
Abstract
Background
Nursing care in isolation environments requires strict infection control protocols, which increase nurses’ physical and psychological burden. Frequent entry into isolation rooms for routine tasks, such as adjusting infusion pumps, exposes healthcare workers to infectious agents, increases consumption of personal protective equipment, and results in inefficient use of nursing resources.
Aims
This study aimed to develop and evaluate the usability of an Internet of Things (IoT) remote control system for infusion pumps (IRCSIP) to support infection prevention, improve nursing efficiency, and enable effective use of resources in isolation care.
Design
Simulation-based, single-group pre-post usability study.
Methods
IRCSIP developed using existing commercial IoT devices. Twelve registered nurses with experience in infusion pump operations and isolation nursing care completed two scenarios: (1) remote operation using the IRCSIP and (2) traditional infusion pump operation. The time required to complete infusion rate adjustment, operational success, and subjective usability were measured. Data were analyzed using paired t-tests and descriptive statistics.
Results
All participants successfully adjusted the infusion rate on their first attempt in both scenarios. Compared with traditional operation, the IRCSIP significantly reduced adjustment time, saving an average of 90.67 s. Usability ratings were positive across all domains: effectiveness “Very good” (58.33%) or “Good” (41.67%); efficiency “Very good” (91.67%); satisfaction “Very good” (66.67%) or “Good” (25.00%); safety “Very good” (41.67%) or “Good” (16.67%); and ease of use “Very good” (58.33%) or “Good” (33.33%).
Conclusion
IRCSIP demonstrated high usability and significantly improved workflow efficiency by reducing the time needed for infusion rate adjustments. This suggests that the system may help reduce nurse workload related to routine infusion pump management. A key strength of the IRCSIP is compatibility with existing infusion pumps, which allows for cost-effective and scalable implementation without the need for new medical equipment.
Introduction
Nursing care for patients with infectious diseases requires strict infection control practices to prevent pathogen transmission and protect healthcare workers and vulnerable patient populations.1,2 The consistent use of personal protective equipment (PPE), environmental cleaning and ventilation control, and infection prevention protocols are fundamental components of such care.1,2 However, these protocols substantially increase healthcare workers’ physical and psychological burden, particularly among nurses. The frequent donning and doffing of PPE may lead to communication difficulties, physical exhaustion, and increased work-related stress, affecting the quality of care delivered in isolation settings.3,4
The COVID-19 pandemic exacerbated these challenges to an unprecedented degree. Globally, as of May 19, 2024, more than 775 million COVID-19 cases and more than seven million deaths have been reported, with more than 34 million confirmed cases and 35,000 deaths reported in Korea. 5 The pandemic resulted in a significant surge in the number of patients requiring isolation, which overwhelmed healthcare systems globally and increased healthcare workers’ workloads and infection risks. 6
Although the COVID-19 pandemic has subsided, patients with compromised immune systems, such as those receiving chemotherapy, organ transplantation, or treatment for chronic illnesses, remain particularly vulnerable to healthcare-associated infections (HAIs). 7 Given this vulnerability, contact between healthcare workers and patients in isolation settings should be minimized to prevent cross-transmission, particularly considering that healthcare workers may act as a source of infection.7–9 Even minor breaches in infection control protocols can lead to severe, life-threatening complications, prolonged hospitalization, and increased mortality among patients with compromised immune systems. 2 Accordingly, minimizing unnecessary physical contact and ensuring a highly controlled care environment is critical for safeguarding this high-risk population.
Infusion pumps, which are widely used to accurately administer intravenous (IV) medications, play an essential role in the care of patients. 10 However, frequent infusion rate adjustments require nurses to repeatedly enter isolation rooms, resulting in increased PPE consumption, physical burden, and a high risk of infection control breaches. 4 Additionally, delayed responses to infusion alarms due to the burden of PPE donning and environmental entry barriers may compromise patient safety and care quality.11,12
Previous attempts to mitigate these challenges included relocating infusion pumps outside isolation rooms. 13 However, this approach introduced new infection control concerns, including contamination risks associated with extended IV infusion lines, medication waste, and increased supply costs. 13 These limitations highlight the need for safer and more efficient infusion pump operation strategies that reduce unnecessary physical contact while ensuring adherence to infection control protocols.
