
Abstract
Technological advances toward consumer-specific expectations require a sustained commitment and coordination across policy- and decision-makers. The present scenario-based study aimed at identifying prevailing perceptions regarding telehealth applications among Austrian healthcare experts. During a two-round online Delphi survey, panelists rated perceived benefits, obstacles, innovativeness, desirability, and estimated implementation date of 10 telehealth scenarios. Panelists (n = 73, 74% males) perceived that the implementation of telehealth scenarios could especially improve patients’ knowledge, quality of social healthcare, and living standard. In contrast, the three top-ranked obstacles were costs, technical prerequisites, and data security. Survey participants rated innovativeness of the presented future scenarios as quite high, whereas perceived desirability was moderate. Overall, ratings suggested precautious attitudes toward technological innovations. The survey findings suggest building taskforces and enhancing communication between healthcare stakeholders to proactively shape the future of telehealth in Austria.
Introduction
Given latest demographic changes and steadily increasing expenditures for high-quality healthcare, telehealth is crucial to tackle bottlenecks in healthcare provision. 1 Although the current life expectancy trends are favorable, two societal factors are colliding in aging societies worldwide. First, due to the baby boom aging wave, the prevalence of chronic health conditions presupposing long-term medical care increases significantly. Second, aging baby boomers among health personnel imply an upcoming shortage of physicians and nursing staff. 2 For the United States, Sargen and co-workers 3 anticipated an imbalance of about 20 percent between demand and domestic allocation of medical workforce in 2025. These future societal trends are prognosticated to cause logistics and supply chain problems, especially in rural communities. 4
The vision of bridging spatial distances between doctors and patients via telephone, Internet, and video to address the increasingly aging population and age-related disabilities and diseases has already been accomplished decades ago. 5 As a far-reaching effect of the digital revolution, telehealth concepts referring to the delivery of healthcare services at a distance using information and communication technology (ICT) are inevitable innovations for modern healthcare provision. Designing ICT-based solutions for medical purposes constitutes an emerging field of activity for medical informatics and related scientific disciplines. 6
If end users accomplish basic communicative and technological skills, telehealth could tremendously support and facilitate patient empowerment and care on multilayered levels of communication, health promotion, and health monitoring. 7 ICT-mediated integration of complex diagnoses with customized preventive medicine and lifestyle suggestions considerably improve patients’ knowledge and compliance, and thus therapeutic success. 8 According to Huh et al., 9 self-monitoring of health parameters in non-clinical settings exerted lasting effects on consumers’ self-responsibility enhancing doctor–patient relationship as well as physical and mental health. Related studies found that ICT-based home care models for myocardial infarction as well as knee replacement rehabilitation positively affect health and well-being.10,11 Hence, increasing patient self-care reduces institutionalization, hospitalization, duplicative testing, and mortality rates. 1
In the rapidly growing ICT and telehealth sector, allocating adequate resources of personnel, financial, and know-how is central for equitably providing high-quality healthcare. 12 However, authoritative healthcare stakeholders own a vested interest in influencing political decision-making processes. We consider that recent liberalization and privatization efforts in telecommunication and network industries in Austria warrant exploring prevailing opinions regarding telehealth applications.
Thus, the current survey studied perceptions among a panel consisting of medical professionals (MP), patient advocates (PA), and administrative personnel (AP). In an anonymous, biphasic online Delphi process, these experts evaluated 10 prospective scenarios regarding perceived obstacles, benefits, innovativeness, desirability, and expected implementation date. The scenarios described possible outcomes of societal and IT development processes categorized into the three main topics (1) doctor–patient communication, (2) health promotion, and (3) pervasive health monitoring.13–15 Regarding doctor–patient communication, we assumed that telehealth influences the traditional relationship and face-to-face interaction between MP and their patients.7,16 Furthermore, we assumed that sustainable health promotion and disease prevention require empowered, self-reliant consumers. Based on consumer-centred doctor–patient communication and health promotion, we assumed that pervasive health monitoring via mobile sensors offers cost-effective health management.17–20
To meet the complexity of the multi-scenario-based approach, our analysis followed a stepwise procedure, picturing the collected data on the micro-, meso-, and macro level, respectively.13–15 Interpretation of single scenarios structured around the three main topics yielded in-depth scenario-specific information on a micro level. Focusing on one of the specific central topics investigated topic-specific assumptions on a meso level. Ultimately, interpreting summarized multi-scenario results compiled gathered data on a macro level. This article focused on the macro level, reporting the consolidated and group-specific findings of the Delphi survey.
