
Abstract
Serious games are increasingly being applied within healthcare, but their integration in psychotherapeutic settings is less documented. Objectives: The present study sought to identify the attitudes of psychotherapists and patients towards the hypothetical use of serious games in psychotherapy in the South African context. Methods: Online surveys assessed acceptance, experience, and requirements for the utilisation of serious games in therapeutic contexts. Clients utilising mental health services (n = 209) and psychotherapists delivering mental health services (n = 156) in South Africa completed the online survey. Results: Knowledge about serious games is limited with only 15% of clients and 16% of therapists reporting knowledge of the existence and application of serious games. Use of serious games is even more infrequent with only 1% of therapists and 6% of clients currently using serious games as an intervention. Despite this, our findings highlight an apparent demand for their use, with 71% of therapists indicating that serious games would be a suitable adjunct treatment modality for their patients. Our results show a general openness toward the use of serious games in psychotherapy. Conclusion: The use of serious games as an e-mental health treatment modality is conceivable for both patients and therapists, particularly as a complementary strategy to traditional face-to-face psychotherapy.
Background
Advances in technology have changed how psychotherapists interact with their patients. Globally, the importance of incorporating technology in psychotherapy has been widely debated, with emphasis placed on meeting patients where they are and preserving the therapeutic relationship at the same time. 1 In recent years, video or computer games have since become a common source of entertainment which youth and adults alike enjoy playing.2,3 The online gaming market in South Africa is showing high growth and currently, South Africa boasts the second-largest ‘gaming market’ on the African continent. Recent evidence showed that there were more than 11 million gamers in South Africa.4,5 Video games may be used as supportive tools in psychotherapy for assessments, building rapport and skills training. 6 Gamification and serious games are two popular approaches that offer similar benefits but there are notable differences between these approaches. Many scholars from diverse fields such as psychology, cultural studies, computer science, sociology and pedagogy have become interested in serious games, although inconsistencies and shortcomings of definitions exist. 7 Serious games are games that have been designed for a primary purpose other than pure entertainment and are used in various areas such as education, healthcare, marketing and other businesses and industries.
Serious games are interactive computer games that train cognitive or behavioural skills in a digital learning environment. Game designers Michael and Chen (2006) define serious games as follows: “A serious game is a game in which education (in its various forms) is the primary goal, rather than entertainment.” 8 Gamification, on the other hand, is the application of typical game design elements in a non-game context such as marketing or training in order to increase engagement and effectiveness. 9 Unlike a game, gamification is not a self-contained unit, with a clear beginning, middle and end. In order to increase engagement, motivation, learning, and problem solving, gamification uses game-based elements and strategies. 9 Serious games follow a typical game structure, but also have some form of educational value and are not simply for entertainment.
Serious games used as treatment interventions differ from electronic games for entertainment as these games are designed for specific health conditions and specific target groups. Game-based interventions, such as serious games, have been developed and used in the management of various health conditions, including mental health problems, 10 for learning and instructional purposes,11,12 and designed to motivate and encourage players to engage in meaningful play. 13 Serious games use video game designs to create fun games with three-dimensional images, while also incorporating evidence based psychological theories to ensure that learning takes place. 14
Research concerning the relatively new application of serious games within a psychotherapeutic context is expanding.15–18 In the context of mental health, serious games have been applied to address various mental health conditions such as attention deficit hyperactivity disorder (ADHD), post-traumatic stress disorder, depression, cognitive function, alcohol use disorder and autism spectrum disorders (ASD), with meta-analytic findings showing a significant effect on improvement of symptoms.19,20 Significant improvement in sustained attention, as well as in cognitive function in patients with depression have been reported. 21 Serious games such as Smart, Positive, Active, Realistic, X-Factor thoughts (SPARX), one of the best evaluated computerised self-help interventions for adolescents seeking help for depression, has been proven to reduce symptoms in help seeking adolescents between the ages of 12 and 19 years old. 22 Patients that used the serious game SPARX acquired skills to deal with negative thought patterns, solve problems, and practice relaxation techniques. 22 Another study showed that using SPARX was comparable to Cognitive Behavioural Therapy (CBT) techniques, with the potential to become a self-help resource, easily accessible to patients in the comfort of their homes.22,23 This computerised CBT game was developed based on the principles of CBT. It is short-term goal oriented, and aims to teach problem solving skills, as well as how to apply these learned skills to real life challenges. The CBT components are incorporated in the game, beginning with rapport building between the guide and the user, and ending with relapse prevention skills. The guide in the game plays the role of a therapist by reflecting on skills learned once each module is completed. This reflection process strengthens rapport with the user; however, the guide does not replace the therapist and the structure of the game allows for face-to-face interactions between the therapist and the user.
Serious games are gradually gaining popularity in psychotherapeutic settings. Many psychotherapists and researchers around the world have argued that serious games can be effectively applied as interventions and facilitate rapport building between therapists and patients. 24 Cocks 25 explored serious games’ narratives and how they create interactive relationships between psychotherapist and patient, arguing that serious games could provide important health information necessary for behaviour change. Moreover, Cocks 25 urged the importance of collaborative work between game designers and researchers to align psychological approaches with evidence-based designs.
