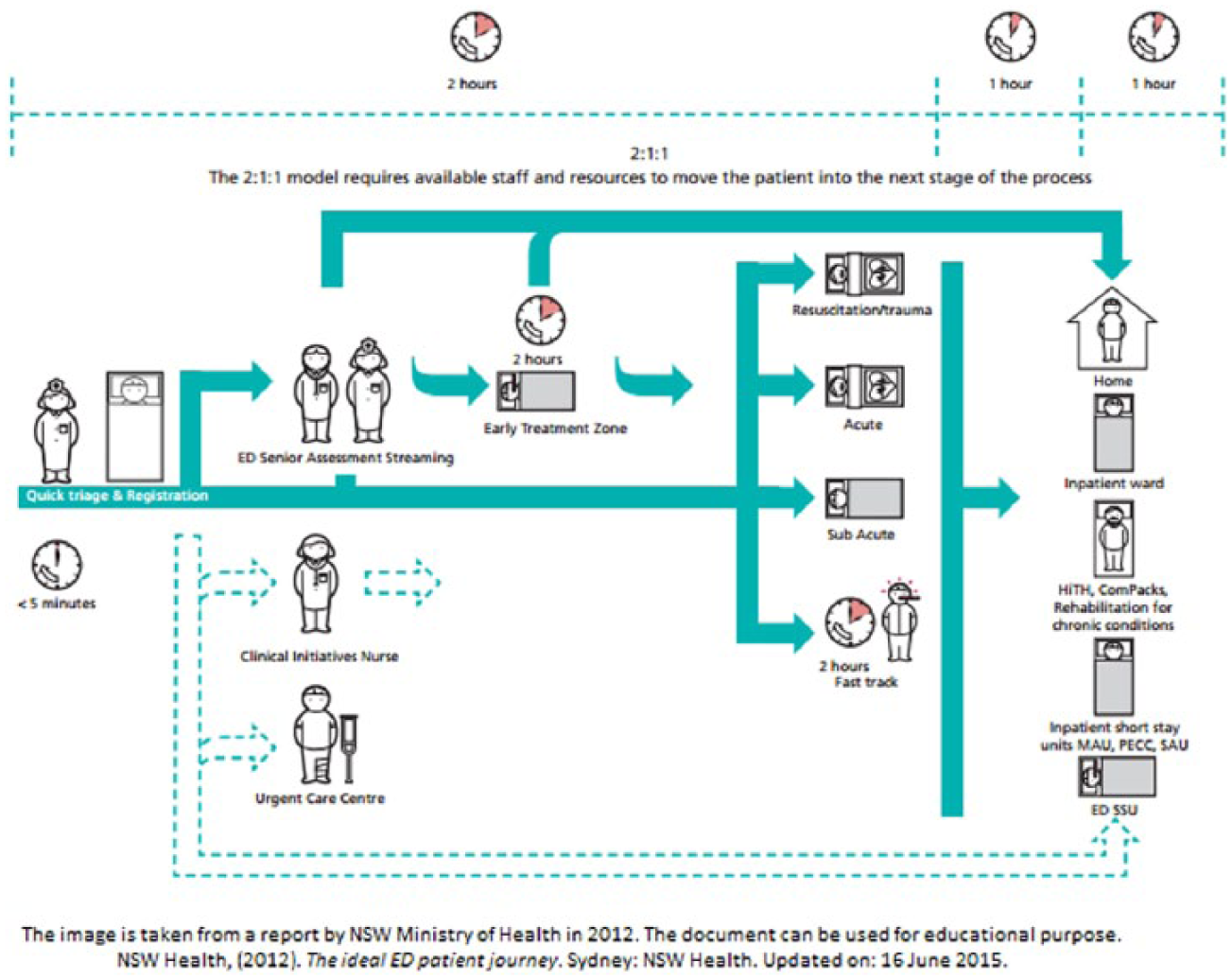
The ideal emergency department patient journey. 3
The dotted line on the top of Figure 1 with time indication represents the time frame and time flow. While the double dotted line ending with dotted arrows on the lower part of Figure 1 represents that parallel to the waiting time for patients (after triage), the patients are also accessed by Clinical Initiative Nurse as well as provided Urgent Care (such as bandage, cleaning cuts and wounds, supportive first aid), which can lead to other department access or even home.
Key areas of ideal ED patient journey in hospitals
Beginning the journey
Triage and registration
Resuscitation and trauma
Acute care of complex, non-ambulatory, high acuity patients
Early senior assessment and streaming of patients to appropriate MOC
Care for lower acuity, complex, non-ambulatory patients (Early Treatment Zone)
Care for non-complex, ambulatory patients (Fast Track and the currently being piloted ‘Urgent Care Centres’)
Non-ED patients (see Short Stay Units, Medical and Surgical Assessment Units).
Australasian Triage Scale
Table 1 shows Australasian Triage Scale (ATS) by Australian Institute of Health and Welfare.
ATS by Australian Institute of Health and Welfare. 7
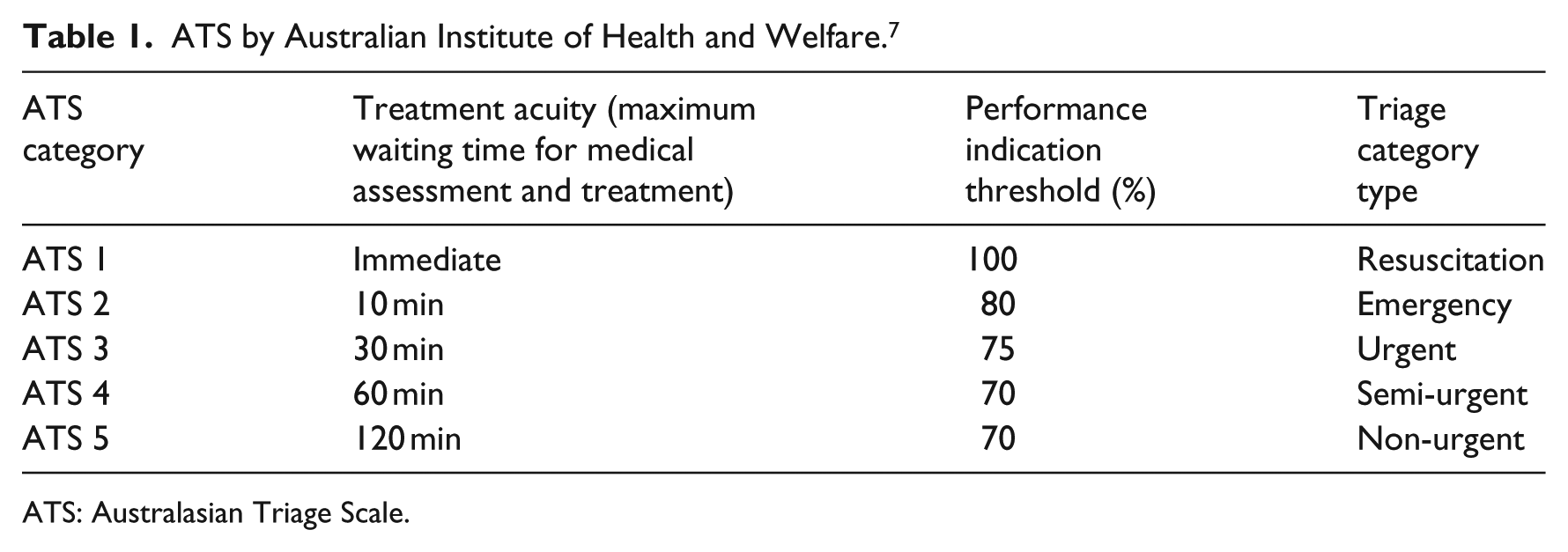
ATS: Australasian Triage Scale.
Current ED process of hospitals
First, a quick registration is done followed by prompt triage by a triage nurse (registered nurse).
The registered nurse will use ATS to categorize patients from triage categories 1 to 5 as per Table 1, where Category 1 is extremely urgent while Category 5 is non-urgent case.
The patients will be sent to the waiting zone in ED, where they will wait their turn for medical treatment.
If the triage process accesses the case to be serious, then it will be forwarded to ED senior assessment streaming where senior doctors and nurses will access their case and refer it to critical care area like resuscitation, acute care, sub-acute, or fast-track care.
There is an Early Treatment Zone for urgent cases facilitated by senior doctors and nurses.
For non-urgent cases, during the waiting time, the patient will continuously be accessed by Clinical Initiative Nurse and facilitated with Urgent Care Centre. The Clinical Initiative Nurse streaming is also facilitated by the availability of junior doctors to support.
The patients will be provided with best possible treatment and fast treatment based on their case; however, this does not mean Fast Track is extra department, it incorporates within ED but gives medical care to patient requiring early treatment.
There are basically four major treatment areas in ED, which include resuscitation, acute, sub-acute and non-urgent.
Furthermore, after treatment from these four areas, the patients are sent home or forwarded to other departments; sent to inpatient short stay unit, rehabilitation for chronic condition, or radiology or physiotherapy sessions; to critical care unit; or to pharmacist – all depending on treatment accessed. 3
Any time between ordering, implementation, result evaluation, consultation, communication and deposition are all included in the overall time indicated on the top of the ideal patient journey. This patient journey is a general overview; the exact scenario might change in accordance of requirement.
The i* Organizational Model for service delivery innovation of ED
The i* notation provides the capability to model organizational context and offer high-level social/anthropomorphic abstractions (such as goals, tasks, soft goals and dependencies) as modelling constructs. It has been argued that such notations help answer questions such as what goals exist, how key actors depend on each other and what alternatives must be considered.
