
Abstract
Objective
To provide practical information regarding needs, preferences of content and format of an app to assist the self-management in patients with multi-morbidity and heart failure (HF).
Methods
The three-phase study was conducted in Spain. Six integrative reviews, a qualitative methodology based on Van Manen's hermeneutic phenomenology through semi-structured interviews and user stories were used. Data collection continued until data saturation was reached. All data were transcribed verbatim and analysed using a framework approach. Thematic analysis technique following the methods of Braun and Clarke was used for emerging themes.
Results
Integrative reviews conducted included practical recommendations to include in the content and format of the App and helped create the interview guide. Interviews revealed 15 subthemes that captured the meaning of narratives offering contextual insights into the development of the App. The main effective mechanisms of multicomponent interventions for patients with HF must contain (a) components that increase the patient's understanding of HF, (b) self-care, (c) self-efficacy and participation of the family/informal caregiver, (4) psychosocial well-being and (5) professional support and use of technology. User stories revealed that patients prioritized improvements in direct contact with health services in case of emergency (90%), nutritional information (70%), type of exercises in order to improve their physical condition (75%) and information about food and drug interaction (60%). The importance of motivation messages (60%) was highlighted by transversal way.
Conclusions
The three-phase process integrating theoretical basis, evidence from integrative reviews and research findings from target users has been considered a guide for future app development.
Introduction
Increased life expectancy, as well as socio-economic improvements and biomedical innovations, has led to a demographic ageing of the population. On the other hand, this implies a considerable increase in chronic conditions, where the patient with multi-morbidity emerges as the great epidemic of the 21st century. Multi-morbidity results in poorer health outcomes and leads to greater disability and poorer quality of life. 1 Although there is a growing interest in patients with multi-morbidity, from an evidence perspective, this population has been excluded from most clinical trials and intervention studies. 2
Among patients with multi-morbidity, heart failure (HF) is a major health challenge. HF is becoming one of the diseases with the highest incidence rate in the world. 3 In the United States, it affects ∼6 million Americans, with prevalence expected to increase by 46% and direct medical costs to reach $53 billion by 2030, 4 and will increase as its prevalence increases. 5 Similar results have been reported in the European context estimating that 30–40% of HF patients have a history of HF hospitalization, which in turn is associated with a worse prognosis and a high health burden. 6 In Spain, HF is also a huge health challenge (it is estimated that there are more than 1,300,000 people with HF) and the mortality rate is very high; every year more than 17,000 people die from this disease, being the fourth cause of death in this country, 7 with 50% dying within 5 years of diagnosis. In addition, HF is the first reason for hospitalization in people over 65 years of age. Reducing readmissions is a priority; it is estimated that 50% of readmissions could be avoidable, 8 although the reality is that continuity of care for these patients is minimal.
The main HF guidelines recognize the importance of patient self-care for the control and management of the disease. It is necessary for the patient to acquire healthy lifestyle habits and adhere to treatment to improve their quality of life. 9 To promote self-care and provide health education, there are various methods, including mobile health applications (mHealth). 10 To date, mHealth studies have been published in which behavioural interventions have led to an improvement in the management of chronic diseases.11,12 They appear to be an effective tool in the care of these patients 13 and specifically in patients with heart disease. 14
The incorporation of telehealth systems in the care of these patients is highlighted by different scientific societies, as revealed by the European Society of Cardiology15,16 and the American Heart Association. 17 They not only provide improvements in disease management but also facilitate social communication. 18 Apps can also serve to improve adherence through automatic alerts or notifications or graphical progress tracking devices. 19 However, they appear challenging for elderly patients because of potential digital health literacy barriers. 20
To facilitate the use of these mobile applications and thereby improve adherence and self-care, the design must respond to the needs of users, offering quality and personalized attention. 21 However, few studies have taken into account the patient perspective and their incorporation into clinical practice in the development of these mHealth tools. 22 In addition, the proliferation of these apps has not been accompanied by the growth of a good design methodology for it. 23
Background
Theoretical foundation provides guidance on the development of behavioural mHealth intervention. 24 According to the theory of self-care in specific HF situations, the factors that have the greatest impact are knowledge about the behaviours to follow for self-management of care (84%), experience with health professionals (84%), beliefs about their experience (69%) and habits related to taking medication (72%). 25
Perceived control is a positive factor in improving self-care, and a decrease in it is associated with poorer outcomes. Interventions to reduce psychological distress combined with self-management support could have a beneficial impact on patients who decrease or persist in poor self-management behavior. 26 However, according to systematically conducted studies on self-care status in HF patients through the Heart Failure Self-Care Index scale, despite the high heterogeneity of the studies, the results indicated that self-care practice is inadequate in all three dimensions of self-care (that is, maintenance, management and trust). 27
Conceptual framework
User-centred design is a well-established approach to develop a mobile app. This design is strategically important because of its insights on users and their context of use. 28 Advantages of user-centred design include the promotion of autonomy, competence, positive emotional experience and sense of relatedness for users. 29 User-centred design focuses on the target audience through an iterative design process that engages users in conceptualization, design and development of an app. 30 User involvement increases appeal and user-friendliness. 31 Target population can select tailored information about their preferred form, which is essential to maximize the acceptability and effectiveness of interventions. 29
Therefore, user stories used in development methodologies are an agile tool to establish user acceptance goals. A user story describes a functionality that will be valuable to a user or purchaser of a system or software. It is a semi-structured description in natural language from the user's perspective of the functionality of the required software system. 32 Thus, user stories help stakeholders share an understanding of the goals and intended functions of the system.33,34
As highlighted by Schnall et al., 28 the Information Systems Research (ISR) approach is potentially useful for designing a mobile app that incorporates the design preferences of end-users. This process consists of three cycles: relevance, rigour and design. In the first cycle, focus groups are conducted with end-users to understand the needs of the target population. In the rigor cycle, a review is conducted to identify technology-based interventions to meet these needs. In the ISR design cycle, usability evaluation methods are used to iteratively develop and refine mock-ups of a mobile health app.
Thus, the aim of this study was to provide practical information regarding needs, preferences of content and format of an app to assist the self-management in patients with multi-morbidity and HF.
Data and method
Design
Following the ISR approach, we used a three-phase process (Figure 1). Although initially the project was designed to conduct focus groups of patients, due to the epidemiological situation caused by COVID-19 and the limited restrictions, the order of the phases was inverted and it was decided to conduct semi-structured interviews.
