
Abstract
Opening and charting in the incorrect patient electronic record presents a patient safety issue. The authors investigated the prevalence of reported errors and whether efforts utilizing the anesthesia time-out and barcoding have decreased the incidence of errors in opening and charting in the patient electronic medical record in the perioperative environment. The authors queried the database for all surgeries and procedures requiring anesthesia from January 2009 to September 2012. Of the 115,760 records of anesthesia procedures identified, there were 57 instances of incorrect record opening and charting during the study period. A decreasing trend was observed for all sites combined (p < 0.0001) and at the off-site locations (p = 0.0032). All locations and the off-site locations demonstrated a statistically significant decreasing pattern of errors over time. Barcoding and the anesthesia time-out may play an important role in decreasing errors in incorrect patient record opening in the perioperative environment.
Keywords
Introduction
Electronic medical records (EMR) have changed the practice of medicine and have been associated with saving time and reducing errors as compared to paper records.1–3 Considered an improvement compared to paper records by most, efforts have been made in the United Kingdom, United States, and Canada to improve electronic health information system safety. 4 The US government incentivized healthcare organizations and physicians to implement EMR systems to improve the quality and efficiency of healthcare with the Health Information Technology for Economic and Clinical Health (HITECH) Act. 5 In addition, government regulation known as Meaningful Use will result in payment reduction for practitioners who do not show quality metrics with EMR. 6
Anesthesia information management system (AIMS) is a specialized electronic health record system that automatically collects, stores, and presents data during the perioperative period. AIMS create more comprehensive perioperative records than hand-written charts.7–9 In the United States, nearly half of the 140 academic anesthesia departments and at least 50 percent of anesthesiologists in non-academic settings surveyed were considering implementing AIMS in 2005. More recently in 2014, approximately 75 percent of academic anesthesiology departments will be using an AIMS with 84 percent adoption between 2018 and 2020.10–12 Implementation of AIMS faces several challenges including inadequate return on financial investments, lack of expertise among anesthesia providers, increasing information technology (IT) costs, and lack of IT support dedicated to AIMS. 13 Further challenges to consider include the poor integration of AIMS with hospital EMR systems, fear of inaccurate records with AIMS and associated legal implications, and lack of support from hospital administration. 11
Advantages with AIMS include a more comprehensive perioperative record, more efficient documentation than with manual methods, the ability to integrate information within a hospital system, record support that facilitates clinical research, and improved revenue capture.8,13 Furthermore, AIMS may provide decision-support logic information such as antibiotic timing and may facilitate compliance with legally required documentation. 9 Efficiency in charting may allow the anesthesia provider to provide patient-centered care rather than focus on documentation. For example, pulse rate, blood pressure, and pulse oximetry are automatically captured by AIMS rather than having an anesthesia provider manually recording these values.7,8 However, editing physiologic data remains a common practice through which the anesthesia provider may attempt to reduce the variability of intraoperative data. 7
Technology itself may also introduce “technology induced errors.” 4 One of these errors includes opening and charting in the incorrect patient record. Incorrect EMR opening and charting in the perioperative environment could have potentially harmful implications for the patient. If the wrong medical record is opened, the incorrect allergy information on the screen could lead to the patient receiving a medication for which he or she has a documented allergy. In addition, if the wrong record is accessed and charted, the patient’s surgical history will remain incorrect in the system and that could have implications for future procedures requiring anesthesia. For example, if a patient with esophageal cancer underwent an Ivor-Lewis procedure that was incorrectly charted in another patient’s EMR, future esophagogastroduodenoscopy procedures without the appropriate documented surgical history and precautions could result in aspiration and possible death. The other patient’s EMR also will have an incorrect surgery charted leaving an incorrect record.