The central concept in i* is that of intentional actor. Intentional properties of an agent such as goals, beliefs, abilities and commitments are used in modelling organizations. The actors represent roles such as doctors, nurses, support staff, management staff, patients and so on. The actor or agent construct is used to identify the intentional characteristics represented as dependencies involving goals to be achieved, tasks to be performed, resources to be furnished, or soft goals (optimization objectives or preferences) to be satisfied. The i* framework also supports the modelling of rationale by representing key internal intentional characteristics of actors/agents. The i* framework consists of two modelling components: strategic dependency (SD) model and strategic rational (SR) model.
Xavier Franch argues that the i* framework, its methods and the models used, discusses actor relationships and dependency, which is an essential aspect with relation to issues identified for service delivery in ED. 4 This article is a major backbone to use i* Organizational Modelling in this project for the purpose of process modelling. An article by a group of authors on strength and weaknesses of i* framework described the empirical evaluation of framework of modelling for requirement gathering. 21 Another article on goal-oriented modelling language by Quartel et al. 22 discussed more on i* modelling technique and its implementation in process development of service delivery.
This project of redefining business process to develop an SDF for ED will first constitute current SD model and SR model created by using i* Organizational Modelling. Next, through consultation, research and analysis, a proposed i* Organizational Model is developed. Finally, on the basis of these i* Organizational Models, a final framework for ED will be produced along with restructuring the ideal ED patient journey.
The i* Organizational Model
Organizational model is a structure that defines an organization through its framework, businessprocess, a line of staff and authority, exchange of task/communication and allocation of resources. 23 The i* Organizational Modelling is an agent-oriented requirement engineering framework, which helps to structure business process. 21 The i* Modelling Framework views organizational model as a network of actors that freely depend on other actors in terms of achieving goals and sub-goals, performing task and obtaining resources. 24
The i* Organizational Model is made up of two modes as SD model and SR model. Both these models put together to bring out the concept of Organizational Modelling by the use of i* framework.
SD model
The SD model describes the dependent relationship with other actors (illustrated in Figure 2) of the organization in terms of tasks, resources, goals and sub-goals. The SD model forms a network of actors who are dependent on other actors with the use of nodes, links and dependency. A node is signified as an actor and a link between actors where they are dependent to each other on purpose of a goal. 24 In SD model, the actor depender is dependent upon dependee by the dependency called dependum (agreement). This dependum or dependency may include tasks, goal, sub-goals, or resources. 25 Figure 2 shows an example of SD model of ED admission and triage.
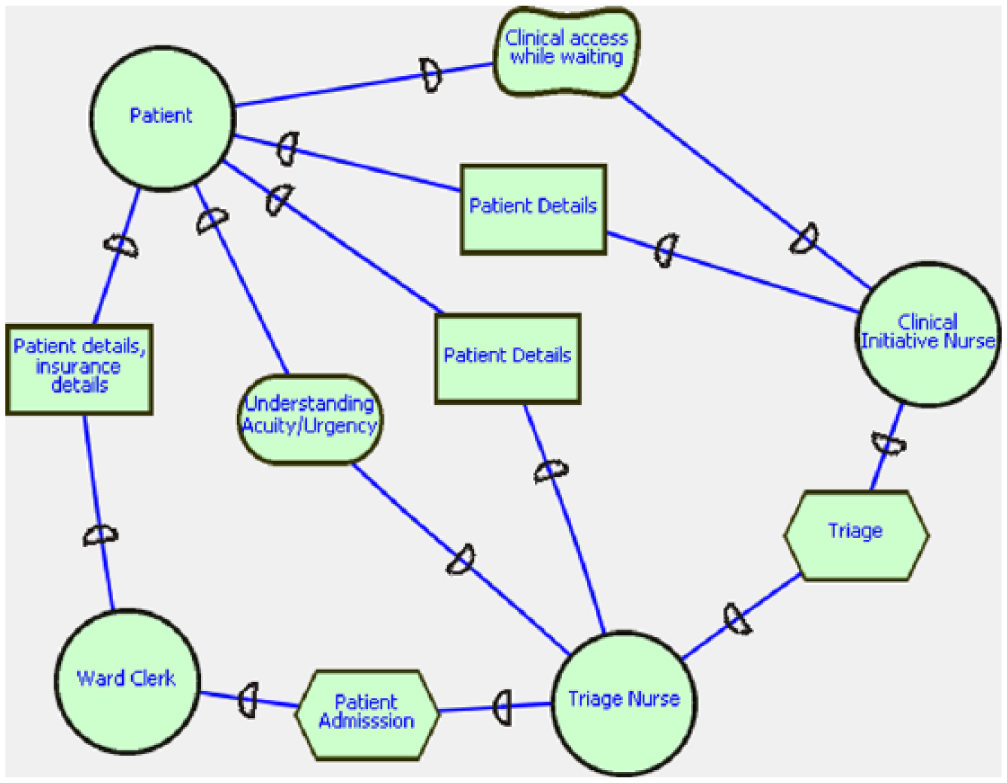
An example of strategic dependency (SD) model of admission and triage in emergency department.
SR model
The SR model is another i* modelling component that describes SD model in greater details by the means of task decomposition and means-end links. Means-end links is a modelling component of i* modelling notation. Using this notation gives the modeller a way to analyse the alternatives of satisfying a goal. The actor in this SR model has an actor boundary, inside which the task decomposition is conducted, and resources are allocated to achieve goals/sub-goals. 24 The SR model represents the structure and rationale behind the organizational process by linking task to goal by means-end links. The SR model clearly shows the task and goal for the dependency among actors. 25 Figure 3 represents an example of SR model of admission and triage in ED.
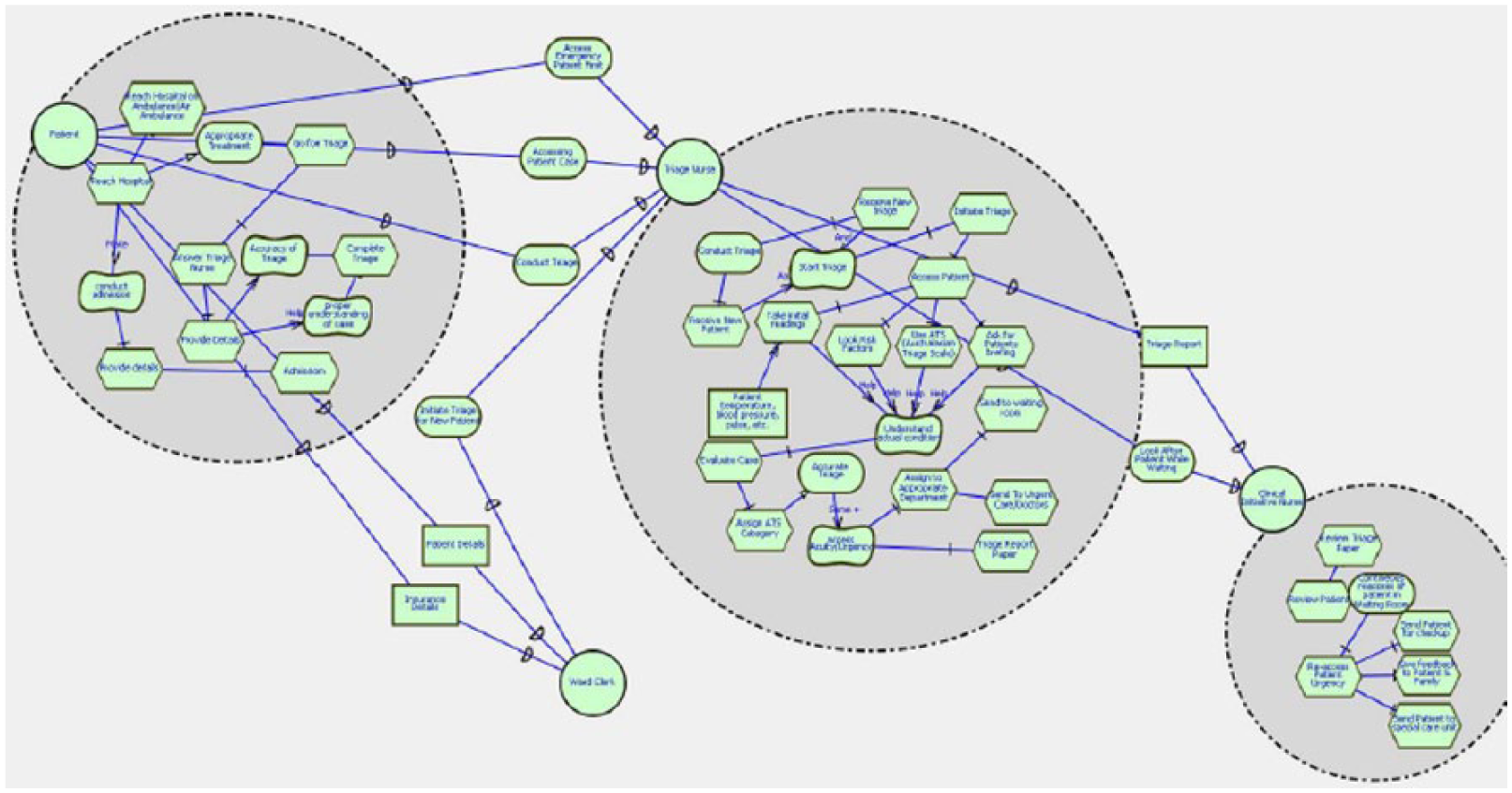
An example of strategic rational (SR) model of admission and triage in emergency department.
