
Abstract
Inter-hospital transfers improve care delivery for which sending and receiving hospitals both accountable for patient outcomes. We aim to measure accuracy in recorded patient transfer information (indication of transfer and hospital identifier) over 2 years across 121 acute hospitals in New South Wales, Australia. Accuracy rate for 127,406 transfer-out separations was 87 per cent, with a low variability across hospitals (10% differences); it was 65 per cent for 151,978 transfer-in admissions with a greater inter-hospital variation (36% differences). Accuracy rate varied by departure and arrival pathways; at receiving hospitals, it was lower for transfer-in admission via emergency department (incidence rate ratio = 0.52, 95% confidence interval: 0.51–0.53) versus direct admission. Transfer-out data were more accurate for transfers to smaller hospitals (incidence rate ratio = 1.06, 95% confidence interval: 1.03–1.08) or re-transfers (incidence rate ratio > 1.08). Incorporation of transfer data from sending and receiving hospitals at patient level in administrative datasets and standardisation of documentation across hospitals would enhance accuracy and support improved attribution of hospital performance measures.
Introduction
Inter-hospital transfers (IHTs) are essential components of a healthcare system aiming to improve access and efficiency in care delivery. 1 Patients requiring more sophisticated care are transferred to hospitals with more capacity or level of specialisations. 2 Although IHTs generally result in better health outcomes for patients, 3 transferred-in patients have elevated service burden and risk of death compared to directly admitted patients at the receiving hospital,4,5 suggesting in-transfer as an independent risk factor for mortality.6,7 Consequently, in performance profiling, several national and regional agencies (e.g. in Canada and Australia) include transfer status in patients case mix for deriving hospital quality indicators based on administrative hospital datasets.8,9 Moreover, attributing performance measure to sending and receiving hospitals is desirable to accurately assess hospitals’ contributions.10,11 The accuracy of transfer information (that includes indication of a transfer for transferred patients and a hospital identifier) in hospital data, although unknown, is essential as under-recording of these data at sending and receiving hospitals can introduce biases in recognising attributions of hospitals, their contributions to patient outcomes, and efficiency of the hospital through partnership.10,12
We aim to measure accuracy of transfer data at hospitals transferring patients to another hospitals (transfer-out) or receiving patients (transferred-in) from other hospitals and associated variability among hospitals, and contribution of patient, admission, and hospital-related factors on the accuracy. We used record-linked data within a 2-year period for all admitted patients in all public acute-care hospitals across New South Wales (NSW), Australia.
Methods
Data source and study population
NSW, the largest health jurisdiction in Australia, has over seven million residents and approximately 500 healthcare facilities with up to three million admissions per year. We used two data sources that are linked – Admitted Patient Data Collection (APDC) and Emergency Department Data Collection (EDDC) – to capture all NSW hospital separations (admissions) and public hospital emergency department (ED) presentations. Records were extracted for 2013–2015 (all admissions from 1 July 2013 to 30 June 2015) from all healthcare facilities in NSW. Record-linked APDC and EDDC use a unique patient identifier to link patient-specific data. 13
We obtained linked records from the NSW Admitted Patient, Emergency Department and Deaths Register, which was established under the public health and diseases registers provisions of the NSW Public Health Act 2010 and is maintained by the Centre for Epidemiology and Evidence (CEE), NSW Ministry of Health. Record linkage was carried out by the Centre for Health Record Linkage. 13 The data were accessed remotely through Secure Analytics for Population Health Research and Intelligence (SAPHaRI) system made available by the CEE. 14 The datasets included 5,085,831 admissions and 4,647,918 ED presentations for 3,331,956 patients in all NSW acute-care hospitals.
Transfer identification and characteristics
We collapsed APDC and EDDC datasets (all hospitals), sorted by arrival time, and utilised both discharge and arrival information of consecutive records for each patient to identify an IHT, the sending and receiving hospitals, and patients/transfer pathways (arriving and departing units). 15
For admitted patients, a transfer-out is recorded in ‘separation mode’ and ‘transferring to’ variables, with values indicating a transfer to another hospital and the receiving hospital identifier, respectively. A transfer-in is recorded in ‘source of referral’ and ‘transferring from’ variables. For non-admitted IHT patients (ED presentation not admitted), hospital identifiers are not recorded.
Using the combined and time ordered dataset, for each patient, all records (index) with an indication of transfer to (from) another hospital were coupled with the subsequent (preceding) records from a secondary hospital and defined as an IHT, if records from the secondary hospital either indicated transfer-in (from), or had an arrival (departure) time within 24 h of the departure (arrival) time of the index record. Records with these indications of a transfer and correct hospital identifier (for admissions only) were considered accurate. Consistent transfer-out and transfer-in data were considered as concordant. IHTs from/to private hospitals (due to inconstancy in coverage over the study period), non-NSW hospitals, non-acute or sub-acute centres, and children’s hospitals were excluded. Incomplete IHTs among public hospitals (sending hospital with no receiving hospital or vice versa) were also excluded (Figure 1).
