
Abstract
The diffusion and adoption of information technology innovations (e.g. mobile information technology) in healthcare organizations involves a dynamic process of change with multiple stakeholders with competing interests, varying commitments, and conflicting values. Nevertheless, the extant literature on mobile information technology diffusion and adoption has predominantly focused on organizations and individuals as the unit of analysis, with little emphasis on the environment in which healthcare organizations are embedded. We propose the social worlds approach as a promising theoretical lens for dealing with this limitation together with reports from a case study of a mobile information technology innovation in elderly home care in Denmark including both the sociopolitical and organizational levels in the analysis. Using the notions of social worlds, trajectories, and boundary objects enables us to show how mobile information technology innovation in Danish home care can facilitate negotiation and collaboration across different social worlds in one setting while becoming a source of tension and conflicts in others. The trajectory of mobile information technology adoption was shaped by influential stakeholders in the Danish home care sector. Boundary objects across multiple social worlds legitimized the adoption, but the use arrangement afforded by the new technology interfered with important aspects of home care practices, creating resistance among the healthcare personnel.
Keywords
Introduction
The past decades have unveiled an impressive trajectory of mobile information technology (IT) innovations, marked primarily by the advancements from early mobile telephones, available to the elite few, to the widespread ownership of highly advanced devices today.1,2 More specifically, mobile healthcare applications have represented emerging and enabling technologies that have been applied in several contexts.3–6 For example, personal digital assistants (PDAs) and smartphones are being used to support elderly home care services in many countries.7,8 These technologies seem to offer advantages compared to the conventional computing devices found in the healthcare sector, such as notebook computers or personal computer tablets. From a technical perspective, the small size, clear screen, and robustness are appealing characteristics, and, from a healthcare personnel perspective, the ability to perform multiple functions at the point of care may be an attractive proposition (e.g. access to databases with client information). 8
Yet the adoption of mobile IT in health care remains more limited than one might expect from the generally hopeful tone in current studies in the area. 9 One impediment to the limited success is the heterogeneity and inter-organizational endeavours of stakeholders characterized by differences in commitments, approaches, and values. 10 The adoption and diffusion of mobile IT is a result of a process of negotiation, where different stakeholders hold and promote various and sometimes, conflicting values influencing the entire process of adoption and diffusion. It is more of a collective achievement 11 requiring collaboration and partnership among heterogeneous stakeholders (e.g. managers, healthcare personnel, and technological vendors) possessing specialized knowledge and resources that can be integrated to achieve the potential benefits from the new technology.12,13
Consequently, as Van De Ven 11 noted, traditional diffusion theories emphasizing the actions and decisions taken by individual firms and individual actors are inadequate when attempting to explain the adoption and diffusion of complex technology systems. Yet in the specific field of mobile IT within health care, scholars7,14–18 have predominantly drawn on traditional perspectives (e.g. Technology Acceptance Models 19 and diffusion of innovation theory 20 ) and focused on organizations and individuals as the unit of analysis with little emphasis on the environment within which organizations are embedded. Although the insights from these studies have enriched our understandings of how and why healthcare personnel adopt and use mobile IT in practice, recent work in the adoption and diffusion of complex technologies highlights its limitations.13,21 More specifically, adopting and diffusing complex technologies such as mobile IT in healthcare settings is complex, problematic, messy, and malleable. 13 Such complex technologies have interpretive flexibility,22–24 and stakeholders construct different meanings about the technology. Van de Ven 11 argued that when innovation is viewed as involving heterogeneous stakeholders and as a distributed phenomenon, it is often characterized by network effects, ambiguity, and combinability.
Similarly, in this article, we draw on empirical material from a case study of mobile IT in elderly home care services in Danish municipalities, emphasizing how adoption and diffusion of mobile ITs is an uncertain process of change involving multiple stakeholders with occasionally competing interests, varying commitments, and conflicting values. In the Danish case, mobile ITs have spread rapidly (Appendix, Table 5), but the process involved negotiations, compromises, and tensions between key stakeholders. To understand this process in more detail, we draw on the concepts of social worlds, trajectories, and boundary objects from the literature of symbolic interactionism.25–28 The social worlds perspective is a well-established and rich sociological tradition to investigate and analyse the politics of socio-technical change, and the tools can be used to connect macro-level and micro-level social phenomena.29,30 In this article, we therefore distinguish between the features of the sociopolitical environment shaping what is possible and desirable concerning the adoption and use of mobile IT, and the organizational level, where each organization’s history further shapes the opportunities and constraints surrounding the new technology.31,32 This perspective helps us see the adoption and diffusion of mobile IT as intertwined, ongoing technical and social negotiation process between heterogeneous social worlds thus challenge the view that the diffusion process is a linear and well-planned process as often depicted in the literature.25,28 This article therefore aims to answer the following questions:
What are the trajectories of adopting and diffusing mobile IT to support elderly home care services in Danish Municipalities?
How did the interaction and negotiation between stakeholders from different social worlds shape the adoption and diffusion process, and how did boundary objects mediate such interaction?
The next section (‘Social worlds, trajectories, and boundary objects’) provides an overview of the social world perspective and the associated notions of trajectory and boundary objects. Section ‘Research approach’ presents our research design. The results of applying the social world perspective to explore mobile IT adoption and diffusion in Danish elderly home care are outlined in section ‘Case description’, and section ‘Discussion’ discusses the key findings and contributions to research. We conclude the article in section ‘Conclusion and implications’ and discuss some of the limitations of our study.
Social worlds, trajectories, and boundary objects
The social world framework has its roots in the American sociological tradition of symbolic interactionism, emphasizing the construction of meaning ‘amongst groups of actors – collectives of various sorts – and on collective action – people doing things together and working with shared objects’ (p. 113). 27 Within this line of thought, the diffusion of technological artefacts is not viewed as a preordained process that is propelled by the inherent efficiency of the technology itself; rather, it is an outcome of social and political negotiations. 29 Concepts such as social worlds, trajectories, and boundary objects which are developed within the symbolic interactionism tradition have potential to open up and explore the dynamic and complex sociopolitical processes of adopting and diffusing technologies.
