
Abstract
African Americans’ greater access to mobile phones makes short messaging service technology a promising complement to health promotion interventions. Short messaging service text messages were added to the Men’s Prostate Awareness Church Training project, a men’s health intervention for African American men. We report on the feasibility and acceptability of the use of short messaging service text messages in the intervention. Short messaging service text messages served as (1) workshop reminders; (2) post-workshop message reinforcement; (3) spiritual/motivational messages; and (4) participant retention. At workshop 4, over 65 percent of participants wished to continue receiving the messages. While there was an increase in recall over time, more than one-third of the participants did not recall receiving the 53 text messages. However, recall was considerably greater among men who attended the Men’s Prostate Awareness Church Training workshops. Overall, the inclusion of text messages in health promotion interventions targeting mature African American men was found to be feasible and acceptable.
Keywords
Introduction
In the context of health disparities or inequities, less attention has been paid to men of color, such as African American men, relative to research and interventions developed for women or those that include both men and women.1–6 Specific to prostate cancer, African American men suffer a greater burden than other men in both incidence and mortality. 7 Particularly with the U.S. Preventive Services Task Force’s recommendation against the use of the prostate-specific antigen (PSA)-based screening for prostate cancer, confusion may arise over whether or not men should be screened. Considering the greater prostate cancer incidence and mortality among African American men, educational interventions are needed to enable and empower African American men to make an informed decision regarding prostate cancer screening.8,9 There have been several prostate cancer educational interventions targeted specifically to reach African American men.10–16 A number of these interventions has been in collaboration with the faith community, which is an effective setting for health promotion, particularly among African Americans.17,18 Because of increasing access in the African American community, health information technology (HIT) is becoming a promising intervention channel. 19
Health information technology
Data collected by the Pew Research Center 20 in 2013 revealed that 85 percent of African Americans use the Internet compared with 86 percent of Whites. However, the method in which African Americans use the Internet differs from that of their White counterparts, with more African Americans accessing the Internet on their mobile phones (74%), compared to 59 percent of Whites. 21 In addition, 80 percent of African Americans have reported using their phone to send or receive short messaging service (SMS) text messages. 21 The increased use of SMS technology in African American communities may be a promising avenue for health promotion and intervention in this group.
African American adults 65 years old and older are more likely to own a mobile phone than a desktop computer.21,22 However, older adults may not own a smart phone, 23 so an intervention using a smart phone application or one that requires the Internet24–29 may not be feasible for this population. Therefore, SMS text messaging may be a suitable channel because it is delivered through a regular cellular phone that does not require Internet service. SMS text messaging has been used in the health field as an assessment tool, 30 for program logistics such as reminders,31–33 or as a health promotion tool.34–37
Although the literature in this area is in a relatively early stage, several studies have demonstrated that SMS text messages may be an effective strategy for stimulating behavior change or supporting behavioral interventions.38,39 SMS text message reminders have been shown to be popular with patients and more cost-effective than paper or telephone-based reminder strategies. 40 Periodic cues via SMS text messages have been found to be effective in reinforcing healthy behaviors. 38
Song et al. 37 developed an intervention involving two-way text messages where minority pregnant women were able to ask questions and receive answers to their questions. The post-test administered at the completion of the intervention revealed a knowledge gain among participants. 37 In “Project Tech Support,” high-risk men who have sex with men (MSM) who use methamphetamine participated in a two-week pilot intervention where they received social support and health education via text messages. 36 Follow-up findings indicated that there was a decrease in methamphetamine use and unprotected sex while using methamphetamine among the participants. 36 Another intervention was based on the Protection Motivation Theory 35 and had participants generate and schedule their own motivational message and reminders to increase exercising behavior. 35
The current study
This article describes the development of the SMS text messaging component of the Men’s Prostate Awareness Church Training (M-PACT) intervention. The overall M-PACT parent study aims to increase informed decision making for prostate cancer screening among African American men. 41 The text messages discussed in the current report were embedded in the context of the M-PACT trial. We address two research questions: (1) Is an SMS text message strategy feasible (e.g. can we develop and send them?; do participants recall receiving them?) for use with African American men age-eligible for prostate cancer screening (40–69)?; and (2) Are text messages with prostate cancer information acceptable (e.g. participant satisfaction ratings of the messages) to this group of African American men?
The M-PACT SMS text messaging component served as a value-added element of the intervention and was not designed (e.g. in the study design as through randomization) to be evaluated for an independent or additive effect on the study outcome of informed decision making. The purposes of the SMS text messages for the M-PACT project were to (1) remind participants of upcoming workshops; (2) serve as post-workshop message reinforcement; (3) provide spiritual/motivational messages; and (4) serve as a participant retention tool. We discuss implications for the use of HIT in community-based health promotion for men of color. The unique focus of this project is the use of HIT in a health promotion intervention for mature African American men.
Method
M-PACT intervention
The M-PACT intervention consists of a church-based, spiritually grounded four-part men’s health workshop series that incorporate scripture and spiritual themes. This work was approved by the University of Maryland Institutional Review Board (#12-0095). The M-PACT intervention is led by trained and certified peer community health advisors (CHAs). The primary aim of M-PACT project is to use a group randomized controlled trial aimed to compare a men’s-only workshop format versus a health partner approach, where the enrolled men were asked to invite an important woman in their lives (e.g. wife/partner; daughter; sister; friend) to attend the workshops with them.