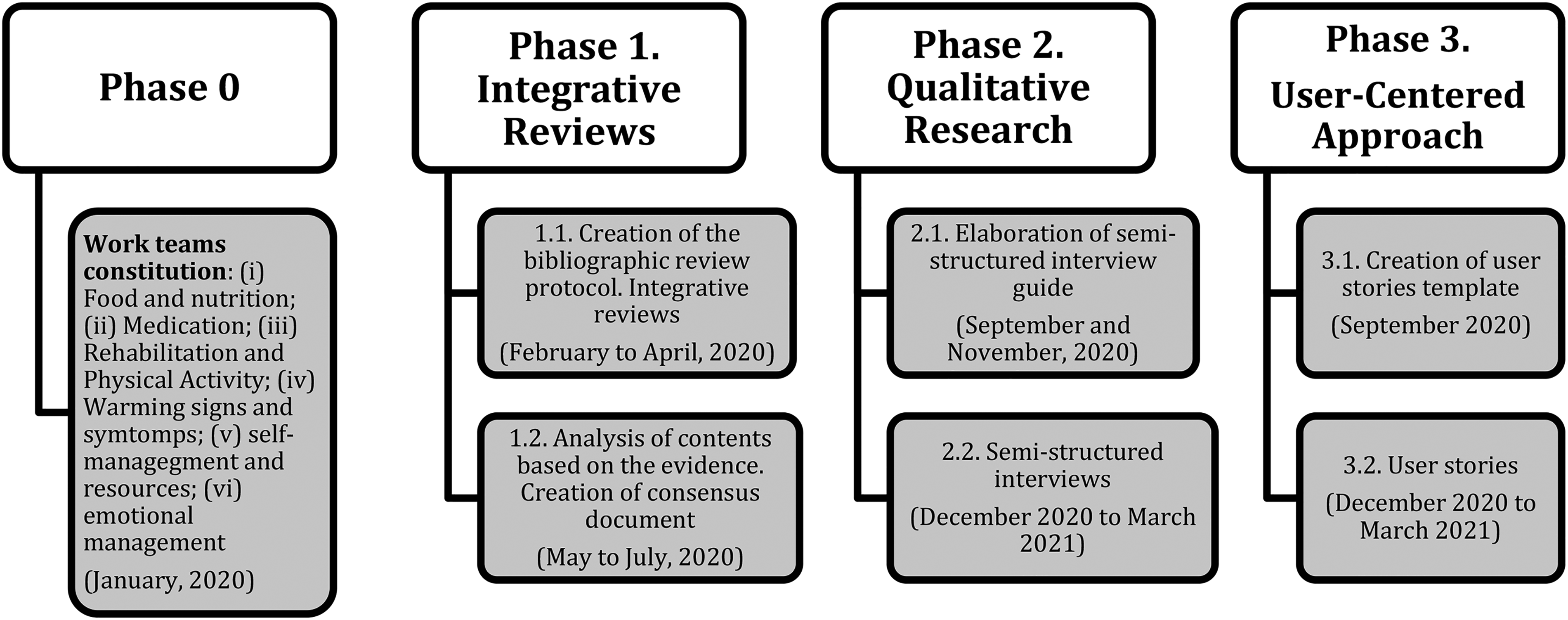
Methodological design phases.
In the first phase, integrative reviews were conducted in order to identify intervention proposals to promote the autonomy/self-management of the patient with multi-morbidity and HF. Secondly, a qualitative methodology based on Van Manen's hermeneutic phenomenology 35 through semi-structured interviews was used in order to identify the needs from our target users. Finally, in the third phase, a user-centred approach (their opinions and experiences) was conducted though user stories. The importance of this research design for the development of a mHealth app focused on people with comorbidities has been demonstrated. 36
The consolidated criteria for reporting qualitative research (COREQ) was used to ensure the quality of the procedure for creating a mHealth App aimed to people with multi-morbidity 37 (see Multimedia Appendix 1).
Setting and participants
The study was carried out within the framework of the project ‘Development and Effectiveness of a Mobile Health Intervention in Improving Health Literacy and Self-management of Patients With Multimorbidity and Heart Failure: Protocol for a Randomized Controlled Trial’ (Trial Registration: ClinicalTrials.gov NCT04725526), whose aims are (a) to develop an app based on the needs of users and deficiencies identified by professionals, which motivates behaviour change through gamification strategies, as per scientific evidence and adapted to the users level of health literacy, and (b) to test its effectiveness in terms of self-management and improvement of personal autonomy to perform basic activities of daily living, reduce hospital admissions, promote therapeutic adherence and increase health literacy. 38
This study was conducted in four basic health areas and two hospitals located in the province of Cadiz (Andalusia, Spain). A non-probabilistic convenience sampling was carried out of patients with multi-morbidity and HF and complex health needs attended by the nurse case manager of the primary care or hospital care centres, nurse or family doctor, specialized care nurse, area specialist physician of the study area or members of HF associations from the study area.
The diagnostic criteria for the sample were patients with multi-morbidity and HF and complex health needs who meet the following diagnostic criteria
39
:
Be classified in clinical category A of chronic pathologies for HF that, in a situation of clinical stability, has been in grade I or II of the New York Heart Association Classification (NYHAC),
40
being able to be simultaneously classified, or not, in other clinical categories for having another chronic disease(s) included in these categories. Patients with at least one of the following complexity criteria: extreme polypharmacy (≥10 chronically prescribed active ingredients), socio-familiar risk (Gijon scale score >10 points
41
, pressure ulcers of stage II or higher, malnutrition (body mass index <18.5 kg/m2), nasogastric feeding (≥3 months) and 2 or more hospital admissions in the previous 12 months.
The inclusion criteria for the participants were (a) to be patients attended by healthcare professionals of the basic health areas participating in the study and (b) over 18 years of age. The following exclusion criteria were applied: (a) patients with persistent cognitive impairment (Pfeiffer with ≥5 errors
42
or Lobo Mini-Cognitive Test score <23
43
or severe mental disorder (e.g. psychotic disorder), (b) patients who refuse to participate in the study and (c) patients with digital health illiteracy.
Participants were recruited for this study by an email or face-to-face. Case management nurses and physiotherapists responsible for cardiac rehabilitation invited the patients who met the inclusion criteria. Moreover, the presidents of the HF associations were contacted (a total of 15 associations); they were key informants and who sent emails to their members.
Those who expressed interest in the study contacted with their health providers, or they simply agreed to participate by returning the invitation message. First contact between researchers and participants was made by e-mail, face-to-face and, preferably, by telephone in order to make an appointment for the interview. Potential participants were informed about the aim, the setup and data privacy of the study. There were no financial incentives to participate in the study. Finally, the sample comprised 20 participants, with no losses or voluntary resignations during the process.