Conversion of current business process into i* Organizational Model of ED
The current i* Organizational Model is depicted from the ideal ED patient journey. The proposed models show the task and resource dependency among the actors. Figure 4 shows the SD model of current ED business process. Figure 4 describes how a patient entering an ED is processed and transferred among different departments and how different actors/personnel are involved in providing treatment. The depicted SD model as shown in Figure 4 lays out that after a patient enters ED, the first personnel to take over is ward clerk and triage nurse. The ward clerk is dependent on the patient to get personal and insurance details while triage nurse is dependent on the patient to understand the criticality or urgency of the situation. The triage nurse conducts triage and assigns an ATS category (Triage category) to the patient and sends them to the respective department/stage. The Clinical Initiative Nurse is dependent on triage nurse for triage report which occurs in waiting period. When a doctor takes over a patient, he is dependent on triage report, assistance from nurse and other doctors, senior advice and other factors for treating the sick individual. Figure 4 shows the set of node and links, where each node represents actors and links represent dependency among the actors.
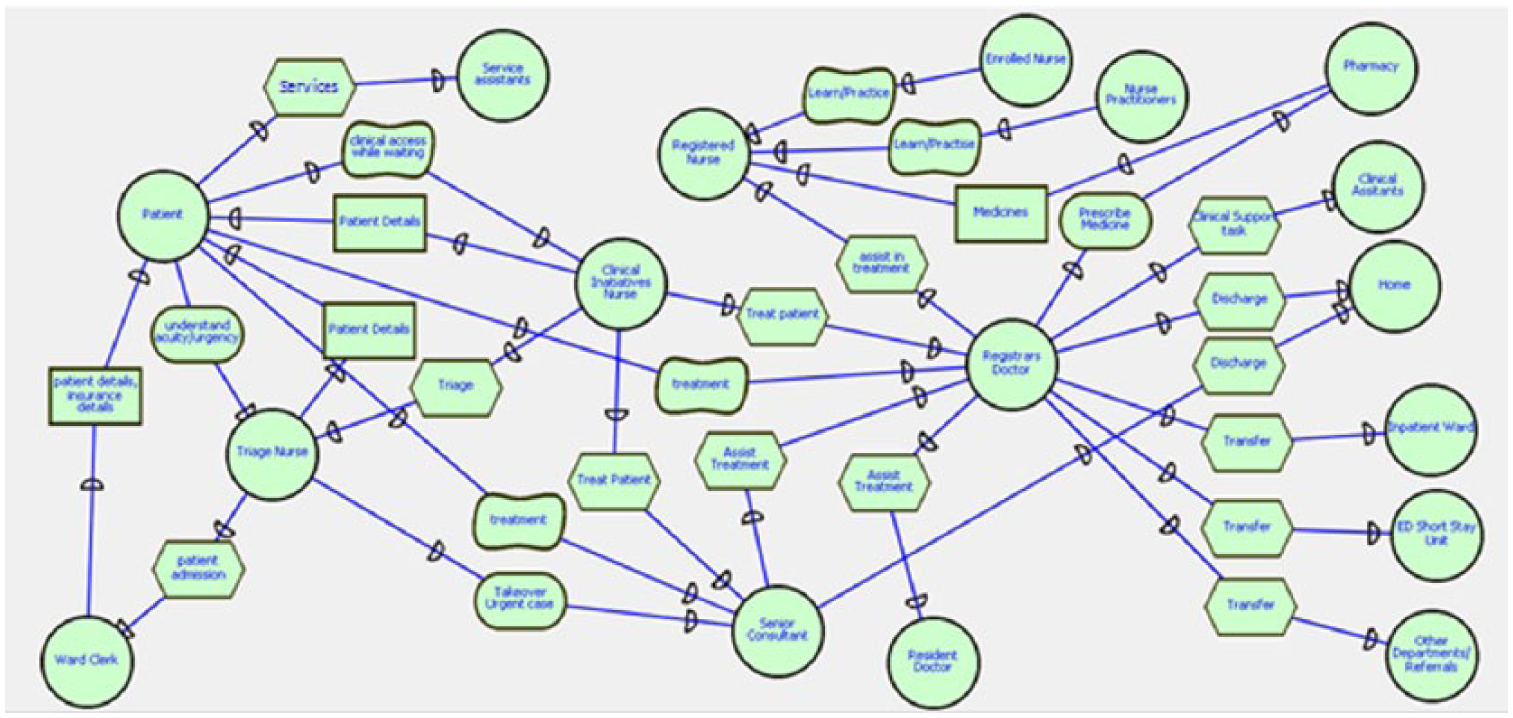
Strategic dependency (SD) model of emergency department between all actors and task (present/current).
Figures 5 and 6 show the SR model of current ED business process. The rational diagram shows the rationale behind the dependency among the actors. In other terms, these diagrams are advanced forms of dependency diagrams which contain greater details. Inside the actor boundary of each actor lies the different tasks and goals/sub-goals (rationale), which creates dependency among the actors. In this case, details of what task each actor in an ED undergoes can be viewed. Furthermore, with the help of the current rational diagram, it is easy to figure out which actor is critical in terms of business process. In this model it is clear that patient, triage nurse and registrar doctors are important actors as they interact with other actors in many occasions in ED.
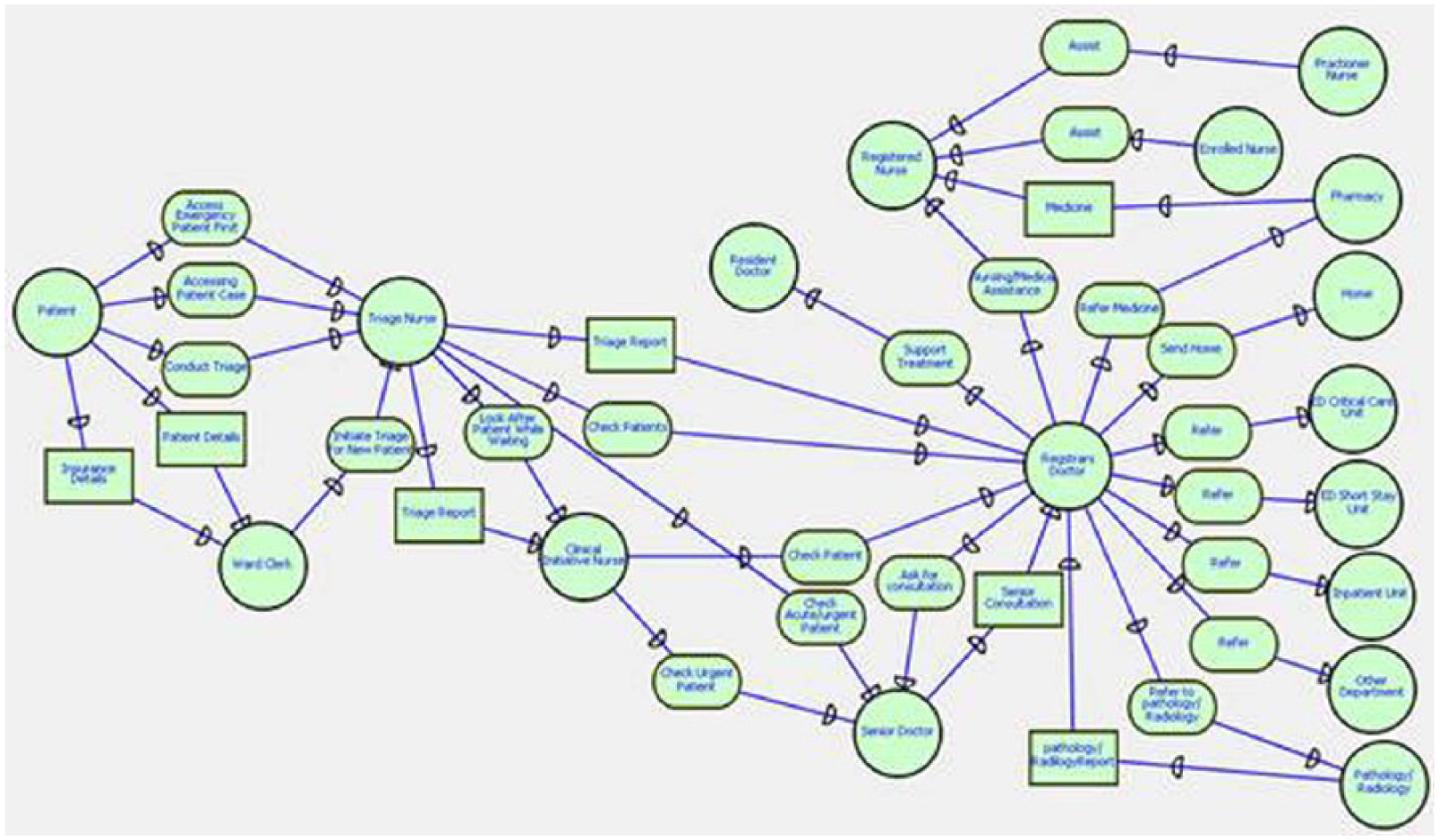
Reduced/restructured strategic rational (SR) model of emergency department between all actors and tasks (present/current).