Smart infusion pumps have also been highlighted as an effective strategy to enhance medication safety, minimize healthcare worker exposure, and optimize resource utilization in isolation care settings. 14 However, they have notable limitations. Delays in wireless drug library updates are common, with some systems experiencing lags of up to several months, increasing the risk of dosing errors. 15 Moreover, frequent alerts often lead to healthcare worker desensitization and high override rates. 16 Additionally, smart pumps require integration with hospital-wide centralized electronic systems, making them costly and less feasible in settings where rapid deployment or resource efficiency is critical, such as resource-limited hospitals and temporary isolation units. 17 Therefore, there is a need for alternative strategies that overcome both physical pump relocation and smart infusion pumps by enabling remote operation.
The rapid expansion of digital health technologies during the COVID-19 pandemic has accelerated the integration of mobile health (mHealth), IoT-based systems, and teleoperated technologies into clinical practice. A recent systematic review demonstrated that mHealth applications played a critical role in sustaining healthcare delivery during infectious outbreaks by enabling remote monitoring, communication, and information management; however, persistent limitations—including infrastructural dependency, interoperability constraints, data continuity challenges, and privacy concerns—continue to hinder sustainable implementation. 18 Furthermore, empirical evidence from infectious disease departments indicates that the adoption of teleoperated and robotic systems is frequently constrained by technological readiness, organizational capacity, regulatory alignment, and workforce adaptation, despite their potential to enhance infection control and occupational safety. 19 Collectively, these findings emphasize that the successful deployment of remote-care technologies requires not only technical feasibility but also contextual adaptability, workflow integration, and institutional support within complex healthcare environments.
The Internet of Things (IoT) represents a transformative technology that enables sensors and smart devices to collect real-time environmental data and transmit it via Internet networks. 20 During the COVID-19 pandemic, IoT technologies were increasingly adopted in healthcare settings due to their compatibility with existing medical devices and their user-friendly interfaces.21,22 These features demonstrated particular utility in infection-prone isolation care environments, where minimizing physical contact is critical. 21 In such settings, IoT was implemented in the form of smart screening gates, wearable patient monitoring sensors, and remote ventilator control systems.23,24 Despite its proven utility and cost-effectiveness in various healthcare domains, the application of IoT in infusion pump systems remains limited. Therefore, there is a growing need to develop IoT-based infusion pump systems that are practical and compatible with routine clinical use.
To address this gap, this study aimed to develop an IoT remote control system for infusion pumps (IRCSIP) and evaluate its usability, enabling nurses to adjust infusion rates remotely while allowing continuous patient monitoring. By integrating IoT technology with existing clinical equipment, the IRCSIP is expected to contribute significantly to infection control, reduce nurses’ physical and psychological burden, enhance resource use, and increase patient safety, particularly for patients vulnerable to infection.
The specific aims of this study were as follows:
To develop an IRCSIP that is compatible with existing clinical equipment. To evaluate the usability of the IRCSIP by comparing it with traditional infusion pump operation.
Methods
This study employed a two-step approach comprising (1) the development and (2) the evaluation of an IRCSIP. The overall process was guided by the Plan–Do–Study–Act (PDSA) quality improvement framework, which is widely used to facilitate iterative testing and implementation in healthcare innovation (Figure 1). 25

PDSA process applied to the development and evaluation of the IRCSIP. IRCSIP: Internet of Things (IoT) remote control system for infusion pumps.
In this study, the Plan and Do phases corresponded to the development step, involving the selection of appropriate devices, system integration, and preliminary testing. The Study and Act phases were aligned with the evaluation step, which focused on assessing the usability of the developed IRCSIP and deriving implications for further improvement and potential clinical application.
Step 1. Development
Plan
The research team identified the clinical problem of frequent nurse entry into isolation rooms for routine infusion pump adjustments, which increases infection risk and resource burden. To address this issue, the team established the objective of developing an IRCSIP that could integrate with existing clinical equipment. Device selection criteria including compatibility, safety, and commercial availability were also defined at this phase.
Do
Device selection
A button-type infusion pump (D infusion pump) was selected because its touchscreen LCD interface displays infusion rates above the control buttons, enabling nurses to view the rate even when the IoT actuator is attached. To reduce safety risks related to device malfunction, several IoT button-pressing devices were reviewed, including Abot, Bbot, and Cbot. Because Cbot was not readily available in South Korea, the final prototypes included Abot and Bbot. Manual override capability was a key selection criterion to ensure safe device control during system failures or emergencies.
Integration of selected devices
Given that the selected IoT devices required a 2.4 GHz Wi-Fi connection while only 5G connectivity was available in the simulation setting, a portable Wi-Fi router was connected to a smartphone hotspot to generate a 2.4 GHz network.
