
Abstract
Telemonitoring is one of the most expedient answers to the strong need for preventive care imposed by the rapidly aging society. We propose an innovative solution to the detection of early signs of frailty by presenting a serious game controlled by a smart sensorized soft plastic ball, designed to achieve continuous home-based monitoring of muscle weakness in older adults. Design, development, and testing of the smart ball and of the game interface devised to guide the monitoring procedure are presented. Reliability and concurrent validity of the system in measuring maximal grip strength against the clinical standard Jamar® were evaluated. Serious game usability and acceptance were investigated on 26 elderlies. Smart ball and Jamar measurements were well correlated (0.76 and 0.80 for dominant and non-dominant hands) and test–retest reliability of pressure measurements was excellent (intraclass correlation coefficient >0.94). The serious game was well accepted by the 96.1 percent of participants, who provided a strongly positive usability score (87.7/100). The smart ball–driven serious game demonstrated excellent reliability and good validity in measuring grip strength. The proposed smart ball–driven serious game can be used for home self-monitoring of grip strength in elderlies.
Introduction
Home telemonitoring is defined as the use of information technology to monitor the user’s status directly at home, where it is used to prevent hospitalization, to improve the feeling of safety, and to empower the patient to manage his or her chronic condition.5,6 Home telemonitoring presents several advantages for community-dwelling elderlies. It offers senior users the possibility to stay in their familiar home environment where they feel safe and comfortable. In addition, the awareness of being under continuous monitoring has a positive impact on their sense of security and quality of life, 7 since they become active participants and not mere passive recipients of health services. 7 Another undeniable advantage is that telemonitoring can identify abnormal behaviors earlier than during a routine screening visit or a medical emergency, 7 thus allowing prompt intervention.
Although the potential benefits of telemonitoring have been well established, there are challenges to be faced before such approach goes mainstream. One of the key obstacles for the uptake of telemonitoring is represented by user’s acceptance. 8 To face this problem, two useful approaches are transparency and user’s engagement; thus, effort should be made to develop systems able to collect reliable and accurate measurements in an unobtrusive and enthralling way. To increase transparency, a possible solution is represented by the use of smart objects, that is, the augmentation of everyday objects with sensing, communication, and networking technology to support specific tasks. 9 In this framework, recent studies have been achieving monitoring of elder users through the implementation of instrumented daily-use objects, such as a cane 10 or insoles. 11 On the contrary, to boost user’s engagement, we have observed a surge of gameful design in the healthcare domain, 12 including assessment, training, and rehabilitation. In this context, gamification, defined as the use of game design elements in non-game contexts, 13 is leveraged to motivate the user and enhance his or her experience. 14 In the context of aging, serious games, defined as games that do not have entertainment, enjoyment, or fun as their primary purpose, 13 have shown their usefulness for both rehabilitation and assessment in the physical 15 and cognitive 16 domains.
In the aging society, an important and increasingly recognized pathology is the “frailty syndrome,” known as the reduction of the individual’s homeostatic reserve, which is the redundancy of physiological functions used to overcome health insults. 17 Age-related decline results in increased vulnerability for which minor stressors can trigger disproportionate changes in the person’s health status. As proposed by Fried et al., 18 a phenotype of frailty is identified by the presence of three or more of the following components: unintentional shrinking, muscle weakness, poor endurance and energy, slowness, and low physical activity level. As for muscle weakness, it is usually measured as the dominant hand’s maximal grip strength. 19 Besides forming a key part of frailty, weak grip strength per se represents an important and powerful predictor of a range of health outcomes. 20 Indeed, several studies have shown a close relationship between a decrease in grip strength and age-related functional decline,21,22 disability in the activities of daily living, 23 and mortality rates. 24 The most widely used instrument to quantitatively assess grip strength is the hydraulic Jamar® handheld dynamometer, which returns the maximal isometric force (in kilograms) exerted by the user while squeezing the handle of the dynamometer. In spite of the prevalent clinical use of the Jamar, which comes with the most extensive set of normative data, the isometric nature of the instrument may cause discomfort in patients experiencing conditions such as rheumatoid arthritis, lateral epicondylitis, or carpal tunnel syndrome. 25 To overcome this problem and increase the comfort of use, recent studies have investigated the concurrent validity of pneumatic instruments, such as the Martin Vigorimeter, compared to the Jamar, reporting very positive results. 26 The Vigorimeter, different from the Jamar, measures the pressure exerted on a bulb attached to a manometer via a tube. The use of both instruments, however, remains restricted to the clinical practice. 27
Weakness, together with the other elements of frailty, tends to slowly but constantly progress over time and, with the current model of care, there is the risk that the onset of muscle weakness might go undetected or identified too late. To face this problem, home telemonitoring can be leveraged to alert formal or informal caregivers when possible early signs of frailty are detected. Concerning grip strength, a first example of a device for home-based self-monitoring of handgrip strength was conceived by Jaber and colleagues,28,29 who proposed to instrument an inflatable plastic ball with a pressure sensor. The sensor was tested without being inserted in the object, reporting a relatively low sensitivity that could hamper its use in detecting small yet relevant changes in handgrip strength.30,31 Most importantly, the work by Jaber and colleagues did not provide the user with a protocol that guaranteed the validity of the measurements. However, when it comes to home-based self-monitoring of maximal grip strength, it is hard to obtain a valid measure without any control on the modality of use.
The current work aims at implementing reliable and transparent home-based monitoring of handgrip strength, specifically envisaged for the early detection of frailty in independent older adults. To do so, we created a system consisting of a smart antistress ball that embeds absolute pressure and inertial sensors placed inside the closed device and transmits data wirelessly to control a serious game. The game was developed with the twofold aim of hiding the burden of the monitoring purpose through a compelling activity and vouching for adherence to the clinical protocol. 32 In the current work, first, design, development, and validation of the smart sensorized antistress ball are presented. The validated device was then used as an input tracker in the serious game implemented to monitor handgrip strength. Finally, the designed game was tested on 26 elderlies to investigate usability and validate the ability to effectively guide the monitoring procedure.
Materials and methods
The system
The system is devised to monitor handgrip strength in older adults, consisting of a smart sensorized plastic ball that controls a computer game.
Smart ball
The smart ball is designed to measure the user’s pressure exerted with handgrip and is intended to be used as an input tracker for a computer game. To be effectively deployed, requirements and specifications have been identified in collaboration with clinicians.