There is emerging evidence concerning the effectiveness of serious games for mental health problems. 26 Zayeni et al. recently conducted a systematic review on the effectiveness of serious games and commercial video games in the treatment or prevention of psychiatric disorders in young patients. 20 Twenty-two studies that targeted various child and adolescents psychiatric conditions such as anxiety, autism spectrum disorder, ADHD, developmental coordination disorder and dyslexia were included in the review. The results showed the effectiveness of serious games and commercial video games in the context of child and adolescent psychiatry. 20 Although there is some evidence for the effectiveness of serious games, there remains a paucity of research on the sustained effectiveness of serious games over time. Longitudinal studies are needed.
A systematic review and meta-analysis of randomized controlled trials that evaluated the accessibility, feasibility and effectiveness of serious games for psychiatric disorders by Lau et al. 19 found that serious games were effective in reducing mental health symptoms. A total of 19 studies met inclusion criteria and the serious games included were developed for individuals aged 7 to 80 years old with depression,22,23 post-traumatic stress disorder, 27 ASD, 28 ADHD, age related decline in cognitive performances 29 and alcohol use disorders. 30 The results showed a moderate reduction in symptoms of the aforementioned disorders and conditions, following the use of serious games compared to control groups without game interventions. Similarly, a systematic review on serious games developed for psychotherapy by Eichenberg and Schott 31 found that serious games were effective, whether used as an adjunct therapeutic tool together with conventional therapy or as an intervention, and were appealing to patients regardless of age and gender.
Although there is an increasing evidence base for the effectiveness of game-based interventions for mental health problems, there may be challenges linked to their use and the collection of data. Some of these challenges, as highlighted by Birk et al, 32 include the influence of patient distractibility and the need for privacy while playing these games. Moreover, how data are handled, accessed, and used during game play may pose ethical concerns, particularly when using video games to assess cognitive performance. Further, psychotherapists may have to deal with additional factors such as the cost of games, 33 training to use these games, practice guidelines, and standards and policies. 34
Eichenberg and colleagues 35 have discussed the current research gap surrounding the acceptance and readiness of serious games as an e-mental health intervention. Their research sought to understand the acceptance of serious games in psychotherapy. The study involved an online survey targeting 234 German-speaking psychotherapists and 260 individuals with experience in psychotherapy. The results demonstrated limited knowledge regarding serious games and limited openness of psychotherapists and patients toward the use of serious games within the therapeutic context.
Although there is increasing evidence for the effectiveness of game-based interventions for mental health problems, the application of these games is rare, particularly in non-Western countries. Building on the work by Eichenberg et al, 35 the present study sought to identify the views and knowledge of psychotherapists and patients towards serious games in psychotherapy in the South African context. South Africa is commonly known as the ‘Rainbow Nation’, a title that captures its diversity and 11 official languages. To our knowledge, this is the first study of its kind to assess acceptance and readiness of serious games in psychotherapy in South Africa. This study has relevance considering that identification of preconditions, opinions, expectations, and general readiness of all stakeholders is essential for the successful development and implementation of serious games for therapeutic purposes.
Methods
Procedure
The present study received ethical clearance. Data were collected from January through June 2020, using an online survey on Survey Monkey. Ethical principles were strictly upheld throughout the research process and all participants were allowed to make an informed decision on whether they wanted to participate in the study or not. The details of the study were explained to participants in the email invitation and again, in more detail on the landing page of the survey. Participants were required to provide informed consent prior to commencing with the survey. All data were kept anonymous and confidential and participants could terminate the survey at any point. The study targeted two groups independently, namely South African psychotherapists and South African patients (referred to as clients from here on) with experience in psychotherapy. These target groups were chosen as a basic understanding of psychotherapy and its course is vital in order to assess if and to what extent serious games use can be envisaged within the context of mental health treatment. No other exclusion criteria were applied. Therapists were contacted via various therapy associations based in South Africa. Therapists self-reported their occupation as Psychologists, Social Workers, Counsellors, Psychotherapists and Psychiatrists using the following psychotherapeutic modalities primarily, although many listed a different school/model: CBT, Humanistic/Existential Therapy, Psychoanalytic/Psychodynamic Therapy, and Systemic Therapy. Clients were recruited through various social media platforms and therapy associations in South Africa. Therapy associations and other organisations targeted to recruit clinicians and clients included: University staff and students, South African Society of Psychiatrists (SASOP), South African Depression and Anxiety Group (SADAG), The South African College of Applied Psychology (SACAP), and Medpages. In total, 209 clients with experience in psychotherapy and 156 therapists completed the online survey.
