
Abstract
Mobile physical activity interventions can be improved by incorporating behavioural change theories. Relations between self-efficacy, stage of change, and physical activity are investigated, enabling development of feedback strategies that can be used to improve their effectiveness. A total of 325 healthy control participants and 82 patients wore an activity monitor. Participants completed a self-efficacy or stage of change questionnaire. Results show that higher self-efficacy is related to higher activity levels. Patients are less active than healthy controls and show a larger drop in physical activity over the day. Patients in the maintenance stage of change are more active than patients in lower stages of change, but show an equally large drop in level of physical activity. Findings suggest that coaching should at least be tailored to level of self-efficacy, stage of change, and physical activity pattern. Tailored coaching strategies are developed, which suggest that increasing self-efficacy of users is most important. Guidelines are provided.
Introduction
A physically active lifestyle has significant positive effects on mental health condition 1 and prevention of chronic diseases such as cardiovascular disease, diabetes, and cancer. 2 A recent development regarding physical activity interventions is using mobile applications to achieve behavioural change. Many applications allow for tracking and scheduling of exercise, while only few applications aim at tracking physical activity over the day. Those that are available typically use an external sensor next to a smartphone, like Fitbit 3 and Samsung Gear Fit. 4 These types of services seem promising in the short-term. 5 However, the effectiveness can be further improved.
Traditional, non-mobile physical activity interventions that aim to improve level of physical activity in the general population,6,7 frequently personalize, or tailor feedback based on theories and models from behavioural sciences to increase effectiveness and even optimize adherence to the intervention. 8 This specific type of tailoring – personalization of information or feedback based on an individual’s score on constructs from behavioural sciences – is called adaptation. 9 Whereas traditional interventions frequently use adaptation of feedback, this is rarely applied in modern-day, mobile physical activity applications. 10
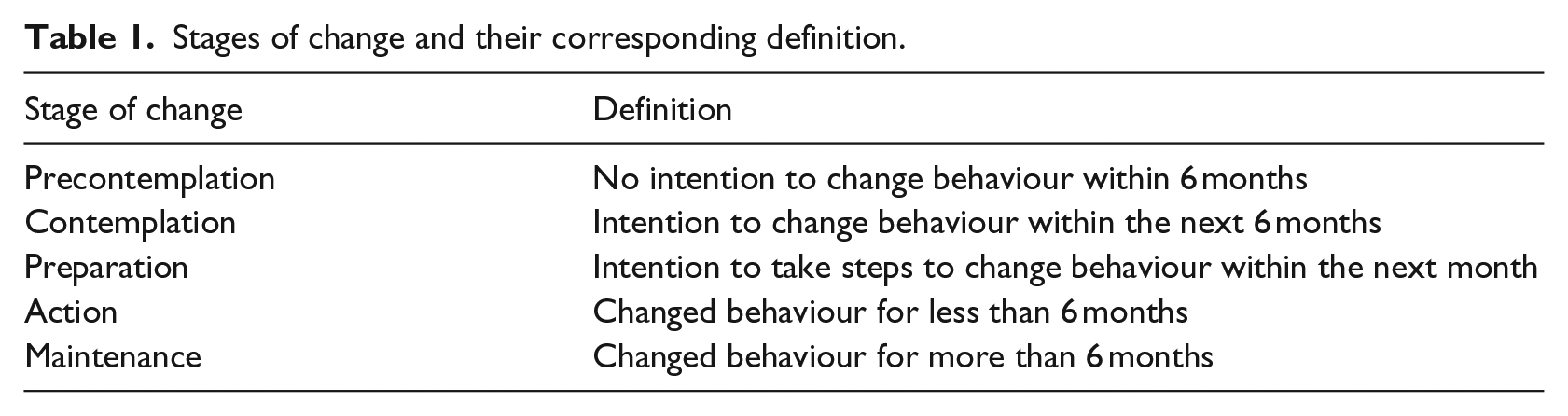
A source for identifying how to apply adaptation is social cognition models (SCMs). These define the cognitive factors that underlie social patterns of behaviour. Three well-known examples are the social cognitive theory (SCT), theory of planned behaviour (TPB), and transtheoretical model (TTM). 8 The SCT assumes that motivation and action are influenced by forethought. 11 It describes three types of expectancies: situation outcome expectancy, action outcome expectancy, and perceived self-efficacy. It states that personal sense of control makes it possible to change behaviour; if people believe they can take action to accomplish a certain goal, they become more inclined to do so and feel more committed to the decision. The TPB states that behaviour is preceded by intentions, that is, motivation or plans to exert effort to perform behaviour. 12 Intentions are constituted by attitudes, subjective norms, and perceived behavioural control. By influencing the various beliefs properly, behaviour can be changed and maintained. Finally, the TTM assumes changing behaviour requires progress through five stages (Table 1) and different cognitions may be of importance at different stages. 13 The stages can be entered and exited at any point and it is possible to relapse to an earlier stage. Next to these stages, the model includes several other constructs: a decisional balance (benefits versus costs), self-efficacy (confidence that one can engage in healthy behaviour; temptation to engage in unhealthy behaviour) and processes of change (activities that people engage in to progress through the stages).