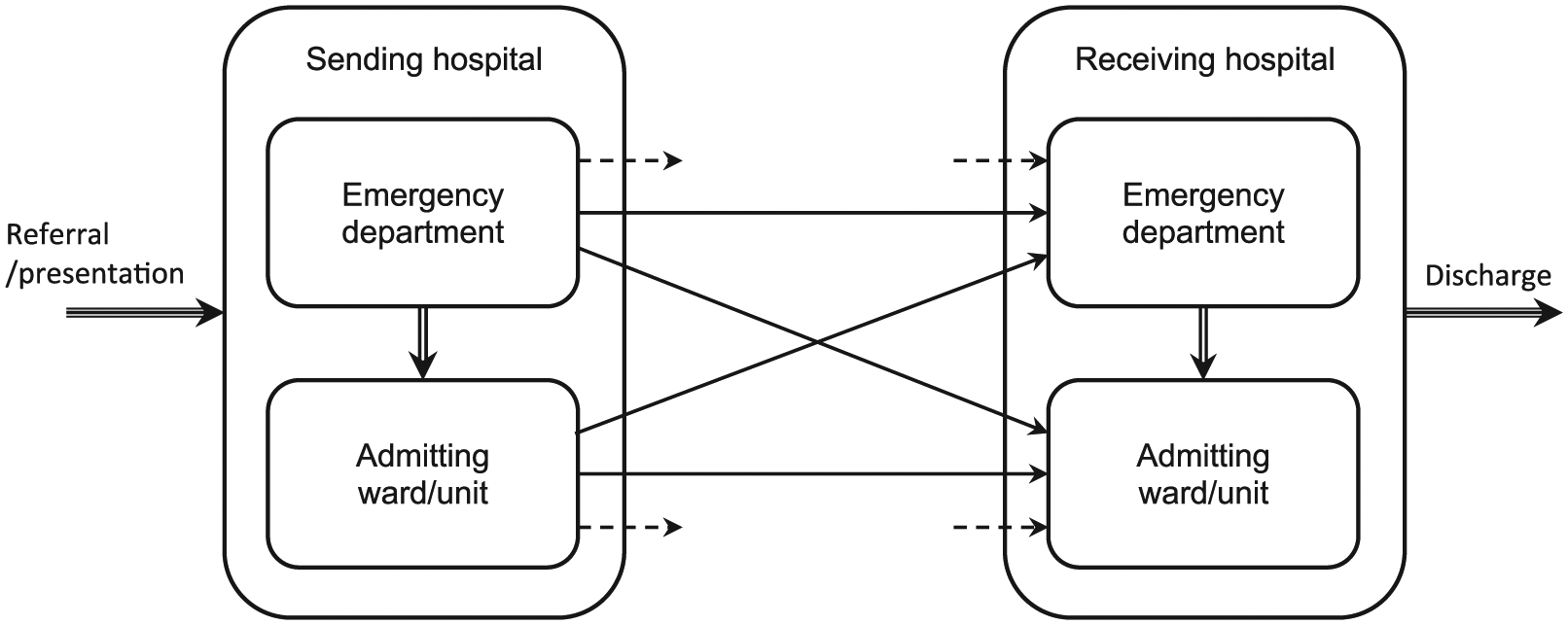
Schematic diagram of inter-hospital transfer pathways.
We assessed three sets of covariates – patient, hospital, and transfer-related factors – for admitted patients’ records only. Patient factors included demographics (age, sex), Charlson comorbidity score 16 based on ICD-10-AM, Eight Edition, 17 length of stay at both sending and receiving hospitals, and survival at receiving hospital. Hospital characteristics included hospital location (metropolitan vs rural), peer groups which range from A1: principal referral hospitals, >35,000 admissions per year and offering highly specialised services; B1: major group 1 hospitals, 17,000–35,000 admissions per year and offering more than one specialised service; B2: major group 2 hospitals, 10,000–35,000 admissions per year and without specialised services; C1: district group 1 hospitals, 4000–10,000 admissions per year; C2: district group 1 hospitals, 2000–4000 admissions per year; D1a: community hospitals with surgery, 200–2000 admissions and >2 per cent surgery per year; D1b: community hospitals without surgery, <2000 admissions and <2 per cent surgery per year, 18 numbers of transfers and number of interacting hospitals (categorised into quartiles). Transfer characteristics were timing of IHT departure and arrival, transfer type based on peer groups (upwards: smaller to larger hospitals, downwards: larger to smaller hospitals, sidewards: between similar-sized hospitals), separation type (re-transferring status) at sending hospitals, pathway (ED presentation: no admission to ward, direct admission to ward: no ED involvement, and admission via ED: ED presentation followed by admission to ward) at sending and receiving hospitals and transfer within versus between local governance bodies (local health district (LHD) in NSW).