The social worlds are groups with ‘shared commitments to the pursuit of a common task, who develop ideologies to define their work and who accumulate diverse resources needed to get the job done’ (p. 412). 33 As such, social worlds are self-organizing units in which people share resources, information, assumptions about what is important, and ideas about what sorts of activities are desirable. 29 The social worlds framework thus assumes formal or informal collective actors (including individuals, groups, and organizations) – social worlds – in which people share meanings, material objects, and joint activities. 34 Social worlds are characterized by a commitment to common assumptions about what is important and what should be done; for example, a task force, academic department, project team, or nurses who share perspectives and meaning forms the basis for collective action. 34 In social worlds, ‘various issues are debated, negotiated, fought out, forced and manipulated by representatives’ of the participating social worlds (p. 239). 27 Social worlds could be studied and analysed on any scale, ‘from smallest (say local world, on local space) to the very largest (in size or geographic spread)’ (p. 421). 26
The question becomes, however, how do diverse, bounded social worlds come together to collaborate and achieve the desired objectives? With regard to this question, Star and Griesemer
35
use the ‘boundary objects’ concept to explain things that exist at the junctures where different social worlds meet in an arena of mutual concern. Since its first appearance in the literature of science and technology studies by Star and Griesemer in 1989, researchers have referred to the boundary objects concept when studying the interactions taking place and the objects that people create and use in the context of crossing the boundaries of different social worlds and communities. Gal et al.
36
describe boundary objects as … abstract or physical artefacts which reside in the interfaces between organizations or social communities and have the capacity to bridge perceptual and practical differences among diverse communities in order to reach common understandings and effective cooperation. (p. 194)
Boundary objects therefore serve as intermediaries (interfaces) between multiple social worlds and facilitate the interaction, communication, and flow of information, concepts, skills, and materials between diverse social actors.37,38 The notion of boundary objects has been applied to denote different things, including physical products or prototypes,39,40 design drawings and blueprints, 41 shared Information Systems (IS),42,43 and standardized reporting forms. 44 Star and Griesemer 35 argued that certain boundary objects are flexible enough to accommodate different interpretations or interests emanating from various distinct social worlds yet robust enough to maintain a common identity across all social contexts, thus allowing translation to take place across the boundary. Clarke 34 pointed out that the process developing and adapting boundary objects (e.g. mobile-based health care) through the actions and interactions of stakeholders from different social worlds ‘is fundamentally an exercise of negotiated order and a robust boundary object achieves this status by satisfying both the particular, local demands of users and the wide arena demands of all the worlds involved’ (p. 134). 34
‘Trajectory’ can be used to conceptualize the ongoing nature of the interactions through which people attempt to get work done. 29 According to Strauss, 30 the notion of trajectory has two main dimensions:
‘The course of any experienced phenomenon as it evolves over time’ and
‘The actions and interactions contributing to its evolution’ (p. 53–54). 30
Strauss and other symbolic interactionists have used the term trajectory quite differently from how it has been used in the economics of technology literature. In the latter case, technological trajectory refers to an inherent property of the technology itself – a set of potentials that almost inevitably propel the technology in a certain direction. 45 In the context of symbolic interactionism, trajectories encompass both technological and human components and they are not predictable. 29 Trajectories change over time as people in the situation engage in ongoing interactions with themselves and/or others. 30 They assess what is going on, predict outcomes, and change and refine their strategies accordingly. Nevertheless, the unforeseen may happen. Coping mechanisms may not work, and a planned trajectory may change direction as people try to repair or salvage the situation.
Garrety and Badham 29 argued that planned and purposeful technological change trajectories usually call for complex interactions and negotiations. In most cases, the people involved (e.g. designers, vendors, users, and managers) come from very different institutional or professional backgrounds. Consequently, the investigation of technological change trajectories requires an analysis of the social worlds involved, the capacities of the different stakeholders, the boundary objects used, and the ensuing negotiations among the involved worlds as the trajectory evolves. 29
The crucial concept motivating our belief in the importance of the theory of social worlds and the associated notions of boundary objects and trajectories is that organizational actors, whether they are designers, developers, managers, or users, are not isolated, independent actors. Rather, when engaged in adoption and diffusion of large-scale and complex technological systems (e.g. mobile IT) that require inter-organizational collaboration, the individual stakeholders develop attitudes and values towards those systems based on their own social contexts. For example, in the process of introducing mobile IT to support Danish elderly home care services, stakeholders from different social worlds interact and negotiate concerning the role and potential benefits of the new technology. The meaning of the technology evolves and transforms when transcending to heterogeneous stakeholders from different social worlds. In early stages of diffusing mobile IT, we demonstrate how boundary objects (e.g. a pilot project labelled CareMobile) mediate the interaction as objects inhabiting several intersecting social worlds and satisfy the needs of the different social worlds. However, this does not mean that the whole process of adopting and diffusing the technology to different organizational contexts has been a smooth process of translating the interests of different stakeholders. Instead, there were occasionally tensions due to conflicts of interest.
Research approach
To explore adoption and diffusion of mobile IT, we used elderly home care services in Denmark as our case setting. The case design represents a single, embedded case design including multiple units of analysis 46 including the organizational level of analysis (home care organization) and the broader sociopolitical environment. The Danish public sector is structured according to state, region, and local government, and at the local level 98 municipalities are responsible for most of the public services, including day-care centres, schools, and elderly care (including home care services). Denmark offers extensive services to the elderly and a high per capita spending on resources. 47 Home care reaches 25 per cent of all citizens aged 67 years and older (more than 200,000 people), and approximately 70,000 care workers and 6000 nurses are employed in this sector. Basic service tasks include personal care (e.g. bathing and dressing) and practical care (e.g. cleaning and washing up). 48 Since the early 1990s, Danish home care has increasingly digitalized its work practices, initially with the adoption of back-office home care IT systems with elaborate client records and more recently with the introduction of mobile ITs, such as PDAs, for healthcare personnel. Preliminary mobile IT experiments took place in 1998–1999. By 2007, approximately 80 per cent of the 98 municipalities had implemented mobile IT in home care (Appendix, Table 5).