Stages of change and their corresponding definition.
Indeed, research shows that traditional interventions that use adaptation based on constructs from SCMs, like attitudes, self-efficacy, stage of change, social support or processes of change, showed significantly larger effect sizes than interventions that did not tailor on these constructs.9,13,14 In addition, guidelines for designing effective physical activity interventions strongly recommend tailoring feedback.6,15 Furthermore, O’Reilly and Spruijt-Metz 16 conclude a systematic review by stating that with respect to using technology for assessment and promotion of physical activity, more research is needed on the effectiveness of interventions that combine real-time, tailored, and adaptive feedback.
Primary objective
It is hypothesized that implementing knowledge from behavioural sciences into modern-day, mobile physical activity applications can further improve their effectiveness, just as in traditional interventions. As such, the aim of this study is to investigate (1) the relation between self-efficacy and objectively measured level of physical activity; (2) the relation between stage of change and objectively measured level of physical activity; and (3) compare level of physical activity between patients and healthy adults.
Secondary objective
Based on the results typical users, that is, personas, will be identified. Tailored feedback strategies will be developed for these personas, which can be used to improve the effectiveness of mobile physical activity coaches in the future. The reason for choosing self-efficacy and stage of change is that these are two aspects which are of central importance in most SCMs and common in traditional interventions.
Method
Data were available for secondary analysis from previous studies performed from 2008 to 2011.17,18 Data about stage of change, level of self-efficacy, and objectively measured physical activity were collected, but not used in any way during and after completion of these studies.
Participants
Data of 407 participants were analysed of which 82 were patients diagnosed with one of the following conditions: chronic obstructive pulmonary disease (COPD) (n = 39), chronic low back pain (CLBP) (n = 20), or cancer (n = 23). All of these patients were grouped together, as the literature shows comparable physical activity data of the separate groups.17,18 The patient group consisted of 43 women and 39 men, averaging 60 years of age (standard deviation (SD) = 12). The healthy group consisted of 149 women and 176 men. All participants signed an informed consent. A local ethics committee reviewed and approved the study.
Equipment
Two types of mobile activity monitoring system were used: the Activity Coach (AC; see Figure 1)5,17,18 and a Commercial Activity Monitoring Device (CAMD). The AC was worn by 139 participants (82 patients and 57 healthy controls (AC control participants)). The CAMD was worn by 268 healthy controls (CAMD control participants).

Activity Coach.
The AC consists of a sensor (MTx-w) and a smartphone (HTC). The sensor includes a tri-axial accelerometer which is used to measure physical activity. It is worm on the hip and sends data to the smartphone through a Bluetooth® connection. Op den Akker et al. 19 provide a complete description of the system.
The CAMD consists of a tri-axial accelerometer. The dimensions of the device are approximately 3 by 3 by 1 cm. Users can wear the device in their pocket, on their belt, or as a necklace.
Procedure
Participants wore the AC the entire day, for seven consecutive days. The goal here was to obtain a baseline measurement of the users’ level of physical activity. They did not receive any kind of feedback during these 7 days; only physical activity was measured throughout the day. Additionally, patients were asked to complete a questionnaire assessing their stage of change 13 and working status at the beginning of the experiment.
Participants using the CAMD completed a questionnaire assessing level of self-efficacy regarding physical activity at the start of the experiment. 20 Low, average, and high levels of self-efficacy corresponded to scores of 5 through 12, 13 through 17 and 18 through 25, respectively. Hereafter, participants wore the device the entire day, for 3 weeks, to obtain a baseline measurement of their level of physical activity. They did not receive any kind of feedback during these 3 weeks; only physical activity was measured throughout the day.