Nevertheless, as more hospital systems adopt AIMS, errors inherent to the system, such as opening and charting in the incorrect patient record, will present a documentable patient safety issue and concern. One technology that addresses the problem of opening the wrong patient record is barcoding. Barcoding technology has been successfully implemented for transfused blood products, surgical sponge counting, and tracking of patients for routing purposes to increase patient safety.14–21
Although barcoding has been used successfully and may have been used for reducing the incidence of wrong patient records accessed, this method is not without problems. Barcoding is not error-proof, and some problems associated with it include unreadable barcodes (crinkled, smudged, torn, missing) on patient wristbands, malfunctioning scanners, failing batteries, uncertain wireless connectivity, and emergencies. 22 Some studies reported disadvantages of barcoding such as patient misidentification if the patient inadvertently received another patient’s identification bracelet or workarounds from the healthcare personnel inappropriately using the barcodes.22–24 Moreover, implementing a barcoding system within a hospital system may present challenges such as administrative acquisition costs, practice change, and process flow. 25
The anesthesia time-out (ATO) utilizing a perioperative checklist is a process that verbally confirms that the correct patient is brought into the correct location and is completed once the patient is brought into the operating room. With the patient involved in this process, the correct patient, medical record number, procedure, allergy information, and anesthetic plan are confirmed by all parties. In addition, the barcode on the patient’s medical bracelet is used to open the patient’s EMR as part of this process. A checklist is included to show the elements of the ATO. The ATO is done before any anesthetic is given to the patient and is documented in AIMS (Figure 1).
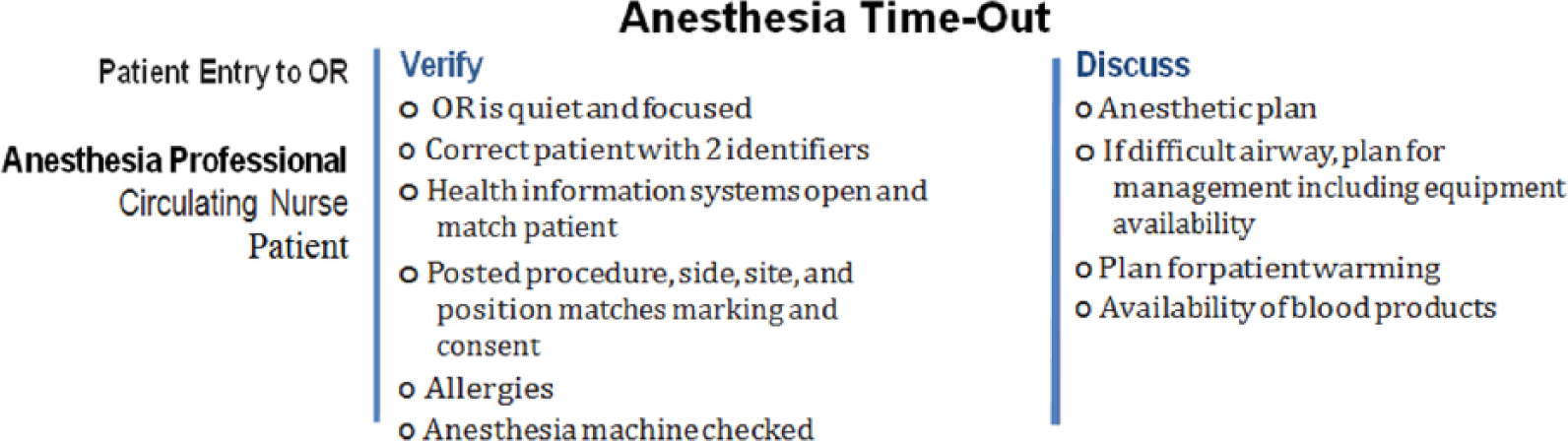
Checklist of ATO process.
To our knowledge, no studies have investigated the incidence of opening and charting in the wrong patient record either prior to or with AIMS. Such information is clearly needed to understand the scope of this problem so that the success of solutions can be accurately assessed. Therefore, we investigated the incidence of reported errors in opening the incorrect patient record in the perioperative environment by location in our practice. We then reported whether barcoding and utilizing the ATO from the perioperative checklist decreased the incidence of wrong patient records being accessed and charted over time.
Materials and methods
Our institution has over 50 separate anesthetizing locations, including 30 operating rooms in the main hospital, 6 operating rooms in the outpatient surgery center, and 15 separate off-site locations. These off-site locations consist of groups of procedures outside the operating room which require anesthesia services. These off-site locations may also be referred to as non-operation room anesthesia (NORA) locations. These off-site locations include gastroenterology endoscopy suite, cardiopulmonary suite, interventional radiology suite, magnetic resonance imaging (MRI) suite, proton therapy center, bone marrow aspiration and biopsy suite, radiotherapy treatment suite, and a suite for pediatric lumbar puncture and intrathecal chemotherapy.