Workshop participants receive culturally targeted print materials and regular SMS text messages. For example, the project’s print materials are based on recommendations from the focus group participants and use an intergenerational picture for the cover design, include pictures of men in the target age group, and incorporate themes of “masculinity” and “pride” throughout. 41 The content is spiritually grounded through use of supportive scripture and religious themes (e.g. “Beloved, I pray that in all respects you may prosper and be in good health, just as your soul prospers. 3 John 1:2” and “Do you not know that your body is a temple of the Holy Spirit … so use every part of your body to give glory back to God. 1 Corinthians 6:19–20”). The content and evaluation are based on the Health Belief Model. 42
Eighteen churches were enrolled, each training and certifying two CHAs for a total of 36 CHAs. The bi-monthly educational workshop series consists of (1) project kickoff and participant enrollment; (2) prostate cancer and screening education; (3) informed decision making for screening; and (4) treatment options and where participants may go to talk to a health provider. The presentation format for the M-PACT workshop series is a combination of didactic content and interactive forum where opportunities for discussion and sharing from participants are available throughout. Intervention development, description, and workshop recruitment and retention are discussed in more detail elsewhere.41,43
All participants (N = 288) in the M-PACT project had the option to enroll in the SMS text messaging component. Similar to the overall M-PACT intervention, the SMS text messaging component was developed based on an iterative community engaged research process involving an advisory panel, a HIT project subcommittee, community partners, and formative research including focus groups. 41 Outcomes of interest were feasibility (e.g. can we develop and send them?; do participants recall receiving them?) and acceptability (e.g. participant satisfaction ratings of the messages) of the use of SMS text messages in the M-PACT intervention.
Formative research
Two church-based focus group discussions were conducted with African American men in order to initially explore the possibility of integrating technology into the M-PACT intervention. A total of 23 African American men between the ages of 40 and 69 shared their views on this topic. The majority of the men reported using technologies such as the Internet, email, and cell phones. Some participants indicated that they received SMS text messages from their place of worship. One participant shared: “We cc everybody, we text everybody, so we do use that [technology].” Another expressed: “You would be remiss if you didn’t use all of them [Internet, SMS text messages, and social media] to get information out about prostate cancer.” However, these men reported that they do not use technology (e.g. checking email) as frequently as their younger counterparts.