We relied on multiple sources of data from the different stakeholder perspectives. The first author collected data during 2007 and 2008. Table 1 provides an overview over the data sources.
Data sources.
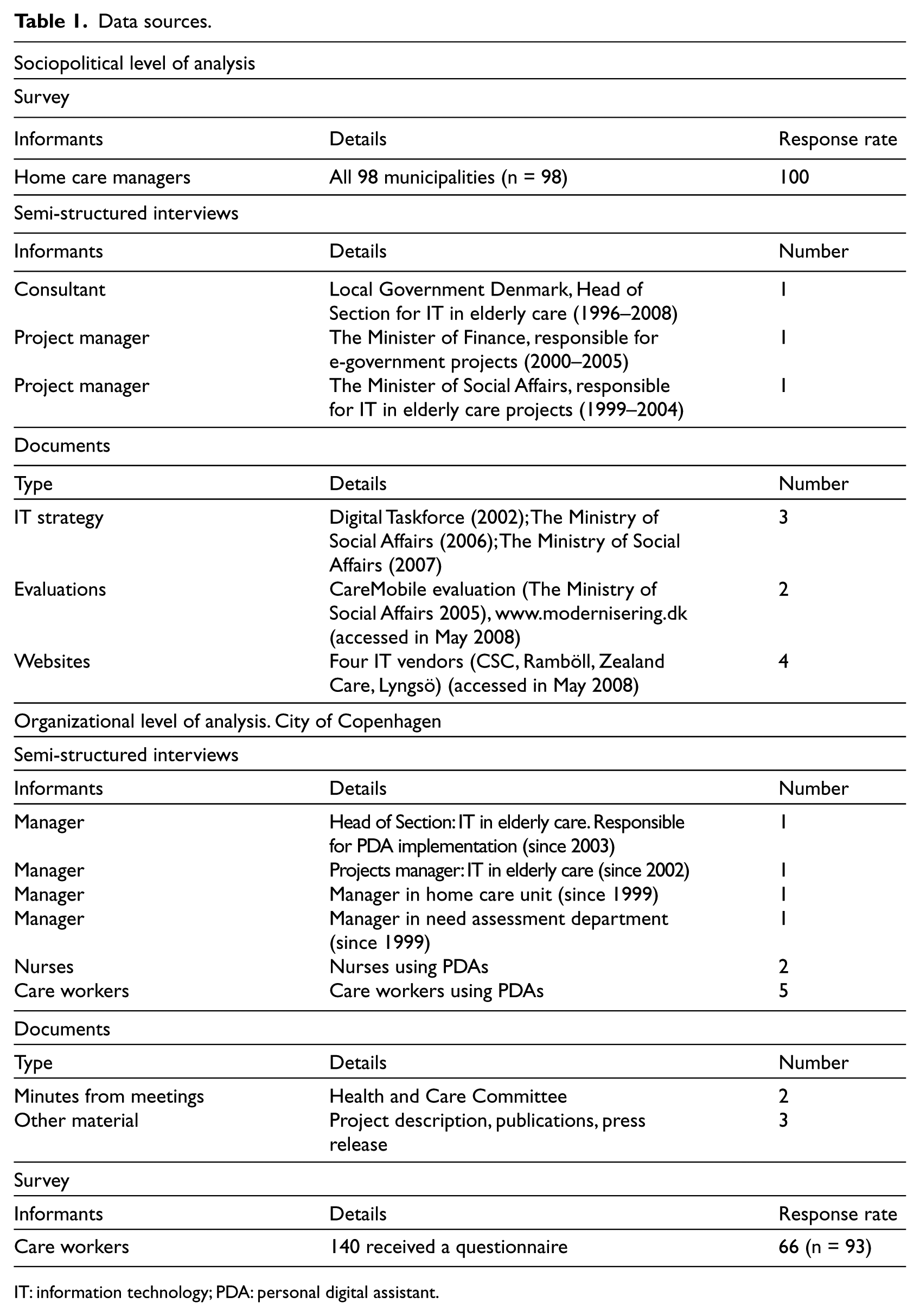
IT: information technology; PDA: personal digital assistant.
We began by conducting a survey of the home care managers in all 98 municipalities to map the diffusion pattern of mobile IT and to improve our understanding of the research context. The survey included questions such as Did the municipality adopt mobile IT in home care? If so, why did they adopt the technology? Which employees make use of the technology? When did the project started? Who have been key sources of inspiration for adoption? The survey was conducted in the form of telephone interviews, ensuring a 100 per cent response rate. Next, we concentrated on how major stakeholders promoted and negotiated mobile IT in the broader home care sociopolitical environment. We reviewed the available policy documents about mobile IT found in government reports and on websites (e.g. IT strategies, modernization strategies, and evaluation reports), we reviewed four technology suppliers’ websites and consultant reports promoting mobile IT. In identifying these specific documents, we relied on what has been reported in previous Danish research on the subject (e.g. Nilsson 49 ), recommendations from interviewed stakeholders, and input from colleagues in academia. It has no guarantee that everything is included, but we assume that the most important documents are captured. From these documents, we were not only able to identify key events in the diffusion and adoption process but also to focus on strategies and meaning construction regarding mobile IT among different stakeholders.
We also interviewed key stakeholders from The Ministry of Social Affairs, The Ministry of Finance, and Local Government Denmark (LGDK) (major interest group for the 98 municipalities) as they were extensively involved in the discussion of mobile IT as a promising way of modernizing Danish home care. The interviews were semi-structured and focused on areas such as (1) important events about the introduction of mobile IT, (2) how different stakeholders were involved in the diffusion process, and (3) the actions undertaken to deal with emergent problem and conflicts. The interviews lasted 1 h on average and were tape-recorded and transcribed.
