
Abstract
Emergency department (ED) operational metrics generated by a new acuity-based rotational patient-to-physician assignment (ARPA) algorithm are compared with those obtained with a simple rotational patient assignment (SRPA) system aimed only at an equitable patient distribution. The new ARPA method theoretically guarantees that no two physicians’ assigned patient loads can differ by more than one, either partially (by acuity levels) or in total; whereas SRPA guarantees only the latter. The performance of the ARPA method was assessed in practice in the ED of the main public hospital (Hospital Compound of Navarra) in the region of Navarre in Spain. This ED attends over 140 000 patients every year. Data analysis was conducted on 9,063 ED patients in the SRPA cohort, and 8,892 ED patients in the ARPA cohort. The metrics of interest are related both to patient access to healthcare and physician workload distribution: patient length of stay; arrival-to-provider time; ratio of patients exceeding the APT target threshold; and range of assigned patients across physicians by priority levels. The transition from SRPA to ARPA is associated with improvements in all ED operational metrics. This research demonstrates that ARPA is a simple and useful strategy for redesigning front-end ED processes.
Introduction
Changes to front-end operations are particularly effective for reducing ED overcrowding 1 because they are usually directly controlled by the ED without the involvement of external stakeholders, which would be practically or politically more difficult. This area for improvement in ED performance has been addressed in the medical literature2–4 as well as in operations research studies.5–8
According to Saghafian et al. 7 the patient pathway from the waiting area to treatment by a physician also impacts on the flow of patients through the ED. Many EDs use the traditional physician self-assignment process, whereby physicians “pick up” patients from a queue where triage nurses place newly registered patients as “ready-to-be-seen.” That is, there is a single queue leading to multiple servers/physicians. This single queue configuration has been demonstrated by traditional queueing theory to be more efficient than a dedicated queue set-up, 9 where incoming patients are immediately assigned to a physician after triage (with a dedicated queue leading to each server).
Nevertheless, empirical medical research reports that performance improvements are obtained when using a dedicated queueing system based on simple rotational patient assignment (SRPA)10–17 as opposed to a single queue configuration. Reported improvements include a reduction in arrival-to-provider time (APT),11,13,14,16,17 an increase in patient satisfaction,11,12 and improvements in length of stay (LOS),4,16,17 discharge rates, 14 left-before-being-seen,16,17 and complaint ratios.16,17
Although the SRPA guarantees that all physicians see the same number of patients, it may lead to unbalanced workloads due to the randomness of patient arrivals. Some studies report physicians’ complaints about this outcome, 4 describing the method as “mercilessly fair”. 16 Though the total number of patients assigned seems equal, without further differentiating acuity or complexity of patient, patients that require a higher-workload may stack at a certain physician. Therefore, we propose a new acuity-based rotational patient assignment (ARPA) that aims to assign patients to physicians with a more even patient-acuity distribution. Since evidence shows that workload is related to patient severity,16,18–21 even patient-acuity distribution can potentially ensure a more equitable workload between physicians, and lead to better quality of care and physician working conditions.
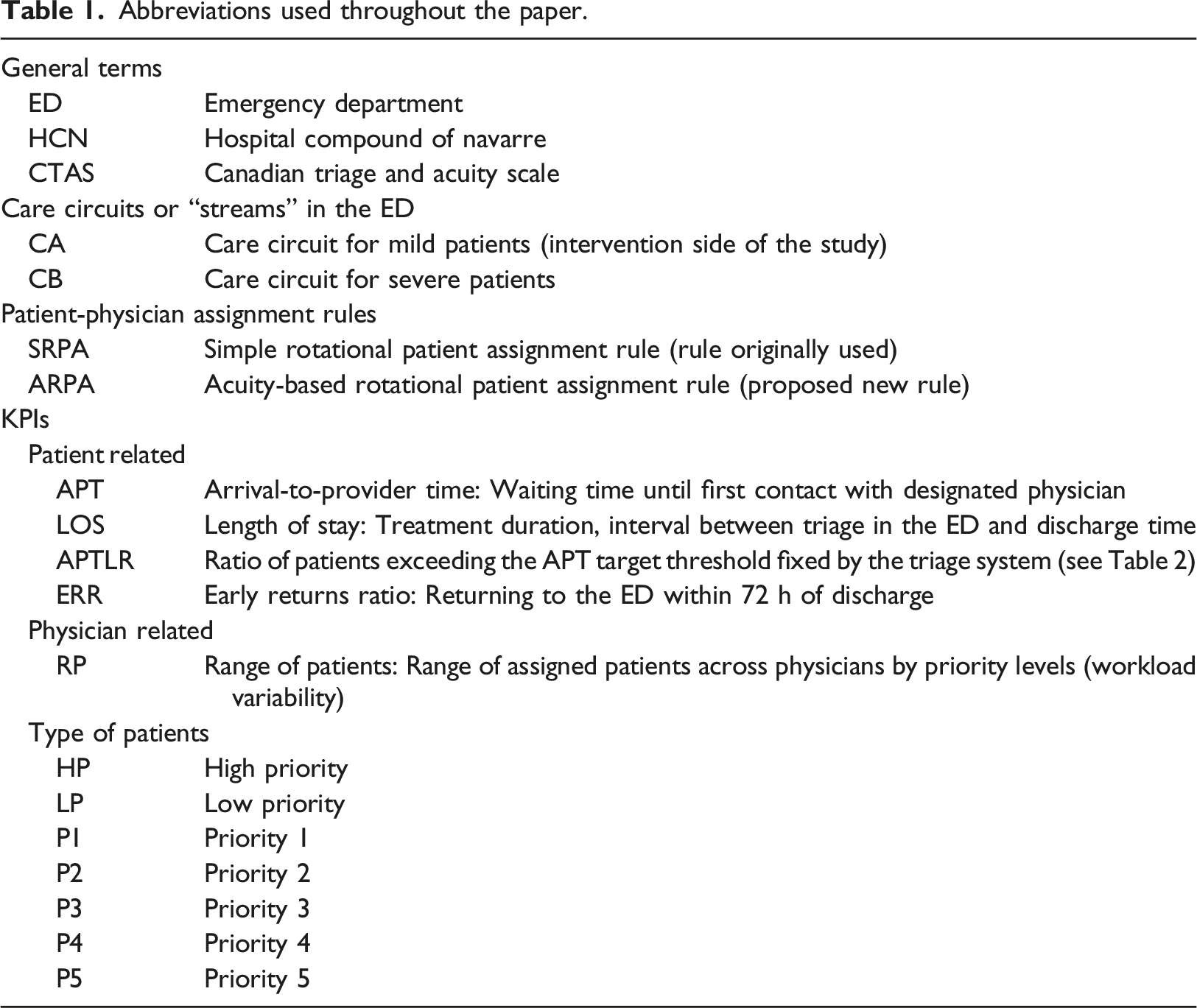
Abbreviations used throughout the paper.
