
Abstract
This article presents and illustrates the main features of a proposed process-oriented approach for patient information distribution in future health care information systems, by using a prototype of a process support system. The development of the prototype was based on the Visuera method, which includes five defined steps. The results indicate that a visualized prototype is a suitable tool for illustrating both the opportunities and constraints of future ideas and solutions in e-Health. The main challenges for developing and implementing a fully functional process support system concern both technical and organizational/management aspects.
Keywords
Introduction
Health care processes are characterized by their high complexity and the large amount of data they have to manage. To provide high-quality care, health care processes require cooperation among different organizational units and medical disciplines, as well as their cooperation with patients. Process orientation is therefore crucial. However, despite its widespread adoption in industry, the process-oriented approach, with supporting information systems (IS), is not widely used in health care.1,2 Instead, organizations typically have their own autonomous IS that support internal processes. These types of systems usually work well for the single unit but do not support inter-institutional cooperation and, hence, cause delivery of suboptimal care. 3 Furthermore, the needs of patients tend to be neglected in these systems. Taking a process-oriented approach can streamline the flow of information and ensure that information is available where and when it is needed. Sharing information that is of high quality efficiently is a fundamental part of an integrated health care system.
IS have enormous potential to improve the quality of health care, in terms of safety, effectiveness and efficiency. They also have the potential to make care patient-centred. However, present IS do not yield the expected positive effects. The current situation regarding the availability of IS that support patient-centred health care is still far from satisfactory.4,5 Often, different care providers are involved in the care of one patient, which requires collaboration for a successful treatment outcome. A key issue in supporting collaboration is the need for information sharing between different care providers. However, for a long time, there have been concerns that the communication between health care professionals, regarding co-treated patients, has been delayed, incomplete or erroneous.4,6–9 There are numerous examples of health related injuries that are caused by the deficient exchange of information between different actors in the care process.8–11 Furthermore, communication between patients and health care providers has major shortcomings. 4
Today, shared patient information is hampered by the existence of numerous IS, so-called stovepipe solutions. Another important factor is the decentralized health care system. In addition, decentralization hinders solutions that take a holistic approach to the problem, from a patient perspective. Furthermore, current IS cause a suboptimal consumption of health care resources and force the patient to act as a ‘carrier’ of their health care information. To achieve a seamless and secure transfer of information between care providers, a more process-oriented approach, with supporting IS, must be considered. A process-oriented approach is an important foundation for achieving a system design that focuses on the care process from the patient’s perspective and thereby sets the patient process in focus. The patient process is defined in Åhlfeldt and Söderström as the process that follows the patient during an event of illness. During this process, important patient information must follow the patient in order to ensure good quality care.12–15 The process-oriented approach can streamline the flow of information and ensure that health care professionals work with the right tasks in the different parts of the health care process as well as always have access to the right patient information when they need it. 16 Having access to patient information at the right time is crucial for providing the best possible care. However, for information to be a usable and useful resource in the long term, it must have a uniform, nationally established structure,16,17 hence, be placed under a common regulatory framework. (For information technology (IT) systems to manage and exchange information, the information must have a nationally defined and consistent information structure. Information must therefore follow a common regulatory framework and be allocated in a uniform information structure. This allows IS to more effectively and efficiently manage and exchange information. A unified national information structure is thus based on a standardized use of terms, concepts and classifications. This is an important prerequisite for both patient safety and follow-up care.) This will allow different IS to manage and exchange information more efficiently and securely. Furthermore, patient safety and the ability to follow up on care activities are contingent on a uniform information structure based on established terminologies and classifications. Structured information and standardized terms and concepts will also facilitate transparent audits and comparisons between health care processes and outcomes, as well as provide support data for quality development.6,16 Furthermore, the Ministry of Health and Social Affairs emphasizes that future IS need to support, involve, motivate and empower individuals/patients by enabling greater accessibility to health care and social services. This provides the prerequisites for empowerment and self-determination and strengthens individuals’ perceived benefit, participation and insight into the interventions that concern them. 16
The aim of this article is to present and illustrate the main features of a proposed process-oriented approach for patient information distribution in health care, by using a prototype. The remainder of this article is organized as follows. Section ‘Research approach’ describes the research approach. Section ‘Key principles for a future IS’, discusses the key principles for developing the prototype, while section ‘Results and print screen examples’ presents the resulting prototype. Section ‘Discussion’, discusses the results and, finally, some concluding remarks are stated in section ‘Concluding remarks’.
Research approach
The prototype presented in this article is a result of a research project, Future Healthcare Information Systems (FHIS). 18 The aim of the project was to develop a visualization of a process support system (PSS) that demonstrate the requirements for future process-oriented IS support in health care. The PSS was developed in close collaboration between researchers and practitioners in the Region of Västra Götaland in Sweden.
