
Abstract
There is a gap in knowledge of women’s perceptions of e-health treatment. This review aims to investigate women’s expectations and experiences regarding e-health. A search was conducted in MEDLINE, EMBASE, CINAHL and PsycInfo in March 2016. We included articles published between 2000 and March 2016, reporting on e-health interventions. The initial search yielded 2987 articles. Eventually, 16 articles reporting on 16 studies were included. Barriers to e-health treatment were lower for women than barriers to face-to-face treatment, such as feelings of shame and time constraints. Women were able to develop an online therapeutic relationship. As reduced feelings of obligation and lack of motivation were women’s greatest challenges in completing e-health treatment, they expressed a wish for more support during e-health treatment, preferably blended care. e-Health lowers the threshold for women to seek healthcare. Combining e-health interventions with face-to-face sessions may enhance women’s motivation to complete treatment.
Introduction
One of the main health challenges is to deliver the best achievable healthcare at the lowest possible cost 1 and to keep healthcare accessible at the same time. In the current 24-h economy, there is a growing need for timely access to information and advice, and this trend continues into healthcare. Shortage of healthcare providers and long waiting times, meanwhile, are preventing patients from receiving the medical help they need. 2 For these reasons, information and communication technologies are becoming an integral part of healthcare delivery.
Internet delivery of healthcare helps to overcome barriers in time, mobility and geography 3 and provides timely access to information as well as the ability to communicate with both providers and peers.3,4 More and more healthcare interventions are delivered over the Internet and are referred to as “e-health interventions.” e-Health interventions have proven to be effective for a wide range of indications5–10 and are continually evolving. 11 Components of e-health interventions are mainly delivered in the form of texts presented on web pages, with support provided via e-mail 12 and interactive online features.12,13 Considerable interest has arisen in tailoring e-health interventions to specific individual needs, which appears to enhance user engagement and might make e-health interventions more effective.4,14
Our specific expertise as a center of women’s health has led us to focus particularly on e-health interventions for women. Women more actively seek for information about their health, which may be reflected in how they utilize information sources such as the Internet. 15 Therefore, women might be an eligible target group for e-health interventions. Also, women more often have to cope with shameful conditions such as urogynecological diseases, which may raise the threshold for them to seek healthcare.16,17 Research suggests that e-health may reduce women’s feelings of shame while seeking healthcare.18–20 The Internet also allows women to multitask on a regular basis, balancing all the activities of work and home at all times.3,21 Previous findings suggest that e-health interventions may offer potential in delivering healthcare to women. However, there is a gap in knowledge of this topic. The objective of this review, therefore, is to investigate women’s expectations and experiences regarding e-health treatment.
Methods
We prospectively registered our systematic review in the Prospero international prospective register of systematic reviews, registration number CRD42016039297. Our review followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) reporting guidelines. 22
Data sources
A search strategy was developed in MEDLINE and adapted to EMBASE, CINAHL and PsycInfo with the assistance of a skilled librarian (A.v.d.S.-S., C.V.). In order to maximize the sensitivity of the search, a combination of free-text and thesaurus terms was used (Appendix 1). The search was run in March 2016. It was extended by manually reviewing the retrieved papers’ reference lists, the previously listed databases, Google Scholar and the content pages of the online Journal of Medical Internet Research related to the theme “Web-based and Mobile Health Interventions,” published until 9 March 2016 (C.V.). We contacted 14 authors because no PDF version of their article was accessible and one author because information appeared to be missing in the article. Publication bias was not formally assessed.
Study selection
All found articles were independently screened on title and abstract by two authors for eligibility of full-paper evaluation (A.v.d.S.-S., C.V.). Table 1 shows our eligibility criteria. Full-paper evaluation was performed in duplicate using a standardized decision model based on our eligibility criteria (A.v.d.S.-S., C.V.). The decision model was developed by one of the authors (A.v.d.S.-S.) and offered three possibilities: definitely included, definitely excluded and possibly eligible for inclusion. In order to reach consensus, researchers discussed articles that were rated by at least one author as “possibly eligible for inclusion” as well as articles they did not agree upon. A third researcher was decisive in the case of persistent disagreement or doubt (D.T.). After consultation of this third reviewer, agreement was reached. An interrater reliability analysis using the Kappa statistic was performed to determine consistency among raters. Interrater reliability was found to be Kappa = 0.67 (p < 0.001), 95 percent confidence interval (CI: 0.55–0.79), which can be interpreted as “substantial agreement” according to Landis and Koch. 23 Most disagreement arose over whether or not the study intervention met our definition of e-health interventions and on the applicability of the study outcomes to e-health in general. These were also the main reasons for exclusion of articles.
Eligibility criteria.