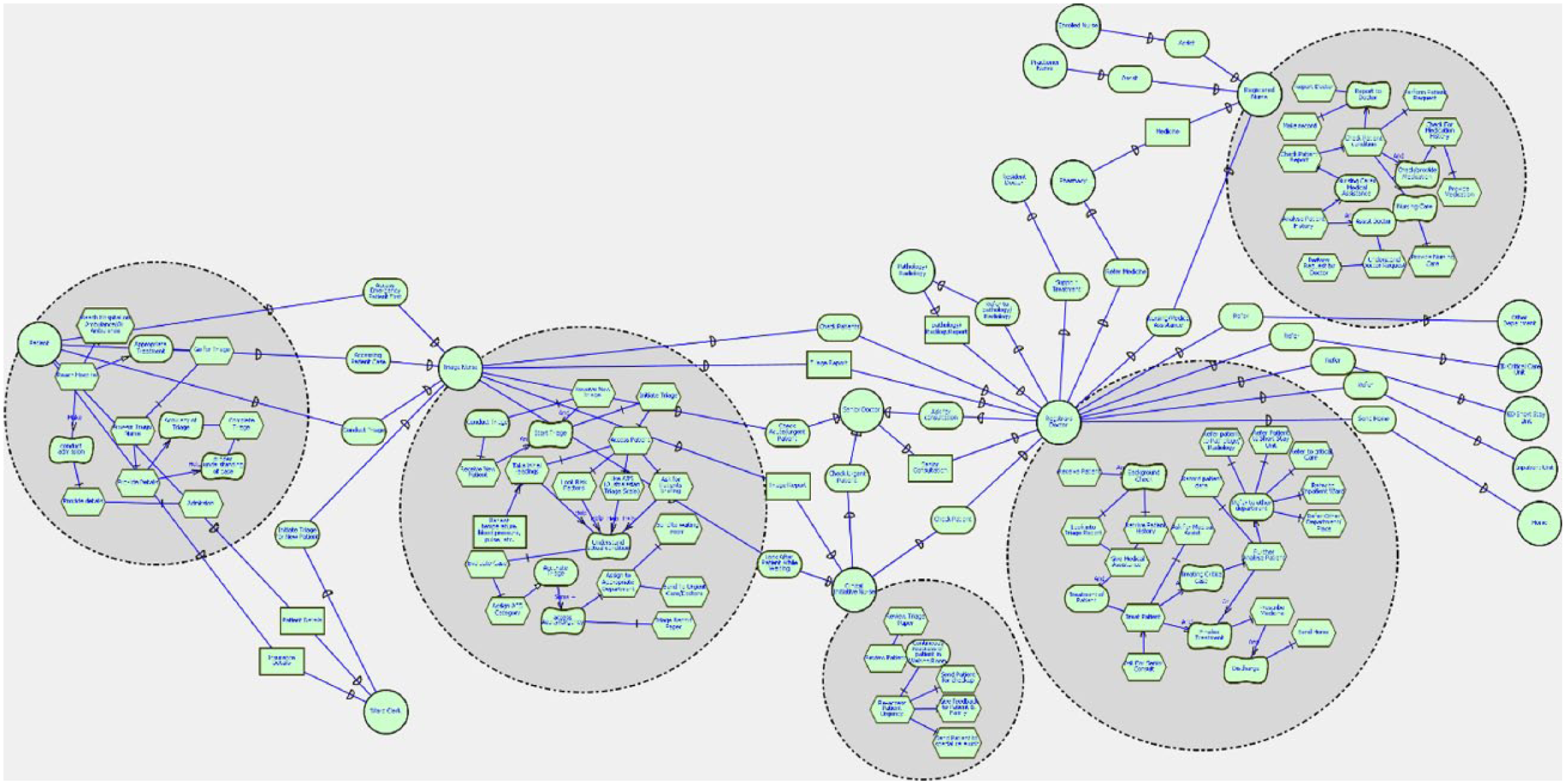
Strategic rational (SR) model of emergency department between all actors and tasks (present/current).
Limitations of current i* Organizational Models
On critical analysis of Figures 4 to 6, it is clear that the most critical actors are the triage nurse and the resident doctors (doctors) in an ED. These actors are vital in terms of efficiency in the business process and possess heavy workload. Any delays and malfunctioning among these actors will affect the whole service delivery system of ED. The key aspects of efficiency and wait time are directly under the effect of these actors’ work and behaviour. Moreover, the workload is very high on these nodes. If any improvements are to be done, then these actors need to be kept in high priority.
Proposed i* Organizational Model of ED
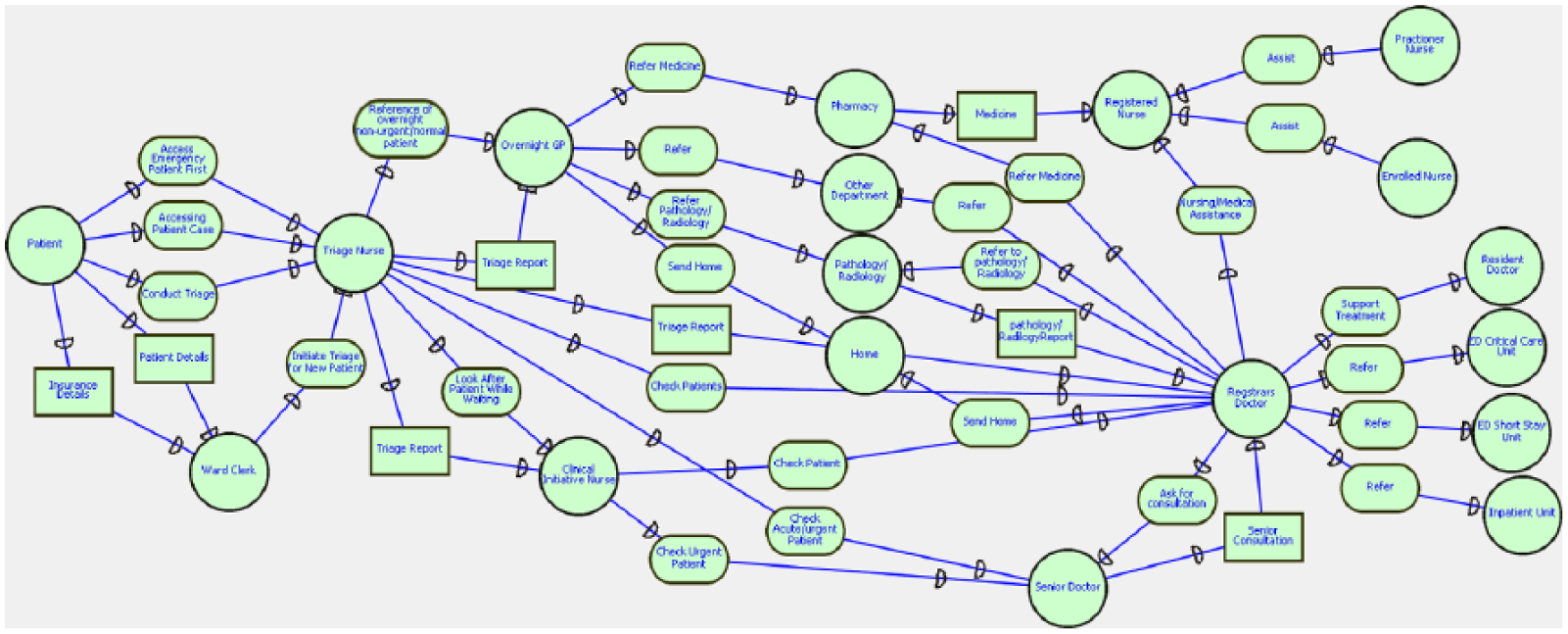
In the proposed i* Organizational Model, certain changes are made to previous i* Organizational Models which will direct the dimension of existing business process into improved version. On changing the business processing, the addition of a new actor as ‘Overnight GP’ (resident general practitioner for overnight shift) is done, who will be sharing the workload at night-time with other staff of ED. Figure 7 is a proposed SD model of ED, which incorporates the Overnight GP. Furthermore, Figures 8 and 9 are the SR model of proposed ED business process, which provides details of the task, dependency, goals/sub-goals and resources related to the Overnight GP. In these proposed i* Organizational Models, all the other aspects except the addition of Overnight GP are same as that of previously presented i* Organizational Models. In the SR models, the tasks, goals and dependency of new actor ‘Overnight GP’ are more clearly shown (see Figures 8 and 9).