Data analysis
The accelerometer of the AC calculates activity counts per minute (CPM) as output which was processed in MATLAB to gain insight in the level of physical activity and physical activity pattern. Level of physical activity was defined as the average amount of Integral of the Modulus of the Accelerometer (IMA) counts per minute per day. A day was considered a valid measurement day if data are collected for 50% of an hour for at least 6 h per day. Furthermore, every day part should contain at least 2 h of valid data. The day parts were defined as morning (08:00 a.m.–13:00 p.m.), afternoon (13:00 p.m.–17:00 p.m.), and evening (17:00 p.m.–22:00 p.m.). The averages of IMA counts per minute per day part were calculated to investigate differences in physical activity patterns over the day.
The CAMD calculates a ratio between calorie expenditure and basic metabolism, based on age, length, weight, and sex, to estimate level of physical activity. It uses PAL as output measure, which has a minimum of 1.1. If participants show a PAL of 1.7 or above, they are considered active. The exact calculation cannot be disclosed, since the CAMD is commercially available.
Statistical analysis
The correlation between age and level of physical activity was calculated and an analysis of variance (ANOVA) was performed to examine differences between sexes regarding level of physical activity and the effect of working status on level of physical activity to identify possible confounding factors. The latter only investigated this effect for the patient group, since data regarding working status were not available for the AC control group. Patients were classified as unemployed (less than 12 h of work per week), part-time (between 12 and 36 h of work per week), or full-time (more than 36 h of work per week).
A univariate ANOVA was performed to test the difference between the level of physical activity of patients and AC control participants. With respect to the patient group, the difference in level of physical activity per stage of change was analysed using an ANOVA. Furthermore, the level of physical activity of patients per stage of change was compared to the level of physical activity of AC control participants.
Repeated measures-MANOVA was executed to analyse level of physical activity per day part (morning, afternoon, evening); testing differences in patterns between patients and AC controls, and between patients per stage of change. An ANOVA was performed to test whether CAMD control participants with different levels of self-efficacy (low, average, high) show different levels of physical activity.
Results
Results regarding the AC
The results show no significant correlation between age and average daily level of physical activity for neither the patient group (r = −.107, p = .356) nor the AC control group (r = .170, p = .21). The ANOVA indicates no significant difference in level of physical activity between sexes in the AC control group (F(1, 55) = 1.99, p = .164) or in the patient group (F(1, 75) = 3.34, p = .072). Regarding working status, 56 patients were unemployed, 11 had a part-time job, and 10 worked full-time. No significant difference in level of physical activity was found between working status (F(2, 74) = 1.75, p = .182). Based on these results, it can be assumed that level of physical activity was not influenced by age, sex, or working status in the current study.
The univariate ANOVA shows that patients (mean IMA = 947.77) are significantly less active than AC controls (mean IMA = 1089.6) (F(1, 132) = 8.58, p = .004). Within the patient group, there is a significant difference in level of physical activity per stage of change (F(3, 72) = 4.00, p = .011) (Figure 2). Patients in the contemplation, preparation, and action stage of change are significantly less active than patients in the maintenance stage of change (β = −197.69 (t = −1.99, p = .051); β = −215,69 (t = −3.03, p = .003); and β = −221.67 (t = −2.01, p = .048), respectively).