Moving to the organizational level, we concentrate on how mobile IT was adapted in a specific home care setting. In the municipality, where our investigation took place (the largest in Denmark), there are about 3300 care workers involved (Table 2). The selected municipality is considered to be a pioneering municipality due to mobile IT usage in Danish home care; PDAs have been used systematically over a longer period of time (since 2002), approximately 2650 devices are in daily use, and the municipality’s mobile IT initiative was awarded the ‘best practice’ in 2006 as part of a nationwide competition. The technical solution included mobile access to electronic databases with client information (e.g. medicine schemes, progress notes, nursing notes, clinical guidelines, and information on doctors and family members) and made it possible for the workers to utilize this information at the point of care. It also became possible to register the time and services provided at the point of care, and paper-based work schedules were replaced by electronic schedules, accessible via PDA devices. Information pertaining to client records was transferred between mobile devices and back-office IT systems via wireless infrared communications (Bluetooth) or a docking station. The system did not include a telephone feature. By selecting this organization for our study, we assume it is possible to obtain rich insight into the process of change and more long-term implications of mobile IT use.
Case setting.
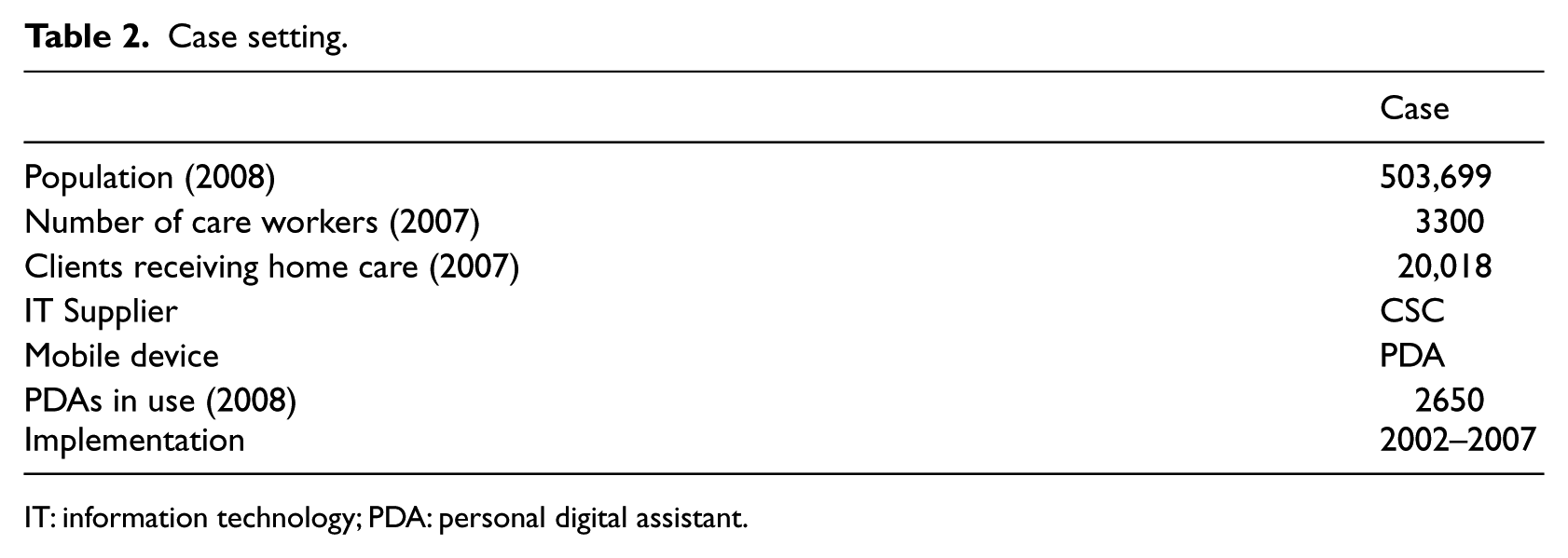
IT: information technology; PDA: personal digital assistant.
In addition, at the organizational level of analysis, we relied on different data sources. Interviews involved home care managers and IT project managers; four key administrative actors in total were interviewed. This was followed up by interviews with five care workers and two nurses using the technology in practice. Interviews included question that allowed the respondents to express how they considered the decision to invest in mobile IT and how they experienced the implementation process and daily use of the technology. These interviews were also tape-recorded and transcribed. We had also reviewed some internal documents and reports such as project descriptions and minutes from different meetings with regard to the adoption of the technology. We have to admit that this was possible because of the willingness of the managers of the municipality in giving us access to the internal documents. However, we had to rely on what they gave us access to. To supplement the information we got from our screening of the internal documents, we also reviewed the municipality’s website, but it has still no guarantee that everything has been comprehensively explored. Finally, we draw on survey data in order to improve our understanding of how healthcare personnel experienced the use of mobile IT. A total of 140 home care workers received a paper-based questionnaire and 93 responded (66% response rate). Hence, survey data were used to confirm and supplement interview data.
The analysis of our empirical data was inspired by established methods for handling qualitative data. 50 To begin with, we read through the transcribed interviews and the collected documents to provide an overview of the total material. The next step was more directly linked to our research question. We began by analysing the data regarding the broader sociopolitical environment (first part of the analysis) and then included the organizational level in the analysis (second part of the analysis). The theoretical apparatus, which embraced the notions of trajectory, social world, and boundary objects, has been used to inform the analysis and thereby served as a sensitizing device 51 for what ‘to look for’ in the data. The next section describes our empirical study of mobile IT adoption and diffusion in Danish home care as it unfolded in the period between 1998 (where the first experiments were carried out) and 2008 (where the vast majority of municipalities had adopted the technology).
Case description
Hasty diffusion
Within the last 10 years, mobile IT in home care has become an important part of the policy agenda on modernizing public administration in Denmark.52–54 Like many other public organizations, the Danish home care sector is faced with major challenges such as limited budgets and demographic changes with respect to the expected growth of the number of elderly in need of care. 55 For years, new technology has been expected to offer part of the solution to these problems. 56 The debate on mobile IT in Danish home care was gaining ground during the late 1990s, suggesting that this specific technology was worth careful consideration as part of modernization efforts. 52
In 2002, a government-financed pilot known as CareMobile 53 made mobile IT a political issue, producing support from influential stakeholders within the home care sector. CareMobile involved multiple social worlds with varying interests (including The Ministry of Finance, The Ministry of Social Affairs, and LGDK) along with four technology suppliers and six pilot municipalities. In fact, CareMobile had the capacity to bridge different interests among diverse stakeholders and became an important piece in the puzzle of justifying mobile IT as a powerful innovation in the modernization of Danish home care.