Data collection
Phase 1: bibliographic reviews
Six working groups were created (corresponding to the main areas of action of the patient with multi-morbidity and HF) in order to analyse the scientific evidence between February and April 2020. They had to identify original articles and/or systematic reviews/meta-analyses that described intervention proposals (in their area assigned topic) to promote the autonomy/self-management of the patient with multi-morbidity and HF. For the elaboration of the contents, based on the evidence, each group was provided with a working document model to fill in (see Multimedia Appendix 2). This document provided a search protocol to standardize the methodology among the different researchers in which the following fields were included: (a) databases consulted, (b) descriptors used, (c) search strategy, (d) descriptions of the interventions and their results in the selected articles and (e) proposals for the presentation of content. Based on the evidence collected, a draft of questions for each theme was prepared for the interviews (phase 2).
Phases 2 and 3: semi-structured interviews and user stories
Data collection was conducted from December 2020 to March 2021. Semi-structured interviews were conducted by five trained interviewers (nurses with a background in qualitative interviewing and experience in dealing with patients with multi-morbidity or HF). Although the majority of members were women, no particular characteristic of interviewers’ profiles was expected to lead to any form of bias in the conduct and analysis of the qualitative interviews. There was a balance between those who worked in clinical settings and those who worked at the university and whose have been involved in the project mentioned above and who is not. There was no prior relationship between the interviewer and the interviewed person. A brief introduction of the interviewers at the beginning was necessary related to their name and surname and the institutions and objectives involved in the study.
According to DeJonckheere and Vaughn, 44 a semi-structured interview guide (see Multimedia Appendix 3) with open-ended questions was conducted according to the themes to be covered: (a) food and nutrition, (b) medication and treatment adherence and compliance, (c) rehabilitation and physical activity, (d) warning signs and symptoms, (e) self-management and resources and (f) emotional management. The interview guide was jointly developed by the researchers from the work teams, who have experience with research or are healthcare professionals with experience in treating HF.
Finally, the interviews were conducted individually by telephone or face-to-face communication (only for institutionalized patients). In the first case, the interviewers made telephone calls at the time that was most convenient for them. In the second case, they were conducted in nursing homes where the participants consulted were staying. Participants were informed about the purpose of the study, and an information sheet was given. This initial contact was followed up by a telephone interview to establish their interest and consent to participate. Quantitative socio-demographic data were also collected through interviews.
In each section (theme), based on the user story approach, 32 participants were asked to fill the following sentence: ‘As a user of the application and/or as a heart failure patient I want/need ________ to _______ achieve/solve the problem/need of ___________’. Finally, at the end of each interview, participants were asked if they wanted to add more information in an open-ended way. Given the age profile of the participants, the interviewers put special emphasis on the repetition of information provided by the interviewees to (a) secure the information received and (b) reaffirm the participant's position.
All interviews were audio-recorded with the consent of the interviewees, and no field notes were required during the data collection process. Double-checking by the interviewers was used to clarify any comments, so it was not necessary to repeat interviews. Subsequently, the sound recordings were transferred to verbatim and adapted for analysis.
The average length of the interviews was 45.82 minutes. Thematic saturation was achieved with the 20 interviews.
Data analysis
A descriptive statistical analysis was carried out using the distribution of absolute frequencies and percentages of the socio-demographic and health variables, as well as the results of the semantic analysis.
Data were audio-recorded and transcribed verbatim. We used thematic analysis following the methods of Braun and Clarke. 45 The themes identified on a semantic level were closely linked to the data using an inductive approach. Each interview was coded according to person and interview number (for instance, N2, nurse in interview number 2; P12, participant in interview number 12; and C4, informal caregiver in interview number 4). Three nurses and a psychologist (all PhD) were separately responsible for the manual analysis using office software. Each made a detailed division of the content of the interviews to group them according to the topics under study. The textual quotations were accompanied by the identifier of the interviewer (e.g. patient (P1) or informal caregiver (C1)). The themes identified on a semantic level were closely linked to the data using an inductive approach. For the semantic analysis of the content of the conversations, the software Sphinx iQ3 v.8.2.2 was used.
Since the themes were already defined and there was no derivation, there was significant internal consistency (100% agreement) between the topics and the resulting data for both major and minor themes. Participants had the opportunity to provide feedback on the extracted data.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki, and approval was obtained from the Cadiz Research Ethics Committee (Trial Registration: ClinicalTrials.gov NCT04725526; protocol date: 31 May 2019). Due to logistical difficulties related to the COVID pandemic, acceptance of informed consent was done via a telephone call.
Results
Sociodemographic characteristics
All interviews included persons with multi-morbidity and HF; twice the patient was joined by their informal caregiver. Most of the recruitment was carried out in outpatients (n = 18), whilst in the remaining cases, it was in the hospital setting (n = 2). Table 1 summarizes the main sociodemographic and health characteristics of those interviewed. The main profile was male, with a mean age of 67.56 ± 13.51 years, married and with secondary education. Likewise, most were in grade I of the NYHAC at the time of the interview (n = 12). Arterial hypertension was the most frequent cardiovascular risk factor in the patients (n = 8).
Sociodemographic and health characteristics of interview participants (n = 20).

NYHA: New York Heart Association Classification.
Phase 1: evidence integrative review
Multimedia Appendix 4 shows the evidence summary for each topic area. This table of evidence has been prepared, distributing the contents by work group, database, search strategy, inclusion criteria, number of studies included, main themes and recommendations proposed by each group.
Phase 2: semantic and thematic analysis
A semantic analysis of the participants’ responses, after excluding non-relevant words, was conducted. Most of the most frequent words were related to (a) health provider-patient communication, (b) the improvements in health that the app produces through reliable information, (c) the need for the app to promote daily interaction with the user and (d) its adaptation to the user's conditions.
After a thematic analysis, 15 subthemes related to the domains of food and nutrition, medication and treatment, rehabilitation and physical activity, signs and symptoms, self-management and emotional management emerged. These subthemes captured the meaning of narratives offering contextual insights into the development of the app. Summaries of the key themes and subthemes are presented in Table 2.
Key themes and subthemes.

Next, a detailed description of the main subthemes emerged is presented.