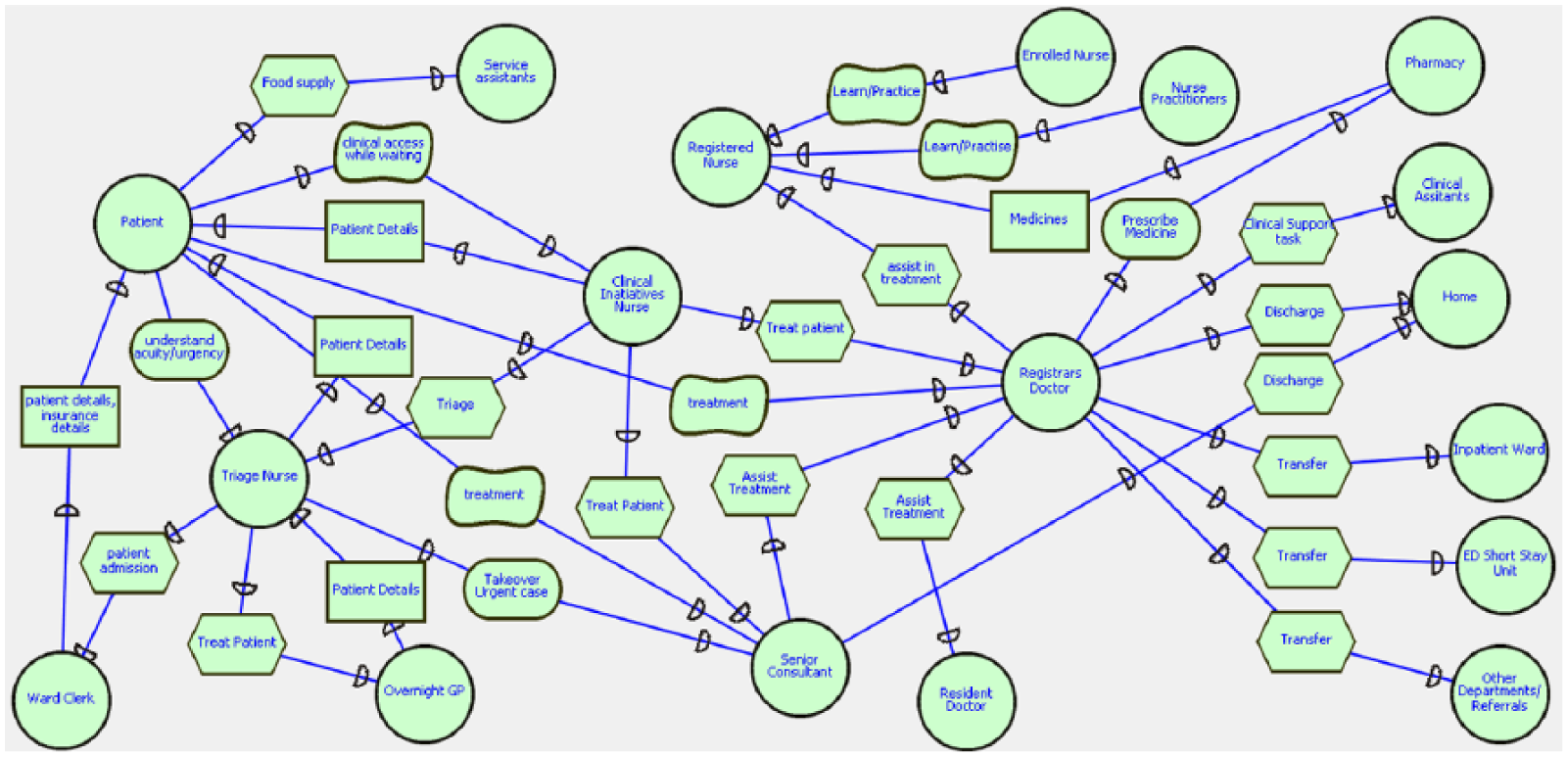
Strategic dependency (SD) model of emergency department between all actors and tasks (proposed).
Reduced/restructured strategic rational (SR) model of emergency department between all actors and tasks (proposed structure).
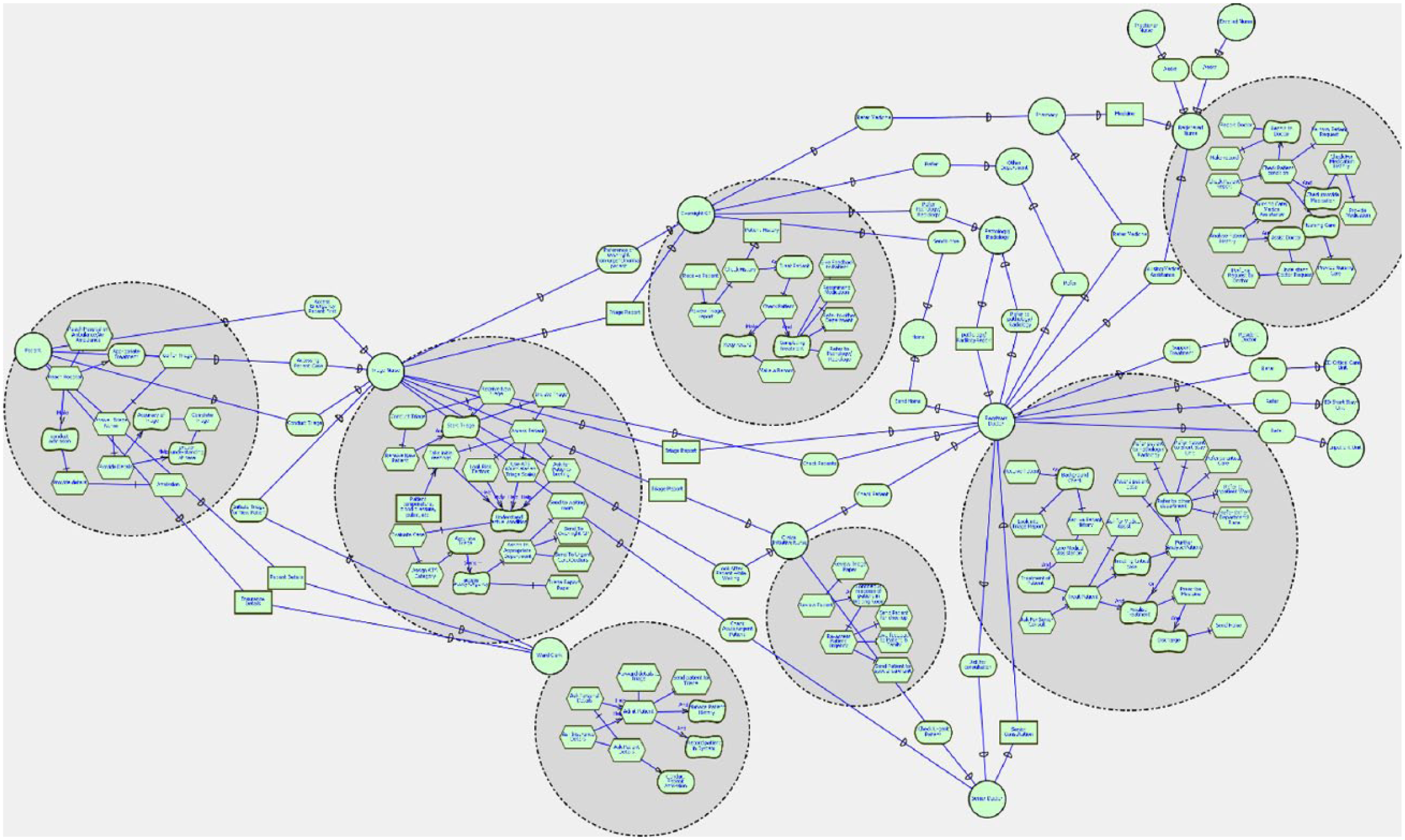
Strategic rational (SR) model of emergency department between all actors and tasks (proposed structure).
The proposed model is developed by a thorough expert analysis and research of different business processes of hospitals around the world. The concept of including an Overnight GP will strongly support the efficiency in ED. The addition of this new actor has no effect on the business process of other actors; however, the motive of producing efficiency is highly supported. However, the actual results will be clear after expert analysis, and actual implementation of the proposed concept is done. At the later section of this article, a detailed justification of the project is provided.
Benefits of proposed i* Organizational Model
The basic concept and idea of the proposed model are the same as the current model with the addition of a new node and links. The addition of a new node, ‘Overnight GP’, has made changes in dependency and link related to other actors. Furthermore, addition of this node has made possible the sharing of workload among other staff during night-time. The main objective for the addition of this node is that the triage nurse can channel down normal and non-urgent patients towards GP, which in turn will reduce heavy workload on staff in ED. Furthermore, another advantage is reducing the wait time and total stay time of other triage patient in the ED resulting from reduction of workload by channelling down non-urgent patient to Overnight GP. On the other hand, the wait time for patients pushed to Overnight GP will automatically be reduced. Normally, the wait time for Triage Category 5 patient is 3 to 4 h, depending on patient flow in ED, and the normal working of the ED is unaffected by this addition, which will only serve as a benefit.