Methods
Telehealth scenarios
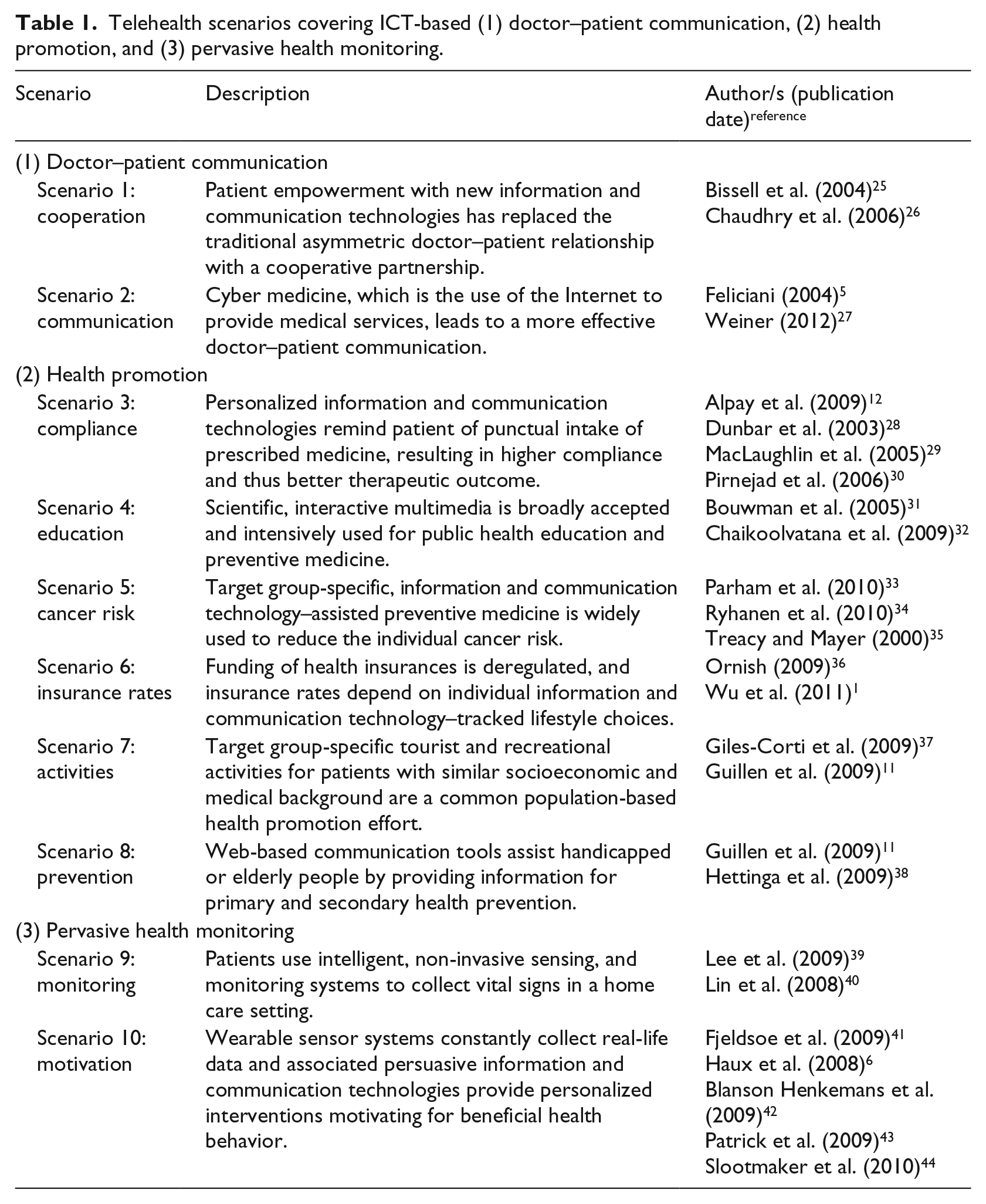
The Delphi survey was conducted in 2010 in accordance with the principles laid down in the Declaration of Helsinki. Ten scenarios illustrated implementation of software and monitoring solutions in the foreseeable future, spanning from quite likely to more innovative descriptions.21–24 We identified the key research fields: ICT-based doctor–patient communication (scenarios 1 and 2), health promotion (scenarios 3–8), and pervasive health monitoring (scenarios 9 and 10). These scenarios were scenario 1: cooperation, scenario 2: communication, scenario 3: compliance, scenario 4: education, scenario 5: cancer risk, scenario 6: insurance rates, scenario 7: activities, scenario 8: prevention, scenario 9: monitoring, and scenario 10: motivation. Table 1 provides an overview of these scenarios and the related literature.