Theme 1: food and nutrition
Subtheme 1.1: useful information for feeding
According to most patients, an app of these characteristics should offer a list of recipes or ingredients, with the possibility of being expanded. In the case of the first option, they would like it to have weekly and maintain a healthy nutritional balance, avoiding unnecessary repetitions in short spaces of time. In the second case, they would like to know what foods they should or should not eat: It would be a quite favorable option, so that everyone could make their own list, so that everyone, starting from a base list, could make their own list and create their own food dishes, which they would like to eat every day, both at lunch and dinner. [P5]
That the recipes are of seasonal foods and that you can buy them anywhere, without rare ingredients. Knowing what foods, I should not eat and how to cook healthy. [P18]
As for the presentation of nutritional information, they preferred that it be provided in image format using pictograms, especially for the ingredients. Only those who do not use cell phones frequently indicated that they would like the information on paper: Everything can be done perfectly. What is the iconography of the vegetables themselves, of the meals themselves that can be made and from there you go configuring with your finger and you go putting it in your package, in your bag, whatever it is called. [P5]
The best thing would be the picture, the ingredients and how you can cook it or how you can prepare it. [P8]
Most of the participants emphasize that a list of allowed and not recommended foods is included: Well, the necessary information at all times is to know what I can and cannot eat… [P5] A detailed list. [P13]
Another functionality commented on was the implementation of a barcode and QR reader or for nutritional labelling. With this, the aim is to have more information and understanding of a food product, especially in cases where they are incompatible with respect to their diseases: The App in this would be great for me. Because if it reads barcodes or QR codes, depending on what it brings, and tells you the negative part it has, because it is a part that matters to me, and the positive part, the good part for your diet, proteins and vitamins and so on, then that application would be great. [P7]
The convenient thing is that we have information about the products. [P20]
Subtheme 1.2: diet monitoring and weight control
In general, the patients considered a dietary follow-up to be appropriate, although opinions were more varied in this regard, with some preferring to carry out the follow-up on their own. Other participants would like a follow-up by a professional trained in the field. As for its implementation in an app, they were more in favour of having it track their weight: That could be done with an App that you go weighing yourself every week and you go seeing your weight and you can manage yourself and say uhh… I'm gaining weight so I have to tighten a little bit more. [P6]
Well either in the nurse's office or through the application. [P19]
However, this opinion would be softened if the application had an interactive help system or remote assistance that would allow it to respond adequately to the questions posed by users. It depends on the technological skills of each person: I think that the application would have to be a little bit like Siri, wouldn't it, that the patient would directly ask the question and that it would have a block of questions that would generate an auto-response, which for example, in elderly people like them, they don't know how to handle themselves with technology, many times it is better to have an auto-response, like a kind of Siri, which would be very good because they like that, it would be more dynamic. [C4]
I think that technology … of course, it depends on the type of person. Because younger people who are more into the world of technology, everything that is technological can be taken, but for older people who are not very much into technology, it might be more difficult. That's why it's better in person, even if it's by telephone. Or virtual, by video call. [P7]
Theme 2: medication and treatment adherence and compliance
Subtheme 2.1: drug–food interactions
In relation to the previous topic, it was found that almost half of the participants were unaware of the existence of drug–food interactions. In this regard, several patients expressed the need for a table of suitable and unsuitable foods with respect to pharmacological treatment or a list of interactions: I think that, with a table, right? In which it specifies which foods are suitable and which foods are not suitable, right? [P4]
It would be ideal if I could see the medications with the contraindications and the foods that can affect me. [P17]
Providing me with a list of the medications I take and what I shouldn't eat so that I don't feel sick. [P18]
Alternatively, they suggested that the app should have a notification system that would detect incompatibilities between their treatment and the foods recorded in the food section. The possibility of automatic removal of foods from the list after including drug treatment was also noted: If any patient has medication entered in that application, and it is incompatible the food with the medication itself should automatically pop up a warning. [P5]
I think that, if one thing were linked to the other, I think that would be the best thing, when you look for food to eat it would be related to the medication. I don't know how it could be linked, if in a way that when you go to look for a food, it would tell you to be careful, you are taking this and you cannot eat it. [P6]
Subtheme 2.2: information on drug treatment
Almost all the persons interviewed were aware of the effects caused by the drugs included in their treatment. This information was provided verbally by their cardiologist and, eventually, by their nurse: I have been lucky enough to have cardiologists and nurses who are a little bit special and they have taught me how to treat myself and how to take the medications. [P6]
Well Paco [the cardiologist] told me to take this, this and this … this has to be in the morning and that at night. [P8]
The doctor at the time. He told me verbally, let's say. [P19]
In case they do not know such information, they usually look for information online or ask the pharmacist. They also write it down on a piece of paper and, failing that, on a mobile note-taking application, since most patients are the ones who control their medication: Yes, when he gave me that I looked up online what each one was. I prepare them myself. [P8]
Yesterday he brought me the medicine, and he brought me one that I didn't know, and I say what is this for? And he had to call the pharmacist and tell him no, this is your wife's cholesterol, and of course, they had changed it for me. [P12]
I don't know. I take 19 pills and I don't know what they're for. … Diabetes, cholesterol … I don't know what. I don't know how much; I don't know what for … I don't know the name of the boxes. You have to write them down on a piece of paper. [P13]
Subtheme 2.3: preventing medication forgetfulness
In general, there was good adherence to treatment in the patients interviewed, although almost half of the participants confessed that they forgot to administer medications on some occasion. The factors were related to overconfidence, polymedication, errors with medications with similar appearance or problems with alarms: That is to say, the issue of forgetfulness at the beginning you take it very rigorously, but later on you become more confident, and confidence, and confidence can kill you! [P5]
Either I missed the alarm or I removed it and then I forgot about it. […] What do I do so that it doesn't happen to me? [P7]
