
Abstract
Research has shown that the quality of care is compromised when healthcare providers respond inappropriately to patient language and cultural factors. However, research indicates that medical education is not keeping pace with the changing composition of the patient population in culturally diverse societies such as Canada and the United States, and many healthcare providers do not possess the attitudes or skills required to be effective within a culturally diverse healthcare setting. Here, we present Fydlyty, a web-based, low-fidelity serious game for medical-based cultural competence education. Fydlyty includes both a scenario and dialogue editor providing the ability to develop conversations, interpret responses, and respond to questions/answers from the game player. These responses are based on predefined cultural characteristics of the virtual patient and on different moods that the virtual patient may express depending on the situation. The results of a usability experiment conducted with medical professionals and trainees revealed that the game is easy to use, intuitive, and engaging.
Introduction
Cultural competence in healthcare has been broadly defined as the ability of medical professionals and organizations to understand and integrate individual values, beliefs, and behaviors that are shaped by various factors, including race, ethnicity, nationality, language, gender, socioeconomic status, physical and mental ability, into the delivery and structure of the healthcare system. 1 When medical practitioners possess cultural competence skills, it generally leads to better communication between them and the patient, and better doctor–patient communication leads to increased patient satisfaction, decreased misdiagnosis, better patient outcomes, and better quality of care. 2 However, health professionals do not automatically possess the attitudes or skills that are needed to be effective within a culturally diverse healthcare setting. Despite the proliferation of cultural competence programs in medical schools particularly throughout North America, research indicates that medical education is not keeping pace with the changing composition of the patient population in culturally diverse societies such as Canada and the United States, 3 even though the quality of care is compromised when healthcare providers do not respond appropriately to patient cultural factors. 2
In the context of medical education, simulation can be defined as an education technique that allows interactive and immersive activity by recreating all or part of a clinical experience without exposing patients to associated risks. 4 Simulation can include devices, technologies, computer programs and virtual spaces, scenarios, standardized patients, and a host of other methods of imitating real-world systems. 5 Simulation (and virtual simulation in particular), offers an alternative to practice in an actual medical environment (e.g. in an operating room, or emergency ward), offering learners/trainees the opportunity to train until they reach a specific competency level. Furthermore, in contrast to working with live patients (and animals), virtual simulation allows learners to intentionally make and correct mistakes. 6 This latter benefit is particularly important since errors in practice serve as a reflection point for learners and educators alike, providing a reference point for the delivery of feedback that drives learning. The rising popularity of video games has seen a recent push toward the application of video game–based technologies to teaching and learning. Serious games (i.e. video games that are used for training, advertising, simulation, or education), provide a high level of interactivity not easily captured in traditional teaching/learning environments. Serious games take advantage of video games to motivate and engage players/learners for a specific purpose and in education, strong engagement has been associated with academic achievement. 7 As with simulation, with respect to medical education, serious games provide medical trainees the opportunity to acquire both cognitive and technical skills outside of the medical environment in an engaging, cost-effective, and ethically safe manner. They allow trainees the opportunity to train until they reach a specific competency level, thus better preparing them before exposure to live patients or before entering physical training centers which are costly to maintain/operate and whose availability may be limited. In contrast to traditional teaching environments where the teacher controls the learning (e.g. teacher-centered), serious games and virtual simulations present a learner-centered approach to education, so that the learner/trainee controls the learning through interactivity thus permitting an active, critical learning approach. 8 Serious gaming can potentially bridge the simulation and gaming worlds by harnessing the educational value of technology-enhanced simulation to teach specific technical or cognitive skills to learners (not only the trainees but patients too), alongside the motivational, interactive, and engaging benefits inherent in games. 9
Kripalani et al. 10 provide an overview of current approaches to cultural competence education, and based on features of successful programs, and by drawing upon established educational principles, they propose a list of nine elements that may improve cultural competence training in medical education including the following which we believe lend themselves nicely to the use of virtual simulations (serious games): (1) use of interactive educational methods such as standardized patient encounters and role play, (2) providing direct instructor observation and feedback, (3) discussing competence throughout the span of one’s clinical education rather than doing so in isolated workshops, and (4) promote cultural diversity at all levels of medical school.
Given the importance of cultural competence in medical education, the fact that cultural competence education is not keeping pace with the changing composition of the patient population in culturally diverse societies, the benefits of serious games, and their ability to fulfill many of the elements suggested by Kripalani et al. 10 to improve cultural competence education, we have developed Fydlyty, a web-based, low-fidelity serious game for medical-based cultural competence education and training. Fydlyty provides an engaging, easily accessible and modifiable, and cost-effective cultural competence training tool that we believe will help improve medical-based cultural competence education. Fydlyty includes both an easy-to-use scenario and dialogue editor that provide medical educators (who may have limited technical experience), the ability to develop conversations, interpret responses, and respond to questions/answers from the game player. These responses are based on predefined cultural characteristics of the virtual patient, and on different moods that the virtual patient may express through facial expression, body language, or speech, depending on the situation. The results of an experiment conducted with medical practitioners and trainees to examine the usability and the ability of the game to engage its users revealed that the game is easy to use, intuitive, and engaging.
The remainder of this article is organized as follows. In section “Background,” an outline of prior related work is provided. Details regarding Fydlyty are provided in section “Fydlyty.” Experimental methods and results are presented in section “Experimental procedure,” while a discussion of the results is provided in section “Discussion.” Finally, concluding remarks and plans for future work are outlined in section “Conclusions.”
Background
Various recent literature reviews related to the application of virtual simulation and serious gaming to medical education are available (e.g. see De Ribaupierre et al. 9 and Wang et al. 11 ) and thus will not be presented here. Despite the availability of various medical education-based virtual simulations and serious games, few have focused specifically on cultural competence. In this section, a brief overview of serious games that are relevant to cultural competence education are presented. The overview is followed with a brief discussion regarding some of the limitations with these approaches.
Zeilke et al. 12 developed a serious game for the United States military whereby the environment is representative of rural and urban Afghan culture. The game player takes on the role of a socially active member of the society and his or her individual actions not only affect the attitude of a virtual non-player character (NPC) but also the society at large. The goal of the game is to: (1) win over NPCs (which represent members of the Afghan culture), by following cultural norms, and (2) characterize the emotional mood of the NPCs (i.e. happy, sad, angry, or frustrated), based on their actions and interactions in the virtual world. This virtual world is asymmetric and non-linear, hence making it similar to the real-world, where inhabitants have an unpredictable behavior. Kim et al. 13 present BiLAT, a game-based simulation and tutoring system that was developed to provide students, initially United States military officers, with an environment to practice preparing for and conducting real-world bilateral negotiations within a safe learning environment. Trainees progress through a scenario and their success with the scenario is linked to their ability to apply the principles and best practices of negotiation. Initially, the system was developed with 10 meeting partners (virtual characters) living in an unspecified Iraqi town. The student, a US Army officer, must work with these people in the town to resolve various town issues. Trainees can employ various meeting and negotiation strategies whether good and bad (e.g. the trainee can socialize by choosing the action “Flatter host,” or “Compliment locale,” or “Talk about religion”). A preliminary assessment study to examine the effectiveness of BiLAT was conducted and results indicate significant situation-judgment gains by novice trainees. Facade 14 employs low-fidelity computer graphics to render a virtual couple. The player’s actions in the virtual world influence the course of the conversation and events that occur during the scenario. Facade provides the user with an interactive experience of human relationships. The user, from a first person perspective, is witness to the ups and downs of another couple’s relationship. The user can interact with the NPCs using sentences in text format or using the mouse and clicking on objects present in the virtual world. The game player here is not provided with any direction and is free to play according to his or her will. The NPCs respond to the player’s open-ended questions or statements very quickly making it highly immersive. To provide culturally relevant nursing care and provide nursing trainees with the opportunity to develop transcultural nursing skills, in collaboration with the Nursing department at the University of North Carolina at Charlotte, Sakpal and Wilson 15 developed Sita, a life-sized (projected) virtual patient representing a 24-year-old Indian girl. Students ask Sita a list of required questions to which Sita will reply. Depending on how the questions are posed and the student’s body language, Sita’s response will reflect the cultural dimensions of young, Indian females. 15 Conradi et al. 16 proposed a three-dimensional (3D) immersive environment using Linden Lab’s virtual world, Second Life. Their immersive environment models different sections of the university to provide paramedic students a realistic environment to which they can relate to. This 3D environment is suitable for professionals who are in different parts of the world and require access from a remote destination. Players joining remotely can communicate with the virtual patient through text-based chat or using their mouse as an input device. These actions will trigger responses from the virtual patient that will help them to proceed in the virtual world. Five specific scenarios were designed and tested, and although not specific to cultural competence, the scenarios could be designed to incorporate cultural competence components.