Methods
This is a retrospective before-and-after observational study in which routinely gathered ED operational data are analysed to compare the effects of the new ARPA system on several Key Performance Indicators (KPIs).
Patient flow in emergency departments
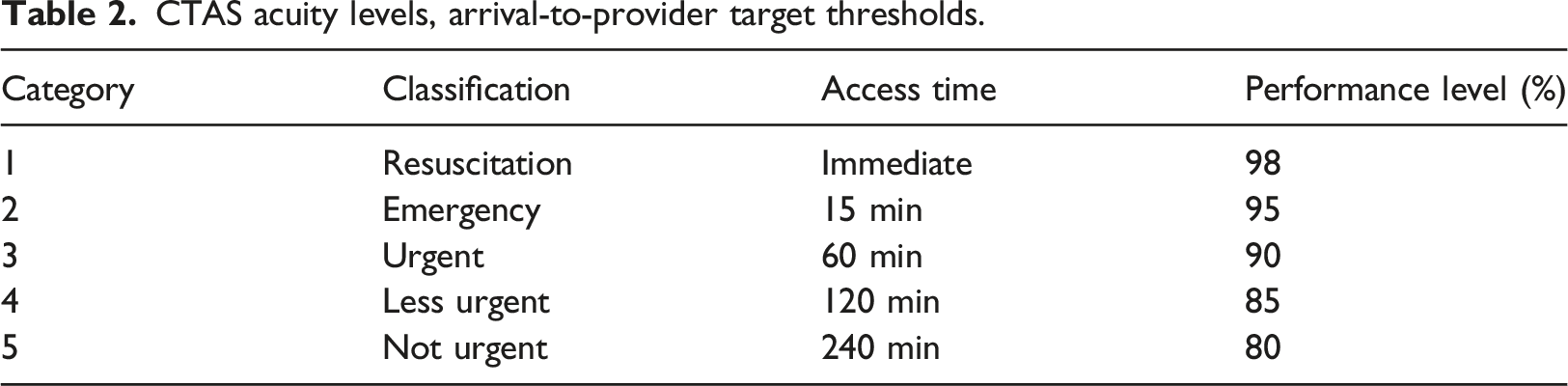
CTAS acuity levels, arrival-to-provider target thresholds.
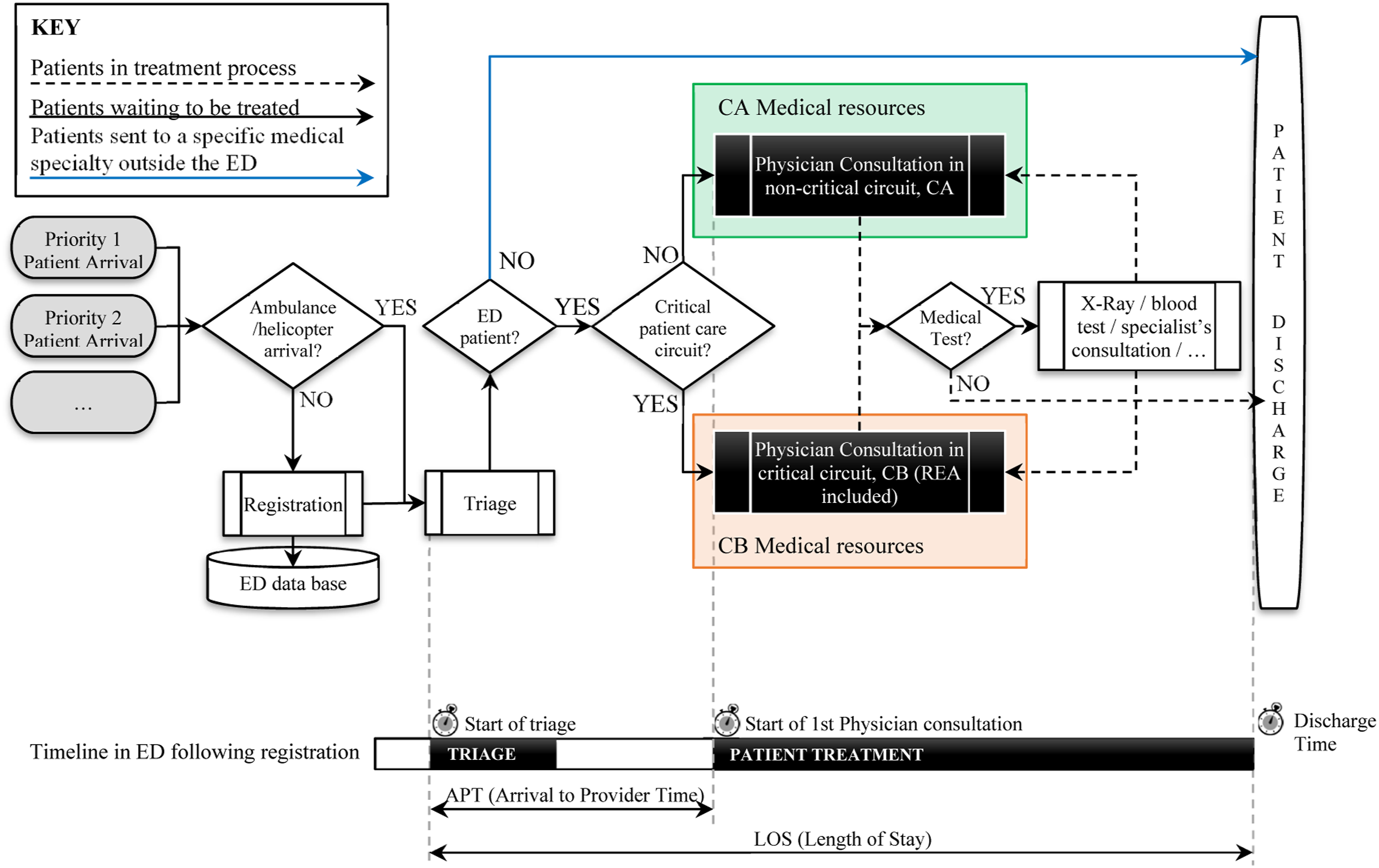
Patient flow in an ED (top of figure). Time records and time intervals considered in the study (bottom section of figure).