In January 2002, our institution began using AIMS (Picis© and Caresuite®, Wakefield, MA) for intraoperative record keeping and has since extended the system to all anesthetizing locations. Institutional review board (Program for Protection of Human Subjects, The University of Texas MD Anderson Cancer Center, Houston, TX) approval was granted for this study. We queried our Picis and Caresuite databases for procedures performed from January 2009 to September 2012 and included all cases that had required documented anesthetic care. Barcoding patients’ identification bracelets have been incrementally integrated in our anesthetizing locations since 2007 with all areas having barcode scanners by 2011. The ATO was implemented in all locations in Quarter 1 of January 2010. We reviewed all cases requiring anesthesia services during the study period. Incorrect opening and charting was recorded by location and time to calculate an error rate. Incorrect record opening was determined from two sources: IT group and Billing Compliance. The anesthesia team realizes incorrect record opening and charting and informs IT to correct the error. Billing Compliance does a daily reconciliation with the surgical cases. We determined that an incorrect record had been accessed and charted from an analysis of the database for all cases requiring anesthesia services from our Perioperative and Critical Care Informatics group. We also had our billing department complete a daily reconciliation for every case that involves anesthesia services.
Statistical analysis
Descriptive statistics such as frequency and proportion were calculated for case type (scheduled, add-on) and location. The number of errors detected is very small; therefore, logarithmic functions are used. The percentage of error was calculated and plotted quarterly. The chi-square test was used to determine the similarity in the proportions of errors across all quarters. A linear model was assumed as a function of time to investigate the existence of a decreasing trend in the percentages of errors. The type III sum of squares from the F-test was used to determine the trend with time. The percentage of errors decreased exponentially with time. Therefore, a logarithmic transformation was used. A p value < 0.05 was considered statistically significant. All analyses were performed using software SAS 9.2 (SAS Institute Inc., Cary, NC), R 2.14.1 (Comprehensive R Archive Network, R Foundation for Statistical Computing, Vienna, Austria), and S-PLUS 8.0 (TIBCO Software Inc., Palo Alto, CA).
Results
Among 115,760 records of anesthesia procedures identified by our database search, we found 57 instances of incorrect record openings during the study period. Among the 57 incorrect records accessed, 49 cases were scheduled cases, 4 were add-on cases, and 4 did not have a date or a location identified. In terms of location, 10 errors occurred in the operating room and 43 incorrect records accessed were of patients who had procedures in off-site locations (Table 1).
Cases which were accessed and charted in error by location.