Materials
The original survey was designed and administered by Eichenberg and colleagues. 35 The South African surveys were administered online using Survey Monkey in English. In order to provide participants with an introduction into the functions and possibilities of serious games in healthcare settings, two serious games for therapeutic use were presented, namely: SPARX: https://research.sparx.org.nz and SCOTT–Social Cognition Training Tool: https://www.scott-training.de/. A brief overview of these two games was provided to clients and clinicians on the landing page of each respective survey at the same time, prior to the commencement of questions. The brief overview included a description of the game (text) and two figures (images) for each game. We did not assess differences based on each presented game, this introduction was merely intended to provide a brief overview and participants were provided with the website for each game for more information. The surveys included various questions relating to attitudes towards serious games in psychotherapy. Five questions related to the specific applicability of serious games in a South African context were added. Survey respondents were asked about: (1) their use of electronic devices, (2) their experience with playing computer and video games, (3) whether they had prior experience with a similar game, and (4) under what circumstances they could imagine utilising serious games. Further questions addressed: (5) the desired access (e.g., online or offline), (6) who should have access to game data, and (7) how much time they would invest in playing on a weekly basis. Therapists were asked: (8) which psychological disorders serious games could best be used to treat, (9) at which point in the treatment process serious games would be useful, and (10) which criteria would be essential to consider in the use of serious games as a psychotherapeutic treatment modality. Both groups’ attitudes were recorded using items in which respondents rated statements on a five-point scale, although not all questions had the same response format. Answers were rated 1-5 (see Supplementary Data for surveys).
Data analysis
Analyses were performed using Statistica version 13 and SPSS Statistics version 26. Descriptive statistics were computed to describe each sample. Group comparisons were computed using parametric and non-parametric models. Inferential statistics such as Correlations, Chi-Square Tests of Association, and Mann-Whitney U tests were performed, using a significance level of 0.05. Open questions were analysed by using frequency analysis. 36
Results
Characteristics of the client sample
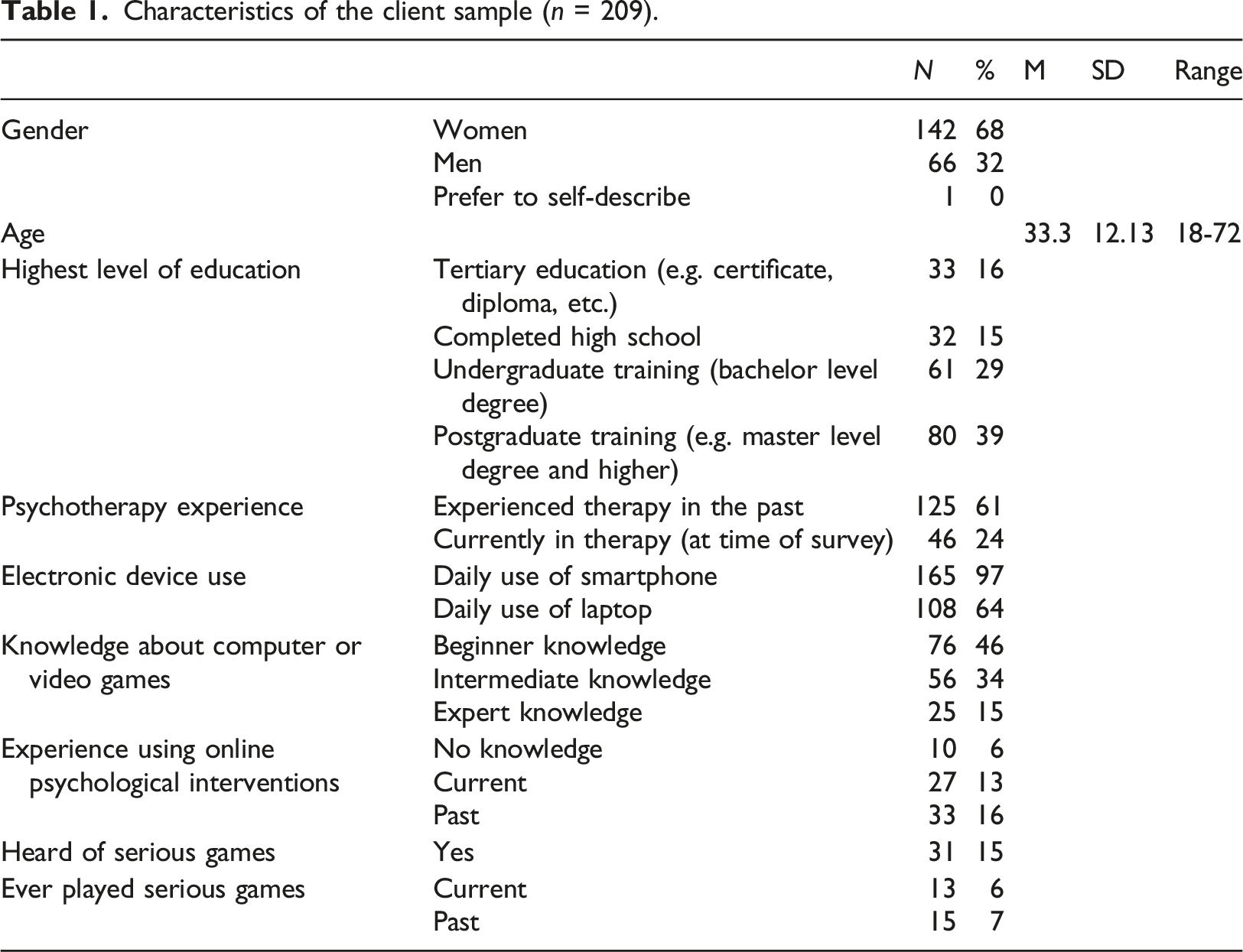
Characteristics of the client sample (n = 209).