Statistical analysis
Negative binomial mixed models were employed to assess factors influencing accuracy of transfer data at sending and receiving hospitals and to quantify associated inter-hospital variations in rates. Incidence rate ratios (IRRs) were reported for factors’ effects derived from a model with all covariates. Median incidence rate ratios (MIRRs) 19 were used to translate variations into risk differences. MIRR is the median of the accuracy rate ratios that could be obtained by comparing two transfer records with identical characteristics taken from two randomly chosen hospitals. Proportional changes in MIRRs were reported for multiple models to examine the contribution of case mix and hospital-related factors on reporting of transfers. Hospital-specific adjusted rate ratios for transfer-in and transfer-out data were derived from the estimated random intercept components of the mixed models and examined. Data preparation was conducted in SAS Enterprise Guide version 6.1 20 through SAPHaRI 14 and analyses were performed in R package version 3.1.2. 21
Results
We identified 164,554 IHTs among 121 NSW public acute hospitals within a 2-year period (Table 1). Approximately, half (53%) of the transfers were for patients who were initially admitted via ED; a further one-fifth (23%) were ED presentations who were transferred without being admitted. At the receiving hospital, most (54%) patients were direct admissions; approximately one-third (39%) were admitted via ED, and less than one-tenth (8%) were discharged from ED without being admitted.
Accuracy of transfer data varied significantly across pathways and sending and receiving hospitals. The most (82%) and least (24%) accurate data, that is, concordance between transfer-out and transfer-in data was for admission via ED to direct admission, and ED presentation to admission via ED pathways, respectively (Figure 2). Data accuracy was higher for transfer-out (87%) than transfer-in (65%), (Table 2). For transfer-out, it was higher for patients who were admitted via ED (IRR = 1.54 vs direct admission), and those who were directly admitted at receiving hospitals (IRR = 0.85 for ED vs direct admission). For transfer-in, it was highest for patients who were directly admitted at sending (IRR = 0.66 and 0.93 for ED presentation and admission via ED vs direct admission, respectively) and receiving (IRR = 0.52 for admission via ED vs direct admission) hospitals. Further analysis revealed ED was recorded as the source of referral in 73 per cent of inaccurate transfer-in data for patients admitted via ED.
Distribution of inter-hospital transfer pathways across NSW public hospitals during 2013–2014FY.
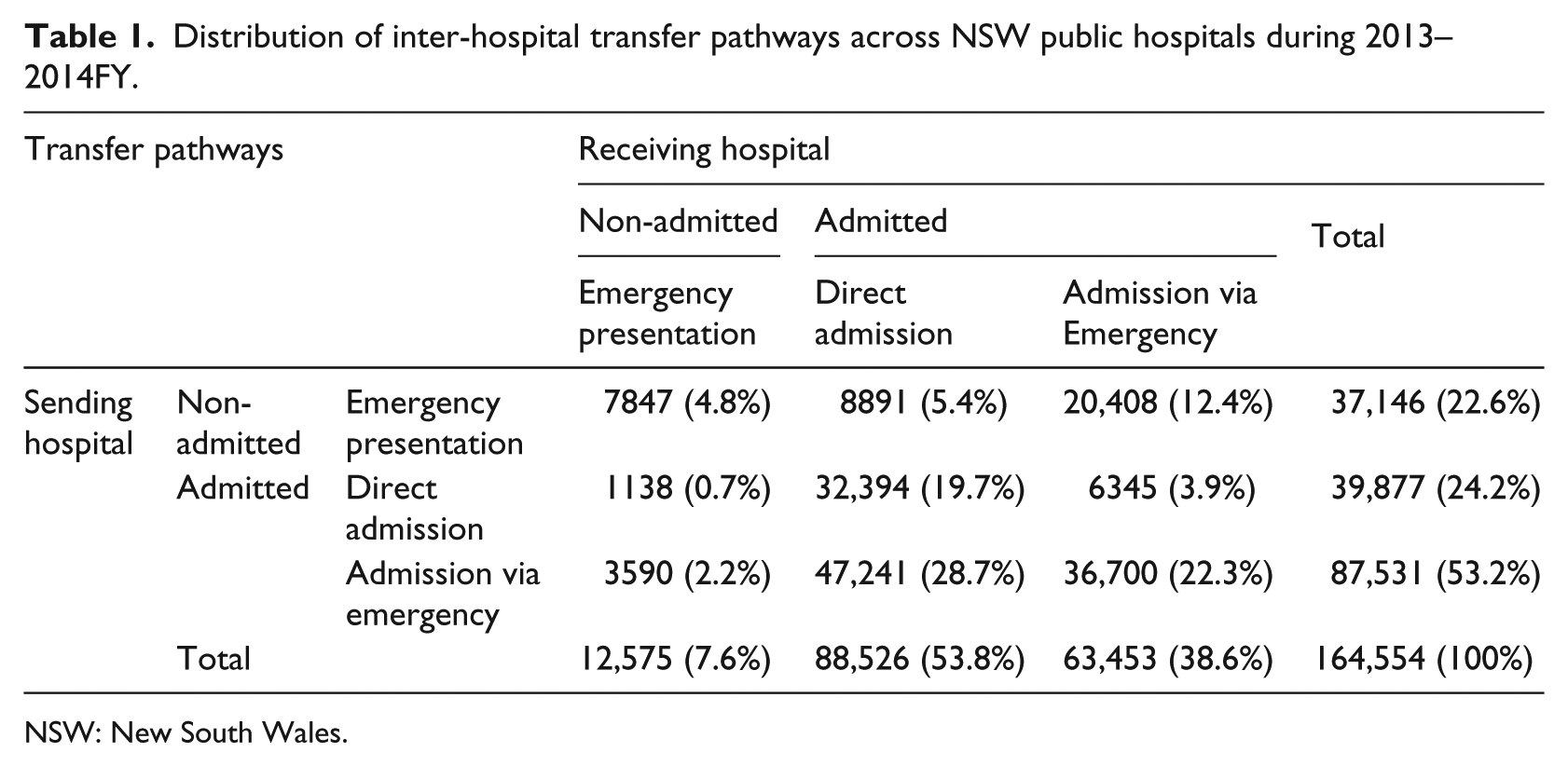
NSW: New South Wales.