Telehealth scenarios covering ICT-based (1) doctor–patient communication, (2) health promotion, and (3) pervasive health monitoring.
The Delphi survey process
The online Delphi survey questionnaire in German language consisted of two autonomous sections.13 –15 The first part assessed socio-demographic characteristics. The second part evaluated each of the 10 scenarios in ascending order using the corresponding fixed questionnaire items for benefits, obstacles, degree of innovation, desirability, and implementation date.
Two multiple-answer-questions assessed relevant benefits (six factors) and obstacles (nine factors) for implementation of telehealth solutions. Choices for benefits were as follows: quality of social healthcare, living standard, patients’ knowledge, funding of social healthcare, doctor–patient relationship, and no improvement. Choices for obstacles were as follows: cost/funding, acceptance by MP, acceptance by PA, acceptance by AP, data security/privacy, technical prerequisites, regulations/standards, influence of stakeholders, and no obstacles.
Furthermore, we evaluated innovativeness, that is, the degree of innovation, of the respective scenario by a 5-point Likert scale ranging from not innovative (=1) to very innovative (=4) as well as the non-response type choice “not applicable.” Subsequently, we dichotomized innovativeness to obtain low (i.e. not innovative, barely innovative, not applicable) and high innovativeness (i.e. somewhat innovative, very innovative). Next, the survey participants stated scenario desirability (desirable/not desirable). Ultimately, we asked the experts to indicate the time horizon of scenario implementation in Austria on a horizontal time line spanning the years 2010–2030.
After pilot-testing, we used SoSci Survey, a software package for scientific surveys, to conduct the Delphi survey. 45 A sample of Austrian experts working for national healthcare providers and health maintenance organizations were eligible for survey participation. The experts were approached via personalized e-mail invitation letters and pre-assigned to the corresponding group membership representing MP, PA, or AP. We selected these three groups due to their known role as key experts in telehealth-related decision-making and implementation processes. 46 Written informed consent was obtained prior to participation in the survey.
For round 1, we distributed a link to the online questionnaire and instructions by e-mail. For round 2, PHP program code and Microsoft Excel charting templates presented the summarized group responses along with individual ratings gathered in the preceding cycle. We invited the panel members to utilize this feedback loop to eventually adapt their previous ratings.
Statistical data analysis
Collected data were statistically evaluated using Excel spread sheet (Microsoft, Seattle, WA, USA) and SPSS version 21.0 (SPSS Inc., Chicago, IL, USA). We assessed frequency of participants endorsing benefits and obstacles per scenario and group-specific frequencies of perceived benefits, obstacles, degree of innovation, desirability, and estimated date of implementation of telehealth scenarios in Austria. For providing consolidated survey data on the 10 scenarios (macro-level analysis), we built a summarized multi-scenario score of scenario- and group-specific means. To further investigate inter-group differences, we conducted Kruskal–Wallis tests for nonparametric statistics on group size-weighted data. 47
Results
In total, 73 participants (74% males; mean age 43.9 years, standard deviation [SD] 9.4 years) fully completed both Delphi cycles. Whereas the subgroups did not differ regarding average age, survey participation rate of males compared to those of females was higher in the subgroup of AP (86%) and MP (84%), and slightly lower among PA (48%). During the biphasic Delphi survey, the panelists evaluated each of the 10 prospective scenarios. As shown in Table 2, the three top-ranked benefits were quality of social healthcare (overall mean 50%), highest in scenario 3 (81%), patients’ knowledge (overall mean 47%), highest in scenarios 1 and 4 (both 69%), and living standard (overall mean 45%), highest in scenario 8 (80%). Scenario 6 (26%) was highest ranked regarding “no improvement.” Compared to benefits, obstacles reached higher ratings consistently. Financial investment was seen as the top priority factor (overall mean 61%), highest in scenario 9 (85%). Acceptance by PA (overall mean 44%), highest in scenario 6 (74%), ranked second and data security/privacy (overall mean 40%) ranked third and highest in scenario 9 (67%).
Overall mean as well as scenario-specific ranking of perceived benefits and obstacles for implementation of telehealth scenarios in Austria.