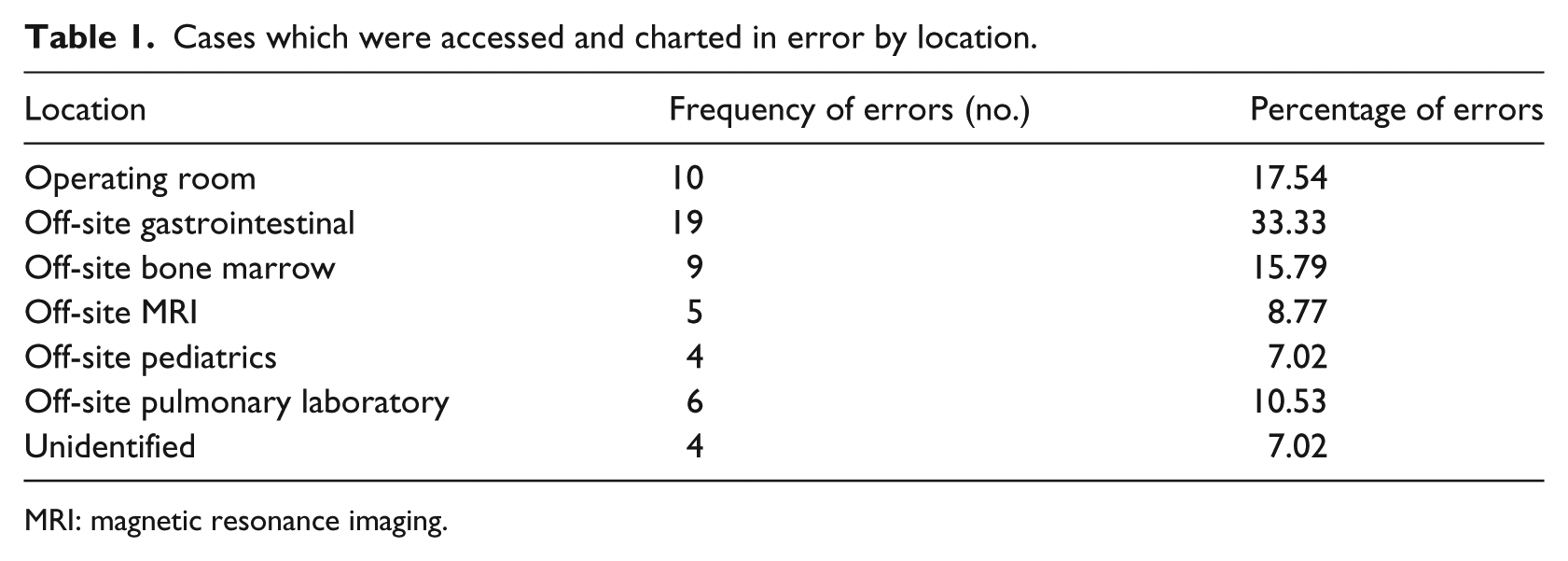
MRI: magnetic resonance imaging.
There is a significant decrease in incorrect records being accessed and charted over time in all locations (Figure 2). Quarters 9 and 12 had zero errors. Log 0 is always undefined, therefore ignored in the graphs. When further examining the decrease in wrong records accessed by anesthesia facility location, the trend did not show a decrease in wrong records accessed over time in the operating rooms (p = 0.2632); however, a significant decrease over time was seen in the off-site locations (Figure 3). Most instances of incorrect records accessed and charted (75%) occurred at off-site locations, which were subcategorized by specific location. The highest incidence of the wrong records being opened, 19 of 18,896 total cases (0.1%), was recorded at the off-site gastrointestinal (GI) procedure areas. Although there was a statistically significant decrease (p < 0.05) in the percentage of record-opening errors in the GI area, there was no significant decrease over time. The technology to track whether a barcode has been used or not to open the patient’s EMR has been available since April 2012, and this data are presented with number of cases and percentage of cases from April 2012 to September 2012 (Table 2).
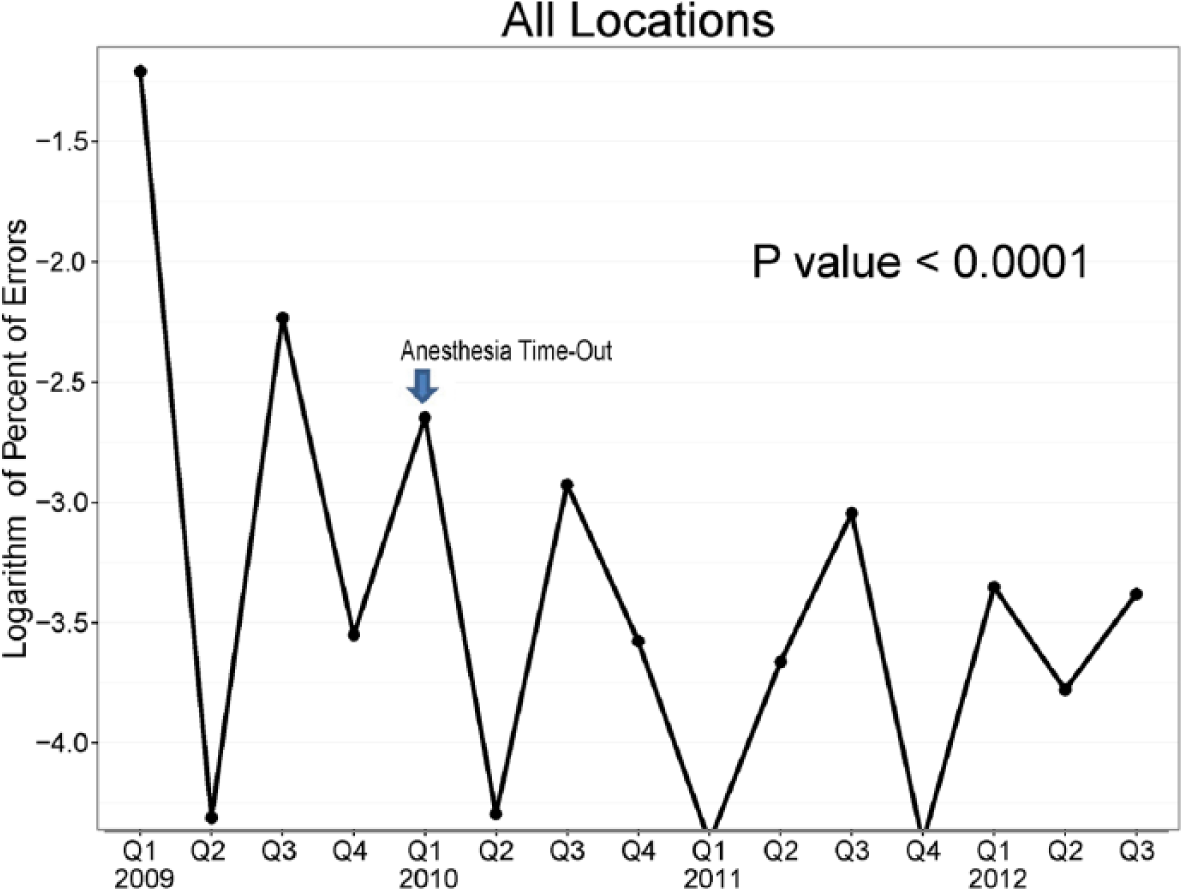
Incidence of incorrect records being accessed and charted over time in all locations.
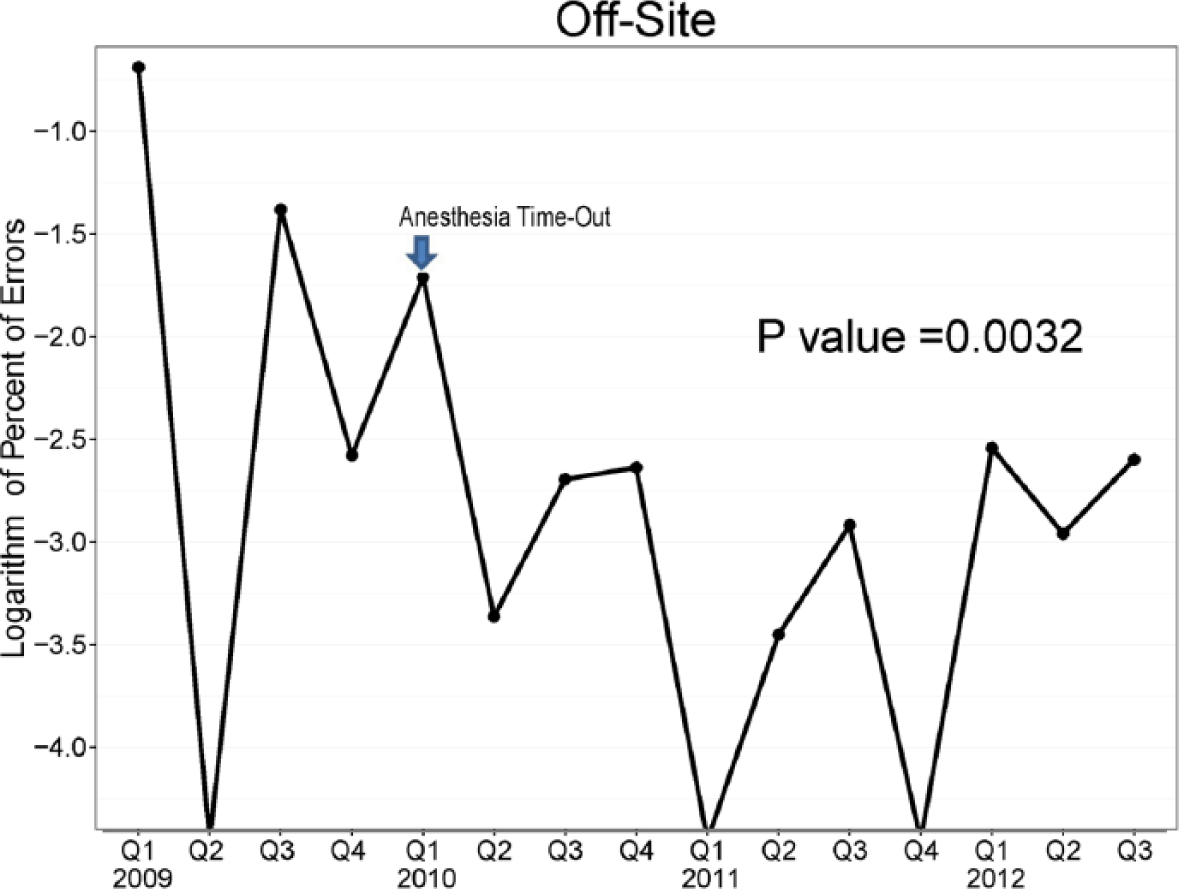
Incidence of incorrect records being accessed and charted over time in off-site locations.