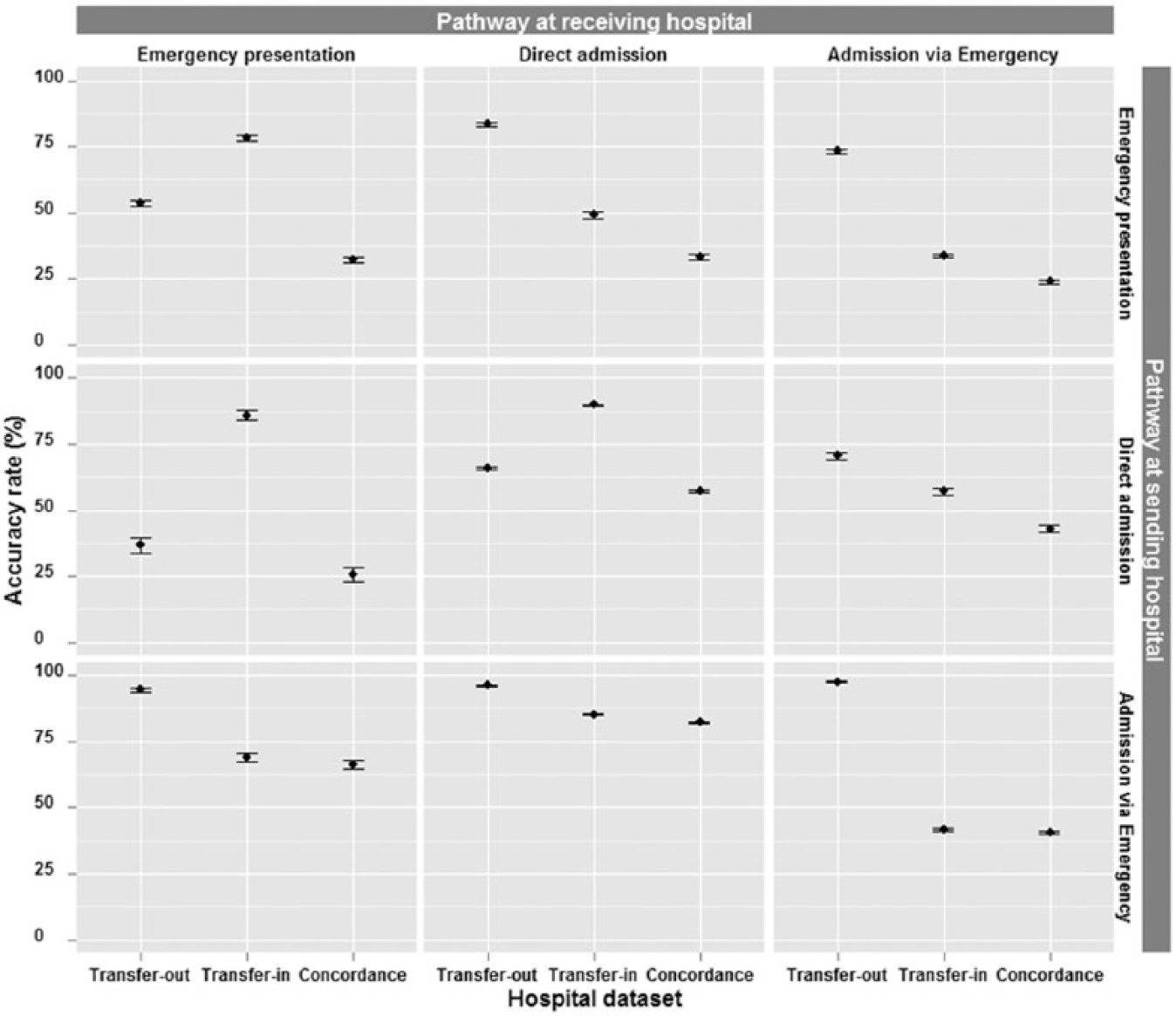
Accuracy rate of transfer data (in, out, and associated concordance) stratified by pathway across NSW public hospitals. Note that accuracy rate for emergency presentation is based only on indication of transfer as hospital identifier does not exist.