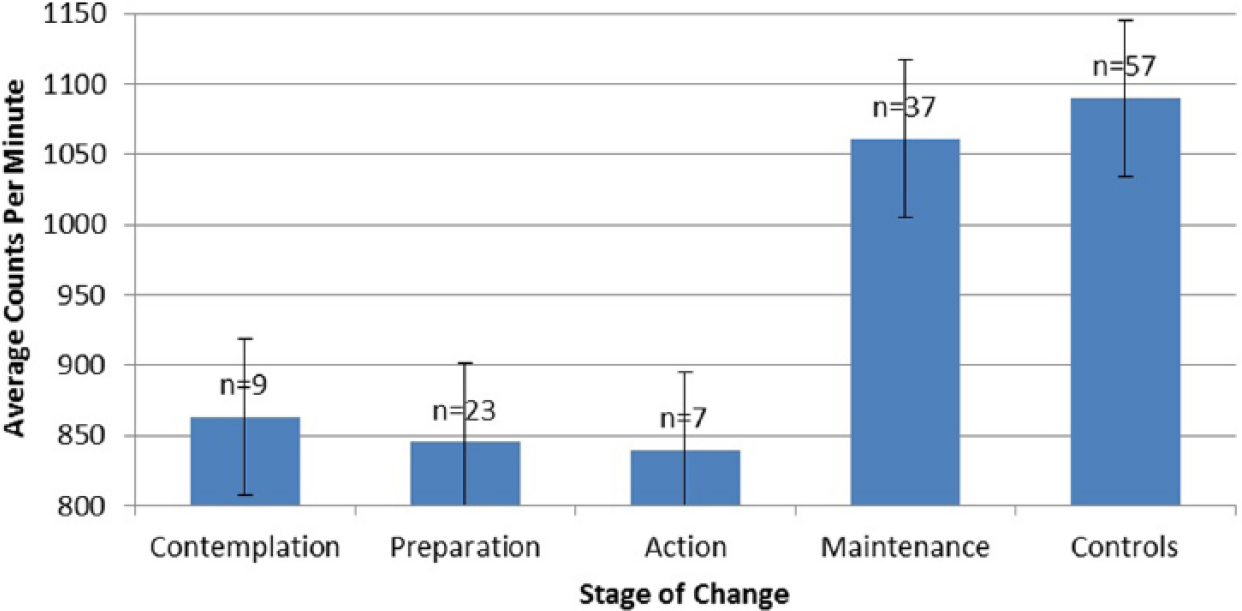
Average CPM per stage of change for patients compared to the average CPM of AC control subjects.
Results also show a significant difference in level of physical activity between patients per stage of change and control participants (F(4, 128) = 5.15, p = .001). Contrasts show that patients in the contemplation, preparation and action stage of change are less active than AC controls (β = −226.17 (t = −2.35, p = .020); β = −244,26 (t = −3.69, p < .001); and β = −250.25 (t = −2.33, p = .021), respectively). No significant difference was found in level of physical activity between patients in the maintenance stage of change and AC control participants (β = −28.58 (t = −.51, p = .61)) (Figure 2).
Regarding physical activity pattern, the repeated-measures-MANOVA shows a significant difference in activity per day part (W = .77, p < .001) (GG: F(1.63, 198.77) = 28.57, p < .001); physical activity over the day of all participants combined shows a quadratic trend from morning to evening (F(1, 122) = 11.93, p = .001). The interaction effect between activity per day part and group (patient/AC control) is significant (GG: F(1.63, 198.77) = 9.45, p < .001), indicating the difference per day part is different