Acuity-based rotational patient-to-physician assignment rule
As discussed in the introduction, after triage, patients are immediately assigned to a specific physician. As an alternative to Simple Rotational Patient Assignment rules (SRPA), which is a cyclical process with no other consideration than order of arrival (see Figure 2), this paper proposes a new rotational acuity-based assignment method (ARPA), whereby patients are classified as either high or low priority (HP and LP, respectively). To show how the method works, Figure 2 depicts a mild patient circuit with five physicians, where level 3 acuity patients (P3) are considered HP and levels 4 and 5 (P4 and P5, respectively) are considered LP. HP patients are assigned rotationally from physician A to E, while LP patients are assigned rotationally from physician E to A (reverse order). These two rotational patterns are repeated indefinitely. The double wheel system provides the double guarantee that no two physicians’ assigned patient loads can differ by more than one, either partially (by acuity levels) or in total; whereas SRPA guarantees only the latter. Differences in patient distributions (workload differences) among five physicians generated by the application of SRPA rules versus the new ARPA rules with the same sequence of 18 incoming patients. ARPA uses a double wheel patient assignment system, whereby high-acuity patient assignment follows an A-B-C-D-E pattern and low-acuity patient assignment follows the reverse E-D-C-B-A pattern.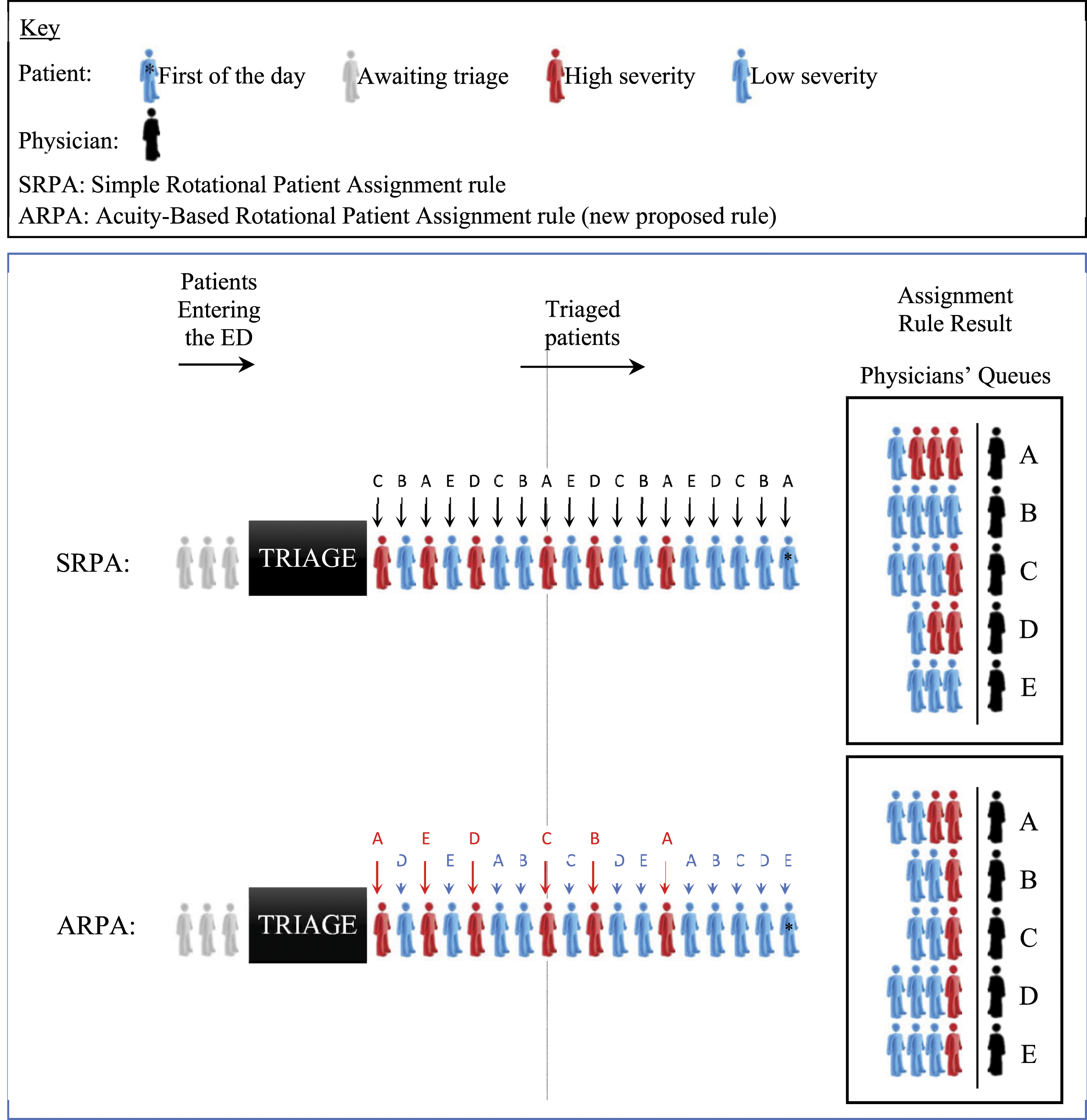
The pseudocode for the software used in the new ARPA is summarised in Algorithm 1. It is a non-commercial program, written in Java programming language and developed in consensus between hospital managers and the research unit of our department.
Algorithm 1: ARPA software pseudocode. Set of Set of Acuity score of patient Initialize End End
End
Setting
The performance of the ARPA was assessed in the ED of the main public hospital (Hospital Compound of Navarra, HCN) of the region of Navarre in Spain. This ED has more than half a million potential patients and attends over 140 000 every year.