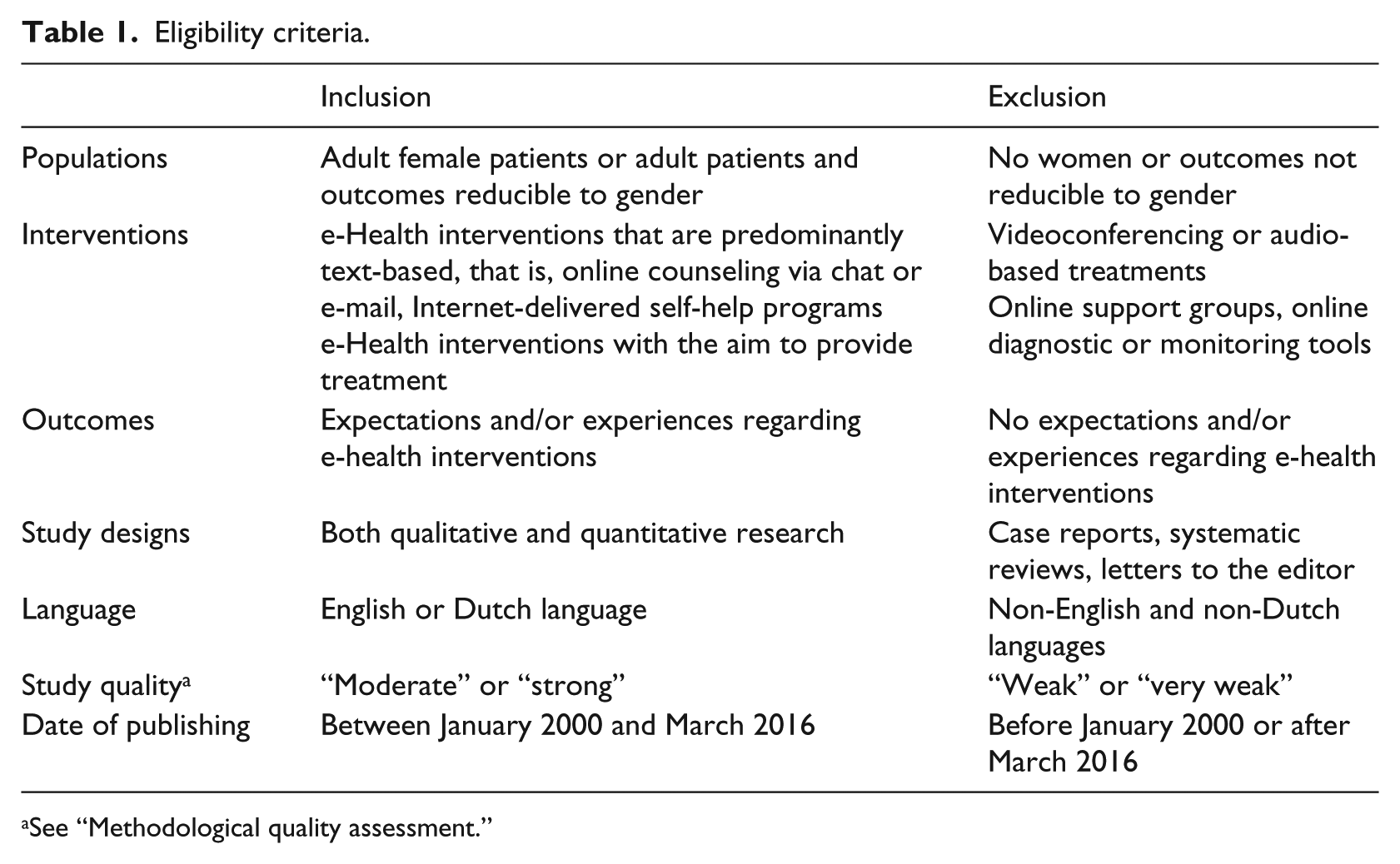
See “Methodological quality assessment.”
Methodological quality assessment
Two researchers independently performed a methodological quality assessment of the selected articles in an unblinded manner (C.V., A.v.d.S.-S.). For qualitative studies, we used a checklist including criteria adapted from the Critical Appraisal Skills Programme. 24 The following items were included: statement of research aims, appropriateness of qualitative research, research design, recruitment strategy, data collection, consideration of relationship between researcher and participants, ethical issues, data analysis, statement of findings and valuability. Maximum score was 20. Scores were classified as very weak (<12), weak (12–13), moderate (14–16) or strong (⩾17).
For quantitative studies, we used the version modified by Oram et al., 25 including the following items: research question, study design, sampling method, study sample, level of non-participation, assessment of exposure, assessment of outcomes, accounting for confounders, statistical analysis, reporting of confidence intervals, precision of results, ethical issues, conclusions, generalizability and fit with existing evidence. Maximum score was 30. Scores were categorized as very weak (<15), weak (15–19), moderate (20–24) or strong (⩾25).
Articles were excluded if study quality was rated as “weak” or “very weak.” In the case of disagreement between both researchers, the researchers met in order to reach consensus. A third reviewer was decisive when disagreement was persistent (D.T.). After consultation of this third reviewer, agreement was reached. An interrater reliability analysis using the Kappa statistic was performed to determine consistency among raters. Interrater reliability was found to be Kappa = 0.90 (p < 0.001), 95 percent CI (0.70–1.09), which can be interpreted as “almost perfect agreement” according to Landis and Koch. 23
Synthesis methods
Data were extracted on population, exposure and outcomes using a standardized data extraction form, which provided the basis for Table 2 (C.V., A.v.d.S.-S.). Data were categorized, and categories were discussed by the research team (C.V., A.L.-J. and D.T.). Discussion was continued until agreement was reached on all themes.