As the different stakeholders promoting CareMobile have different interests, the process of making choices about mobile IT use involved negotiations and compromises between these stakeholders. For the Ministry of Social Affairs, the main issue was to support a marketization movement in Danish home care. Such change process required, among other things, more accurate documentation of the costs of home care service delivery to guarantee fair competition between public and private providers. Mobile IT was seen as an important tool in the collection of more accurate documentation, especially in terms of how healthcare staff spend their time.
57
LGDK focused on getting rid of existing control and barcode scanners and replacing them with new mobile devices ‘that could do much more than merely record time’, thereby ensuring better working conditions for the healthcare personnel (interview, representative from LGDK). For The Ministry of Finance, it was more about identifying a sound business case for mobile IT use, thereby concentrating on economic and business-related issues (interview, representative from The Ministry of Finance). However, during the project and in the final evaluation of CareMobile, the issue of measuring effects and, especially, efficiency ultimately left an indelible mark on the project. Indeed, this was the agenda of The Ministry of Finance. For example, an interview with a representative from the Ministry of Social Affairs is formulated in the following manner: This is now a matter of documenting an effect of mobile IT use with the intention of creating a proper foundation that may assist other municipalities in their decision making. The basic challenge was to document the release of resources as an effect of mobile IT use. (interview, representative from the Ministry of Social Affairs)
The evaluation of the CareMobile project, which was communicated in national reports (e.g. The Ministry of Social Affairs 53 ) and on government websites (e.g. www.modernisering.dk), clearly found that the dissemination of the use of mobile IT had positive effects. These reports communicated in favour of mobile IT in terms of progress and cost–benefit, and the evaluation served as evidence that the investments in mobile IT would pay for themselves after 1 year. 53 CareMobile became a powerful vehicle for the subsequent trajectory of the adoption and diffusion of mobile IT. The successes with CareMobile encouraged the Danish government to finance future mobile IT adoption, 65 as the government allocated approximately 45 million euros in the 2006 Budget to strengthen this process. These subsidies ensured the rapid diffusion of mobile IT in 2006–2007, where 81 of the 98 municipalities in Denmark received government funding. Moreover, the CareMobile experience provided powerful inspiration for municipalities to adopt mobile IT. In fact, the home care managers regarded the technology suppliers, other municipalities, and CareMobile as the main sources of inspiration (Appendix, Table 6).
Our empirical data also suggest that the suppliers were not only involved in designing and developing technological solution but also in the construction of mobile IT into an appealing management idea. In order to convince home care organizations about the superiority of the technology, one supplier (Zealand Care) presented mobile IT as the ‘solution of the future’, highlighting how home care organizations could not only achieve better resource utilization and improved services but also more satisfied healthcare personnel and clients. Another supplier (CSC) presented a video on their website illustrating the benefits of mobile IT use. In the video, politicians, managers, care workers, and nurses all described the benefits of using the technology. These are practical case examples of how suppliers use the technology as a boundary object to persuade powerful stakeholders and to gain support towards its adoption and implementation.
Problematic adoption and implementation process
Moving to the organizational scene (i.e. the City of Copenhagen), we see how optimistic announcements from government bodies and technology suppliers were echoed by top managers. Yet the use arrangement afforded by the new technology interfered with important aspects of home care practices, thus creating user resistance. In this way, we illustrate how tensions between different social worlds (managers vs healthcare personnel) occurred as mobile IT was implemented and used in day-to-day work. Consequently, mobile IT in practice did not serve as a boundary object that had the capacity to bridge perceptual and practical differences among managers and workers; 36 rather, the technology seems to reinforce exciting differences.
Since the mid-1990s, the City has acknowledged its need to improve time management in home care. 59 Home care reforms, including marketization principles and activity-based billing, reinforced this need for more accurate documentation. It was emphasized that ‘…time control is critical as exceeding with five minutes per visit in home care corresponds to exceeding the budget by 17 million Euros per year’. 49 Before introducing mobile IT, the City experimented with barcodes to improve documentation, but mobile IT was seen as a more modern solution. 59 Consequently, the members of the Copenhagen City Council decided to invest in PDAs in 2001. Implementation took 5 years, from 2002 to 2007, including employee training, following a stepwise implementation strategy by one district at a time.
Home care managers welcomed the new technology, which they perceived as offering a means for collecting accurate information about working hours, thereby improving strategic decision-making. The technology enabled the home care units to collect detailed information about the work on a daily basis and in a partially automated manner, for example, by registering the visits and service delivery. This information could then be automatically transmitted to political and administrative decision makers who could use the data to make strategic decisions (e.g. on the number of employees or adjustment of service levels). 49 Despite this progress, however, it was not possible for the City to identify efficiency gains which can be traced to the introduction of mobile IT. Instead, the budget was exceeded several times during the implementation process, for example, due to technical problems and the PDAs having a shorter lifespan than expected. 49
Moreover, this case represents an example on how different social worlds collide. While managers had a predominantly positive view of mobile IT use and presented mobile IT use as a success, 60 the perceptions among the care workers and nurses were more mixed. Some workers experienced technical problems while using the technology and reacted critically to how the technology was used for managerial control. As expressed by one care worker, ‘I feel as Big Brother is watching’. Others remained critical because the technology apparently did some work task more challenging: ‘It’s difficult to write in the system. It’s much easier to write on paper and then give the paper to our group leader’. And some workers did not follow the guidelines from managers when using the technology. ‘I write down the delivered hours and services on paper … then I register the time later in the system’. However, other workers found that the use of mobile IT indeed improved their work as they could now ‘go about their work much quicker’. Some even emphasized how the technology made their work appear advanced and/or more professional in the eyes of their clients: ‘I often use the PDA when I’m with clients. They think it’s a cool technology’.
