
Abstract
People with multiple chronic conditions often struggle with managing their health. The purpose of this research was to identify specific challenges of patients with multiple chronic conditions and to use the findings to form design principles for a telemonitoring system tailored for these patients. Semi-structured interviews with 15 patients with multiple chronic conditions and 10 clinicians were conducted to gain an understanding of their needs and preferences for a smartphone-based telemonitoring system. The interviews were analyzed using a conventional content analysis technique, resulting in six themes. Design principles developed from the themes included that the system must be modular to accommodate various combinations of conditions, reinforce a routine, consolidate record keeping, as well as provide actionable feedback to the patients. Designing an application for multiple chronic conditions is complex due to variability in patient conditions, and therefore, design principles developed in this study can help with future innovations aimed to help manage this population.
Keywords
Introduction
Increased life expectancy around the world has resulted in a rising number of individuals with chronic diseases, as well as people with multiple chronic conditions (MCCs), which is the co-existence of two or more diseases.1–4 People with MCCs have complex health needs and often require the use of more health services.5–11 Seniors with three or more chronic conditions have nearly three times the number of healthcare visits than seniors with no reported comorbidities. 3 In Canada, seniors with MCCs account for 40 percent of healthcare use among seniors, even though they comprise only 24 percent of the senior population. 3 With the increasing prevalence of people with MCCs, it is important to identify alternatives to conventional patient management and monitoring in order to address their complex care needs while reducing costs.1,12
One way to help with the clinical management and self-care of patients with MCCs is through telemonitoring.13–16 Telemonitoring enables patients to collect and transmit physiological data (e.g. blood pressure and weight) from home to their healthcare providers.17–19 It can support self-management with automated self-care messages based on the physiological data. 15 While systematic reviews and meta-analyses have indicated improved health outcomes (e.g. reduced hospitalization) from telemonitoring,18,20–23 there are several studies including notable large-scale trials that have found no benefits from telemonitoring.19,24,25 Therefore, it appears that telemonitoring technologies have the potential to support patients in self-management and aid healthcare providers in clinical decision-making if designed and implemented appropriately. 26 However, these tools are often stand-alone solutions geared toward the management of single chronic diseases, such as diabetes, depression, and asthma. 27 Patients with MCCs have more complex requirements, have higher risks of adverse medication events, and can receive potential conflicting clinical advice from multiple providers responsible for individual chronic diseases, which hinders their ability to self-manage their conditions effectively. 28
The objective of this study was to identify the challenges of managing patients with MCCs and to use the findings to inform design principles for the development of a smartphone-based telemonitoring system tailored for these patients. The following chronic conditions were included in the study: heart failure (HF), chronic obstructive pulmonary disease (COPD), chronic kidney disease (CKD), diabetes mellitus (DM), and hypertension (HTN). These five conditions were chosen because (1) they are highly prevalent (including in combinations with each other) and (2) they are commonly targeted in telemonitoring studies due to the high potential benefit of telemonitoring of these conditions.3,6,17,29–31
Methods
This was a qualitative study using semi-structured interviews with patients with MCCs and clinicians with expertise managing patients with MCCs. The study was approved by the Research Ethics Boards of University Health Network (#13-7085-BE), North York General Hospital (#14-0017), and Mount Sinai Hospital (#14-0075-E).
Participants
Patient recruitment
Patients for the semi-structured interviews were recruited from Family Health Teams (primary care organizations that comprise a team of family physicians, nurse practitioners, nurses, social workers, dieticians, etc.) at three hospitals (University Health Network, North York General Hospital, and Mount Sinai Hospital) through referrals from physicians and nurse practitioners. A convenience sampling technique was used to select participants with the following characteristics: 18 years or older, ability to communicate in English, ability to give informed consent, and diagnosed with any two or more of the specified chronic illnesses (HF, COPD, CKD, HTN, and/or DM). The family physician or nurse practitioner, who identified an eligible patient during a regular clinic visit, introduced the research study to the patient and asked if the patient would be interested in meeting with the Study Coordinator (M.S.) to discuss the study further. Interested patients met with the on-site Study Coordinator to obtain details of the study and provide informed consent. Patients agreeing to participate in the study were interviewed immediately before or after their clinic visit depending on their availability.