Summary
A dialogue between the virtual patient and the player in the majority of virtual simulations and serious games is typically based on a set of predefined questions and answers. The dialogue scripts become redundant and the scenarios can be anticipated. Furthermore, many of the virtual characters (patients) lack emotional traits which are an important entity when teaching cultural competence and are a normal component in human–human communication. That being said, developing serious games that employ complex dialogues and scenarios in addition to virtual characters/patients that exhibit emotions is not trivial and can be costly. This is further complicated by the fact that traditionally, developers of virtual simulations and serious games strive for high fidelity (fidelity is defined here as the extent to which the appearance and/or behavior of the simulation matches the appearance and behavior of the real system). 17 Fidelity has potentially significant implications for designers and developers of virtual environments in general, given that with our current technology, we cannot faithfully recreate a real-world scenario particularly across all of the senses, 18 let alone, past research has been inconclusive with respect to the effect of visual fidelity on learning. 19
The Fydlyty serious game incorporates a scenario editor and dialogue authoring tool (DAT) that was specifically developed to allow for the creation of new scenarios or the modification of existing ones, in a simple and intuitive manner. Fydlyty can not only enhance cultural competence skills in medical students, but can also enact an extensive variety of scenarios that involve communication between two or more people. Fydlyty is a web-based application that employs low-fidelity visuals making it easily accessible to educators and students globally with minimal hardware requirements.
Fydlyty
Fydlyty has been designed to address two types of users: (1) educators/curriculum designers, and (2) trainees (game players). The trainees are the game players who take the role of the medical professional and play the game while the educators/curriculum designers are able to create scenarios, modify dialogue scripts, and assess the overall progress of each trainee. At the start of each session, the trainee, taking on the role of a medical professional, begins at the “index” page. The index page provides an overview of the scenario. More specifically, as shown in Figure 1, left part of the index page depicts the virtual patient while on the right of the index page, the preliminary description of the patient is provided. These traits include (1) name, (2) gender, (3) marital status, (4) role of player, (5) context, and (6) scene. The context and scene provide a short introduction to the game, motivation behind it, objectives, and cues of how to proceed forward in the game. This basic information helps the trainee familiarize himself or herself with the game environment before starting the actual conversation. At the bottom, a counter keeps track of the time elapsed from the start to the end of the conversation. A comment box provides the player with feedback while they progress through the scenario. The game world is viewed in a first person perspective and the mouse is the primary source of input from the trainee to the system.
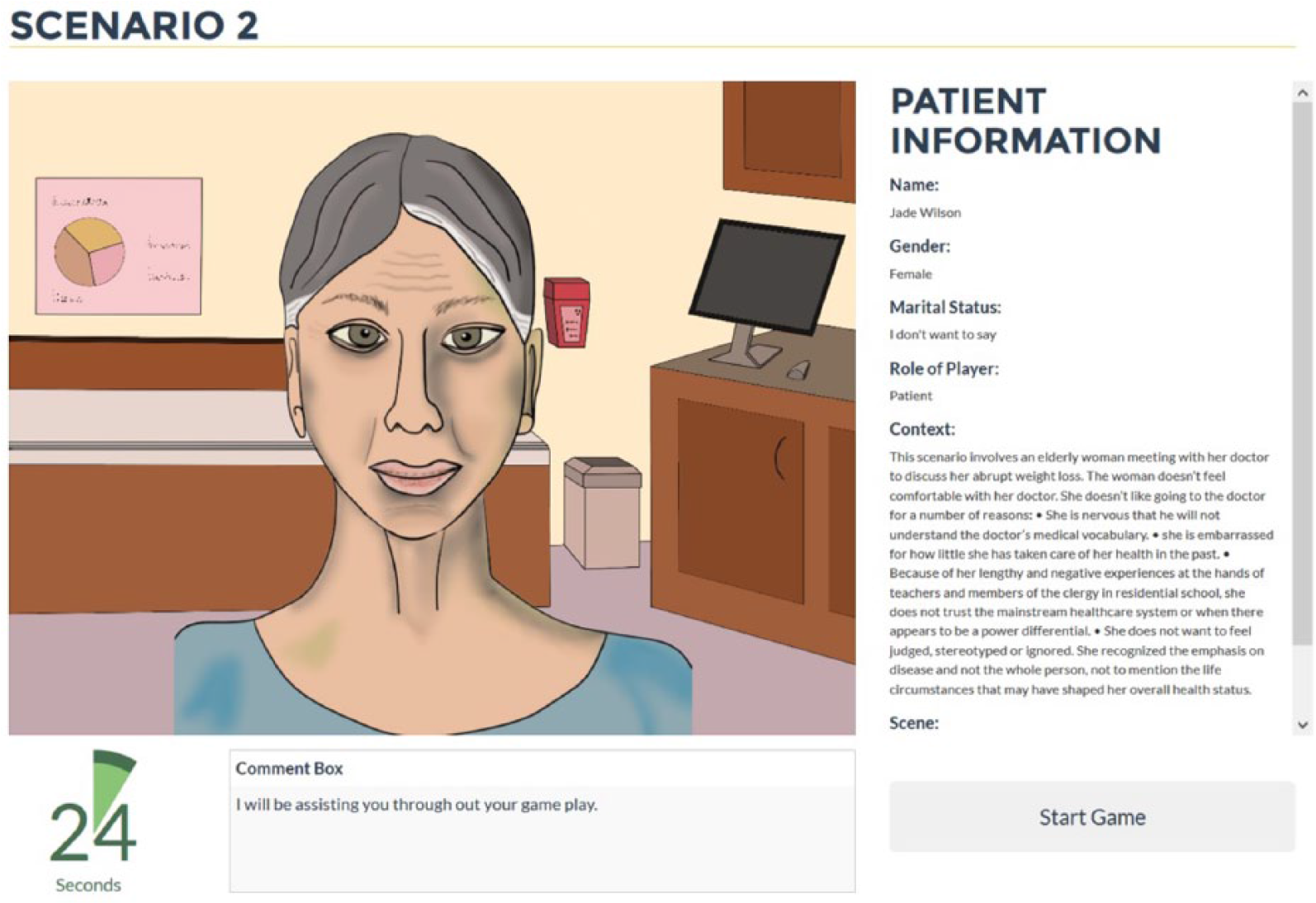
Patient information screen shows the information regarding the scenario and the virtual patient.
After obtaining the virtual patient’s information, the trainee proceeds by clicking on the “Start Game” button at the bottom of the page which leads to the next page (see Figure 2). At the top right section is the virtual patient console (labeled at (a) in Figure 2). This console shows automated replies from the virtual patient so that the trainee reads and accordingly chooses his or her next reply. The next section (labeled (b) in Figure 2) provides a list of potential replies that the trainee can choose. The virtual patient will have a counter response to each selection. This response can be verbal (e.g., an answer to the question), physical (e.g., change in the mood), or both. Verbal responses will be shown in the virtual patient console, whereas physical responses will be depicted by the change in the virtual patient’s expressions.