Since the overall health care process is extremely complex and demanding, to tackle it all within one project would clearly not be feasible. Therefore, one of the first tasks of the project was to select a suitable sub-process for the work to focus on. Some criteria used for the selection included that the chosen sub-process should
be one in which the patient can play a truly active role,
be relevant for more than one level of care (primary care, hospital care and municipal home care), in order to demonstrate general applicability,
be relevant for more than one health care profession,
be complex enough, particularly in terms of information flow, to demonstrate a substantial difference between the existing way of working and the proposed future way of working,
be used often enough for the changed way of working to have a substantial impact on both health care professionals and patients.
The project selected the process of initiating, planning, carrying out and following up a patient’s visit to a health care provider. This process was termed ‘Patient Visit’ and was limited by involving only ambulatory care. It is a process which occurs frequently and exists in both primary and hospital care. Instances of the process in primary and hospital care also communicate with each other. Hence, it involves the desired element of complexity. Several professional groups are involved in the process and the patient needs to play an active role. In addition, the chosen process was also suitable to demonstrate the intricacies of the communication between a patient and health care providers. In order to make the demonstrator concrete and illustrative, two scenarios of the ‘Patient Visit’ process were chosen for implementation (see section ‘Results and print screen examples’).
Firstly, a current state analysis was conducted, 19 involving both health care professionals and patients. 4 The main research activities included observations of patient visits; interviews with health care professionals, health care administrators, patients and patient organizations, as well as workshops involving professionals from a broad range of disciplines.
Following the current state analysis, earlier research results mentioned above and in conjunction with the results from the workshops, a number of goals were identified for the future state: increased access to information, both from professionals’ and patients’ perspective, increased coordination of both clinical and administrative information based on the patient process, a holistic approach based on the patient’s perspective, increased patient involvement, and improved quality of care.
Based on the assessment of the current situation and As-Is process models, work began by sketching the proposed future state (To-Be models). First, the overview of the general patient visit was elaborated, in order to identify the sub-processes and information flows involved. Then, process models of the different sub-processes, comprising activities, roles and information flows, were created. An important part of this work was to identify the detailed contents of the information needed for the various activities in the process models. The information content was sketched in forms using the Visuera Business Process Modeler 2007 tool. 20 Process models and information content were validated by various professionals from both primary care and specialist care in workshops, brainstorming sessions seminars and lectures, which also took patient input into account. Key design principles were identified and after a number of iterations, to ensure the quality of processes and information content, a prototype of a PSS was developed to visualize the key principles.
Finally, the resulting prototype (see section ‘Discussion’) was evaluated in relation to user requirements identified through observations, workshops and interviews. In addition to this, identified user needs were also evaluated in relation to the Swedish national strategy for e-health and in seminars involving health care professionals, patients and IS providers.
The choice of which health care providers to involve in the development and evaluation of the PSS was partly governed by the fact that the research project was commissioned by Region Västra Götaland. They chose the sub-region on which the main portion of the research was to focus. In addition, the researchers chose to involve a convenient sample of other referenced health care providers and patient organizations, based on the researchers’ existing contacts in the region. Within the respective organizations, the involved individual stakeholders were selected to reflect a broad spectrum of stakeholder perspectives. In the evaluation phase, the circle of involved stakeholders was widened to also include the national perspective. For example, feedback was collected during the main Swedish professional conference and exhibition on health care and IT.
The approach used for modelling the chosen process and for prototype development was the Visuera method, 20 chosen for the following reasons:
The Visuera method is a process modelling approach that enables the modelling of activities and related actors in an organizational process. One particular feature of the method is that it integrates the flow of information with the activities in the process and also allows for the definition of the concepts used in the process. Since the general focus of our research is to enhance the support that information can provide to health care processes, this was considered an important feature.
It is fairly easy for non-experts to understand the models produced with the method. Since an important part of the work was for health care professionals to evaluate the feasibility of the proposed future process, before it was implemented in the demonstrator, the aspect of usability for non-experts was considered to be essential.
The method comes with a supporting tool that can take a graphical model describing a process and related information flows and ‘translate’ it into simulation/demonstrator of how a system will work and how it will look, without actually implementing the system. Since the objective was to develop a demonstrator, it was a reasonable choice.
The researchers in the project had previous experience with the method and its supporting tool.
The method contains five steps:
Analysing the As-Is processes. In this step, current activities are documented in a graphical As-Is process model.
Specifying the requirements (To-Be). Here, components in the As-Is process models, which have the potential to be made more efficient, are identified. A To-Be process model is developed. Efficiency can be achieved by: Automating work currently performed manually. Removing manual or automated tasks with no significance for activities later on in the process. Improving the quality of activities in the process. Making sure that the end result of all the activities has the highest quality. Improving throughput time by adding, deleting or reassigning tasks in the process. Improving information quality in the processes.
Developing supporting IS if technological change is necessary, based on To-Be process models.
Deploying the new process and IS. In this step, employees affected by the IS are educated.
Production and monitoring of improved processes and their support systems.