SMS text message development
SMS text messaging was selected as the best strategy for use with this priority population because of its regular use of cellular phones and familiarity with receiving SMS text messages. However, these men did not necessarily use smart phones or have Internet access, and, therefore, SMS text messages were identified as the most suitable channel because Internet access is not required. The SMS text messages were developed by a project subcommittee with expertise in health literacy, health communication and informatics, and web development (Table 1). Methods used to develop the SMS text message strategy included (1) review of previously published literature, (2) examination of successful SMS text message interventions presented in national and local conferences and events (e.g. 2011 mHealth summit, NIH mHealth Listserv, research forums), (3) review of existing spiritually based SMS text messages, and (4) review of health-related Biblical scripture. Inspirational, spiritual messages were reviewed for appropriateness and contextual meaning by community partners, advisory panel members, and project team members who were closely affiliated with the faith community by role (i.e. ministerial and/or lay leaders). Although SMS text message length must be brief (140 characters or less), we included information about the source of the message (e.g. “from the M-PACT project”) in an effort to maintain trust and increase visibility of the intervention through use of its branding.
Examples from the M-PACT SMS text messaging library.
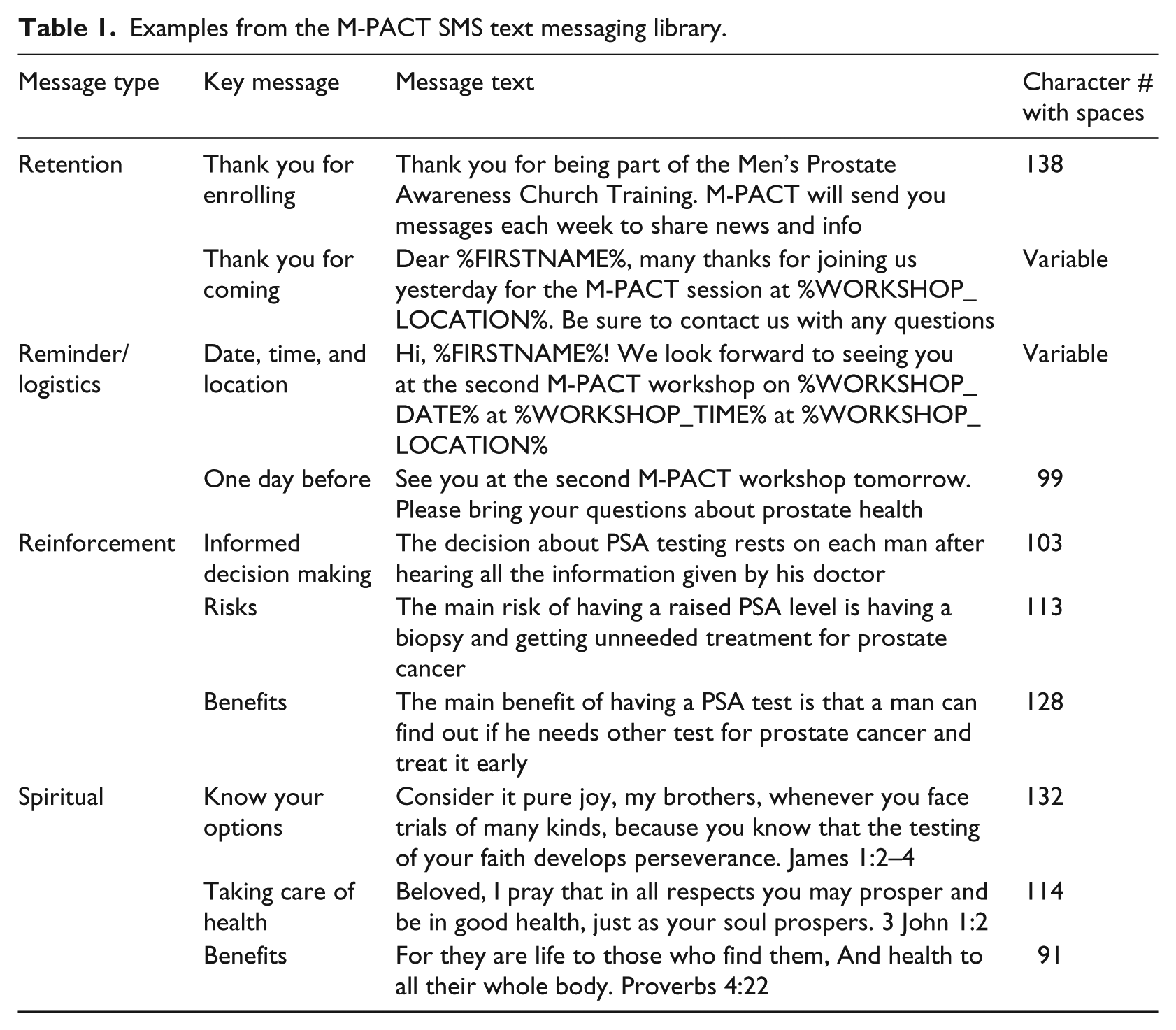
Part of the SMS text message strategy included determining the optimal frequency and timing of message delivery. The frequency that SMS text messages were delivered was determined by the needs and expectations of the target audience. For example, while younger audiences may prefer to receive more frequent texts (e.g. daily), older audiences appear to prefer receiving messages less frequently (a theme from our formative research findings). Development of the SMS text message library was based upon the bi-monthly timing of the men’s health workshops in the M-PACT intervention (Figure 1). The SMS text message library included pre-workshop messages, messages to be sent out between workshops 1 and 2; 2 and 3; 3 and 4, and retention messages to continue after workshop 4 until the 12-month follow-up. Workshop reminders were sent 1 day in advance, and post-workshop messages were sent 1–5 days after the workshops.
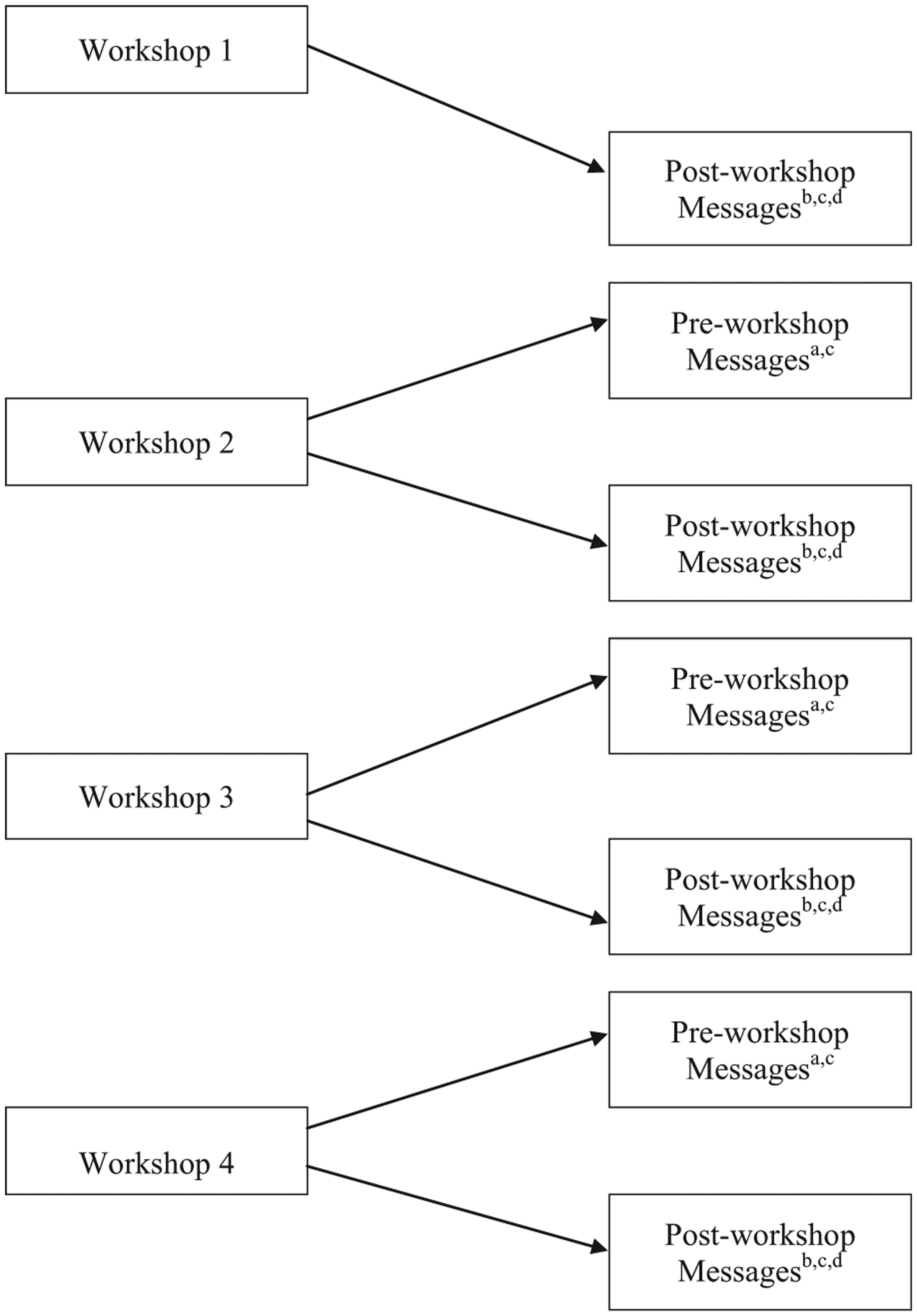
SMS text messaging timeline and type.