Summary table of studies investigating expectations.
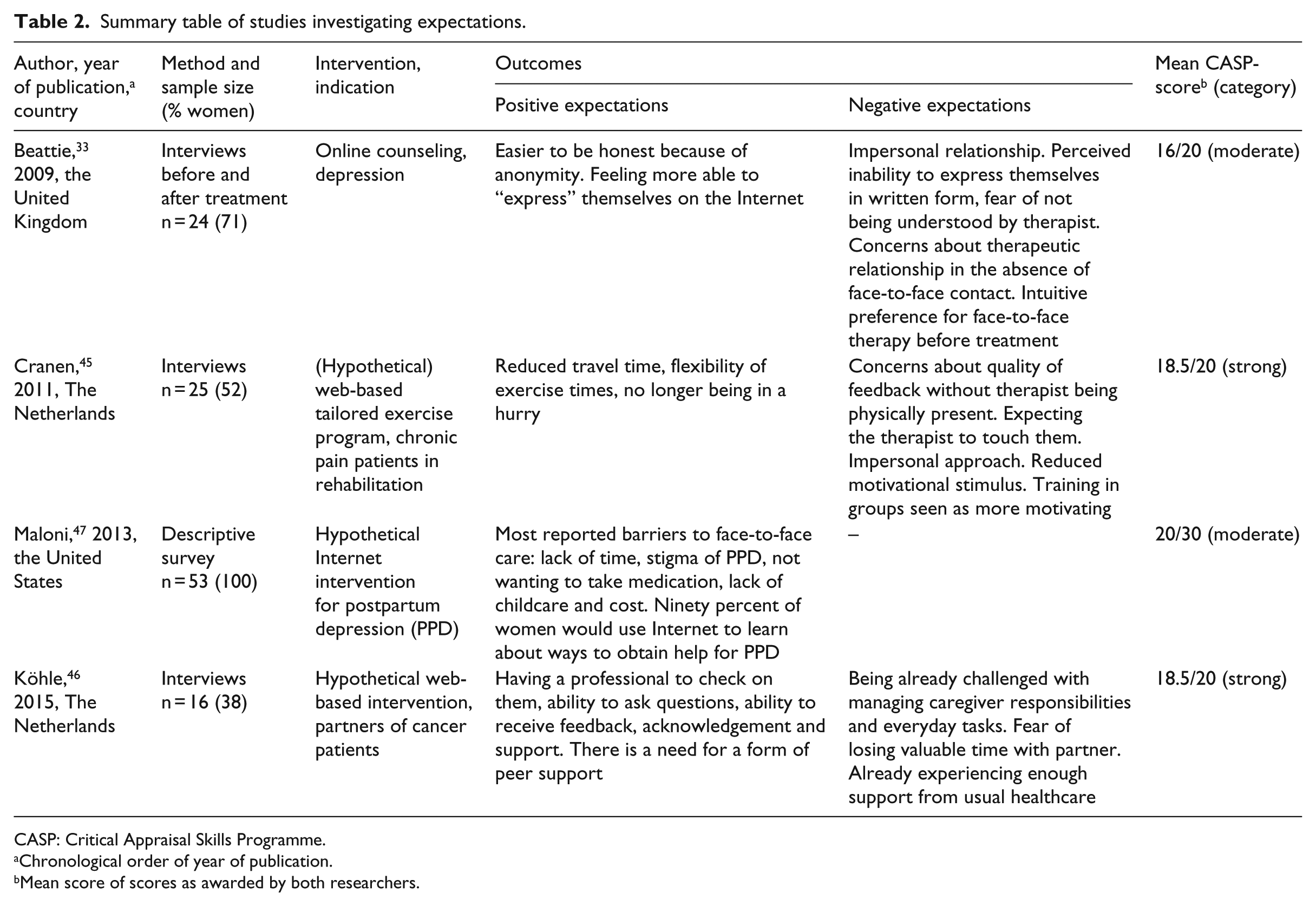
CASP: Critical Appraisal Skills Programme.
Chronological order of year of publication.
Mean score of scores as awarded by both researchers.
Results
Search results
The initial search yielded 2398 articles (Figure 1). Based on title and abstract screening, 2161 articles were excluded, leaving 237 articles for full-paper evaluation. Of these, 23 articles met our eligibility criteria. Methodological quality assessment led to the exclusion of another seven articles.26–32 As a result, 16 articles were included, reporting on 1 quantitative study, 2 mixed-methods studies and 13 qualitative studies. The results of the methodological quality assessment and study characteristics of the included studies are shown in Tables 2 and 3. The results of the methodological quality assessment and study characteristics of the excluded studies are shown in Table 4.