for patients than for AC controls. Figure 3 shows that the decline in level of physical activity over the day is much steeper for patients than for AC controls; they are as active as AC controls in the morning (β = 13.042 (t = .17, p = .865)), but whereas AC controls show an increase of physical activity in the afternoon, patients show a decrease (β = −191,489 (t = −3.27, p = .001), and an even steeper decrease than AC controls in the evening (β = −287.064 (t = −4.95, p < .001)).
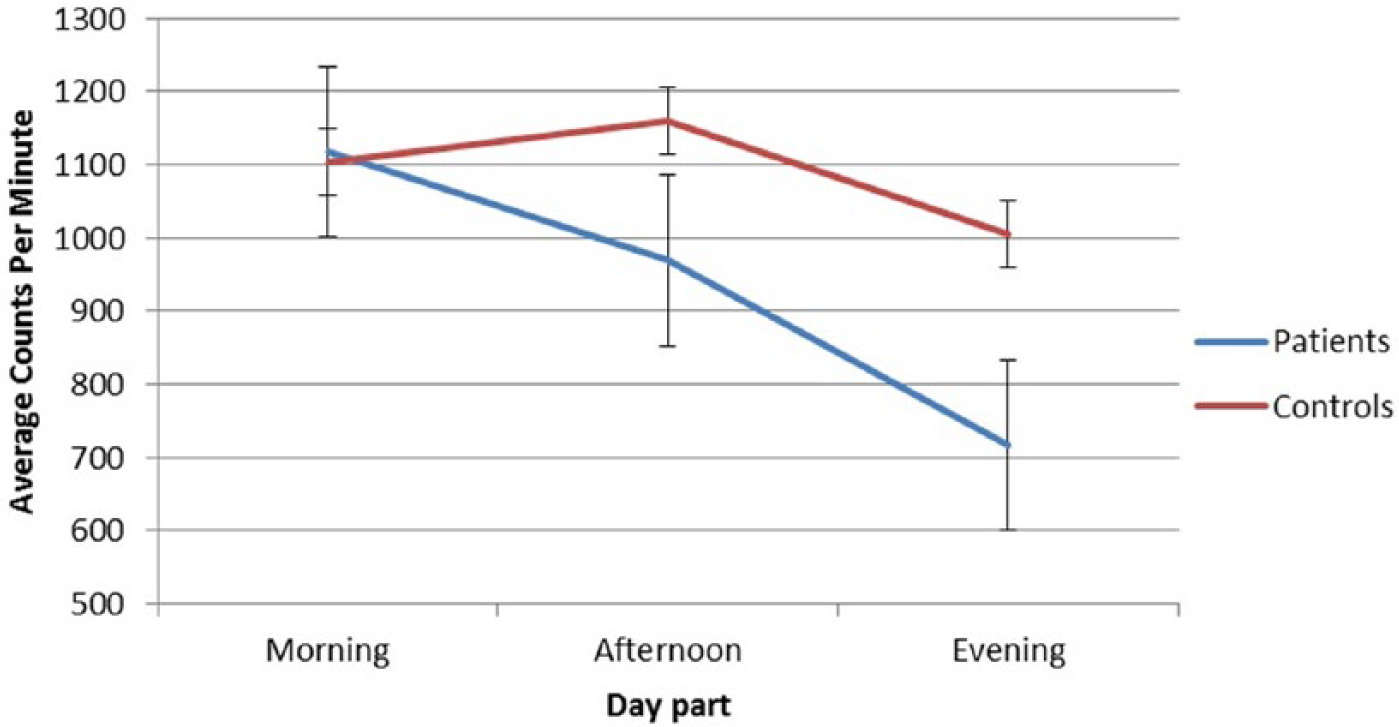
Average CPM per day part for patients and AC control subjects.
With respect to the group of patients, the difference in activity per day part is not different per stage of change (W = .700, p < .001) (GG: F(4.61, 95.35) = 1.15, p = .34). To provide an overview, Figure 4 shows the level of physical activity per day part for patients per stage of change as compared to the level of physical activity per day part of AC control participants. Whereas AC control participants show a small drop in level of physical activity over the day, all patients show the same pattern of high decline in level of physical activity from morning till evening, regardless of the participant’s stage of change.
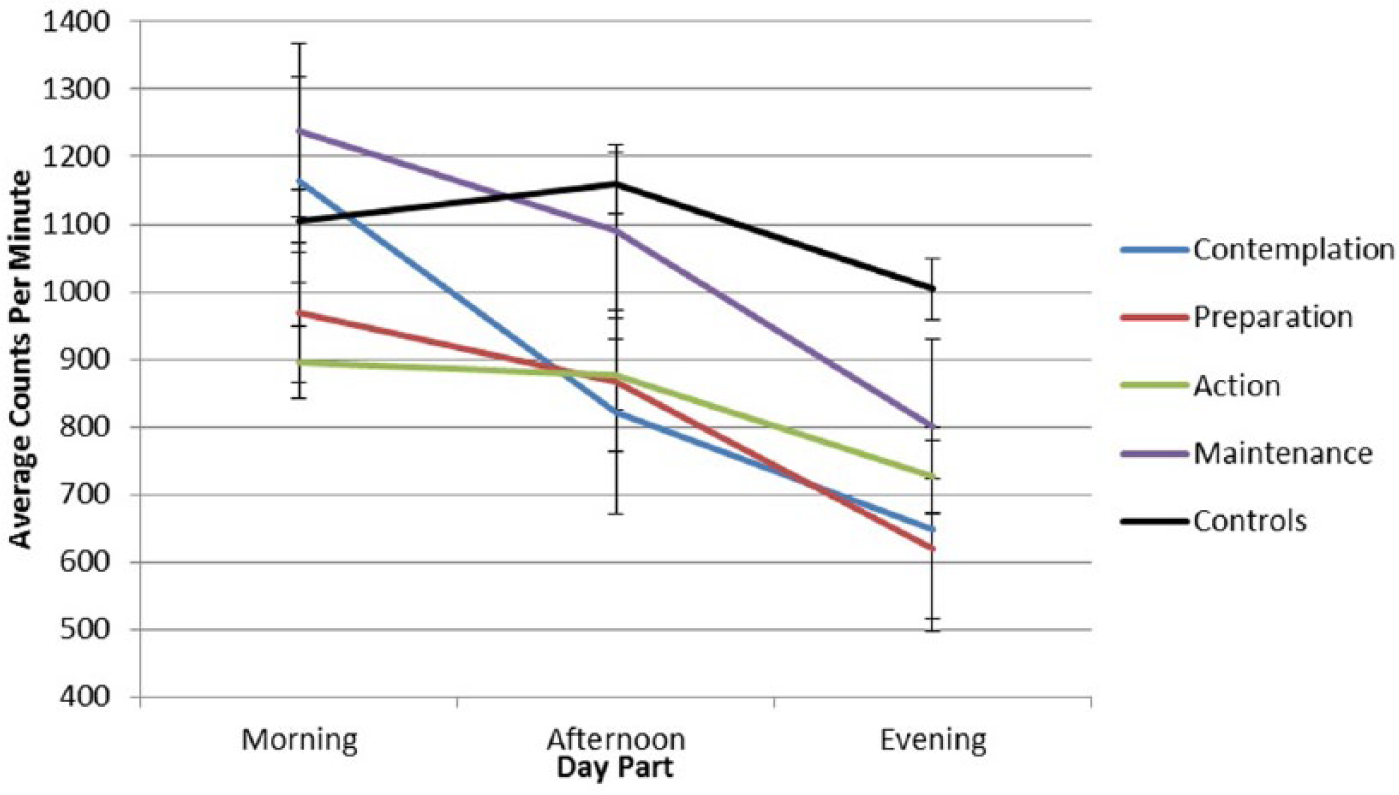