Preliminary testing
Bbot did not generate enough pressure to reliably actuate the D infusion pump's buttons, so the Abot was selected. Three Abot units were mounted on the infusion pump's control buttons. Remote operation was enabled using the Abot Hub Mini and monitored with Abot HomeCam and Bbot smart IP cameras. Researchers installed the Abot and Bbot applications on tablet PCs to control the infusion rate and monitor the display screen (Figure 2). A demonstration video showing the actual function of the D infusion pump with the IRCSIP is included as supplemental material. A summary diagram illustrating the IRCSIP workflow is shown in Figure 3.

Tablet interface used for operating and monitoring the IRCSIP. IRCSIP: Internet of Things (IoT) remote control system for infusion pumps.

Diagram of IRCSIP workflow.
Step 2. Evaluation
Study
Scenario development
A clinical scenario was used to simulate the application of the IRCSIP in an isolation ward (Table 1). The scenario included patient data and tasks typical of acute care settings, such as adjusting intravenous heparin infusion rates based on laboratory test results.
Scenario for a usability test of the IRCSIP. a

IRCSIP: Internet of Things (IoT) remote control system for infusion pumps.
KF94 mask: Korean Filter 94 mask, a Korean-certified medical respirator with a ≥ 94% filtration efficiency for 0.3 μm particles, functionally comparable to N95 respirators.
Usability evaluation
Design
This study employed a single-group pre–post experimental design to evaluate the usability of the developed IRCSIP. A total of 12 participants were recruited according to the Medical Device Good Manufacturing Practice Guidelines and the recommendations of Six and Macefield (2016),26,27 which suggest 10–12 participants for formative usability testing. The inclusion criteria were as follows: Registered nurses (a) with at least one year of clinical experience in direct patient care at a tertiary general hospital, (b) with previous experience using infusion pumps and providing care for patients in isolation, and (c) who understood the purpose of the study and voluntarily agreed to participate.
Ethical considerations
All participants provided written informed consent before participation. Participant recruitment was conducted from 10 January 2024 to 22 January 2024, and the experiment was conducted on 22 January 2024.
Experimental procedure
The experiment was conducted at the simulation center in the Yonsei University College of Nursing. The environment included two simulation rooms (Rooms A and B) and a mock isolation room. PPE, including KF94 masks (Korean filter 94 respirators with a ≥ 94% filtration efficiency for 0.3 μm particles, functionally comparable to N95 respirators), face shields, gloves, gowns, and caps, was provided in the vestibule (anteroom) connected to the isolation room. Participants were instructed to arrive at the simulation center at their scheduled times. Before the simulation began, they received an overview of the study and provided informed consent.
In Room A, a researcher briefed the participants on the traditional infusion pump operation methods and PPE usage. Subsequently, participants entered the isolation room individually, where they donned full PPE and manually adjusted the IV infusion rate. During this process, the researcher recorded the time taken and the accuracy of task completion. After completing the scenario, the participants were given a rest period.
The participants received instructions for the IRCSIP. Each participant operated the system via a tablet PC at the nursing station adjacent to the isolation room to remotely adjust and verify the infusion rates. Simultaneously, a researcher recorded the time and accuracy of each performance.
Following the completion of the IoT-based remote control scenario, participants completed a structured questionnaire assessing demographic characteristics (age, sex, education, current department, and duration of clinical experience (months)) and their perceived satisfaction and ease of use regarding system usability. System usability was evaluated using the Ministry of Food and Drug Safety (2021) usability guidelines, 26 which include five domains: effectiveness, efficiency, satisfaction, safety, and ease of use. Effectiveness measured whether participants operated the infusion pump as intended using the IoT-based remote control method. Efficiency assessed the ratio of effort to outcomes in the IoT-based remote control of infusion pumps. Satisfaction captured participants’ overall satisfaction with the IoT-based remote control. Safety measured whether participants perceived any potential risk when using the IoT-based system. Ease of use assessed how easily participants could operate the IoT-based infusion pump remote control. Each domain was rated on a 5-point Likert scale: “Very poor,” “Poor,” “Neutral,” “Good,” and “Very good.”