All patients undergo nursing triage in a dedicated examination room, at which time an encounter record and patient chart are generated. The daytime triage protocol assigns patients, according to their severity, to one of five clinical acuity categories (P1-P5) and to one of two distinct care circuits or “streams.” Severe patients are channelled into the critical care circuit, CB, and mild patients into the non-critical care circuit, CA. Within the selected circuit (CA or CB), both of which have dedicated resources in terms of medical staff, examination rooms, etc. Patients are then assigned to a specific physician, who is responsible for their treatment until their discharge from the ED. Described in what follows is the implementation of the ARPA method in the CA circuit, which receives P3, P4, and P5 patients. Figure 3 shows the layout of the ground floor of the HCN ED building. Layout of the ground floor of the ED building of the HCN.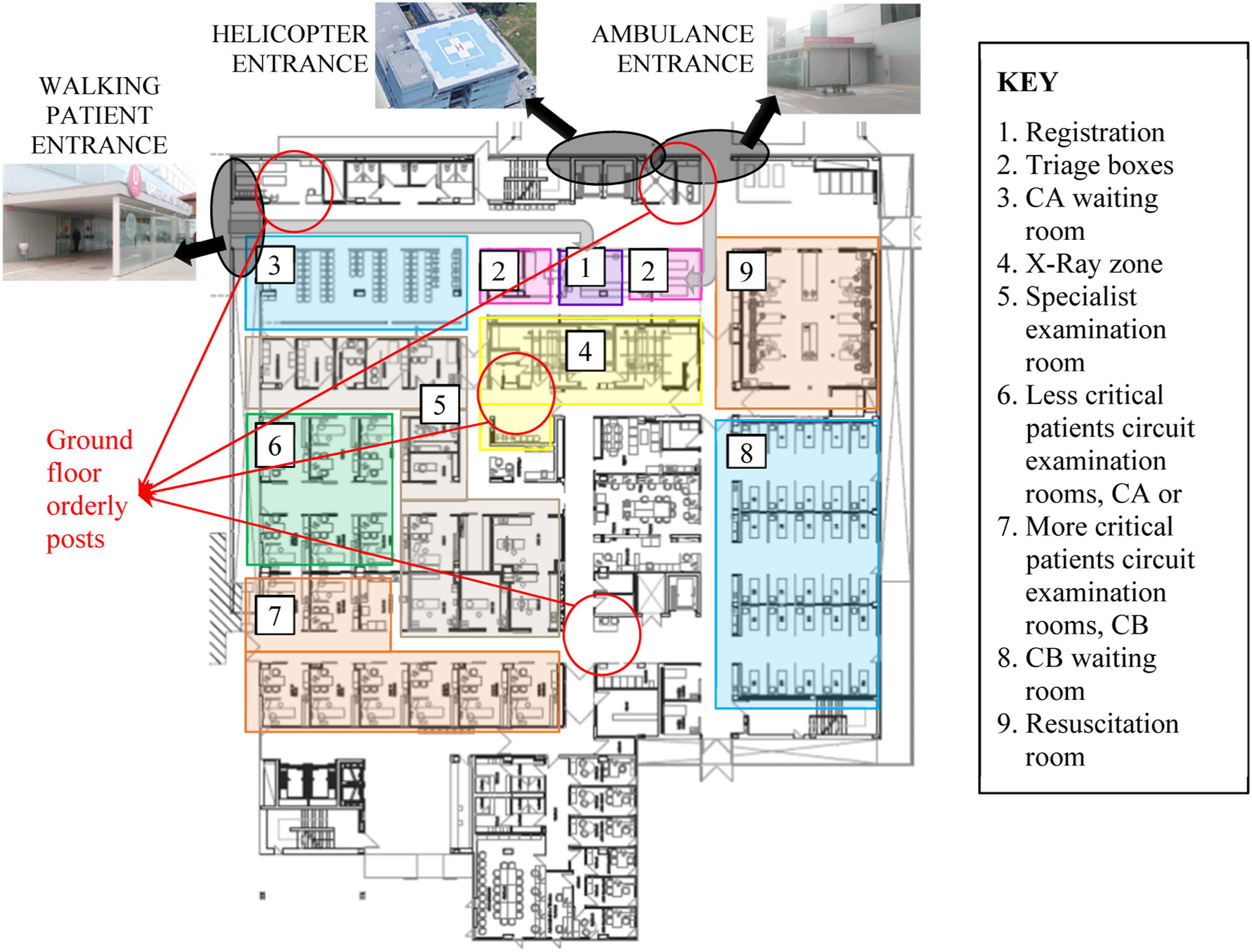
Data collection
All emergencies for a period of four full weeks (June 4 to July 1 of 2019), comprising 8,892 patient visits, are compared to those of the corresponding four full week period of the previous year (June 5 to July 2 of 2018), comprising 9,063 patient visits. The ARPA method is used during the 2019 period to assign patients to physicians in CA, while SRPA is used in CB during both periods and in CA during the 2018 period.
The performance of the ED was analysed in the busiest time of day (from 12:00 to 20:00) to avoid any bias due to physicians’ behaviour. Prior research suggests that there is a drop in work pace at low workload levels because servers see no need for speed when capacity is slack; and physicians, as strategic servers, are able to adjust their service rate by reducing their work pace, as happens in other sectors.24,25
The ED electronic medical record and electronic tracking board software are the same during both phases of the study period, as are factors such as ED physical structure, triage system and process, workflow (Figure 1), personnel compensation (salaried with no component for clinical productivity), organization, and human resource endowment. To avoid any alteration or interference in their activities, the ED physicians were not informed that this study was in progress.
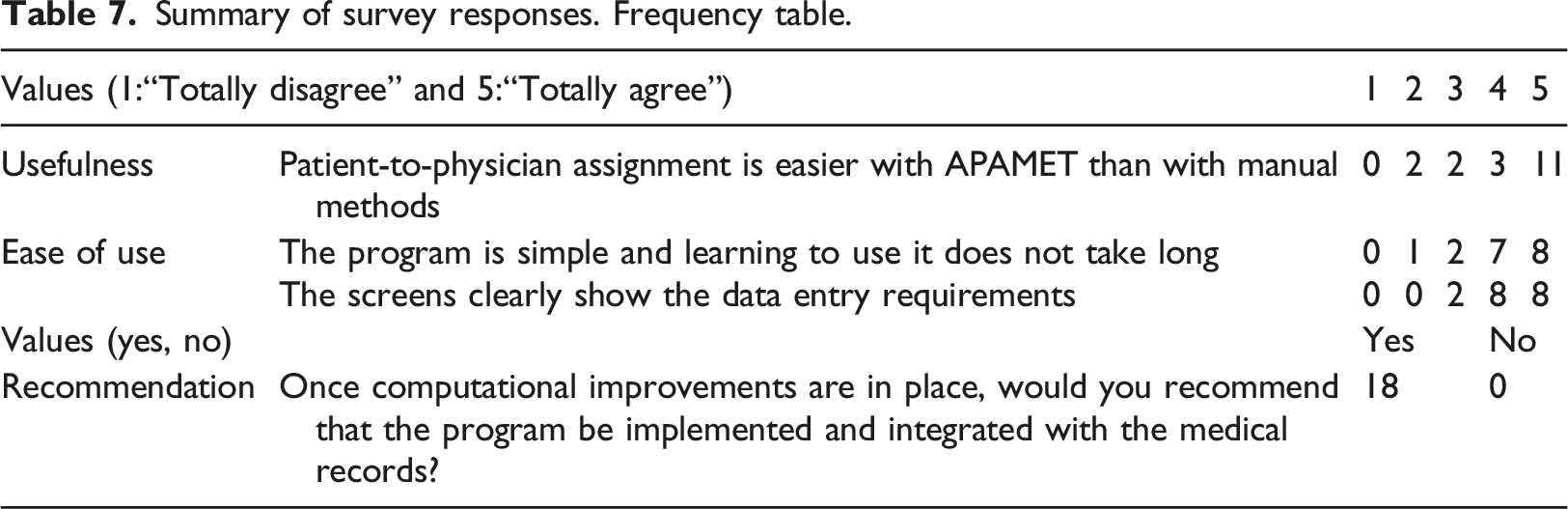
The chief of nurses proposed that a survey be conducted, after the pilot test period, to investigate the ED users’ (triage nurses) assessment, perception, and acceptance of the software that implements the new assignment rule.