Characteristics of the therapist sample
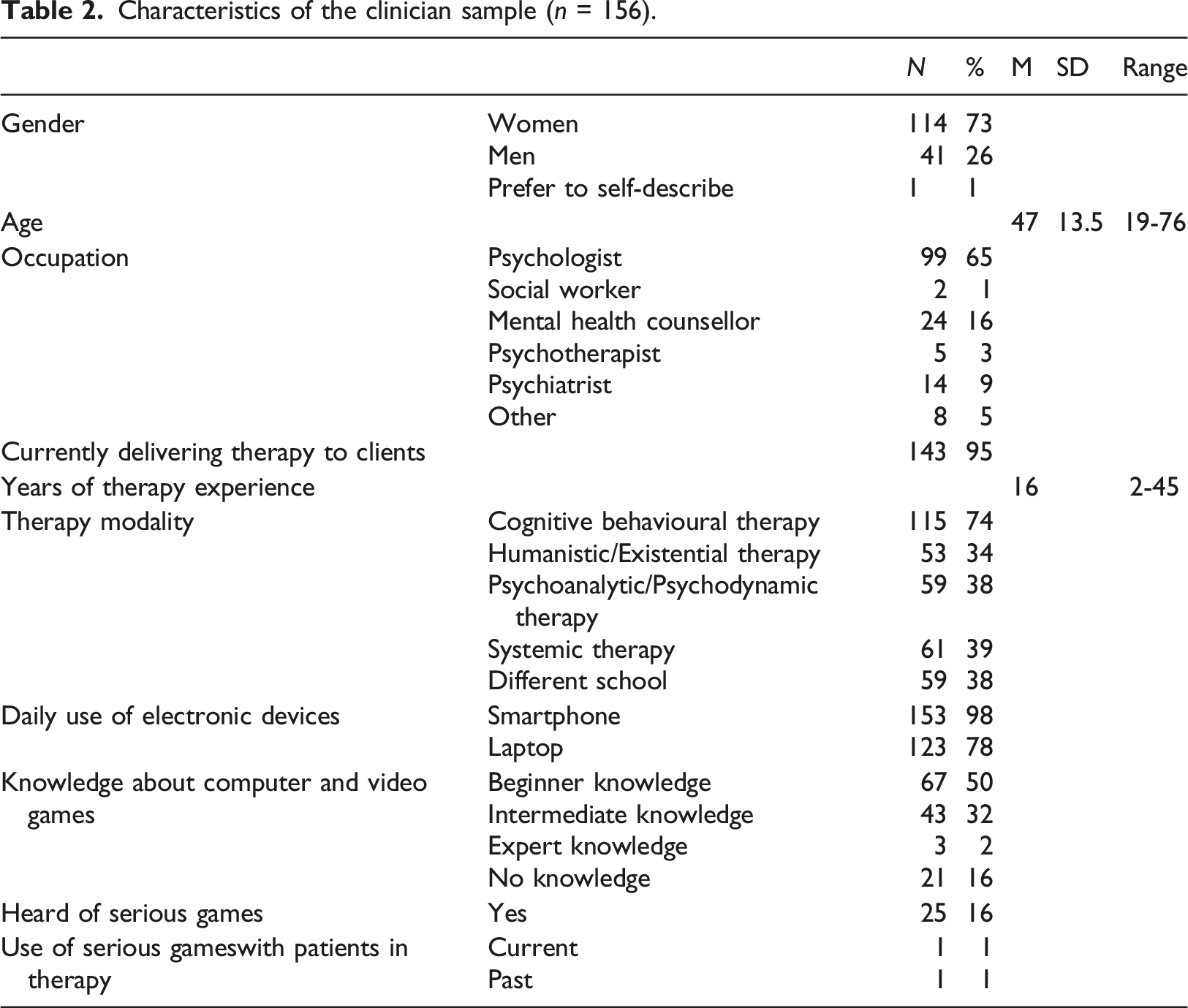
Characteristics of the clinician sample (n = 156).
Client perspectives of serious games
The majority of clients (81%) reported that they could imagine themselves using serious games, mostly at home (73%), with some (30%) indicating they would make use of these games on the go (e.g. while travelling on a bus, train, etc.). Clients who self-rated their level of expertise with computer and video games as higher had a higher likelihood of considering using a serious game within psychotherapy (U = 0.02, p = .04; 95% CI 1.49, 1.78). The vast majority of clients (84%) reported that they would be willing to spend between 1 and 3 hours a week playing a serious game, 10% would play a serious game up to 5 hours a week, and 6% would play a serious game more than 51 hours a week. The majority of clients (44%) indicated that they would use serious games as an adjunct to psychological therapy/consultation, 41% indicated they would use it as a prevention method, 21% before therapy/consultation begins, 38% as support after therapy, and 13% instead of psychological therapy. When asked what essential characteristics serious games would need to have for clients to consider using them, easy access and applicability was regarded as the most important criterion (95%), followed by evidence of efficacy (88%), endorsement by therapeutic associations or expert guidelines (87%), and the entertainment value of the game (83%). When asked to explain why they could not imagine themselves using serious games, only a small fraction of clients answered these questions. In total, 9% reported not knowing enough to picture themselves using them, 4% said they did not like the idea of computers helping people with psychological problems, 4% indicated that they did not know if serious games work or if they are effective, 2% felt that a serious game could not help them and 1% indicated they would not trust a serious game. The majority of clients (80%) reported that they would be prepared to independently purchase and/or use a proven serious game for a purpose other than psychological therapy (e.g. to learn a language or another skill). Clients who do not currently play computer or video games significantly differed 95% CI [2.43, 2,97] from clients who do on expected long-term effects from serious games (U = 0.01, p = .01; 95% CI [2.05, 2.47]). In comparison to clients who do not currently play computer or video games, those who do currently play tended to disagree with the statement that they do not expect long-term benefits from serious games.