The Visuera method follows strict rules and has its own tool; the Visuera Business Process Modeler, which aims to ensure that process models have the same look and feel, regardless of organizational domain. The process models contain only a few symbols that intend to be intuitive. The process models can be abstracted or detailed into an unlimited number of levels. The prototype, presented in this article, acquired all of its sample data and flow logic directly from the process model.
Key principles for a future IS
Overall architecture of PSS
The vision for PSS is that health care providers and patients should have access to effective collaborative IS that supports process-oriented care in which the patient is a distinct and active collaborator. This means that
Appropriate parts of the PSS are available to both patients and professionals taking into account usability for different user groups.
Involved roles interact through the PSS. The underlying approach is process oriented.
Various, relevant individual IS interacts with patients and professionals through the PSS.
The PSS may be viewed as a layer of abstraction or user interface above the various individual IS, enabling enactment of the process and interaction between patients and professionals through computers and mobile devices, without accessing each individual system. 15 The PSS drives the process forward ensuring that it is carried out properly and, hence, supports the users in their work. The PSS also provides a user interface to the various systems involved in performing a task. The principle is described in Figures 1 and 2.
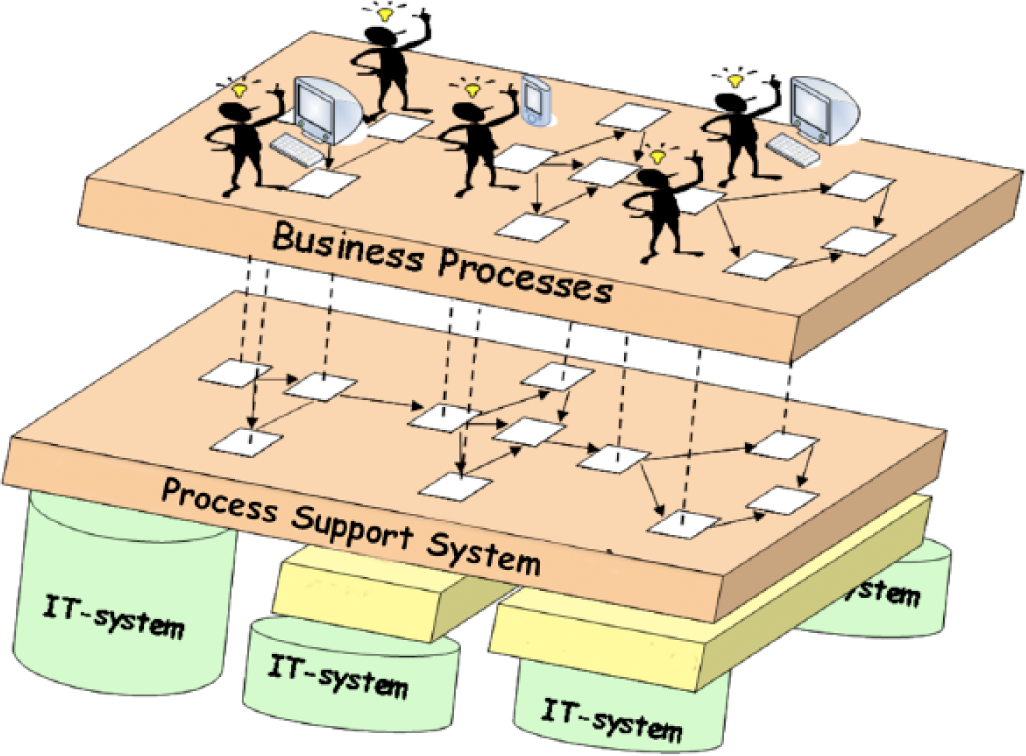
The principle of the PSS (adapted from Perjons et al. 14 ).