Data analysis
LOS is defined as the time interval between patient triage and discharge from the ED and APT as the time interval between patient triage and first physician examination (see Figure 1). LOS and APT data are reported in minutes. A patient exceeds the APT target threshold when he/she has not been seen by the physician within the access time determined by the triage system (see Table 2), and an early return is defined as re-presentation to the ED within 72 h of discharge. APTLR and ERR are reported as ratios. Equity in the number of patients (LP and HP) assigned across physicians is measured as the daily range of assigned patients across physicians by priority levels,
The confounding variable data, which include patient demographics (age, gender, acuity, and medical test requirements), and ED daily operational metrics and volume, are collected and analysed after discussion with the ED medical staff. The daily volume of each ED circuit is defined as the number of patients registered between 8:00 and 21:00 on the day in question.
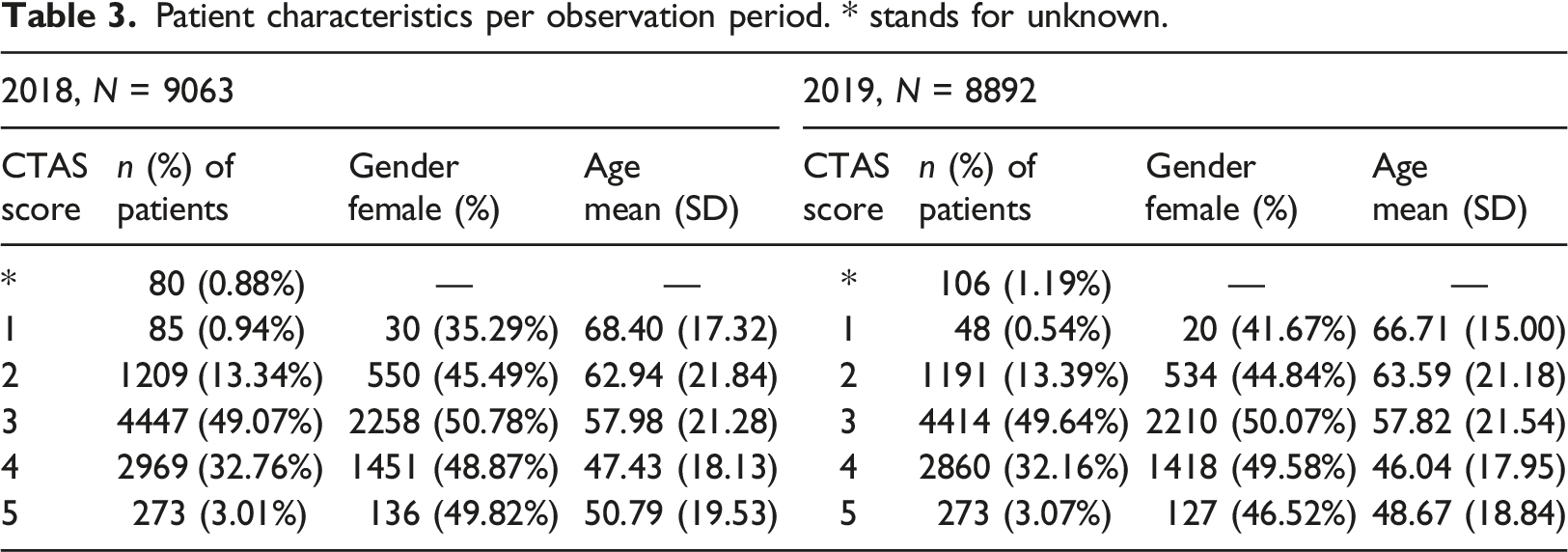
Electronic medical records provide data for age, gender, Canadian Triage and Acuity Scale (CTAS) score, ED volume, volume of ED patients requiring medical tests, LOS, APT, APTLR, and ERR. Age is registered as age at last birthday prior to arrival date. Gender is registered according to the patient’s declaration. Acuity is measured as CTAS scores assigned by the nursing staff in standard fashion (1 to 5), and maximum ED waiting time per priority category as shown in Table 2.
For purposes of analysis, age, gender, and daily ED volume are reported as means and standard deviations (SDs) for comparison. The gender data are reported as counts and percentage of female patients per level; and the CTAS scores as counts and percentages per level. A comparison of mean difference in patient volume per period and proportion difference of patients needing medical tests is performed using the t-test and Z-test, respectively. All statistical analyses are performed in Minitab®. 26
In the primary analysis, ATP and LOS are reported in minutes, and RP in terms of number of patients. Means and SDs (and medians with interquartile range (IQR) in the case of ATP and LOS) are included for purposes of comparison. The t-test is used for mean difference comparison of LOS, APT, and RP, and the Mann–Whitney U test is used for median difference comparison of LOS and APT; all other metrics are compared by proportion differences.
The secondary analysis uses regressions to control for patient and ED characteristics. Linear regression is used for LOS, APT, and RP, and logistic regression to measure improvement in APTLR. LOS is stratified by medical test requirement and immediate discharge following initial examination. CTAS scores are sorted by patient priority level (HP vs LP) for all regression models.
Results
Patient characteristics per observation period. * stands for unknown.
CA daily number of patients (8:00–21:00).