The study advisory panel recommended delivering the SMS text messages in the morning to ensure that participants were able to view them prior to engaging in their daily activities. Participants were registered into the SMS text message component when they submitted their cell phone number and provider at project enrollment. Participant enrollment could take place at any of the four workshops. Participants also had the option to opt-out in the future if the text messages became burdensome for them.
Technical specifications
Technological specifications required that key information be collected from the participants (e.g. cell phone number and service provider). The SMS text messaging program could then be populated with modestly tailored and personal information such as name of church, workshop dates, and the first and last names of the SMS text message recipients. The SMS text messaging program is a Microsoft-based database on a Windows server with a dot net framework/platform. The structured query language (SQL) database is password-protected for participant confidentiality.
This SMS text messaging program was developed with the following capabilities: (1) supports all mobile device carriers; (2) dynamic and modestly tailored SMS text messages (e.g. name of church, workshop dates, and participant’s first and last name can be replaced for individuals); (3) design of multiple SMS text message templates (e.g. the ability to set up the time of day, frequency, and length of days the SMS text messages are sent); (4) query and search features for any data field; (5) sorting function of any field; (6) full editing function for the data records including delete and update; (7) real-time summary reports showing the number of sent messages and how many days (as well as the specific times) the SMS messages were sent; and (8) ability to download the database as a Statistical Package for Social Sciences (SPSS) file.
Participant data collection
Participants were asked for their cell phone numbers and providers and were entered into the SMS text messaging system by project staff. Participants responded to questions about access to cell phones and their preferred frequency of receiving SMS text messages from future projects like M-PACT. Project surveys were administered at workshops 2, 3, and 4 and included questions about whether participants remembered receiving the text messages, how many they remembered receiving, the topic of the messages, and evaluations of acceptability of the messages. Given the importance of having the correct cell phone number and provider on record for each of our participants, we also continued to collect, double check, and update this information at each of our subsequent workshops to the best of our ability.
Feasibility considerations included the extent to which we were able to develop and distribute the SMS text messages and the extent to which the participants recalled receiving them. Acceptability was assessed using six questions on participants’ satisfaction with text messages (e.g. “I enjoyed getting text messages about the program” and “The M-PACT text messages kept me engaged in the program”). These statements or questions were measured using four-point Likert response scales that ranged from strongly agree to strongly disagree, with a fifth response option indicating that they did not receive the messages.
Results
Participant demographics
Participants were church-attending men between 40 and 69 years old (N = 288). The average age of the participants was 56.0 years (SD = 7.6 years). Over half (59.7%) of the participants indicated that they were working full-time, while 12 percent were retired. Approximately 32 percent of this highly educated sample comprised individuals who have graduated college (4 years of college or more). The median annual household income of the participants was between US$70,001 and US$80,000.
Cell phone access and SMS text messaging interest
Analyses are reported using baseline data from M-PACT participants who provided information about their mobile phone use and preferred SMS text message frequency (Table 2). Since participant enrollment and completion of the baseline survey could take place at any of the four workshops, baseline information reflects data from all M-PACT workshops. Of the N = 288 participants, an overwhelming majority reported that they used a cellular device (98.3%). Of those that had a cell phone, 220 (77.8%) responded that they used their cellular device for SMS text messaging, and more than half reported having a smart phone (61.1%). Among those that indicated that they were open to SMS text messaging, the two largest categories in terms of preferred frequency were on an “as needed” or “monthly” basis (37.8%, combined).
Mobile phone use and preferred text message frequency for all enrolled M-PACT participants.