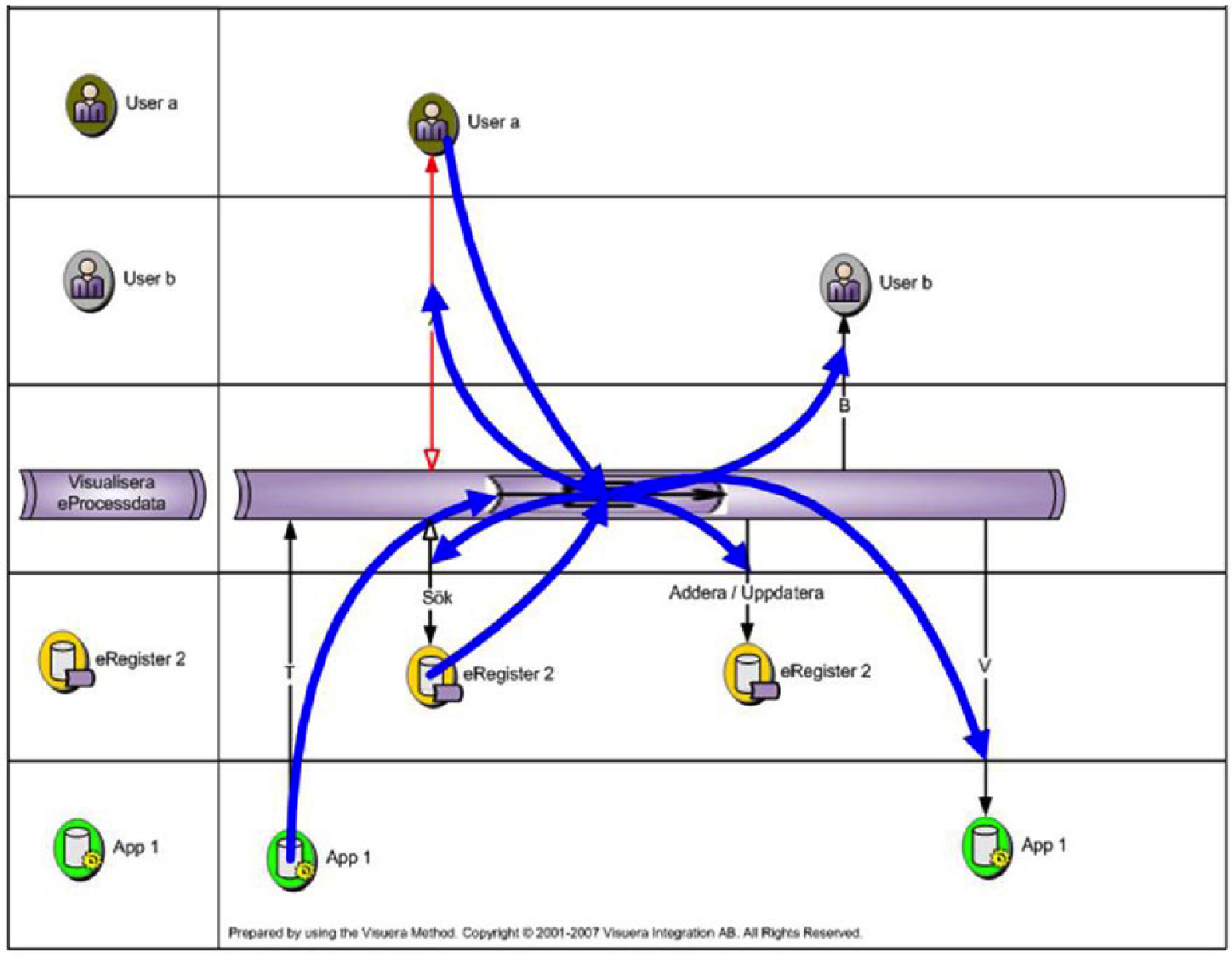
Communication between user, PSS and IS (adapted from Visuera Integration AB 20 ).
Furthermore, this architecture makes it possible, at least in theory, to replace individual IT systems without necessarily significantly affecting the user.
The PSS connects the following aspects:
Relevant patient information, both medical and administrative.
Process control providing integrated support for the user.
Medical knowledge through integrated links to internal and external sources of medical knowledge and other kinds of decision support.
In the PSS, process data can be collected, regarding how each instance of the process is executed. This enables various types of quantitative evaluation of processes, for instance, the waiting time between activities can be traced in order to identify bottlenecks.
Key design principles for PSS
This section describes the key design principles for PSS and how they are related and implemented in the PSS.
The patient process in focus
Due to the lack of a holistic approach from the patient’s perspective, for example, information that does not follow the patient satisfactorily between health care providers, the PSS has been designed to follow the patient’s path through the health care system. This is visualized by showing how the patient sends an own care request to primary care, participates in an appointment in primary care, is referred to specialist care and participates in an appointment in specialist care.
Another important key principle was to include both medical information (e.g. medical record, lab-response, drug list) and administrative information (e.g. appointments) in the PSS, following the idea that all information needed by patients and professionals when preparing for and carrying out an appointment should be at hand, regardless of whether it is medical or administrative. Medical and administrative information is currently often separated in different systems.
When the patient leaves the consultation room, it is not always easy to remember what was decided during the visit. Often the patient goes directly to the nurses in the waiting room and asks, ‘What did the doctor say?’ Therefore, the PSS enables the physician to briefly document the patient’s disease and the medical actions taken for the patient. This can be in paper or electronic form. In the latter case, it can be accessed later through the patient view in the PSS.
Shared goal for the patient visit
To overcome the lack of a common vision for the patient visit, 4 the PSS provides an opportunity for patients to state their expectations beforehand. It is important to emphasize that just because the patient indicates his/her expectations it does not mean that they will be fulfilled. Instead, the aim is that the patient’s expectations should be made clear to the professional involved so that the expectations can be addressed and discussed.
PSS is based on standardized information
Having the right information when it is needed is a challenge in the health care context. To make this possible, it is essential that the information is standardized and structured. In order to achieve this in the PSS, the information content of the national quality registers for selected diagnoses has been used. The types of information stored in quality registers have been transformed into checklists for each diagnosis. A further challenge was to provide the correct information for each level of care.