Therapist perspectives of serious games
The vast majority (88%) of therapists indicated that they could imagine using serious games with their patients. Systemic therapists showed the greatest support for the use of serious games as a psychotherapeutic tool (95%), closely followed by therapists from other/different schools (93%) and the behavioural and humanistic-existential therapists, who showed equal support for the use of serious games (90%). Therapists with a psychoanalytic orientation could envisage the use of serious games to a lesser extent (85%). Unlike clients, clinician self-rated level of expertise with computer and video games was not associated with the likelihood of using a serious game within psychotherapy. Clinicians who self-rated their level of expertise with computer and video games as higher did not report a higher likelihood of considering using a serious game within psychotherapy (U = 0.93, p = .99; 95% CI 1.07, 1.38). When asked what essential characteristics serious games would need to have to consider using them with their patients, easy access and applicability was regarded as the most important criterion (99%), followed by evidence of efficacy (96%), endorsement by therapeutic associations (87%), and their use as a means to track clients’ progress (84%). The majority of therapists (71%) indicated that they would use serious games as an adjunct to psychological therapy/consultation, 35% indicated they would use it as a prevention method, 34% at a client’s request, 24% before therapy/consultation begins, 51% as support after therapy, and 4% instead of psychological therapy. When asked to explain why they could not imagine themselves using serious games with their patients, only a small fraction of therapists answered these questions. A total of 8% reported not knowing enough to picture themselves using them, 6% felt the games do not fit to their therapeutic modality or practice, 3% felt there has not been enough scientific evidence to support the use of serious games, 3% did not like the idea of computers helping people with psychological problems, 2% did not like the idea of games being used for serious psychological problems, 1% felt their clients would not trust a serious game, and 1% felt their clients’ needs are too complex to use a serious game.
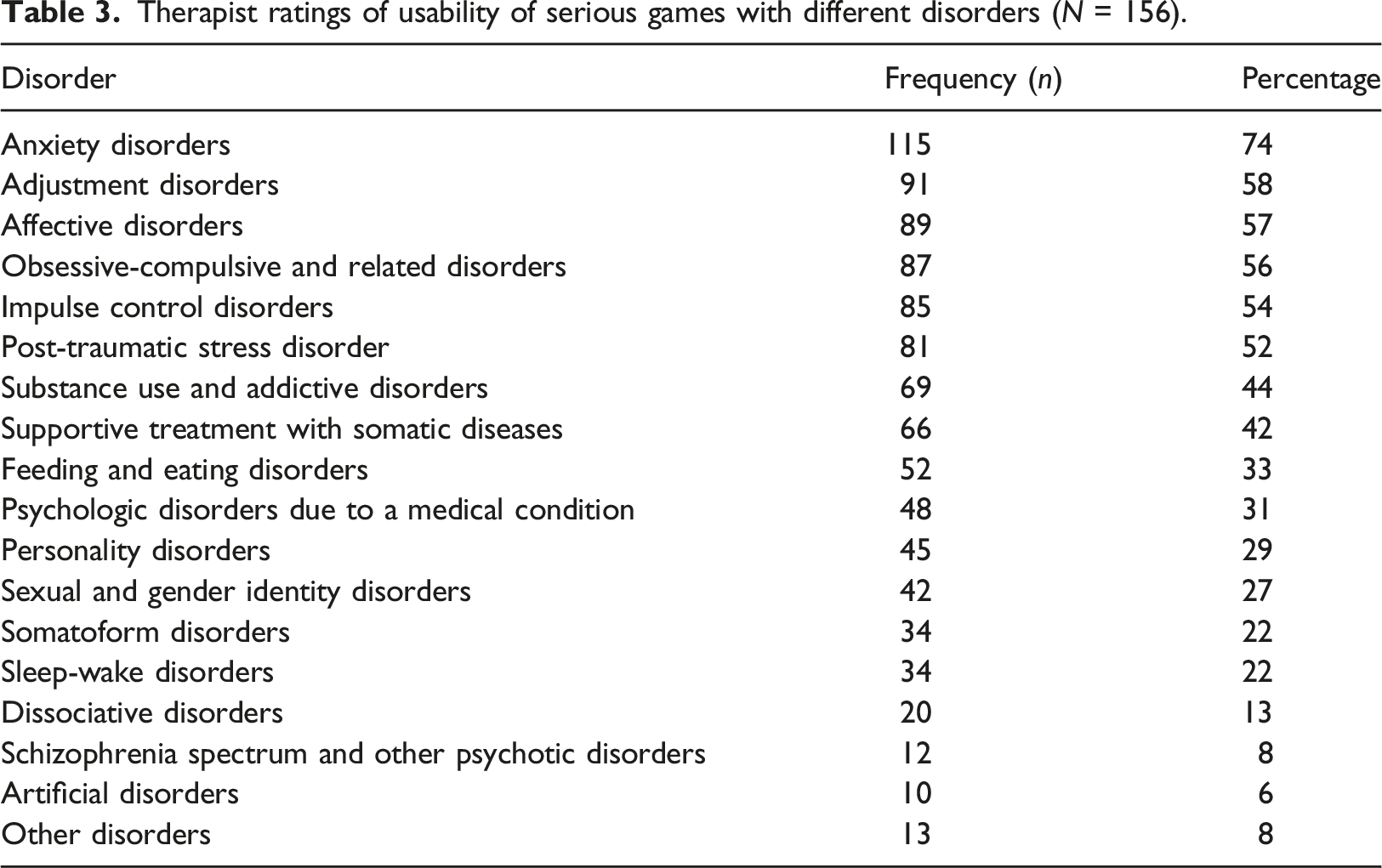
Therapist ratings of usability of serious games with different disorders (N = 156).
