
Abstract
Supporting clinicians in decision making using advanced technologies has been an active research area in biomedical engineering during the past years. Among a wide range of ubiquitous systems, smartphone applications have been increasingly developed in healthcare settings to help clinicians as well as patients. Today, many smartphone applications, from basic data analysis to advanced patient monitoring, are available to clinicians and patients. Such applications are now increasingly integrating into healthcare for clinical decision support, and therefore, concerns around accuracy, stability, and dependency of these applications are rising. In addition, lack of attention to the clinicians’ acceptability, as well as the low impact on the medical professionals’ decision making, are posing more serious issues on the acceptability of smartphone applications. This article reviews smartphone-based decision support applications, focusing on hospital care settings and their overall impact of these applications on the wider clinical workflow. Additionally, key challenges and barriers of the current ubiquitous device-based healthcare applications are identified. Finally, this article addresses current challenges, future directions, and the adoption of mobile healthcare applications.
Keywords
Introduction
Ubiquitous devices such as tablets and smartphones, which are gaining more attention in every aspect of human life, are also playing an important role in healthcare delivery. 1 Smartphones provide the high computing power of a personal computer as well as the wireless connectivity of a mobile. Moreover, they are compact and have fast processing features and several in-built sensors, making them suitable for use in the healthcare setting. They can be employed for patient administration, billing, health information, making appointments, monitoring of laboratory results, and clinical decision support (CDS). It is beyond the scope of this review to cover all ubiquitous devices and applications in healthcare; instead, the focus will be on decision support and patient monitoring applications (apps) in hospital care settings.2,3
Mobile healthcare apps can be seen as the future of low-cost ubiquitous devices in healthcare and can be categorized as portable or data logging devices. Usually, the portable or wearable devices operate in conjunction with wireless body area networks or wireless personal area networks, as available communication technologies/medium. Additionally, apps for data logging medical devices (consumer and/or hospital grade) usually work with Bluetooth (BT) and wireless sensor networks for device-to-device integration to collate raw data from the human body using portable sensors.4,5
CDS apps are facing challenges in providing up-to-date and accurate information continuously at the point-of-care for clinical decision making. This becomes even more complex when there is no single best option and/or when decisions are based on real-time and patient-centered care.2,3,6
The success of smartphone-based CDS apps in hospital care settings is still debatable. 7 There are limited studies regarding the successful implementation and/or clinically trailed apps in wider hospital care settings. However, there are reports on the design, development (prototype), and accuracy (by simulation) in hospital care as well as other clinical and non-clinical settings, which lack system-related issues such as implementation, consultation, and user accessibility. Providing smartphone-based CDS is a challenging task, due to the limitations specific to mobile platform, interoperability application development, and various device–data integrations. 7
Materials and methods
An extensive search has been carried using major academic research databases, comprising Scopus, SpringerLink, IEEE Xplore, and PubMed for articles related to “smartphone healthcare,” “mobile healthcare,” “tablet health monitoring,” and “smartphone CDS apps.” We considered papers that discussed technical design, innovation, evaluation, or use of smartphones for healthcare professionals in hospital care settings and limited to “mobile decision support systems,” “ubiquitous devices,” and “ubiquitous healthcare systems.” Studies involving “tablet” related to medication were removed from the research. The search for articles was limited to “hospital” or “hospital care” or “secondary healthcare” or “smartphone health applications.” Articles dealing with advanced technologies and innovative methodologies, especially those focused on CDS, were considered. Furthermore, studies dealing with in-built sensors/feature applications within the CDS area were also included. Initially, the search yielded 76 articles, but 10 reviews and 44 articles (general sensing, fitness, activity, and non-hospital) were excluded. Finally, 22 potential studies from 2014 to 2016 were selected for this review based on the above inclusion and exclusion criteria.
Smartphone-based CDS applications
Smartphones are emerging as evidence-based tools designed to reduce clinical workflow and assist with clinician decision making and patient participation. 8 The International Patient Decision Aids Standards (IPDAS) has identified key components and standards of a high-quality patient decision aid. 9 Four basic features of most smartphone apps include (1) data sharing; (2) data organization (alerts, reminders, and history); (3) decision support/interpretation; and (4) user knowledge and support. These features of smartphone apps can be enhanced by integrating electronic patient health records into various mobile devices. 10
Four major areas of an overall healthcare system are key to enabling successful CDS applications (Figure 1).1,8,11,12 These areas are (1) structured information that includes standard and structured data (clinical information) such as coded problems of a patient available in the patient record, (2) information exchange that includes vast areas of cross-platform availability of various apps, (3) transformation that includes digital transformation from the traditional/manual methods, and (4) data analysis that interprets raw data into meaningful and actionable data via a smartphone application for supporting clinicians to make better decisions.