Clinician recruitment
Clinicians recruited for the interviews were medical specialists from tertiary clinics for the specified chronic conditions and family physicians, nurses, or pharmacists from the Family Health Teams involved in the treatment of patients with MCCs. Clinicians were sent an email with information about the study to ask them if they would be willing to participate in an interview. Written consent was obtained prior to commencing the interview sessions.
Study procedure
The Study Coordinator conducted the interviews individually with each patient and clinician in a private meeting room (i.e. meeting room in the local clinic, office, or other convenient location). Patients were asked to complete a pre-study questionnaire prior to the interview in order to provide demographic information. Each interview was between 45 min and 1 h in duration, and was audio recorded and later transcribed. The Study Coordinator also took notes during the interviews and collected samples of documents such as sample patient medication lists.
The patient interview guide was adapted from a guide used previously for research with older adults with MCCs in primary care settings.11,28,29 The interview guide included questions on patients’ goals and challenges pertaining to managing multiple health conditions including their medications, treatments, symptoms, and care provided by different healthcare providers. Questions on telemonitoring and use of technology were added in order to understand the patients’ comfort with using mobile phones and computers. The clinician interview guide included questions to explore clinical requirements for health conditions, complications faced during treatment of patients with MCCs, and their thoughts on the implementation of telemonitoring. Conventional content analysis, a type of qualitative research technique, was conducted to derive insights from the interview data. 32 The health belief model (HBM) was utilized to frame the perceptions of the participants and identify barriers and motivational factors that could be utilized in designing a system for self-management of MCCs. 33 However, the analysis was not constrained to any particular construct of the HBM and the data were categorized freely to identify barriers and motivational factors. The Study Coordinator and an additional reviewer independently determined the themes through the review of the transcripts and then later discussed the themes until a consensus was reached. Additional participants were interviewed until saturation of information was achieved (i.e. when no new information was being gained through additional interviews). Design principles for a telemonitoring system were then developed to address the challenges identified in the themes. User-centered design principles were finalized through an iterative process, leveraging the team’s previous experience in developing smartphone applications for management of single chronic conditions. Specifically, each challenge was analyzed to determine if it could be mitigated during the design process. The methods of addressing these challenges were then combined to develop design principles. The design principles were then discussed with the research team to iteratively refine them.
Results
Participant demographics