Clinicians who do not currently play computer or video games significantly differed (95% CI 2,45, 2,89) in their view on whether serious games provide clients with professional support compared to clinicians who do currently play (U = 0.03, p = .03; 95% CI 2,80, 3,32). In comparison to clinicians who do not currently play computer or video games, those who do currently play were more ambivalent and tended to neither agree nor disagree with the statement that serious games do not provide clients with professional support. Moreover, clinicians who do not currently play computer or video games significantly differed (95% CI 3,31, 3,76) in their view on whether the guidance of clients is more individual in psychotherapy than in serious games (U = 0.02, p = .03). In comparison to clinicians who do not currently play computer or video games, those who do currently play tended to agree more with the statement that the guidance of clients is more individual in psychotherapy than in serious games (95% CI 3,67, 4,21).
Comparative results of clients and therapists
For clients, expertise with computer and video games correlated positively with self-rated likelihood of using serious games within psychotherapy (r = 0.178, p = 0.026). For therapists, results did not reveal any correlation between the experience level with computer and video games and the likelihood to consider using serious games in psychotherapy (r = −0.002, p = 0.982).
The majority of participants in both groups could imagine using a serious game before commencement of therapy. Therapists and clients similarly reported using serious games as a prevention method. The biggest relative differences existed in the application of serious games as an adjunct to therapy (Χ2 (1) = 26.79, p < .01) and as assistance after completion of therapy (Χ2 (1) = 6.61, p = .01). See Figure 1. Application areas of serious games.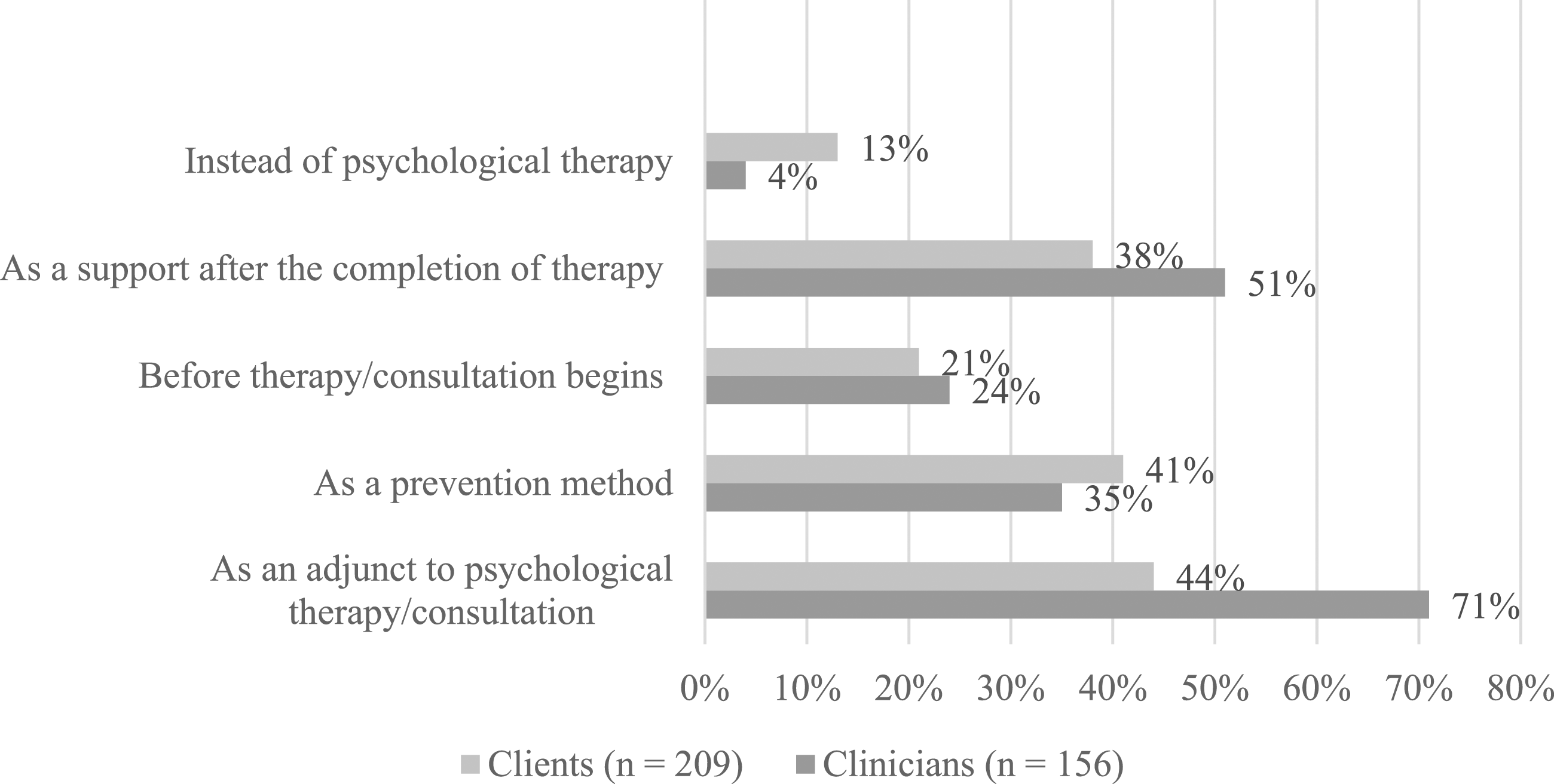
Serious games in South Africa
Although the vast majority of clients indicated that South Africa is a country where many individuals may not have access to a computer, they felt that serious games is a practical intervention for the majority of the population (69%). Therapist responses for the latter were similar (73%). Clients and therapists similarly (81%) indicated that serious games may be limited with regard to the type of audience they could reach in the South African context. When asked if it would be relatively simple to teach someone how to use serious games if they had never used a computer before, the majority of clients (32%) were undecided (neither agreed nor disagreed). For therapists, 36% neither agreed nor disagreed. The vast majority of therapists (92%) and clients (89%) indicated that South Africa is a country with widely diverse, multicultural communities and that it is necessary for serious games to take the many cultures that are present in the South African population into consideration. 80% of therapists and 75% of clients agreed that South Africans could benefit from serious games more if they were tailored to be more culturally specific and applicable.
Positive and negative perceived aspects about serious games use in South Africa
Patients