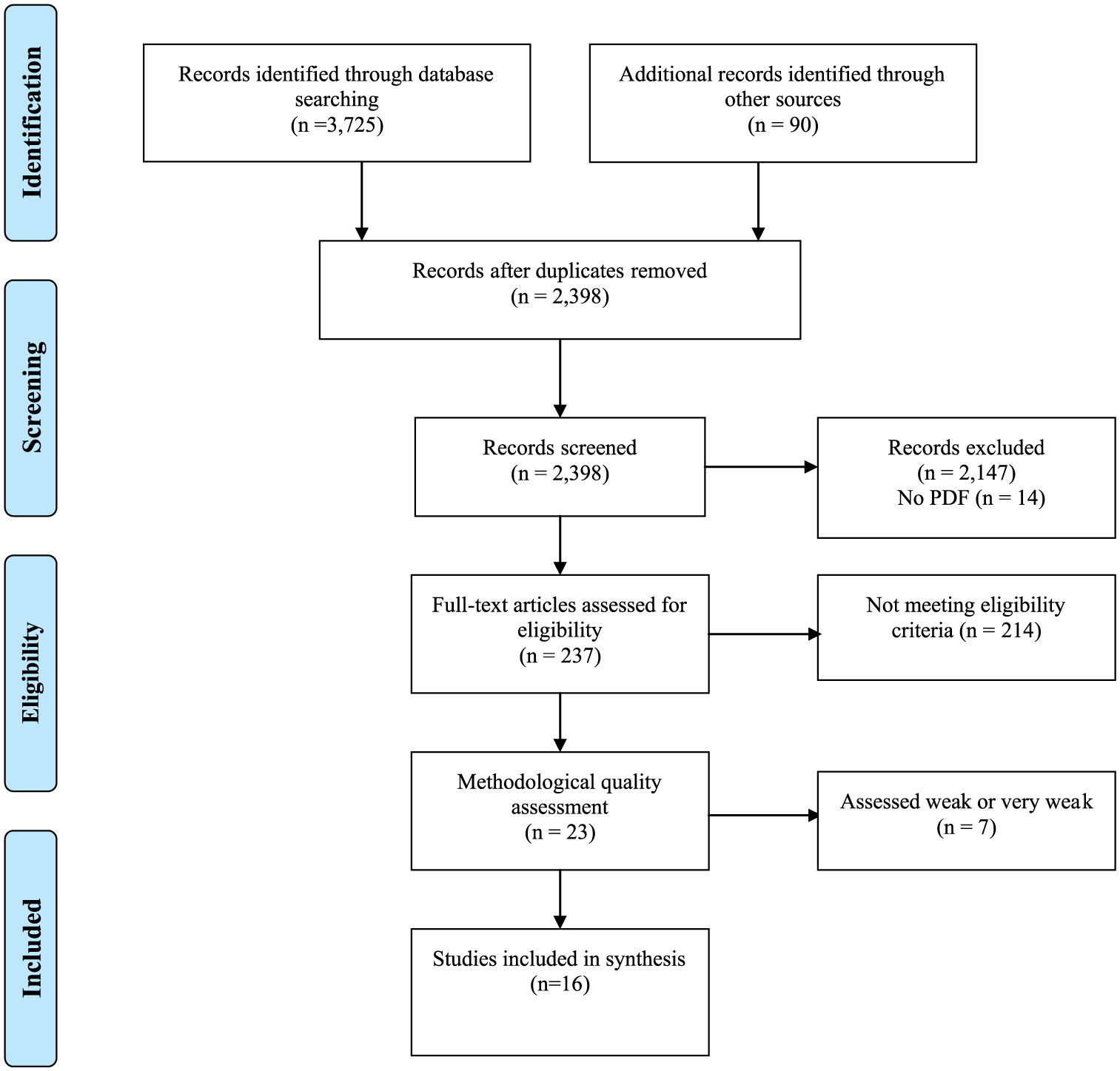
PRISMA 2009 flow diagram. 22
Summary table of studies investigating experiences.