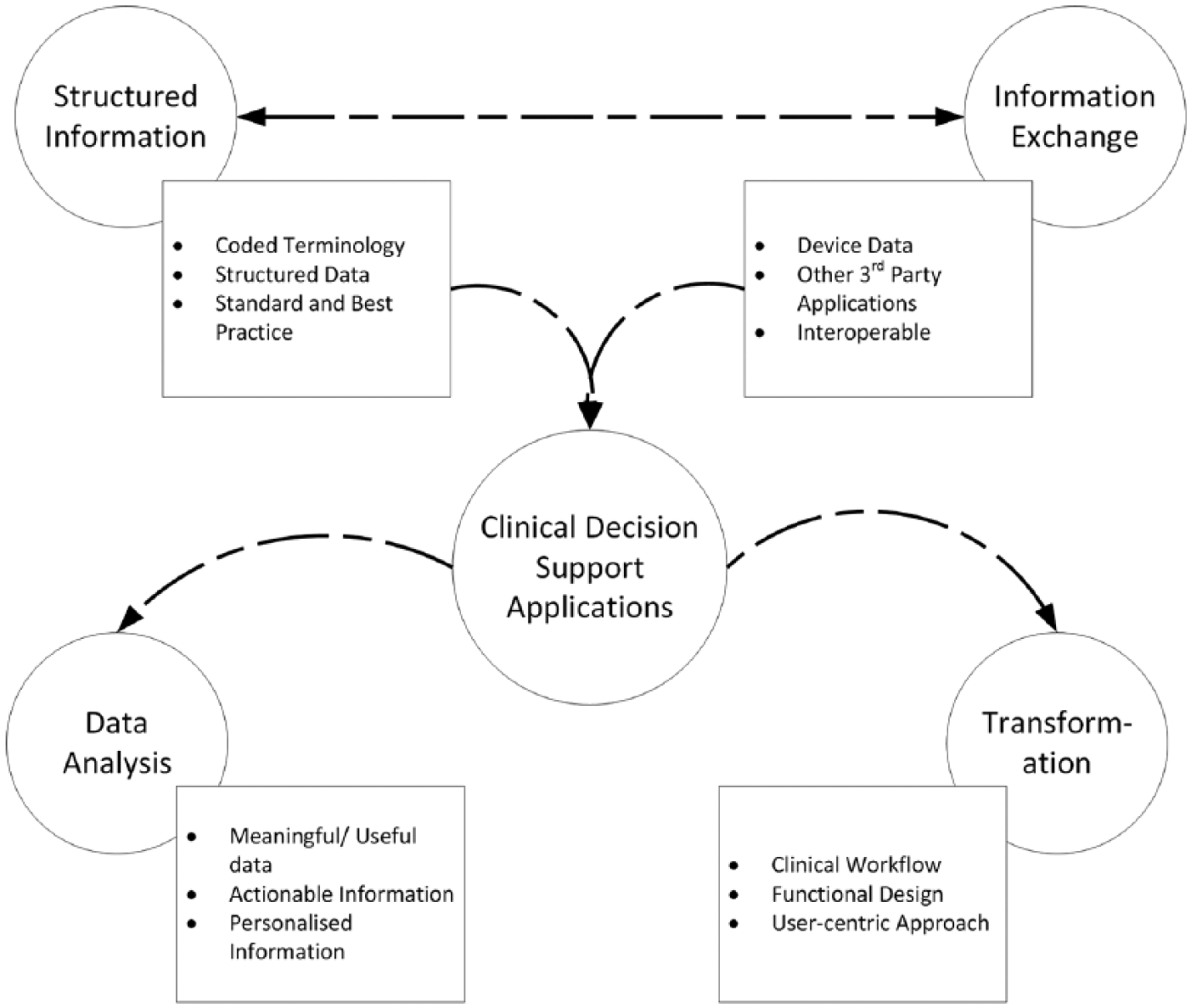
The four key areas required for efficient and functional smartphone CDS applications.