Average CPM per day part for patients per stage of change as compared to AC control subjects.
Results regarding the CAMD
With respect to the CAMD and the relationship between self-efficacy and physical activity, sex was added to the model as a fixed factor, as the ANOVA showed a significant difference in level of physical activity between sexes (F(1, 266) = 6.55, p = .011); men (mean PAL = 1.657; SD = .133) are more active than women (mean PAL = 1.616; SD = .124).
Most CAMD participants were classified as having an average level of self-efficacy regarding physical activity (n = 144), 60 participants reported a high level of self-efficacy and 55 participants indicated a low level of self-efficacy. The test shows a significant difference in level of physical activity per category of self-efficacy (F(2, 253) = 8.69, p < .001). The interaction effect with sex is not significant. Contrasts indicate that participants with a low or average level of self-efficacy are significantly less active than participants with a high level of self-efficacy (β = −.080 (t = −2.07, p = .039) and β = −0.090 (t = −2.70, p = .007), respectively) (Figure 5).
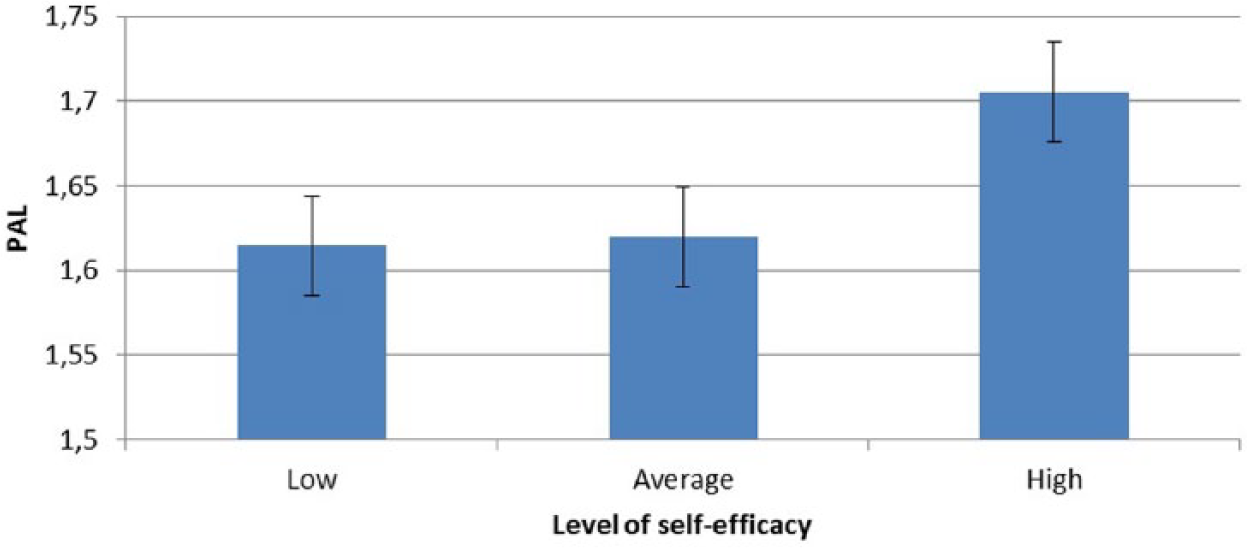
Average level of physical activity per category of self-efficacy.