Positive aspects associated with serious games utility were expressed by 78% of all patient survey respondents. In total, 139 answers were given by patients who mostly advocated the opportunity of using serious games as an adjunct to face-to-face therapy (N = 26). This was followed by perceived advantages of the online setting by reaching specific age or patient groups (N = 22), the possibility to train, learn, and improve new skills (N = 20), and the entertainment value (N = 7). Disadvantageous aspects were mentioned by 75% patients, which resulted in a total of 121 given answers. Lacking access to digital devices or internet (N = 23), the consequence of isolating behaviour (N = 14), and risk of addiction (N = 14) were negatively stated by patients. Furthermore, the sample of patients also addressed concerns regarding the suitability of serious games use for the therapeutic setting (N = 15), especially for severe disorders (such as Schizophrenia spectrum and other psychotic disorders) or in case of crisis management. Interestingly, data privacy concerns were not articulated at all.
Psychotherapists
About 91% of psychotherapists gave 137 answers to the questions regarding positive aspects resulting from serious games application. As for the patients, additional serious games support before, during, or after psychotherapy (N = 22) was the most cited benefit. The reach of certain patient or age groups, such as patients at young age or who have difficulties to open up in traditional therapy settings (N = 20), the entertainment factor (N = 18), additional skills development (N = 11), increased feelings of self-accomplishment and self-control for patients (N = 10), were also frequently stated as favourable aspects. Negative aspects were mentioned by 93% of therapists, which resulted in a total of 111 given responses. Again, lacking access and digital competencies was the most addressed negative aspect (N = 16), followed by fear of addiction and other adverse effects (N = 15), incorrect handling of serious games if used unguided (N = 13), risk of isolation and absence of personal contacts for patients (N = 9), and potential replacement of therapy by patients (N = 8).
Discussion
This study sought to expand the knowledge base of e-mental health research, with a focus on knowledge and experience of serious games in two important stakeholder groups, namely patients and therapists. Moreover, we sought to address the readiness to utilise serious games as a treatment modality in these stakeholders.
Our results show a general openness toward the use of serious games in psychotherapy, although therapists were more reluctant to consider the application of serious games for more severe disorders (such as Schizophrenia spectrum and other psychotic disorders). Therapists in particular felt that the application of serious games contradicts the key personal characteristics of psychotherapy, such as face-to-face consultation and rapport building.
Studies have shown that the learning behaviour achieved from serious games may be influenced by a number of factors including individual factors such as attitudes toward gaming ability. 38 In a large e-mental health survey, readiness to engage with e-mental health was significantly higher in persons who were already using relevant technological devices. 39
In our study, clients who self-rated their own level of expertise with computer and video games as higher were more likely to consider using a serious game, compared with patients with lower levels of self-rated expertise. Our study suggests that increased engagement and experience with computer and video games leads to more readiness to use serious games and this may facilitate therapists in identifying suitable patient groups for the application of serious games as a treatment modality.