Efficient information flows
Using a process-oriented approach, the information flow can be more efficient. The PSS can ensure that patients and professionals carry out the appropriate activities in different parts of the process. The challenge here is to define, in today’s decentralized health care, which health care provider should be responsible for which activity and what information should be provided to the PSS.
Furthermore, it is important to ensure that certain necessary information sets are completed. The PSS should ensure that such information is not omitted.
A major advantage of a process-oriented approach and tools to support the process is that the PSS drives the process forward. When a task is completed, it will initiate and show nearby activities. For example, when the professionals in specialist care have written and signed the final documentation for the patient record, PSS automatically picks up the form ‘response to care request’ that will be sent back to primary care.
The right information at the right time, in the right place and for the right person is a vision strongly related to patient safety. By using the PSS that drives the process forward to the right person (predefined roles), place (e.g. the right level of care) and time (no unnecessary intermediate storage or manual handling), while the right information (standardized checklists designed according to the national quality register) follows throughout the whole process, a more efficient information flow can be achieved. Another consequence of the above approach is that it minimizes duplication of documentation. Already registered information comes with the whole process and does not need to be entered again.
Digital booking and coordination of patient treatments and examinations
In the PSS, it is possible to book treatments and tests and to see the status of these activities. When, for example, a plan is made for a hip osteoarthritis patient, the PSS provides support for prioritization using checklists showing obligatory and recommended treatments/tests. Furthermore, another care provider in the process should be able to view made orders including the status. If some activities, such as lab tests, are not completed before the scheduled visit, they can be cancelled in advance. This saves the patient the inconvenience of comming to the consultation and then being sent home.
Enhanced security
In the current version of the PSS, no specific technical security solutions are implemented. Instead, it is based on the assumption that the current national system for secure identification and access controls, including existing and secure infrastructure platforms, has been implemented. Implementation of national security solutions is required for systems that deal with information which follows the patient in his/her care process. Otherwise, they will not operate under existing laws and regulations. However, patient safety is further improved when information management is controlled by a PSS in a standardized manner. The PSS can, based on the information content, ensure that sensitive information is not disclosed.
Increased coordination with secure infrastructure
Another step towards improving security, and also towards increasing the coordination between different health care organizations, is the outlined integration with national solutions, such as the National Patient Summary (NPS), which contains excerpts from patient records kept by different health care providers. In the patient’s view of the PSS, the patient can access their own NPS. It is also possible for both professionals and patients to access NPS in their PSS views.
Results and print screen examples
This section describes the resulting PSS.
PSS design
To clarify the future PSS function and usage, two scenarios were designed: one for a hip osteoarthritis patient and one for an angina patient. In both scenarios, the patient first seeks admission to the primary health care centre, after which he/she is referred to specialist care with a following visit. This means that each scenario implements two patient visits, one at the primary care and one at specialist care. Sending and planning the ‘care request’ precede both visits. The scenarios were developed in collaboration with doctors and nurses at a local hospital in the Region of Västra Götaland in Sweden.
Hip osteoarthritis scenario
The hip osteoarthritis scenario concerns a 55-year-old man who has been a sportsman for many years and has accumulated pain for a long time. The patient cannot currently play tennis due to hip pain. In addition, he is self-employed and does not want to be on sick leave for long periods.
Angina pectoris scenario
The angina pectoris scenario concerns a 67-year-old man, a former mechanic who is married and has two children. He has worked for 43 years and has taken early retirement for labour market reasons. The patient has previously been treated for chest pain and takes medicine for high blood pressure.
Views for different roles in the future state process
There are three general views in the PSS, representing the main roles in the target process: the Patient View, the Care Planner View and the Patient Visit Leader View. Patient Visit Leader is defined as the professional (e.g. doctor or nurse) who is responsible for the patient visit. Care Planner is defined as the professional (e.g. nurse or secretary) who prioritizes patients and plans the upcoming visit. These views are repeated in both primary care and specialist care.
Patient View
The Patient View (Figure 3) should be accessed through a national health portal. The idea is that the patient logs in with secure identification and strong authentication mechanisms using national solutions for secure infrastructure. Patients also have the option to upload their profile. In the upper part of the view to the left, credentials showing the patient’s name and social security number are presented. To the right, a direct link to the NPS in which the patient can see the nationally stored patient information, as well as an entrance for creating a new care request, has been made available. The process starts by creating a care request and selecting the care unit. An inbox with unread read and untreated messages is found in the left part of the view. There is also storage provision for processed messages. In the middle of the view, there is a message box where the patient receives the messages displayed. In the lower part of the view, there is a task management field which allows the patient to see his/her upcoming visits as well as history from completed ones. The field of active cases are colour coded. Yellow illustrates waiting, for example, for an upcoming visit (Figure 3). This indicates that more information will be given, for example, confirmation of the appointment. Red illustrates action – the patient should give some response, for example, fill in a health declaration. Green illustrates that the visit is ready to be carried out – all necessary planning and information gathering has been completed before the patient visit. Figure 3 shows a picture of the Patient View in which the patient, Tommy Johansson, is logged. He has made two visits, one at the health care centre in Lerum and one at the orthopaedic clinic at a local hospital. The message field displays information from the last visit. The digital documentation that Tommy asked for is now available in the message field. The upcoming visit field shows that Tommy has a surgical appointment. This field is also highlighted in yellow, indicating that further information to the patient about the surgery will come later.