A total of 15 patients were interviewed. Of the five targeted chronic conditions (i.e. HF, COPD, CKD, HTN, and DM), a total of 5 patients (33%) had three of the conditions, while the remaining 10 patients (66%) had combinations of two of the conditions (Table 1). Other commonly reported conditions such as arthritis, asthma, Crohn’s disease, and depression were also prevalent.
Demographics of patients participating in interviews.
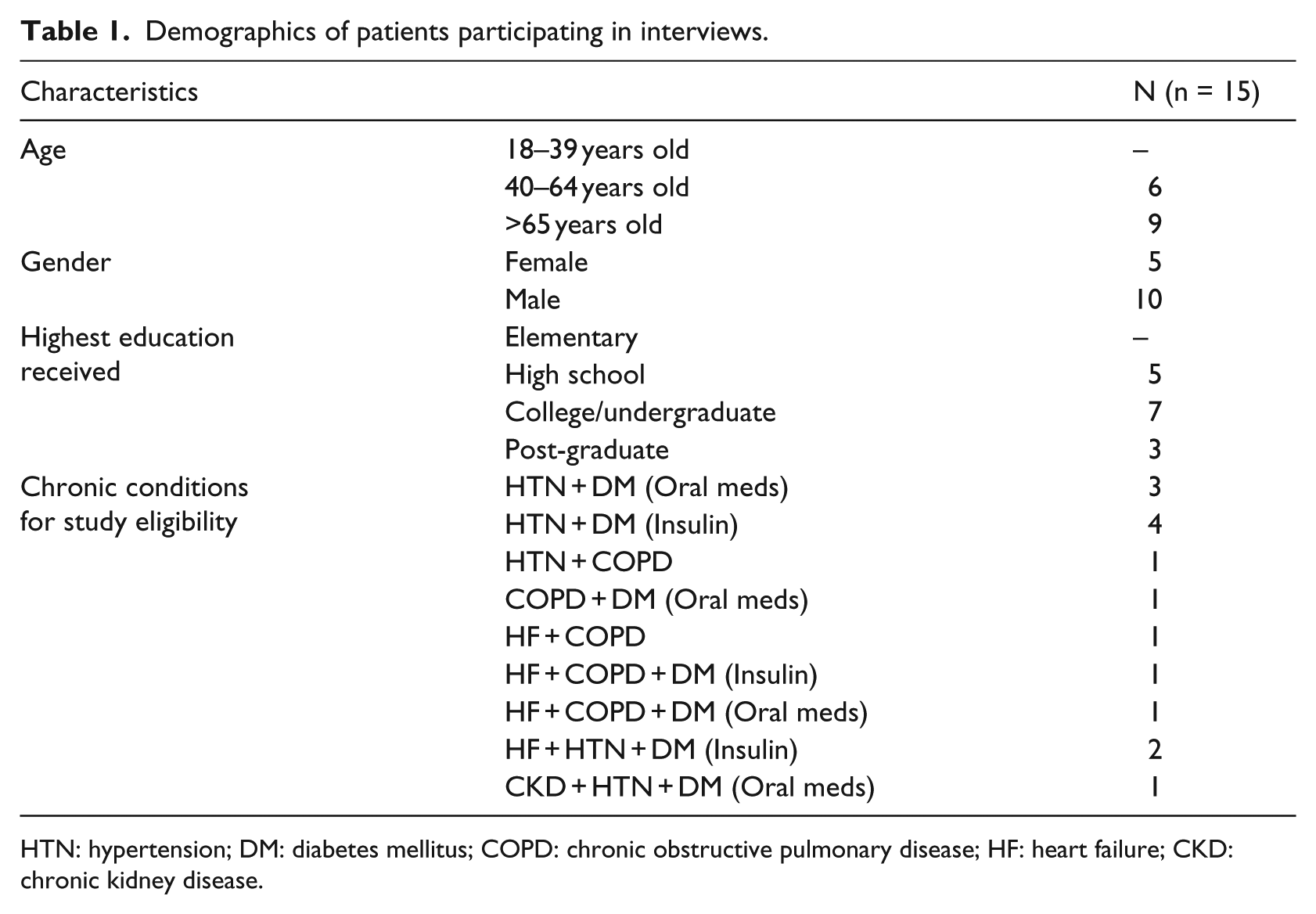
HTN: hypertension; DM: diabetes mellitus; COPD: chronic obstructive pulmonary disease; HF: heart failure; CKD: chronic kidney disease.
In total, 10 clinicians participated in semi-structured interviews. Two clinicians were specialists from tertiary clinics, one in HF and the other in COPD. One clinician was a pharmacist from a CKD clinic. Six of the clinicians were primary care physicians, and one was a nurse from a Family Health Team.
Themes
Six themes were identified in the interviews with patients and clinicians.
Theme 1: each patient has unique needs
Clinicians identified that different parameters should be monitored for different chronic conditions. For example, for self-management of HF, the main factors were changes in weight, blood pressure, and symptoms. For DM, the most important factors were blood glucose levels, health behaviors, and maintaining a diet appropriate for people with diabetes. In addition, the need for self-monitoring by patients differed depending on the severity of their conditions. Patients who were part of tertiary specialized clinics generally had the most severe conditions, and therefore required more frequent monitoring. For example, a clinician from a tertiary clinic stated, Patients who come to our clinic are sicker so they need closer monitoring. Stage 1 patients, they don’t come to our clinic. They go to see general nephrologist, they could use maybe a lighter version [of the smartphone application] because these patients in the earlier stages don’t need the close monitoring. However they could benefit from the education about things that they can do on their own. They won’t be too dependent on this app. (Clinician 1, CKD Clinic)
Clinicians believed that patients in primary care clinics in contrast mainly had milder forms of chronic conditions and thereby required minimum home monitoring: Primary is responsible for the totality of their health. In primary care, they have a milder form of all the diseases. At primary care we will have more people in the mild levels and fewer in the severe levels. Prevent the mild from getting more severe, because there wouldn’t be a large application at the primary care level if you focus on the advanced level of any of these conditions. (Clinician 2, Primary Care)
Patients supported this theme by highlighting that telemonitoring requiring frequent monitoring would not be useful for their milder forms of the chronic conditions because they were not currently required to measure their parameters at home. Aside from some patients with diabetes who monitored their blood glucose daily (i.e. those who required insulin), only one other patient took daily measurements because of advanced HF. The variance in required self-care practices demonstrated that patients with MCCs have unique needs based on the combination and severity of each of their conditions.