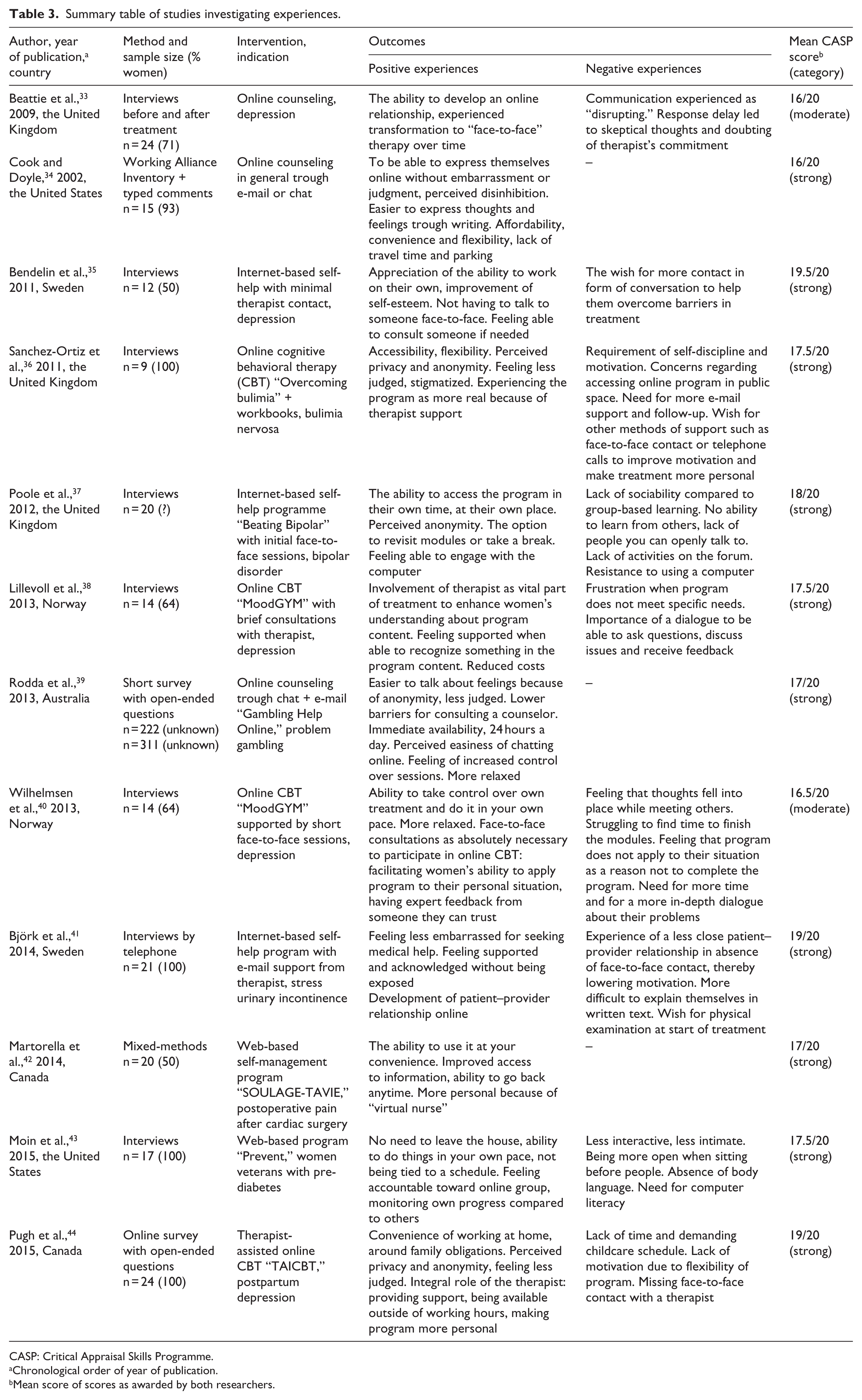
CASP: Critical Appraisal Skills Programme.
Chronological order of year of publication.
Mean score of scores as awarded by both researchers.
Summary table of excluded studies.
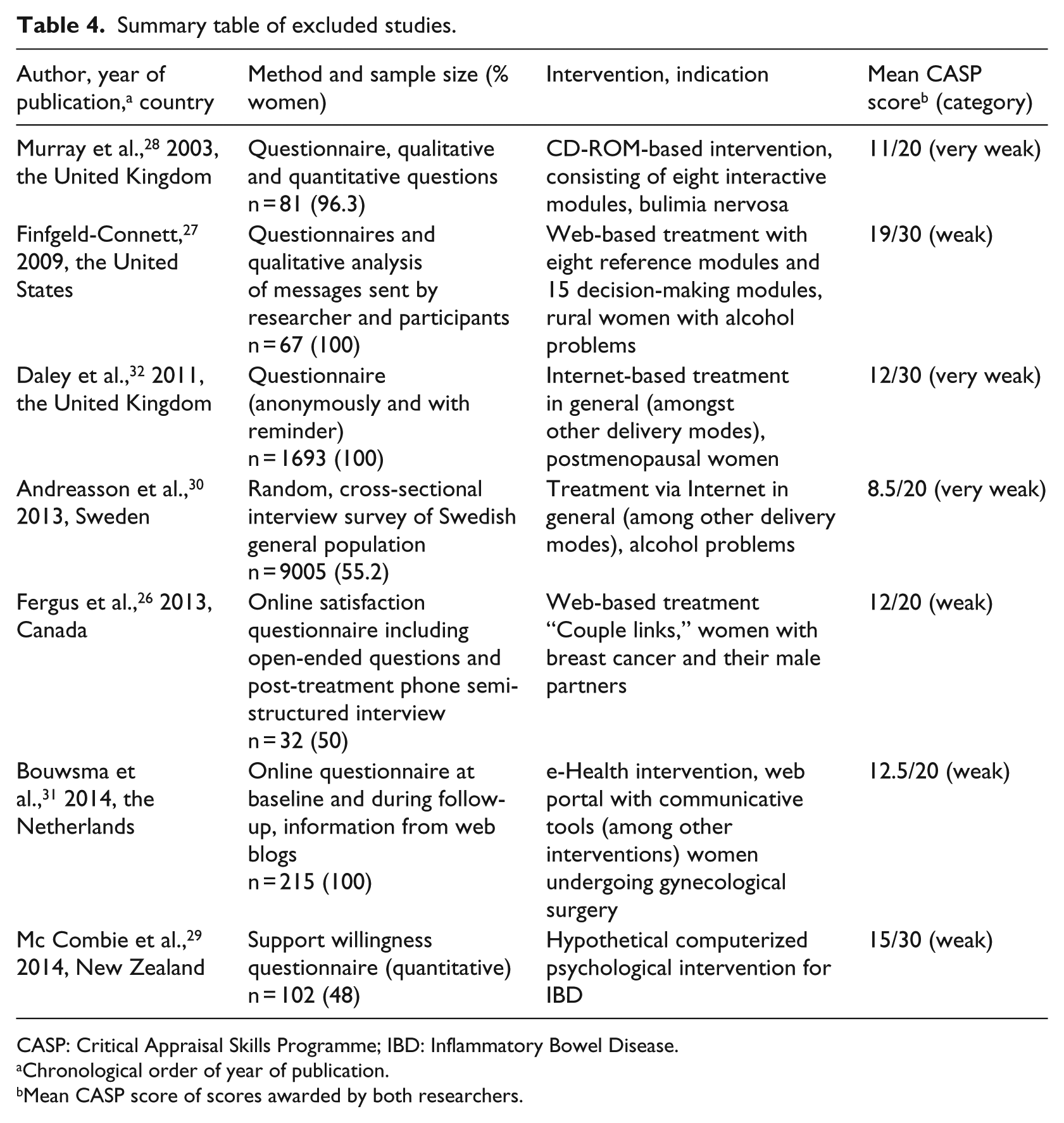
CASP: Critical Appraisal Skills Programme; IBD: Inflammatory Bowel Disease.
Chronological order of year of publication.
Mean CASP score of scores awarded by both researchers.
Outcomes
We divided the outcomes into two themes: expectations and experiences. The expectations and experiences were further subdivided into positive and negative expectations and experiences.
Expectations
Four studies investigated women’s expectations of e-health treatment.33,45–47 Outcomes regarding women’s expectations are shown in Table 2.
Positive expectations
Women with postpartum depression (PPD) reported lack of time, the stigma of PPD, not wanting to take medication, lack of childcare and costs involved as the most common barriers to face-to-face care. Of these women, 90 percent reported to be willing to use the Internet to obtain help for their PPD. 47 Women in general expected that the anonymity provided by the Internet would make it easier for them to talk about their problems and to express themselves. 33 Women in telerehabilitation for chronic pain considered their current group meetings as inhibiting and believed that they would be more capable of expressing their feelings in individual treatment. 45 Most women were also attracted by the flexibility of the exercise times and reduced travel time of e-health compared to face-to-face therapy. 45 Women who were partners of cancer patients were interested in e-health intervention because they were looking for acknowledgement, information, advice and support in addressing their specific needs. 46 Women believed that an online counselor could check on them, improve their motivation to complete treatment and would enable them to ask questions. 46