Likewise, the occurrence of unforeseen events at the time of administration was one of the most frequently mentioned reasons. The error procedure followed the following dynamics: (a) the alarm for medication administration sounds, (b) the user turns off the alarm and proceeds to take the medication, (c) an unexpected event occurs before administration and (d) the user forgets to take medication: Because I finish eating and get up and start to pick up and when I realize it, I forget to take it. [P6]
Being at work there are times when I've forgotten to take my pill, a couple of times that's been, mostly going into the afternoon shift. [P19]
Among the suggestions proposed by the participants, the use of alarms and repetitions to remember the administration of medication, as well as counting the pills whilst reviewing the information provided by the App, should be highlighted: I make the alarm repeat; it repeats within 5 minutes so that I don't forget. [P7]
Subtheme 2.4: drug replenishment
Some patients commented that non-compliance with treatment was due to forgetfulness regarding the purchase of medications. Through the responses, a lack of foresight in refills was identified. The importance of having a functionality that indicates on what date the contents of the medicine containers will be used up is also highlighted: Well another thing, that if maybe … this I see it more silly than telling you to know how much I have and when I'm going to run out. Or somehow, how do I know … the other night I was going to take gabapentin and I went to take it and I didn't have any and I didn't take it at night and I didn't take it in the morning either and it is a medicine that is important for the heart. Of course, it would be useful to know how much medication you are going to take per day and when the day will come when you are going to run out so that you can prevent it and buy it and go to the pharmacy and take it a day or a couple of days before. [P6]
Well, in my case, what I do have to be very careful about is that I never forget to refill my medications. Because of course, if I'm travelling or here, but when I'm going to prepare the pills, I go to the pharmacy and I take out the necessary medicines, so that when I go to refill the pill box I don't forget. [P7]
Theme 3: rehabilitation and physical activity
Subtheme 3.1: types of exercise
Practically, all the participants were interested in the existence of exercise tables, especially weekly and, to a certain extent, monthly or quarterly. They emphasized the importance of varying the types of exercises to prevent the lack of motivation. They preferred their presentation on paper by means of images, although in the case of a mobile application, they would like to use didactic videos: Because doing continuous exercise during the period of 1 year is boring as hell. I tell you this because for the first 5 years I went to the gym and every 3 months or 2, 2 and a half months or so they changed the exercises. Because of course it was so boring that there came a time when you knew it by heart. [P5]
Even if in the application they also record videos and help you to do those exercises and you do it at home … or drawings of course where they tell you what kind of exercise you have to do, not to make the effort you know. [P8]
In terms of their preferences, most usually opt for walking due to the limitations in activities of daily living due to their comorbidities. Some participants, mainly those with fewer limitations and/or greater motivation, commented on their preferences for performing strength and stretching exercises indoors: The main one and the most comfortable for me and, well I don't know if it will be the healthiest, but the most relaxing, yes, walking. Walking every day. At least one hour, quietly if you have to stop a little bit, because of course, it will depend on how each person is, but walking, getting some air and seeing that it is much more relaxing. [P7]
Well, every day, walk, walk, walk and the more the better. [P10]
And here at home maybe I do two or three exercises lifting my legs, my arms, things like that when I do it here at home. [P12]
Subtheme 3.2: monitoring of physical activity
Given that many participants reported walking as a form of exercise, the use of the pedometer on the mobile phone is crucial for monitoring. In general, especially with regard to HF, they commented on the need for heart rate and respiratory rate monitoring and, to a lesser extent, oxygen saturation and electrocardiogram. To this end, it is important for the application to have Bluetooth connectivity with smart watches: It would be best if, within the App, it had a device that could connect to a watch and take your heart rate. [C4]
I walk as long as necessary. I have a pedometer that tells me the steps and kilometers so I control the walking. [P9]
In addition, they valued positively that there were didactic videos on breathing control, with follow-up, if possible, by a personal fitness trainer. For them, this characteristic is of vital importance during physical activity: The truth is that it helps a lot when you are exercising because if you don't suffocate, your heart rate goes up and when you control your breathing the exercise becomes much more bearable, easier. [P6]
Through explanatory videos, follow-up and online classes by the Physiotherapist. [P17]
Subtheme 3.3: suggestions and motivation for physical activity
The use of inactivity alarms with exercise suggestions and physical activity tracking was the strategy most commented on by participants: Have the App alert me and tell me to look and move. I go down to my patio and walk around two or 3 times and come back up. [P8]
By an alarm every so often, reminding me to get up from the couch. [P18]
Other functionalities commented on to promote physical activity were the provision of information about its benefits and recommendations and a system of goals or achievements. Some participants suggested the possibility of connecting with people in similar situations to get together and engage in group physical activity: With rewards, saying well look, if you do that, well you have such a thing, you have a reward. [P4]
When we go for a walk on Tuesdays and Thursdays, we do what we call the million steps, and that is that we meet a few people from a place and we do a route and we walk a few of them. What happens is that when you go walking with more people chatting and so on, you get more distracted and it is more bearable and you don't make excuses. [P6]
Informing us well of the benefits we are going to get. [P18]
Theme 4: warning signs and symptoms
Subtheme 4.1: detection and action
Half of the people interviewed were concerned about dyspnoea, as well as the fatigue derived from this symptom. They also considered precordial pain as another of the most worrying symptoms: Now I noticed that I was getting bad because I was choking a lot when I got up, when I moved … when I moved, I was just choking and there I said I have to go to the doctor. [P4]
If I get a little pain in my arm, the only thing I do is stop, then I notice that my heart goes faster, and I stop and wait for it to go away and then I continue. [P10]
Some patients went directly to the emergency department, although most reported knowing how to act when these signs and symptoms appear, as well as going to the emergency department when, after trying, they are unable to control it. In general, patients reported preferring to try to control their symptoms rather than constantly going to health centres. In many cases, they have rescue medication for certain symptoms and know how to use it correctly. If, after trying on their own or with this rescue medication, the symptoms persist and they are unable to control them, they seek medical help (they generally go to hospital emergency departments): Put a little pill under my tongue. […] If I don't get over it, I put another one on and if I don't get over it, I call 112. [P5]
Normally I have waited for it to go away and other times I have to go to the emergency room. [P19]