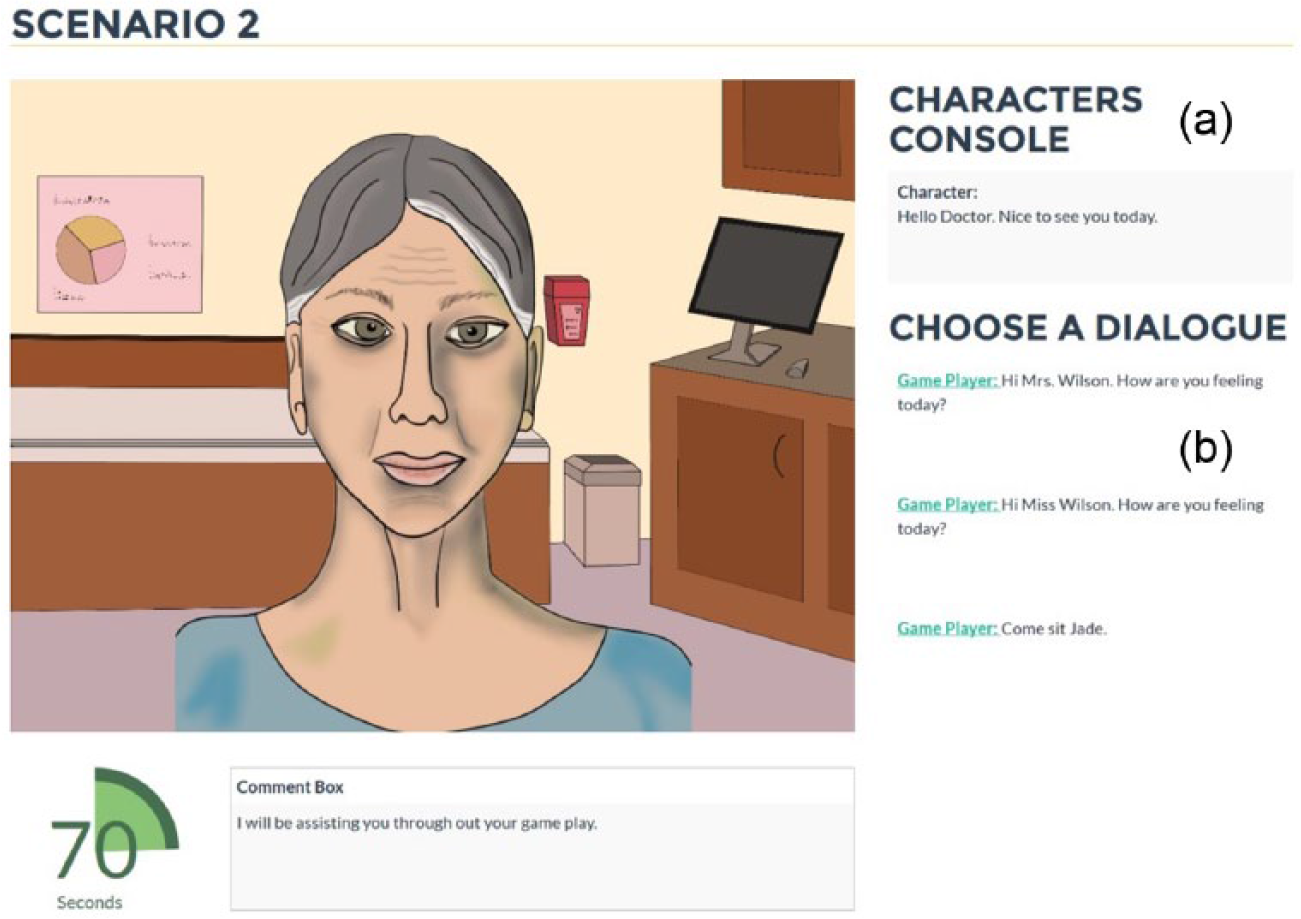
(a) Virtual patient console and (b) choices for player.
Virtual patient
The fidelity of the patient can be either basic or advanced. Here, fidelity is defined with respect to facial expression, body language, and voice-based dialogue. The virtual patient in the advanced fidelity level includes facial expressions and voice-based dialogue. Figure 3 illustrates the allowable moods that are expressed via the virtual patient’s facial expression. The eyes, lips, and forehead of the virtual patient are clearly visible to the game player, providing enough cues to judge any exhibited emotions. On the contrary, with respect to the basic fidelity level, as illustrated in Figure 4, although the virtual patient exhibits body expressions, it is difficult to judge any facial expressions. In this example, the body language is a convenient form of expressing one’s gratitude or disapproval. Both virtual patients can be categorized as low-fidelity designs at least with respect to graphical fidelity.
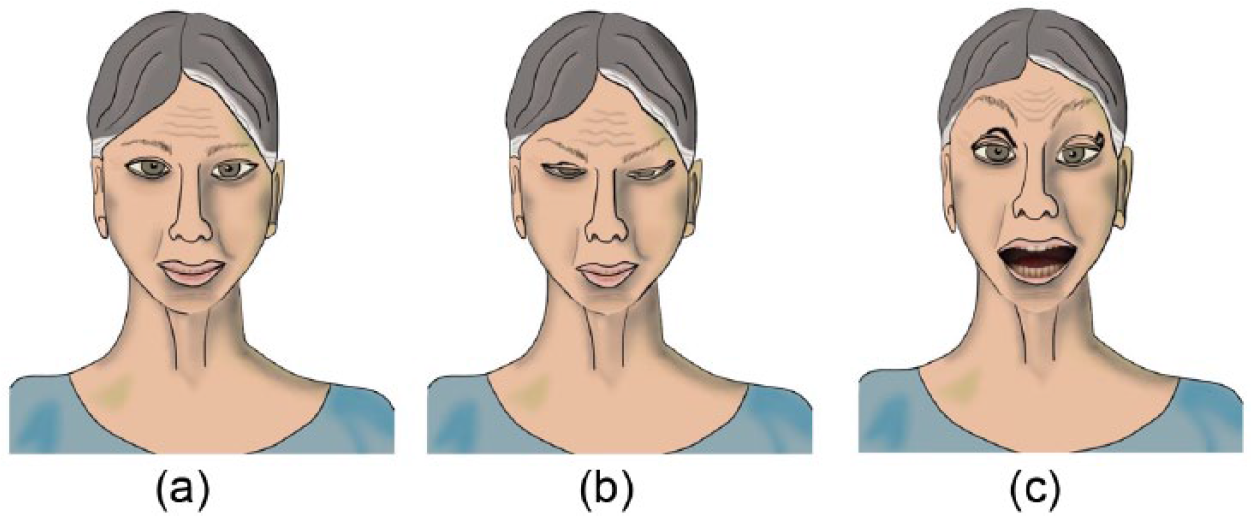
Advanced fidelity level. The facial expressions for each of the three virtual patient moods: (a) neutral, (b) upset, and (c) angry.
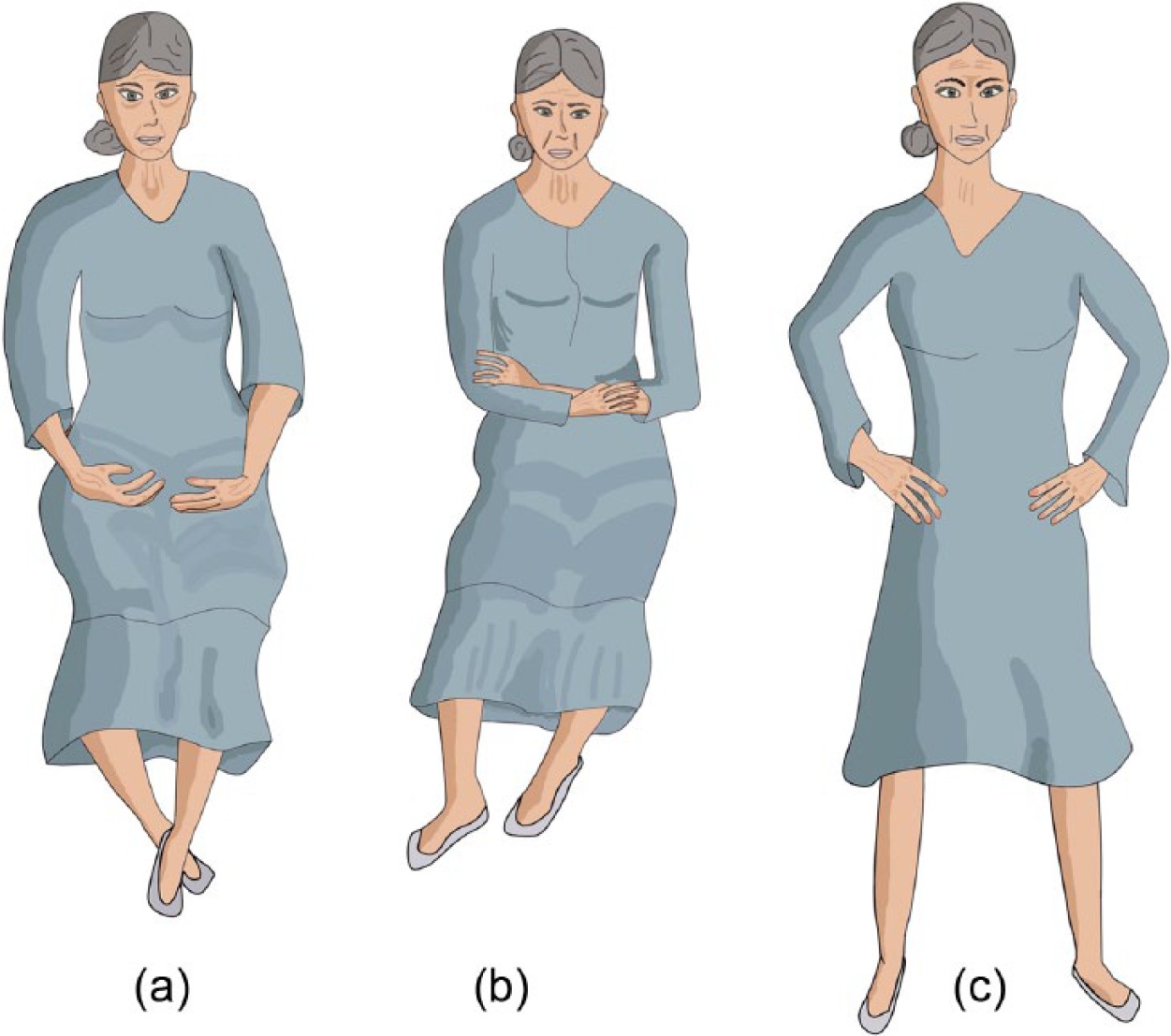
Basic fidelity level. The body language for each of the three virtual patient moods: (a) neutral, (b) upset, and (c) angry.