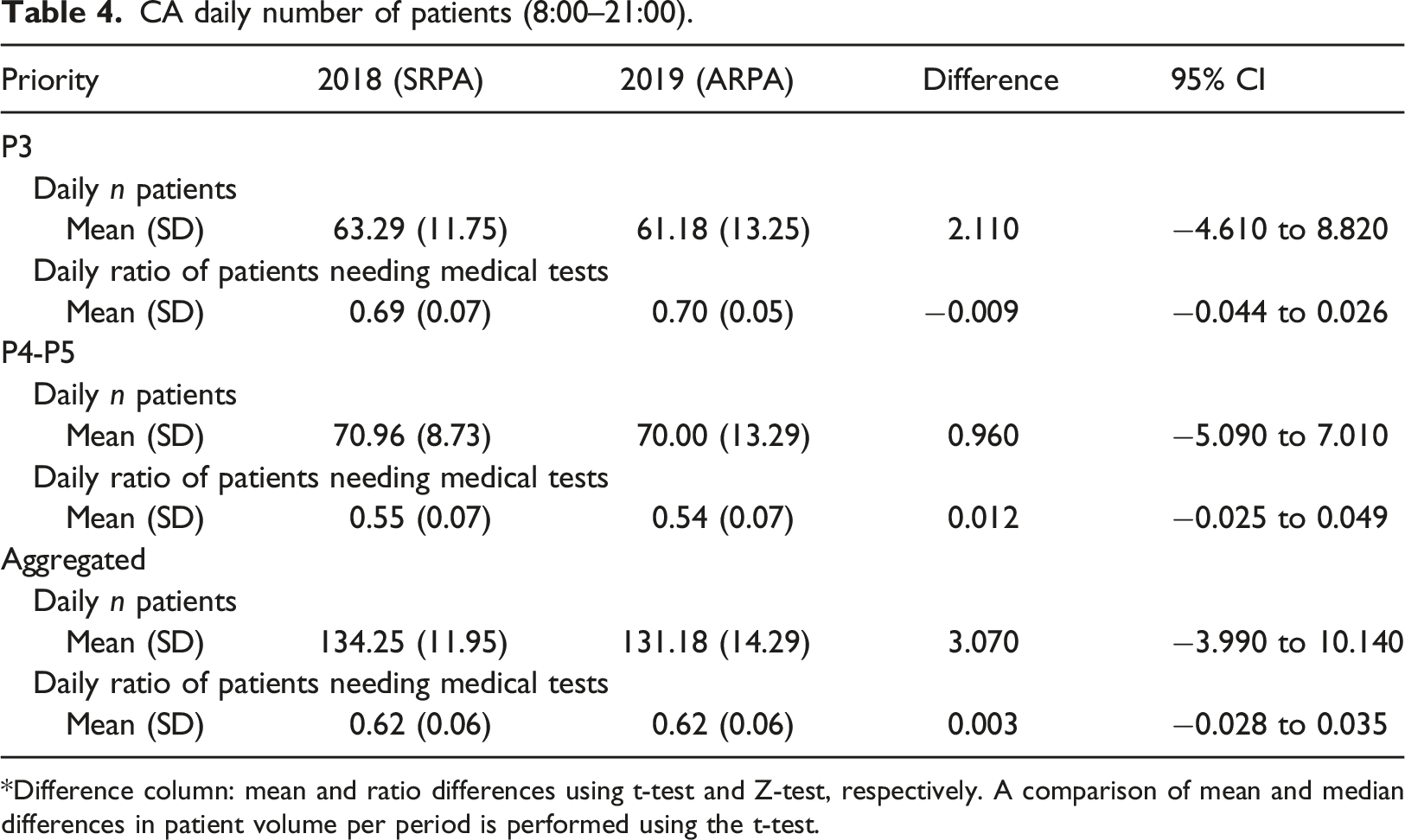
*Difference column: mean and ratio differences using t-test and Z-test, respectively. A comparison of mean and median differences in patient volume per period is performed using the t-test.
Patient and physician outcomes in CA.
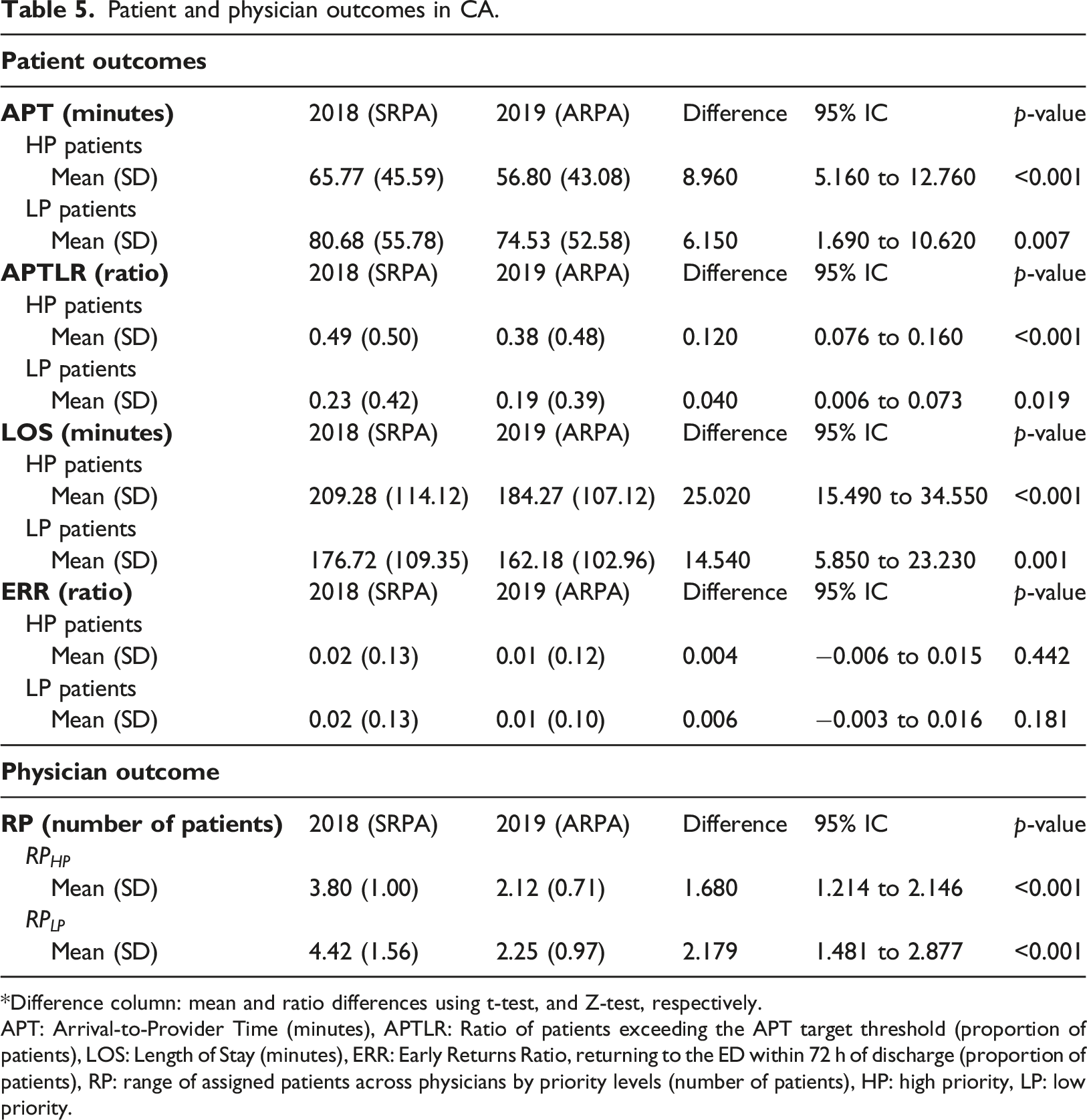
*Difference column: mean and ratio differences using t-test, and Z-test, respectively.