To resemble as much as possible a real antistress ball, the object should have a diameter smaller than 8 cm to allow an ergonomic grasp. To look like a real daily-use object, the electronics should be placed entirely inside the ball. The Spordas ALLBall® soft plastic sphere was chosen for its deformability, which permits to squeeze the ball with the maximum force without creating an excessive deformation, and its size (7.6 cm diameter), which allows an ergonomic grip. In addition, the chosen ball presents a valve to allow inflation, which is a necessary requirement for a close object.
As a second requirement, wireless data transmission should be provided with at least a 30-Hz frequency to obtain real-time interaction during gameplay. The Bluetooth Low Energy (BLE) protocol has been selected for wireless data transmission since low power consumption is key to reduce the charging frequency and enable long-lasting charge. In addition, BLE technology is characterized by short wake-up and connection times, which make it an optimal solution to increase usability during gameplay. A proprietary protocol was implemented for BLE transmission of all raw data. Application programming interfaces (APIs) have been implemented for data transfer from the ball to the host at 50 Hz.
In terms of sensors, the ball should be equipped with an absolute pressure sensor able to measure grasping pressures (i.e. the difference between the total absolute pressure and the initial pressure of the ball) corresponding to a grip force in the range 0–60 N. 33 To be used as an input tracker for computer games, the ball should also be instrumented with a tri-axial accelerometer and gyroscope to detect movement. The battery should be rechargeable and chosen as a trade-off between encumbrance minimization and duration maximization. An LED should be included to notify battery discharge. We looked for suitable electronics that could have been reliably inserted inside the ball plastic shell. Among the available solutions, the SensorTile evaluation kit (EVK) by ST industries (©STMicroelectronics) was selected since it combines three desirable features: compactness, modularity, and flexibility. The SensorTile is a tiny module (13.5 × 13.5 mm2) that packs all that is required for our application. In particular, the BlueNRG-MS single-mode network processor, compliant with Bluetooth specification v4.1, was used to implement BLE connectivity. Among the wide spectrum of motion and environmental MEMS sensors included in the SensorTile, the three-dimensional (3D) accelerometers and gyroscopes (LSM6DSM) and the absolute pressure sensor (LPS22HB: optimal pressure range: 260–1260 hPa; 24-bit pressure data output) were leveraged. Moreover, to acquire, filter, and transmit the signal, the 80-MHz STM32L476JGY microcontroller was used. Finally, the certified 100 mA h Li-ion rechargeable battery of the tile was selected.
A printed circuit board (PCB) was developed to connect the SensorTile with the external battery charger and to control the battery state (through the BLE battery level state characteristic). The PCB also activates two operational LEDs to indicate the state of the battery (red) and the keep alive status of the ball (green).
All the electronics are protected by a 3D-printed plastic case and inserted in the soft plastic sphere, which is cut on one side and then closed with a 3D-printed rigid plastic part, to which the plastic case is attached. The final weight of the smart ball is 54 g.
To recharge the battery enclosed inside the ball, induction charging has been chosen. A wireless charger has been designed and 3D printed to host the recharging circuit powered by a USB cable (Figure 1).
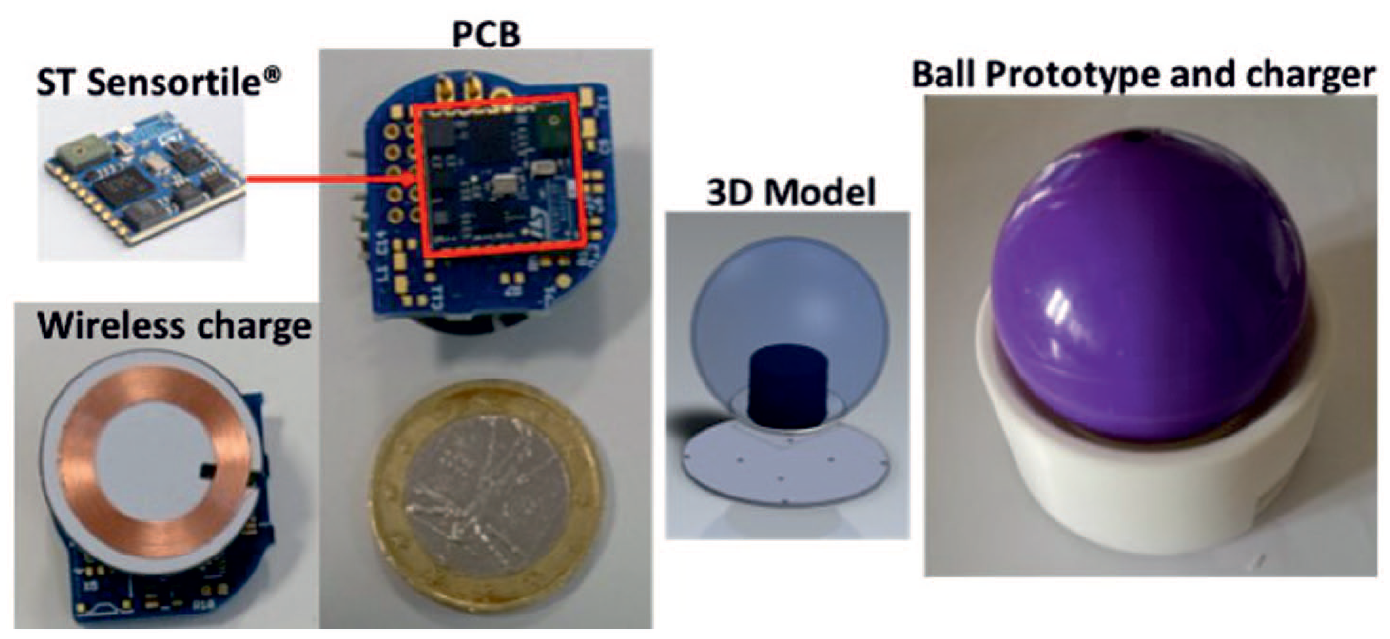
From left right: The SensorTile mounted on the PCB, the WiFi battery charger, the 3D model of the prototype with the internal case to protect the electronics, and the final prototype of the ball placed in its charging station.
The game
The core of this work is the implementation of a serious game to mimic the American Society of Hand Therapists (ASHT) 34 protocol required to assess maximum handgrip strength, consisting of three 3-s trials of maximal force with a minimum of 15-s between-trial rest. The game is targeted to older users and it should thus follow some practical guidelines recommended when designing games for elderlies. 35 The game should be engaging and rewarding, but at the same time simple, since elderly people often suffer from a reduced attention span. The game should be displayed on a large monitor or computer screen and allow to be played while sitting.