Our care worker surveys also demonstrate these diverse views regarding mobile IT use (Table 3). Interestingly, the care workers do not seem to lack the skills to use the technology – the majority find the technology easy to use (76% strongly agree or agree). Yet PDA use seems to increase control (61% strongly agree or agree), only 6 per cent agree that PDA use ensures a less stressful working day, and 72 per cent agree that technical difficulties hinder use. Overall, the care workers remained divided towards mobile IT use. In 2008, 52 per cent preferred mobile IT, 40 per cent wished to return to the previous system, and the remaining 8 per cent could not decide (Table 4).
Care worker experience of PDA usage (%, 2008).
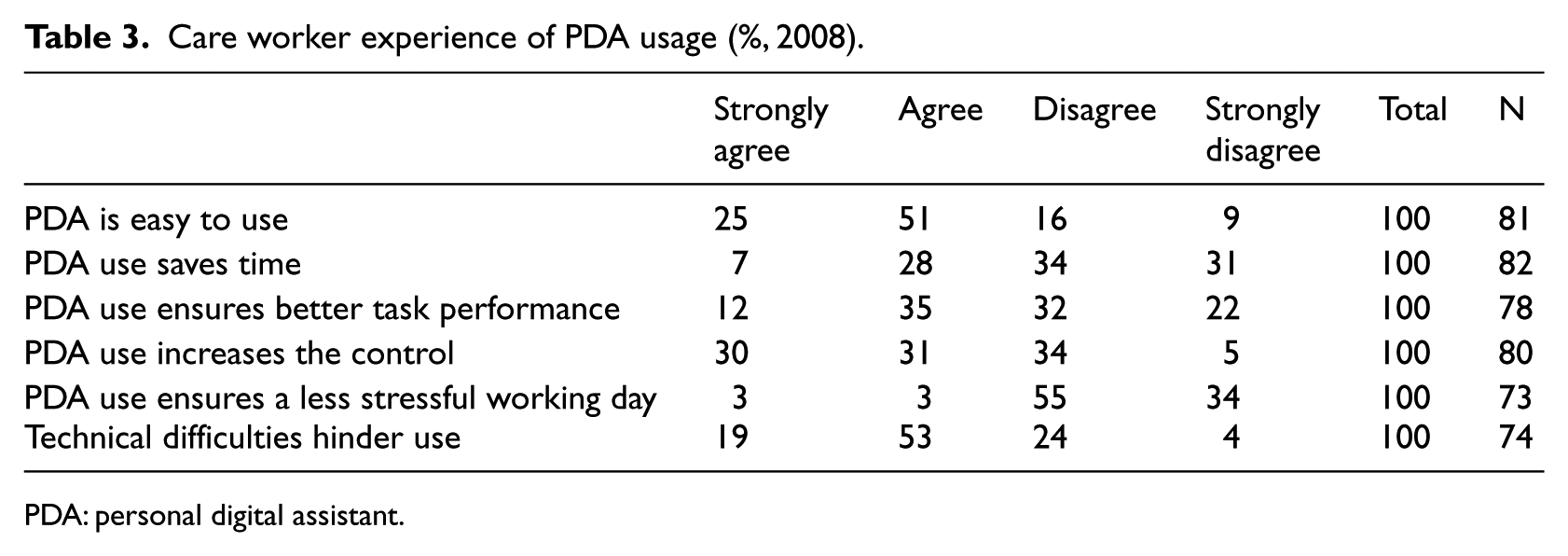
PDA: personal digital assistant.
Care workers’ preferences towards current mobile IT use and previous system (%, 2008).
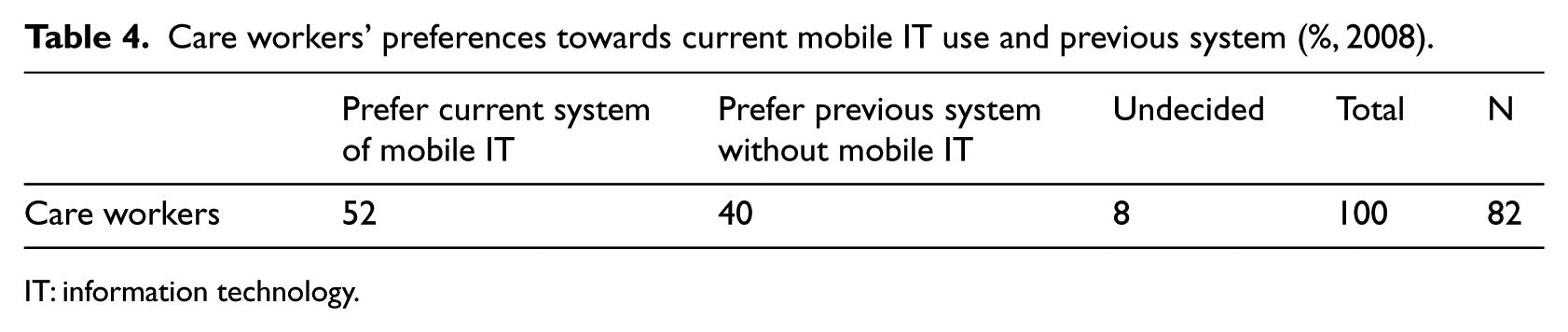
IT: information technology.
Some of the scepticism towards mobile IT is related to the experience of control and frustration with technical problems (e.g. slow transfer rates between the PDA and back-office systems). However, there also seems to be other explanations. Chau and Turner’s 8 study of mobile technology use in the Australian healthcare sector emphasized that employees’ scepticism may very well be rooted in a basic resistance to change. It also seems evident in the present case. The interviews indicate that some employees made a virtue out of criticizing the new technology. Care workers tell about situations in which applause followed in home care units when the new technology system had breakdowns, and the managers again handed out paper.
Overall, we identified tension between the interest of management in managing and controlling as opposed to considerations for healthcare personnel autonomy. There was consensus among the interviewed actors that mobile IT use has reinforced a general trend whereby work has become more centrally controlled and more closely monitored. In this sense, mobile IT, or more precisely the use arrangement afforded by the technology, illustrates tension between the managerial world and the professional world. In fact, mobile IT did not serve as a negotiable platform between managerial and professional interests. Rather, managerial intentions (e.g. time management) conflicted with professional norms and values (e.g. client-centered autonomy).