An improved SDF for ED based on developed i* Organizational Models
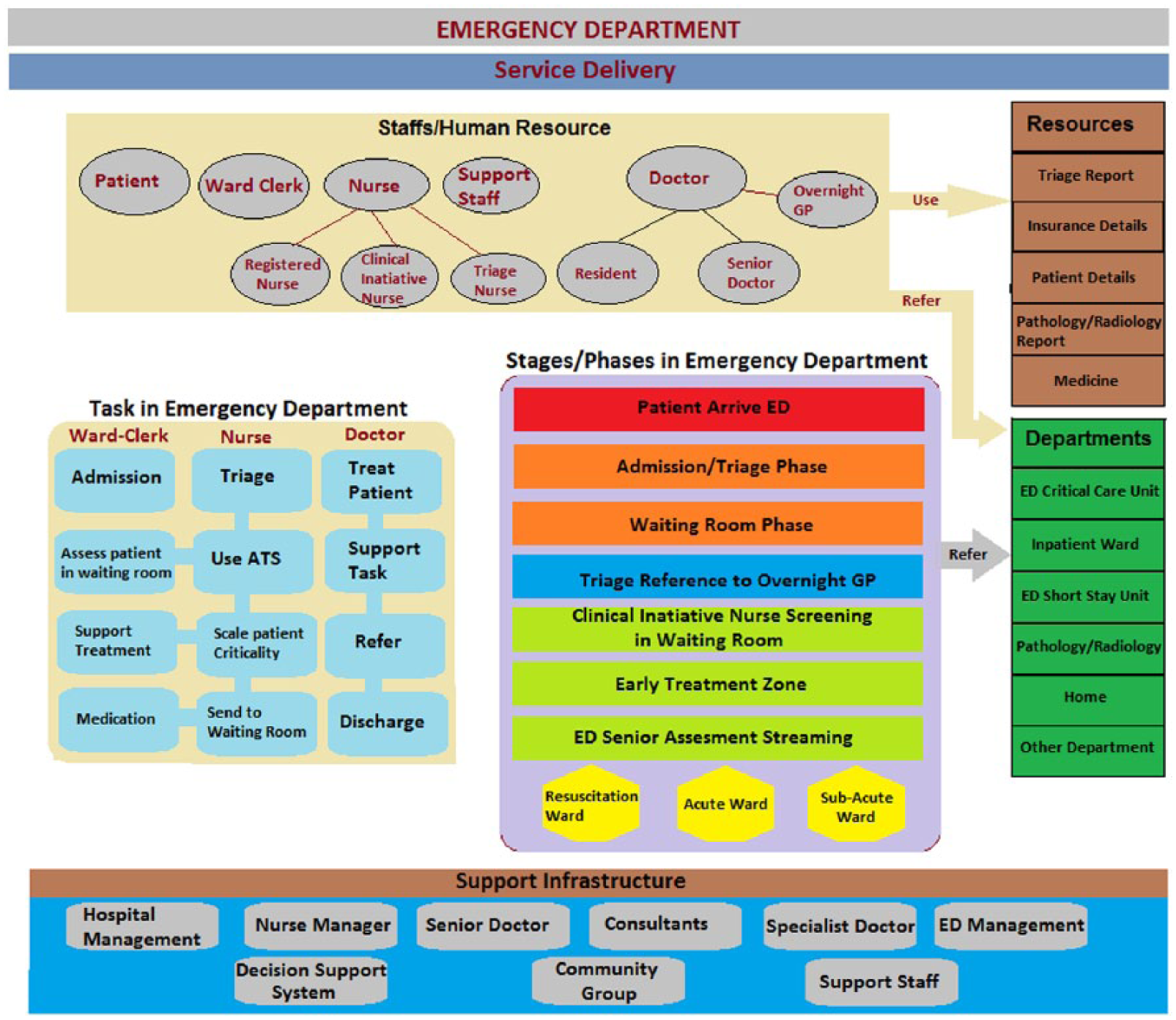
Based on the above-mentioned concept and analysis, development of an SDF for ED as shown in Figure 10 is completed. The foundation of this framework is based on the current scenario obtained from ‘The Ideal ED Patient Journey’ and the concept of business process from i* Organizational Models. Different staff, resources, departments, support infrastructure, major task in ED, and different phases/stages in ED are presented in the framework to depict a standard concept.
Service delivery framework of ED.
The framework above identifies the service delivery concept in ED of a typical hospital. It is a multilayer structure which is divided into different distinct parts. At the topmost layer lies the Staff/Human Resources. This layer is a critical aspect in this structure as all the tasks and phases/stages are worked in here. The different human resources referred to include patient, ward clerk, nurses, support staff and doctors. Doctors and nurses are broad terms for other sub-staff in this setup. The addition of Overnight GP is remarkable in this particular frame.
The next layer identifies all major tasks that are undertaken in an ED. There are three major staff who conduct these tasks. The task of admission is conducted by ward clerk. There are multiple tasks conducted by the nurse which are linked together for easy identification. The tasks of the nurse include triage, use of ATS, scale patient urgency, sending patients to waiting room, providing medication, support in treatment and accessing patients in the waiting room. At the end, the task of the doctor is highlighted, which includes treating patient, supporting task, referring to other departments and discharging patients.
The next section deals with the different stages/phases of ED. This section outlines different segments and zones in ED, which are undertaken by the human resources (located above) while conducting the task (on the left of framework). The stages/phases identified here are arrival of patient, triage/admission, reference to Overnight GP, sending patient to waiting room, Clinical Initiative Nurse (CIN) screening of patient in waiting room, Early Treatment Zone and ED senior assessment streaming. Furthermore, the section is identified by emergency wards as resuscitation ward, acute ward and sub-acute ward. This section of framework is an essential part, where all tasks, staff and resources work together to produce an effective service delivery system for patients in ED.
The stage of reference to Overnight GP is controlled by triage in this framework. The triage is conducted on the patient admitted, and if the case is non-urgent and can be handled by GP, then the triage nurse refers the patient to Overnight GP. This reference to Overnight GP is valid only during the night-time. This enables workload sharing for staff and makes functioning of ED efficient. Furthermore, significant reduction on wait time can be gained for such non-urgent patients to almost half. A dilemma can occur that who will control the functioning of Overnight GP. In addition, confusion on locating the GP might occur (within ED or outside ED). The functioning of Overnight GP is conducted by triage nurse, and general patient cannot directly access the Overnight GP who is an actor added to facilitate ED only. Since the focus is to deliver effective service for ED and provide excellent assistance to patients, location of Overnight GP is not a matter of concern.
Alongside lie the resources and departments that support the task of ED. These resources and departments expedite the different phases/stages/areas of ED for effective functioning. The staff/human resource applies the resources to perform tasks and to refer patients and tasks to other departments.
At the lowest part of the framework under discussion is the support Infrastructure. These infrastructures include hospital management, nurse managers, specialists, ED management and other support areas. All these support infrastructures ensure that the framework allows efficient and a standard service to be delivered.
A demonstration of improved business process of ideal ED patient journey
With the proposal of framework, patterning i* Organizational Models and restructuring the business process of ED, it is essential to work out and restructure the basic diagram (ideal ED patient journey). In Figure 11, the proposed ideal ED patient journey is exhibited. Major changes have not been made, and the whole diagram is almost the same as the previous one except for adding the Overnight GP.
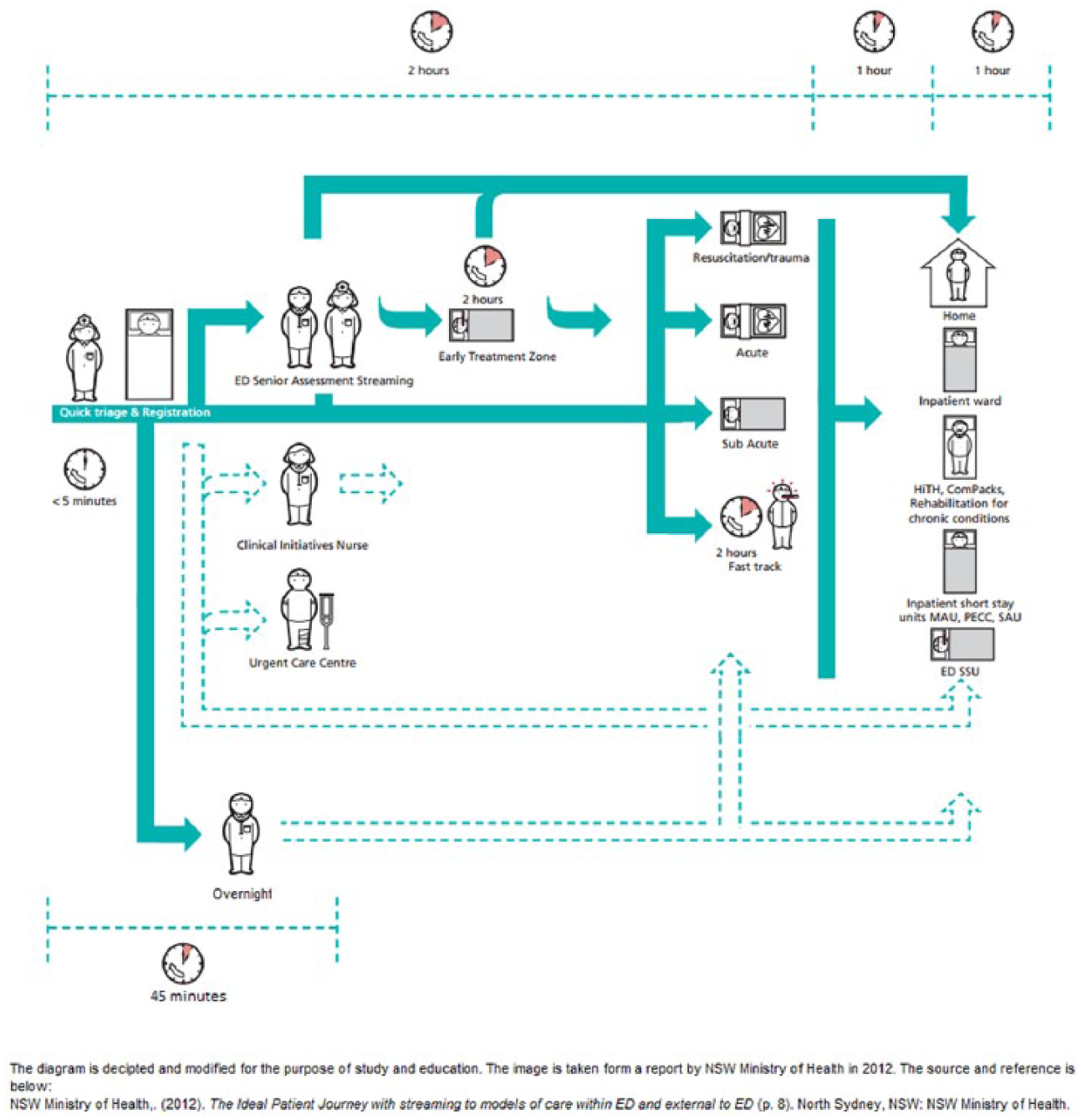
A demonstration of improved business process of ideal emergency department patient journey adapted from NSW Health Ministry. 3
The new patient journey now features an Overnight GP, which is channelled up by triage process. The triage nurse makes a call for Overnight GP for non-urgent cases. Figure 11 clearly shows how the call is made by the triage nurse for the GP and how the GP makes a call or refers a patient to other departments/wards/sections, if necessary. Furthermore, the timeline shown is significant in this figure, where the normal non-urgent patient would require up to 4 h for complete treatment in normal/current ED here it has been reduced to 45 min of overall stay time. The time saved is 3.25 h in terms of stay time for non-urgent patient. Furthermore, workload on ED staff is reduced, which brings efficiency to the department. This will significantly drop the wait time and stay time of the patients who are not forwarded to Overnight GP (other triage scale patients) in ED.