Scenario editor
The scenario editor design is based on: (1) background, (2) virtual patient(s) (whose mood can be neutral, upset, or angry), (3) script, and (4) role of the game player. The background is represented by an image (JPEG or PNG) that is rendered at the interface level when each scenario is loaded. Similar to the background, the virtual patient is also comprised of a set of images or avatars created using Real Illusion’s Crazy Talk. Each set of the virtual patient images (files) represents three different moods (i.e. neutral, upset, and angry). These images are rendered in a seamless manner so that the game player cannot determine any change on the screen during game play. Depicting different moods also provides the trainee with immediate feedback, and more specifically, with a sense of achievement (when the mood is positive), or concern (when the mood is negative). The script that each scenario is based on consists of: (1) context, (2) scene, and (3) dialogues. The context describes the circumstances that form the setting of the event so that the game player can fully understand and assess the environment. The scene describes the characters involved in the event and the location where it will occur. Finally, the dialogues, which are uploaded using a comma-separated version (CSV), describe the narrative between the game player and the virtual patient, are described in greater detail in the following section.
The dialogue authoring tool
The DAT has two primary functionalities: (1) to manage dialogues (read, write, and update) in the dialogue database and (2) propose different variations of each dialogue to the educator when a new dialogue script is uploaded in the system. The original dialogue script is uploaded by the educator as a CSV file. The DAT reads the original dialogues from the file and saves each dialogue with reference to its parent. Once the original hierarchy is saved in the database, the DAT will then create different variations of each trainee’s dialogues that were previously stored. The DAT now refers to a predefined list of phrases which it will use to replace the original phrase with. Depending on the number of alterations, the new mood (upset or angry) is associated with the dialogue. Each dialogue is editable, making it the educator’s added responsibility to ensure that the final dialogue script is grammatically and factually correct.
Debriefing
Once the trainee reaches the end of the scenario, the system redirects the user to the debriefing page which displays a summary of the session from the start to the end. The debriefing page is divided into two sections. The first section provides an overview of the player, the scenario he or she played, and the time in seconds taken to complete the scenario. The second section is directly related to the game play. It shows the virtual patient’s dialogue (if the game player started the conversation, then the response of the virtual patient), the choices the trainee was given during the game, the response he or she chose out of the provided choices, and the mood of the virtual player after the choice was made by the trainee.
Technical details
Fydlyty was developed on the open-source Django framework and utilizes the Model View Controller (MVC), design pattern. All of the graphical models were created in-house using Adobe PhotoShop and Autodesk Maya. The animations for the advanced level avatar were accomplished using the facial animation software Crazy Talk, a tool that employs voice and text to animate facial images. The Interactive Plug-in is an add-on for Crazy Talk that allows developers to convert and export Crazy Talk avatars for web-based application. These assets can be shown on any browser screen using the unity-web plug-in. All of the virtual patient dialogues stored in the database are dynamically converted (during game play) to audio files using Google Text to Speech (GTTS). MySQL is used to store the data associated with a scenario.
Experimental procedure
Participants
The participants were five volunteer medical professionals and nine trainees from the (University of Ontario Institute of Technology). All participants were female with the minimum, maximum, and average age of 18, 58, and 35 years, respectively. The authors did not participate in the experiment and the experiment abided by the (University of Ontario Institute of Technology) Ethics Review process for experiments involving human participants.
Experimental methods
The experiment took place in a small room with dimensions of 12.2 m × 6.0 m × 2.5 m. Participants were seated in front of a laptop computer (Alienware 14) connected to a mouse, keyboard, and a 21″ extended display (the game was displayed in full-screen mode). Only the participant and the experimenter were in the room. Once the participants were comfortably settled and understood the instructions provided, they played the game (all participants played the same scenario), in the Mozilla Firefox browser. In this scenario, the participants took on the role of a physician and the virtual patient was an elderly female named Jade Wilson who visited her doctor to discuss her abrupt weight loss. This particular scenario was selected from a list of already existing doctor–patient excerpts related to cultural competence. 20
Upon completion of the scenario, participants were asked to complete two questionnaires. The first questionnaire was based on the Questionnaire for User Interaction Satisfaction (QUIS), developed by a multi-disciplinary team of researchers to assess users’ subjective satisfaction with specific aspects of the human–computer interface and is highly reliable across many types of interfaces. 21 QUIS-based questions are classified into five categories: (1) overall reactions to the game, (2) learning which occurred through the game, (3) system capabilities, (4) satisfaction with teaching methods, and (5) self-confidence in learning. The second questionnaire was the Game Engagement Questionnaire (GEQ) which contains 19 questions and provides a psychometrically strong measure of levels of engagement specifically elicited while playing video games. 22 Upon completion of the questionnaires, participants were asked to complete several “open-ended” questions regarding the game. These open-ended questions were answered using a 5-point Likert scale.
Experimental results
Figures 5 to 10 present a graphical summary of average values for the responses to the QUIS-based questions. The minimum and maximum values in this category were 4.8 and 7.3, respectively. To a great extent, participants claimed that the interaction with the system was very easy (7.3), and a wonderful experience (6.1). The average score was 6.5 when asked if the interaction with the system was satisfying. However, participants felt that the interaction with the system was not very flexible (4.8). With respect to graphics and sound, participants believed that the amount of information displayed on the screen was adequate (7.1). They also felt that the information was logically placed on the screen (7.0). With respect to the graphics and sound quality, the average values received were 5.3 and 4.7, respectively. The perceived fidelity of the visual scene was similar (4.8). Although these values are on the lower end of the scale, it should be noted that the system in discussion is a low-fidelity design (with respect to visuals/graphical rendering) and does not claim to provide high visual fidelity that would generally require high-end computational resources. The average values for the category “Learning to play the game” were highly ranked. The participants believed that learning to operate the system was easy (8.3), getting started was easy (7.6), commands were easy to remember (8.3), learning to use the system was fast (8.4), and the feedback obtained to complete the steps within the scenario was clear (6.1). Furthermore, the minimum and maximum average score for the systems capabilities was 7.2 and 8.6, respectively. Therefore, to a great extent, the participants were satisfied with the speed of the system (7.4), response time (7.4), rate at which information was displayed (7.2), system reliability (7.6), operation dependability (7.9), and system dependability (8.6).
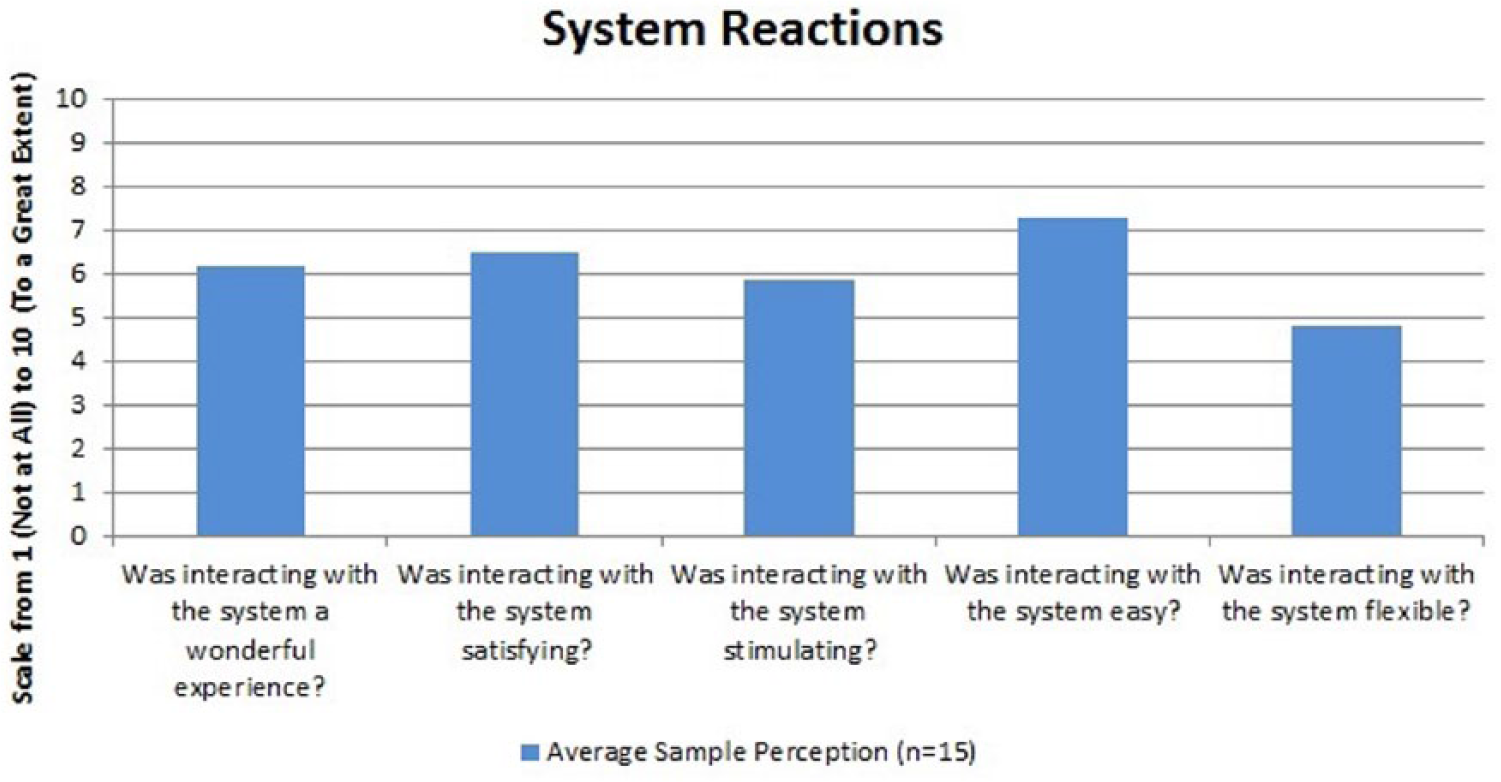
Experimental results: system reactions.