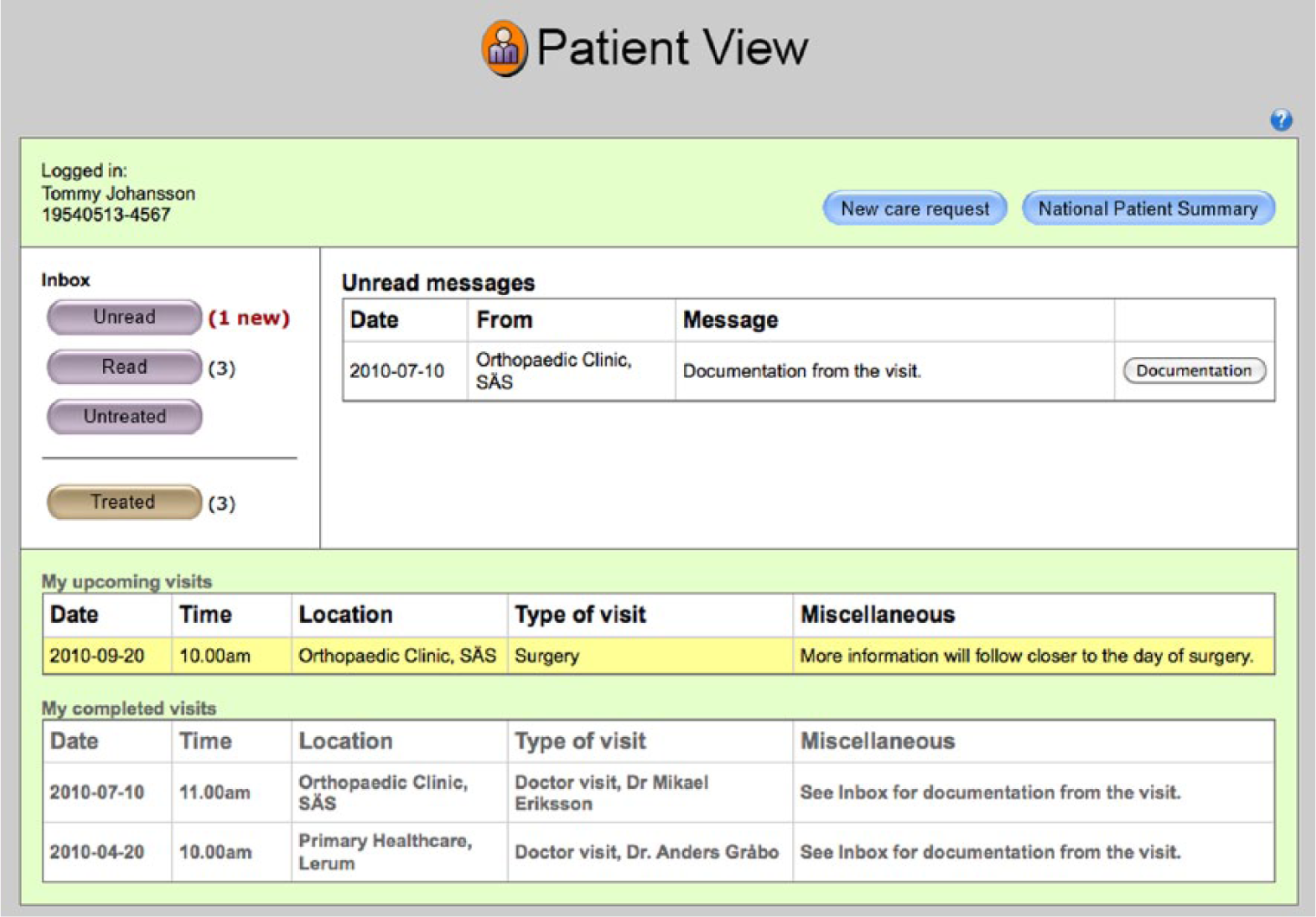
Overview of the patient view.
Care Planner View and Patient Visit Leader View
The layout of the Care Planner View and Patient Visit Leader View is basically the same as in the Patient View, but in a simpler form. The upper left part of the view shows the credentials of the person who is logged on. In the PSS, only the roles of care planners and patient visit leader are implemented. The left part of the view contains an inbox with unread read and untreated messages. Processed messages can also be accessed. In the middle of the view, there is a message box which displays received messages.
Snapshot of the patient’s ‘care request’
Figure 4 illustrates how the PSS, in this case the ‘own care request’, is based on standardized checklists designed from national quality registers.