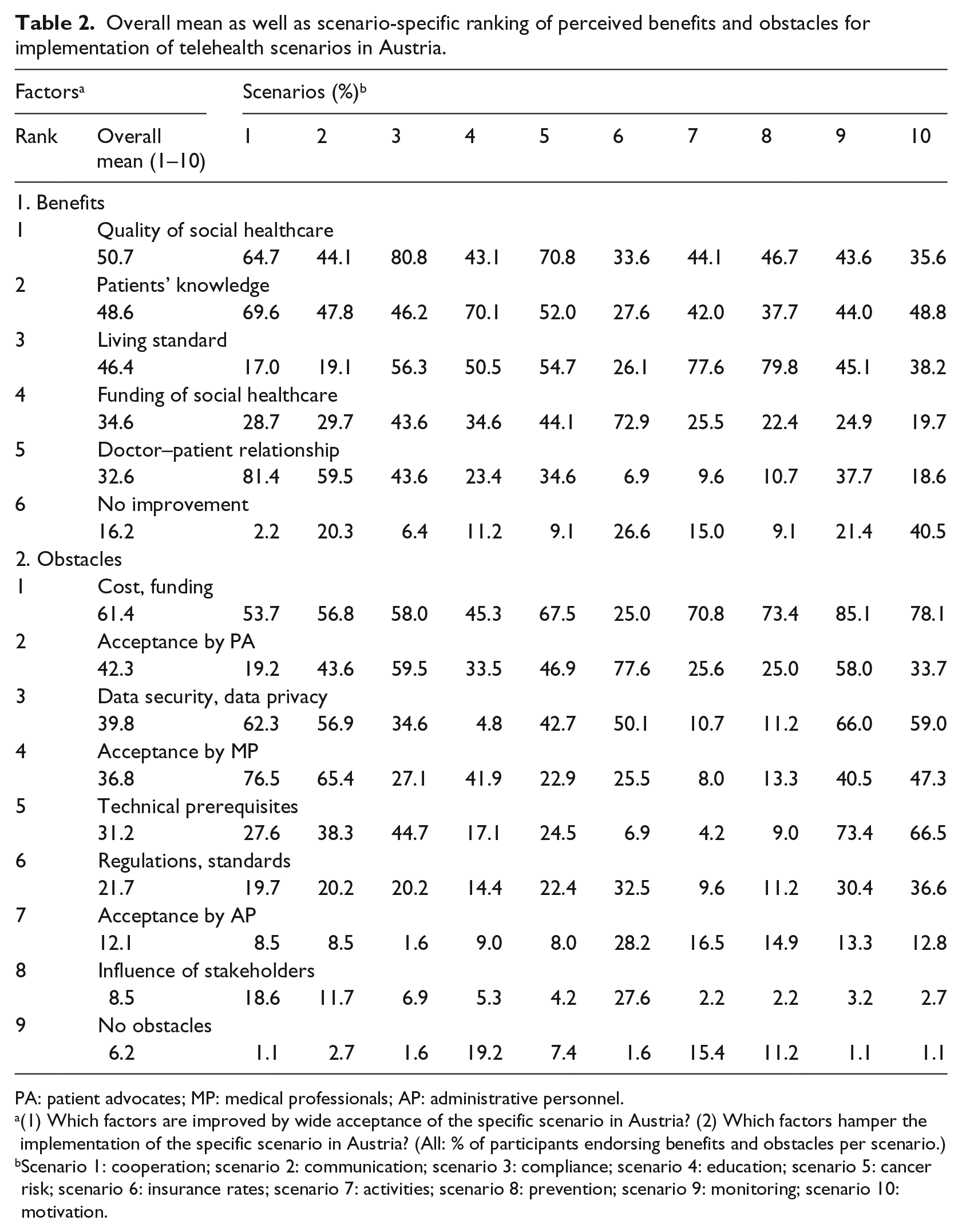
PA: patient advocates; MP: medical professionals; AP: administrative personnel.
(1) Which factors are improved by wide acceptance of the specific scenario in Austria? (2) Which factors hamper the implementation of the specific scenario in Austria? (All: % of participants endorsing benefits and obstacles per scenario.)
Scenario 1: cooperation; scenario 2: communication; scenario 3: compliance; scenario 4: education; scenario 5: cancer risk; scenario 6: insurance rates; scenario 7: activities; scenario 8: prevention; scenario 9: monitoring; scenario 10: motivation.
Table 3 depicts group-specific ratings, revealing that MP consistently picked fewer beneficial factors, “no improvement” more often (22% vs overall mean 16%), and “no obstacles” less often (5% vs 6%) compared to the other groups. Furthermore, regarding group self-assessment, the second ranked factor acceptance by PA yielded lowest agreement among PA (37% vs 42%) and the fourth ranked factor acceptance by MP received lowest agreement among MP (31% vs 37%). Reversely, the seventh ranked factor acceptance by AP attained highest agreement among AP (19% vs 12%).