The game was developed in Unity 3D and the ball was used as the input tracker. The.NET Core libraries were used to set up the communication with the ball through BLE protocol, and the game was built as a Universal Windows Platform app to be run on a CPU device. Such choice was based on the need to display the game on a wide screen, such as a computer monitor or TV screen, to increase usability for the elder user. 35 Nevertheless, the use of Unity 3D allows to build the game under several platforms, including iOS or Android, in order to obtain apps for tablet or smartphones.
Before gameplay, the user can select to visualize a tutorial to receive instructions about the game itself, the recommended posture, and the use of the ball. When the game is launched, once a connection with the smart ball has been established, the battery level of the object is checked. If the smart ball is running out of battery, gameplay is not allowed and a message is displayed to the user to inform him or her about the need to put the object under charge.
To replicate the ASHT protocol, the game includes three scenes. In the Rocket launch scene (Figure 2(a)), subjects are guided to squeeze the ball with their maximal strength for 3 s. The rocket’s size increases according to the exerted force (ΔP). At the end of the 3-s period, the rocket is launched (Hitting Stars scene; Figure 2(b)) and starts hitting stars and collecting score points. The greater the force exerted, the highest is the level reached by the rocket and the points gathered. An encouraging message “Good Job” is displayed. To implement the resting phase between two consecutive maximal force trials, as required by the ASHT protocol, the Wheel of Star scene is used (Figure 2(c)). In this scene, the rocket spins in the center of five stars of different sizes arranged in a circle. The highest score is associated with the smallest star. The user is instructed to turn the smart ball to shoot and hit a star. Such rotation is detected through the module of the angular velocity, acquired through the ball’s gyroscopes, based on a threshold algorithm. The sequence of the three scenes is repeated three times in a row as requested by the ASHT protocol, for a total duration of about 1 min.
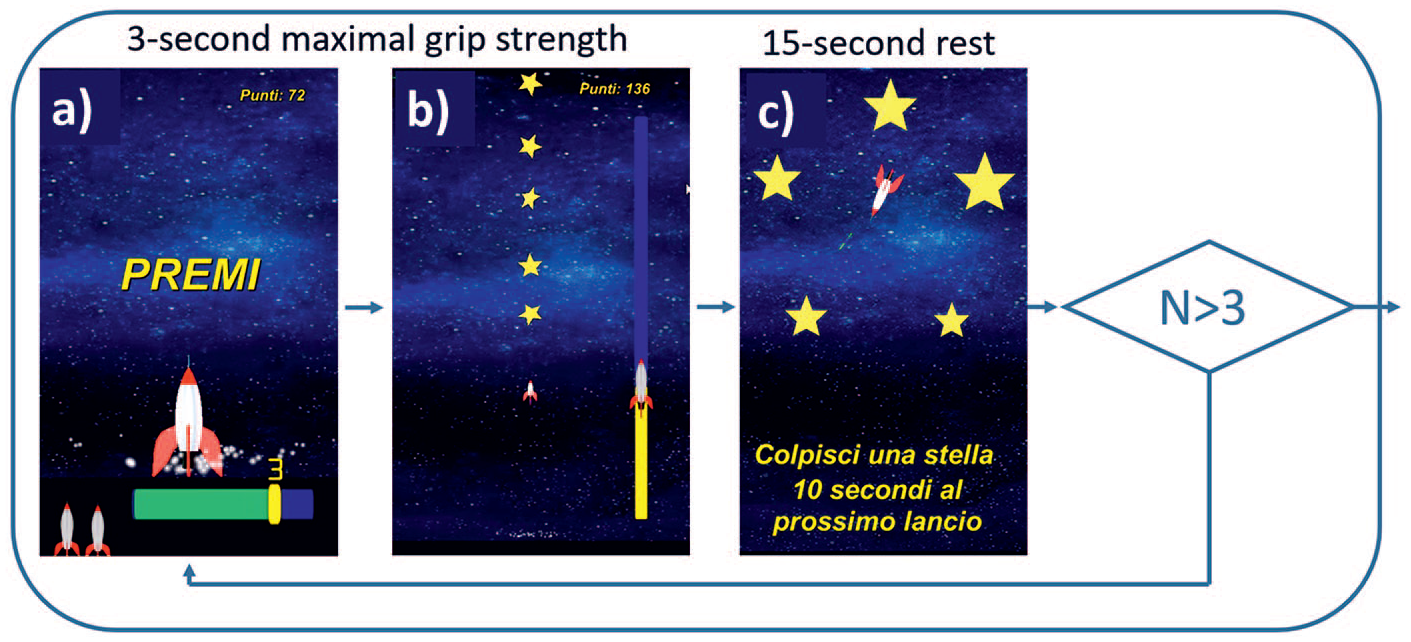
Computer game scenes implemented to test maximal grip strength. Panel a: Rocket launch scene - the user is guided to squeeze the ball with his(her maximal strength for three seconds while the rocket increases in size according to the exerted force. Panel b: Hitting Stars scene - the rocket is launched to a level proportional to the maximal grip strength and collects stars (score points). Panel c: Wheel of Star scene - the rocket spins in the center of five stars of different size (and value) and the user is instructed to turn the smart ball to shoot and hit a star.
At the end of gameplay, a message is displayed to show the user the final score and, since the game is envisaged for a longitudinal use, also to inform him or her whether the performance improved compared to the previous time. However, game score is not directly correlated to the user’s maximal grip strength, since it is composed by the sum of the points obtained from the three launches of the rocket (proportional to the force exerted) and the points earned when shooting at a star in the Wheel of Star scene. In this way, the user is encouraged to squeeze the ball as strong as possible to obtain a higher game score but, at the same time, he or she is not directly informed about the force exerted. On the other hand, for every game session, the user’s maximal grip strength, together with the raw data collected from the sensors of the smart ball, are collected and stored in a separate file. In this way, data collected during gameplay allow us to longitudinally keep track of the user’s muscle weakness.
Protocol
The Ethical Committee of Politecnico di Milano approved the study protocol including both the concurrent validity tests against the Jamar (section “Validation against the Jamar dynamometer”) and the serious game usability tests (section “Game testing”).
Smart ball validation
To validate the use of the smart ball as a reliable device to monitor handgrip strength, a twofold validation test was carried out: (1) reliability of the measures provided by the smart ball at different initial pressures was studied using an electromechanical testing system and (2) concurrent validity of the smart ball in measuring the user’s maximal grip strength was tested against the clinical standard, using a Jamar dynamometer.