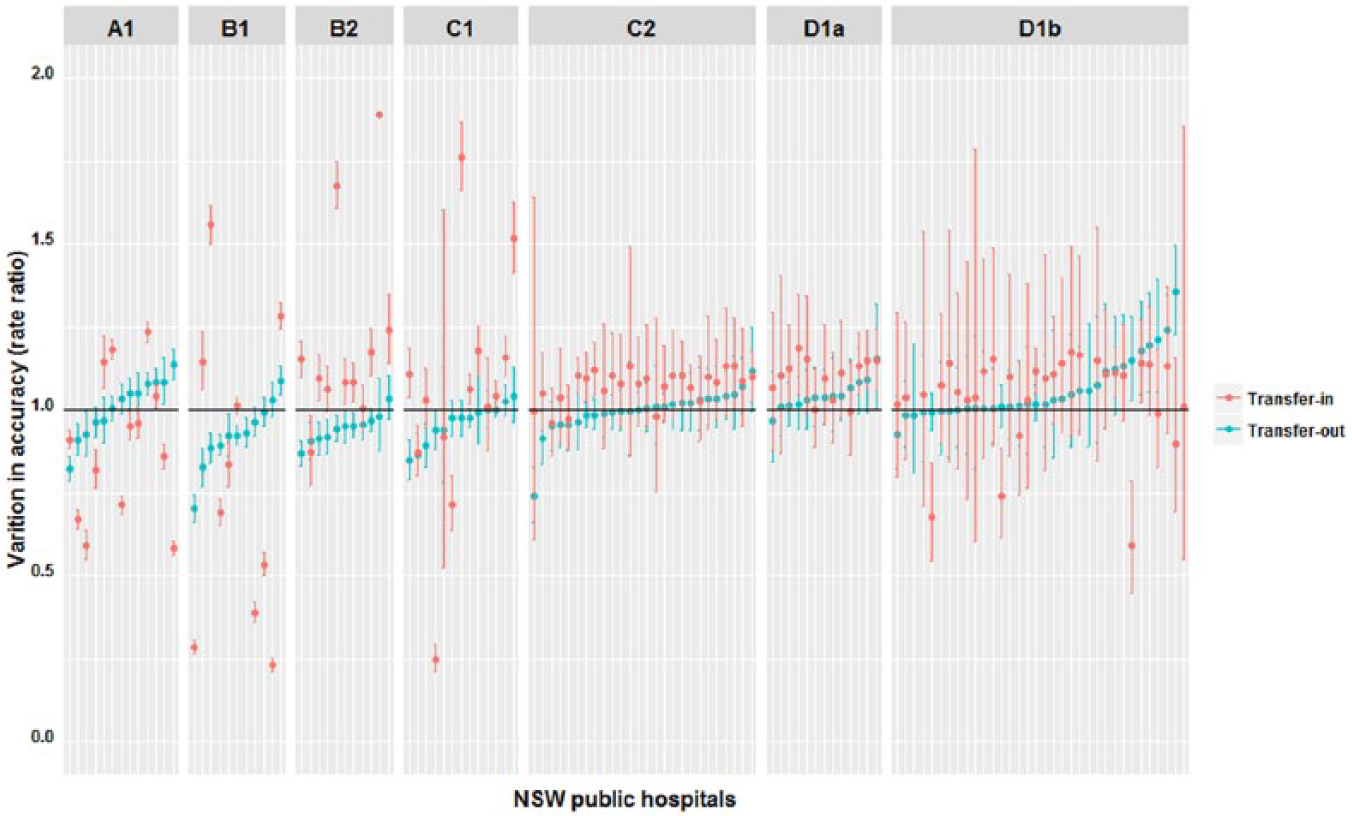
Variation of adjusted accuracy rate ratios (compared to average) for transfer-out and transfer-in data across NSW public hospitals clustered by NSW peer groups.
Accuracy rate was moderately associated with patient characteristics (Table 2). Data accuracy was higher for transfers that occurred before or after the daylight shift (8:00 a.m.–4:00 p.m.), on weekends, from larger to smaller hospitals (down-transfer), and for patients who were experiencing a second transfer, that is, a re-transfer (IRR > 1.08).
Variation in the accuracy rate of transfer-out data across all hospitals (MIRR = 1.10, 10% difference) and within peer groups (up to 11%) was low, with only 3 per cent of the variation explained by covariates (Figure 2 and Table 3). On the other hand, it varied significantly for transfer-in data across hospitals (MIRR = 1.36, 36% differences) and within peer groups (between 5% and 96%), with only 12 per cent of the variation explained by covariates (Table 3). Compared to large principal referral hospitals, transfer-out data accuracy was lower in major group 1 (IRR = 0.91) (Table 2). For transfer-in data, accuracy was higher in major group 2 (IRR = 1.38) and smaller hospitals of district group 2 (IRR = 1.27) and community with surgery hospitals (IRR = 1.30), but varied notably among major group 1 (MIRR = 1.97) and district group 1 hospitals (MIRR = 1.55). Transfer density and number of interacting hospitals had no effect on data accuracy. No strong association between accuracies in transfer-out and transfer-in at hospital level existed as depicted in Figure 3.