Perceived benefits, obstacles, degree of innovation, desirability, and estimated date of implementation of telehealth scenarios in Austria, stratified by expert groups.
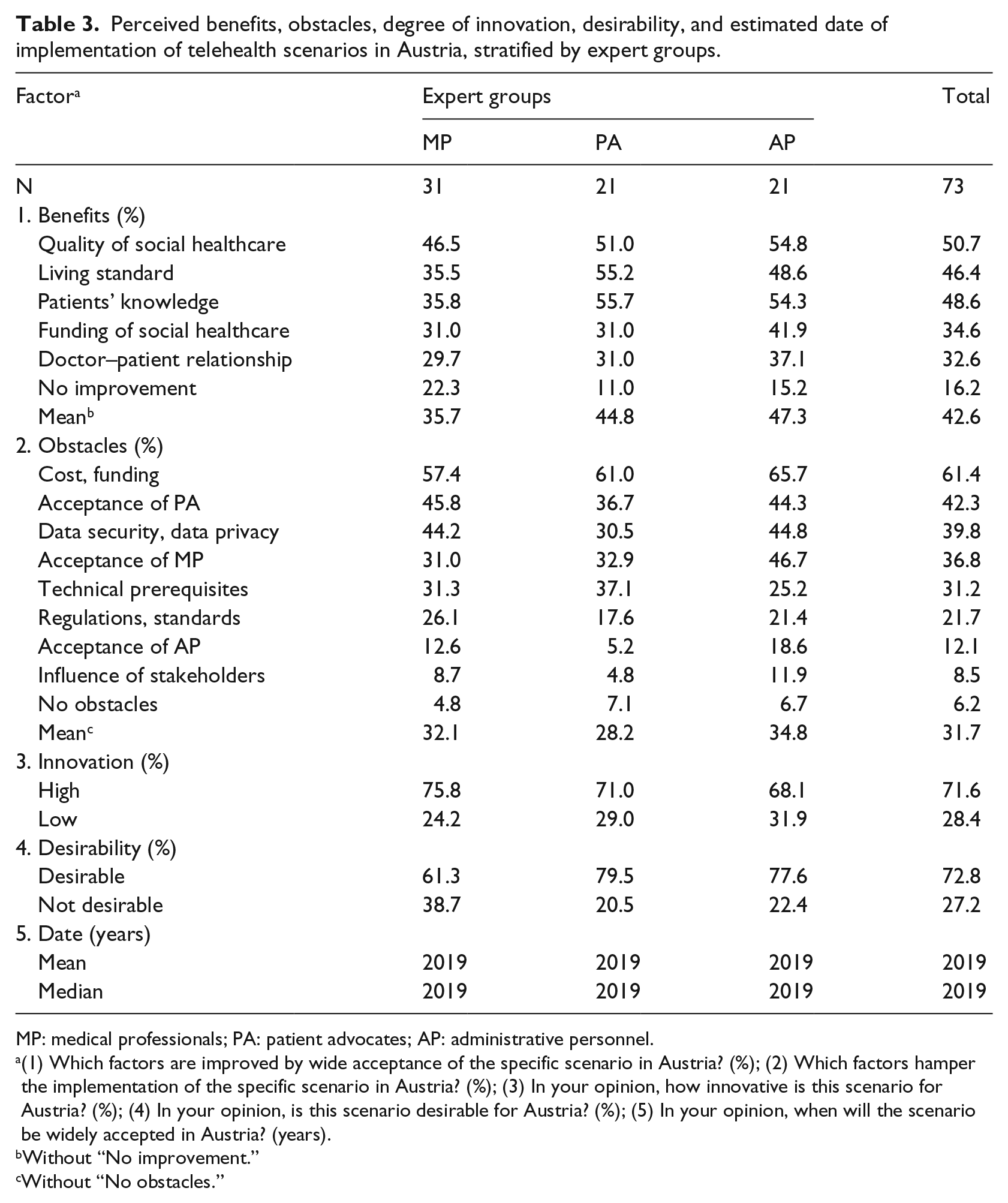
MP: medical professionals; PA: patient advocates; AP: administrative personnel.
(1) Which factors are improved by wide acceptance of the specific scenario in Austria? (%); (2) Which factors hamper the implementation of the specific scenario in Austria? (%); (3) In your opinion, how innovative is this scenario for Austria? (%); (4) In your opinion, is this scenario desirable for Austria? (%); (5) In your opinion, when will the scenario be widely accepted in Austria? (years).