1. Validation against an electromechanical testing system
The force applied to the smart ball was quantified by means of the MTS Synergie 200 electromechanical testing system. This system is controlled in displacement and is equipped with a load cell to measure the force provided with an accuracy of 0.56 percent in the range 50–1 kN. The force range used was limited between 50 and 200 N to avoid any possible damage to the internal electronics, especially when the ball was highly deformable (as for low initial pressures). The smart ball was placed inside an ad hoc 3D-printed case, which tried to mimic the contact area of a hand (40 cm2) while squeezing a 7-cm diameter handle. 33 The ball, fixed inside the case, was positioned between the two extremities of the actuator, as shown in Figure 3. Four levels of initial pressure (P0 = 1.0, 1.1, 1.2, 1.4 bar) were used and each level was tested twice. In each trial, the MTS system exerted a compression to the ball that was increased in steps of 10 N. The variation in the pressure values measured by the ball (ΔP) in correspondence to the exerted force steps was stored. The acquired data were used to evaluate both the relative and the absolute reliability of the ΔP measured by the ball at different initial pressures and to support in the selection of the most appropriate initial pressure P0.
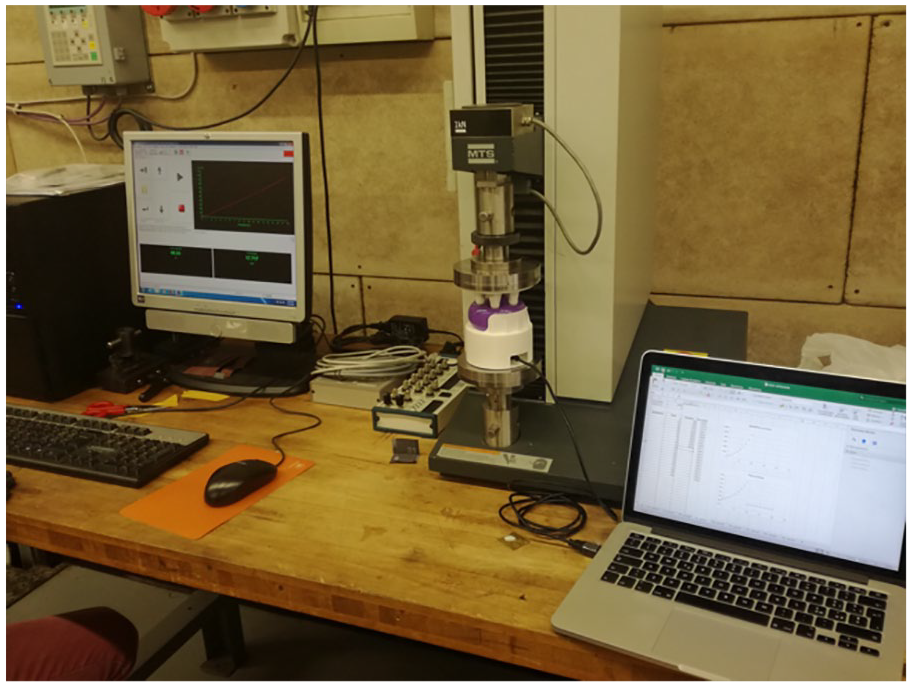
The experimental setup used to validate the reliability of the measure of absolute pressure provided by the smart ball at different initial pressures (P0). The ball, fixed inside the 3D-printed plastic case, is positioned between the two extremities of the actuator. On the left, the unit to control the displacement of the actuator. On the right, the laptop with the software for acquiring data from the smart ball.
2. Validation against the Jamar dynamometer
Using both the Jamar dynamometer and the smart ball, each participant was asked to perform his or her maximal grip strength with both hands following the guidelines of ASHT. 34 Subjects were asked to sit straight on a chair with the forearm at rest in neutral position and the elbow flexed at 90°. Three 3-s trials of maximal force with a minimum of 15-s between-trial rest were performed for each of the two devices using both hands. Dominant and non-dominant hands were always alternated. The order of the devices and of the hands was randomized to avoid any possible systematic error due to fatigue or training.
Game testing
The serious game was tested with a twofold aim: to evaluate usability and acceptance of the game and to assess concurrent validity and reliability of the maximal handgrip strength measured during gameplay.
Each subject was asked to perform one game session using his or her dominant hand. After completion of the game, the subject was asked to fill out a questionnaire made up of two parts: (1) the Italian version of the System Usability Scale (SUS) 36 —original scores were converted into a 0–100 range and a total score above 68 would be considered above average; 36 (2) a set of questions related to gameplay which included Likert-type scale and open questions. More specifically, the following Likert-type scale questions were included: (a) I found the game interface amusing and intuitive, (b) I felt at ease when using the smart ball to control the game, (c) I would like to use this system at home, and (d) I am very satisfied with the experience. The open questions, instead, asked the user: (a) Is this the first time you practice a similar computer game? (b) List possible perceived discomfort in the use of the system, (c) Indicate the most appreciated aspects in the use of the system, and (d) Indicate the least appreciated aspects in the use of the system.
Participants
Tests with adults were performed to study both the concurrent validity tests against the Jamar (section “Validation against the Jamar dynamometer”) and the serious game (section “Game testing”). The exclusion criterion was any diagnosis of neurological and vascular disorder affecting the upper limbs.
Sample size was calculated to test the concurrent validity of the use of the smart ball with the clinical standard; to do so, a population size of at least 50 subjects was estimated, considering a significant correlation coefficient (r) of 0.5, a statistical power of 80 percent, a type I error of 1 percent, and allowing a 20 percent dropout rate. Among the total subjects, a subgroup of at least 25 older adults (age ⩾65 years) was required to test the computer game on target users.
A total of 55 subjects (age 49.3 ± 24.7 years; gender: 22 males and 33 females; dominant hand: 55 right-handed) were recruited to test the concurrent validity of the use of the smart ball with the Jamar dynamometer. Among them, gameplay was tested on the subgroup of older adults, composed of 26 subjects (age: 73.96 ± 6.52 years; gender: 10 males and 16 females; dominant hand: 26 right-handed; education: 13.9 ± 5.3 school years).