Theme 2: support for healthy lifestyle habits is required
Patients expressed difficulties with maintaining or establishing healthy lifestyle habits, but at the same time many also expressed their commitment to trying to do so because it was important for preventing the health conditions from worsening. Maintaining a proper diet was one of the most problematic self-management behaviors due to factors such as having to limit foods high in salt or carbohydrates, eating at the right times, breaking old established eating habits, boredom from maintaining a healthy diet, or not having enough information on a proper diet. Few patients also faced financial constraints that limited purchasing of healthy foods. Clinicians corroborated that diet management was not isolated to any one particular health condition. Patients were trying to maintain healthy diets for multiple common health conditions such as diabetes, cardiovascular disease, HTN, dyslipidemia, and obesity.
Physical activity and weight control were also seen as beneficial across multiple conditions, with some patients making an effort to integrate exercise into their schedules: I lost 25lbs. I eat healthy, exercise—walk 30 min to 40 min every day. I started this 1 year ago. I consciously made the effort to change. (Patient 10)
However, many patients were limited in their abilities to establish healthy lifestyle habits due to pain and physical limitations. One 79-year-old female patient, for example, had limited mobility due to diabetic neuropathy as well as arthritis. Another 81-year-old female patient stated, “I can’t exercise. I have osteoarthritis. They did advise me to walk, but I can’t. I get half a block, and it gets so painful.” Examples such as these illustrate that physical activity, though required for maintaining a healthier lifestyle, could often times be limited or prevented due to situations such as pain in joints from arthritis, pain in feet from neuropathy, or low endurance and fatigue.
Theme 3: routines for self-management activities need to be established
Patients who had developed routines and had managed to figure out self-management strategies fitting their lifestyles appeared more adherent to self-care practices. Routines helped patients both remember and carry out self-management behaviors efficiently by making day-to-day decision-making easier. For example, patients would perform the same physical activity regularly or follow a daily diet plan. However, a routine was established only after patients had been able to organize their self-management activities: “I’m trying to organize and it’s become a routine … But perhaps before the routine, you have to figure out how to and everything” (Patient 4). In particular, medication adherence was reported to have improved for patients who had their complex medication regimen organized according to the time of the day. Some patients with developed routines also learned to plan ahead, for example, by ensuring they took their required medications during their travels: “I use pillboxes. I concentrate and put 7 days of pills. If I go out [travelling], I make for 2 weeks. I have another one readily available if I run out” (Patient 4).
Theme 4: consolidating health information is burdensome
During interview sessions, patients were observed to be carrying multiple loose sheets of paper containing items such as list of medications, health conditions, measurements, and some had a mix of electronic and paper records which they carried with them to their clinic appointments. Record keeping was further exacerbated by patients’ health information scattered across different providers and facilities: “I’ve got multiple doctors for medications” (Patient 10). Patients often encountered problems keeping proper record of their measurements, with records getting misplaced and lost: But to take a record is frustrating. I take blood sugar, but it’s missing. [Patient shows her blood sugar logbook]. I took the reading and didn’t put it right away for any reason, and I really don’t know what it was. It’s missing. (Patient 4)
Some patients did not know their medical history well, such as one 83-year-old patient who was unaware that he had COPD and HF but knew that he sometimes had difficulties breathing and is taking medications for a heart condition. Most patients, especially those with milder conditions were reluctant to spend time monitoring and recording their health information, preferring to “have as little intervention as possible” (Patient 1) in their daily lives. Clinicians corroborated that patients should not be overburdened and should only be required to record “a couple of major markers, not a lot” (Clinician 7) by determining what data patients can collect by themselves at home and what data can be collected from external clinical databases.
Theme 5: patients need clinically accurate and actionable feedback
For many patients, the journey into self-management can start with education and learning the technical skills related to their specific conditions. Most patients found their healthcare team to be a great source of information and teaching, but also sought information and help from their family and friends, as well as from the Internet and books. However, as one clinician pointed out “many patients will Google information which is not always correct or accurate” (Clinician 2). Therefore, it is important to ensure that patients are provided with clinically validated information.