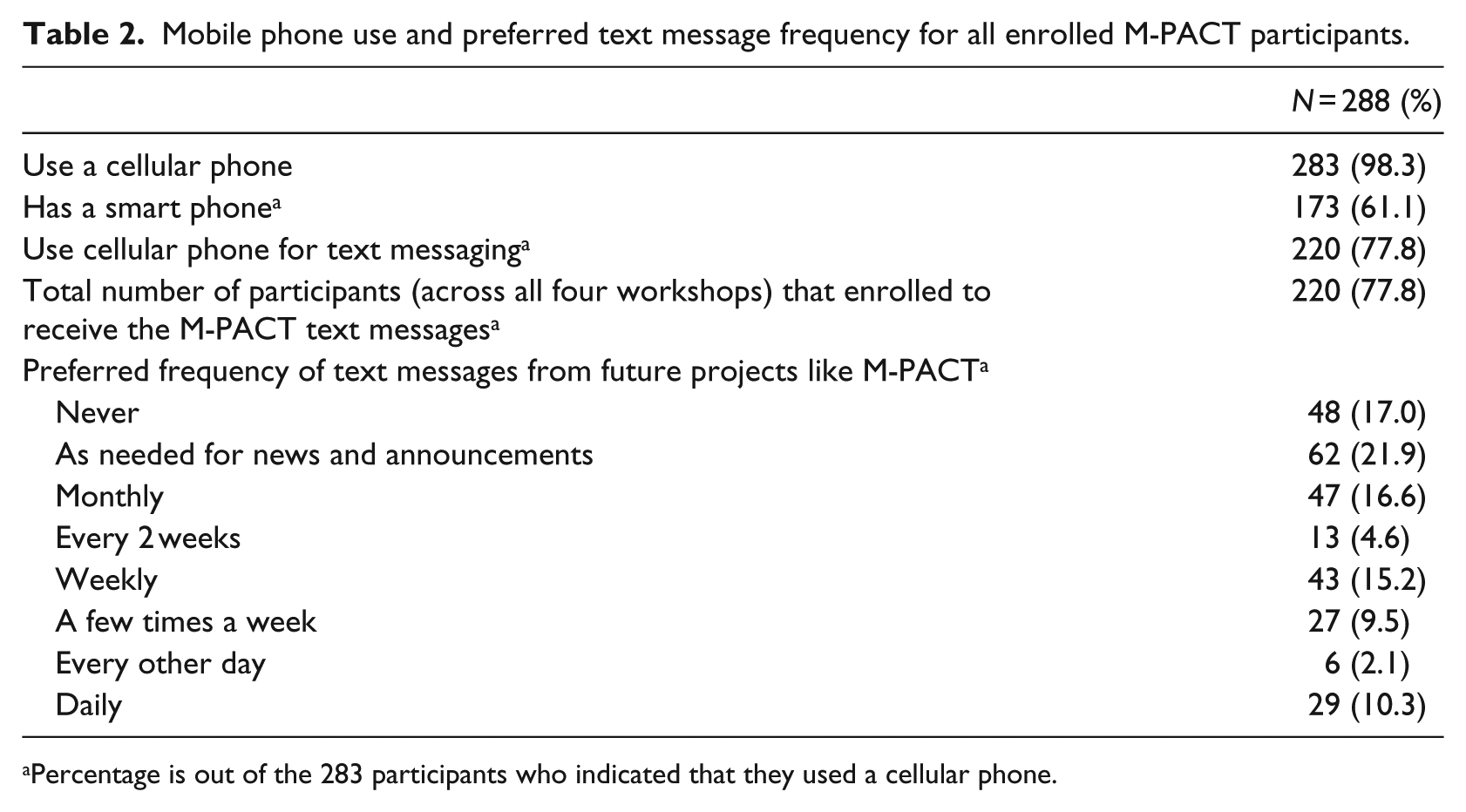
Percentage is out of the 283 participants who indicated that they used a cellular phone.
SMS text messaging implementation
Of the 220 men who reported using their cellular device for texting, all of them agreed to enroll in the M-PACT SMS text messaging component (Table 3). Table 3 not only shows the workshop attendance and retention rate for all participants, but also displays the comparison between workshop attendance and retention rates for those enrolled in the SMS text messaging component with those who were not enrolled in the text messaging component. There was not a significant difference for workshop attendance and retention rates between the two groups. Of the returning participants who were previously enrolled in the M-PACT trial, roughly three-quarters of them were enrolled in the SMS text messaging component during the subsequent workshops (i.e. workshops 2, 3, and 4).
Workshop attendance for all participants, those enrolled in the SMS text messaging component, and those not enrolled in the SMS text messaging component.