Statistical analysis
Smart ball validation
1. Validation against an electromechanical testing system
First, for each of the four P0 tested, a one-way repeated measures analysis of variance (ANOVA) was used to compare the ΔP measures in the two sessions in order to ensure the absence of any systematic error. 37 Then, relative reliability was assessed computing the intraclass correlation coefficients (ICC two-way mixed-effects model, absolute agreement). ICC values of 0.70–0.85 indicate good and excellent reliability, respectively. 38 Absolute reliability was assessed computing the standard error of measurement (SEM), estimated as the square root of the mean square error term in the repeated measures ANOVA.37,38 Then, the measurement error was estimated by the minimum detectable change (MDC) calculated as follows

where 1.96 is the z score associated with the 95 percent level of confidence, and the square root of 2 reflects the additional uncertainty introduced by using difference scores based on measurements made at two time points. 39
2. Validation against the Jamar dynamometer
Separately for dominant and non-dominant hand, concurrent validity between the smart ball and the Jamar measures was assessed through correlation analysis. 40 Given the data normal distribution (Lilliefors test), the Pearson correlation coefficient was used.
Separately for the four sets of measurements obtained from the two devices using both the dominant and the non-dominant hands, one-way repeated measures ANOVA was used to compare the values of maximum strength obtained from the three repetitions to assess the absence of any systematic error. 37 Relative reliability was computed through ICC (two-way mixed-effects model, absolute agreement). For both devices, the measurement error was estimated through the MDC, given the three repetitions of maximal grip strength per condition (see section “Validation against an electromechanical testing system”). This value will be useful to discriminate real changes of grip strength when monitoring users over time.
In addition, separately for the two devices, two-way mixed design ANOVA was used to investigate the effect of hand and sex on the average of the maximal force (Jamar) and ΔP (smart ball) measured (“lme” function; 1 within-subject factor: hand (two levels: dominant, non-dominant); 1 between-subject factor: sex (two levels: male, female)).
Game testing
A frequency analysis on the answers to the SUS and satisfaction questionnaire was carried out to evaluate usability and user’s acceptance.
To assess the validity of the game in measuring the maximum grip strength, a correlation analysis was carried out between maximal grip force acquired using the Jamar dynamometer and the maximal ΔP registered during game execution. Given the data normal distribution (Lilliefors test), the Pearson correlation coefficient was used.
Relative reliability of the three ΔP measures registered during game execution was computed through ICC (two-way mixed-effects model, absolute agreement). Statistics was run using RStudio version 1.0.143 (RStudio Inc., Boston, MA). Significance level was set at 5 percent for all tests.
Results
Validation of the smart ball
Validation against the electromechanical testing system
For each of the four tested levels of initial pressure (P0), the pressure variation values (ΔP) measured by the smart ball at different force levels are reported in Figure 4. The slope of the regression lines increases as the ball deformability increases (i.e. as P0 decreases). Independently from the P0 tested, test–retest reliability of the ΔP measured by the smart ball was excellent (ICC > 0.99) (Table 1). Consequently, in terms of absolute reliability, the estimated SEM increased with decreasing initial pressure, ranging from 0.72 hPa for the ball inflated at 1.4 bar to 1.41 hPa for the ball inflated at 1.0 bar. Thus, the MDC ranged from 1.71 to 3.91 hPa, with lower values obtained when the smart ball was inflated at the highest initial pressures.
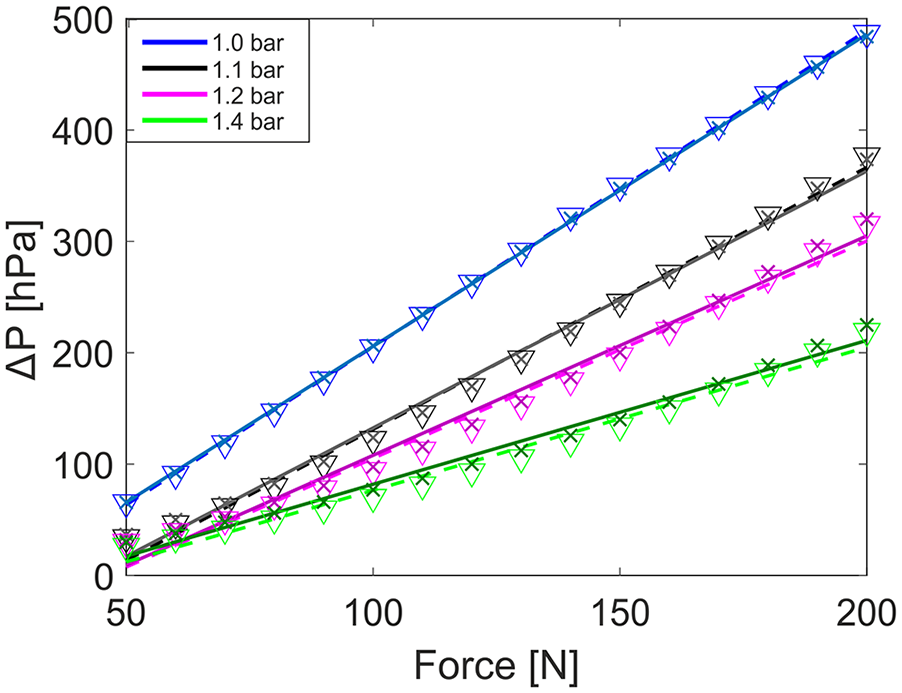
Experimental data obtained for the four P0 tested. For each P0, the ΔP measured by the ball at each force level is indicated with a triangle and a cross for the first and second trials, respectively. The best-fit regression line is reported with dashed or solid line for the first and second trials, respectively.
Relative reliability (ICC), absolute reliability (SEM), and minimum detectable change (MDC) of the ΔP measured by the smart ball during the validation against the linear actuator (N = 16 for each P0 tested).