Discussion
In practice and research alike, the diffusion and adoption of mobile IT in health care has evolved into an increasingly significant area of interest. 5 This article contributes to this emerging research domain by using notions of social worlds, trajectories, and boundary objects and applying these constructs in an empirical investigation in Danish elderly home care. Our discussion therefore focuses on two key issues: to what extent different interests among multiple social worlds have been negotiated in the trajectory of adopting and diffusing mobile IT and to what extent boundary objects have aligned the interests of stakeholders from different social worlds.
When studying the trajectories of adopting and diffusing technologies (e.g. mobile IT) in complex organizational settings (e.g. elderly home care services), it is necessary to consider how actors work together to shape this process. 29 Our analysis revealed that not only organizational decision making but also the sociopolitical environment shaped the diffusion of mobile IT. In fact, the diffusion process was heavily supported by key stakeholders in the sociopolitical environment, most prominently the Danish government agencies as they financially sponsored its adoption. The vital momentum for the hasty diffusion of mobile IT in home care started in 2002 when the central government launched a pilot project (CareMobile). At this time, mobile IT use gained a place on the national policy agenda and attracted powerful stakeholders from different social worlds.
CareMobile served as an influential boundary object between different social worlds. Although this boundary spanning was infused with negotiation and compromises, it eventually became a key factor in justifying mobile IT diffusion and adoption. The CareMobile project was not only initiated by government agencies but also involved other prominent stakeholders such as technological suppliers and municipalities. While the different stakeholders all promoted and supported the national initiative (CareMobile), the stakeholders also promoted their own internal interests and agendas. Yet these different interests have been mediated due to the flexibility of the boundary object (CareMobile) in accommodating different interpretations or interests emanating from various social worlds, and yet it is robust enough to maintain a common identity across all social contexts, thus allowing translation to take place across the boundary of different worlds. For example, three powerful national actors (the Ministry of Social Affairs, LGDK, and the Ministry of Finance) have implicitly pursued their own agendas while simultaneously attempting to persuade other actors to align their interests towards the adoption of mobile IT in the home care sector. Despite the different interests, effective alignment of interests was established in the final evaluation of the CareMobile project. To this end, even controversial issues (such as the control and monitoring) and other criticisms linked to technical problems, implementation difficulties were deliberately downplayed. This finding also indicates that different stakeholders have different capacities to alter trajectories at different levels. For example, our analysis demonstrated the significance of the role of the Ministry of Finance in determining the course of adoption. Although most of the stakeholders acknowledged the common target – the adoption of mobile IT – the trajectories and approaches taken to that target were somewhat diverse.
Turning to the organizational context in which mobile IT was applied, other social worlds (including managers and care workers) played a more significant role in shaping the trajectories of adopting and implementing the technology. In the City of Copenhagen, mobile IT became subject to new and conflicting interests, demands, and pressures. As our data illustrates, there were tensions with respect to how the technology was perceived and how it implicated work performances by the different social worlds, mainly from the social worlds of home care mangers and care workers. Home care managers generally consider the adoption of mobile IT to be a positive initiative with many potential benefits. In fact, home care managers shared their ideas as to what was beneficial with those important stakeholders outside the organization. To this end, they demanded the immediate adoption of the technology throughout the organization.
The healthcare personnel, on the contrary, displayed mixed interests. Some care workers recognized that the use of mobile IT had improved their work. However, there were substantial number of care workers with negative attitudes towards the technology. Some care workers even perceived the adoption of the technology merely as a tool for managerial control as opposed to a tool for improving their work performance. As a result, mobile IT in practice did not serve as a boundary object to bridge the different interests among managers and care workers. Our findings of managers and care workers attaching different meanings towards the nature of the technology is in line with Gal et al.’s
36
argument of how IT artefacts create social identities across different social worlds and communities. They suggest that IT should be understood not only as objects that can enter an organisation and change it in any number of ways, but also as an artefact that is used by diverse actors and groups who attach different meanings to it and construct different identities in relation to it.
36
(p. 205)
This observation stands in contrast to the traditional view on the diffusion of innovation, which characterizes an innovation as an object that can diffuse among its users in a linear and unproblematic fashion. Instead, our empirical evidence shows that technological artefacts (such as mobile IT) are always in the making and evolve while traversing to new social worlds, as the enrolment of new actors changes the meaning of the technology itself over time.
Conclusion and implications
Our analysis of the trajectories of actions and interaction among stakeholders from multiple social worlds shows that there are a number of key issues to be taken into account when implementing innovative technologies such as mobile IT in complex organizational settings in the health sector. Primarily, we recognize that the adoption and diffusion of mobile IT in health care has been investigated and presented to the literature by several scholars (e.g. Zhang et al., 7 Chau and Turner, 8 Hong et al., 17 and Vishwanath et al. 18 ). However, the trajectories of adopting and diffusing mobile IT with coalitions of diverse social worlds and their representatives that are involved in managing and executing the adoption and diffusion process have not been explored in depth. Most mobile IT adoption studies in the healthcare domain have primarily focused on individuals and organizations as the unit of analysis. However, we illustrate how crucial it is to understand how key activities not only take place within healthcare organizations, where the new technology is materialized, but equally importantly are shaped within the broader sociopolitical environment of suppliers, interest organizations, and government agencies. 61 The contribution of this article, therefore, lies in the exploration of the dynamic trajectories of interaction and negotiation among different social worlds in the process of adopting and diffusing mobile IT.
We believe that the theoretical framework we have adopted in this article provides a promising analytical lens for understanding the complex dynamics of adapting and diffusing mobile-based IT innovations in a context characterized by diverse stakeholders with competing interests and values. By taking a social world perspective, we show how mobile IT facilitates and mediates negotiations and collaboration among stakeholders at once and becomes the source of tension and conflicts at other times within and between different social worlds in the context of elderly home care. For example, even in the same setting, the managers and care workers revealed completely different interpretations of the value and potentials of the technology.