Accuracy of transfer data and associated patient, transfer and hospital characteristics rates, and ratios for transfer patients between public NSW hospitals, 2013–2015.
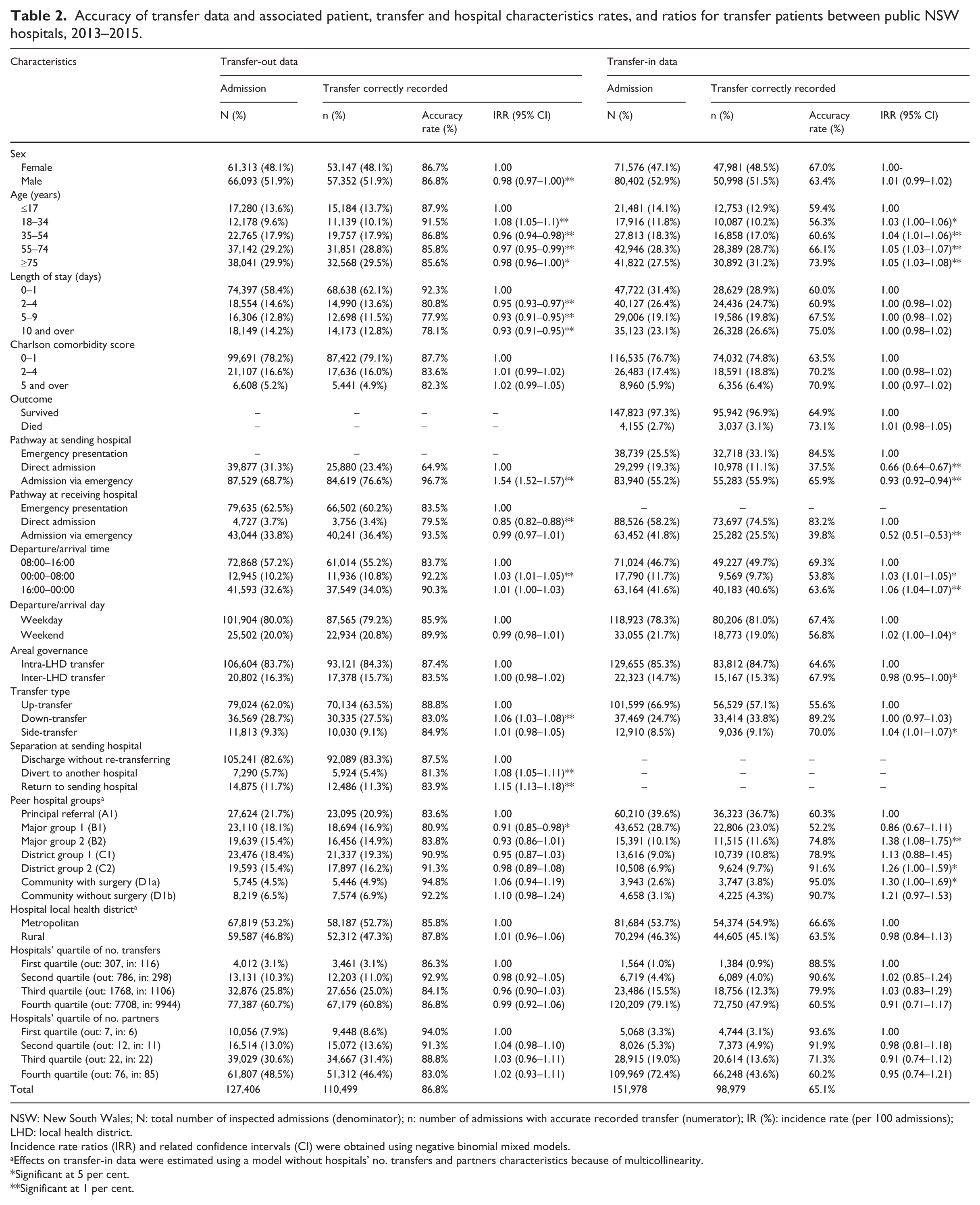
NSW: New South Wales; N: total number of inspected admissions (denominator); n: number of admissions with accurate recorded transfer (numerator); IR (%): incidence rate (per 100 admissions); LHD: local health district.
Incidence rate ratios (IRR) and related confidence intervals (CI) were obtained using negative binomial mixed models.
Effects on transfer-in data were estimated using a model without hospitals’ no. transfers and partners characteristics because of multicollinearity.
Significant at 5 per cent.
Significant at 1 per cent.
Inter-hospital variation in accuracy of transfer data across NSW public hospitals, 2013–2015.