Evaluation of proposed model
Evaluation in a practical project is an attempt towards explaining why a proposed model/framework is effective to solve a particular problem of a working environment. Furthermore, a justification is required to explain how to implement the solution in the practical environment. A set of comprehensive analyses must be provided, and a satisfactory result on problem solving is required. 26 This section will evaluate the proposed model and business process to see whether it can be justified to be used in ED. The evaluation is conducted under four parameters – key to the issue of efficiency in ED (i.e. workload, human resource, wait time and time of stay).
Context of evaluation
The practical implementation of this proposed model is not possible at this point of time, as preparing this report will not be an easy task and criteria have to be met before implementation. Furthermore, the absence of previous work on a similar subject prevents comparative study as well. Hence, in this article, justification of the model based on expected outcomes with current status is conducted. Selection of parameters on justification enables to define the scope of work. The common parameters to prove the efficiency of the proposed service delivery system and proposed framework are wait time, overall stay time, human resource and workload on staff. All these parameters are connected to each other, as any alteration on any, or a combination, of them produces changes in efficiency of service provided by the ED. Furthermore, these parameters are also interconnected because any changes in one produce changes in other parameters as well. The efficiency and results of this proposed model will be evaluated in terms of these parameters.
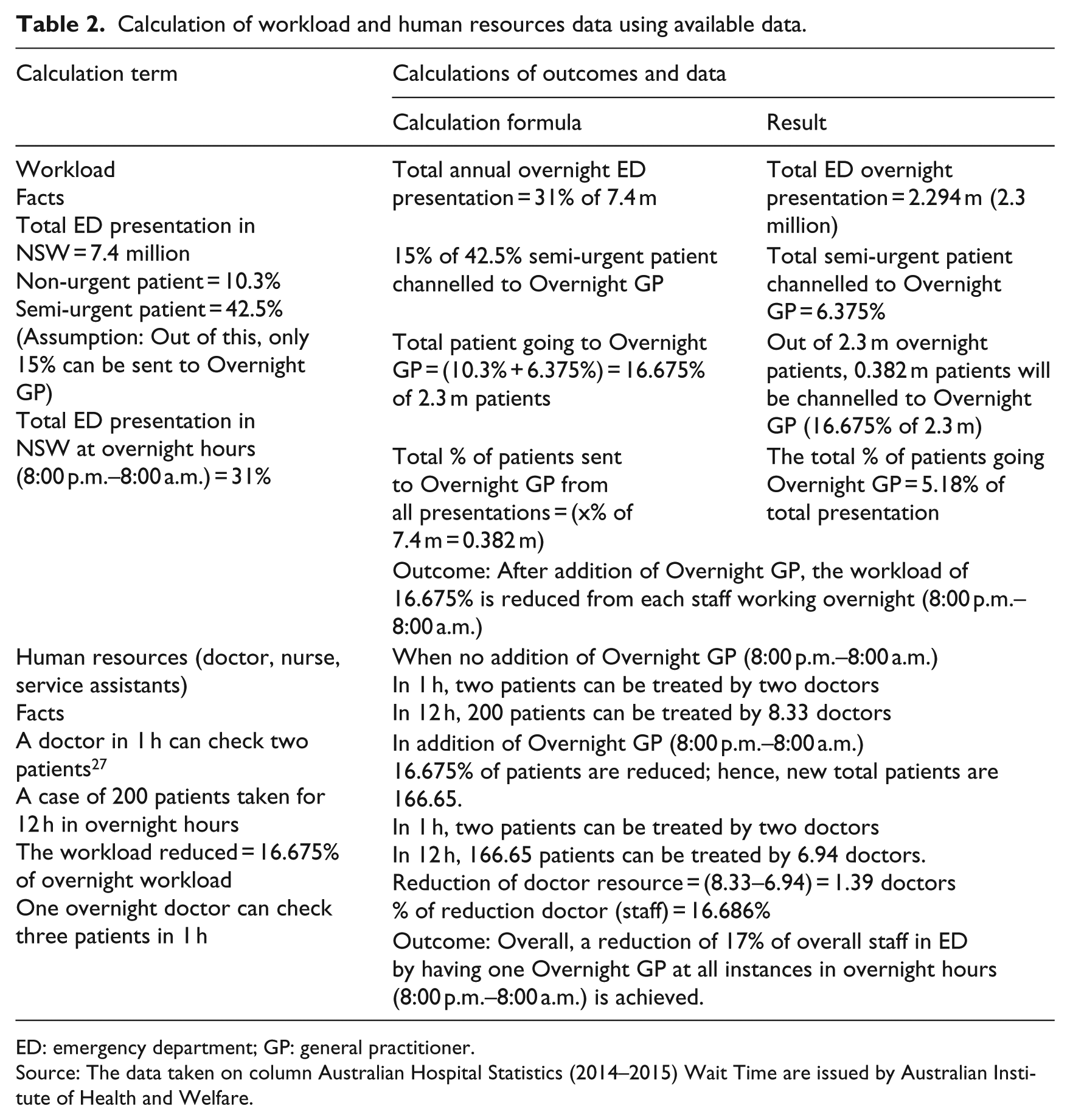
The case of Australian ED data is considered to access the justification. Table 2 shows all the calculations and outcomes for the parameters, workload and human resource.
Calculation of workload and human resources data using available data.
ED: emergency department; GP: general practitioner.
Source: The data taken on column Australian Hospital Statistics (2014–2015) Wait Time are issued by Australian Institute of Health and Welfare.
Workload
According to the online Cambridge Dictionary, 28 workload is ‘the amount of work to be done, especially by a particular person or machine in a period of time’. Here, the situation is about workload on the staff in an ED. The workload of ward clerk and triage nurse of the ED will be the same even after the addition of Overnight GP. However, workload on the staff who attend and access patient after the triage will drop significantly. From the calculation given above, it is claimed that, on an average, the workload of the staff working overnight will be reduced by 16.675 per cent per staff. If workload decreases, the staff will be able to provide better service to patients as they are not pressurized. Furthermore, this also increases the focus and communication of staff towards patients enabling better performance.
Human resource
The online Oxford Dictionary 29 defines human resource as ‘The personnel of a business or organization, regarded as a significant asset in terms of skills and abilities’. The term human resource here indicates all actors, except patient, such as staff, doctors, nurses, support staff, service assistants, specialized doctors, business office personnel and so on. On average, an ED in the United States has the facility and physicians who can see two patients per hour per doctor, as per the study provided by Collins. 27 But if this number goes up to 2.3 to 2.8, then the situation requires addition of more human resource. 27 The exact figure of human resource in Australian Hospital is not available even in the Hospital Resource 2013–2014. 7 In this state where no data are available from Australian Hospital, a standard of two patients per hour treated by a doctor is adopted.
Now, calculation of percentage reduction on doctors (human resource) is done as below, by taking 200 patients in 12 h overnight shift:
In 1 h, two patients are checked by one doctor;
In 12 h, 200 patients are checked by 8.33 doctors.
After addition of Overnight GP, reduction of patients is by 16.675 per cent. Hence, total patients in new case are 166.65 patients.
In 12 h, 166.65 patients are checked by 6.94 doctors after adding Overnight GP;
Percentage reduction on doctor’s resource per overnight is 16.686 per cent.
An Overnight GP is allocated on non-urgent patients; hence, they can check three patients per hour, which will turn in 12 h that they can check 36 patients, which means they can easily handle the patient channelled from Triage.
Overall, a reduction of 17 per cent of overall staff in ED by having one Overnight GP at all instances in overnight hours (8:00 p.m.–8:00 a.m.) is achieved.