Structured information for mHealth applications
Digital health technologies, including electronic medical records (EMRs), imaging, e-prescribing and the increasingly prevalent use of connected devices to monitor health, have the potential to generate large amounts of data that could be of considerable benefit to researchers and policymakers if the data could be structured and coded.
CDS apps make use of the structured and coded data to assist clinicians by providing evidence so that they can make better and informed point-of-care decision. There are three processes required to achieve these benefits: unlocking value in EMRs, new forms of access that allow patients direct control, and pervasive computing and connected devices (m-health) to enable expansion of the “real-time” patient data. Unfortunately, reviewing tailored information with each patient is costly in terms of time and resources. 11 In an attempt to engage clinicians and patients during their hospital stay, a tablet application was developed to provide interactive information to patients.13,14 The application focused on providing the clinicians with meaningful data to make better decisions instead of pushing raw data which is of no use to the clinicians.13,14
Moreover, ubiquitous devices are useful to the clinicians if they provide the required flexibility and adaptability. 5 The exponential growth of the Internet, the application of smartphones in our daily lives, and the deployment of 4G networks should result in the provision of higher quality of healthcare services. However, the majority of the reviewed apps focused on data analysis, and on one specific, and/or early detection using complex gadgets, making these apps inefficient in non-specialized consultations. It is recommended that mobile apps need to be integrated with the electronic health records (EHRs), cloud storage, or data mining systems to multiply their efficiency and significantly improve the overall clinical outcome. 15
Digital transformation for CDS applications
In the contemporary era, digital technologies have become increasingly ubiquitous across all social institutions. The emergence of mobile digital devices such as smartphones, tablet computers, and wearable devices enables collection of massive digital datasets, knowledge production, and data mining. Manual article/hard copy–based “tools” and “scales” are being automated with easy to use graphical user interface (GUI) via smartphone apps to integrate advanced technologies into medical settings. For example, a smartphone wound care application 16 was developed to replicate the paper-based pressure ulcer scale for healing (PUSH tool), 17 Braden scale, 18 and the Bates-Jensen tool. 19 This system automated the existing tools and allowed clinicians create, view, access, delete, and re-assess patient records relating to wound care. Critical design considerations were given to the smartphone application, such as simplifying GUI, minimizing visual elements on any given screen to reduce clutter, and using color cues to focus information and converge critical information. The number of steps to complete a common task related to wound care were also significantly reduced using mobile tools. The application was developed for a Nexus 4 smartphone and Nexus 7 tablet and tested by eight nurses with an age range of 31–60 years. There was a very strong perceived correlation between the paper-based forms and the wound care application in terms of content and data entry expectations, with scores of 4.60/5.00 for the Braden Scale and 4.57/5.00 for the PUSH tool. 16
Future CDS apps must leverage existing capabilities from the sophisticated features (hardware and software) of the ubiquitous devices and integrate them with electronic patient health records. 20 Healthcare information could be uploaded to the cloud where observations from various ubiquitous devices would be integrated. 21 By utilizing data analytics and machine learning techniques, visualized trends or patterns embedded in massive data collected in parallel at runtime from millions of mobile devices could be explored for accurate and timely decision support.22,23 Smartphones, in contrast to personal computers, allow much needed “flexibility.” They are also characterized by mobility due to their size and weight, intuitive handling through touchscreen and gesture navigation, and low barriers relating to their operations and maintenance. 24 They offer an innovative concept of software delivery and offer state-of-the-art methods for service design and delivery in an organizational context. Smartphone’s advanced built-in sensors and features are understood to be one of the driving forces toward the global adoption of such technology in hospital care. 25
Data analysis using smartphone applications
The rapid emergence of apps, combined with the relative low-cost, high processing speed, and power of real-time data analysis, has resulted in the mHealth application adoption. 8 Data analysis and data interpretation techniques can be applied to provide insights for clinicians.