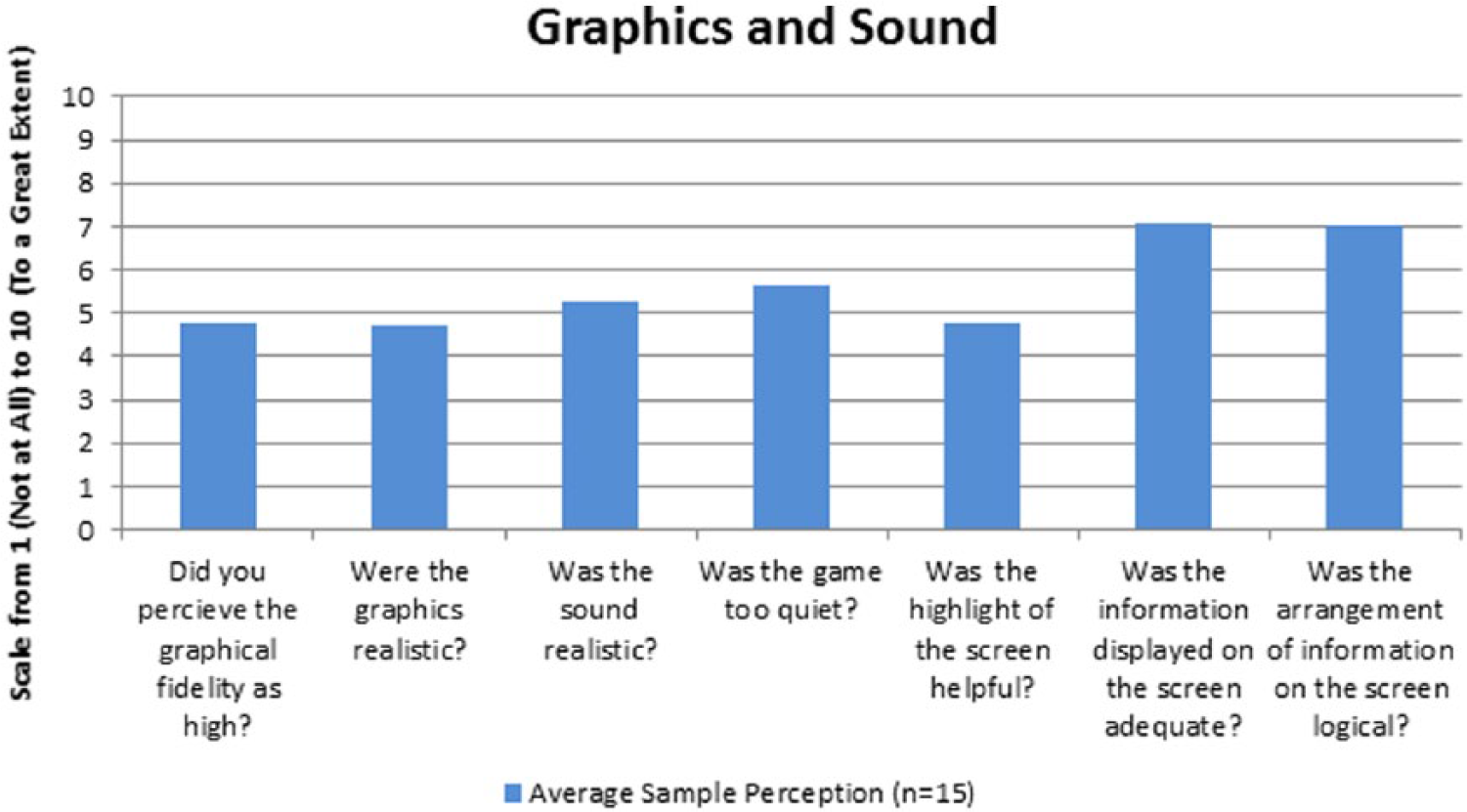
Experimental results: graphics and sound.
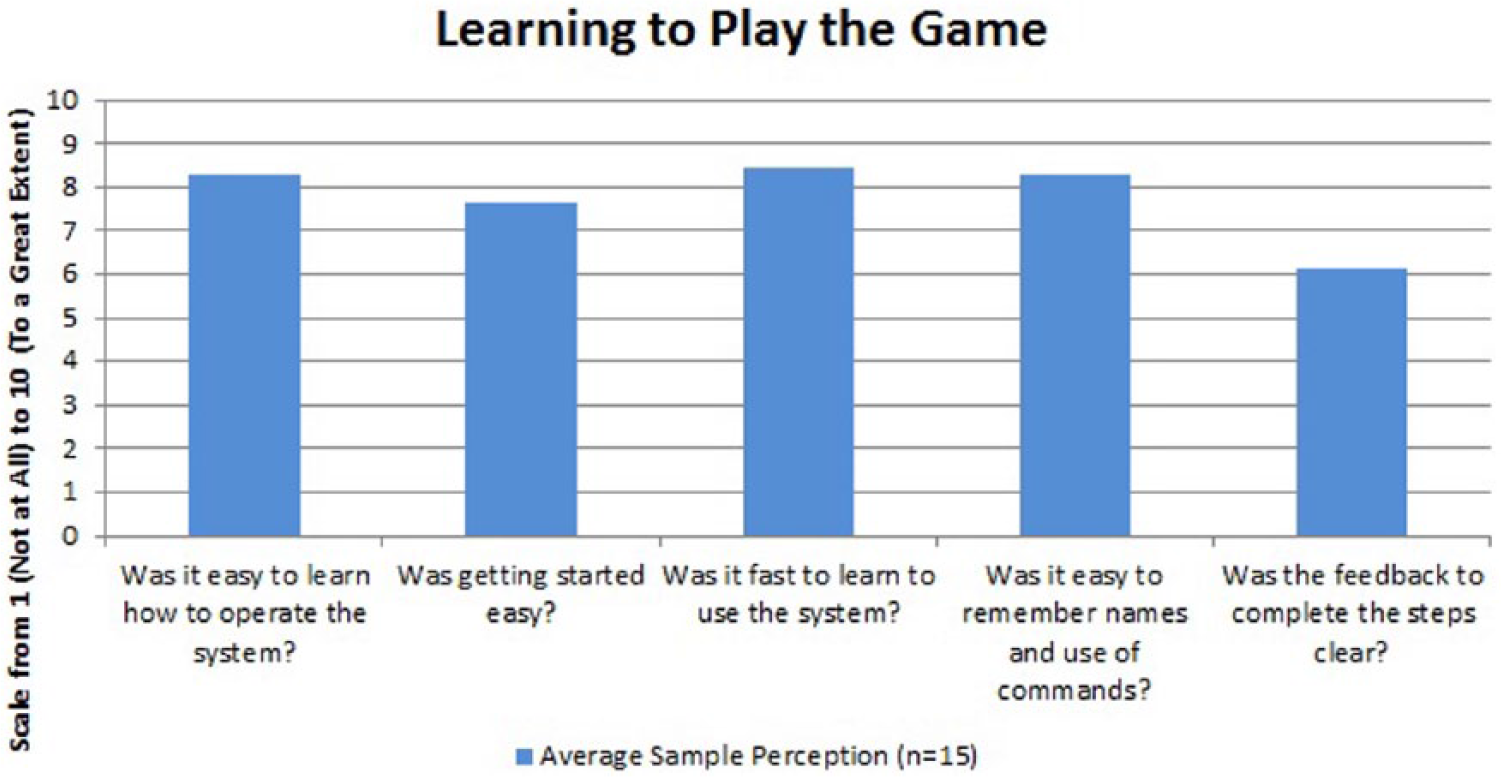
Experimental results: learning to play the game.