Discussion
The primary aim of this study was to investigate (1) the relation between self-efficacy and objectively measured level of physical activity, (2) the relation between stage of change and objectively measured level of physical activity, and (3) compare level of physical activity between patients and healthy adults, in mobile physical activity interventions. Secondary, based on the results, typical users were identified and corresponding tailored feedback strategies were developed. Results show that the three factors are significantly related to objectively measured physical activity: self-efficacy, stage of change and being healthy or suffering from a disease.
With respect to self-efficacy, higher levels of self-efficacy are related to higher levels of physical activity. The more participants believe that being sufficiently physically active is within their control, the higher their level of physical activity. These findings are consistent with traditional physical activity research, which shows that participants who have not started to exercise regularly show low levels of self-efficacy, whereas those who have started show high levels of self-efficacy. 21
Having a chronic disease also influences level of physical activity. Patients are less active and show a steeper decline in level of physical activity over the day than healthy participants. Research suggests that patients tend to do all must-tasks (e.g. cleaning, groceries) in the morning, leaving them with little energy to do social and fun activities in the evening.5,17
With respect to stage of change, patients in the maintenance stage of change are more active than patients in other stages of change; they are as active as healthy participants. However, patients in the maintenance stage of change show an equally large drop in level of physical activity over the day as other patients and, as such, have an improper activity pattern.
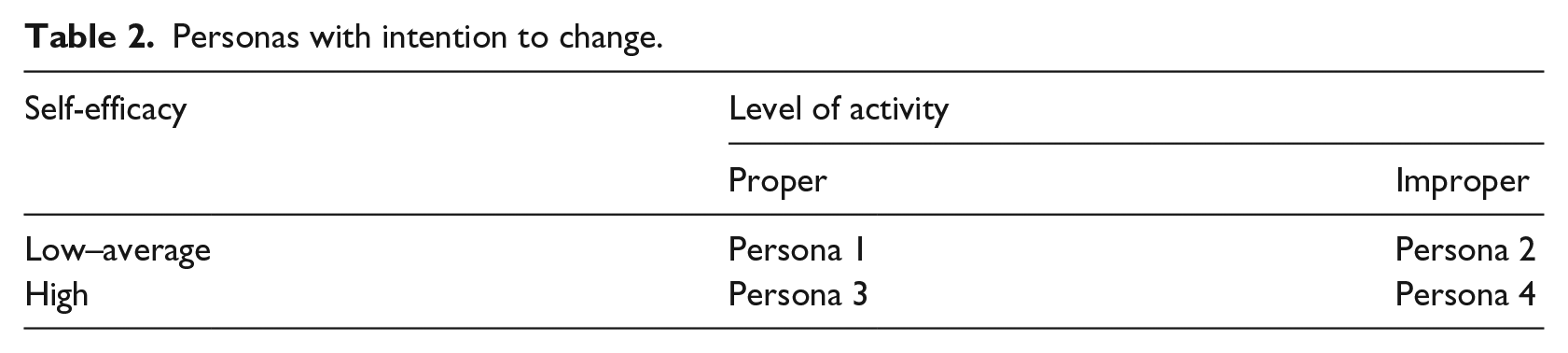
Based on these results, participants can be categorized into eight typical personas, who should receive different coaching strategies based upon the three important variables stage of change, self-efficacy and level of physical activity (Tables 2 and 3).
Personas with intention to change.
Personas without intention to change.