Multiple clinicians also emphasized the importance of teaching patients to be aware of changes in symptoms and measured parameters, and learning to take appropriate actions: It’s an understanding of the changes of their symptoms, alert them to notify us. Having an action plan and knowing how to act is important. Most people would be a milder situation, where they can contact us, talk to the nurse in the urgent basis, and then you can decide where to go—appointment, ER, etc. (Clinician 9)
Clinicians saw potential in using a smartphone application to provide actionable feedback to the patients, referring to the smartphone application as a “teaching opportunity” (Clinician 5). However, ensuring patients with MCCs are provided with correct information and feedback is complicated by the fact that these patients usually see multiple healthcare providers, and different healthcare providers have different treatment preferences based on what they consider to be more important. Providing appropriate actionable feedback is further complicated by the lack of established guidelines for clinicians to follow in providing care for different combinations of health conditions. Furthermore, treatment for one health condition could cause exacerbation of another condition, leading to patients receiving conflicting advice: How we deal with diuretics is very different. HF clinic would dose very aggressively. We however won’t because it will make the kidneys dry up too much … In those cases, between HF and CKD clinics, we have to determine who is taking over. If HF takes over, then CKD won’t touch the diuretic medications. We have fair amounts of those types of patients. Even conflicting advice about diet—healthy heart diet would say to eat whole wheat and incorporate fruits and vegetables. In contrast, CKD requires white everything, no fruits, no vegetables. Patients are left confused. What are we supposed to follow? (Clinician 1)
Therefore, a general understanding expressed by all clinicians was the need for resources that can help reduce conflicting advice.
Theme 6: communication and clinical integration must be efficient
Patients with MCCs often receive care from multiple clinicians, who may work independently from each other, resulting in fragmented and poorly coordinated care for the patients. Each of the clinicians may provide one or more of the services that comprise the full spectrum of care the patient needs, such as medical, mental health, rehabilitation, prevention, and supportive services. Most of the interviewed patients had the impression that their clinicians were communicating efficiently with each other regarding the patient’s care.
However, clinicians often identified that communication pathways between the different care providers were suboptimal. In particular, specialists wanted the family physicians to be more aware of the changes in the patients’ care plan. Similarly, family physicians were dissatisfied with the lack of proper communication by the specialists. By functioning as separate entities, the clinics often do not have complete information about the patient’s condition or treatment history.
Patients and clinicians were supportive of having a telemonitoring system with an automatic real-time alerting system that would notify healthcare professionals of deterioration in a patient’s condition, with alerts enabling clinicians to be proactive instead of reactive to the patient’s conditions: Measuring of vitals and weight and have alerts when we are concerned, for example for increased weight gain or blood pressure elevations that would be useful. (Clinician 2)
However, clinicians were concerned about managing a high volume of alerts and determining which clinician(s) will be responsible for managing the alerts: “I worry a lot about when the alerts will get sent and if this is going to happen in business hours or outside business hours. What happens when they feel symptoms at 3am?” (Clinician 3). One primary care physician stated that their clinic already had on-call physicians and alerts generated through a telemonitoring smartphone system “will just replace one sort of workflow with another. So instead of getting phone calls from the patients, I’ll get alerts from those patients.” Understanding the workflow of the clinics would be imperative for efficient integration of a telemonitoring system and communication of information between patients and clinicians.
The themes identified through the interviews provided insight into design principles for the smartphone-based telemonitoring system for patients with MCC. Table 2 summarizes the design principles that were generated from each theme.
Findings and resultant design principles.