Subtheme 4.2: usefulness of a mHealth app in emergency circumstances
It was repeated on several occasions that a list of alarm signs and symptoms that are explained and what to do in case they appear would be useful. However, some participants emphasized that in the event of presenting any worrying symptom, they would not look at this list, so they commented on the possibility of having access to a telephone line that could put them in contact either with their primary healthcare centre or with an emergency professional (or even be able to call the emergency services from this menu), either for the patient or their informal caregiver to communicate: I go to the application and in the application, it comes to me describing that this type of symptom can happen with heart disease, then it is an alarm sign, then I already say, well this can be that. [P4]
If you put that in the App, the ambulance to you would show up in a minute, that would be a miracle or it would be connected to a hospital center. I'm talking about this … I wish, but I know this is … (complicated) connected to a health center, to a hospital or some patient going in an emergency so that when you get there, they have everything ready. [P8]
The possibility that, in case of using a smart device connected to the application, it could show an alert in case of detecting any anomaly in the figures of any vital constant was mentioned. Likewise, on some occasions, the idea was expressed that, in the event of requiring attention by the emergency services, they could also access the data collected in the app (medication and vital signs, among others) to find out more information about the patient: If we have a device that emits information to the application and this device catches you that the values and constants of your body are different from what you should really have. […] Well, then, obviously, an alarm should go off in the application, why? to pick up that there is a defect and that there is a problem that can arise at any time. [P5]
At the very least, to be able to give the doctor all the information that you've collected. [P7]
Theme 5: self-management and resources
Subtheme 5.1: knowledge about health resources close to the user
Throughout most of the interviews, the participants were unaware of the health resources around them or only mentioned the hospital or their health centre. They were receptive to the idea of being able to access a map showing the available social and healthcare resources, where they could also access information and contact details. One patient commented that it would be a good idea to locate on a map which facilities have an automated external defibrillator (AED). The need for the application to geolocate the user, in case of an emergency, was also mentioned. In other cases, it was mentioned to implement a videoconferencing system, new resources and communication from the app with the communication service with the health system: The main thing is to have 1 or 2 contacts in terms of the caregiver or guardianship, to which it is subject or either through the 112 health authorities, and of course always have a direct contact with this type of associations that are dedicated to the care of people, in this case, so that the whole year know how to direct you, your new life, where you have to route it. [P5]
One thing I would like to know is where there are resuscitators, where is the place, for that recognition of all of us who are cardiac patients. [P9]
Subtheme 5.2: informal caregiver involvement
All participants wanted their informal caregivers to be able to access the app. In this regard, there was some consensus on access to the patient's records, especially on the evolution of vital signs and symptoms. On the other hand, they suggested the need for a separate section for the informal caregiver in the App with information on how to act in different situations: Super important. Otherwise, who else. […] Well, it can help because, first, the App should take the patient's data with the heart disease with the disease he suffers from, and a record of his history so that the caregiver can see a bit of the patient's profile. [C4]
Providing the necessary information about care, nutrition, medication and how to act in case of a worsening. [P17]
Theme 6: emotional management
Subtheme 6.1: personal motivational strategies and family support resources for treatment compliance
This was one of the aspects where there was the greatest diversity of opinions, as some are self-motivated and others need family support to stay motivated: I always go to the people closest to me, which is my wife and daughters. I don't go to, or phone my doctor or cardiologist or nurse. No, it is the family that has the power together with you to help you stay within the established limits. [P5]
Nobody. I put up with it. … But since no one paid attention to me, I didn't go to anyone. [P13]
Some participants expressed their desire and need to be motivated by third parties, especially with community activities carried out in associations or groups of sick people. However, they expressed their sadness about the decrease in activities given the pandemic situation: We have people from the association, what do we say: thank God we found the association and I have a totally different life. [P6]
And in the association, it is always good to see people who are in the same situation as you, because it always gives you comfort. [P7]
Well yes, I usually go to everything organized by the Clover of Hearts association, although right now nothing is being done with the pandemic, but these years there was a talk, anyway, to try to motivate us and the recognition of the symptoms and the rest. [P9]
Subtheme 6.2: mHealth strategies for emotional management
Almost all the interviewees expressed the need to be listened to, either by their family or by a health professional. In the latter case, the need for a psychologist emerged. On the other hand, it was suggested that the app could have a telephone to communicate with someone or to form group sessions or support groups: Well, mentally the psychologist is the most favorable, right? It's the right thing to do. But the fact that someone listens to, well, the psychologist. […] Or at least that there was a phone number where the person could call and talk to someone, even if he/she is not a psychologist. [P7]
In general, a lot of importance is given to everything related to leisure activities and hobbies. Other strategies for implementation in an app would be mood assessment and videos on relaxation techniques. Information on controlling negative thoughts is also relevant to them: So, now, through the App how can we carry those feelings. The watch I wear measures my stress, and the fact of relaxing, of doing or not doing, the App can check your mood. […] I knew how to control myself with the experience and both the relaxation techniques and all the psychology sessions they gave me at the health center, and thanks to that I learned to control myself because, at the end of the day, nobody is going to do anything for you, you have to do it by yourself. [P5]
Well, that would be a very good point because relaxation really helps a lot. We also practice relaxation at the association. [P6]
Phase 3: user story
In each section (theme), based on the user story approach, participants were asked to fill the following sentence: ‘As a user of the application and/or as a heart failure patient I want/need ________ to _______ achieve/solve the problem/need of ___________’. Users were asked a total of six times for each interview and participant. As a transversal element, in a large part of the user stories (n = 12; 60%), the need to receive motivational messages appears (on the various topics). Table 3 details the opinions of users who completed the user story for each section.
Most frequent user stories, divided by subtheme.
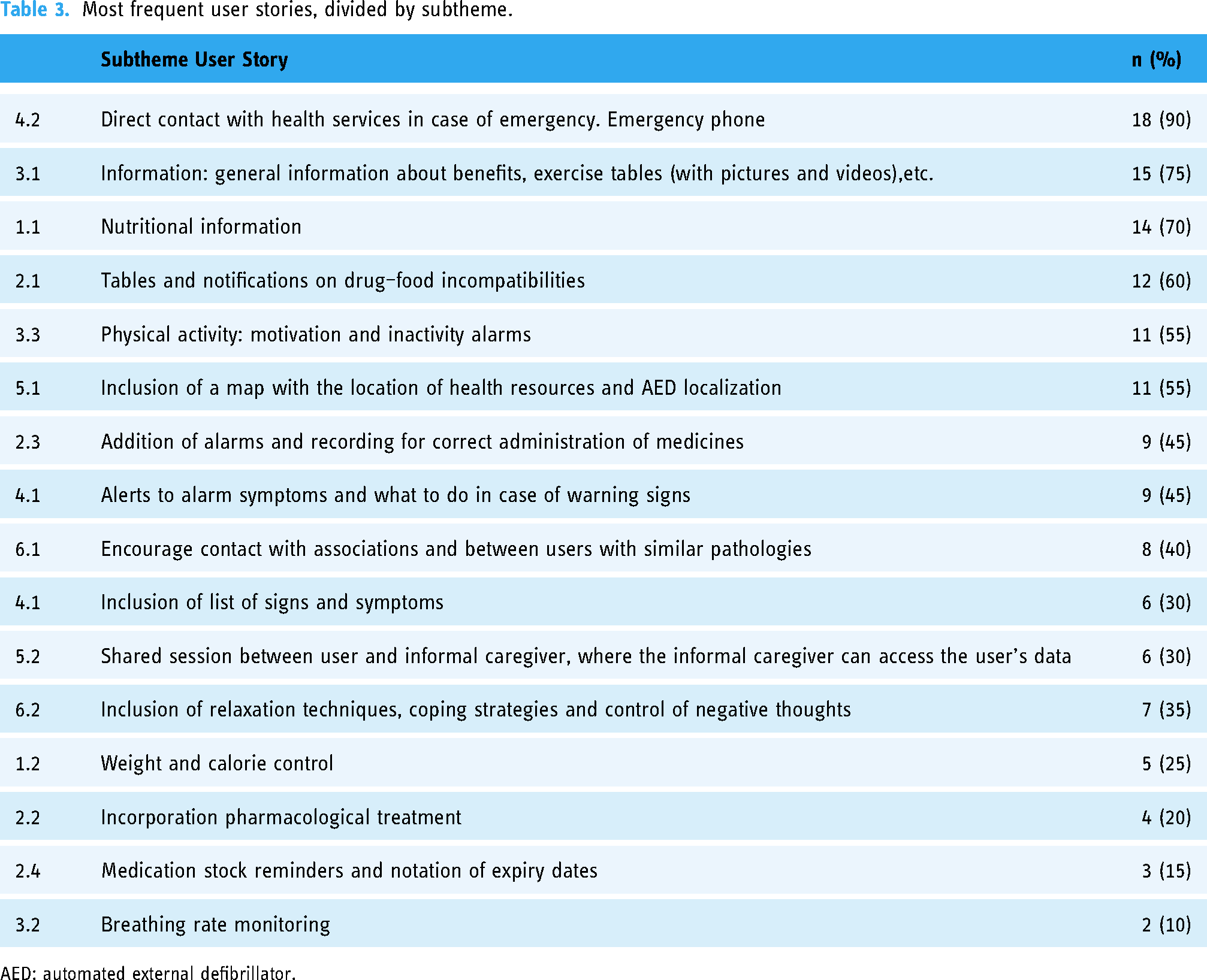
AED: automated external defibrillator.