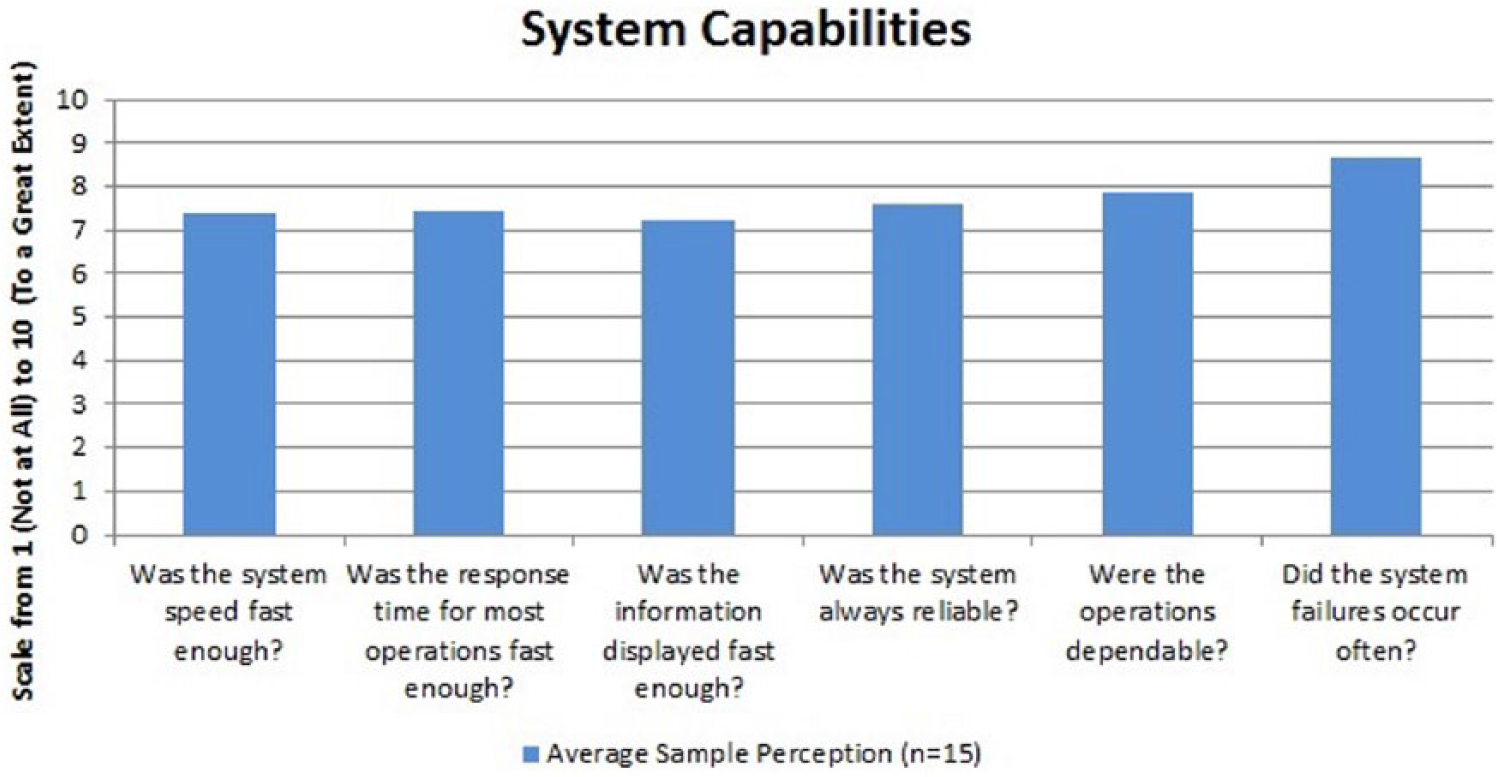
Experimental results: system capabilities.
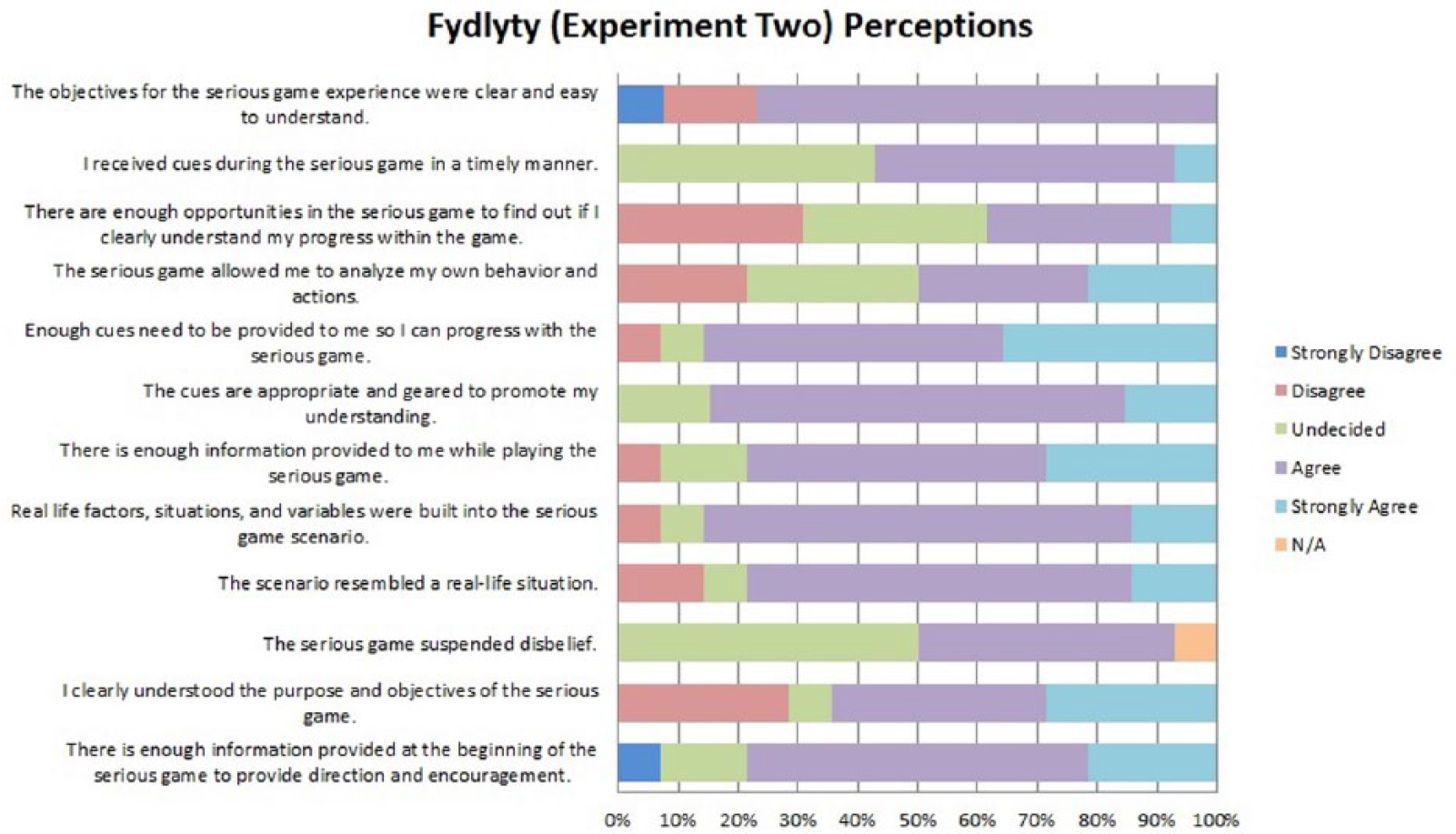
Experimental results: user perceptions I.
Experimental results: user perceptions II.