APT: Arrival-to-Provider Time (minutes), APTLR: Ratio of patients exceeding the APT target threshold (proportion of patients), LOS: Length of Stay (minutes), ERR: Early Returns Ratio, returning to the ED within 72 h of discharge (proportion of patients), RP: range of assigned patients across physicians by priority levels (number of patients), HP: high priority, LP: low priority.
The average ranges of HP patients for SRPA and ARPA are 3.80 and 2.12, respectively, which is, in both cases, significantly narrower (p < 0.001). The average ranges of LP patients are 4.42 and 2.25, respectively, which is again, in both cases, significantly narrower (p < 0.001). Note that a strict application of the ARPA patient-to-physician assignment method would lead to observed daily range values (and therefore, also mean range values) of no more than one. However, the collected results show values greater than one because the triage nurses may overrule the assignment algorithm because a physician is taking a long time over a very difficult case or the queue for a particular physician is being held up for some other reason. Even without 100% application of the rule, the improvement in the results is evident.
Regression analysis.
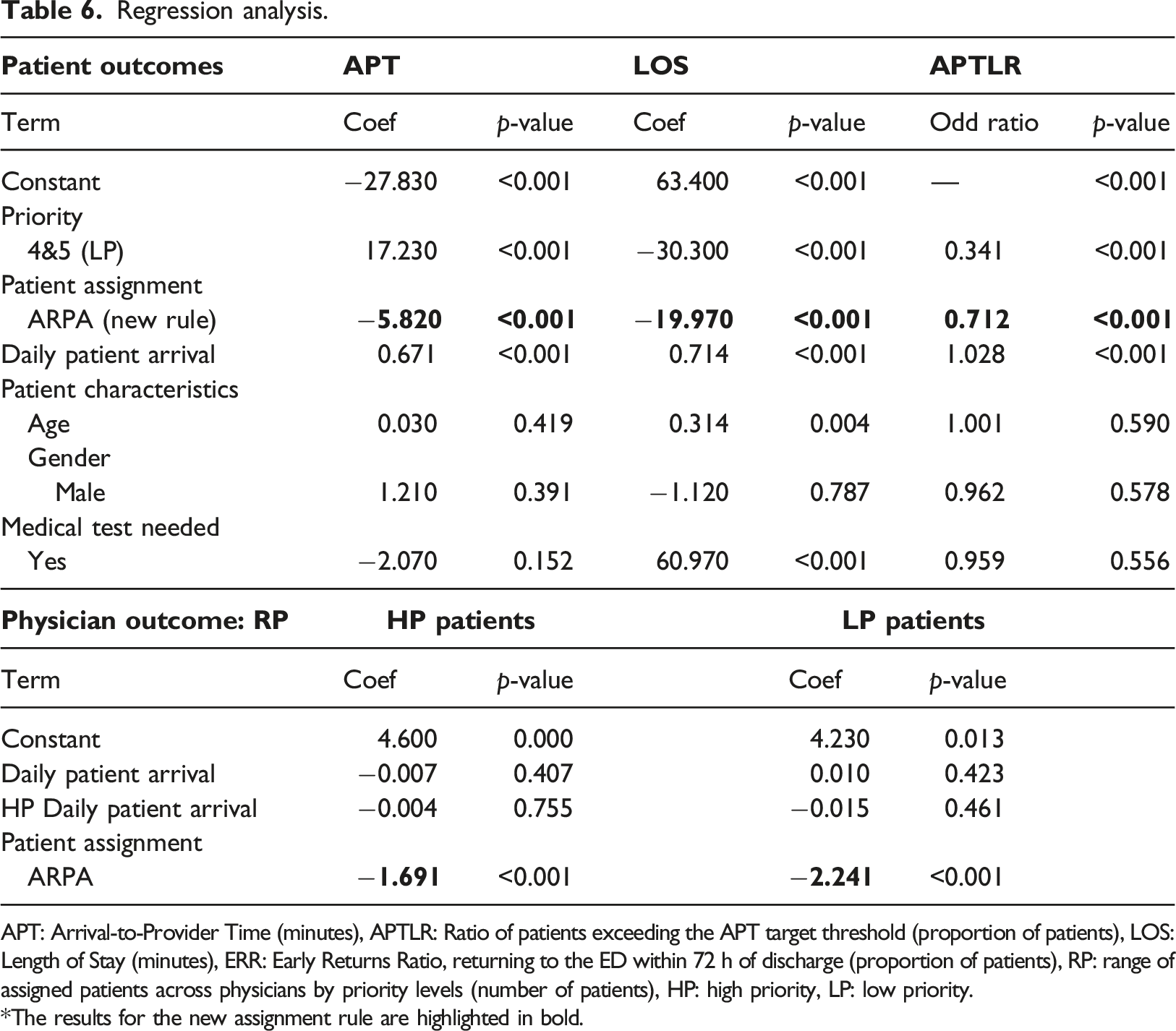
APT: Arrival-to-Provider Time (minutes), APTLR: Ratio of patients exceeding the APT target threshold (proportion of patients), LOS: Length of Stay (minutes), ERR: Early Returns Ratio, returning to the ED within 72 h of discharge (proportion of patients), RP: range of assigned patients across physicians by priority levels (number of patients), HP: high priority, LP: low priority. *The results for the new assignment rule are highlighted in bold.
Summary of survey responses. Frequency table.