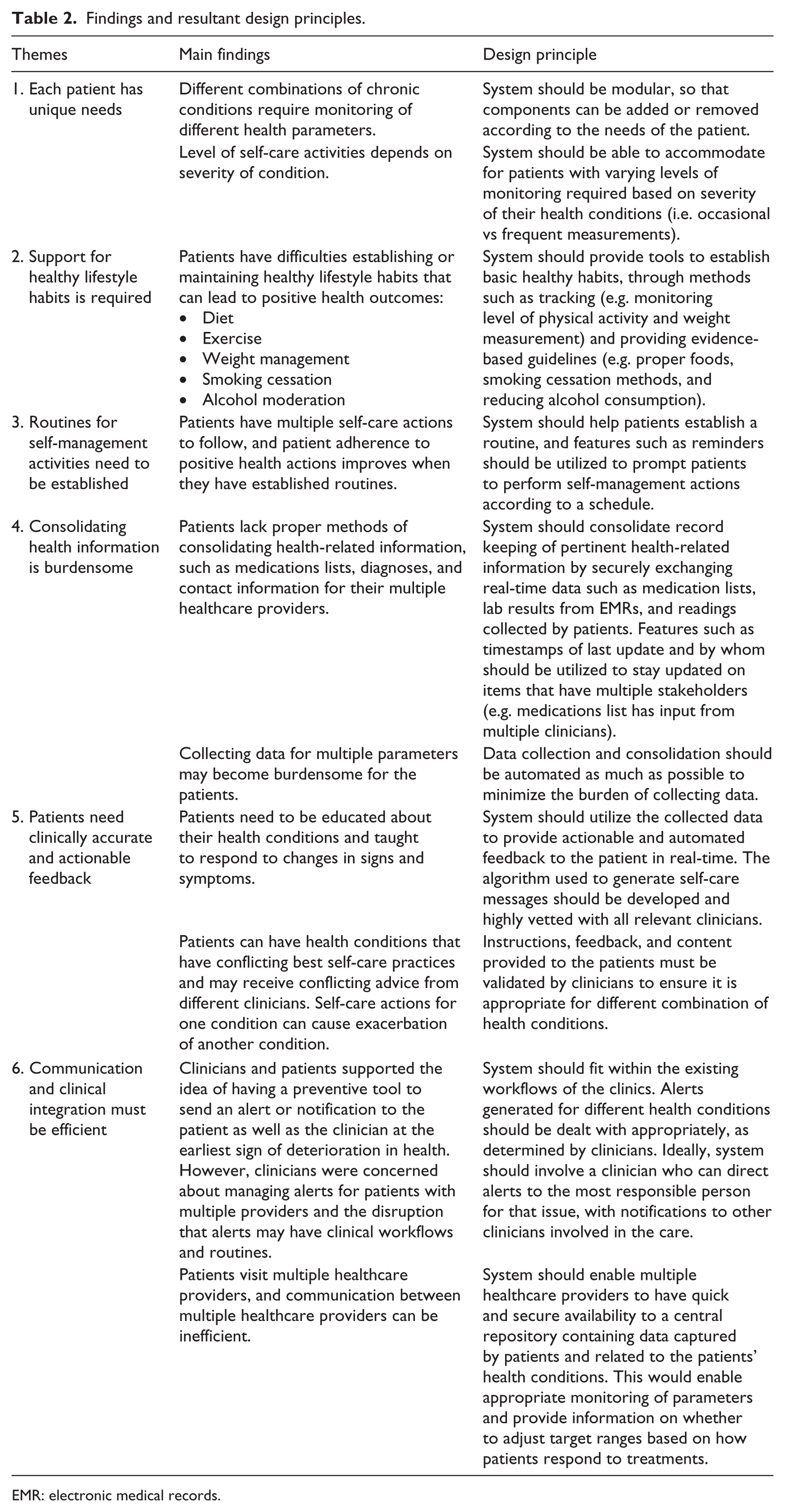
EMR: electronic medical records.
Discussion
This research sought to understand the complex challenges of patients and clinicians in managing MCCs. The challenges identified were then used to generate design principles. The implications of the themes and design principles to the development of the telemonitoring system are summarized below.
Tailoring to the unique needs of the patients
Patients with MCCs experience barriers to self-care due to the simultaneous and competing demands of their conditions. Additionally, the self-care support needed among the patients varies with the combination of chronic conditions and severity of the conditions. Therefore, an intervention aiming to help patients with self-management should be tailored to the unique needs of the patient. Telemonitoring studies have shown to be successful if the target patients are severely ill and frequently hospitalized.25,30,34,35 Thus, one option could be to develop modules for the telemonitoring system based on the severity of the conditions. For the severe group of patients, the application should concentrate on frequent monitoring and prevention of adverse events by alerting the patient and clinician(s) about abnormal parameters. For the mild to moderate group, the focus should be toward establishing healthy lifestyle behaviors as well as pain and symptom management without requiring daily data collection because frequent monitoring would be unnecessarily burdensome for patients with mild severity (e.g. controlled HTN and early stage CKD).