This study also provides important practical insights. One important issue has to do with the necessity to involve end users in the design and implementation of IT innovations. End-user involvement in the design and implementation of IT-based systems has been considered to be an important determinant of the eventual success of any information system (see for example, Mumford and Weir, 62 Franz and Robey 63 ). User participation is more of a bottom-up approach that promotes the empowerment and involvement of intended users in the design, development, and implementation of IT-based systems in organizations. However, our findings revealed that the implementation of mobile IT at the organizational level was more of a top-down approach where especially managers endorsed its adoption and implementation. As a result, the process seems to lack end-user participation to ensure that the system will improve work performance and increase efficiency. As Vimarlund et al. 46 pointed out, ‘allowing end users to participate and to identify requirements helps to ensure that the system will promote, rather than interfere with, important aspects of home healthcare practice’ (p. 207). Besides, as the end users have better knowledge of the work processes, their involvement brings new insights in customizing the technology to fit to local requirements. As such, this article acknowledges the importance of adopting a bottom-up participatory approach that empowers the intended users of the system in adopting and implementing new technologies in different organizational settings. Such an approach could enhance the long-term viability and sustainability of the new system by reducing possible user resistance as we have observed in our case study.
Our research is not without limitations. Drawing on a single case limits our ability to conduct cross-case comparisons and account for institutional variations. 64 Future studies may apply multiple case study designs to validate our findings and further develop the proposed notion of social worlds related to the diffusion and adoption of healthcare IT innovations, such as mobile ITs. Another limitation has to do with the data we have collected for our study. Although drawing on a variety of data sources (Table 1), our study would have benefitted from field observations as a means of understanding the diffusion and adoption of mobile IT in practice. Future studies may therefore include ethnographic methods to further our understanding of how negotiations, interactions, and boundary objects unfold in diffusion and adoption processes.
Footnotes
Appendix
Sources of inspiration for mobile IT adoption.
| Source of inspiration a | The number of municipalities indicating that this source was a primary inspiration |
|---|---|
| IT suppliers | 29 |
| Other municipalities | 28 |
| CareMobile | 25 |
| From ‘old’ municipalities (in amalgamated municipalities) | 10 |
| Professional networks and conferences | 6 |
| Consulting firms | 3 |
| LGDK | 3 |
| Media | 1 |
| Other | 9 |
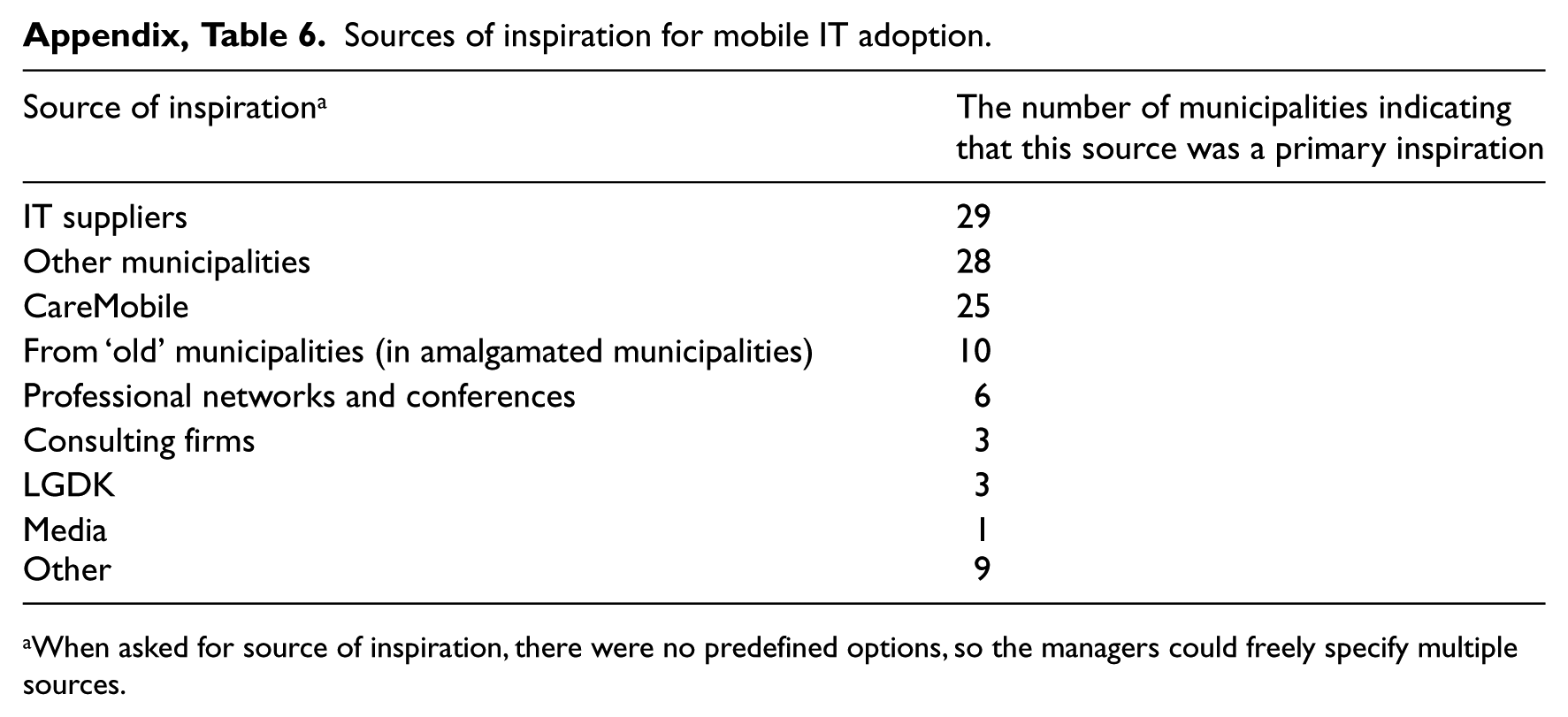
When asked for source of inspiration, there were no predefined options, so the managers could freely specify multiple sources.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.