Number of cases and percent of cases utilizing barcode technology by location.
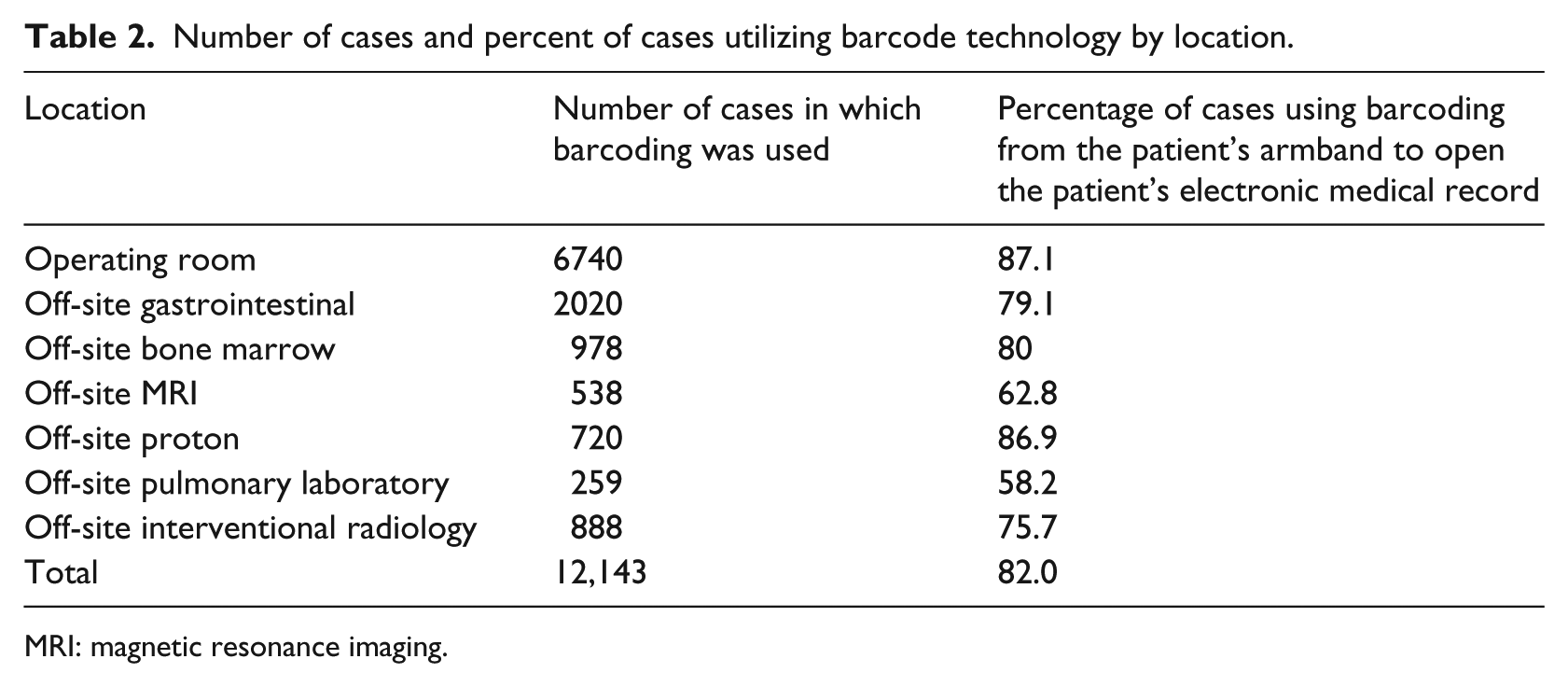
MRI: magnetic resonance imaging.