The high-resolution display of the tablet (Apple’s iPad™) performed equally to conventional desktop liquid crystal display (LCD) monitors in preliminary interpretation of emergent computed tomography (CT) brain exams after minor modifications were made to the tablet’s zoom function capabilities. 26 Sterile tablet computers have been successfully utilized in the operating room by neurosurgeons as a substitute for expensive commercial intraoperative imaging equipment for image guidance during tumor resection procedures. Another study found internal medicine residents (junior doctors) felt subjectively more efficient on the wards when they were provided with ubiquitous devices (iPad tablets) loaded with the hospital EMR access programme. 12
Sclafani et al. 27 reported that both tablet-owning and non-tablet owning physicians viewed the tablet computer as a useful educational utility and endorsed integration of the device into clinical practice and medical education/decision making. It is quite early to establish the success of smartphone application (especially their decision support capabilities) in hospital care settings. However, the literature suggests that mobile healthcare apps (using ubiquitous devices) are fast emerging as a decision support tool for clinicians in acute care settings. 27
Doty et al. 28 outlined a wrist-worn integrated health monitoring device that collected data from six bio-signals measuring, including fall detection, electrocardiogram (ECG), blood pressure, pulse oximetry (SpO2), respiration rate, and body surface temperature. This solution provided real-time information of the patient’s condition, such as vital bio-signals and location information. The developed system provided rapid and appropriate directions in emergency situations and alerted the user or caregiver to manage the changes in the patient’s health condition.28,29
In one study, 30 the authors proposed a system on falls prevention, detection, and biofeedback monitoring using ubiquitous devices. The system used infrared sensors or vision cameras to detect falls. It included a three-axis accelerometer motion system and smart shoes. The signals were measured and processed by a mobile device, allowing the analysis and diagnosis of the routine ambient-assisted living (AAL). To improve the accuracy of the proposed application, a frequency-adaptive sensor fusion method and a kinematic model were utilized to construct the whole-body motion in real time and were continuously updated for optimization. Starostenko et al. 31 described a system with four sensors, including ECG, three-axis accelerometer, temperature, and