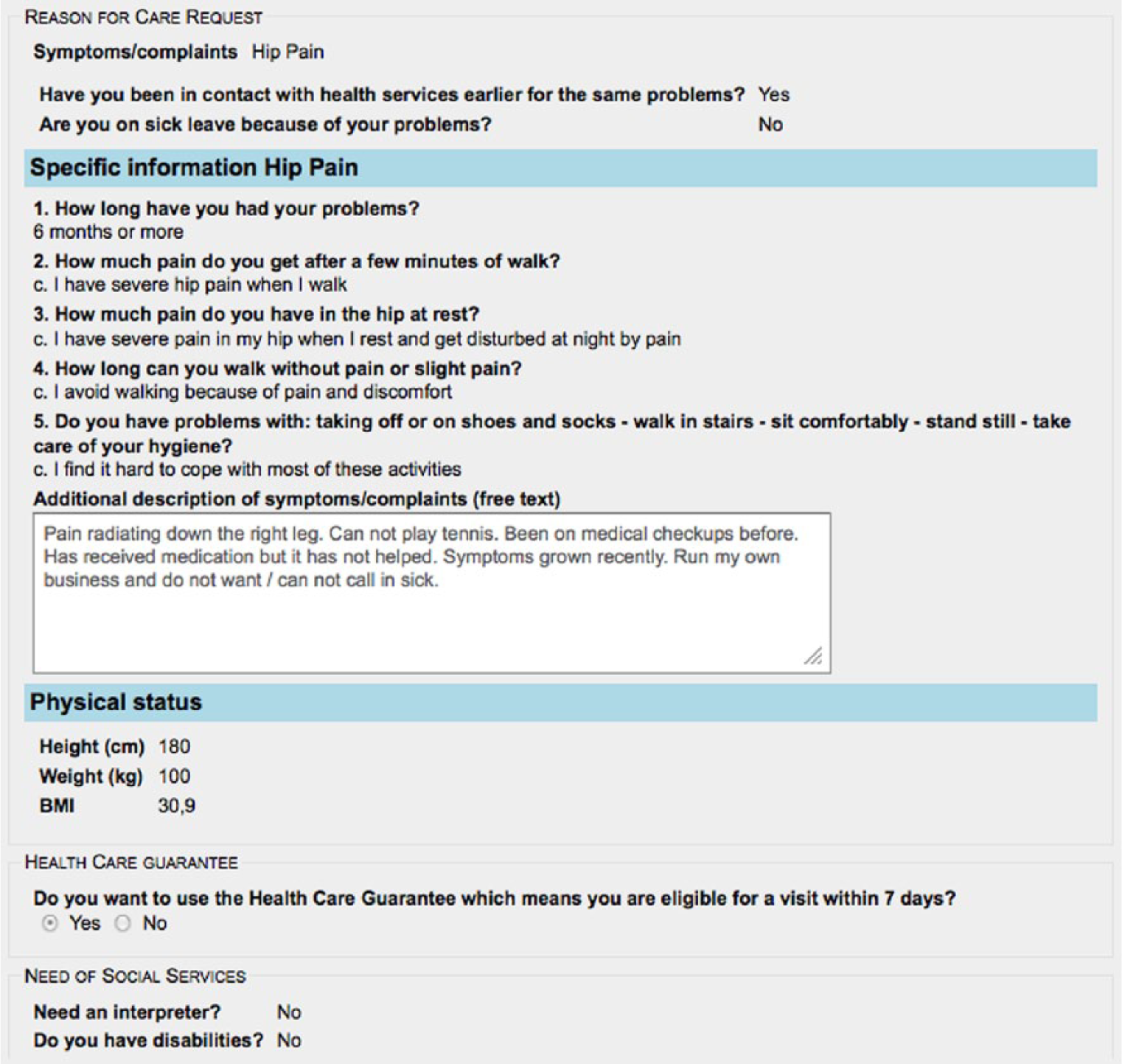
A snapshot of the patient’s digital ‘care request’ in the Care Planner Vie4.3 Description of the PSS process flow.
When the patient fills in the symptom/disease, for example, hip pain, the patient is requested to provide specific information related to the hip pain, depending on his/her situation and reality. When the patient has submitted the ‘own care request’ to primary care for further planning, the role of Care Planner checks the information and plans for further actions. This information then follows the patient throughout the entire care process, regardless of the level of health care organizations involved in the patient process. It should be noted that only health professionals involved in the patient’s care have access to the information.
A more detailed description of each part of the patient visit process, primary and specialist care follows.
Part 1: primary care
The process begins when the patient from the PSS patient view electronically fills in his/her ‘own care request’ and forwards it to primary care. At primary care, the ‘own care request’ is planned and prioritized by the role of Care Planner. A confirmation is then sent back to the patient who is prompted to complete the health declaration for the upcoming primary visit. Patients can also fill in their expectations for the visit. The patient subsequently enters the health care centre and the patient visit starts. The role of Patient Visit Leader, that is, the professional (e.g. doctor or nurse) that meets with the patient, has had the opportunity to access information about upcoming visits in the Patient Visit Leader view of the PSS and can there see clearly which patients are ready for their visit. The Patient Visit Leader can also access the patient’s ‘own care request’, the submitted health declaration and any expectations that the patient has stated.