Discussion
Principal results
The aim of this study was to provide practical information regarding needs, preferences of content and format of an app to assist the self-management in patients with multi-morbidity and HF. This study uses an innovative perspective including a theory-informed and evidence-driven approach and user involvement, in developing a mobile app for a healthy lifestyle program in patients with multi-morbidity and HF.
We can consider that the main effective mechanisms of multicomponent interventions for patients with HF identified in our study must contain (a) components that increase the patient's understanding of HF, (b) self-care, (c) self-efficacy, (d) participation of the family/informal caregiver, (e) psychosocial well-being and (f) professional support and use of technology, which are in line with those previously identified by Clark et al. 46
The use of a qualitative approach to elicit the user's views during intervention development is considered a good practice. 47 This user-centred design is tailor-made to the end-user perspectives because it can ensure that the app is desirable and suitable for end-users 29 by selecting preferable content, technology platform, user interface, interactivity and functionality. The triangulation of the information is important in qualitative analysis. Therefore, this study illustrates how intervention development may be enriched with theoretical basis, systematic reviews and thematic analysis technique of the interviews.
Of the total of 6 thematic areas proposed in the script of the interviews, a total of 15 subthemes emerged oriented to the design and development of the contents of the app. Taking into account the user stories approach, our results indicate that participants want an informal interface with an app that provides a highly individualized experience to facilitate participation in healthy levels of physical activity, nutrition, medication adherence, control of warning signs and symptoms and help to control the emotional state and an app that is easy to use and provides you with feedback on your current status through simple check-ins. Finally, it is very important to connect with health professionals and with other people in the same situation. This can be achieved by an app that provides real-time feedback and personalized content sensitive to the users or allows care coordination between health personnel and the user.
Patients prioritized improvements in direct contact with health services in case of emergency (90%), nutritional information (70%), type of exercises in order to improve their physical condition (75%) and food and medical interaction information (60%). The importance of motivation in several issues is also confirmed by the high number of respondents regarding alerts, motivational pop ups and alerts to avoid forgetfulness (60%). Similarly, according with the study by Pianese et al., 48 which used a mixed approach to evaluate the perception of needs in outpatients with acute HF, the areas of needs identified were knowledge of social resources and available health information (40%), information on disease and lifestyle habits (20%), clear identification and/or contact with the care manager (30%) and identification of warning signs and symptoms and worsening of symptoms (25%).
In our results, 30% of the interviewees considered it positive to be able to share the application with their main informal caregiver. These results coincide with those obtained by Buck et al. 49 on the effectiveness of multiple interventions in patients with HF self-care.
Although anxiety and depression are very frequent consequences in patients with HF and despite the fact that, among the main aspects to consider in the emotional area, patients indicated the need for relaxation techniques and coping strategies in 35%, few studies have evaluated the effectiveness of specific psychological interventions to reduce these undesirable psychological effects in this group of patients. 50 HF patients appear to be underrepresented in this area of research. In a recent study, 51 which included a large sample of patients with HF and a percentage to be considered who suffered from moderate depression, it was concluded that telemedical care improved depressive symptoms and had a positive influence on quality of life in patients with HF and moderate depression.
There were little to no controversies in the respondents’ statements and their user stories, except for the importance of the motivational messages. On the other hand, the users’ statements have been supported by the scientific evidence where the gamification strategies play an important role in this type of interventions. Thus, in line with the literature, the patient diary is presented as an alternative to incorporate into mHealth tools to alleviate some of the needs considered in the qualitative analysis (e.g. forgetfulness, monitoring, follow-up and interactions). Through this system, patients will be able to record their constants, their daily evaluations and main signs and symptoms through the application to assist their self-management. In addition, this is of interest for the clinical follow-up of the HF patients.
Limitations
Focus groups were not possible due to mobility restrictions and the risks involved in a face-to-face methodology with vulnerable groups during the COVID-19 pandemic. Most of the interviews were conducted by telephone, which meant that it was not possible to analyse all the components of the non-verbal communication. However, the audio recordings made it possible to provide information on the paralinguistic elements of the voice, and when it was necessary, the emotions aroused were asked by the interviewers.
The information obtained was essential to understand the needs of patients for the development of an app. Indeed, there are authors that consider virtual interviews like a strength because they can increase access to participation among those who may be limited by transportation or logistical barriers. 52 Finally, although the three cycles of the ISR approach have not followed the same order in this study (because of the COVID-19 pandemic), the preliminary results of the integrative reviews support the flow carried out, helping to the structure of the interview guide and facilitating the data collection.
Strengths
The research team of this project is characterized by its multidisciplinary nature (psychologists, nurses, area specialists, computer engineers, physiotherapists and graduates in physical activity and sport sciences). The participation of members with clinical and academic experience and the Health Literacy Spanish Network favoured the necessary synergy and feedback between theory and practice, which ensures the application of the knowledge generated in research to the reality of healthcare, promoting the sustainability of the scientific–technical progress achieved. Undoubtedly, one of the strengths of this project is the participation of potential users in the design of the mobile application.
In comparison to classical software development methods (e.g. waterfall model (Royce, 1970) 53 and V-model (Weilkiens et al., 2016)), 54 apps have the advantage that the necessary (evidence-based) knowledge and expertise for integration into clinical processes is gathered in cooperation with stakeholders before the software is developed.
The triangulation of the information is important in qualitative analysis. So that, this study illustrates how intervention development may be enriched with theoretical basis, systematic reviews and thematic analysis technique of the interviews.
Conclusion
This study underpinned that evidence and qualitative research are beneficial steps prior to designing apps. Our study identified important opportunities for future research to better understand the preferences of patients in the management of HF and addressed a gap identified in the literature in which interventions for patients with comorbidities are frequently excluded. The user stories enabled us to identify a range of patient-relevant attributes for potential inclusion in specific apps.
The results of this study have been the basis for the development of the mICardiApp application, which is currently in the pilot phase.