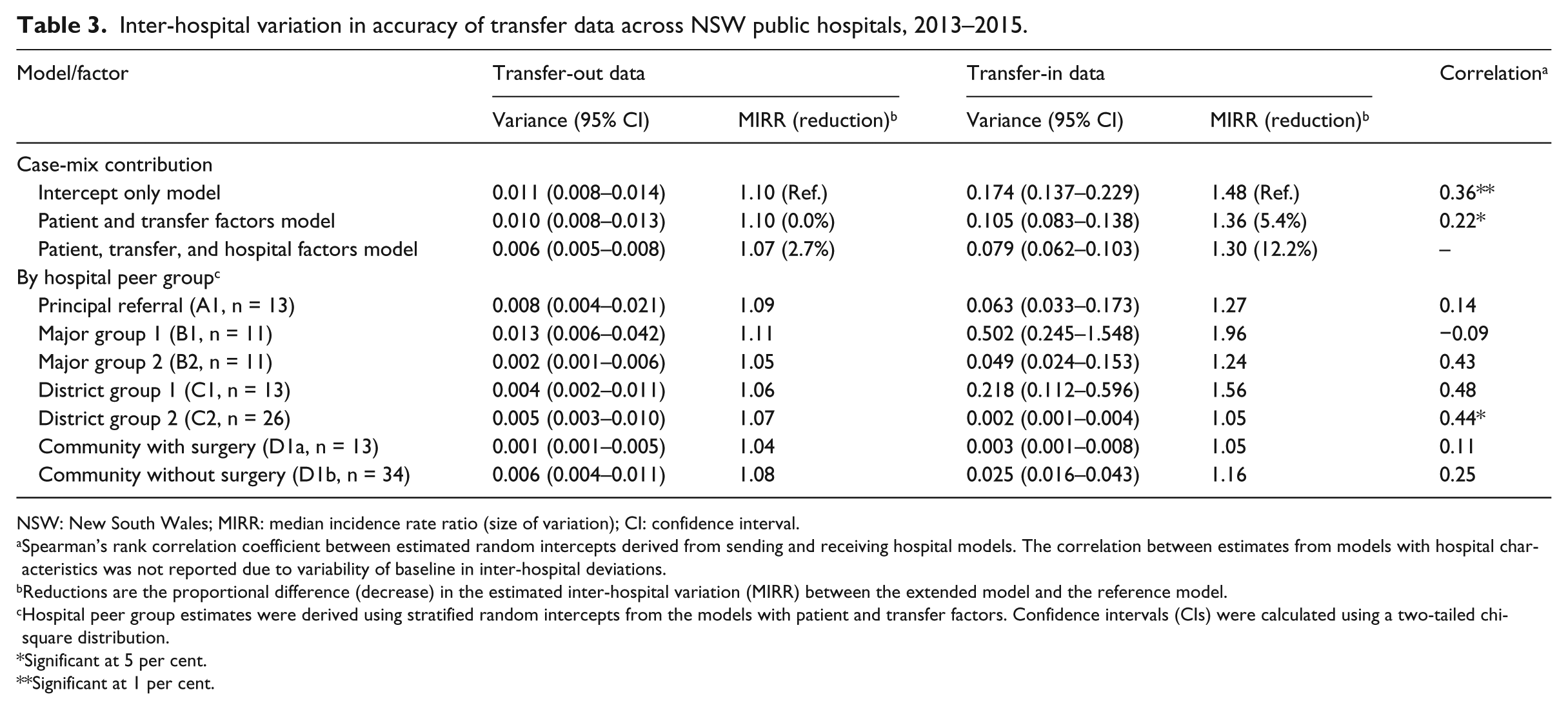
NSW: New South Wales; MIRR: median incidence rate ratio (size of variation); CI: confidence interval.
Spearman’s rank correlation coefficient between estimated random intercepts derived from sending and receiving hospital models. The correlation between estimates from models with hospital characteristics was not reported due to variability of baseline in inter-hospital deviations.
Reductions are the proportional difference (decrease) in the estimated inter-hospital variation (MIRR) between the extended model and the reference model.
Hospital peer group estimates were derived using stratified random intercepts from the models with patient and transfer factors. Confidence intervals (CIs) were calculated using a two-tailed chi-square distribution.
Significant at 5 per cent.
Significant at 1 per cent.
Discussion
This large population-based study using admissions and emergency presentations from 121 NSW public hospitals over a 2-year period identified a higher accuracy in transfer-out data (87% vs 65%), with lower variation across hospitals (10% vs 36% differences) compared to transfer-in data. Hospital size had weak and varying effect on accuracy and inter-hospitals variability although its effect was greater for transfer-in data. Transfer pathway influenced data accuracy, and in particular, ED involvement at receiving hospitals (46% of all in-transfers) reduced the accuracy of data. Most of the variability in accuracy across hospitals remained unexplained and accuracy rates for transfer-out and transfer-in were not associated or influenced by density of transfers or peer group of interacting hospitals.