Negative expectations
Women mentioned some negative expectations of e-health as well. Women were afraid that the absence of face-to-face contact would make their treatment more impersonal.33,45 Some of them feared that this would impact negatively on their relationship with the therapist, 33 their motivation33,45 and subsequently on their therapy results. 45 These women stressed the importance of being able to talk to their therapist in person and talk about their feelings 45 and were skeptical about communicating with their therapist in the absence of non-verbal cues. 33 Women wished to be able to ask questions during their treatment 46 and receive feedback from their therapist. 45 In the study by Beattie et al., 33 women often expressed an intuitive preference for face-to-face therapy prior to therapy, with the exception of a small minority that reported previous negative experiences with face-to-face therapy. 33
Women in telerehabilitation for chronic pain anticipated that working at home would be more distracting or considered training in groups as more motivating. 45 Some women worried about the time investment required of an e-health intervention because they were already challenged balancing caregiver responsibilities and everyday tasks. 46 Other women were concerned about their writing skills and were afraid that they would not be able to express themselves correctly, and, hence, would be misunderstood by the therapist. 33 Women in telerehabilitation for chronic pain expected their therapist to be physically present during exercises because they doubted the quality of feedback without the therapist’s physical presence. 45
Experiences
A total of 13 studies investigated women’s experiences with e-health treatment.33–44,48 Outcomes regarding women’s experiences are shown in Table 3.