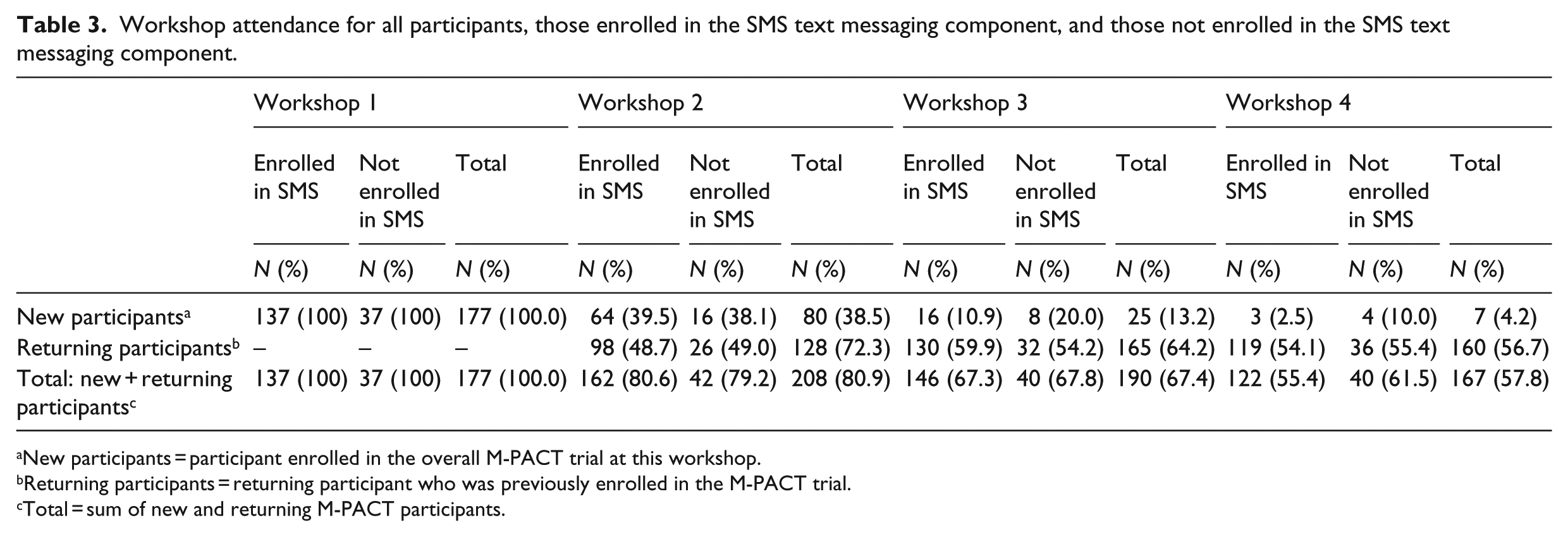
New participants = participant enrolled in the overall M-PACT trial at this workshop.
Returning participants = returning participant who was previously enrolled in the M-PACT trial.
Total = sum of new and returning M-PACT participants.
General workshop reminders, men’s health, and religious/spiritual messages were sent at least three times per week. The software transmitted an average of 19 SMS text messages to each participant between each workshop. Implementation of the SMS text messaging component began after workshop 1 and thus follow-up information regarding the text messages were not collected until workshop 2 (Table 4).
Participant text message recall and acceptability ratings; frequencies (percentages).
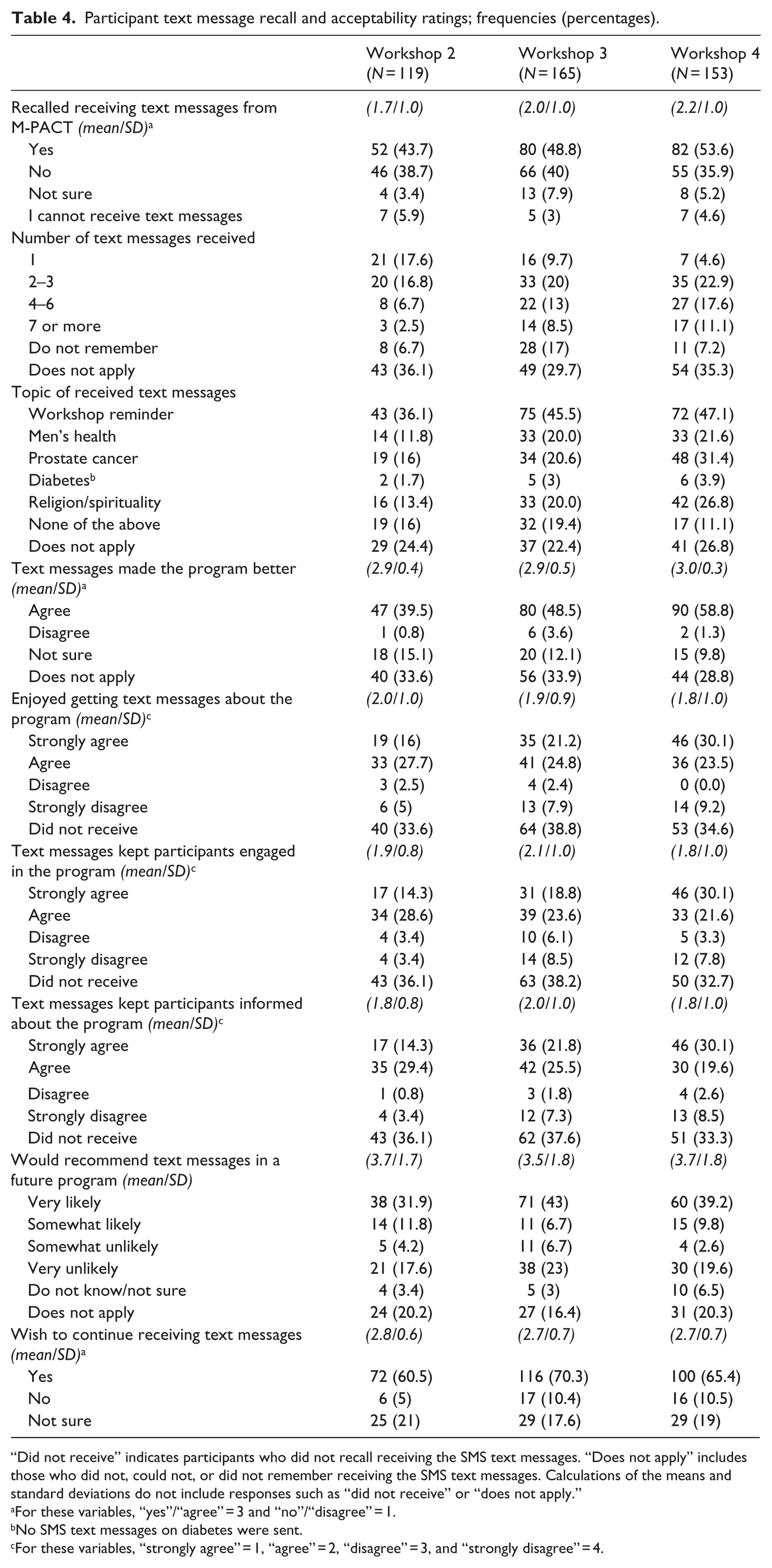
“Did not receive” indicates participants who did not recall receiving the SMS text messages. “Does not apply” includes those who did not, could not, or did not remember receiving the SMS text messages. Calculations of the means and standard deviations do not include responses such as “did not receive” or “does not apply.”