Data analysis
All statistical analyses were conducted using IBM SPSS Statistics (Version 26). The Shapiro-Wilk test confirmed the normality of the data. A paired t-test compared the time required to complete tasks between the traditional method and IRCSIP. Statistical significance was set at p < .05. Hedges’ g and its 95% confidence interval (CI) were calculated to indicate effect size and adjust for small sample bias. 28
Results
General characteristics
A total of 12 nurses participated in the study. The general characteristics of the participants are presented in Table 2. Their mean age was 31.08 ± 4.48 years, and the majority were female (n = 9, 75%). Most participants held a bachelor's degree (n = 8, 66.67%), while the remainder held a master's degree (n = 4, 33.33%). Regarding the clinical department, (n = 10, 83.3%) worked in the emergency room, while (n = 1, 8.33%) each worked in the intensive care unit and the general ward. The mean duration of clinical experience was 88.00 ± 48.79 months.
General characteristics of participants (N = 12).

Usability of the IRCSIP
Efficiency
All participants completed the infusion rate adjustment on the first attempt in both the IRCSIP and the traditional infusion pump operation methods, resulting in a 100% operational success rate across both scenarios (Table 3). The time required to complete the task was significantly shorter with the IRCSIP compared to the traditional infusion pump operation (Table 3). The mean completion time was 32.50 ± 7.29 s with the IRCSIP, compared to 123.17 ± 17.97 s with the traditional infusion pump operation. This difference was statistically significant (p < .001, 95% CI = 79.83–101.51) (Table 3). The effect size, calculated as Hedges’ g, was 18.34 (95% CI = 2.83–7.04), indicating a large effect (Table 3 and Figure 4).

Boxplots for time to complete tasks (seconds).
Comparison of efficiency between the IRCSIP a and the traditional infusion pump operation method (N = 12).
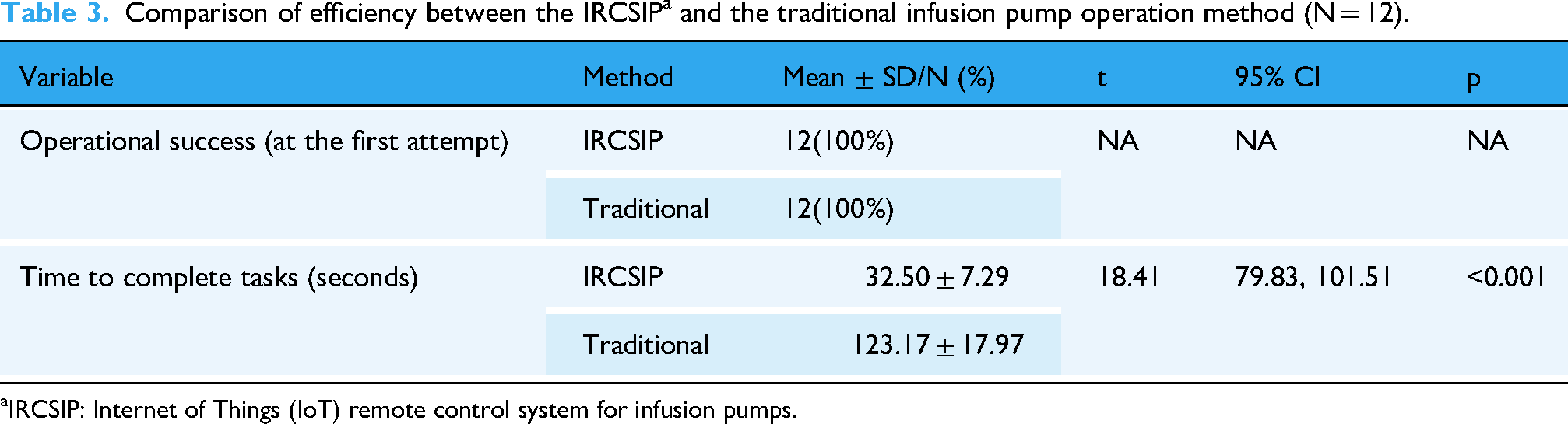
IRCSIP: Internet of Things (IoT) remote control system for infusion pumps.
User experience
Effectiveness was rated “Very good” by 58.33% and “Good” by 41.67%. Efficiency was rated as “Very good” by 91.67% and “Neutral” by 8.33%. Satisfaction was rated as “Very good” by 66.67%, “Good” by 25.00%, and “Neutral” by 8.33% of participants. Safety was rated as “Very good” by 41.67%,“Good” by 16.67%, “Neutral” by 25.00% and “Poor” by 16.67%. Ease of use was rated as “Very good” by 58.33%, “Good” by 33.33%, and “Neutral” by 8.33% of participants (Figure 5).