Without “No improvement.”
Without “No obstacles.”
Participants perceived high innovation degree for all scenarios (overall mean 72%), with highest agreement for scenario 1 (88%), whereas low innovativeness (28%) was most prominent in scenario 6 (41%). Regarding desirability, 71% of participants perceived the scenarios as being desirable with highest agreement in scenario 3 (88%). Accordingly, 29% of panelists rated low overall desirability with the lowest rank for scenario 10 (62%). The year 2019 was the median expected scenario implementation date with the furthest away year (all: 2020) for scenarios 2, 6, 9, and 10.
Furthermore, we investigated group-specific survey response frequencies and differences (Table 4). Kruskal–Wallis tests revealed statistically significant overall group size-weighted, inter-group differences for benefits (mean 2.2 ± SD 1.3, p = 0.003), obstacles (2.4 ± 1.2, p = 0.010), as well as desirability (71%, p < 0.001). MP scored lowest in the categories benefits (1.8 ± 1.3) and desirability (0.6 ± 0.2), whereas PA scored lowest in obstacles (2.2 ± 1.2) compared to the other stakeholder groups. MP scored highest in these two domains compared to the other experts (innovativeness: 3.1 ± 0.9, date estimates: 2019.3 ± 2.8). Nevertheless, we did not find statistically significant differences for innovativeness (overall 3.0 ± 0.9) and date estimates (overall 2019 ± 3.0), all: p = n.s.
Group size-weighted, inter-group comparisons of perceived benefits, obstacles, degree of innovation, desirability, and estimated date of implementation of telehealth scenarios in Austria.
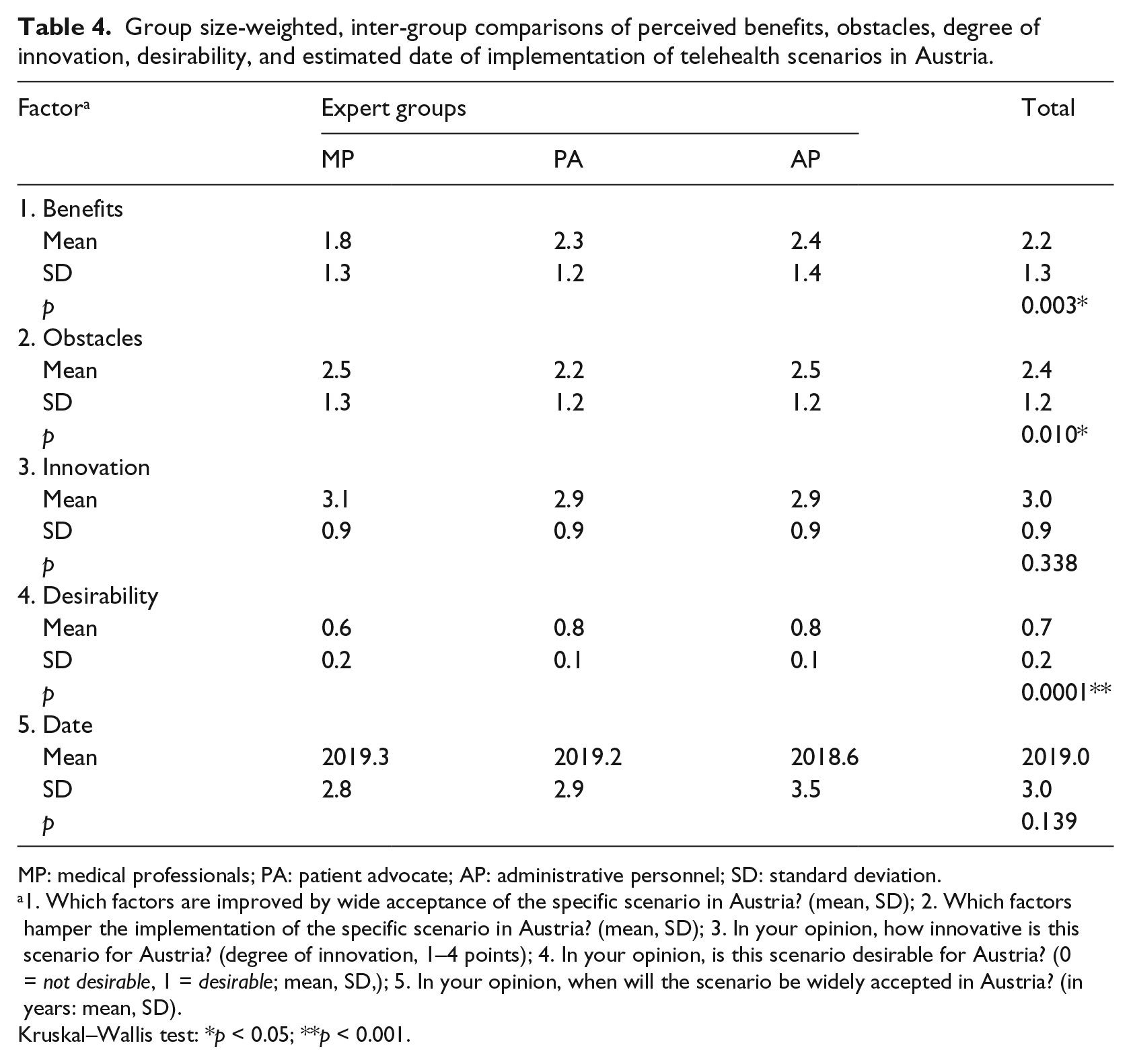
MP: medical professionals; PA: patient advocate; AP: administrative personnel; SD: standard deviation.