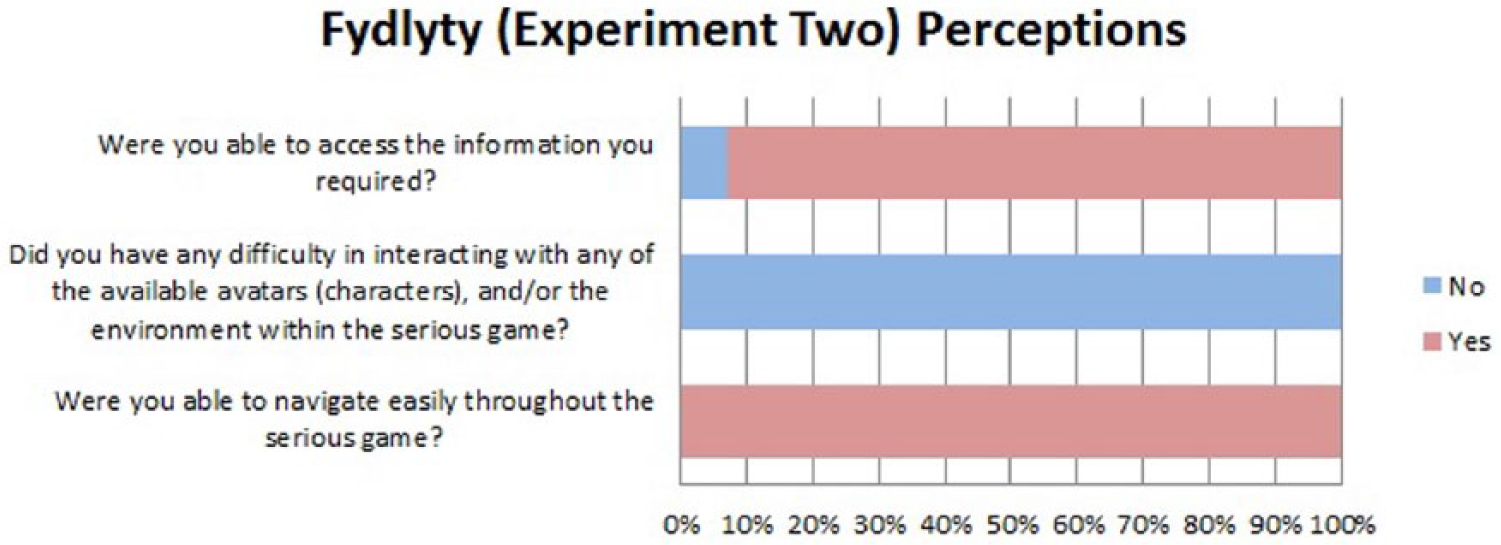
The results (percentages) for the subset of open-ended questions are graphically presented in Figures 11 and 12. In all, 77 percent of the participants believed that the objectives of Fydlyty were presented clearly and were easy to understand. When asked about the cues in the game, 57 percent said that they received cues in a timely manner, 86 percent claimed that enough cues were provided to progress in and complete the game, and 84 percent thought that the cues were appropriate to promote understanding. Furthermore, the majority of the participants believed that the scenario resembled a real-world situation (78%) and that real-world factors were built into the game (76%). In total, 63 percent agreed that they clearly understood the purpose and objectives of the Fydlyty serious game. Approximately 39 percent agreed that the game provided enough opportunities to find out about one’s progress. All of the participants stated that they did not have any difficulty in interacting with the virtual patient, and all of the participants claimed to navigate through the game easily, with a majority of them (93%), were able to access the information they required.
Experimental results: absorption/immersion.
Experimental results: flow.
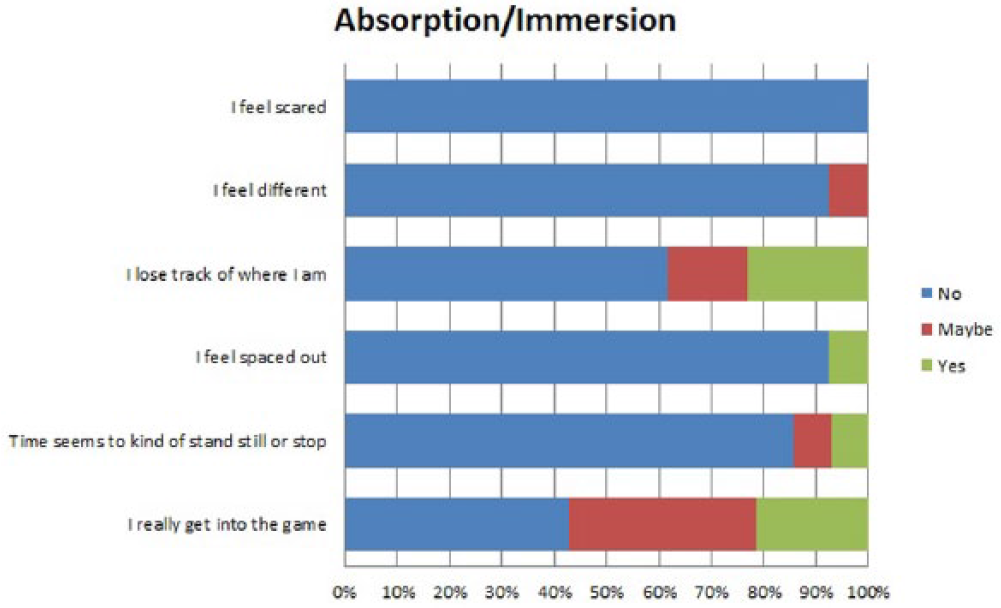
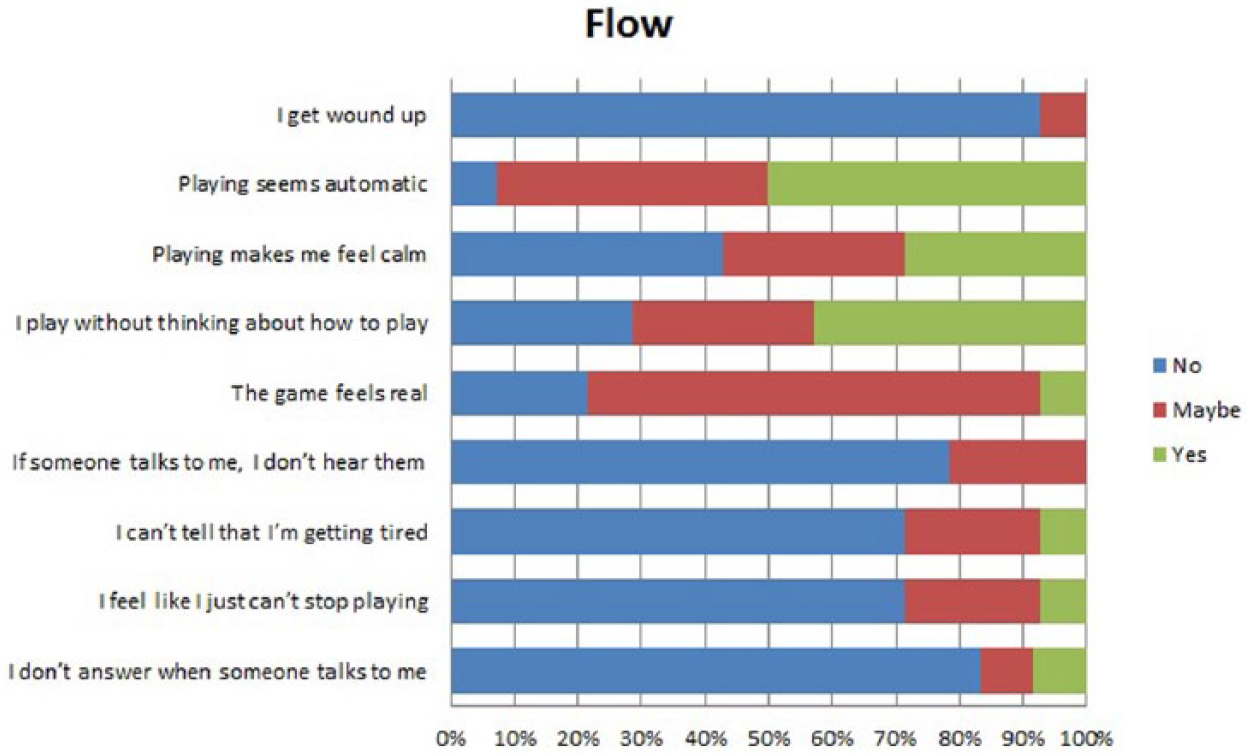
With respect to the GEQ results, the average values for absorption and immersion are presented graphically in Figure 11. Examining the results for immersion, only a small percentage of participants (21%) believed that they were immersed into the game. However, 36 percent remained indecisive. Similarly, on average, the participant response to the measure of absorption was “No.” The majority of the participants did not feel scared (100%), different (92%), lost track of time (62%), spaced out (92%), or that time stopped while playing the game (86%). Lower absorption scores indicate the need of improving the user experience perhaps through the use of more advanced interactions and sounds. With respect to flow (see Figure 12), 50 percent of the participants believed that playing the game seemed automatic, whereas 43 percent were indecisive. A majority (93%) believed that they did not get “wound up” while playing the game. When asked if the game felt real, 71 percent participants were indecisive and only 7 percent said “Yes.” Furthermore, 43 percent claimed that they played the game without thinking about how to play it (29% indecisive), and 29 percent believed that playing the game made them feel calm. A majority of the participants (71%) believed that events in the game seemed to happen automatically while they played (see Figure 13). In total, 35 percent were indecisive when asked if their thoughts paced quickly during game play while 21 percent did believe their thoughts paced quickly. A majority of the participants (62%) did not lose track of time, and 86 percent claimed that they did not play the game longer than they were asked to do so.