Therapeutic approach is an additional factor that appears to affect the readiness and potential uptake of serious games, with the most support from systemic, behavioural and humanistic-existential therapists. Therapists with a psychoanalytic orientation could envisage the use of serious games to a lesser extent, mirrored by previous research findings showing a more negative stance toward the use of electronic media among psychodynamic therapists.35,40 Serious games tend to employ cognitive behavioural techniques,31,38 possibly explaining the more positive stance among clinicians engaged in therapy utilising cognitive models. 41
Previous research highlights the disparity between a lack of knowledge surrounding e-mental health and widespread integration. 39 Our study shows that the current knowledge about serious games is limited with only 15% of clients and 16% of therapists reporting knowledge of the existence and application of serious games. Use of serious games is even more infrequent with only 1% of therapists and 6% of clients currently using serious games as an intervention. Unfamiliarity with digital tools affects the use of technology as a therapeutic tool.
Currently there are no clear ethical guidelines or training of therapists on how to use technology such as serious games in therapeutic spaces. Most therapists are only trained to offer face-to-face traditional therapy, and are unfamiliar with technology, despite its drastic growth and expanding application in psychotherapeutic contexts. It is understood that both therapists and clients may not have enough experience on how to use technology in the therapeutic space. This therefore affects how technology is perceived and used within the context of therapy. Although knowledge and use of serious games is still limited, our findings highlight an apparent demand for their use, with 71% of therapists indicating that serious games would be a suitable adjunct treatment modality for their patients and 51% of therapists indicating that serious games would provide support for their patients after completion of treatment.
Clinicians’ attitudes towards the use of serious games after and/or as an adjunct to psychological therapy may be influenced by unfamiliarity with technology and concerns over technology replacing the therapeutic relationship. However, serious games may be useful educational tools used during and after psychological therapy to reinforce skills learned with the therapist. Our study findings highlight various perceived benefits and concerns, notably easy access and applicability of serious games as a key consideration and benefit for both clients and therapists, and neglect of relationship and communication components of therapy possibly resulting from distraction from and/or substitution of therapy with serious games as a concern. However, studies suggest that guided internet treatments can be as effective as face-to-face treatments, with key relationship and communication components successfully integrated into non-game-based e-mental health treatment modalities. 42
Our findings closely align to the findings of the study carried out by Eichenberg and colleagues in Germany. The results of this study similarly demonstrated limited current knowledge regarding serious games but a general openness toward the concept was observed in both patients and therapists. 35 To identify potential cultural differences in the readiness to utilise serious games within e-mental health, our study builds on previous work by Eichenberg and colleagues, 35 through additional inquiry into the use of serious games in the South African context. In South Africa, a minority of the population have multiple access routes to digital literacy in their sociocultural environments. A less privileged majority still come from under-resourced sociocultural backgrounds where digital technology is rare, and access unevenly distributed. 43 Marginally, over one-tenth (10.4%) of South African households have access to the internet at home. 44 Moreover, nearly three quarters of mental health sufferers in South Africa are not accessing any form of mental health care at all and 85% of these patients are dependent on public health-sector services. 45 Not surprisingly, when asked about their perceptions of the integration of serious games as a treatment modality in South Africa, clients and therapists alike indicated that serious games may be limited with regard to the type of audience they can reach in the South African context. The vast majority of therapists and clients indicated that South Africa is culturally and linguistically diverse and that it is necessary for serious games to take the many cultures that are present in the South African population into consideration. Nevertheless, the majority in both stakeholder groups agreed that South Africans could benefit from serious games more if they were tailored to be more culturally specific.
Future considerations should include the integration of e-mental health interventions into psychotherapy training as well as the provision of professional development opportunities for qualified clinicians. 34 Moreover, increased collaboration between game developers and game users should be encouraged when evaluating and developing serious games for psychotherapy. Finally, future considerations should include whether serious game designs need to be adapted for the user. Our findings demonstrate that therapists’ readiness to integrate serious games may be influenced by the therapeutic approach. In light of this, future studies should conduct in-depth analyses focusing on the difference in opinion between therapeutic approaches in order to provide a clearer understanding of this influence.
Limitations
A limitation of this study is that data were collected using an online survey. Given the online survey methodology employed in the present study, this may have resulted in a sample bias, as well as response and non-response bias. Therefore, caution should be taken in generalising these findings. Nevertheless, this is the first study in South Africa to assess attitudes toward the integration of serious games in psychotherapeutic practice for the treatment of mental health disorders. Our findings are in line with a similar study conducted in Europe. 35
Conclusion
The present study evaluates a novel treatment modality in e-mental health and the findings underscore the importance of considering the integration of serious games in psychotherapy, tailored to be culturally specific and contextually relevant.
Footnotes
Acknowledgements
Professor Martin Kidd from the department of Statistics and Actuarial Sciences of Stellenbosch University provided statistical assistance.
Author contributions
CE, SS, JH, GS contributed to the study conception and design. Data collection and analysis were performed by GS. The manuscript was written by GS and OM and all authors commented on previous versions of the manuscript. All authors read and approved the final manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This work is supported by the South African PTSD Research Programme of Excellence and the South African Medical Research Council/Stellenbosch University Genomics of Brain Disorders Research Unit.