1. Which factors are improved by wide acceptance of the specific scenario in Austria? (mean, SD); 2. Which factors hamper the implementation of the specific scenario in Austria? (mean, SD); 3. In your opinion, how innovative is this scenario for Austria? (degree of innovation, 1–4 points); 4. In your opinion, is this scenario desirable for Austria? (0 = not desirable, 1 = desirable; mean, SD,); 5. In your opinion, when will the scenario be widely accepted in Austria? (in years: mean, SD).
Kruskal–Wallis test: *p < 0.05; **p < 0.001.
Discussion
It is evident that on-going technological achievements impact all levels of healthcare. Given the complexity of today’s healthcare environments, successful telehealth adoption presents multidimensional and inter-professional challenges, depending explicitly on human-related, social, and institutional factors. Apparently, diverse interest groups emphasize different aspects depending on the organizational system they belong.25,48 To assess multidisciplinary perspectives, this study’s Delphi panel consisted of experts serving as representatives of the medical professional, patient, as well as administration perception.13,14
In our survey, experts anticipated that quality of social healthcare, patients’ knowledge, and living standard as the top-ranked factors could eventually profit from future telehealth scenarios. Finding these qualities among the top three benefits could represent a change in paradigm, resulting in improved health services along with end users’ empowerment, autonomy, and self-assertion.1,7 These results are in accordance with Haux et al., 6 who suggested that quality of healthcare delivery significantly benefits from interactive, long-distance counseling and pervasive health monitoring applications.
Expected costs, acceptance by PA, and data protection were among the most relevant obstacles for the nationwide adoption of innovative health technologies. Other important obstacles included acceptance by MP and technical prerequisites. Given scarcity of funding, every resource spent on health promotion has opportunity costs in other economy sectors. Hence, we suggest that the aforementioned rating reflected a shift toward consumer-centric healthcare using existing resources (e.g. privately owned smartphones) without overstraining the available capacities.
Concerns about IT security are increasingly advancing, as shown by other surveys,26,27,49 and quantified by the share of spending budget for achieving acceptable levels of security and ensuring system resistance to security compromises. 27 Data privacy measures include confidentiality and privacy aspects, but also safekeeping of data manipulation. Data security awareness of staff members could minimize risks of IT breaches and security vulnerability. Effective technical prerequisites require organizational and personnel measures to ensure privacy and security of sensitive patient data. Ultimately, the patients’ trust in the fact that doctors ensure all conceivable aspects of privacy constitutes an extremely valuable asset for everyday doctor–patient relationships.49,50
Our findings on external assessment and self-assessment of acceptance suggested that PA and MP undermatched the level of how other interest groups perceived their halting attitudes in telehealth implementation. Contrarily, AP were more likely to be self-confident regarding their respective positive attitudes.
The multifarious, fragmented internal structures of health organizations have been claimed responsible for slower IT integration and adoption in the healthcare sector compared to other branches. 48 We assessed estimates of time frames for scenario implementation to seize the prevailing temporal expectations among experts involved in respective decision-making. The ratings pointed toward a date approximately 10 years ahead of the year 2010 when this study was conducted, a surprisingly long time period considering that the scenario-based telehealth solutions were already conceived by then. These findings on quite reluctant temporal estimates might provoke experts to reframe priorities of doctor–patient communication, health promotion, and pervasive health monitoring applications.