User experience ratings for the IRCSIP.
Discussion
This study developed and evaluated an IRCSIP through the Plan-Do-Study phases of the PDSA cycle. Based on the findings, the final Act phase involved identifying system improvement strategies and assessing the feasibility of clinical application. IRCSIP demonstrated its effectiveness in improving nursing efficiency, enhancing infection control, and increasing nurses’ satisfaction in isolation settings. The system significantly reduced the time required for infusion pump adjustment and minimized physical entry into isolation rooms, which is critical for maintaining controlled environments and protecting patients and healthcare workers.
Maintaining environmental stability is essential for effective infection control in isolation settings, where frequent room entry caused by medical device adjustments can increase the risk of pathogen escape.29,30 By enabling nurses to operate infusion pumps remotely, the system minimizes unnecessary physical contact and helps maintain the integrity of the isolation environment. This approach strengthens infection prevention protocols and is particularly beneficial for immunocompromised patients, who face a higher risk of healthcare-associated infections.7–9 By reducing direct interactions, the IRCSIP adds a crucial layer of protection for these high-risk individuals.
The IRCSIP contributes to addressing healthcare workers’ critical challenges of fatigue related to repeated donning and doffing of PPE. Nurses working in isolation units frequently report significant physical and psychological strain from intensive PPE use, which contributes to job-related stress and burnout. 4 By reducing the need for frequent room entry, the IRCSIP can alleviate this burden, helping to preserve nurses’ physical energy and mental well-being. Additionally, the system optimizes nursing workflow efficiency. Traditional infusion pump operations are time-consuming and detract from essential nursing care, including patient monitoring, medication administration, and education. Remote operability allows nurses to reallocate time to these core responsibilities, thereby improving nursing care quality and patient satisfaction.
The key advantages of this approach are its cost-effectiveness and ease of implementation. The system does not require investment in new infusion pump hardware but instead enhances the usability of the existing clinical equipment by integrating remote-control capabilities. Such advantages make this technology particularly attractive for healthcare facilities seeking to improve infection control and nursing efficiency without incurring significant infrastructure costs. Furthermore, the IRCSIP is designed for intuitive operation and allows prompt disengagement in case of system malfunction or user preference, enabling nurses to revert to traditional infusion pump operation methods. This operational flexibility ensures patient safety and compatibility with existing workflows.
The demonstrated benefits of IRCSIP, including enhanced infection control, improved nursing workflow, increased cost-effectiveness, and ease of use, are anticipated to be further amplified in situations requiring enhanced PPE protocols. While this study employed a simplified PPE protocol, it is important to note that enhanced PPE protocols, such as those implemented during the early COVID-19 pandemic or in emerging infectious disease outbreaks, require more extensive PPE and substantially longer donning and doffing procedures. These requirements contribute to increased physical burden and fatigue among healthcare workers.31,32 Under such demanding circumstances, IRCSIP is expected to demonstrate even greater effectiveness, providing practical advantages in resource-limited settings.
Furthermore, the IRCSIP can ensure continuity of care during intra- and interhospital transports and extended procedures, thereby enhancing patient safety. Intra- and interhospital transports often involve risks such as equipment disconnection, delayed medication delivery, and communication failures.33,34 These risks are amplified when nurses conduct prolonged or solitary transports without support, leading to increased cognitive and emotional burden. 35 The IRCSIP enables nurses to monitor and control infusion pumps remotely during transports, ensuring uninterrupted care and allowing timely intervention when needed. As a result, it can reduce nurses’ workload and minimize the likelihood of adverse events during patient transport both within and between hospitals.
Therefore, the IRCSIP offers a practical approach to enhancing isolation care by simultaneously addressing infection control, nursing efficiency, resource utilization, and patient safety. It also contributes to the overall satisfaction of both patients and healthcare workers. The integration of this system into healthcare settings could enhance preparedness for future infectious disease outbreaks while ensuring safer patient transport and maintaining continuity of care.
Strengths of the study
First, this study addresses infection control challenges by proposing a scalable, low-cost solution that enhances both patient and worker safety without requiring expensive technological overhauls. The IRCSIP utilized commercially available devices, making it easy to implement using existing clinical equipment. Second, the system was evaluated using a simulation-based usability test, reflecting realistic clinical working environments in isolation care. The use of a structured scenario, along with both quantitative and qualitative assessments for the usability test, enabled a rigorous comparison with traditional infusion pump operation methods. Finally, this study employed a structured PDSA cycle for system development and evaluation, offering a replicable framework for digital health innovation.