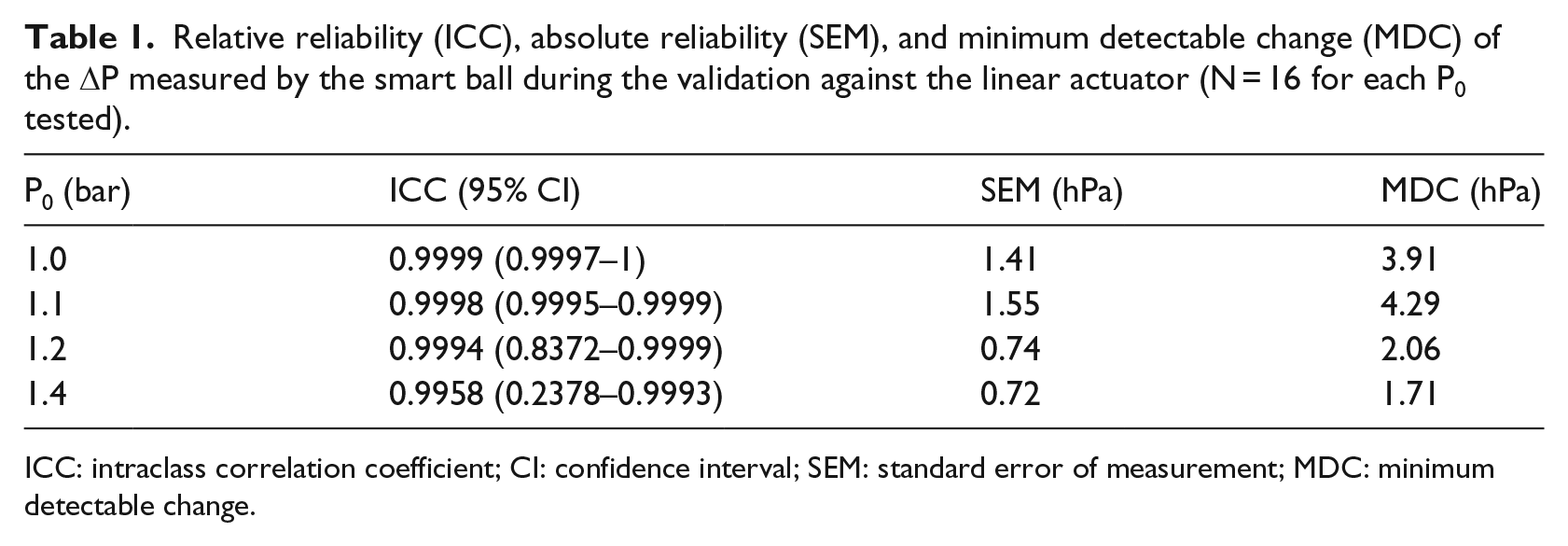
ICC: intraclass correlation coefficient; CI: confidence interval; SEM: standard error of measurement; MDC: minimum detectable change.
During such tests, the ball inflated at 1.0 bar showed high deformability which led to reach great ΔP values even when a low force level was exerted; such feature could easily cause damages to the internal electronics. On the other hand, the ball inflated at 1.4 bar resulted too rigid, thus reducing usability.
Such results and observations were used to support the selection of the most appropriate initial pressure to be used in the next steps of the work, which turned out to be 1.2 bar. Indeed, a P0 of 1.2 bar resulted in low values of SEM (0.74 hPa) and MDC (2.06 hPa).
Validation against the Jamar dynamometer
Figure 5 shows the scatterplots comparing the mean grip strength measured by the smart ball and the Jamar dynamometer for dominant and non-dominant hands. The Pearson correlations (N = 55) between the ΔP measured by the smart ball and the grip strength measured by the Jamar dynamometer were 0.76 (p < 0.01) and 0.80 (p < 0.01) for the dominant and non-dominant hand, respectively. When considering only the older adult subgroup (N = 26), the Pearson correlation coefficient slightly decreased to 0.61 (p < 0.01) and 0.68 (p < 0.01) for the dominant and non-dominant hand, respectively.
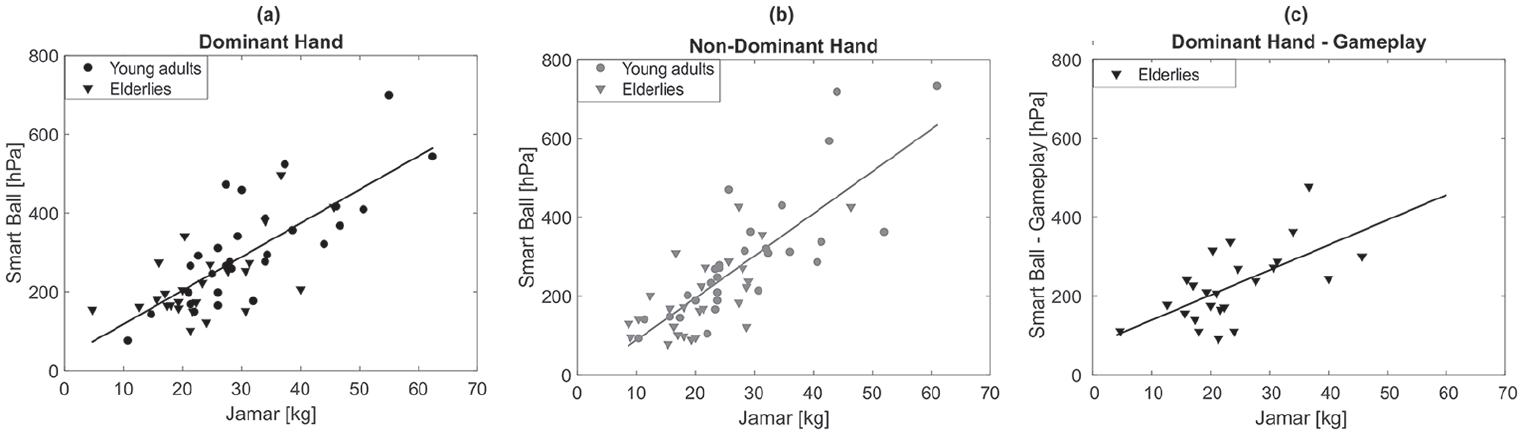
Scatterplots comparing the mean grip strength measured by the smart ball and the Jamar are reported (a) for the dominant hand, (b) for the non-dominant hand, and (c) for the dominant hand during gameplay. Circles and triangles indicate values obtained from the young and older adults, respectively. The best regression line is shown in each panel.
The ICCs obtained for the three consecutive trials of maximum grip strength performed with the two devices and the MDC are reported in Table 2. As expected, for both the smart ball and the Jamar, such values are way higher than the MDC emerged from multiple repetitions of the tests with the linear actuator, which did not include the intra-subject variability that typically characterizes the human system.
Relative reliability (ICC), absolute reliability (SEM), and minimum detectable change (MDC) of the force measured by the Jamar and the ΔP measured by the smart ball for all subjects (N = 55) and for the two subgroups of young (N = 29) and older (N = 26) adults.