Inter-group comparison regarding desirability revealed that PA and AP perceived more scenarios as desirable compared to MP. This finding confirms the notion that MP might be more critical about telehealth and related technological applications. 48 As a possible explanation, the perceived undermining power of profoundly embedded professional constructs of doctor–patient interactions could hamper acceptance of telehealth among physicians’ health culture, age, and gender independently.31,32,51 However, according to Anderson, 52 general practitioners perceive that ICT applications could increase patient empowerment and reduce expenses. Respective “soft” obstacles include insufficient IT knowledge, privacy, and legal concerns, whereas high initial costs and lack of financial support are seen as “hard” barriers. 53
As physicians’ intention to telehealth use is vital for national-scale implementation, highlighting the expected telehealth merits could increase technology adoption.32,34 Akesson et al. 36 reported that telehealth users felt more empowered and better informed about their health status. Also, these consumers did not perceive ICT utilization, absence of face-to-face consultations, and privacy issues as obstacles. In their review article on mobile apps used in health behavior interventions, Payne et al. 37 proposed good acceptance of mobile apps to assist individuals in modifying their health habits, though identifying a lack of best practice evidence. Health-related technologies might be more difficult to adopt especially for the elderly or neglected strata of the population such as mental healthcare consumers, requiring particular consideration regarding their training, support, and specific personal needs.38,54
Smartphone apps offer a huge range of health- and fitness-related applications for preventive, curative, as well as recreational purposes. 55 Given nearly ubiquitous Internet access nowadays, identification of individual preferences and health information needs of consumers is a prerequisite for effective telehealth solutions.11,56 Along with empowerment of end users and improved collaboration of healthcare stakeholders, governmental strategies for adequate funding and performance incentives are required to implement future costumer-tailored telehealth services.
Austria started a nationwide test run of a shared electronic health record (EHR) system in 2015. 57 Through this new electronic health management tool, laboratory and radiology reports, hospital discharge letters, and a patient medication history called eMedication will be electronically available. Although the concept of this new electronic health management tool is well-founded, the expected organizational and procedural challenges dramatically decreased acceptance by MP. This skepticism and resistance to adopt the EHR delayed its implementation several years. Our Delphi survey adds to the body of knowledge in the research field so far missing insight into Austrian experts’ perception of future health-related ICT solutions. Additionally, we introduced 10 future scenarios and developed an online questionnaire for collecting data of a two-round online Delphi survey.
Strengthens and limitations
A strength of the study was the large study population consisting of experts (n = 73) in high-ranking positions in the Austrian healthcare sector from all nine Austrian provinces. We conducted the survey over two rounds to maintain robust feedback and to minimize high attrition rates inherent in multiple feedback rounds. The survey results could be used to validate evolving demands of modern healthcare systems including target group-specific user acceptance. The consolidated results synthesized the expert opinions and corresponding inter-group comparisons. As such, the insights gained in this study could help to more comprehensively evaluate the complex interplay between consumers, health practitioners, and policy makers. Further research could adjust the survey to on-going technological advances and refine our findings using cross-sectional, quasi-experimental, and mixed method approaches, subsequent focus groups, and consensus conferences. 58
The results of the study should be considered within the context of study design and associated limitations. Noteworthy, the data have been gathered in 2010, and more recent societal as well as technological developments should be taken into account when referring to our findings. Panelists were not able to unerringly predict prospect technical developments in a Delphi survey setting. However, their opinions could be of interest due to their influence as key decision-makers shaping the future of Austrian telehealth. The scenarios were intended to strongly link to the currently existing concerns of policy makers addressing the key question of where to place resources in telehealth implementation processes. The telehealth scenarios were not intended to formulate ideal, best-case, or worst-case scenarios. Nevertheless, findings from this survey might represent a conceptual basis for increasing mutual understanding and activating critical examination of current practices.
Conclusion
As both human and organizational factors affect successful telehealth adoption, this study suggests potential targets for facilitating mutual policy- and decision-making processes. Measures should be taken to increase respective public knowledge and skills. The findings of this Delphi survey recommend increasing awareness on interest group-specific needs regarding future healthcare by establishing close cooperation, networking, communication, and practice sharing among competent authorities. Telehealth stakeholders should feel obliged to focus on transparent and rigorous quality and safety assurance procedures. To avoid health inequalities in aging societies, these stakeholders should address the digital divide that refers to unequal telehealth access by disadvantaged populations typically affecting disabled and elderly people.
Footnotes
Acknowledgements
The authors sincerely appreciate the contribution from all participants of this Delphi survey.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.