During the patient visit, the Patient Visit Leader concludes that the patient needs to be referred to the next level of care, which in these scenarios is specialist care. The Patient Visit Leader therefore completes, in the PSS, a care request (referral) to specialist care, and assesses what other measures should be taken. Thereafter, documentation is provided to the patient digitally through the PSS Patient View or in written form. It is also possible for the Patient Visit Leader to begin documentation during the visit through the Patient Visit Leader View of the PSS. Thereafter, the patient visit is concluded and documentation in the patient’s health record is completed and signed. The information is transferred automatically to the underlying individual IS (Figure 1).
When the patient comes home, he/she may access his/her patient record via the Patient View of the PSS. Information about upcoming visits and treatments can also be accessed from the Patient View.
Part 2: specialist care
At specialist care, the care request is planned and prioritized. Confirmation of the date for the visit is then sent to the patient, together with necessary information about the patient’s condition, through the Patient View. Also, a new health declaration, targeting the specific information that specialist care needs, is made available to the patient through the Patient View. The patient completes the health declaration which is then made available to specialist care through the Care Planner View.
The Patient Visit Leader may in his/her view see upcoming visits, whether the patient is ready for the visit, and access available information about the patient. When the patient arrives for the visit, health related actions to be initiated are considered. The Patient Visit Leader will also continue the process by documenting in the patient record via the PSS and write the documentation that is provided to the patient. As the patient visit ends, the documentation is finalized by the Patient Visit Leader who chooses whether to dictate the note using noted information as a support or to write the additional information directly in the PSS. The next step in the process is to verify and sign the documentation. Thereafter, the Patient Visit Leader writes a ‘care request response’, which is sent via the PSS back to the health care unit that originally sent the request for care in this case the primary care.
Discussion
The following aspects are linked together in the PSS:
Relevant patient information, both medical and administrative.
Process control providing integrated support for the user.
Medical knowledge through integrated links to internal and external sources and other kinds of decision support.
In the PSS, so-called process data collected about each instance of the process is executed. This provides opportunities for different types of a more quantitative follow-up. For example, waiting times between different activities can be followed up to identify bottlenecks.
Much work remains before the above presented suggested principles for a PSS can be fully implemented. We have identified the following main challenges for developing a fully functioning PSS.
The interfaces between PSS and the underlying IT systems need to be developed
The PSS requires standardized information exchange between individual IT systems and the PSS. Perhaps the biggest challenge is that concepts used are frequently defined and written in different formats in different systems. This is particularly difficult for key concepts. One example is the social security number that is sometimes written in different ways in the existing systems. It is not just a question of how this is technically possible, it is also a question of information quality. Poor information quality causes unnecessary risks for the patient.
PSS usability for the patients, need to be secured
In the PSS, certain documentation is made available to the patient after the visit. This means that documentation in the patient record will have a new, more communicative role in the patient process. One challenge will then be to ensure that the patient is able to assimilate the information. This relates to the fact that patients perceive problems in communication with health care, in terms of language barriers. 4
Inclusion of all patients in using the PSS
The question whether all patients can be expected to make use of a computerized solution for communication with health care has been raised during the validation. It is worth noting that this has never been the purpose in the design of PSS. Since patients have different requirements and conditions for communicating with health care, several options must be available to patients. However, from a patient perspective, there are considerable benefits in having a secure, computerized channel of communication.
Cross-organizational responsibility for managing the PSS
Besides detailing how the various design principles can be implemented efficiently in the PSS, development and further research must, above all, be carried out in terms of ownership and responsibility of a PSS that crosses organizational boundaries and supports patient-centred care. For example, who owns all the process data generated in the PSS, who takes responsibility for the quality of the process data, who will be the process owner of the entire patient process? If the technical challenges can be solved, this will be the biggest challenge for implementing the PSS.
Concluding remarks
This article has presented a prototype that visualizes the future of information management as a solution to the problems identified in earlier research. However, we can conclude that a visualized prototype is a suitable tool to illustrate both the opportunities and constraints of future ideas and solutions. Nevertheless further research is clearly needed, particularly addressing the identified challenges, for instance, the responsibility for PSS, that cross health care organizational boundaries, the ownership of process data and the quality of information flows both for professionals and patients.
Health care information management is a complex task which forces IS to be able to manage this complexity. Reliable health care information is also an important condition for obtaining high-quality care. Therefore, future IS need to support both patients and professionals in carrying out their respective roles. This requires that health care IS are more process oriented from the perspective of the patient process, structured, standardized and, above all, are more patient-centred. 19 A PSS, as proposed in this article, is one step towards that direction.
Footnotes
Acknowledgements
Special thanks to the health care professionals at Södra Älvsborgs hospital for great collaboration.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The Future Healthcare Information Systems (FHIS) project was funded by Region Västra Götaland and the University of Skövde.