The first version underwent a preliminary evaluation by the research team to establish that the contents were valid and to improve the final version. A mock-up of the app was made to create a first draft of the interface and its navigation, whose content was validated by experts (professionals and patients). 55
The final version of mICardiApp is structured with a first screen leading to a registration form. After that, the app shows profile and emergency buttons and nine main sections: cardiac rehabilitation and physical activity, nutrition, medication, emotional support, signs and symptoms, resources, learn and have fun, goals and alerts.
mICardiApp appears as proposal for health literacy for patients with multi-morbidity and HF considering their basic dimensions 56 : at a functional level, it gives a gaming strategy to improve the knowledge and self-management of the disease; at an interactive level, it incorporates the possibility of preparing questions for the next health appointment, contacting with other people with their condition and specific organizations and/or patients’ schools; and at a critical level, it encourages an aware health-related, decision-making process. Regarding self-care, mICardiApp integrates a self-check-in and monitoring of alarm signs and symptoms, reminders for taking medicine and starting physical activity, stocking of drugs, specific recommendations on diet, physical activity and cardiac rehabilitation, monitoring of fluid, body weight and recommended heart rate for physical activity according to functional capacity as well as emotional management and promoting positive thinking.
However, there are contents that could not be incorporated into the application due to the high technical requirements and, consequently, were discarded due to their cost/benefit ratio (for example, SIRI or barcode reader for medicines). It should be remembered that these requests arose from isolated users and were not a general requirement. On the contrary, it was possible to incorporate the most requested content.
Let us not forget that this application is a complement for the self-care of these patients; it should never replace the care provided by healthcare professionals.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231180466 - Supplemental material for Needs of patients with multi-morbidity and heart failure for the development of a mHealth to improve their self-management: A qualitative analysis
Supplemental material, sj-docx-1-dhj-10.1177_20552076231180466 for Needs of patients with multi-morbidity and heart failure for the development of a mHealth to improve their self-management: A qualitative analysis by Pilar Bas-Sarmiento, Martina Fernández-Gutiérrez and Miriam Poza-Méndez, Mª Ángeles Carrasco-Bernal, Magdalena Cuenca-García, Mercedes Díaz-Rodríguez, Mª Paz Gómez-Jiménez, Olga Paloma-Castro, Alezandra Torres-Castaño, Antonio-Jesús Marín-Paz in DIGITAL HEALTH
Supplemental Material
sj-docx-2-dhj-10.1177_20552076231180466 - Supplemental material for Needs of patients with multi-morbidity and heart failure for the development of a mHealth to improve their self-management: A qualitative analysis
Supplemental material, sj-docx-2-dhj-10.1177_20552076231180466 for Needs of patients with multi-morbidity and heart failure for the development of a mHealth to improve their self-management: A qualitative analysis by Pilar Bas-Sarmiento, Martina Fernández-Gutiérrez and Miriam Poza-Méndez, Mª Ángeles Carrasco-Bernal, Magdalena Cuenca-García, Mercedes Díaz-Rodríguez, Mª Paz Gómez-Jiménez, Olga Paloma-Castro, Alezandra Torres-Castaño, Antonio-Jesús Marín-Paz in DIGITAL HEALTH
Supplemental Material
sj-docx-3-dhj-10.1177_20552076231180466 - Supplemental material for Needs of patients with multi-morbidity and heart failure for the development of a mHealth to improve their self-management: A qualitative analysis
Supplemental material, sj-docx-3-dhj-10.1177_20552076231180466 for Needs of patients with multi-morbidity and heart failure for the development of a mHealth to improve their self-management: A qualitative analysis by Pilar Bas-Sarmiento, Martina Fernández-Gutiérrez and Miriam Poza-Méndez, Mª Ángeles Carrasco-Bernal, Magdalena Cuenca-García, Mercedes Díaz-Rodríguez, Mª Paz Gómez-Jiménez, Olga Paloma-Castro, Alezandra Torres-Castaño, Antonio-Jesús Marín-Paz in DIGITAL HEALTH
Supplemental Material
sj-docx-4-dhj-10.1177_20552076231180466 - Supplemental material for Needs of patients with multi-morbidity and heart failure for the development of a mHealth to improve their self-management: A qualitative analysis
Supplemental material, sj-docx-4-dhj-10.1177_20552076231180466 for Needs of patients with multi-morbidity and heart failure for the development of a mHealth to improve their self-management: A qualitative analysis by Pilar Bas-Sarmiento, Martina Fernández-Gutiérrez and Miriam Poza-Méndez, Mª Ángeles Carrasco-Bernal, Magdalena Cuenca-García, Mercedes Díaz-Rodríguez, Mª Paz Gómez-Jiménez, Olga Paloma-Castro, Alezandra Torres-Castaño, Antonio-Jesús Marín-Paz in DIGITAL HEALTH
Footnotes
Acknowledgements
The authors thank the Institute of Research and Innovation in Biomedical Sciences of the Province of Cadiz (INiBICA) for funding support for this project. They also express appreciation to all of patients who took part in the semi-structured interviews. Similarly, our thanks to the independent researchers who participated supporting in the data recollection: Mª José Lamas-Toranzo, Pablo Soler-Martins, Arantxa Barrera-Smidi and Nuria Rodríguez-García.
Finally, the authors wish to thank the other participants of the ASyAG_PPIC Team (José María Cano-Guerrero, Inés Carmona-Barrientos, Mónica Casado-Daza, José Castro-Piñero, Cristina Castro-Yuste, Ignacio del Arco-Herrera, Pedro Díaz-de Souza, María Falcón-Romero, Jorge del Rosario Fernández-Santos, Laura Gallardo-Amaro, Gloria González-Medina, Eulalia Hernández-Encuentra, Luis Javier Moreno-Corral, Petronila Oliva-Ruiz, Francisco Javier Ordoñez-Muñoz, Ceferino Prieto-García, Inmaculada Ramón-Macías, Manuel Rosety-Rodríguez, Víctor Segura-Jiménez, Juan Carlos Paramio-Cuevas, Mercedes Ruiz-Carreira, Eduardo Sánchez-Sánchez and Javier María Yagüe-Sánchez) for their contribution in the general project.
Contributorship
PBS and MFG conceptualized the paper, designed and the coordinated the study. AMP, MPM, MPGJ and MACB provided data; PBS, MFG, AJMP and MPM analysed them. All authors wrote the manuscript draft. OPC provided overall guidance. PBS, MFG, ATC, MCG and MDR reviewed the results; PBS, MFG, ATC and MCG reviewed the final draft and edited the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Ethical approval
This study has been approved by the Cadiz Research Ethics Committee.
Funding
This project (code: LI19/20IN-CO19) was supported by the Institute of Research and Innovation in Biomedical Sciences of the Province of Cadiz (INiBICA).
Guarantor
PBS and MFG
ORCID iDs
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.