Positive experiences
Several women experienced barriers related to help-seeking in face-to-face treatment, which they did not experience or to a lesser extent in e-health treatment. Some women believed that their problem was not severe enough to justify seeking traditional healthcare or were afraid of not being taken seriously by their healthcare provider. This was sometimes caused by previous experiences. 41 Women felt less embarrassed seeking help during e-health treatment and were less afraid of being judged.34,36,39,41,44 They were attracted by the perceived anonymity, privacy and confidentiality of e-health.34,36,37,39,41,44,48 This anonymity made it easier for them to disclose themselves.34,39 Meeting face-to-face made them feel exposed and pressured by the need to answer straightaway.41,48 e-Health treatment, therefore, was perceived as less confronting than face-to-face therapy. 39
The greatest perceived practical barriers to traditional healthcare were lack of time, the need for transport and financial costs,34,38,43,44,48 as well as time restrictions and lack of continuity of healthcare providers.38,48 Due to the flexibility of exercise times and availability outside of working hours, women found it easier to integrate e-health interventions in their everyday life.34,36,37,40,42–45,48 Most women preferred the immediate access provided by e-health interventions to the appointment-based nature of traditional healthcare. 39 They felt comfortable and relaxed doing things at home and at their own pace.37,39,40,43 Some women were enthusiastic about the ability to go backwards and forwards anytime and to skip parts of the program that they considered unsuitable.36,37,40,42,48 By being able to decide when to use treatment, women gained a feeling of being in control.39,40,48 They liked the ability to do something to help themselves and, hence, felt empowered.35,40,48 Women felt supported when the program met their individual needs. 38
All women stressed the importance of the therapist during their treatment. Some even experienced their relationship with the therapist as a vital part of their treatment.36,38 They valued being able to consult someone if needed.35,36,39 The therapist made the program more personal and provided empathy and sympathy.33,44 The therapist’s support also helped them overcome barriers in treatment and increased the women’s motivation.35,38,41,44 Finally, the therapist enhanced women’s understanding of the program and their ability to apply the program to their personal situation.38,40
Women commented on the strength of their relationship with the therapist, noting the care and respect their therapist demonstrated. 34 Women undergoing online counseling for various indications filled in a working alliance inventory and rated their relationship with an online counselor higher than their relationship with a face-to-face counselor and significantly higher for the “goal” subscale. 34 A patient–therapist relationship developed despite the lack of face-to-face contact.33,41 Some women were surprised because they felt it was like face-to-face contact. 33
Negative experiences
Although women benefited from the perceived privacy and anonymity, some mentioned that the absence of face-to-face contact made the treatment more impersonal.36,37,43,45,48 They missed receiving empathic response during their treatment 48 and stressed the importance of non-verbal communication.33,41,43,48 These women anticipated that they would be more open when sitting in a room face-to-face with their therapist and preferred to talk to a professional in person and share feelings.38,40,43 Others mentioned that e-health treatment was less interactive than face-to-face therapy. 43 They stressed the importance of a conversation, in which they would be able to ask questions and discuss problems with the therapist35,38 and were in need of a more in-depth dialogue about their problems.
The delayed typing time during the online sessions could be interpreted as disrupting communication, causing women to doubt the therapist’s involvement by speculating whether he or she was undertaking parallel activities. 33 Some women found it more difficult to explain complex situations and feelings in written text than face-to-face and were afraid that the therapist would not understand them correctly.33,41 As a result, some women experienced the online patient–provider relationship as less close than face-to-face therapy.33,41
The flexibility and lack of obligations of the e-health interventions required more self-discipline and motivation than face-to-face treatment. The absence of face-to-face contact also led to reduced feelings of obligation, 48 as it was more tempting to skip exercises.41,45 Therefore, some women found it difficult to complete the exercises and to adhere to the treatment schedule.36,44,48 They struggled to find time to finish the homework modules.35,40,44,45 Furthermore, women felt frustrated if the program did not meet their own specific needs, which lowered their motivation.38,48
Women with urinary incontinence undergoing e-health treatment expressed a wish to have a physical examination at the start of their treatment. They were looking for reassurance that everything looked normal and for confirmation that they were using the right muscles during pelvic floor muscle treatment. 41 Likewise, women undergoing telerehabilitation for chronic pain anticipated that they would prefer to receive feedback from a therapist that is physically present. 45 Some women viewed e-health treatment as complementary or as follow-up treatment to traditional healthcare rather than as standalone treatment. 45 Generally speaking, women expressed a wish for more substantial monitoring and support.36,48
Discussion
This review provides an overview of women’s expectations and experiences regarding e-health. To our knowledge, no systematic review has been performed investigating e-health from women’s perspective in particular. The most important finding is that e-health lowers the threshold for women to seek healthcare, according to both women’s expectations and experiences. This supports the findings of Mohr et al., 49 which indicate that telephone and Internet treatments may help men and women to overcome barriers that would otherwise have prevented them from receiving healthcare.
In line with women’s expectations, the anonymity of the Internet makes it easier for women to talk about their problems. In the study by Van der Vaart et al., 50 on the other hand, most men and women observe that discussing thoughts, feelings and difficulties should still be done face-to-face. Although, prior to therapy, women are skeptical about developing a therapeutic relationship with their healthcare provider in the absence of face-to-face contact, they are able to develop an online therapeutic relationship. In the end, some women even consider this online relationship as if it were face-to-face contact. This finding matches that of Preschl et al., 51 indicating that a strong working alliance can be established in an online setting comparable to that established in face-to-face settings. However, some women experience this online relationship as less close and personal than a relationship established in face-to-face settings.