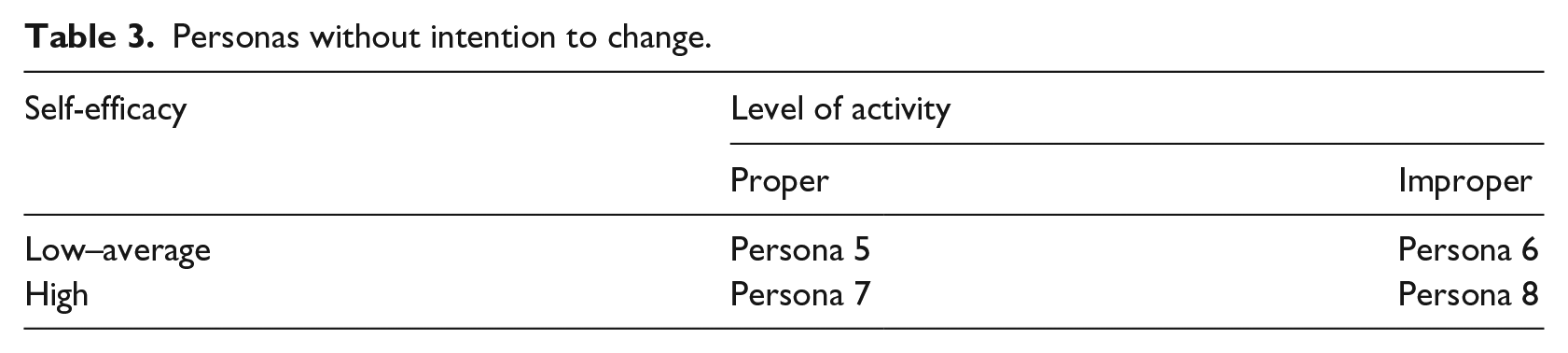
Based on stage of change, participants can be categorizes as either having (contemplation, preparation, action) or not having (precontemplation, maintenance) an intention to change behaviour. Based on the activity pattern, participants can show a proper or improper level of physical activity. A proper level of physical activity means sufficient physical activity and a balanced physical activity pattern; improper indicates insufficient physical activity or an imbalanced pattern. Regarding self-efficacy, participants can be categorized as having ‘low to average’ or ‘high’ self-efficacy. Low and average levels of self-efficacy were taken together, as these participants did not show differences in level of physical activity. Ideally, scores on these constructs should be assessed regularly to identify whether they are still categorized as the correct persona, or if they have changed to, for example, a higher level of self-efficacy, for which an adjustment of the coaching strategy is needed.
The personas described above can be used to develop corresponding feedback strategies that can be included into new mobile physical activity applications. It is clear that coaching should at least be tailored to users’ level of self-efficacy, stage of change and physical activity pattern. As high self-efficacy not only increases intention, but also leads to actual performance of the target behaviour, 22 much research has focused on how self-efficacy can be influenced and especially on how to increase it. Bandura 23 describes four sources that can be used to increase self-efficacy: mastery experience, vicarious experience, social persuasion and physiological and emotional states. Regarding personas 1, 2, 5, and 6, who have low levels of self-efficacy, mastery experience could be implemented by setting challenging but attainable, personalized goals, 24 leading to success experiences. Adding optional data sharing leads to vicarious experience and additionally sending persuasive feedback messages makes for higher exerted effort of users to achieve their goal. A meta-analysis showed that of these four strategies to increase self-efficacy, feedback on previous performance or previous performance of similar others cause the highest effect sizes, followed by vicarious experience. 25 As such, this might also be hypothesized to be the most effective strategy to include in mobile physical activity applications.
Regarding stage of change, 10 specific strategies to move from stage to stage, or processes of change, have received much attention and empirical support. 26 Five can be identified as experiential processes (increasing awareness, emotional arousal, social reappraisal, social liberation, and self-reappraisal), and the other five are referred to as behavioural processes (stimulus control, social support, counter conditioning, rewarding, committing). Experiential processes are primarily used for early stages, while behavioural processes are recommended for later stages. 23 Therefore, coaching for personas 1, 2, 3, and 4 should focus on behavioural processes of change, whereas coaching for personas 5, 6, 7, and 8 should focus on experiential processes.
The coaching strategies were implemented into the AC (Figure 1) and are currently tested in a field study. First, level of self-efficacy, stage of change and level of physical activity are assessed at baseline, after which participants are automatically identified as one of the eight personas, which determines what feedback messages they will receive during the intervention; different personas receive different feedback messages.
Conclusion
Just as traditional physical activity interventions, modern-day mobile physical activity applications should include adaptation and tailored feedback strategies into their coaching, which might lead to increased effectiveness and hopefully to even better intervention adherence, and adherence to physical activity guidelines. This is not yet known. However, this study can be regarded as first step towards testing this. It identifies personas and provides guidelines for development of feedback that takes into account individual scores on constructs from behavioural sciences. The next step is to test these findings in daily life. Additionally, there are many other factors associated with physical activity (e.g. social support, benefits, barriers, etc.), and as such, future research should investigate further adaptation and tailoring of feedback strategies in mobile physical activity interventions using knowledge from social cognition models.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
This publication was supported by the Dutch national program COMMIT (project P7 SWELL).