The unavailability of comparative data for examining the accuracy of transfer data is concerning, given that IHTs are an integral component of improved access to appropriate healthcare within healthcare systems. 1 IHTs are a routine component of optimal service delivery, experienced by approximately 1 in 20 patients in the United States and Australia12,22 and one in five at small community hospitals. Higher than our observed 13 per cent inaccuracy rate for transfer-out, Kahn and Iwashyna 23 reported that in US administrative data, 22 per cent of transfers to long-term acute-care facilities were not identifiable. The high inaccuracy rate can hinder efforts to identify transferred patients with elevated risk of adverse events,4,5 hospitals’ attributions and ultimately their contribution to patients’ outcomes and efficiency of the system through inter-hospital interactions.10,12 The existing nature of hospital administrative data to partially capture patient sharing among hospitals because of inherent biases and under-recording of information24–26 warrant due consideration of these data as the main source of information for research, planning, and performance profiling.27–30
Recent studies reported that the accuracy of recording morbidities in hospital administrative data varies across hospitals and regions,25,26,31 and between one-fifth to half of the variability is attributable to patient and mostly to hospital-related factors in NSW. 25 In contrast, our observed low and inconsistent effect of hospital size and location on accuracy of transfer data implies that individual hospital characteristics and other unseen factors are drivers for variability, in particular for transfer-in data. Organisational characteristics such as staffing, professional development, and standardisation of training are among factors identified to enhance data quality and reduce variation.32–34 In this study, there existed excessive data inaccuracy associated with transfer-in patients, and in particular, for those who were admitted via ED (ED mostly recorded as the referral source). This may stem from varied local policies for recognising transfer-in patients, tools for documentation and information exchange between and within hospitals, non-integrated systems among hospital departments, or varying degrees in uptake of information technologies,35,36 despite developed national and regional guidelines37,38 and state-wide information platforms. 39 Current fragmented hospital administrative data platform across NSW health services and districts does not support real-time identification of patient journey and transfers. 40
Admission on weekends and at non-daylight hours are reportedly associated with poorer outcomes for patients and elevated medical and handover errors.41–43 In contrast, we observed greater accuracy of data within these periods, consistent with a few studies reporting better communication and documentation.44,45 Less workload and possible shift related modifications that might affect transfer pathway may have contributed to our results. The observed increased accuracy for transfer-out data for patients who were re-transferred, in particular those returned to the originating hospitals, implies the potential positive influence of a pre-determined patient journey and related accurate documentation. However, at the hospital level, no significant association was seen between hospital-specific accuracies in transfer-out and transfer-in data. Furthermore, no volume effect (number of transfers and interacting hospitals) was evident in data accuracy. Slightly lower accuracy was associated with inter-LHD transfers, the less common transfer type in NSW,12,46 suggesting the value of investigating routinised partnership between hospitals to improve data accuracy.
Quality enhancement in administrative datasets can be achieved through improvement in acquisition processes 47 and incorporation of information from other data repositories and resources.26,48–51 Recently, the observed very low false-positive rates in administrative datasets24,26,49,52 prompted the use of internal data linkage and temporal accumulation of information as methods to measure and reduce discrepancies resulting from different data recording practices and rules.25,36,53,54 Similarly, we combined patient-specific admission and ED presentation records from both sending and receiving hospitals to capture all transfers regardless of their pathways and local strategies in documentation. This design enabled us to directly estimate inaccuracy in transfer data and associated variation, in particular for in-transfers, which can be eliminated through patient-level data linkage across datasets and hospitals. Nevertheless, we observed incomplete IHTs that may be false positives or due to missing records or unmet inclusion criteria (e.g. 24 h).
Our study raises several important policy implications. Firstly, despite recognition of elevated burden associated with transfer-in patients, the significant inaccuracy and variability in identification of transfers in the administrative dataset could lead to imprecise conclusions and potential biases. Secondly, there is a need to standardise recognition and documentation of transfers while addressing pathways across facilities. Linking data at patient level in a fragmented system and further integrating information exchange across providers can minimise data inaccuracy. Lastly, education and engagement of hospital administrators, information technologist and researchers within the health service domain for improvement in data quality should be encouraged.
This study benefited from its design, using large population-based record-linked datasets to access all admissions and ED presentations in all acute-care public hospitals within the most populated health jurisdiction in Australia to explore for the first time accuracy in transfer data. The design utilised internal references based on routinely collected data that could readily be used for real-time monitoring of data quality and improvement through data accumulation. We may have under-reported the total inaccuracy in the absence of an external reference for measuring false-positive rates; chart review on randomly sampled cases would be useful. Variation analysis was limited to transfers between public acute hospitals as determined by data availability; inclusion of private hospitals as well as non-acute facilities could provide addition insight. Furthermore, consideration of readmission within a tight time frame irrespective of transfer status could enhance assessment of care sharing and hospital contribution.11,55 Models incorporating staffing, documentation rules, and information technology platforms may also better explain variability.
Conclusion
Information for transferred patients in hospital administrative datasets are inaccurate. Transfer pathways and hospitals individually contribute to the observed incidence and variation in discrepancies. Consequently, case-mix adjustments for performance profiling could be biased because of inaccuracy and varying levels of inaccuracy across hospitals. Variation in information technology and documentation practices is yet to be investigated. Data linkage at patient level across facilities and regions and recognition of patient journey in an integrated data platform combined with standardisation of documentation across hospitals would enhance accuracy of routinely collected datasets and the related validity of case-mix adjustment, hospital attribution, and partnership.
Footnotes
Acknowledgements
The authors thank Drs Kim Hill and Elizabeth West and Ms. Naomi Van Steel (Westmead Hospital) for their advice on IHTs and documentation.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.