tight-switch, which enabled remote monitoring. The ECG, measured with wearable electrodes, used steel textile to generate the real-time heart-rate estimator. The tight-switch sensor and filter impulse response (FIR) filter technology were applied to get the best heart-rate accuracy. Moreover, the device had low-power consumption to transmit detected bio-information from these four sensors. Such transmission makes this device highly suitable for apps such as remote healthcare and wellness monitoring. 31 Table 1 summarizes ubiquitous healthcare systems with CDS features.
Ubiquitous healthcare systems with clinical decision support (CDS) features.
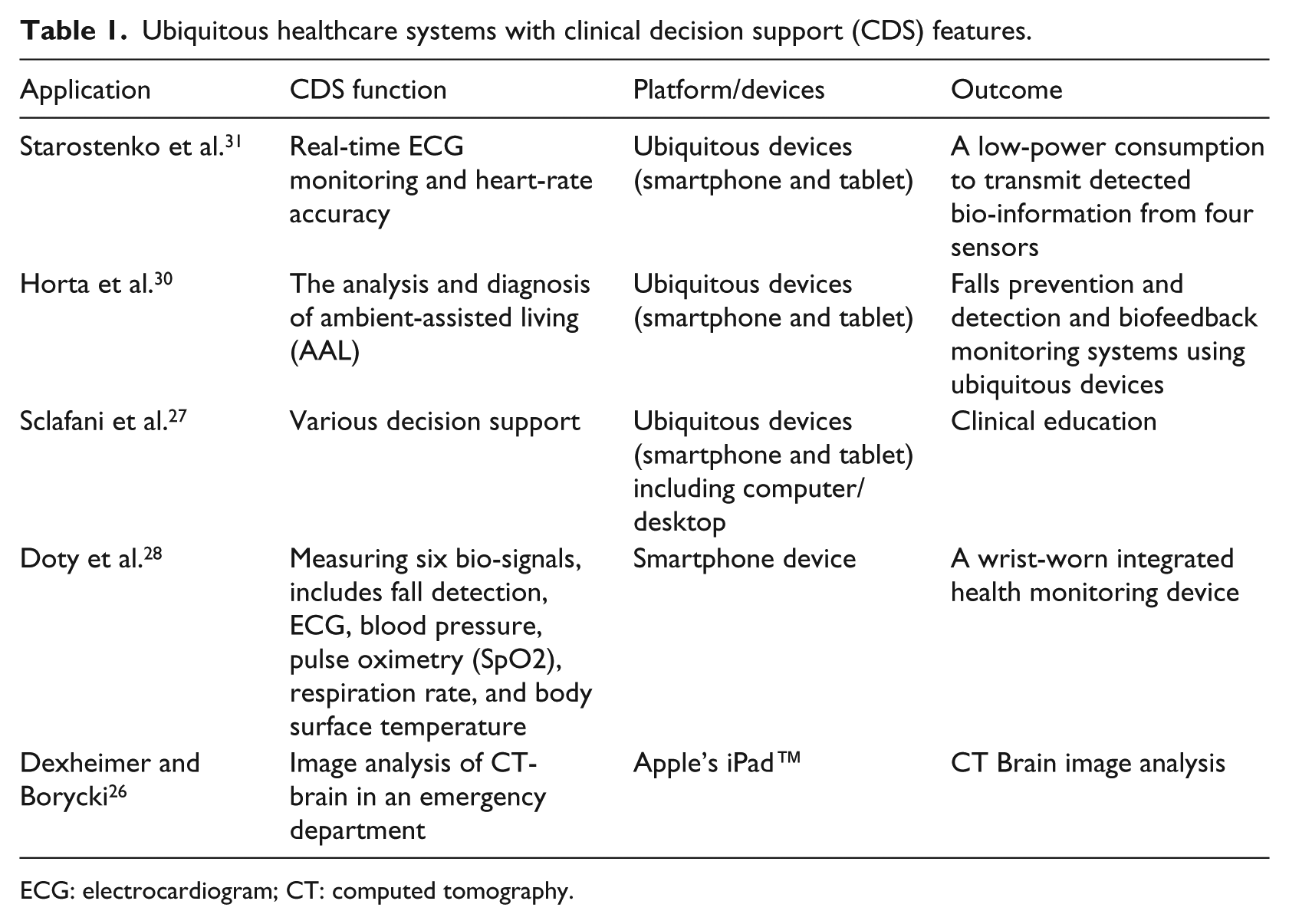
ECG: electrocardiogram; CT: computed tomography.
Current issues and challenges of smartphone applications in hospital care settings
In the past 30 years, there have been significant advances toward decision support tools, initially with paper-based manual tools, scales, scores, and charts gradually transferred into computerized and semi-automated systems. 32 Currently, emerging mHealth apps are being fully integrated with the EHR systems to support clinicians in their decision making. Despite the significant advances in decision support technologies, there are still gaps remain that prevent the wider adoption in healthcare settings. 33 Health innovations using the latest technologies and techniques offer great advantages, but at the same time, they pose security and privacy threats to the patients’ personal information, clinician and end-user acceptability, data storage, data access, and data organization and processing. 6 In addition, data processing on a local device impacts the device’s battery life, and this is currently one of its greatest drawbacks. 34
In the context of this review, we sought to identify critical issues related to decision support systems. Therefore, we excluded common smartphone-/tablet-related issues which have been previously extensively covered by other researchers, for example, power consumption, 2 battery life,35,36 user acceptance, 37 and clinical data security and privacy.3,38 Instead, we focused on issues related to decision support capability and their acceptance in hospital care settings, data processing and analysis,39,40 and information exchange, as required for optimal integration of mHealth apps. Smartphone apps and their issues and challenges are shown in Figure 2. The major issues and challenges can be categorized into four main divisions: (1) clinician/user consultation, (2) transmission and processing, (3) data integration, and (4) design and development, as discussed below.