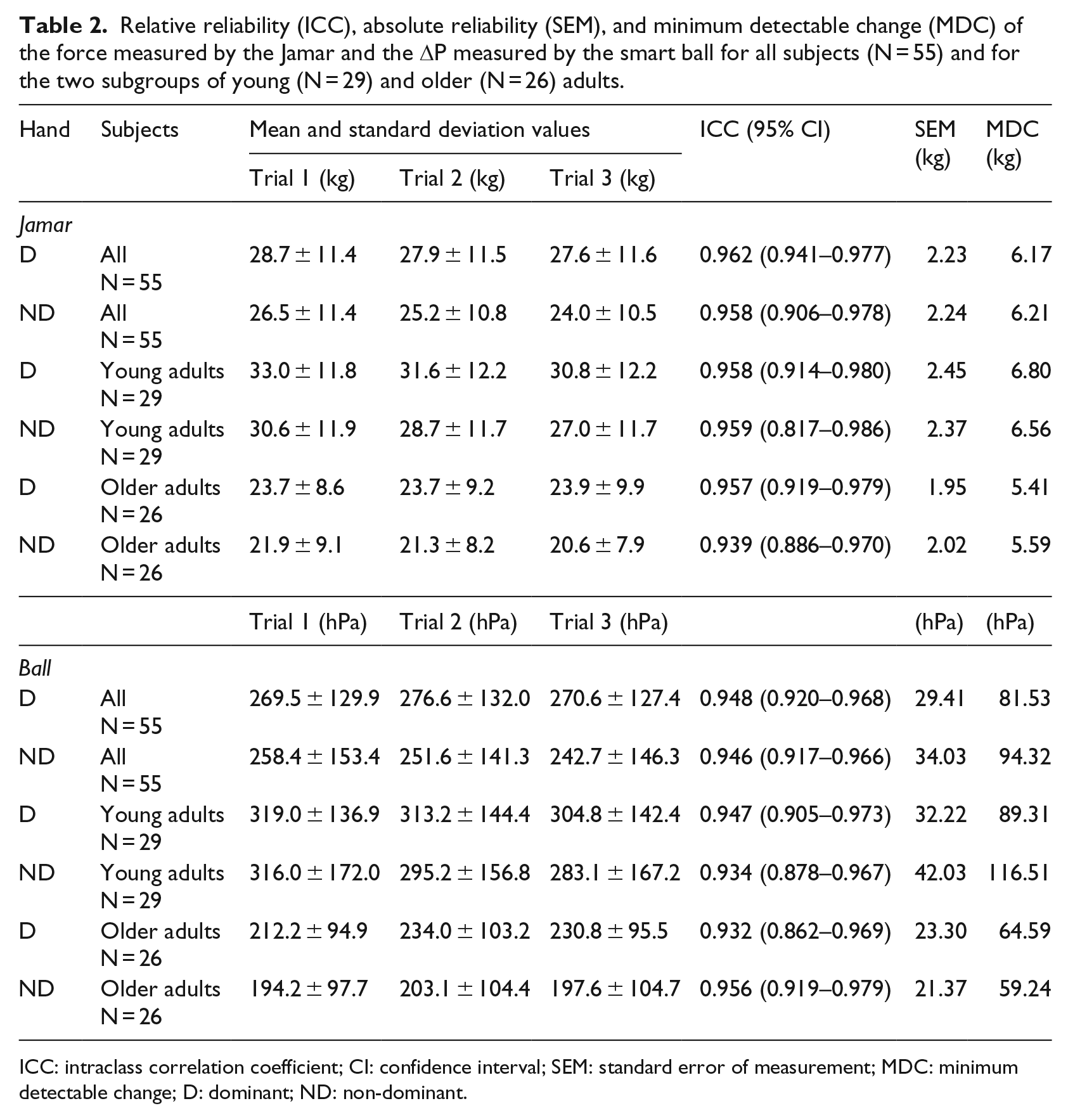
ICC: intraclass correlation coefficient; CI: confidence interval; SEM: standard error of measurement; MDC: minimum detectable change; D: dominant; ND: non-dominant.
Significant differences in maximal grip strength between dominant and non-dominant hands and between men and women were found when using both the Jamar and the smart ball (Table 3). No interaction between hand and sex was found, meaning that both men and women presented a greater maximal handgrip strength for the dominant side.
Two-way mixed design ANOVA results.

ANOVA: analysis of variance; D: dominant; ND: non-dominant; Δ(D, ND): difference between dominant and non-dominant hands; M: male; F: female.
Game testing
The usability and satisfaction questionnaire reported strongly positive results. In terms of usability, the average SUS score obtained was 87.7 (±10.9), with the 92.3 percent of participants presenting a positive usability score (⩾68). Similar results emerged in terms of satisfaction. The majority of users (69.2%) was strongly satisfied with the overall experience, the 26.9 percent was satisfied, while the 3.9 percent only had no opinion. All subjects felt at ease when using the smart ball to control the game (76.9% strongly agree; 23.1% agree). In addition, 61.5 percent of subjects (46.1% strongly agree; 15.4% agree) would like to use the computer game at home, and 96.1 percent of them (69.2% strongly agree; 26.9% agree) appreciated the graphical interface (3.9% no opinion). Concerning the open questions, all subjects reported no perceived discomfort, except one who stated that the instructions of the Wheel of Star scene were not clear. It is important to point out that, during the protocol, the users did not leverage the game tutorial provided for home deployment of the game. According to the questionnaire, the most appreciated aspects were the ease-of-use (three participants), the engagement (three participants), the Wheel of Star scene (three participants), the space theme of the graphic interface (two participants), and the amusement (one participant). On the other hand, no participant pointed out negative aspects. Importantly, from the questionnaire emerged that none of the users ever practiced a similar game before.
The Pearson correlation (N = 26) between the ΔP measured by the smart ball during game execution and the grip strength obtained through the Jamar dynamometer was 0.62 (p < 0.01) (Figure 5(c)). The ICC obtained for the three consecutive trials of maximum grip strength performed during game execution was 0.9046 (95% confidence interval (CI): 0.8230–0.9541).
Discussion
This work proposes an innovative and expedient solution for valid and continuous home-based monitoring of maximal grip strength, with the final aim of detecting early signs of frailty in community-dwelling elderlies. To this end, we devised a serious game controlled by a sensorized soft plastic ball to guide the user through the instructions of a clinical protocol typically used to assess muscle weakness.
The current work falls within the concept of telemonitoring, a new model of preventive care in which people live in their own environment surrounded by intelligent interfaces integrated into everyday objects. 41 Such smart objects have the potential to transparently acquire useful information about the users’ health status. In this framework, we designed and implemented a prototype of a smart ball sensorized with an absolute pressure sensor able to measure grasping pressures and with tri-axial accelerometers and gyroscopes to detect movement.