It should be noted that irrespective of the severity of their health conditions, establishing healthy lifestyle habits, especially diet and exercise, was found to be a challenge by each patient interviewed in this study. Therefore, one generic module to guide patients through a process of behavior change that could lead to healthy lifestyle habits and appropriate management of their illnesses would be beneficial. However, this module must allow for tailoring based on health conditions, for example, to ensure patients receive proper information on diet based on established guidelines for their health conditions (e.g. CHF compared to CKD).
Attaining a routine is key to setting a foundation for self-management. 36 Therefore, the smartphone application should guide patients through tasks such as completing their measurements and taking their medications based on certain established schedules determined by clinician/patient preferences. Having consistent times with reminders in place may reduce the cognitive demands of having to remember to take self-management actions. 37
Providing patients with disease-specific instructions
Multiple clinicians in this study cited lack of established guidelines to be a barrier in providing care for patients with MCCs. Clinical guidelines and disease management programs have predominantly focused on single diseases.11,12,38,39 Guidelines for management of MCCs are important in developing algorithms for a smartphone-based system aiming to provide actionable feedback to patients upon input of reading parameters (e.g. blood glucose, blood pressure, and weight) and symptoms. Smith et al. 40 reviewed the effectiveness of multiple interventions and concluded that interventions are more effective if they either target specific combinations of common conditions (disease-specific) or specific problems of patients with MCCs. Disease-specific algorithms provide an opportunity to guide patients on specific actions required for each of their diseases, such as specific instructions on what to do for COPD exacerbations or specific instructions about diuretic medications for HF based on significant changes in weight over a short period of time.31,35
However, the complexity in disease-specific instructions arises when the same reading parameter is addressed differently for different conditions. For example, blood pressure is one of the determining factors for HF, CKD, and HTN,35,41,42 and disease-specific algorithms may require different instructions based on changes in the parameters, as described in Theme 5. Therefore, disease-specific instructions may be appropriate for an application for patient’s with MCCs only if instructions and recommendations are tailored to clusters of diseases.12,39
Viewing of telemonitoring data by clinicians
By functioning as separate entities, primary and tertiary care clinics often do not have complete information about the patient’s condition or treatment history. However, a web-based dashboard integrated with existing EMRs can be used to securely exchange real-time data such as medication lists, lab results, and readings collected by patients, thereby enabling seamless communication among clinicians and interconnecting data between patients’ smartphones and clinicians. The dashboard could further enable clinicians such as a complex care nurse to triage alerts and notifications generated, providing the opportunity to better manage the patients’ conditions. Having a nurse managing telemonitoring patients has been observed in multiple randomized controlled trials with positive outcomes.42–44 Nurses or nurse practitioners in primary care clinics could be in the ideal position to work in partnership with tertiary clinicians for effective communication and management of patients with MCCs across the care continuum. 35 The web-based dashboard included as part of the smartphone-based telemonitoring system would therefore be able to reduce fragmentations and enable better decision-support capabilities that can assist patients in managing chronic conditions.
Limitations
Patients were recruited from clinics that were well-established and had allied healthcare incorporated into the care system. The clinics and clinicians participating in this study were highly engaged in management of their patients and also experienced in facilitating research studies, and hence, there could be a bias as to why most patients were satisfied in the information exchange and care provided by their healthcare providers. It is possible that the findings from this research may not be transferable to other patient populations, such as those who live in rural areas or have limited access to healthcare providers.
Conclusion and future directions
Designing an application that is tailored to the needs of patients with MCCs is complex due to variability in conditions and lack of comprehensive evidence-based guidelines for management of patients with MCCs. The design principles identified in this research can be used to inform the development of a patient-centered smartphone telemonitoring application that specifically addresses the challenges associated with managing MCCs. The development of the application should include patient and clinician involvement throughout the process to ensure their needs and preferences are met. While the design principles were created to help inform the development of a telemonitoring system for patients with MCCs, they also may be applicable in the development of other innovations aimed to improve clinical management and/or self-care of patients with MCCs.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/orpublication of this article: Funding support for this research was provided through a partnered grant between the Natural Sciences and Engineering Research Council of Canada Strategic Research Network–entitled Healthcare Support through Information Technology Enhancements (hSITE) and Research in Motion.