Discussion
There is no published literature concerning the errors related to informatics in the perioperative setting. We addressed this deficit by investigating the incidence of errors in opening the wrong patient records in the perioperative environment. Furthermore, we reported our results by location in our practice. We also determined whether efforts to reduce such errors using barcoding and ATO decreased the incidence of wrong patient records accessed and charted.
We found that using barcoding and ATO in our practice resulted in a statistically significant decrease in the incidence of accessing and charting the wrong patient records over time in all sites. The off-site areas had the largest number of wrong records opened, with the greatest number of errors seen in the GI procedure suites. Although there was a statistically significant decrease in percentage of errors in the off-site GI areas, there was no significant decrease in errors over time. It is currently our practice that every patient having a procedure done in the operating room or off-site location has the barcode scanned on their patient identification bracelet to open their EMR.
One potential criticism of this study is the possibility that some incorrect records opened were not detected and not analyzed. This is certainly true of self-reporting and IT records were our only detection system. However, the billing group in our Anesthesiology department completes a daily reconciliation for every case that involves anesthesia. The group also verifies that the procedures had pre-approval from financial sources and that the procedure was done on the scheduled date. These steps served as independent verification that ensured no undetected wrong record openings. Such cross-checking prevents an occurrence of unaccounted error. We do not expect the error rate to equal zero because of exigent circumstances that are part of clinical practice. Barcoding and ATO have significantly reduced the error rate in our practice. However, if a near miss occurred and the anesthesia record was incorrectly opened and not charted, this would not be captured. Only records in which there was incorrect accessing and charting were included. An additional advantage of barcode identification and usage is that it is impossible to superimpose a name on an incorrect record since patient records are accessed by medical record number rather than by name. Barcode scanners were available in all locations from 2011, and the frequency of barcode scanning utilization is available from April 2012; however, having providers adapt to the new practice and avoid workarounds continues to be a goal. We cannot rule out a learning effect. The error rates are very small and repeat offenders are unusual. We attempt to address process issues rather than assign blame to individual anesthesia members. Internal Quality Improvement investigations showed that barcoding was not utilized because of process issues such as failed scanners, scanners that could not reach the patient’s identification bracelet, wrong record scanned but patient’s identification band was not used.
Our results suggest that the implementation of the ATO and barcoding on every case in the operating room and in the off-site locations decreased the incidence in accessing and charting in the incorrect patient record. The sharp decline in wrong records accessed between Quarter 5 and Quarter 6 in 2010 may have been due to the implementation of ATO in the operating rooms and off-site locations. The use of barcoding in the perioperative environment has been incremental due to cost and practice culture issues. The practice of anesthesia outside the operating room to off-site locations has increased dramatically over the last 6 years, and adapting to this change as well as a learning effect may also be involved. We believe that the decrease in opening and charting in the incorrect anesthesia record is due to both the ATO and the barcoding. We could not separate the ATO and barcoding because the ATO emphasized barcode opening of the electronic record as part of its checklist.
This study supports the use of barcoding and ATO which has allowed us to examine process flow and implement improvements in high error areas. Interventions such as ATO and barcoding may play an important role in decreasing errors in wrong patient record opening and charting in the perioperative environment. Further investigation is warranted to determine the significance of decreasing incorrect opening and charting of patient EMR.
Footnotes
Acknowledgements
The authors would like to acknowledge John Frenzel, Joel Berger, Juan Cata, David Grosshans, Charles Cowles, Keith Shook, and Wade Altman for their contributions in preparation of this manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.