Also in line with their own expectations is that women are attracted by the flexibility of e-health, which enables them to do things at their own time, place and pace. Women thus gain a sense of self-control, leading to feelings of empowerment, a process through which people gain greater control over decisions and actions affecting their health. 52 Nonetheless, some women perceive this flexibility as a barrier to completing their treatment, due to reduced feelings of obligation and motivation. Women’s intrinsic motivation increases if the program meets their individual needs. This suggests the importance of tailoring interventions to individual needs, which appears to improve user engagement in both men and women according to findings by Schubart et al. 4 The therapist plays an important role in overcoming barriers in treatment, as he or she makes the program more personal and enhances women’s motivation.
In addition to previous research, indicating better adherence to supported e-health interventions than to unsupported e-health interventions independent of gender,4,8,11,53 our results now show that women express a wish for more support during e-health treatment to help them overcome barriers in treatment. In agreement with findings of Waller and Gilbody 54 and Schneider et al., 11 who investigated experiences of both men and women, some women view e-health treatment as complementary rather than as standalone treatment.
Two studies investigated an e-health intervention based on the principles of at-home physical exercise. In the study of Cranen et al., patients with chronic pain were asked about their expectations of home telerehabilitation. In the study of Björk et al., women with stress urinary incontinence received an e-mail-guided Internet-based treatment or a non-guided postal treatment. The results of these studies similarly show that women performing physical exercises at home in the absence of a therapist worry whether they perform the exercises correctly. In the study of Cranen et al., women expected the therapist to touch them during the exercises and were concerned about the quality of the feedback without the therapist being physically present. In the study of Björk et al., women expressed a wish for physical examination at start of their treatment, to reassure that everything looked normal, and for a confirmation that they were using the right muscles. Thus, women undergoing at-home physical exercise seem to be in need of guidance from a therapist that is physically present.
Although women may gain a feeling of self-control and empowerment during e-health treatment on one hand, their insecurities about their own performances in the absence of a personal confirmation may negatively enforce them on the other hand. This balance might be of great importance for a successful treatment. Face-to-face guidance from a therapist is needed to strengthen women’s power during e-health treatment, especially during at-home exercise.
Limitations
Our systematic review has some limitations. First of all, limitations that apply to systematic reviews in general, such as the risk of publication bias and the risk of incomplete retrieval of literature, also apply to our study. As we only included publications in the English or Dutch language, language bias could not be ruled out. A disadvantage of using one tool for quality assessment is the possibility of missing articles that would have been included if we had used another tool. Nevertheless, we believe that the tool we used is one of the most accurate ones. Because we aimed to learn more about women’s perceptions of e-health, we included all studies involving female patients. We also included studies involving predominantly male patients, because we believe that every opinion might be of value, as qualitative research aims to provide insights into individual’s thoughts and feelings rather than to measure the incidence of various views and opinions. We included one study involving 14 women and 1 man, in which outcomes were not reducible to gender, but decided to accept this detail because we expected its effects on our results to be minimal. As with any other overview, another limitation is that patient populations, interventions and outcomes differ between studies, which may affect comparison and interpretation of results.
As the results of this review predominantly relied on women’s self-reporting, they may be at risk of social desirability or reporting bias, which should be taken into account while interpreting the results. Because women that are more familiar with the Internet are more likely to engage in e-health interventions, there is a risk of selection bias in all included studies. This risk is further enhanced as some studies recruited their participants by online advertisements. Due to the limited number of studies for each condition, it was impossible to make subgroup analyses, and no conclusions can be drawn, therefore, regarding individual conditions. Finally, some of the statements may not be related to e-health treatment in particular but to undergoing treatment in general. We do believe, however, that we conducted a review based on the best available evidence as we used extensive search strategies and only included articles with sufficient methodological quality.
Conclusion
The findings of this study support the hypothesis that e-health lowers barriers to healthcare in women who might otherwise not seek help. The anonymity of the Internet also helps women to disclose their feelings. Findings show that an online therapeutic relationship can develop, although some women experience this online relationship as less close than a relationship established in a face-to-face setting. Reduced feelings of obligation and lack of motivation are women’s greatest challenges in completing e-health treatment. Therefore, women often express a wish for more substantial monitoring and some form of face-to-face contact. More research needs to be conducted to determine what women might benefit from e-health interventions.
Practice implications
The outcomes of this review provide insight into women’s expectations and experiences regarding e-health. This information may help healthcare providers and policymakers to develop e-health interventions that are tailored to women’s wishes. Generally speaking, e-health appears to be well accepted by women. Due to its perceived anonymity, e-health may be particularly attractive to women with disorders that are perceived to be embarrassing or stigmatizing, such as urogenital and intimate problems. Its flexibility may enable women with competing priorities, such as working women and women with caregiver responsibilities, to integrate e-health into their everyday lives. As e-health appears to be helping women to overcome barriers to treatment, a subset of women who would otherwise not receive healthcare may be reached. In order to increase women’s motivation to complete their treatment and thus improve their treatment’s chances of success, we recommend that e-health interventions are combined with face-to-face sessions, which is also referred to as “blended care.”
Footnotes
Appendix 1
Acknowledgements
The authors would like to thank Mrs R. Deurenberg-Vos and Mrs E. Pieters, advisor information specialists at the Radboud University Medical Centre Nijmegen, the Netherlands, for their contribution in developing the search strategy and Mr R. Stuve for his language assistance.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.