Key requirements for an instrument designed to measure handgrip strength are test–retest reliability and concurrent validity with respect to the clinical standard. For this reason, maximal grip strength of dominant and non-dominant hands were measured, following the ASHT protocol, on 55 young and older adults using both the smart ball and the Jamar dynamometer. Results showed that test–retest reliability of the pressure measurements was excellent, with ICC values above 0.94 for both hands. Such results were comparable with the ones obtained from the Jamar, showing that the relative reliability of the smart ball approaches the clinical standard. In addition, results revealed very high significant correlations between measurements of the smart ball and the Jamar dynamometer which varied between 0.76 and 0.80 for dominant and non-dominant hand, respectively. These strong correlations support the concurrent validity of measurements obtained with the smart ball with respect to the Jamar dynamometer. Unfortunately, the different physical quantities measured by the two instruments (i.e. pressure for the smart ball and force for the dynamometer) did not allow us to verify agreement between the two instruments (e.g. through Bland–Altman plots). However, the results obtained from the comparison of the smart ball with the clinical standard improve the findings emerged from a previous research that conceived a first device for home-based self-monitoring of grip strength. Such device was tested in 88 older adults, reporting strong correlation (ranging between 0.69 and 0.78) with the Jamar. 30 However, the prototype tested by previous work was able to detect only larger grip strength differences, such as between-sex differences, while it could not distinguish between dominant and non-dominant hands. This result was probably due to the choice of the pressure sensor, which presented a resolution of 12 hPa. The reported lack of sensitivity could hamper the use of the device in monitoring the small strength changes that characterize the slow but continuous physical degeneration of elderly people. The pressure sensor inserted in our smart ball was instead characterized by a higher resolution (0.24 hPa), which allowed to discriminate the pressure exerted by dominant and non-dominant hands, whose difference is typically in the range of 10–20 hPa.
When it comes to technologies for home care, providing a well-functioning system is not a pledge for success. Indeed, user’s acceptance is one of the main obstacles for the uptake of the solution, especially for elder users. 8 For this reason, to increase usability, the plastic ball was chosen for its soft and handy nature, in order to avoid possible discomfort in weak joints, such as those reported for the use of the Jamar dynamometer. 25 The idea of instrumenting a soft tool to measure handgrip strength with the view to a daily use was first introduced by Vermeulen et al. 30 However, the device tested was not a proper daily-life soft ball, but consisted of a modified Martin Vigorimeter in which the manometer was replaced by the electronics, which was then attached to the bulb via a cumbersome rubber tube. For our device, instead, sensors and electronics are placed inside the ball, thus creating a compact and easy-to-use solution that properly replicates a real antistress ball. The comfort of use of the developed device was confirmed by the positive results of the questionnaire, which showed that all the elder participants felt at ease when using the smart ball.
However, the main innovation introduced by our work in terms of usability is represented by the use of gamification to guide the elder through the proper use of the smart object. Valid home-based self-monitoring of maximal grip strength is hard to obtain without any control on the modality of use, and no previous research ever tackled such nontrivial issue. To face this problem, we successfully devised and developed an innovative smart ball–driven computer game that reproduces the ASHT protocol, allowing to obtain meaningful information about the elder’s maximal grip strength while engaging him or her in a compelling activity. The game was tested on 26 elderlies, reporting successful results. Test–retest reliability and concurrent validity of the smart ball in measuring maximal grip strength during game execution, with respect to the Jamar dynamometer, were comparable with the ones obtained from the stand-alone use of the smart ball during the standard ASHT protocol. The game was implemented following specific guidelines recommended when designing games for elderlies, 35 thus obtaining an engaging yet simple activity, able to guide the user with clear and simple instructions. Moreover, game control was easily achieved by simply squeezing or rotating the ball. System usability and acceptance were confirmed by our results. A positive usability score was reported by the strong majority of users (92.3%). In terms of user’s acceptance, the vast majority of participants showed to be satisfied with the overall experience and would like to use the system at home. No negative aspects were pointed out by the users. Such positive results are even more striking if we consider that none of the users ever practiced any similar activity before.
The encouraging results, emerged in terms of both user’s acceptance and system reliability and validity, are of crucial importance to deploy the implemented system in a home setting, with the final aim of achieving transparent, continuous monitoring of handgrip strength in older adults. With the view to long-term use, a useful result emerged here concerns the MDC computed during user’s performance, to estimate whether a change between the user’s repeated tests represents random variation or a true change in performance. This value is a key requirement to discriminate real changes of grip strength when monitoring users over time, and it is thus crucial for longitudinal monitoring.
The developed serious game is now ready to be deployed at home to test the long-term usability of the system. To this end, useful information will be collected within the MoveCare Project (http://www.movecare-project.eu), 42 which aims at developing a comprehensive system for monitoring, assisting, and promoting activities to counteract decline and social exclusion in independent elderlies. Within this project, the present system will be deployed at home and integrated in a community-based activity center that offers a number of different physical and cognitive activities. Diverse data will be acquired also from a heterogeneous net including environmental sensors and daily-use smart objects based on the new paradigm of the Internet of Things (IoT). 43 The heterogeneous data transparently collected from the user will be fed to an intelligent virtual caregiver, a key entity in the cloud in charge of the reasoning. Obtaining a comprehensive picture of the physical and cognitive status of community-dwelling elderlies from daily activities performed at home is key to detect possible early signs of decline and alert formal and informal caregivers. In this framework, it is crucial to keep in mind that MoveCare-like systems should not and cannot replace human care providers or clinicians, but they should rather provide possible recommendations of seeking further professional help, thus representing cost-effective solutions.
Conclusion
In the current work, we devised a nifty system composed of a smart soft plastic ball to control a serious game specifically designed to measure age-related muscle weakness while engaging elder users in a compelling activity.
This study presents a step forward in the context of home telemonitoring for prevention of age-related frailty, since we leverage smart objects and gamification to increase system reliability and acceptance, with the final aim of providing remote support to elder people in the detection of early alert situations. The innovative solution presented here paves the way toward the adoption of usable and well-accepted technology transparently integrated in daily-use objects, having the potential to make important contribution to research and practice in the field of preventive care.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Ethical approval
The Ethical Committee of the Politecnico di Milano approved the study protocol (n. 05/2018).
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the European H2020 project MoveCare: grant number (ICT-26-2016b—GA 732158).