Limitations of the study
Despite its strengths, this study has several limitations. The usability evaluation took place in a controlled simulation environment rather than a real clinical setting, which limits ecological validity. Real-world variables, including unstable network conditions, emergency interruptions, patient alarms, and competing clinical demands, were not represented. Future studies should validate the system in real-world clinical environments, examine its performance under variable conditions, and assess its broader clinical impact.
In addition, the single-group pre–post design may have introduced learning or fatigue effects because participants completed the traditional scenario before the IRCSIP scenario. Therefore, some of the observed time reduction may result from increased familiarity with the task rather than the system itself. As this study is a pilot test, the findings are preliminary. Further development and validation require a crossover or randomized controlled trial design in diverse clinical settings and multiple hospitals in real-world environments.
The sample size was small and included mainly nurses from emergency and acute care units at one institution, which may have introduced selection bias and limited generalizability to other clinical settings and types of isolation units. This study examined only infusion rate adjustment, so the usability findings apply only to this function and do not extend to more complex nursing tasks such as responding to occlusions, changing medication bags, or managing alarms. Future studies should evaluate a broader range of clinical tasks to determine wider applicability.
The technical setup, network configuration, and potential risks, including mechanical failure, connectivity disruption, and cybersecurity, were not described in sufficient detail to allow full replication, because the prototype used commercially available consumer-grade devices. For clinical deployment, developers should establish a dedicated system architecture that includes secure hospital-grade networks, firewall integration, and institution-managed servers to ensure data security and operational reliability.
Conclusion
The findings of this study showed that the IRCSIP demonstrated high usability and significantly improved workflow efficiency by reducing the time needed for infusion rate adjustments. This suggests that the system may help reduce nurse workload related to routine infusion pump management. A key strength of the IRCSIP is its compatibility with existing infusion pumps, which allows for cost-effective and scalable implementation without the need for new medical equipment.
Potential implications and areas for future research
The IRCSIP may reduce nurse fatigue, improve nursing care efficiency, and support infection control protocols in isolation care settings. It could also serve as a model for developing other remote-control systems in clinical environments, such as life-support equipment and patient monitoring devices. Its affordability and compatibility with existing clinical equipment make it suitable for resource-limited or pandemic-affected settings. In clinical practice, the physical distance between nursing stations and isolation rooms often delays care delivery and requires nurses to spend more time reaching patients. Therefore, the IRCSIP could provide greater time-saving benefits than those shown in this study.
Future studies should examine the real-world implementation and long-term efficacy of IRCSIP. In addition, hospital-wide initiatives, such as pilot testing and system demonstrations, should be encouraged to evaluate feasibility and support broader adoption in clinical practice.
Supplemental Material
sj-pdf-1-dhj-10.1177_20552076261433143 - Supplemental material for Improving safety and efficiency in isolation rooms using an Internet of Things remote control system for infusion pumps: Usability test
Supplemental material, sj-pdf-1-dhj-10.1177_20552076261433143 for Improving safety and efficiency in isolation rooms using an Internet of Things remote control system for infusion pumps: Usability test by Jeongok Park, Junghyen Lim and Youngkyung Kim in DIGITAL HEALTH
Supplemental Material
Footnotes
Acknowledgments
Not applicable.
Ethical considerations
The study protocol was reviewed and approved by the Institutional Review Board of Severance Hospital (No. 2023-3085-004).
Consent to participate
All participants provided written informed consent before participation.
Contributorship
Conceptualization: JP and JL. Data curation: JL and YK. Formal analysis: JP and JL. Funding acquisition: JP. Investigation: JP, JL, and YK. Methodology: JP, JL, and YK. Project administration: JP and JL. Software: JL. Supervision: JP and JL. Validation: JP, JL, and YK. Writing—original draft: JP and JL. Writing—review and editing: JP, JL, and YK.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Korea Medical Device Development Fund (No. RS-2020-KD000077), a 2023 Faculty-Student Research Grant from Yonsei University College of Nursing (No. 6-2023-0046) and a 2024 Multidisciplinary Research Grant from Mo-Im Kim Nursing Research Institute, Yonsei University College of Nursing (No. 6-2024-0143).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
All the data analyzed during the current study are available from the corresponding author on reasonable request.
Guarantor
Not applicable.
Supplemental material
Supplemental material for this article is available online.