For these variables, “yes”/“agree” = 3 and “no”/“disagree” = 1.
No SMS text messages on diabetes were sent.
For these variables, “strongly agree” = 1, “agree” = 2, “disagree” = 3, and “strongly disagree” = 4.
Feasibility and acceptability of the SMS text messaging
The SMS text messaging component showed some feasibility and positive acceptance among M-PACT project participants. Feasibility was evidenced by the development of the SMS messaging system and delivery of messages to participants. Most of the participants (78%) agreed to enroll in the text messaging component of the intervention at baseline. The 78 percent enrollment rate was calculated based on the total number of individuals that enrolled to receive the M-PACT text messages over the total number of individuals who indicated that they used a cellular phone (i.e. 220 out of 283). With regard to acceptability, participants expressed generally positive attitudes toward the SMS text messages, with only three participants opting out after enrollment. Of the participants who were enrolled to receive the SMS text messages and completed the follow-up surveys at workshops 2, 3, and 4, roughly half (43.7%, 48.8%, and 53.6%, respectively) recalled receiving SMS text messages from the M-PACT project, with numbers showing an increase over time (see Table 4). Of these men, 26 percent, 41.5 percent, and 51.6 percent recalled receiving two or more SMS text messages from the project. Men had greatest recall for workshop reminder messages, followed by messages about men’s health, prostate cancer, and religion/spirituality with about equal frequency.
The percentage of participants who agreed that “the text messages made the program better” steadily increased through the three follow-up periods, from 39.5 percent, 48.5 percent, and to 58.8 percent, respectively (see Table 4). With about half of the participants agreeing or strongly agreeing, growing positive trends over time also appeared when the participants were asked whether they “enjoyed getting text messages about the program,” whether the “text messages kept them engaged in the program,” and whether the “text messages kept them informed about the program.” While 43 percent of participants from workshop 3 would be “very likely” to recommend the inclusion of SMS text messages in a future program, another 23 percent reported they would be “very unlikely.” Yet a majority (over 60%) in each workshop indicated that they wished to continue to receive SMS text messages from the M-PACT project.
Discussion and conclusion
This analysis in general suggests that the M-PACT SMS text messaging strategy was feasible; however, recall of the messages overall was modest, but most men who recalled receiving the messages were satisfied with them. With increased cellular phone and Internet penetration through “smart phones,” particularly in racial and ethnically diverse communities,20,21,23,44,45 it was appropriate to investigate the feasibility of using technology as a means to reach diverse populations in efforts to reduce health disparities. Most African American men in our sample indicated that they owned a mobile phone and used it to send and receive SMS text messages.
Results from the baseline data allowed us to determine the preferred frequency of SMS text messages for future interventions like M-PACT, on an “as needed” or “monthly” basis. Our findings suggest that similar interventions should keep in mind not to over-saturate their population with messages on a too-frequent basis. Data collected from the follow-up surveys at the end of each workshop allowed us to assess acceptability of the SMS text messages in this population.
SMS text message recall
Recall of the M-PACT SMS text messages was modest, but did increase over time. This increase is likely due to exposure from multiple messages sent on a regular basis. Though recall did increase over time, still only about half of the participants overall remembered receiving the M-PACT SMS text messages (43.7%, 48.8%, and 53.6% at workshops 2, 3, and 4, respectively). This is interesting as by workshop 3, participants who were enrolled during workshop 1 were scheduled to have received an average of 53 messages (e.g. roughly 19/bi-monthly). Even with branding the messages with the study’s name, over one-third of the participants indicated that they did not remember receiving them. It is possible that simply branding our text messages with the study’s name may not have been enough. For participants who already receive text messages from their other social and/or faith-based networks (e.g. from their individual church groups or directly from the Pastor at their respective churches), perhaps the M-PACT messages did not distinguish themselves enough for participants to recall receiving them.
However, recall of the messages among men who actually attended the workshops was greater than men overall. Table 3 indicates that M-PACT workshop attendance was variable. Examining data from Tables 3 and 4, text message recall for men who attended workshops 2, 3, and 4 was 32 percent (52/162), 55 percent (80/146), and 67 percent (82/122), respectively. This suggests that men who were engaged in the M-PACT project had (1) greater text message recall, and (2) a sharper increase in recall over time than men overall, which included those men who did not attend the workshops.