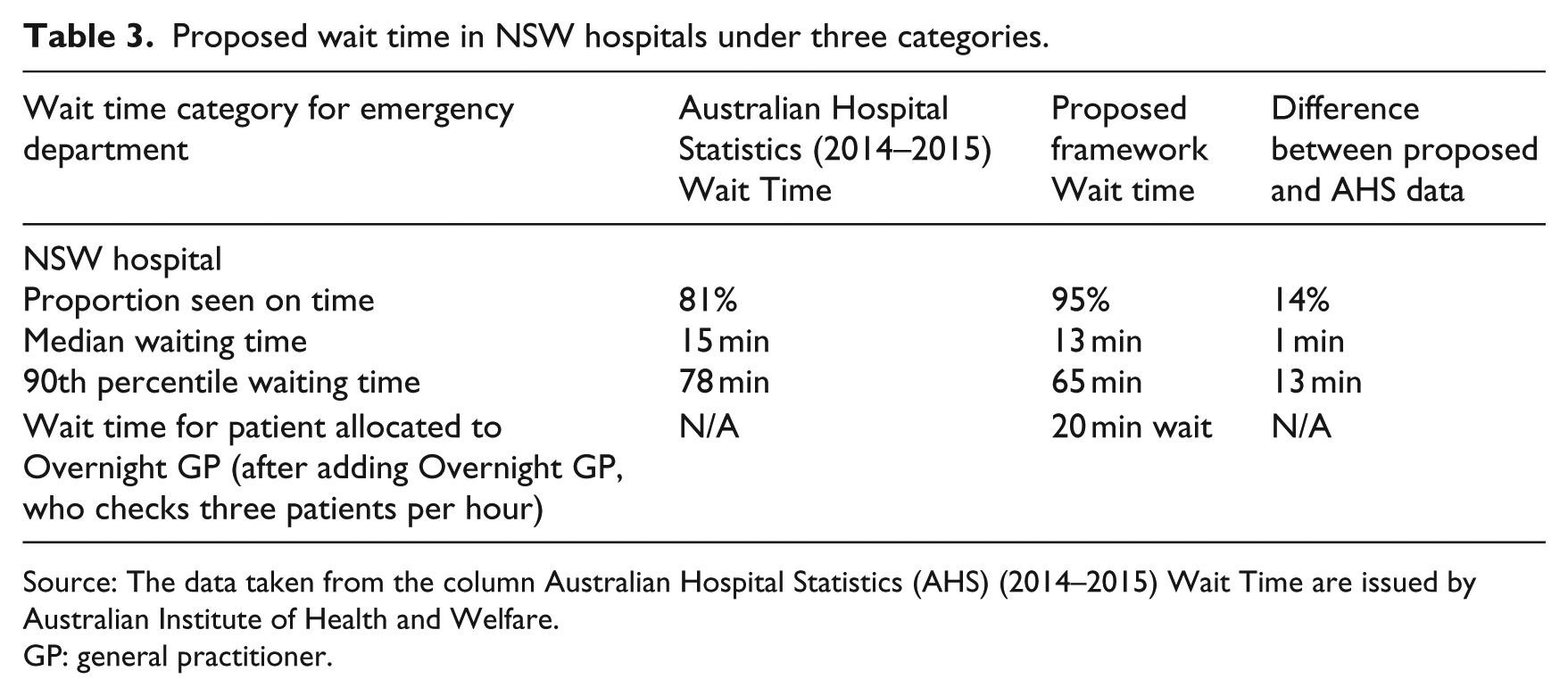
Wait time
Wait time is the time that elapsed from patient presentation in ED to commencement of treatment. 30 This justification is done for data of NSW hospitals only. The statistics released by Australian Institute of Health and Welfare has used three prospects of wait time calculation, which are as follows (see Table 3):
The proportion of presentations seen on time;
The 50th percentile waiting time (median waiting time where 50% of presentation has commenced clinical care);
The 90th percentile waiting time (where 90% of presentation has commenced clinical care).
Proposed wait time in NSW hospitals under three categories.
Source: The data taken from the column Australian Hospital Statistics (AHS) (2014–2015) Wait Time are issued by Australian Institute of Health and Welfare.
GP: general practitioner.
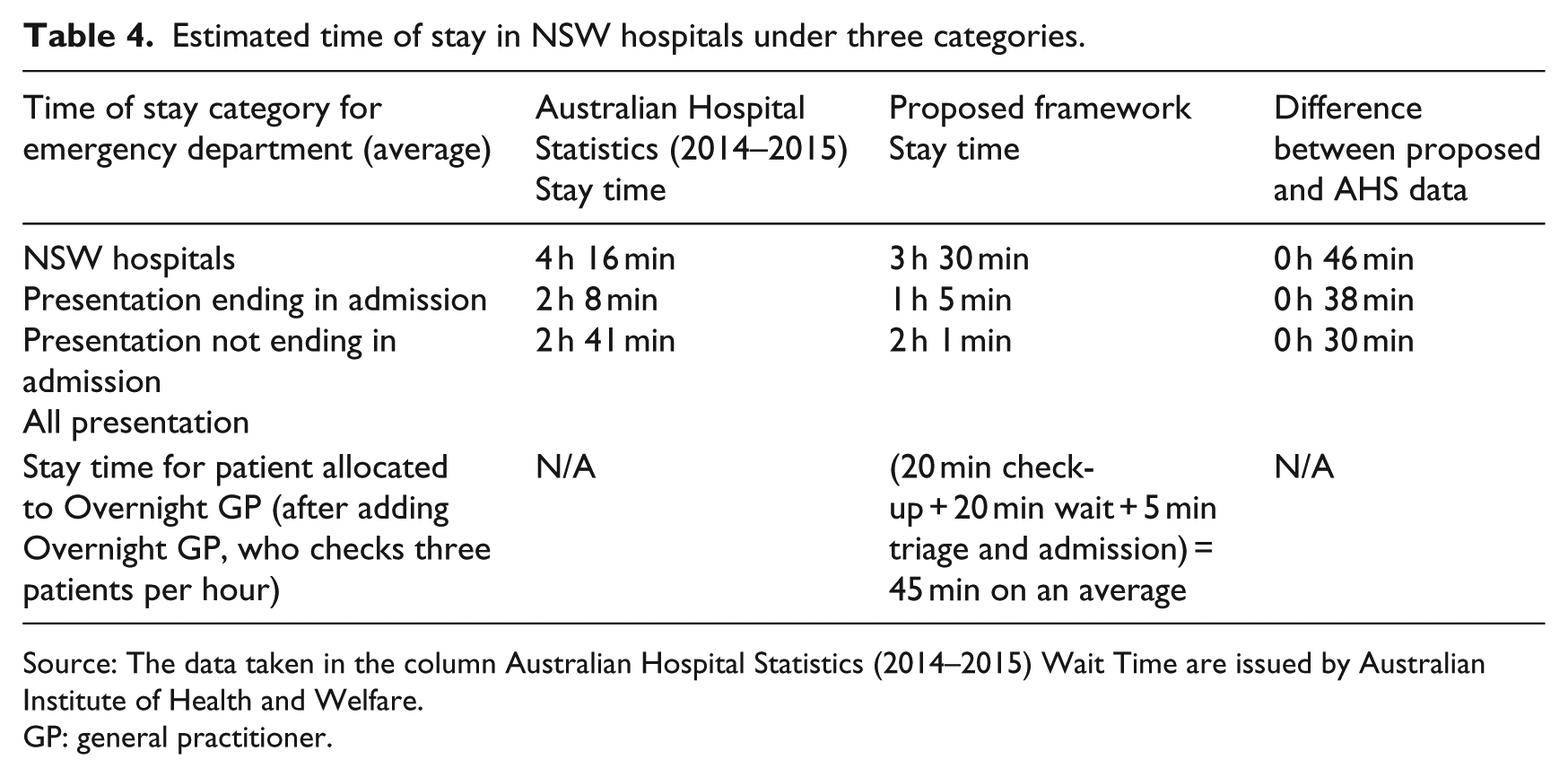
Time of stay
The time of stay in the ED is the overall time spent in an ED after entering it and until leaving the ED. The time range can end in other departments, including referral from ED or discharge. The statistics by Australian Institute of Health and Welfare 7 states three categories for calculating time of stay (see Table 4):
Presentation ending in admission;
Presentation not ending in admission;
All presentation.
Estimated time of stay in NSW hospitals under three categories.
Source: The data taken in the column Australian Hospital Statistics (2014–2015) Wait Time are issued by Australian Institute of Health and Welfare.
GP: general practitioner.
Conclusion
This article identified major service delivery issues within hospital EDs and proposed an improved model based on i* Organizational Model. The service delivery in ED has been severely affected by the overcrowding, long wait time, long stay time and workload on staff. The project explored a number of approaches and solutions to the key issues of service delivery in ED. The article shows that there were many cases and research papers on business process improvement to produce effective services in health sector. In this project, the new approach in business process by the addition of Overnight GP has solved these issues. The evaluation of the proposed model clearly shows that there is significant drop on wait time and stay time of patients in ED.
This innovative article has summarized both the current and proposed business processes of ED into i* model, which, when studied in detail and properly interpreted, justifies the use of i* framework in ED. The project of innovation of service delivery in ED has introduced the Overnight GP into the proposed framework and ideal ED patient journey with better results than previous practice. The project has successfully incorporated the use of i* Organizational Modelling technique for the purpose of business process improvement. The aim of the project is to bridge a gap in ED by using i* Modelling technique out of BPM. This has also been achieved.
In addition, the article has successfully evaluated the proposed model, framework and business process in terms of the key elements like wait time, stay time, workload and human resource. The drop on wait time and stay time as shown by evaluation is the most significant success of the proposed concept. The study shows that the patients pushed to Overnight GP have a new proposed wait time of 20 min and stay time of 45 min which is a significant figure. Furthermore, pushing non-urgent (ATS 5) patients and 15 per cent of semi-urgent (ATS 4) patients to Overnight GP will make sure that the ED is not crowded, and service is delivered efficiently with reduced wait and stay times. Moreover, the evaluation has proved that there is a drop of 16.675 per cent of workload from each staff as well as a reduction of 17 per cent of staff from ED. We look forward piloting this project in the future by keeping the financial and operational aspects into consideration.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.