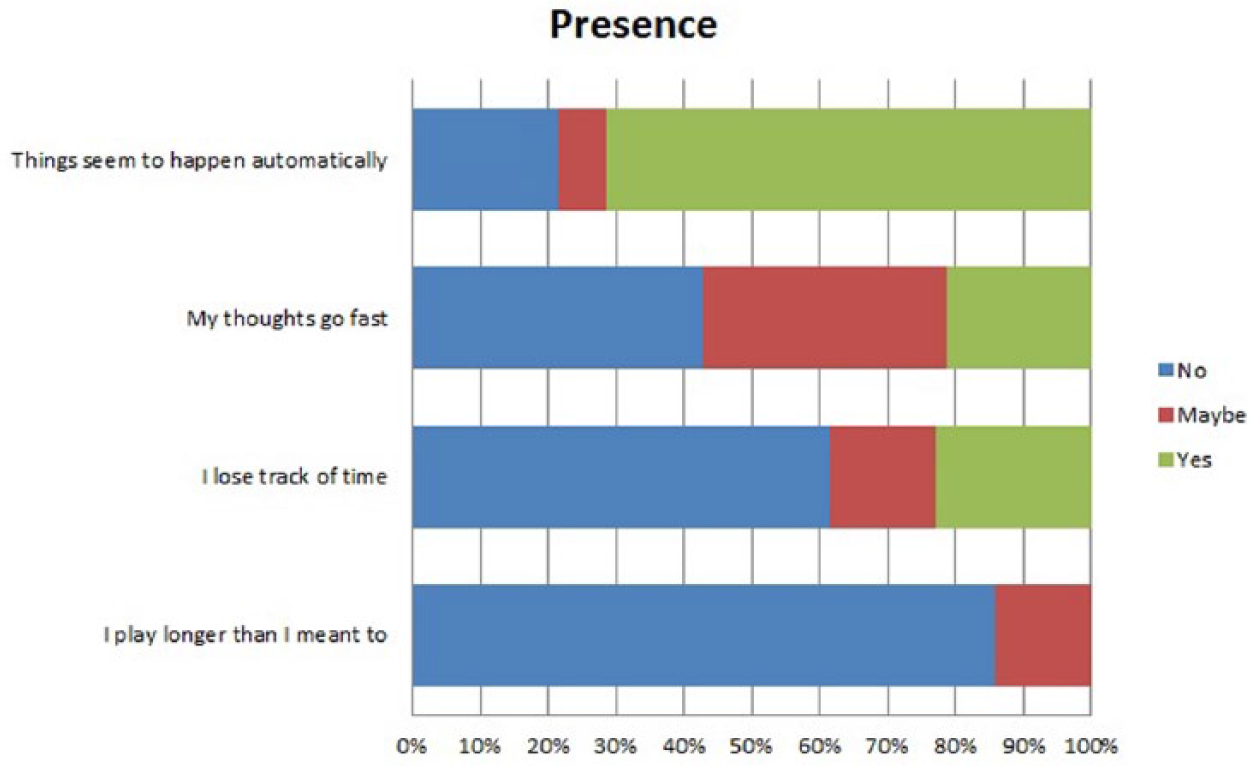
Experimental results: presence.
Discussion
The QUIS-based results regarding the system capabilities and system interface are very encouraging. More specifically, participants believed that the interaction with the system was a “wonderful experience” (6.1), satisfying (6.5), easy to use (7.3), fast to respond (7.4), reliable (7.6), and dependable (7.9). Furthermore, to motivate users to play a game again and again, it is viable to provide enough opportunities to learn how to play the game. Gee 23 describes the initial levels of a game as “hidden tutorials,” which are essential in setting up the users’ cognitive skills for solving complex problems in the game ahead. Fydlyty provides initial steps in the scenario where the trainee, taking on the role of a medical professional, is provided information regarding the virtual patient and then responds to something as simple as a salutation. During these introductory steps, the trainee receives ample opportunity to learn how to play the game; this is reflected in the participant feedback. To a high extent, participants also agreed with the amount of information provided on the screen and its arrangement (approximately 7.0 each). With respect to graphics and sound, the average sample perception was not highly rated (4.7 and 5.3, respectively). However, it should be reinforced that audio and visual cues were rendered in a low-fidelity environment without burdening any computational resources.
The measure of absorption was very low for both the medical professional and trainee participants. A high majority believed that they did not feel scared (100%), different (92%), spaced out (92%), or lost track of where they were (62%). These results can be explained as follows: (1) the low-fidelity design, and (2) a disconnect from the scenario provided in the experiment. The former cannot be relinquished without assessing the effect of using this tool to learn cultural competence skills in medical-based education. Although this is beyond the scope of this article, it will be addressed in the future. Fydlyty is a tool to help educators and experts to develop various scenarios, and therefore, new and improved scenarios can be added to the system. Furthermore, absorption is interrelated with immersion and plays an important role in the participant immersion. 24 Even though the majority of participants did not feel immersed, the results for immersion have been distributed across the three categories (i.e. No = 43%, Maybe = 36%, and Yes = 21%). When asked if the game felt real, 71 percent of the participants were indecisive. This is very encouraging in respect to a low-fidelity design. Improvements in the current design, and adding a few components such as a story-line, can refine the results. The majority of the participants (86%) believed that they did not play the game longer than they were required to. Adding game elements (e.g. multiple levels, leaderboards, or scoring elements) may improve the attention span of the game player captured by the game.
In the free-form section of the survey, the participants were asked what they best liked about Fydlyty. Some of the notable responses are as follows:
It was quick yet effective. It got you involved and interacting due to the emotions it elicited. (Anonymous, September 2015) How it related the medical portion of what I am studying. (Anonymous, September 2015) Made you think of the implications of your actions more than just blindly acting. (Anonymous, September 2015)
The participants also highlighted the issue regarding the limited responses provided to the trainee by the system. Some comments are as follows:
The response options were limited. The feedback (when I noticed it) didn’t really provide a lot of information about why a response might be inappropriate. The patient responses were always the same, regardless of which option I chose. (Anonymous, September 2015) Feeling forced to select response options that did not necessarily reflect how I would want to interact with the patient. (Anonymous, September 2015)
When asked if the participants felt that the serious game would be useful for improving cultural competence skills, a majority of the participants (64%) believed that such a tool can be used effectively for cultural competence training:
Yes, if certain scenarios are expanded/developed. It would be a good space to teach (maybe evaluate) some of the soft skills. (Anonymous, September 2015) Yes as it will make people aware of how important their responses are perceived by other people, people particularly who do now share the same cultural. (Anonymous, September 2015)
Conclusion
Here, we presented Fydlyty, a low-fidelity, web-based serious game for medical-based cultural competence education. Fydlyty allows for a wide variety of scenarios to be easily developed and/or edited using a simple scenario editor, ensuring it is practical across a wide variety of areas and applications. A study was conducted with medical professional participants to examine the usability, engagement, and satisfaction of Fydlyty. The results of this study revealed that the web-based low-fidelity tool provided an easy-to-interact interface for professionals and trainees along with being highly accessible to them. Furthermore, it was also noted that medical trainees, with little to no gaming background, felt comfortable while using the tool and did not face trouble while completing the scenario. Although greater work remains, the results presented here encourage the development of a simple (and low-budget), low-fidelity serious game and highlight the simplicity, accessibility, and reliability of using a web-based platform.
Future work will examine what, if any effect low-fidelity visuals (graphics) have on learning. This will be accomplished through a pre- and post-testing study that will include three groups of participants: (1) control group which will not use Fydlyty but will receive all of the educational material using traditional methods, (2) a group that will use the low graphical fidelity version of Fydlyty, and (3) a group that will use Fydlyty with higher graphical fidelity and auditory cues.
Footnotes
Acknowledgements
The financial support of the Natural Sciences and Engineering Research Council of Canada (NSERC) in the form of a Discovery Grant to B. Kapralos is gratefully acknowledged. The financial support of the Social Sciences and Humanities Research Council of Canada (SSHRC), in support of the Interactive and Multi-Modal Experience Research Syndicate (IMMERSe) initiative, is also gratefully acknowledged.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.