Discussion
This research presents a new ED patient-to-physician assignment rule based on double rotational HP versus LP patient assignment. It controls variability in the number of HP versus LP patients assigned to each physician by ensuring that neither the total number of patients overall nor the number of HP versus LP patients per physician differs by more than one. This assignment system represents an improvement over the commonly used SRPA rule, which ensures an equal distribution of patients, day-to-day (or even patient-to-patient) but can lead to perceived unfair workload distribution due to randomness and marked differences in patient-acuity distributions between physicians.16,18–20 The medical staff of HCN, like physicians in other studies, 4 have complained about this issue.
Past studies of patient-to-physician assignment rules (some conducted prior to the universal adoption of electronic patient tracking,4,11–13 and others more recently) 17 support the transition from physician self-assignment to SRPA, based on significant observed improvements in some ED operational metrics: shorter APT12,13,16,17 and LOS.16,17 All previous studies demonstrate that the transition from the self-assignment of patients by physicians to the inflexible system of rotational patient assignment leads, counterintuitively, to efficiency gains. Heightened professional responsibility,11,12 patient ownership, 14 and equitable distribution of patients 12 have been reported as reasons for these results.
However, the uneven distribution of HP and LP patients also affects patient quality of care, because queues with more severe patients advance more slowly than those formed by the less severe. This queue dynamic can lead to situations in which some physicians are very busy while others are unoccupied. Some of the indirect effects of the uneven distribution of patient types are the lengthening of treatment access time and LOS and an increase in the ratio of patients whose time-to-treatment oversteps the target threshold.
In this research, we propose transition from the SRPA rule to the ARPA rule, which is designed to mitigate the problem of inequitable composition of patients queues across physicians, thereby also improving the operational patient treatment metrics. This intervention study describes the application of the new assignment rule in the less critical patient care circuit, CA, while the more critical patient care circuit, CB maintains the status quo. This is a replication of the experimental design found in other studies. For example, Hirshon et al. 4 describes the institution of SRPA for residents on the “medical side” of a “medical side/surgical side” ED at a teaching facility. The results of our intervention show that, in CA, several ED operational metrics improve while CB performance shows no significant change.
We assess the performance of both methods based on classic ED operational metrics (APT, LOS, APTRL) and a new metric to measure equity in workload distribution (RP) among physicians.
Our study finds that a patient assignment system taking patient priority into account is associated with a reduction in APT, APTLR, and LOS and a more equitable distribution of patient types across physicians. Meanwhile, statistical comparison of these metrics for CB patients under the SRPA rule reveals no significant difference between the two periods, and precludes rejection of the hypothesis of equal means (p-values >0.1).
In addition, equitable workload distribution reduces physician stress, 27 a serious work-related health risk, thereby preventing burnout.28–30 Methods for forecasting the total amount of workload in the ED1,31 help to reduce uncertainty, which is a stress-inducing factor. 27 This intervention achieves an objective reduction in the variation of the ratio of HP to LP patients per physician, and thus a better workload balance.
To the best of our knowledge, no other ED has implemented the transition from SRPA to ARPA or reported the observed benefits. Therefore, we are unable to compare our results and can only present them as a benchmark for future studies.
Other triage-related interventions to improve patient flow in the ED have been presented in the specialized literature. Oredsson et al. 32 reviewed these interventions and grouped them into streaming, fast track, team triage, point-of-care testing (performing laboratory analysis in the emergency department), and nurse-requested X-ray. The results of these interventions are not conclusive. For example, Parris et al. (1997) 33 concluded that no statistically significant reduction in transit time was demonstrated by allowing triage nurses to initiate X-rays, while Lindley and Finlayson 34 reported a 36% mean time reduction of 37.2 min (95% confidence interval 30.2 to 44.2, p = 0.000) from the time of triage to the time of treatment decision. A subsequent review by Elder et al. 35 concluded that advanced practice nursing roles, physician-assisted triage, and medical assessment units are models of care that can positively impact ED throughput. However, the most recent review by Freitas et al. 36 finds that the evidence supporting interventions to improve ED patient flow is weak and concedes that only the fast-track intervention has moderate evidence to support its use. Our study adds to this research by providing a simple intervention that improves both time-related KPIs for patient quality of care and physician workload balance.
The subjective views of nursing staff regarding this intervention (gathered by means of a survey conducted after the ARPA period) were positive; thus complementing the effectiveness of the method for balancing the workload and improving patient care quality. Their unanimous declaration of willingness to recommend the new assignment rule for use in the ED was reported to the hospital management team.
This is an observational study and, despite our attempts to account for multiple confounding variables, there is no guarantee that all key factors were incorporated into the regression model. We rely on system-generated data and, as there was no change in electronic data processing during the study period, we are confident that any flaws would likely be distributed equally across both periods. The number of admitted patients awaiting an inpatient bed may have an impact on medical and nursing care. This variable has not been directly considered in our study because no data were available. The LOS refers to time spent from patient admission to treatment decision, and not to the exit of the ED. In the case that patient acuity level correlates positively with the need for an inpatient bed, then balancing the distribution of patients by acuity also favours the distribution of bed-blocked patients among physicians. If no correlation exists, then bed blocking at the exit affects both management policies considered in our study equally.
Conclusion
This paper proposes and evaluates a real-world application of a new bidirectional acuity-based rotational patient-to-physician assignment protocol, labelled with the acronym, ARPA (Acuity-based Rotational Patient Assignment). Analysis of the collected data shows performance improvements in the circuit in which ARPA was implemented, while the circuit which maintained the simple rotational rule remains unchanged. ARPA is therefore appropriate for those EDs in which patients are allocated to physicians after triage. This assignment system enhances the SRPA and may serve as a useful model for EDs seeking to improve patient care, ED throughput, and medical staff workload balance. ARPA can be instituted with no need for extra nurses, physicians, space, or data collection; therefore its success does not depend on additional resource endowment. 1
Important factors in the introduction of new information technology are usefulness, impact, feasibility of usage and widespread acceptance by staff members. 37 The usefulness and impact of this methodological innovation have been demonstrated by the intervention described and statistical results presented in this paper; and its feasibility and acceptance by the results of a survey conducted on all the triage nurses who used the software during the intervention.
Supplemental materials
Supplemental materials - Acuity-based rotational patient-to-physician assignment in an emergency department using electronic health records in triage
Supplemental materials for Acuity-based rotational patient-to-physician assignment in an emergency department using electronic health records in triage by Marta Cildoz, Amaia Ibarra, and Fermin Mallor.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Ministerio de Ciencia e Innovación (MTM2016-77015-R (AEI, Spain, FEDER UE)) and Ministerio de Ciencia e Innovación (PID2020-114031RB-I00 (AEI, FEDER EU)).