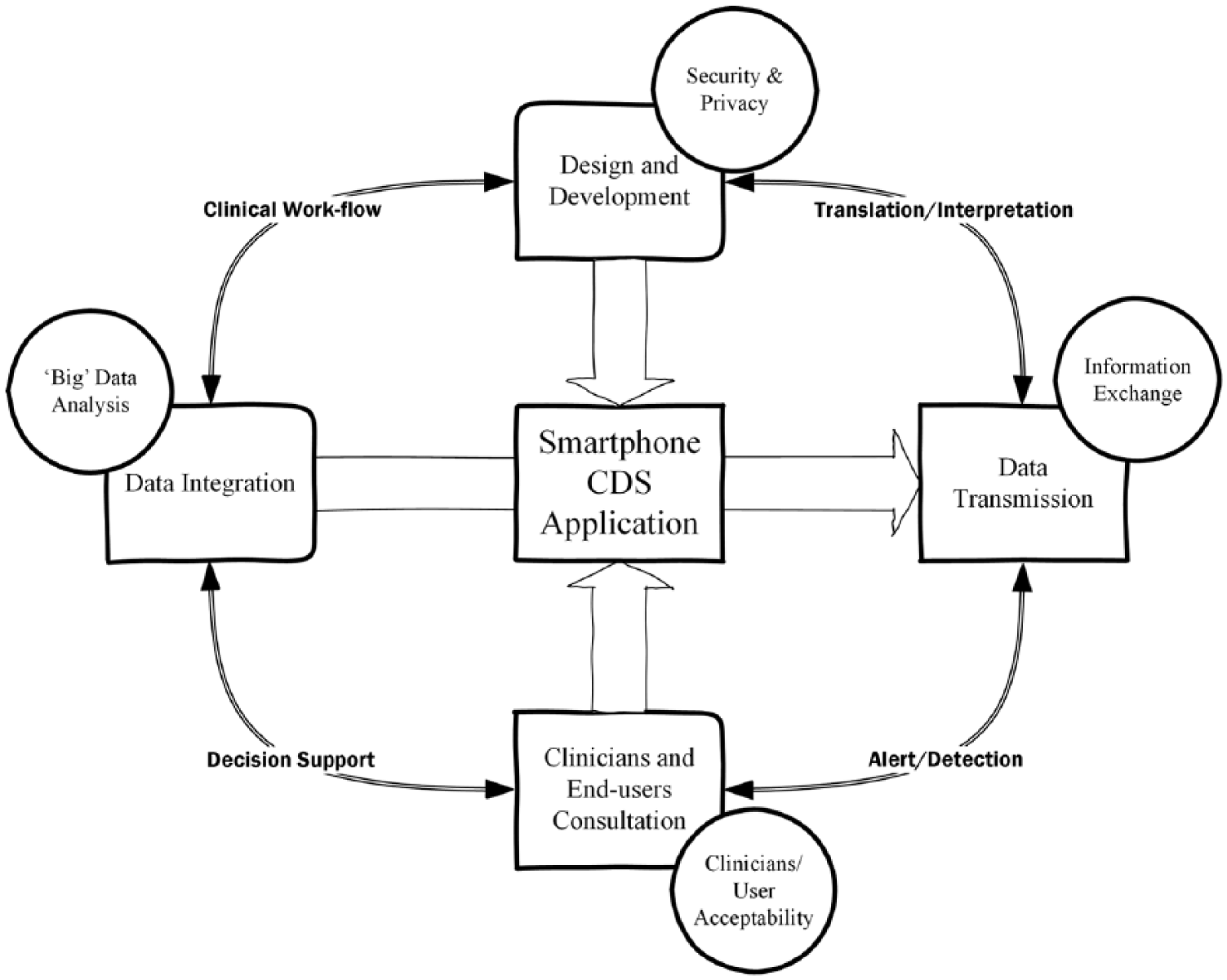
Smartphone applications and their issues and challenges.
Data processing and “big” data analysis
Medical standards compel the use of high-quality data in mHealth apps for high accuracy and reliable communications. 41 Various techniques have been applied to collect high-quality health data.7,42,43 Examples include a novel unbiased and normalized adaptive noise reduction application to suppress random noise in ECG signals, which includes two-stage moving-average filter, an infinite impulse response comb filter, an additive white noise generator to test the system’s performance in terms of signal-to-noise ratio, 44 a low-cost online acquisition of ECG signal using MATLABTM and LabVIEWTM and time-plane feature extraction from digitized ECG samples that uses a statistical approach, 45 a mobile-based physiological parameter detection and analysis algorithm 46 ARTiiFACT, a tool for collecting real-time ECG data from integrated sensors and mobile platform to directly collect and analyze the data, 47 ECG signal processing and digital filtering on 8-bit microcontroller, 48 and a mean shift-based self-adaptive model. 49
Personalized and predictive medicine can greatly benefit from data integration and its machine learning model (big data analytics). 39 Today, most health systems use a combination of rules-based approaches, as well as manual methods, to best interpret medical data. Big data analysis seems to be a solution for rapidly increasing medical data resulting from the increased use of electronic medical devices and storing of digital data. However, big data analysis is at an early stage and needs more time to achieve clinical acceptance. 39
Data processing can be broadly classified into two categories. First, data analysis and processing methods implemented on a smartphone in real time with dense impact on the devices’ battery life. Mostly, such apps cannot be implemented as continuous monitoring apps due to their large power consumption. Moreover, due to the limited hardware and processing powers of the device, sophisticated data processing and interpretation are limited when compared with high-end personal computers. 50 Second, collected data are being pushed to cloud-based services for processing, and only alerts are transmitted back (generated by the cloud-based apps) and pushed to various other devices. In such apps, the alert will be delayed depending upon Internet connectivity and cloud-processing capabilities, that is, medical decision support rules set up in the cloud.51,52
Security and privacy
The privacy and security of healthcare data are of the highest importance, especially when healthcare apps deal with personal health data or store patients’ health records, vitals, or laboratory results. Security issues can be classified into two categories: system security and information security. Ng et al. 53 have classified threats and attacks into two major categories—passive and active. Kargl et al. 54 and Williams 55 have discussed the mHealth apps security and privacy in detail and highlight the types of privacy attacks as modification of medical data; forging of alarms on medical data; denial of service, location, and activity tracking of users; physical tampering with devices; and jamming attacks.