It is also possible that there were technical issues with the text messaging system, which resulted in some men not receiving the messages. Not having pilot-tested the system, other than with study team members, it is difficult to determine whether the low recall rates were due to recall or to messages not having been received. In some cases, there were problems with participant contact information (e.g. incorrect information or changes in cellular phone numbers and/or carrier information), which was updated on a case-by-case basis at the workshops. Future text messaging initiatives should ultimately build in a way to verify if messages have been received.
Of those that did remember receiving text messages, recall was accurate as few men (1.7% during workshop 2 [2/119], 3% during workshop 3 [5/165], and 3.9% during workshop 4 [6/153]) endorsed the “foil” option of diabetes messages, which were not included in the message content. Men tended to recall workshop reminders to a greater degree than health-related or even spiritually based messages, which was surprising. One possible explanation is that the participants considered all the M-PACT related SMS text messages to be general reminders about the project. The reminder texts could have also acted as cues to action, making them easier to remember.
Feasibility and acceptability
The integration of an SMS text messaging component into the intervention was reasonably accepted, as reflected by roughly half of the participants who said the messages made the program better and enjoyed receiving the messages. Of those who did not rate the messages positively, many indicated that they did not remember receiving the messages as opposed to not liking them. An unnoticed glitch in the SMS text messaging program, inaccurate contact information from the participants, or change in their mobile capabilities could have all attributed to the gap between the SMS text messages sent from the project and participant recall. To address some of these logistical concerns, we did follow up with participants who indicated they were not receiving the text messages. At each of the workshops after the first, we re-confirmed participant contact numbers and service providers and double-checked that this information was also correctly input into the text messaging database.
Interestingly, one-fifth (20%) of the men indicated that they would not recommend the SMS text messages for use in a future program. Perhaps future initiatives could engage in formative research to explore reasons for this response and make recommendations for improving the salience of subsequent messages. Only 11 percent of the men said that they did not wish to receive future SMS text messages from M-PACT, and only three participants opted out, which were both reasonable indications of feasibility and acceptability among these participants. As the men’s evaluations of the messages tended to build in positivity over time, particularly by the third workshop, research is needed to understand whether familiarity with the program, relevance of the messages, or other factors may have been associated with improved ratings.
The literature on the inclusion of text messages in health interventions is growing, and a number of these interventions target African Americans. These studies that incorporate HIT into interventions among African Americans focus on issues including sexual health,46–48 physical activity,49–51 diabetes, 52 or heart disease. 53 Results obtained from this study are similar to those found in the literature in terms of feasibility and acceptability of SMS text messaging, with high acceptance among both African American adolescents and adults in these interventions.46,53
Strengths and limitations
This study had both strengths and limitations. The decisions about how to deploy the text messages was grounded in formative research that was conducted to assess whether such approach should be considered for inclusion in the intervention. Participants’ responses indicated that the approach merited further study. The HIT-subcommittee included experts in health communication and informatics. All spiritual messages were reviewed by church leaders to ensure that they were appropriate for the target audience. The text messages contained personalized information pertaining to the workshops such as name of the church, and dates and times of future workshop sessions.
However, the message content itself was not pilot-tested with members of the priority population. Several technical difficulties could have been identified and corrected prior to roll-out if the SMS text messaging system itself was also pilot-tested. Another limitation was that the current system did not allow active participation in the form of two-way texting. Thus, it cannot be used to collect data and feedback from participants, as done in other existing systems.46,54,55 An improvement to the M-PACT SMS text messaging system would be to involve the initial text message asking for verification that the user received it. Finally, the SMS text message aspect of the study was not evaluated for an independent or additive effect on the study outcome of informed decision making. We did not anticipate that the SMS messages themselves would be sufficient to produce an intervention effect but rather would be a value-added component of the existing intervention.
Implications for future research
Future studies can evaluate a stand-alone SMS text messaging intervention to examine its impact on behavioral outcomes such as informed decision making. Other capabilities of the mobile technology can also be included in future research. For people with smart phones, messages can connect participants with additional information using hyperlinks to trustworthy websites. In this case, a uniform resource locator (URL) shortening service can be used to take into account the character limit for SMS text messages. Allowing participants to submit keywords to receive specific information can also be explored in further studies. Additionally, a two-way messaging or a mobile application intervention could be considered to allow participants to ask specific questions that could be answered by a designated program staff.
Conclusion
Few previous interventions have used SMS text messages in cancer prevention and education 56 or have targeted mature African Americans particularly in a faith-based setting. 53 Incorporating SMS text messages in health interventions is a promising avenue to reach mature African American men. Technological advances have made this platform more accessible among this group. SMS text messages can be used for a variety of purposes from reminders to health content to retention. SMS text messaging is supported by most mobile phones, is inexpensive, and can be accessed at a time that is convenient for the recipient. 38 This approach can be an important asset in empowering African American men to make an informed decision about prostate cancer screening, and their health in general. However, it is apparent that in this sample of men, the SMS text messages were not uniformly recalled or embraced, suggesting avenues for future research in this area.
Footnotes
Acknowledgements
The team would like to acknowledge the work of Ralph Williams, Koko Barnes, Dr Tony Whitehead, and Dr Michael Naslund for their extensive contributions to this study. We would also like to especially thank all the churches, community health advisors, and volunteers that participated and supported this research project to educate men about prostate cancer and early detection.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by a grant from the American Cancer Society (RGST-10-113-01-CPPB). Clinical trial registration number: NCT02131779.