A number of security and privacy frameworks have been developed, designed, and tested for their reliability in mHealth apps, and 22 free web-based personal health record privacy and security policies have been analyzed by Carrión et al. 56 These researchers reported that a high level of user’s security occurs with apps such as Google Health, ZeabraHealth, Keas, and Microsoft HealthVault.38,57–59 Various recent reviews and recommendations on security and privacy of mobile healthcare applications have been published.60–63
Data transmission and information exchange
Mostly, mHealth apps are developed to be either web based or local smartphone based. 64 In both cases, they can be connected to another software (service) for transfer of information. 65 However, the local application usually lacks data integration capabilities with other clinical databases to fetch patient data for processing; they mostly relay on local patient data and are limited to analyze specific localized issues. Local machine-based apps have the advantage of patients’ information security and privacy, but have two critical drawbacks: memory space and limited historical patient data access. 4 However, fully connected apps have the advantage of analyzing wider patient data from other data repositories in order to predict/interpret decision support. Such apps are usually connected to cloud-based environment for information transmission but do require additional information and communications technology (ICT) infrastructure with cost implications at the initial stage. The cloud-based architecture raises issue with privacy and security of patients’ personal information. 38 It is suggested that there should be balance between clinical use and ICT dependence for mHealth apps. For example, if the medical device or hospital Internet connectivity fails, then the entire application is unusable by the clinicians because the data are stored in the cloud due to the smartphone/tablet’s limited space.4,66
It is recommended that in limited resource settings, it is optimal to use the local smartphone application for the specific healthcare area so that huge ICT-related costs could be saved. 67 Wilcox et al. 68 attempted to minimize such barriers using advanced data encryption processes where data are encrypted on the tablet computer before being transmitted to the cloud server and data were only decrypted after being retrieved by the target organization. To address the issue of integration/connectivity, the study 68 used a local application on the device rather than using the tablet computer as a browser for web-based forms. This reduced workflow issues because of connectivity, but also carried the risk of storing information on the device. 68 Again, this illustrates the importance of ICT infrastructure being able to store and handle huge amounts of incoming patient data. However, storing information on the hand-held device introduces the risk of losing the device (easier to lose the smartphone device than desktop work station) and one cannot physically steal or lose the cloud.
Clinician and end-user consultation
The design of effective mHealth apps is becoming increasingly important. mHealth apps continue to increase, but with little evidence for their effectiveness being shown in clinical outcomes. 69 Many current mHealth interventions are based on existing/traditional healthcare models and may not be as effective as those that involve end-users in the design process. 70 Apps need to be produced with adequate consideration of the needs of their intended users so that they become easy to use and perceived as useful.69,70 Clinician and patient-centric design thinking is required in the initial phase of app design. One of the common scenario of the basic mHealth app requirement is the reviewing of laboratory results with a patient by showing them data from their EHR using patient apps. 71 Thus, an app may enhance the provider–patient experience rather than detract from the overall interaction. An added benefit from such interactions is the ability to transmit educational materials right from a practitioner’s device to the patient, thus reducing the transfer of paper and increasing the likelihood of it being retained for access by the patient. User-centered design is essential in order to incorporate these perceptions into the end-user product, especially at the earlier stages of the project development. 72 When considering the user’s needs, the solution designer should consider a number of factors such as task analysis, surveys, interviews, and focus groups to address user acceptability issues. 73 Highly sophisticated data analysis techniques will become irrelevant if users do not understand the operation and its user interface. 74
Discussion
Clinical workflows such as nursing documentation, inpatient communication tools, and patient health records are required to be connected to the wider healthcare delivery ecosystems for efficient clinical outcomes. The smartphone-based CDS apps could be seen as a potential standard/best practice tools that will help clinicians to deliver better and more accurate outcomes. The app design, implementation, and evaluation of such platforms require platform rigorous and systematic workflow methodologies. Zheng et al. 75 identified that there is a discrepancy across the findings of health information technology (IT) studies in terms of their impact on workflow. As they speculated, the discordance may be due in part to oversimplified workflow modeling practices. The patient-orientated workflow methodology and the available automated tool can assist researchers with collecting data that can greatly help clinicians in decision making.4,66,74 Ng et al. 76 recommended five main characteristics of smartphone apps in order for them to be clinically acceptable: (1) information exchange to support such apps, (2) evaluation of apps including testing and user training, (3) careful planning to develop robust and safe application, (4) stakeholder involvement toward decision support tools, and (5) traditional face-to-face interaction should not be reduced or compromised and final decision making should be based on the clinicians’ experience and knowledge and not solely technology-driven. Current smartphone apps can accurately support the time-based actions such as alerts, reminders, notifications, and warnings. These apps can be considered to be a reliable data collector and transmitter tool which supports the structured data collection and storage. However, most of the healthcare apps lack other system integration, have poor execution of CDS, and have low user acceptance and also lack of implementation in the hospital care setting.8,42,71
It is now widely believed that younger generations have been exposed to technology from an early age and a large percentage of their education has utilized some level of technology exposure. Therefore, they exhibit favorable attitudes toward innovative technology, thus resulting in its rapid adoption. 77 A study revealed that new technology was initially utilized in hospital care, because it was popular in the workplace among other colleagues. It was not until the device was used for some time in practice that experienced medical professionals recognized its full potential (when compared to younger medical professionals). It is also possible that due to their greater knowledge and experience, they needed these devices less than their younger colleagues. Due to this technological exposure, it may be assumed that less experienced (younger) physicians are more rapidly adopting smartphone technology into hospital care/clinical practice than other more experienced medical professional.78,79
Conclusion
Three common issues are currently facing the wider mHealth application domain. First, smartphone apps are being tested/evaluated in hospital care settings involving senior clinicians. Second, there is a need for the continuous involvement of medical professional and end-user in the app design. Third, accurate data analysis and interpretation can be provided to the medical professional via smartphone application in a reasonable time frame. Existing studies have emphasized the smartphone’s efficiency as a communication and educational tool, a reference source and a decision resource for both patients and healthcare providers.7,27 Furthermore, recent survey results have demonstrated a positive patient perception of physicians who use smartphone apps in the clinical setting regardless of patient age, race, gender, or income.74,80
This review also provides an overview of the literature on a broad range of smartphone healthcare apps in hospital care settings. Most of the systems described are either in their development stage or simulation stage but not actually implemented in the hospital care (except systems conducted clinical trials). Further focused research is required in such apps with respect to their clinical implementation, end-user acceptability, evaluation by medical professionals, and security and privacy.
However, the complexity of CDS computation requires a significant amount of processing power during data analysis and executing the decision support algorithms/models. Such models do not permit direct utilization of ubiquitous devices supporting healthcare services due to their limitations. Therefore, instead of complex data processing, either simplified algorithms are suggested to apply on the device or only alerts/notifications should be pushed on the device.
We have identified two core “areas of concerns” related to smartphone computer technology. First, clinicians and patients are the underused resources in smartphone apps design and development. Early collaboration between developers, clinicians, and the target users is critical if the successful healthcare apps are successfully implemented in the hospital care setting. Second, the appropriate use/representation of data including data analysis, interpretation, translation, integration, and processing should be transparent and presented to the medical professional in a simple and easy format. Due to the “big data” coming from multiple eHealth sources, it is now a critical task to represent the raw data in a way that is as meaningful/useful as possible to the clinician. In this way, decision support can be enabled efficiently and in real-time. Currently, most systems lack clinical or secondary care implementation. Very few apps are available today which incorporate and address critical aspects such as design, development, implementation, and user/clinicians collaboration.
Footnotes
Declaration of conflicting interest
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.